
Abstract
Recent research suggests that mild traumatic brain injury (TBI) may exert deleterious effects on endogenous pain modulatory function, potentially underlying the elevated risk for persistent headaches following injury. Accumulating research also shows race differences in clinical and experimental pain, with African Americans (AA) generally reporting more severe pain, worse pain modulation, and greater pain sensitivity compared with Caucasians. However, race differences in pain-related outcomes following mild TBI have rarely been studied. The purpose of this study was to explore race differences in endogenous pain modulation, pain sensitivity, headache pain, and psychological factors among AA and Caucasian individuals with mild TBI in the first month following injury compared with healthy controls and across time. Patients with mild TBI were recruited from local emergency department trauma centers. Sixty-three participants with mild TBI (AAs: n = 23, Caucasians: n = 40) enrolled in this study and completed study sessions at 1–2 weeks and 1-month post-injury. Forty-one mild-TBI-free control participants (AAs: n = 11, Caucasians: n = 30), matched on age and sex, completed one study session. Assessments included a Headache Survey, Pain Catastrophizing Scale, Center for Epidemiological Studies—Depression Scale (CES-D), and quantitative sensory testing (QST) to measure endogenous pain modulatory function. QST included conditioned pain modulation (CPM) to measure endogenous pain inhibitory function and temporal summation (TS) of pain and pressure pain thresholds (PPTs) of the head to measure pain sensitization and sensitivity. Two-way analysis of variance (ANOVA) was used to determine whether the outcome measures differed as a function of race, mild TBI, and time. Mediation analysis was used to explore potential mediators for the race differences in headache pain intensity. The results showed that AA participants with mild TBI reported significantly greater headache pain and pain catastrophizing and exhibited higher pain sensitivity and worse pain modulation on QST compared with Caucasian participants with mild TBI. These same race differences were not observed among the healthy TBI-free control sample. The mediation analyses showed complete mediation for the relation between race and headache pain intensity by pain catastrophizing at 1–2 weeks and 1-month post-injury. Overall, the results of this study suggest that AAs compared with Caucasians are characterized by psychological and pain modulatory profiles following mild TBI that could increase the risk for the development of intense and persistent headaches following injury.
Introduction
Epidemiological studies suggest that at least 3.5 million adults experience traumatic brain injuries (TBIs) each year in the United States, 1 with the majority of TBIs classified as mild. 2 Accumulating research suggests racial and ethnic disparities exist in the incident rates, health care, and research efforts of TBI. For example, the literature on moderate to severe TBI documents higher incident rates of TBI, less effective medical care, and poorer outcomes following injury among racial minorities, including African Americans (AAs). 3,4 Less is known regarding racial differences in mild TBI, although the limited research suggests similar trends as found in moderate to severe TBI. 5 Alarmingly, a high percentage of research studies on TBI do not report specific information regarding the racial or ethnic composition of the samples. 3 Thus, further investigation is warranted to explore whether racial and ethnic disparities exist in health outcomes following mild TBI.
One of the most common, disabling, and chronic symptoms following mild TBI is the post-traumatic headache. 6 The mechanisms underlying the development of chronic pain following a mild TBI are likely multi-faceted but still not well defined. Patients with mild TBI often experience post-traumatic stress following injury, 7 including depression, anxiety, and pain catastrophizing. 8 Substantial evidence in the pain field demonstrates the significance of these psychological factors in influencing pain-related experiences, including post-traumatic headaches. 9 –12 Studies also show that mild TBI is characterized by deficient and unbalanced endogenous pain modulatory function (i.e., decreased pain inhibition on the conditioned pain modulation [CPM] test, increased pain sensitization on quatitative sensory testing [QST]) after the head injury, which likely contributes to the development of chronic pain. 13,14 For example, we have previously shown in a longitudinal study that reduced pain inhibition on the CPM test in the first month after mild TBI predicts the occurrence of persistent post-traumatic headaches 4 months after a mild TBI. 13 Importantly, racial differences in clinical and experimental pain outcomes have been reported in studies on healthy adults, and on individuals with pain due to motor vehicle accidents and other chronic pain conditions. 15 –17 However, to our knowledge, no research has considered the impact of race on pain-related outcomes following mild TBI.
Thus, the primary purpose of this study was to explore race differences in pain outcomes among AA and Caucasian patients with mild TBI in the first month following injury, compared with healthy controls and across time. A secondary aim of the study was to investigate potential mediators for the race differences in headache pain intensity. Headache pain intensity, QST of endogenous pain modulation and pain sensitivity, pain catastrophizing, and depression were measured in a sample of participants with mild TBI at 1–2 weeks and 1-month following mild TBI. These same measures were collected in a healthy mild-TBI-free control group at a single time-point. We hypothesized that AA patients with mild TBI would exhibit greater pain sensitivity, worse pain modulation on dynamic QST, and increased depression and pain catastrophizing compared with Caucasian patients with mild TBI. We also hypothesized that race differences in headache pain would be mediated by QST or psychological variables.
Methods
Participants
These data are part of a larger study that assessed risk factors for persistent post-traumatic headache. 8,13 This study explores differences in the outcomes between participants with mild TBI who identified as AA or Caucasian. Mild TBI was defined according to the criteria endorsed by the World Health Organization Task Force, 18 which included: 1) a Glasgow Coma Scale score between 13 and 15 when assessed at an emergency department; 2) a computed tomography scan of the head that indicates no abnormal findings, to rule out secondary disorders (i.e., cerebral hemorrhage or vein thrombosis, hematoma); and 3) the occurrence of one or more of the following symptoms: post-traumatic amnesia for <24 h, disorientation or confusion, or a loss of consciousness (LOC) for <30 min. Further, symptoms of the mild TBI cannot be caused by other injuries or treatments for other injuries, medications, drugs, alcohol, a penetrating craniocerebral injury, or by other problems such as psychological trauma or coexisting medical conditions. Also, patients with mild TBI and polytrauma (e.g., fractures, sprains, dislocations, but not minor bruises or scrapes) were excluded. All participants with mild TBI enrolled in this study were seen at a Level 1 trauma center for their mild TBI.
