
Abstract
Traumatic brain injury (TBI) is a leading cause of death and disability in the United States. Early triage and treatment after TBI have been shown to improve outcome. Identifying patients at risk for increased intracranial pressure (ICP) via baseline computed tomography (CT) , however, has not been validated previously in a prospective dataset. We hypothesized that acute CT findings of elevated ICP, combined with direct ICP measurement, hold prognostic value in terms of six-month patient outcome after TBI. Data were obtained from the Progesterone for Traumatic Brain Injury, Experimental Clinical Treatment (ProTECTIII) multi-center clinical trial. Baseline CT scans for 881 participants were individually reviewed by a blinded central neuroradiologist. Five signs of elevated ICP were measured (sulcal obliteration, lateral ventricle compression, third ventricle compression, midline shift, and herniation). Associations between signs of increased ICP and outcomes (six-month functional outcome and death) were assessed. Secondary analyses of 354 patients with recorded ICP monitoring data available explored the relationships between hemorrhage phenotype/anatomic location, sustained ICP ≥20 mm Hg, and surgical intervention(s). Univariate and multi-variate logistic/linear regressions were performed; p < 0.05 is defined as statistically significant. Imaging characteristics associated with ICP in this cohort include sulcal obliteration (p = 0.029) and third ventricular compression (p = 0.039). Univariate regression analyses indicated that increasing combinations of the five defined signs of elevated ICP were associated with death, poor functional outcome, and time to death. There was also an increased likelihood of death if patients required craniotomy (odds ratio [OR] = 4.318, 95% confidence interval [1.330–16.030]) or hemicraniectomy (OR = 2.993 [1.109–8.482]). On multi-variate regression analyses, hemorrhage location was associated with death (posterior fossa, OR = 3.208 [1.120–9.188] and basal ganglia, OR = 3.079 [1.178–8.077]). Volume of hemorrhage >30 cc was also associated with increased death, OR = 3.702 [1.575–8.956]). The proportion of patient hours with sustained ICP ≥20 mm Hg, and maximum ICP ≥20 mm Hg were also directly correlated with increased death (OR = 6 4.99 [7.731–635.51]; and OR = 1.025 [1.004–1.047]), but not with functional outcome. Poor functional outcome was predicted by concurrent presence of all five radiographic signs of elevated ICP (OR = 4.44 [1.514–14.183]) and presence of frontal lobe (OR = 2.951 [1.265–7.067]), subarachnoid (OR = 2.231 [1.067–4.717]), or intraventricular (OR = 2.249 [1.159–4.508]) hemorrhage. Time to death was modulated by total patient days of elevated ICP ≥20 mm Hg (effect size = 3.424 [1.500, 5.439]) in the first two weeks of hospitalization. Sulcal obliteration and third ventricular compression, radiographic signs of elevated ICP, were significantly associated with measurements of ICP ≥20 mm Hg. These radiographic biomarkers were significantly associated with patient outcome. There is potential utility of ICP-related imaging variables in triage and prognostication for patients after moderate-severe TBI.
Introduction
Traumatic brain injury (TBI) is a leading cause of death and disability in the United States, 1 resulting in an estimated 2.87 million emergency department visits per year, approximately 288,000 hospitalizations, and 56,800 deaths. 2 A TBI is a heterogeneous disorder with variability in hemorrhage phenotype, volume of hemorrhage, extent of surrounding intraparenchymal edema, and anatomical location of pathology. 3 Factors such as diffuse axonal injury (DAI) and/or cerebral edema, in the setting of evolving cerebral hemodynamics and secondary brain injury, also influence intracranial pressure (ICP) and patient outcome. 4,5 Heterogeneity in TBI phenotype and the effects of polytrauma physiology make the tasks of triage, treatment, and prognostication challenging.
Outcomes after TBI do not reliably correlate with a single diagnostic tool, such as cerebral imaging. Therefore, clinicians must correlate pathophysiology, imaging findings, evolving cerebrovascular hemodynamics, and patient neurological exam. Tools that combine these metrics and correlate measurements with patient outcome are limited. 6
Early prognostic models of TBI utilized patient findings on computed tomography (CT) to predict death. 7 The Marshall score was the first of these tools and remains the most widely accepted, using CT findings such as: midline shift, compression of basal cisterns, and presence of hemorrhagic lesions >25 cc. 8 A newer CT-based predictive model, the Rotterdam score, incorporates presence of epidural hematoma (EDH) and intraventricular (IVH) or subarachnoid hemorrhage (SAH), while omitting hemorrhage volume data. 9 Both the Marshall and Rotterdam scores perform well at predicting death; however, neither strongly predicts functional outcome. 10 Nevertheless, these scales are based on initial post-trauma CT scan, making them useful tools for the immediate triage and classification of injury after impact/injury.
