
Abstract
A considerable number of patients with mild traumatic brain injury have been known to “talk and die.” Serial neurological examinations, however, have been the only method of determining the necessity of repeat computed tomography (CT), and no validated method has been available to predict early deterioration of minor head injury. This study aimed to evaluate the association between hypertension and bradycardia, a classic sign of raised intracranial pressure (Cushing reflex) on hospital arrival and determine the clinical consequences of minor head injury after blunt trauma. We created a new Cushing Index (CI) by dividing the systolic blood pressure by the heart rate (equaling the inverse number of the Shock Index, a score for hemodynamic stability) and hypothesized that a high CI would predict surgical intervention for deterioration and in-hospital death among patients with minor head injury. To test our hypothesis, a retrospective observational study was conducted using a nationwide trauma database. Accordingly, adult blunt trauma with minor head injury (defined as a Glasgow Coma Scale of 13–15 and Abbreviated Injury Scale score of ≥2 in the head) who were transported directly from the scene by ambulances were included. Among the 338,744 trauma patients identified in the database, 38,844 were eligible for inclusion. A restricted cubic spline regression curve for risks of in-hospital death was created using the CI. Thereafter, the thresholds were determined based on inflection points of the curve, and patients were divided into low-, intermediate-, and high-CI groups. Patients with high CI showed significantly higher in-hospital mortality rates compared with those with intermediate CI (351 [3.0%] vs. 373 [2.3%]; odds ratio [OR] = 1.32 [1.14–1.53]; p < 0.001). Patients with high index also had a higher incidence of emergency cranial surgery within 24h after arrival than those with an intermediate CI (746 [6.4%] vs. 879 [5.4%]; OR = 1.20 [1.08–1.33]; p < 0.001). In addition, patients with low CI (equal to high Shock Index, meaning hemodynamically unstable) showed higher in-hospital death compared with those with intermediate CI (360 [3.3%] vs. 373 [2.3%]; p < 0.001). In conclusion, a high CI (high systolic blood pressure and low heart rate) on hospital arrival would be helpful in identifying patients with minor head injury who might experience deterioration and need close observation.
Introduction
Traumatic brain injury (TBI) remains a major cause of death and disability worldwide. 1 Although studies have reported relatively low mortality and morbidity rates for patients with minor head injury, defined as those with a Glasgow Coma Scale (GCS) score of ≥13 on arrival, 2%–7% of them have been known to deteriorate and die, a phenomenon called “talk and die.” 2 –6 Considering that delays in computed tomography (CT) evaluation and oversight on hypoxia and/or coagulopathy occasionally occur in such populations, early recognition of deterioration and optimal intervention would be needed to improve clinical prognosis. 2
Cushing reflex is a classic sign of increased intracranial pressure (ICP), which is composed of hypertension, bradycardia, and abnormal breathing. 7 Although hemodynamic instability has been associated with increased death among trauma patients, 8 those with TBI also exhibit unfavorable clinical outcomes when presenting with hypertension or bradycarida. 9 –11 It remains unclear, however, whether signs of increased ICP can be a surrogate marker for the severity of intracranial injury or predict deterioration of brain injury. Further, no validated studies have investigated whether hypertension/bradycardia can predict the need for emergency cranial surgery.
Accordingly, we performed a retrospective nationwide observational study to elucidate the association between the Cushing reflex and clinical consequences of minor head injury after blunt trauma. We developed a Cushing Index (CI) by dividing the systolic blood pressure (SBP) by the heart rate (HR), yielding a number inverse of the Shock Index. In line with this, a high CI would indicate increased ICP, whereas a low CI (equal to high Shock Index) would suggest hemodynamic instability. We hypothesized that a high and low CI on hospital arrival would be associated with increased in-hospital death, whereas only a high CI would be associated with higher incidences of surgical intervention for the deterioration of minor head injury.
Methods
Study design and setting
This retrospective cohort study was conducted using data from the Japan Trauma Data Bank (JTDB), a Japanese nationwide trauma registry established in 2003. The JTDB comprises 288 hospitals and has been maintained by the Japanese Association for Acute Medicine and Japanese Association for the Surgery of Trauma. Prospectively collected data are entered by treating physicians or medical assistants into an online data collection server. All collaborating hospitals obtained approval by the individual local Institutional Review Board for the Conduct of Human Research before study initiation. The requirement for informed consent was waived given the anonymous nature of the data used.
