
Abstract
Sport-related concussion (SRC) is associated with several post-injury consequences, including neurocognitive decrements and psychological distress. Yet, how these clinical markers interact with each other, the magnitude of their interrelationships, and how they may vary over time following SRC are not well understood. Network analysis has been proposed as a statistical and psychometric method to conceptualize and map the complex interplay of interactions between observed variables (e.g., neurocognitive functioning and psychological symptoms). For each collegiate athlete with SRC (n = 565), we constructed a temporal network as a weighted graph, with nodes, edges, and the set of weights associated with each edge at three time-points (baseline, 24–48 h post-injury, and asymptomatic), that graphically depicts the interrelated nature of neurocognitive functioning and symptoms of psychological distress throughout the recovery process. This graph shows that the inter-group relationships between neurocognitive functioning and symptoms of psychological distress were stronger at the 24–48 h time-point than at baseline or at the asymptomatic time-point. Further, all symptoms of psychological distress and neurocognitive functioning significantly improved from the 24–48 h time-point to asymptomatic status. The effect sizes of these changes ranged from 0.126 (small) to 0.616 (medium). This research suggests that significant improvements in symptoms of psychological distress appear necessary to drive related improvements in neurocognitive functioning and vice versa. Therefore, clinical interventions should consider the importance of managing psychological distress during the acute care of individuals with SRC to help ameliorate negative outcomes.
Introduction
Sport-related concussion (SRC) is associated with a myriad of post-injury consequences, including neurocognitive changes 1,2 and psychological distress. 3 –6 Although the majority of athletes who sustain SRC return to pre-injury levels of functioning within 7–12 days, 7 –10 a sizeable minority report persisting symptoms. 11 –13 The etiology of persisting symptoms is unclear and likely includes both pre- and post-injury factors, as well as their interrelationships. 14
The neurocognitive functioning and psychological symptoms expressed after SRC are typically used as markers of post-injury recovery trajectories and are integral to return-to-play (RTP) decisions. These constructs have been shown to be both independent 15,16 and shared 17 –22 factors in recovery. Yet, how these post-injury consequences interact with each other, including the magnitude of their interrelationships, and how they may vary over time, remain poorly understood. A more complete understanding of these dynamics between neurocognitive functioning and psychological symptoms following SRC would likely provide greater insight as to the recovery trajectories and optimal treatment strategies for individuals who sustain SRC. 23,24
Network analysis has been proposed as a statistical and psychometric method to conceptualize and map the complex interplay of interactions between observed variables (e.g., neurocognitive functioning and psychological symptoms). 25 –27 For example, the covariance between variables such as depressed mood and cognitive processing speed is explained in terms of a pattern of causal interactions between them. Network analysis has been utilized in numerous studies, particularly in the field of psychiatry and the study of mood disorders, to significant and insightful effect. 28 –30 This powerful method provides greater explanatory power for why certain mental health symptoms and disorders co-occur, demonstrates differences among groups to aid in prediction of future disordered states, and provides actionable symptom-level understanding of disorder(s) in order to effectively target therapeutic interventions. 30 However, it has been underutilized in the SRC research literature with respect to post-injury variables despite its potential in identifying important post-SRC factors and their interrelationships. 31,32
The present proof-of-concept study utilizes network analysis to study post-SRC variables in a large prospective sample of collegiate athletes with SRC. We describe the network architectures of neurocognitive changes and psychological symptoms, as measured by the Brief Symptom Inventory-18 (BSI-18) and Immediate Post-concussion Assessment and Cognitive Testing (ImPACT), of collegiate athletes with SRC at three time-points: baseline, 24–48 h, and when athletes reach asymptomatic status. The BSI-18 is frequently used in SRC research to measure athletes' somatization (i.e., the expression of mental phenomena as physical symptoms), depression, and anxiety symptoms. 33 As this is one of the first empirical investigations to implement network methodologies in SRC, we included only BSI-18 and ImPACT variables in the networks so as to provide a more clear and interpretable graphical depiction of results unburdened by the inclusion of more variables. Additionally, the inclusion of similar variables measured by separate instruments was avoided as there is currently no agreed upon manner in which to group these variables. Thus, the currently reported networks allow us to rigorously evaluate the change in variables over time and identify variables that are highly correlated at each time-point. Through this study we demonstrate the evolution and interconnectedness of post-SRC variables.