Control participants who had never experienced a TBI were also enrolled in this study. We attempted to match control participants to participants with mild TBI based on age, sex, and race. All participants had to be between 18 and 65 years of age at the time of enrollment. Exclusion criteria for mild TBI and control participants were the following: metabolic disease (e.g., diabetes), uncontrolled hypertension, chronic cardiovascular disease (such as coronary artery disease, myocardial infarction, heart failure, cardiomyopathy, valvular disease), renal disease, serious psychiatric conditions (e.g., schizophrenia, bipolar disorder) or hospitalization in the previous year for psychiatric illness, neurological disease (e.g., Parkinson's disease, multiple sclerosis, epilepsy), chronic headaches defined as 15 days or more of headaches per month over a 3-month period (before the mild TBI for mild TBI participants), chronic opioid use (e.g., have a prescription for opioids or have taken them on a regular basis for the past month), current involvement in litigation, and current use of narcotics.
Recruitment
Adults with mild TBI were recruited from three Level 1 trauma centers located in Indianapolis. Study recruiters screened the electronic medical records of patients with a head injury who were admitted to the emergency department. The recruiters identified whether patients met the inclusion and exclusion criteria. The attending emergency department physician also confirmed the diagnosis of mild TBI via e-mail or verbally. The identification and contact information of potentially eligible patients with mild TBI was put into a secure database. Then, the research staff called or e-mailed the potential participant within 48 h to determine whether the individual was interested in the study and to review the inclusion and exclusion criteria again with the participant. For individuals interested and potentially eligible, the first study visit was scheduled within 2 weeks of the injury. Mild TBI participants had to be enrolled in the study within 2 weeks of their injury. Based on recruitment data from two of the trauma centers, approximately 22% of individuals who were potentially eligible based on their emergency department visit were actually enrolled in the study. The percentage enrolled from the third trauma center is unknown.
Research staff directly recruited the control participants based on the demographics of the mild TBI participants. Controls were recruited from the Indiana University Purdue University Indianapolis campus and local community with e-mail advertisements and flyers. Individuals interested in the study contacted the research staff via phone or e-mail. The interested individuals then received more information about the study. Individuals who were still interested, potentially eligible, and a match based on race, age, and sex to a participant with mild TBI were then scheduled for a study visit for enrollment.
Procedures
This study was approved by the Indiana University and Ascension St. Vincent Indianapolis Hospital Human Subject Review Boards. Participants with mild TBI were asked to complete three study visits, with visit 1 occurring within 2 weeks after the injury, visit 2 occurring approximately 1-month post-injury, and visit 3 occurring 4–6 months post-injury. Due to sample size issues, this study focused on the data collected at visits 1 and 2. Control participants completed one study visit. During the first visit, participants reviewed and signed an institutional review board-approved written informed consent. Participants also completed a health history questionnaire, supplemented by interview and blood pressure measurement to verify that participants met the inclusion and exclusion criteria. The health history questionnaire also collected demographic information, including asking participants to identify their race. Participants were asked to check one of the following options for race: African American, Asian/Pacific Islander, Caucasian, Hispanic, Native American, or Other. After eligibility was established, participants completed several QST tests and questionnaires. These assessments were also collected in visit 2 for participants with mild TBI, and they are described below. All participants were asked to not consume caffeine or take pain-relief medication on the day of study visits prior to the visit.
Outcome measures
Questionnaires
Pain Catastrophizing Scale (PCS)
The PCS includes 13 items that evaluate respondents' emotional and cognitive responses to actual or anticipated pain. 19 Participants rate on a Likert scale from 0 (not at all) to 4 (all the time) the degree to which they have various thoughts and feelings related to pain. A total score (ranging from 0 to 52) and three subscale scores of rumination, magnification, and helplessness can be calculated. Higher scores indicate greater pain catastrophizing.
Headache Survey
Participants completed a Headache Survey that has been utilized in prior research of post-traumatic headache. 6,20 The survey included questions regarding the intensity of headaches, frequency of headaches, duration of headaches, medication use and other treatments, headache triggers, pre-injury history of headache, and symptoms of ongoing headache. Participants were asked to rate on a 0 to 10 numeric rating scale (NRS) the average pain intensity of their headaches during the past week, with 0 indicating no headaches at all and 10 indicating the worst pain possible. This pain intensity rating was used in data analysis.
Center for Epidemiological Studies—Depression Scale (CES-D)
The CES-D includes 20 items that assess symptoms associated with depression. The total score ranges from 0 to 60, with higher scores indicative of increased depression. The CES-D is valid and reliable in the general and clinical populations. 21 A cutoff score of ≥16 suggests risk for clinical depression. 22
Measures of pain modulatory function and pain sensitivity
Participants were first familiarized with each QST test and taught the 0–100 pain rating system. The temporal summation (TS) of pain test was performed first, followed by pressure pain thresholds of the head, and then the CPM test. At least 10 min separated each QST test.
Mechanical temporal summation (MTS)
TS of pain is an indirect method of assessing hyperexcitability of the central nervous system (CNS). 23 MTS was assessed on the middle of the forehead and the back of the hand with a von Frey filament (Touchtest Sensory Evaluator 6.65) calibrated to bend at 300g of pressure. TS on the forehead was assessed while the participant was lying down on an exam bed. TS on the hand was assessed while the participant was sitting in a chair with the hand resting on a hard surface. A single pinprick with the von Frey filament was first applied to the body site. Participants rated the perceived pain intensity of the pinprick using the 0 (no pain at all) to 100 (worst pain imaginable) NRS. Then, 10 pinpricks with the same monofilament were administered to the same body site within an area of 1 cm2 and at a rate of 1 prick per sec. Immediately following the 10 pinpricks, participants rated the greatest pain intensity experienced using the 0–100 NRS. The MTS score was calculated by subtracting the pain rating after the first stimulus from the pain rating after the 10 stimuli. The MTS procedure was completed two times at each body site with 60 sec between trials. The two trials at each body site were averaged for a single MTS forehead score and a single MTS hand score.