In Japan, initial management of head injury is based on the Japan Advanced Trauma Evaluation and Care, 12 which is generally compliant with Advanced Trauma Life Support, by emergency physicians or neurosurgeons because of the limited number of trauma surgeons. With easy access to CT scanners and universal health coverage, most patients with head injuries undergo CT regardless of disease severity. Almost all patients with head injury (Abbreviated Injury Scale [AIS] 2 or higher) are hospitalized and are generally observed for about a week in Japan.
Study population
We retrospectively analyzed data from patients with minor head injury using the JTDB between January 2004 and March 2019. Patients who satisfied the following criteria were included: (1) aged ≥18 years; (2) presented with a blunt injury; (3) transported directly from the scene by ambulance; (4) AIS 13 score of ≥2 in the head; (5) and GCS ≥13 on hospital arrival. Therefore, this study included not only patients with isolated head injury, but also patients with both head injury and extracranial injuries. Patients with missing values for survival status and those who presented with cardiopulmonary arrest (CPA) on arrival were excluded.
Data collection and definitions
Collected data included age, sex, pre-hospital vital signs, vital signs on arrival, mechanism of injury, transport time, medical histories, any surgical procedures, AIS score, Injury Severity Score (ISS), length of hospital stay, and survival status at discharge. As a marker of Cushing reflex, CI was calculated by dividing SBP with HR on hospital arrival. Cranial surgery was defined as craniotomy, craterization, intracranial hematoma evacuation, or internal/external decompressive craniectomy based on the type of surgery recorded, and those performed within 24h after admission were defined as emergency cranial surgery.
Outcome measures
Primary outcome was in-hospital death, whereas secondary outcomes included incidence of emergency cranial surgery, craniotomy because of elevation of ICP, incidence of cranial surgery, and length of hospital stay.
Statistical analysis
To investigate the association between CI and clinical consequences of minor head injury, patients were divided based on the CI. Considering the possible non-linear relationship between CI and in-hospital death, a restricted cubic spline regression model with CI was used to detect thresholds that affected prognosis, in which age and ISS were adjusted. A cubic spline curve showing risk for in-hospital death depending on CI was created.
To determine a higher threshold of the index, inflection points of the curve were chosen visually, and then a lower threshold of the index was selected as the point that has an equivalent log odd for the higher threshold. Both the higher and lower thresholds were set with a round number, considering clinical feasibility. 14,15 Therefore, three groups (i.e., namely the low-, intermediate-, and high-CI groups) were generated. Appropriateness of thresholds was examined using sensitivity analyses.
The clinical utility of the CI to predict in-hospital death and secondary outcomes was assessed using unadjusted models wherein low- and high-CI groups were compared with the intermediate group. Adjusted models were developed by incorporating GCS on arrival, AIS in the head, and comorbidities (coronary artery disease, diabetes mellitus, and cerebrovascular disease), after which the primary outcome was compared among the groups.
Sensitivity analysis was conducted using different thresholds for CI to validate whether the results were independent of the cutoffs. Moreover, another sensitivity analysis was performed using pre-hospital CI calculated using pre-hospital SBP and HR. The association between high-/low-CI and in-hospital death was examined using sensitivity analyses.
In addition, the predicting ability of CI and GCS for in-hospital death was compared with one of GCS only. The receiver operating characteristic (ROC) curves were drawn for both models and the area under the ROC curve (AUC) was compared.
Subgroup analysis was performed after dividing patients based on age (<65 vs. ≥65 years), vital signs on hospital arrival, including GCS (13 vs. 14 vs. 15), SBP (<150 vs. ≥150 mm Hg), and HR (≤60 vs. >60/min), ISS (<16 vs. ≥16), type of TBI (contusion, subarachnoid hemorrhage, acute subdural hemorrhage [ASDH], acute epidural hemorrhage, and diffuse brain injury), and patients without significant comorbidities (coronary artery disease, diabetes mellitus, and cerebrovascular disease).
Descriptive statistics are presented as median (interquartile range [IQR] or number [%]). Comparisons among groups were conducted using Mann-Whitney U tests, χ 2 tests, or Fisher exact tests as appropriate. All statistical analyses were conducted with Microsoft Excel (Microsoft, Redmond, Wash) and SPSS version 27 (IBM, Armonk, NY), with a two-sided α threshold of 0.05 indicating statistical significance when testing all hypotheses.
Results
Patient characteristic
A total of 338,744 trauma patients were identified in the database. Among them, 40,263 patients satisfied all inclusion criteria, and 1399 were then excluded because of CPA on hospital arrival or missing survival data, leaving 38,864 patients eligible for analysis. The patient flow diagram is summarized in Figure 1.