Methods
Data were obtained from the National Collegiate Athletic Association (NCAA)-U.S. Department of Defense (DoD) Concussion Assessment, Research and Education (CARE) Consortium—a multi-site, longitudinal study across 30 NCAA institutions, comprising four U.S. service academies and 26 civilian colleges and universities. The structure and methods of the CARE Consortium have been described elsewhere. 34 Overall, the CARE Consortium data set included 47,518 pre-season baseline examinations from 34,709 athletes and 3603 diagnosed SRCs collected between the 2014 and 2020 academic years. For each participant diagnosed with an SRC, post-injury examination data were collected within 6 h after the injury, 24–48 h after the injury (i.e., 24–48 h), at the time that the athlete began the RTP protocol (i.e., asymptomatic), and at the time that the athlete was cleared for unrestricted RTP. Study participants completed several post-SRC evaluations, including objective assessments of neuropsychological functioning and self-report of current psychological symptoms. Post-SRC examinations were conducted by the local medical team at the athletes' institution using a standardized injury definition. 35 The local institutional review board (IRB) at each of the performance sites, as well as the U.S. Army Medical Research and Materiel Command Human Research Protection Office, reviewed and approved all study procedures. Participants provided written informed consent prior to participation. This study was performed in accordance with the standards of ethics outlined in the Declaration of Helsinki.
Participants
Our study sample included any athlete or cadet with a diagnosed SRC during the study period for whom BSI-18 and ImPACT data were available at baseline, 24–48 h, and asymptomatic time-points. These three time-points generally represent meaningful changes in neurocognitive functioning and psychological symptoms throughout the pre- and post-injury management processes and are thus suitable for our analysis. Moreover, the asymptomatic time-point includes more data than the unrestricted RTP time-point, improving the statistical power of our study.
Figure 1 presents the study participant consort flow diagram. Time to asymptomatic has been defined by the CARE Consortium as the number of days from injury until the athlete is cleared by their clinician to begin the RTP process. 36 As one of the primary purposes of the current study is to describe the complex interplay of post-SRC neurocognitive functioning and psychological symptoms in collegiate athletes over time, we excluded all SRCs that were missing BSI-18 and/or ImPACT data at any of the three time-points. If an athlete sustained multiple SRCs, only the first SRC was included in the analyses. To better understand the recovery networks of the average athlete with SRC, we excluded athletes who required more than 7 days to initiate the RTP protocol, which is the median time for CARE participants with SRC. 7 Given the substantial variation in the time to initiate the RTP protocol (see Supplementary Fig. S1), the choice of 7 days allows us to include enough data to perform a meaningful analysis while avoiding the challenge of introducing substantial noise and variation in this proof-of-concept modeling analysis. No additional exclusion criteria were applied.