Pressure pain thresholds (PPTs) of the head/neck area
As have been conducted in prior research, 24 PPTs were administered on five sites of the head and neck areas including the middle of the forehead, the left temple, the parietal area (top of head), the posterior neck/vertebral level C2, and the left trapezius. Pressure was applied to each body site with a digital, handheld algometer (AlgoMed, Medoc Advanced Medical Systems, Durham, NC, USA) that had a 1.0 cm2 probe. Pressure was applied gradually and increased at a slow constant rate of pressure (30 kPA/sec). Participants were instructed to verbally identify when they first experienced pain caused by the pressure algometer. Then, the algometer was immediately removed. Two trials were administered at each body site with 20 sec separating each trial. The PPT scores at all the head/neck sites were averaged for a single PPT score (PPT-Head), which was used in the data analysis. 24
Conditioned pain modulation (CPM)
The most commonly used assessment of endogenous pain inhibition in humans is CPM. CPM represents a “pain-inhibition-by-pain” paradigm, in which pain produced by a test stimulus is reduced by a second noxious conditioning stimulus applied at a remote body site. 25,26 To assess CPM, PPTs (test stimulus) on the left volar forearm were administered before and immediately after the submersion of the right hand in a cold-water bath (conditioning stimulus). Participants sat quietly for 7 min between the administration of the pre-conditioning PPT trials and the start of the conditioning stimulus. This 7-min period was included to prevent within-session adaptation. 27
Test stimulus: The test stimulus was administered using the same PPT threshold procedures as described above (except different body location) on the left volar forearm. Two trials were conducted consecutively for each pre- and post-conditioning test. The post-conditioning trials were conducted immediately after participants removed their hand from the cold-water bath (conditioning stimulus). The PPT trials were averaged for a single pre-conditioning and post-conditioning PPT score.
Conditioning stimulus: Participants put their right hand up to the wrist in a cold-water bath (VersaCool 7, Thermo Scientific) for 1 min. The temperature for the water was maintained at 10°C. Participants were asked to rate the cold pain every 15 sec using the 0 to 100 NRS. The cold-water pain ratings were averaged for a single cold-water pain score for each participant.
Calculation of CPM: To measure the magnitude of CPM, a percent change score was calculated for the test stimulus using the following formula: [(post-conditioning PPT trial score – pre-conditioning PPT trial score)/pre-conditioning PPT trial score] * 100. A positive percent change score indicated that PPTs increased following the conditioning stimulus, indicative of pain inhibition.
Statistical analysis
We calculated descriptive statistics for all outcome variables. Chi-square tests were used to determine whether groups differed by sex, education, LOC and cause of head injury (mild TBI groups only), and frequency of headaches (mild TBI groups only). A 2 (Group: mild TBI, control) × 2 (Race: AA, Caucasian) between subjects ANOVA was conducted to determine whether groups differed by age. We conducted 2 (Group: mild TBI, control) × 2 (Race: AA, Caucasian) between subjects analysis of covariances (ANCOVAs) with sex added as a covariate to determine if the primary outcomes at 1–2 weeks post-injury differed as a function of race and mild TBI. Then, to determine whether the outcomes measures varied between races over time in the mild TBI participants, we conducted 2 (Race) × 2 (Time: Visit 1, Visit 2) mixed model ANCOVAs with repeated measures on time. Sex was added as a covariate. Follow-up tests to significant interactions were performed with Tukey's honestly significant difference (HSD) test. The p-value for significance was set at p < 0.05. Effect sizes were also calculated to determine the magnitude of difference in the outcome measures between races within the control and mild TBI groups separately. Cohen's d was defined as the AA group mean minus Caucasian group mean, divided by the pooled within group standard deviation (
We also examined the QST and psychological variables as potential mediators of the race differences in headache pain at 1–2 weeks and 1-month post-injury. Only QST and psychological variables that differed by race were tested as mediators. Analyses were conducted separately for the 1–2 week variables and the 1-month variables. We used Hayes' PROCESS macro SPSS 37 to examine these mediation models (Model 4). This mediation analysis used bootstrapping to perform inference tests for the indirect effects. 28,29 Path estimates and the indirect effects were produced using 95% bias-corrected bootstrap confidence intervals (CIs) based on 10,000 bootstrap samples. Paths were considered statistically significant when the 95% CIs did not contain zero. Sex was included as a covariate in all mediation analyses.
Results
Participant characteristics
The power analysis for the current study is reported below in the Transparency, Rigor, and Reproducibility Summary. Sixty-three participants with mild TBI (23 AA, 40 Caucasian) and 41 control participants (11 AA, 30 Caucasian) completed the first study visit. Seven participants with mild TBI withdrew before the 1-month visit and therefore 56 participants with mild TBI (20 AA, 38 Caucasian) also completed a second study session at 1-month post-injury. At the 1-week visit, 1 participant did not complete the PPT and TS assessments on the head (declined assessment because of extreme sensitivity of head), 2 participants did not complete the CPM test due to equipment malfunction, and 2 participants did not correctly complete the CES-D. Participant demographics by mild TBI group and race are presented in Table 1. Mild TBI and headache characteristics for the mild TBI group by race are presented in Table 2. The results indicated that the groups did not differ in age and distribution of sex, education obtainment, and household income (p's > 0.05). AA and Caucasian participants with mild TBI did not differ in the cause of head injury (p = 0.195), percent who experienced LOC during the mild TBI (p = 0.134), and frequency of headaches at 1–2 weeks (p = 0.249) and 1-month post-injury (p = 0.381). The most common causes of mild TBI for both races were falls and motor vehicle collisions.
Participant Demographics
HS, high school; TBI, traumatic brain injury.
Mild TBI and Headache Characteristics for Mild TBI Group
LOC, loss of consciousness; NSAIDs, non-steroidal anti-inflammatory drugs; TBI, traumatic brain injury.
Group and race differences in pain modulatory function and pain sensitivity at 1–2 weeks post-injury
Pain sensitivity of the head
See Table 3 for the means, 95% CIs, and effect sizes for all the primary outcome variables by race and mild TBI group at 1–2 weeks post-injury. The between subjects ANCOVA conducted on PPTs of the head revealed a significant race × group interaction (p = 0.001). First, control participants regardless of race had significantly greater PPTs of the head compared with all participants with mild TBI. AA controls had significantly greater PPTs compared with Caucasian controls. However, AA participants with mild TBI had significantly lower PPTs of the head compared with Caucasian participants with mild TBI.