Patient flow diagram. Among the 338,744 trauma patients in the database, 38,864 were eligible for this study. AIS, Abbreviated Injury Scale; GCS, Glasgow Coma Scale; CPA, cardiopulmonary arrest.
In the restricted cubic spline curve, the higher and lower thresholds were visually determined as 2.0 and 1.5, respectively (Fig. 2). The patient characteristics of the low-, intermediate-, and high-CI groups are summarized in Table 1. The median HR, SBP, and CI were 82/min, 142 mm Hg, and 1.7 in the intermediate-CI group (reference group); 71/min, 168 mm Hg, and 2.3 in the high-CI group; and 96/min, 120 mm Hg, and 1.3 in the low-CI group, respectively.
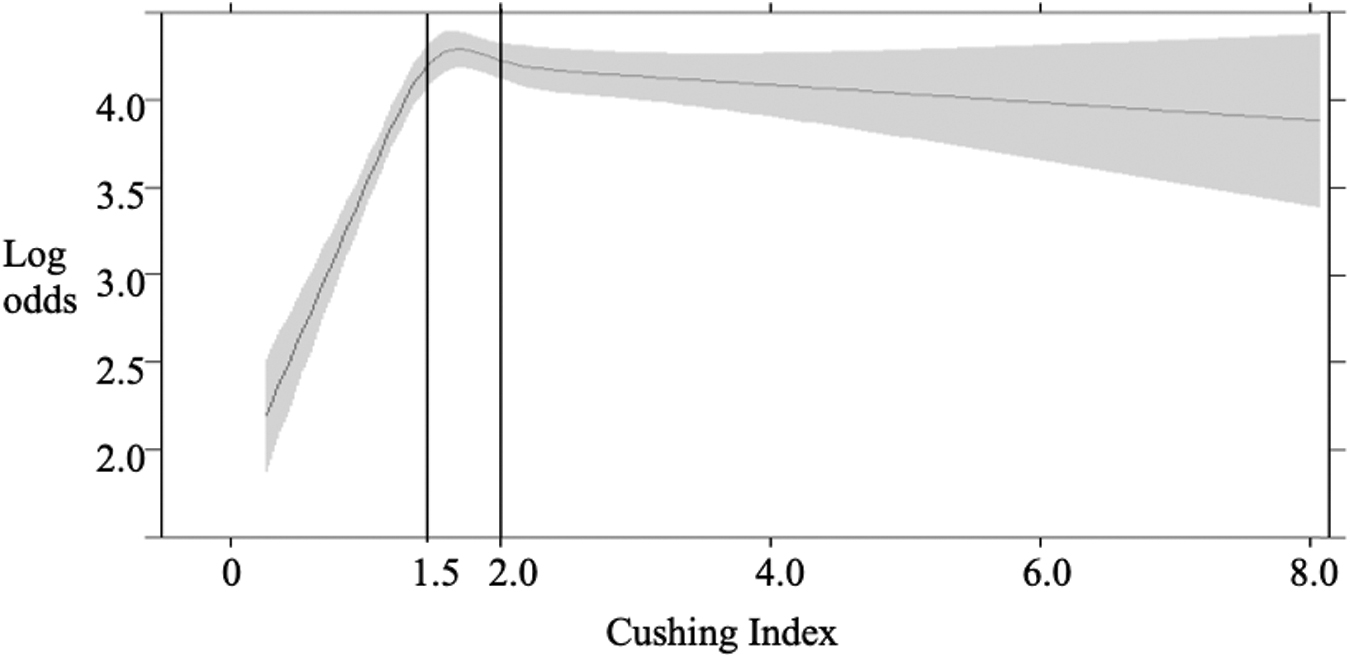
Restricted cubic spline regression model with the Cushing Index. The restricted cubic spline regression model with the CI, adjusted for age and ISS, was used to detect thresholds that affected prognosis. The gray shading represents the 95% confidence interval for the log-transformed odds ratio for survival. Inflection points on the spline curve indicating the high and low threshold were 2.0 and 1.5, respectively. CI, Cushing Index; ISS, Injury Severity Scale.
Compared with patients with intermediate CI, those with high CI were older, had higher AIS in the head, and presented more frequently with contusion, subarachnoid hemorrhage, and ASDH (Table 1). Only a few patients in the high-CI group (2 [0.0%]) had a SBP <90 mm Hg on hospital arrival. The GCS on arrival, ISS, and transportation time were comparable between patients with a high and intermediate CI. Conversely, patients with a low CI were younger and had lower AIS in the head and higher ISS than those with an intermediate CI. Patients with a low CI had lower incidence rates of diffuse brain injury and ASDH compared with those with an intermediate CI.