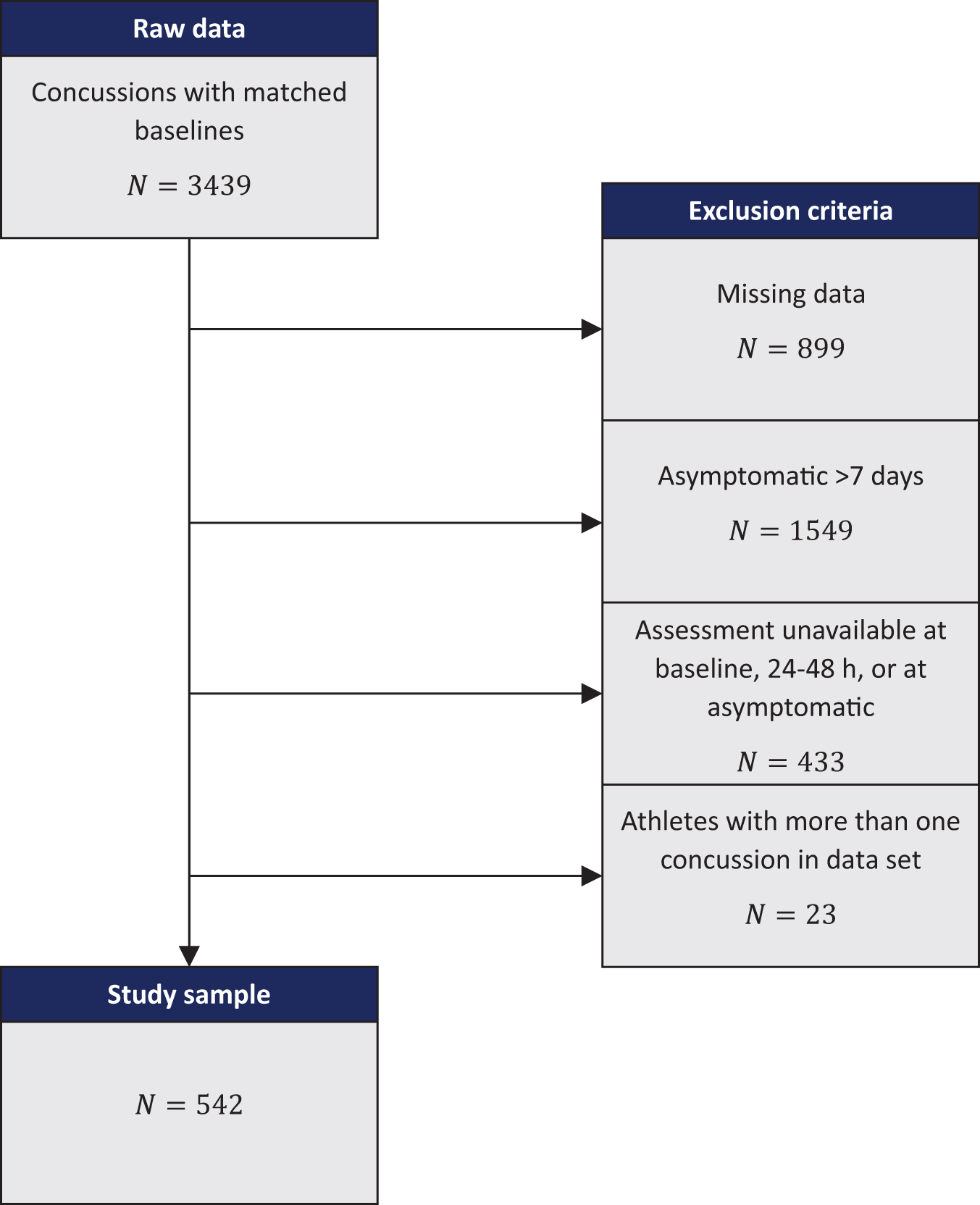
Study participant consort flow diagram. Color image is available online.
Measures
For each participant, we extracted basic demographic information (i.e., age, gender, and race). Our network analysis included scores from the BSI-18 and ImPACT. The BSI-18 was used to measure current symptoms of psychological distress. It is composed of three, six-item scales measuring somatization, depression, and anxiety symptoms. 33 Our analysis used the sum of scores of the somatization, depression, and anxiety scales, each ranging from 0 (no symptoms) to 24 (most severe). ImPACT is a computerized neurocognitive test battery that objectively measures several cognitive domains, including verbal memory, visual memory, and reaction time. 37 We used ImPACT composite scores in analyses.
Statistical analyses
Graph construction and graphical measures.
We constructed a temporal network as a weighted graph
where S = {Somatization, Anxiety, Depression, Impulse Control, Reaction Time, Verbal Memory, Visual Memory, Visual Motor} is the set variables measured by the BSI-18 and ImPACT and T = {baseline, 24–28 h, asymptomatic} is the set of time-points. Thus, in the final graph, |S| is 8, |T| is 3, and |N| is 24.
Each athlete, n, has a score associated with node i, that is denoted by,
When constructing G, we use edge weights
To understand the interactions between different variables, it is important to understand how the variables relate to each other and if they change in coordination. The correlation between two variables shows if a linear relationship is present and can be indicative of how variables relate to each other. Therefore, for edges connecting nodes
To determine how an individual variable is affected by a concussion, we follow the evolution of that variable throughout the concussion recovery process. The information about the variable provided at all three time-points can be used to determine the difference in the population average scores between consecutive time-points. These differences can indicate whether a given variable is worsening or improving. For edges connecting one variable between consecutive time-points (nodes
We evaluate the impact of a concussion on an individual variable by performing a paired t-test. This test is used to determine whether the population average differs between two groups while exploiting the paired nature of our observations to improve statistical power and mitigate the effect of confounding factors. For each variable, s, we calculate the statistic
To further investigate the effect size of a concussion on any given variable we also computed and reported Cohen's d statistic. Cohen's d statistic measures how many standard deviations lay between two sample means. In other words, it provides information on the effect size of the injury after 24–48 h and on subsequent healing time. This quantifies the extent to which the null hypothesis, that a variable's prevalence does not change following the injury, is false.