Primary Outcome Measures (Means, 95% Confidence Intervals) at 1–2 Weeks Post-Injury
Data are reported as mean [95% confidence interval]; d = Cohen's d effect size.
Significant Group × Race interaction; bsignificant main effect of group; csignificant main effect of race.
CES-D, Center for Epidemiological Studies—Depression Scale; CPM, conditioned pain modulation; PPT, pressure pain thresholds; TBI, traumatic brain injury; TS, temporal summation.
Mechanical temporal summation (MTS)
The results revealed no significant main effects of race (p = 0.918) or mild TBI group (p = 0.762) and no significant interaction (p = 0.891) in mechanical TS on the hand. Similarly, no significant main effects of race (p = 0.513) or mild TBI group (p = 0.439) and no significant interaction (p = 0.239) were found for mechanical TS on the head.
Conditioned pain modulation
The analysis revealed a significant main effect of mild TBI group (p = 0.023), with participants with mild TBI having lower pain inhibition on the CPM test compared with controls, regardless of race. The main effect of race (p = 0.659) and the interaction (p = 0.254) were not significant.
Group and race differences in psychological factors and in headache pain at 1–2 weeks post-injury
Depression
The analysis on CES-D scores demonstrated a significant main effect of mild TBI group (p < 0.001) and race (p = 0.002). Participants with mild TBI had higher depression scores compared with controls. Also, AAs had higher depression scores compared with Caucasians, across both mild TBI groups. The interaction was not significant (p = 0.174).
Pain catastrophizing
The analysis revealed a significant race × mild TBI group interaction (p = 0.007). No differences existed between the AA controls and the Caucasian controls. All participants with mild TBI exhibited greater pain catastrophizing compared with control participants. Additionally, AA participants with mild TBI had greater catastrophizing compared with Caucasian participants with mild TBI. When evaluating the PCS subscales independently, a significant race × mild TBI group interaction was also present for the Rumination (p = 0.013), Magnification (p = 0.001), and Helplessness (p = 0.044) subscales. The same trend was found for each subscale, with AA participants with mild TBI having significantly higher scores compared with all other groups. No significant differences in subscale scores were found between the AA controls, Caucasian controls, and the Caucasian mild TBI group.
Headache pain
The between subjects ANCOVA demonstrated a significant race × mild TBI group interaction (p = 0.019). All participants with mild TBI reported significantly greater headache pain compared with all controls. Additionally, AA participants with mild TBI reported greater headache pain compared with Caucasian participants with mild TBI.
Race differences across time in pain modulatory function and pain sensitivity in mild TBI participants
Pain sensitivity of the head
Figure 1 shows the means and standard errors (SEs) of the pain sensitivity and pain modulation variables across time in Caucasian and AA patients with mild TBI. The mixed model ANCOVA conducted on PPTs of the head revealed no significant main effects of race (p = 0.096) or time (p = 0.071) and no significant interaction (p = 0.835).
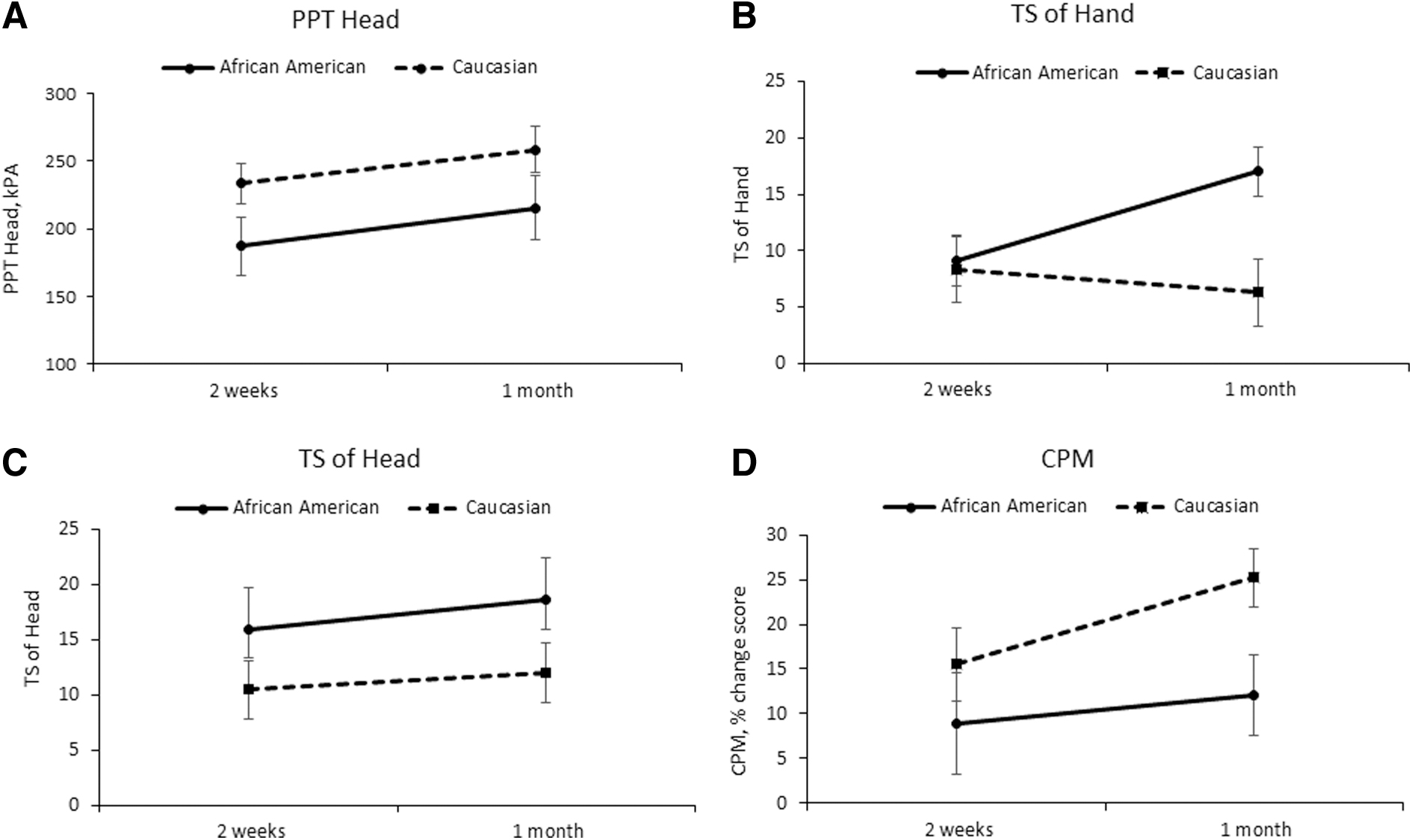
Experimental measures of pain at 1–2 weeks and 1-month post-injury in mild TBI patients. PPT, pressure pain threshold; TS, temporal summation; CPM, conditioned pain modulation.