Primary and secondary outcomes
Patients with a high and low CI had significantly higher in-hospital death compared with those with an intermediate CI (332 [3.0%] vs. 356 [2.3%]; p < 0.001 and 475 [4.1%] vs. 356 [2.3%]; p < 0.001, respectively; Table 2). Adjusted analysis incorporating GCS on arrival, AIS in the head, and comorbidities also revealed that patients with a high and low CI had higher in-hospital death than in those with an intermediate CI (odds ratio, 1.17 [1.00–1.37]; p = 0.046 and 1.91 [1.66–2.21]; p < 0.001; Table 2].
Characteristics of Patients With Minor Head Injury
IQR, interquartile range.
Presence of shock is defined as systolic blood pressure <90 mm Hg on arrival.
Cushing Index and Clinical Outcomes
CI, confidence interval; ICP, intracranial pressure; IQR, interquartile range.
Adjusted models were developed by incorporating Glasgow Coma Scale on arrival, Abbreviated Injury Scale in the head, and comorbidities (coronary artery disease, diabetes mellitus, and cerebrovascular disease).
Emergency cranial surgery was defined as craniotomy or craterization performed within 24h after admission.
Cranial surgery was defined as craniotomy, craterization, hematoma evacuation, and internal/external decompressive craniectomy performed during hospital admission.
Incidences of emergency cranial surgery within 24h after admission and any cranial surgery during hospital stay were higher among patients with a high CI than among those with an intermediate CI (712 [6.4%] vs. 835 [5.3%]; p < 0.001 and 721 [6.5%] vs. 843 [5.4%]; p < 0.001, respectively; Table 2) but were comparable between those with a low and intermediate CI (587 [5.1%] vs. 835 [5.3%]; p = 0.335 and 604 [5.2%] vs. 843 [5.4%]; p = 0.548, respectively; Table 2).
Also, craniotomy because of elevation of ICP was significantly higher in patients with high CI, compared with those with intermediate CI (594 [5.3%] vs. 680 [4.4%]; p < 0.001; Table 2). Conversely, the frequency of craniotomy because of elevation of ICP was similar between patients with intermediate and low CI (680 [4.4%] vs. 463 [4.0%]; p = 0.159; Table 2). Patients with a high and low CI had a longer hospital stay than those with an intermediate CI (Table 2).
Sensitivity and subgroup analyses
Sensitivity analysis was conducted to validate whether the primary outcome was independent of the cutoff obtained from the inflection points on the spline curve. After setting cutoffs at 1.9/1.4 and 2.1/1.6, we found that in-hospital death was similarly higher in the high and low CI groups than in the intermediate CI group (Table 3). Another sensitivity analysis using pre-hospital vital signs also revealed that patients with a high pre-hospital CI had higher in-hospital mortality rates compared with those with an intermediate pre-hospital CI (Table 3). Also, predicting ability for in-hospital death by CI and GCS was better than by GCS only (AUC, 0.651 vs. 0.359, p < 0.001).
Cushing Index and In-Hospital Death in Sensitivity Analysis
CI, confidence interval; Ref, reference.
Cushing Index was calculated using pre-hospital blood pressure and heart rate.
Our subgroup analyses (Table 4) showed an association between a high CI and increased in-hospital death among patients with a GCS of 13 and 14, SBP <150 mm Hg, HR ≥60/min, ASDH, patients without significant comorbidities, and severe and non-severe injuries (ISS ≥16 and <16).
High Cushing Index and In-Hospital Death in Subgroup Analysis
CI, confidence interval, GCS, Glasgow Coma Scale, sBP, systolic blood pressure, ISS, Injury Severity Scale.
Comorbidities included patients with coronary artery disease, diabetes mellitus, and cerebrovascular disease.
Discussion
The current study found that a high CI was associated with increased in-hospital death among patients with minor head injury after blunt trauma, suggesting that a high CI could indicate elevation of ICP related to the occurrence of pathological intracranial events. In addition, in-hospital death was also higher in patients with a low CI, a value equal to a high Shock Index, suggesting that a low CI could reflect hemodynamic instability from hemorrhage rather than TBI. Notably, patients with a high CI, but not those with a low CI, had a significantly higher incidence of emergency cranial surgery.
CI was calculated using SBP and HR, where a high index should reflect an even small increase in SBP and decrease in HR. Considering that the increment of systemic arterial pressure is a response to the elevation of ICP and bradycardia is then activated by intracranial vagus nerve, 16 patients with deteriorating TBI could exhibit a high CI. Notably, the association between a high index value and unfavorable outcomes was identified in patients without obvious hypertension (SBP <150 mm Hg) and those without bradycardia (HR ≥60/min), which suggests that the CI could be useful even without significant hypertension or bradycardia.