We investigate changes in relationships between two variables by taking the correlation between the two variables at a fixed time-point and determining if the change in that correlation across time is significant. For example, consider the correlation between anxiety and depression. We want to address the question: “Does the correlation between anxiety and depression change significantly from baseline to 24–48 h post-injury?” To express this mathematically, consider the nodes
However, because correlation coefficients are not normally distributed, we cannot apply traditional comparison methods. Instead, we follow Steiger's method
38
for non-overlapping, dependent variables. Our cohort is considered non-overlapping because we consider different, discrete periods of time (t and
Results
In Table 1, we present the demographic features of our study cohort obtained from the NCAA-DoD CARE Consortium. These data include 565 collegiate varsity athletes and military service academy cadets with a mean (standard deviation [SD]) age of 19.1 (1.3) years. Of the 565 participants, 367 (65.0%) identified as male. Additionally, 386 (68.3%) of the participants identified as white, 72 (12.7%) identified as African American, and 59 (10.4%) identified as multiple races.
Study Participant Demographic Information
SD, standard deviation.
Figure 2 illustrates the temporal network structure built from our study cohort, where within time-point edges indicate correlations across study variables at the same time-point and edges across different time-points indicate the change in an individual variable across time-points. Symptoms of psychological distress (as measured by the BSI-18) are represented by red nodes and domains of neurocognitive functioning (as measured by ImPACT) are represented by blue nodes. This graph highlights that the between-group (purple) edges are much thicker at the 24–48 h time-point compared with the baseline and asymptomatic time-points, indicating that subjects experienced increased interactions between variables immediately following SRC.
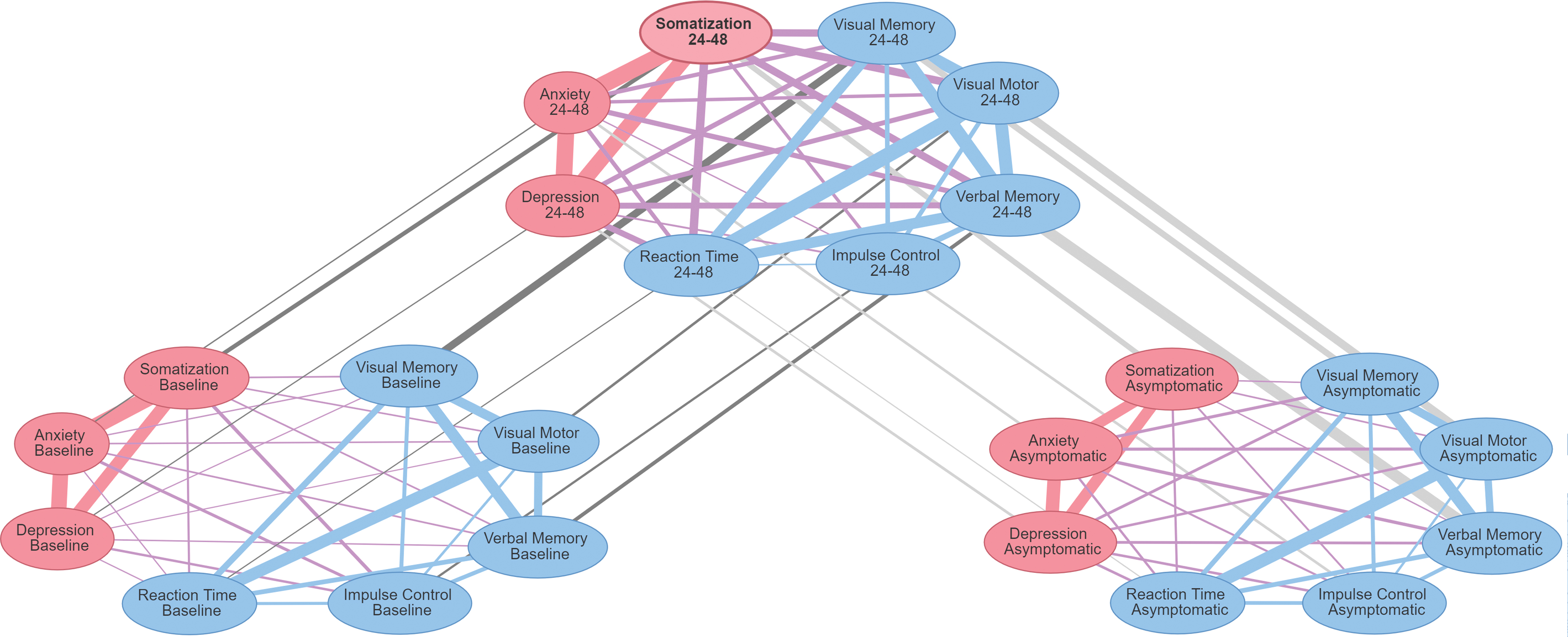
Graphical depiction of the temporal network architectures of neurocognitive functioning and psychological symptoms at baseline, 24–48 h, and asymptomatic time-points. There are two types of edges: those connecting two different variables at one time-point and those connecting one variable across two time-points. The latter of these edges are colored gray and indicate the average change in the level of the variable in the cohort. The width of these edges is indicative of the magnitude of the change. Dark gray edges indicate a worsening in scores from time-point 1 to time-point 2, whereas light gray edges indicate improvement in scores from time-point 1 to time-point 2. At any of the three time-points, edges connecting two BSI-18 symptoms are red, edges connecting two ImPACT domains are blue, and edges connecting BSI-18 symptoms and ImPACT domains are shown in purple. The width of these edges indicates the strength of the correlation between the two variables: the thicker the edge, the stronger the correlation. BSI-18, Brief Symptom Inventory-18; ImPACT, Immediate Post-concussion Assessment and Cognitive Testing. Color image is available online.