Mechanical temporal summation (MTS)
The analysis conducted on TS of the hand demonstrated a significant race × time interaction (p = 0.034). AA participants with mild TBI demonstrated greater TS at 1-month compared with 1–2 weeks and compared with Caucasian participants with mild TBI at both visits. The analysis conducted on TS of the head revealed no significant main effects of race (p = 0.129) or time (p = 0.642) and no significant interaction (p = 0.815).
Conditioned pain modulation
The analysis revealed a significant main effect of race (p = 0.034), with AA participants with mild TBI (mean [M] = 10.5, 95% CI [3.2, 17.8]) having lower pain inhibition on the CPM test compared with Caucasian participants with mild TBI (M = 20.4, 95% CI [15.1, 25.6]), across time (d = −0.62). The main effect of time (p = 0.783) and the interaction (p = 0.468) were not significant.
Race differences across time in psychological factors and headache pain in mild TBI participants
Depression
Figure 2 shows the means and SEs of the headache pain and psychological variables across time in Caucasian and AA patients with mild TBI. The analysis on CES-D scores demonstrated a significant main effect of race (p = 0.029). AA participants with mild TBI (M = 23.1, 95% CI [18.4, 27.9]) had higher depression scores compared with Caucasian participants with mild TBI (M = 16.8, 95% CI [13.4, 20.2], d = 0.62). The main effect of time (p = 0.367) and the interaction were not significant (p = 0.230).
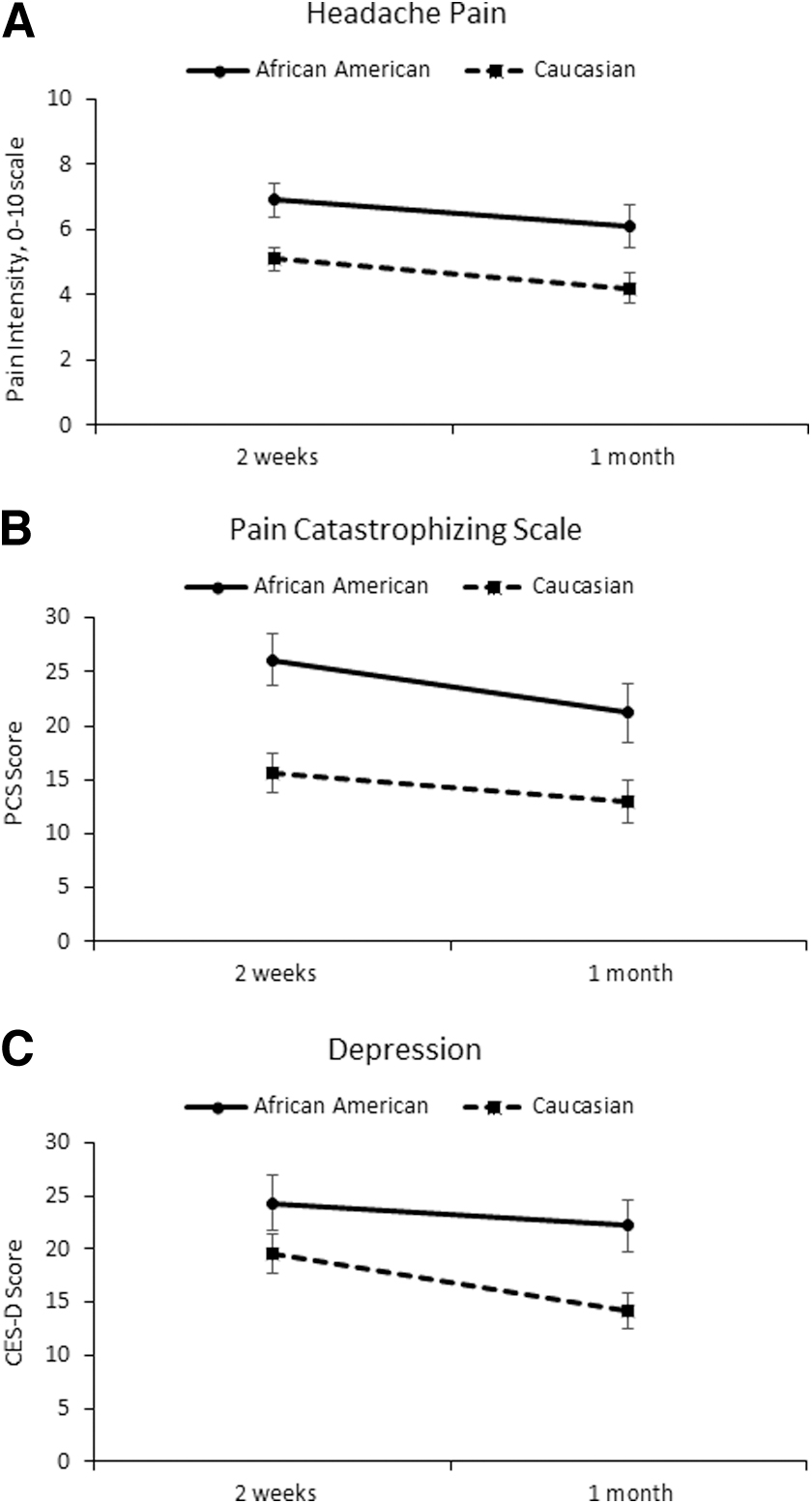
Clinical and psychological outcomes at 1–2 weeks and 1-month post-injury in mild TBI patients. CES-D, Center for Epidemiological Studies—Depression Scale; PCS, Pain Catastrophizing Scale.