Given that the high CI group showed a significant increase in the frequency of emergency cranial surgery, the CI could also be useful in predicting the need for emergency surgical intervention of minor head injury. Because patients with minor head injury usually do not undergo ICP monitoring, 17 the CI can be a clinically feasible surrogate for ICP. Moreover, considering the unclear clinical signs indicating the necessity for repeat CT, 18 –20 the index, along with GCS and pupil findings, may be used as a new physiological parameter for identifying patients requiring close observation and those under consideration for repeat CT. Further studies should be conducted to determine whether chronological changes in the index could be useful for the accurate prediction of cranial surgery.
Subgroup analyses indicated that a high CI was associated with increased in-hospital death in patients with ASDH. Considering that ASDH more frequently necessitates neurosurgical intervention and has been associated with worse clinical outcomes compared with other TBIs, 21,22 the CI could be particularly useful for predicting the expansion of subdural hematoma, thereby enabling prompt and appropriate surgical management in such population.
Moreover, another subgroup analysis on the initial GCS indicated that the index was associated with increased death only among patients with a GCS score of 13–14. Therefore, the CI should be evaluated especially in patients with minor head injury who present with mild disturbance in consciousness. The clinical utility of the CI should be further examined in patients with a GCS score of 15 given the limited number of patients with such a score in this study.
Notably, given that the CI is an inverse of the Shock Index, the CI can be used as a marker for both intracranial hypertension and hemodynamic instability. The association between a low CI and increased in-hospital death without changes in the incidence of cranial surgery implied that patients with a low CI (i.e., a high Shock Index) had unfavorable outcomes because of hemorrhagic shock rather than head injury. Notably, the current study set the lower threshold of the CI at 1.5; therefore, a CI of <1.5 would suggest an increase in the in-hospital death because of bleeding among patients with minor head injury, which corresponds to a Shock Index of >0.67.
Given reports suggesting that a cutoff Shock Index value of 1.0 can be an indicator of hemodynamic instability in trauma patients, including those without TBI, 23 the lower threshold (0.67) in the current study could be attributed to the intolerance of hemodynamic instability among patients with minor head injury considering that patients with TBI need relatively greater cerebral blood flow to maintain cerebral tissue perfusion. 24
Given the several limitations of the current study, the results must be interpreted in the context of our study design. First, we analyzed patients included in the JTDB, which does not record facility characteristics, such as management strategy for minor head injury, indications for emergency surgery, and availability and experience of neurosurgeons and trauma surgeons, thereby limiting the generalizability of our results.
Second, although intracranial pressure itself is not available in the JTDB, indications for craniotomy included “elevation of intracranial pressure” and therefore retrieved these data. The results showed a relationship between high CI and ICP elevation necessitating surgery, although there remained the possibility that high CI just reflects conditions that did not lead to pathological elevation of ICP.
Third, because the results were obtained from the population including those with certain comorbidities, patients with such comorbidities may have an elevated CI from their comorbidities rather than TBI. Although the subgroup analysis on patients without comorbidities showed the association between high CI and increased death, usefulness of the CI remains unclear in patients with certain comorbidities.
Fourth, given the unique epidemiological characteristics of Japan, such as longevity and low incidence rates of injury, 25 international validation of the results is needed. Fifth, despite selecting the CI thresholds from a restricted cubic spline regression curve and obtaining similar results from sensitivity analyses using slightly different thresholds, other clinically feasible cutoff values may exist. Finally, given the retrospective nature of the current study, our results remained inconclusive. Unmeasured confounding and survival predictors could have affected our results.
Conclusions
Our results showed that a high CI, which indicates a high SBP and low HR, was associated with increased in-hospital death and a higher incidence of emergency cranial surgical intervention among patients with minor head injury. In addition, low CI was associated with increased in-hospital death without a higher incidence of emergency cranial surgical intervention. Therefore, the CI could be a useful marker for detecting both intracranial hypertension and hemodynamic instability.
Footnotes
Authors' Contributions
KM and RY conceived and designed the study. KM and RY acquired and managed the data. KM and RT contributed to the analysis and interpretation of the data. KM drafted the manuscript. KM, RY, RT, and JN contributed substantially to the critical revision of the manuscript for important intellectual content. JS contributed to study supervision.
Funding Information
The authors have nothing to disclose.
Author Disclosure Statement
No competing financial interests exist.