The correlations between all variables at baseline, 24–48 h post-injury, and asymptomatic are given in Table 2. In general, most variables experience a significant change in correlation with another variable across time-points. However, some variables have a greater number of significant changes than others. For instance, the change in correlation from baseline to 24–48 h post-injury is significant for four variable pairs that include somatization: somatization/reaction time, somatization/verbal memory, somatization/visual memory, and somatization/visual motor. This may indicate there is a connection between somatization and ImPACT variables after SRC, and the relationship between these variables should be further investigated. Along with somatization, reaction time, verbal memory, and visual motor speed also significantly change in correlation from baseline to 24–48 h post-injury with five other variables. From 24–48 h post-injury to asymptomatic, the change in correlation is significant for five pairs of variables that include somatization: somatization/anxiety, somatization/reaction time, somatization/verbal memory, somatization/visual memory, and somatization/visual motor. Reaction time and visual motor speed both are included in four pairs of variables that experience a significant change. These significant relationships demonstrate that somatization, reaction time, and visual motor speed may play a key role in SRC recovery and prolonged recovery.
Correlation Coefficients Between Neurocognitive Functioning and Psychological Symptoms at Baseline, 24–48 h, and Asymptomatic Time-Points
Adjusted p < 0.05, where p-value adjustments are made using the Bonferroni correction for multiple comparisons. Indicates significant changes compared with the previous time-point.
In each cell, results are listed from top to bottom as correlation at the baseline, 24–48 h, and asymptomatic time-points.
The average difference between the athletes' scores for each variable at each time-point (i.e., the edges spanning across time-points), along with their SDs, are reported in Table 3. In general, few variables changed significantly from baseline to 24–48 h, but all variables changed significantly from 24–48 h to the asymptomatic time-point. From 24–48 h to the asymptomatic time-point, there were statistically significant mean decreases in somatization, anxiety, depression, and reaction time. There were also significant mean increases in verbal memory, visual memory, and visual motor speed.
Differences in Study Participant Neurocognitive Functioning and Psychological Symptoms at Each Time-Point
adjusted p < 0.05; indicates significant changes.
Positive mean values are indicative of an increase from baseline to 24–48 h or from 24–48 h to asymptomatic, whereas negative mean values indicate a decrease.
SD, standard deviation.