Pain catastrophizing
The analysis on pain catastrophizing revealed a significant main effect of race (p = 0.003). AA participants with mild TBI (M = 23.6, 95% CI [18.9, 28.4]) had greater catastrophizing compared with Caucasian participants with mild TBI (M = 14.3, 95% CI [10.9, 17.8], d = 0.89). The main effect of time (p = 0.578) and the interaction (p = 0.398) were not significant. When evaluating the PCS subscales independently, the significant main effect of race was present for the Rumination (p = 0.001) and Magnification (p < 0.001) subscales, but not the Helplessness subscale (p = 0.122)
Headache Pain
The mixed model ANCOVA demonstrated a significant main effect of race (p = 0.006). AA participants with mild TBI (M = 6.5, 95% CI [5.4, 7.6]) reported significantly greater headache pain compared with Caucasian participants with mild TBI (M = 4.6, 95% CI [3.9, 5.4], d = 0.82). The main effect of time (p = 0.311) and the interaction (p = 0.820) were not significant.
Mediation analyses
Mediation analyses were conducted to determine potential mediators of the race differences in headache pain intensity in the mild TBI sample. The outcome variable was either headache pain intensity at 1–2 weeks or 1-month post-injury. The independent variable was race. Sex was added as a covariate. Pain catastrophizing was the only significant mediator for the race differences in headache pain intensity at each time-point. As shown in Figure 3, the model at 1–2 weeks predicted significant variance in headache pain intensity (p < 0.001). This model showed that race differences in headache pain intensity were completely mediated through pain catastrophizing. AA participants with mild TBI reported greater pain catastrophizing, which was associated with greater headache pain intensity. As shown in Figure 4, a similar model at 1 month also predicted significant variance in headache pain intensity (p = 0.004), with pain catastrophizing mediating the relationship between race and headache pain.

Mediation model showing how race group influences headache pain intensity at 1–2 weeks post-injury, mediated through pain catastrophizing. The direct effect of race on headache pain intensity was completely mediated by pain catastrophizing. *p < 0.05, **p < 0.01. Sex was included as a covariate. CI, confidence interval.
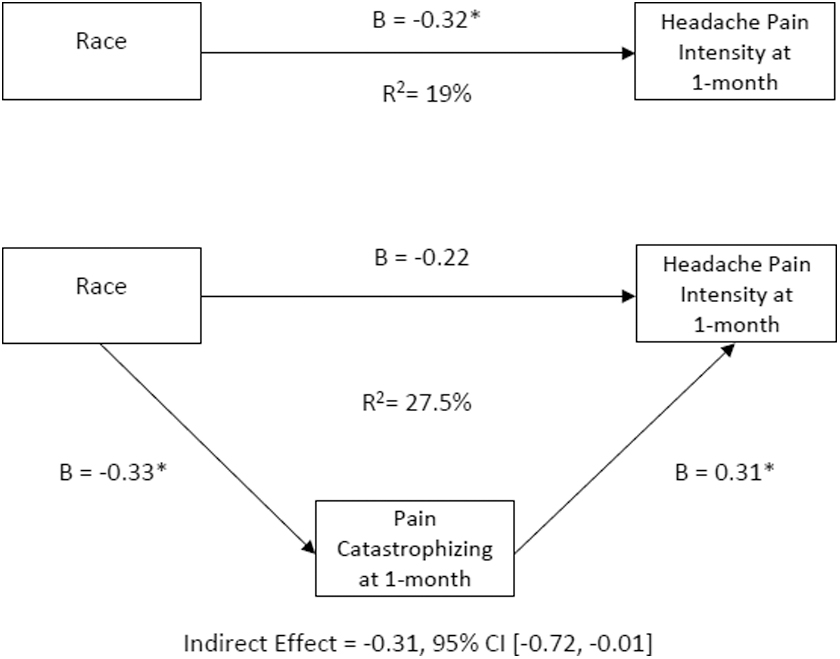
Mediation model showing how race group influences headache pain intensity at 1-month post-injury, mediated through pain catastrophizing. The direct effect of race on headache pain intensity was completely mediated by pain catastrophizing. *p < 0.05, **p < 0.01. Sex was included as a covariate. CI, confidence interval.
Discussion
Limited data are available regarding race differences in pain outcomes among individuals with mild TBI. Addressing this gap in knowledge, our study provides the first comparison of AAs and Caucasians on a comprehensive set of pain outcomes following mild TBI including experimental pain sensitivity, endogenous pain modulation, psychological factors, and clinical pain. As hypothesized, AA participants with mild TBI reported higher levels of headache pain and pain catastrophizing and exhibited higher pain sensitivity and worse pain modulation on QST tests compared with Caucasian participants with mild TBI. Importantly, these same race differences were not observed among a healthy TBI-free control sample. Further, we provided evidence for pain catastrophizing as a mediator of race group differences in headache pain intensity following mild TBI. These individual findings are discussed further below.
Patients with mild TBI are characterized by increased pressure pain sensitivity on the head early after the head injury. 8 The results of the current study identified race differences in pressure pain sensitivity in the control participants and patients with mild TBI, but only at the 1–2 week time-point. Surprisingly, AA controls had lower pain sensitivity compared with Caucasian controls. Other studies in healthy adults have shown no race differences 30 –32 or greater pressure pain sensitivity 33 in AAs compared with non-Hispanic Whites (NHWs). However, none of these studies measured pressure pain sensitivity on the head. It should also be mentioned that these studies had larger sample sizes for the AA groups compared with the current study's AA healthy control group (sample ranges 28–81 vs. 11). Thus, the AA control versus Caucasian control differences in PPTs in the current study should be interpreted with caution.
In the mild TBI sample, our hypothesis was supported. AA participants with mild TBI exhibited greater pressure pain sensitivity of the head compared with Caucasian participants with mild TBI at 1-week post-injury. Few studies have investigated race differences in pressure pain sensitivity in clinical populations, with findings consistent with our mild TBI data. These studies have focused on knee osteoarthritis and found increased pressure pain sensitivity at the knee in AAs compared with NHWs. 34,35 Race differences in pressure pain sensitivity likely depend on an interaction of the stimulation site and participant characteristics (e.g., healthy, knee osteoarthritis, mild TBI).
Collectively, animal and human research indicates that mild TBI may exert deleterious effects on endogenous pain inhibitory function early after the injury, 14,8 increasing the risk for persistent post-traumatic headaches following injury. Supporting this research, our results revealed decreased pain inhibition on the CPM test in participants with mild TBI compared with controls at 1–2 weeks post-injury. Race differences in CPM only became evident once the 1-month CPM assessment was also included in the analysis. Inspection of the data indicated that although both AA and Caucasian participants with mild TBI trended toward increased pain inhibition from 2-weeks to 1-month post-injury, the magnitude of improvement appeared much larger for Caucasian participants. Thus, by 1-month post-injury, Caucasian participants with mild TBI exhibited CPM scores that were in a similar range to the control participants (20–30% CPM score range), whereas this was not the case for AA participants with mild TBI. Prior evidence for differences in CPM between AAs and Caucasians is mixed in healthy adults 32,33,36,37 and extremely limited in clinical populations. In patients with knee osteoarthritis, Cruz-Almeida and colleagues found that AAs exhibited pain facilitation during the CPM protocol, whereas NHWs had no changes in pain ratings. 34
As a measure of pain facilitatory processes in the CNS, TS of mechanical pain was measured on the forehead and hand in the current study. Elevated TS is characteristic of many chronic pain conditions 24,38,39 and may increase risk for chronic pain. 40 Prior research showed increased TS of pain in AAs compared with NHWs in healthy and chronic pain populations (i.e., knee osteoarthritis, low back pain). 34,41 The results of the current study indicated that TS was not elevated in the participants with mild TBI compared with controls at 1-week post-injury, with no differences between races. However, race differences emerged at 1-month post-injury for TS on the forearm. Indeed, TS significantly increased from 1-week to 1-month post-injury for AA participants with mild TBI, whereas TS remained stable for Caucasian participants with mild TBI. Taking the TS and CPM results together, our findings indicate that race differences in endogenous pain modulatory mechanisms are magnified over time within the first month after mild TBI.
The present study also investigated race differences in psychological factors including pain catastrophizing and depression. Prior research showed elevated depression and pain catastrophizing in patients with mild TBI compared with controls. 8 Our study further confirmed this finding, but also revealed higher depression in AA participants compared with Caucasian participants, regardless of the presence of a mild TBI. This finding is consistent with a recent study of the general U.S. population, which found higher rates of probable depression for non-Hispanic Black (NHB) compared with NHW persons. 42 Interestingly, these racial differences in probable depression no longer existed when assets were statistically controlled for. 42 In a study of patients with TBI of all severity, AA patients with TBI reported greater depression, anxiety, and lower satisfaction of life compared with Caucasian patients with TBI at 1-year and 2-year follow-ups, 43 even after education, annual earnings, and TBI severity were controlled for. This longitudinal study did not have participants without TBI for comparison. Given the collective TBI and depression findings, health care providers should assess depressive symptomology in all patients in the acute and chronic stages of traumatic injury.
Also, as hypothesized, pain catastrophizing was greater in AA participants with mild TBI compared with Caucasian participants with mild TBI, whereas no race differences were evident in the controls. The latter finding contrasts with several studies in non-clinical samples showing AAs report higher pain catastrophizing compared with Caucasian individuals. 44 The lack of differences in pain catastrophizing within the control group could have been due to the small sample size for AA controls. Additionally, the control sample was largely recruited from the university campus, and therefore differences in education and socioeconomic status (SES) between races were minimized. However, whether educational attainment and SES play a role in pain catastrophizing levels is not known. Race differences in pain catastrophizing have also been found in adults with knee osteoarthritis 45 and chronic low back pain. 41
The mechanisms underlying greater pain catastrophizing in AAs compared with Caucasians is not well understood. Our examination of the individual subscales of the PCS suggested that the observed race differences in catastrophizing were likely driven more so by differences in magnification and rumination of pain than feelings of helplessness. Others have hypothesized that disparate and negative experiences in the health care system (e.g., lack of understanding by health care providers) by AAs could facilitate negative thinking about their pain and injury, including feelings that their symptoms and pain will worsen. 45 In support of this hypothesis, substantial research has documented racial disparities in the U.S. health care system. 46 Most relevant to the current study's population, research by emergency departments has shown that AA patients in the emergency room wait longer to see emergency physicians compared with Caucasian patients. 47 Specific to mild TBI, AAs are more likely to get emergency department treatment from a resident than a staff physician and less likely to be recommended to the referring physician for post mild TBI follow-up. 5 However, whether these disparities in health care could contribute to greater catastrophic thinking about pain following injury is unclear and only speculation.
Despite the increasing literature on race/ethnicity and pain, no data previously existed on race differences in post-traumatic headache following mild TBI. Therefore, we also determined race differences in the intensity of post-traumatic headaches, the most common pain symptom following mild TBI. Across the whole sample, over 90% and 85% of patients with mild TBI reported headaches at 1–2 weeks and 1-month post-injury, respectively. Importantly, we have previously shown that greater headache pain intensity at 1–2 weeks post-injury increases the risk for persistent post-traumatic headaches. 13 In the current study, AA participants with mild TBI reported significantly higher intensity of headache pain compared with Caucasian participants with mild TBI at both assessments.
Studies in other clinical samples show a similar trend to our data. For example, in a study of older adults with knee osteoarthritis, NHB individuals reported greater knee pain severity compared with their NHW counterparts, even after controlling for education and income. 45 Interestingly, a recent study using data from the 2010 to 2018 National Health Interview Surveys on adults found that AAs compared with Caucasians reported significantly greater severe pain (i.e., how much pain) but a lower prevalence of any pain (i.e., low back pain, neck pain, headache or migraine, or facial or jaw ache/pain in last 3 months). 48 However, AAs experienced less severe pain than Caucasians, when comparisons were made in adults at a similar SES level. This finding highlights the potential importance of considering the role of other demographic and SES factors when comparing the clinical pain experiences of different races.