Discussion
SRC have been recognized as a significant public health concern at every level of sport participation by military and civilian communities. Post-SRC consequences often result in immediate but transient alterations to neurocognitive and psychological functioning; however, data suggests that approximately 20% of injured athletes may have a recovery lasting >14 days. 7 The interconnected nature of neurocognitive functioning and psychological symptoms is well-known, yet it is unclear how and to what extent these relationships change throughout SRC recovery. With the present novel study, we rigorously applied network analysis in a large sample of collegiate athletes and military service cadets with SRC to objectively evaluate how the relationships between neurocognitive functioning and symptoms of psychological distress change over time and the degree to which they are interconnected.
SRC is an injury defined by the presence of a biomechanical force acting on the brain that results in a cluster of consequences. Our primary findings, as depicted in Figure 2, show the complex dynamic interplay of these consequences and their magnitude. At baseline, although BSI-18 symptoms are highly intercorrelated, there are small relationships between the BSI-18 and neurocognitive functioning variables. However, immediately post-injury we see larger correlations between BSI-18 and ImPACT variables. Although the exact mechanisms potentially underlying these relationships is unknown, 39 our results clearly demonstrate that neurocognitive functioning is strongly related to symptoms of psychological distress, particularly 24–48 h post-injury. In particular, analyses showed that somatization (i.e., the expression of mental phenomena as physical symptoms that are common following SRC) was significantly correlated with reaction time, verbal and visual memory, and visual motor abilities at the 24–48 h and asymptomatic time-points. These results suggest that somatization is a key contributor to observed post-injury neurocognitive functioning changes and may assist in predicting recovery time and may point to a viable avenue of intervention in athletes with prolonged recovery. 40 Such a targeted intervention, due to demonstrated highly interconnected variables, may elicit functional improvements in a related domain (i.e., neurocognitive functioning) in addition to the specified symptoms (i.e., somatization) for which the intervention was designed.
Our results demonstrate a significant negative correlation between anxiety symptoms and verbal memory at the 24–48 h time-point. Moreover, the network model depicts a moderate edge between anxiety and depression symptoms with measures of neurocognitive functioning, although the correlations were not statistically significant. This finding is consistent with prior research by Kontos and colleagues 41 who reported a similar non-statistically significant increase in depression symptoms that coincided with worse neurocognitive functioning. Our results thus may imply that the connections between symptoms of psychological distress and neurocognitive functioning are highly variable from athlete to athlete, 42 and future research should attempt to identify athletes for whom these connections are clinically meaningful and for whom they are not.
Interestingly, all symptoms of psychological distress and neurocognitive functioning significantly improved from the 24–48 h time-point to asymptomatic status, rather than a small subset of interrelated variables driving recovery reporting. The effect sizes of these changes ranged from 0.126 (small) to 0.616 (medium; Table 3). By definition, a reduction in these variables was expected and necessary to achieve asymptomatic status post-SRC, yet the breadth and extent of improvements further illustrates the interconnected nature of these variables as it appears unlikely that an athlete would reach asymptomatic status if only a few were significantly improved. That is, significant improvements in symptoms of psychological distress appear necessary to influence related improvements in neurocognitive functioning and vice versa. These findings again demonstrate potential avenues of clinical intervention following SRC as treating both sets of variables may be crucial to effective amelioration of negative consequences.
Limitations
The limitations of the present study are primarily a result of how study participants were defined, and the measures utilized to assess variables of interest. In light of these considerations, we discuss the following limitations. First, athletes who required more than 7 days to begin the RTP protocol were excluded from analyses. Although this was done to ensure the methodological rigor of our novel application of network analysis to an SRC sample, and to ensure the models were not overly influenced by those athletes who required much more time to reach asymptomatic status, it likely artificially restricted the between-variables relationships identified by the network. 7 To include a broader range of time-points (e.g., unrestricted RTP) and all athletes regardless of recovery time, we plan to develop multiple graphical models following development of the present proof-of-concept methodologies in order to better understand how observed variables and time influences these networks.
Second, possible sex differences were not included in the present analysis in order to simplify these proof-of-concept analyses. Future research that instead considers sex differences in the various interconnected networks of neurocognitive functioning and symptoms of psychological distress following SRC is warranted. 43,44 Third, pre-injury mental health diagnoses (e.g., depression, ADHD) were also not included in analyses, which possibly influenced athletes' neurocognitive functioning performance and self-report of current psychological symptoms. 45 And fourth, our analysis comprised primarily linear correlations between assessments. Although several insights were gleaned from this analysis, future investigation should consider the possibility of more complex relationships between measures, including non-linear and partial correlations.