To increase our understanding of factors that might underlie the race differences in headache pain intensity, we explored the QST and psychological variables as mediators of this relationship. The only significant mediator at both time-points was pain catastrophizing. AA patients with mild TBI reported higher pain catastrophizing relative to Caucasian patients, and higher levels of catastrophizing was associated with higher intensity of headache pain. Similarly, Fullwood and colleagues recently showed that pain catastrophizing mediated the relationship between race (NHB vs. NHW) and intensity of knee pain in patients with knee osteoarthritis. 45 Overall, our data add to the accumulating evidence indicating that pain catastrophizing is an important mediator of race differences in pain outcomes among healthy 49,50 and pain populations. 41,45
Limitations
Several limitations of this study should be acknowledged. A primary limitation was a smaller sample size, which precluded the inclusion of additional races (e.g., Asian, Hispanic) in the data analysis, as well as investigating potential sex by race interactions. Indeed, a growing body of research shows that racial disparities in pain outcomes extend to other minority groups. 48 Additionally, future studies with larger mild TBI and control samples are needed to better control for sociodemographic factors such as SES, education, and income. Also, we were only able to recruit approximately 22% of potentially eligible participants at two of the recruitment sites and the percentage from the third site is unknown. Therefore, our sample could suffer from a selection bias. Finally, based on the cross-sectional nature of our mediation analysis, it is possible that greater headache pain led to greater pain catastrophizing. Most likely, the pain–pain catastrophizing relationship is somewhat bidirectional. Indeed, other studies have shown that higher pain levels can lead to greater catastrophizing. 45,51,52 Given that catastrophizing is a modifiable construct, future research should investigate whether interventions designed to reduce pain catastrophizing could eliminate the racial differences in severity of acute post-traumatic headaches.
Conclusions
This study provides the first evidence for race differences in pain modulatory profiles, psychological profiles, and severity of acute post-traumatic headaches in the early stages following mild TBI. Overall, AA patients with mild TBI demonstrated worse endogenous pain modulation, greater pain catastrophizing, and greater intensity of headache pain compared with Caucasian patients with mild TBI. Given that greater acute headache pain intensity and reduced pain inhibitory capacity are risk factors for persistent post-traumatic headache, 13 future longitudinal research needs to determine whether AAs are at an increased risk for developing persistent post-traumatic headaches following mild TBI. Further, future research needs to explore the mechanisms underlying race difference in pain outcomes following mild TBI. Notably, poorer outcomes in the experimental pain responses and pain catastrophizing by AAs were only observed in the mild TBI sample (as opposed to controls) and thus are likely the result of a complex interaction of biopsychosocial mechanisms that emerged after the injury.
Transparency, Rigor, and Reproducibility Summary
This study is not a clinical trial and was not formally registered. The analysis plan was also not formally pre-registered. However, the study design and methods were assessed and pre-approved by the study's external funders. 1 Our power analysis showed that a sample size for detecting an interaction in the 2-way between subject ANOVAs with a moderate effect size of f = 0.25 with an alpha level of 0.05 and power of 0.80 was 128 subjects. Our final sample size for the between subject ANOVAs was n = 104, which allowed us to detect a moderate effects size of f = 0.028 with an alpha level of 0.05 and power of 0.80. Additionally, our power analysis showed that a sample size for detecting a within-between interaction in a 2-way mixed model ANOVA with a moderate effect size of f = 0.25 with an alpha level of 0.05 and power of 0.80 was 34 mild TBI subjects. Our final sample size for the mixed model ANOVA was n = 56, which allowed us to detect an effect size of f = 0.195 with an alpha level of 0.05 and power of 0.80. 3
Eighty participants with mild TBI and 50 control participants enrolled in the larger study. One participant with mild TBI was a screen fail after enrollment. Sixteen participants with mild TBI and 9 control participants did not identify as Caucasian or AA and therefore were not include in this study, which resulted in a total of n = 104 (63 mild TBI). Seven participants with mild TBI withdrew before the 1-month visit and therefore were not included in the analysis across time (n = 56). At the 1-week visit, 1 participant did not complete the PPT and TS assessments on the head, 2 participants did not complete the CPM test due to equipment malfunction, and 2 participants did not correctly complete the CES-D. 4 Participants were not told the results of their assessments. 5
Details of data acquisition and handling are provided in the article. All data sets were analyzed at the same time. 6 All surveys and questionnaires are widely available. All equipment used to conduct the quantitative sensory testing is available from Medoc Advanced Medical Systems and North Coast Medical & Rehabilitation Products. 7 The key inclusion criteria and outcome evaluations are established standards. 8 CIs and effect sizes are reported in Table 3 and the main text for primary outcome variables. 9 Tukey's test was used for follow-up comparisons, which accounts for multiple comparisons and maintains experiment-wise alpha at the specified level. 10 No replication or external validation studies have been performed. 11 De-identified data from this study will be made available (as allowable according to institutional review board standards) by e-mailing the corresponding author. 12 The authors agree to provide the full content of the manuscript on request by contacting the corresponding author. 14
Footnotes
Authors' Contributions
KMN, FAW, and JS conceived and designed the study. TN and JAS conducted data collection and processing. KMN analyzed the data. KMN, FAW, TN, JAS, and JS helped interpret the data. KMN drafted the manuscript. All authors revised and provided critical feedback to the manuscript draft. All authors have given final approval for this article to be published and are accountable for the integrity of the work.
Funding Information
This study was funded by the Department of Defense's Peer Reviewed Medical Research Program Investigator-Initiated Research Award (W81XWH-18-1-0433; W81XWH-18-1-0434), the Indiana Spinal Cord & Brain Injury Research Fund from the Indiana State Department of Health and the St. Vincent Foundation, and R01 NS102415/NS/NINDS NIH.
Author Disclosure Statement
No competing financial interests exist.