Although several assessments were used to evaluate athletes following SRC, this study limited analysis to include only the BSI-18 and ImPACT tests. The manner in which we interpreted findings from the BSI-18, particularly at the 24–48 h time-point, differs from its original construct. That is, participant responses reported herein may reflect the presence of common post-SRC symptoms rather than enduring psychological distress. Finally, we did not include in the present network analyses all possible neurocognitive functioning and psychological symptom variables obtained during participation in the CARE Consortium studies. For example, we excluded the Standard Concussion Assessment Tool (SCAT) symptom checklist even though some portions of the checklist measure neurocognitive functioning. However, all the pertinent variables in the SCAT are already measured in the ImPACT test. As such, this restriction of variables was done to avoid overburdening the networks in order to more clearly demonstrate the methodological merits of network analyses in this population. In the future, network analyses that include more post-SRC variables (e.g., balance/vestibular functioning) should be completed to obtain a more accurate understanding of the heterogenous nature of post-SRC consequences.
Conclusions
The present study utilizes network analysis to graphically depict the complex and dynamic interrelationships between neurocognitive functioning and psychological symptoms that frequently occur following SRC at three time-points. This graph (Fig. 2) shows that the interrelationships between these variables were stronger at the 24–48 h time-point than at baseline or at the asymptomatic time-point. Further, all symptoms of psychological distress and neurocognitive functioning significantly improved from the 24–48 h time-point to asymptomatic status. The effect sizes of these changes ranged from 0.126 (small) to 0.616 (medium). This research suggests that significant improvements in symptoms of psychological distress appear necessary to drive related improvement in neurocognitive functioning and vice versa.
Data Sharing
The NCAA-DoD CARE data set is available in the FITBIR database. The network analysis code is accessible by contacting the corresponding author.
Footnotes
Acknowledgments
Alphabetically by last name, CARE Consortium Investigators include: Thomas Buckley, EdD (University of Delaware); Michael Collins, PhD (University of Pittsburgh); Stefan Duma, PhD (Virginia Tech); James Eckner, MD (University of Michigan); Luis Feigenbaum, PT (University of Miami); April Hoy, MS (Azusa Pacific University); Thomas Kaminski, PhD (University of Delaware); Anthony Kontos, PhD (University of Pittsburgh); Christina Master, MD (University of Pennsylvania); Jason Mihalik, PhD (University of North Carolina at Chapel Hill); Christopher Miles, MD (Wake Forest University); Patrick O'Donnell, MHA (University of Massachusetts Memorial Health); Justus Ortega, PhD (California Polytechnic University Humboldt); Julianne Schmidt, PhD (University of Georgia); Adam Susmarski, DO (United States Naval Academy).
We would also like to thank Jody Harland, Susan Perkins, Barry Katz, Janetta Matesan, and Larry Riggen (Indiana University), Ashley Rettmann, Nicole L'Heureux (University of Michigan), Melissa Koschnitzke (Medical College of Wisconsin), Michael Jarrett, Vibeke Brinck, and Bianca Byrne (Quesgen), Thomas Dompier, Christy Collins, Melissa Niceley Baker, and Sara Dalton (Datalys Center for Sports Injury Research and Prevention), and the research and medical staff at each participating site.
Authors' Contributions
SWL, CBT, ACS, and G-GPG contributed to the design of the study, data analysis, and writing of the manuscript. PFP, MAM, TWM, and SPB obtained the data set, secured funding, and revised the manuscript.
Funding Information
This publication was made possible in part by the NCAA and the U.S. DoD. The U.S. Army Medical Research Acquisition Activity (820 Chandler Street, Fort Detrick MD 21702-5014, USA) is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Combat Casualty Care Research Program, endorsed by the U.S. DoD, through the Joint Program Committee 6/Combat Casualty Care Research Program – Psychological Health and Traumatic Brain Injury Program under award no. W81XWH1820047. Opinions, interpretations, conclusions, and recommendations are those of the author and are not necessarily endorsed by the U.S. DoD.
Author Disclosure Statement
PFP, MAM, TWM, and SPB received research support from the NCAA and the U.S. DoD.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.