Since the Brain Trauma Foundation (BTF) guidelines 4th edition for the management of severe TBI were published in 2016, 11 it has become standard of care to directly measure ICP after TBI in patients with Glasgow Coma Scale score ≤8. Multi-modal data including ICP, cerebral perfusion pressure, and cerebral oxygenation, add further specificity to the characterization of the physiological effects of injury. An ICP ≥20 mm Hg has been directly correlated with functional outcome and death, and thus represent one target for intervention after TBI, although other thresholds (e.g., ICP ≥22) have also been proposed. 12,13 -15
Correlation of these data with CT-based imaging findings related to phenotype of injury has not been studied previously in a prospective cohort, although identifying imaging biomarkers of elevated ICP could enhance early predictive models, when assessed in combination with variables such as hemorrhage volume, location, and phenotype. 3,9,16 Previous investigators have tried to create scoring systems based on combinations of imaging and clinical data.
The International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) scoring system was derived from the Corticosteroid Randomization after Significant Head Injury (CRASH) trial. IMPACT includes imaging findings, laboratory data, and the neurological examination available on initial patient admission. Being outside of the scope of these databases, however, these data do not assess the total burden of physiological response to injury, such as duration of sustained elevated ICP, hypoxemia, hypotension, or fever. 17 No20previous investigation has assimilated the prospectively captured measurement of intracranial pathophysiology and CT-based biomarkers over time. 18
The Progesterone for Traumatic Brain Injury, Experimental Treatment (ProTECTIII) trial cohort benefited from rigorous recruitment and monitoring standards and has been studied previously to construct predictive models that incorporate physiological parameters, such as: mean arterial pressure (MAP), blood oxygenation, cerebral perfusion pressure (CPP), ICP, brain tissue oxygenation (PbtO2), temperature, anemia, and coagulopathy to correlate these data with patient outcomes after TBI. 1,13 Prediction of outcome after TBI requires the correlation of such data to aid in the assessment of evolving physiological and anatomical pathology. Factors such as maximum value of ICP ≥20 mm Hg, sustained ICP ≥20 mm Hg, hemorrhage phenotype/location, and surgical intervention are related to functional outcome and death. 19
While prediction of death has been demonstrated previously, predicting patient functional outcome in the early post-injury period has remained challenging. In the present study, we utilized prospectively collected data from 881 patients enrolled in the ProTECTIII trial to study the hypothesis that acute CT findings of elevated ICP, combined with direct ICP measurement, predict six-month patient outcome after TBI. The association between CT biomarkers and physiological characteristics of TBI was analyzed via multi-variate regression analysis. The CT biomarkers were correlated with six-month patient functional outcome and death. This model provides valuable data that may lead to better prediction of outcome and improved guidance for clinical decision-making.
Methods
Data source
Data were derived from the prospective dataset obtained during ProTECTIII, 1 a randomized multi-center phase-III clinical trial to determine the efficacy of intravenous progesterone as a neuroprotective agent when administered within 4 h of TBI. Patients with non-penetrating moderate to severe TBI (Glasgow Coma Scale score [GCS] 4–12) who presented to participating United States trauma centers within 4 h of injury were screened for enrollment. Patients with hypoxia, hypotension, spinal cord injury, status epilepticus, and bilateral unreactive pupils were excluded.
A composite functional outcome metric using the Glasgow Outcome Scale, Extended (GOS-E) and Disability Rating Scale (DRS) endpoints was measured at six months, the limit of prospective follow-up during ProTECTIII. The 882 patients were enrolled in ProTECTIII from 2010 to 2013 before its cessation for futility in the primary outcome (effect of progesterone vs. placebo). Data from this cohort, however, include rigorously adjudicated multi-modal monitoring and cross-sectional imaging, representing one of the largest prospective TBI cohorts nationally.
Standardization of methods throughout the clinical trial was optimized; for example, all baseline head CT data were acquired within 4 h of TBI. All imaging findings were coded prospectively in a standardized imaging case report form (CRF) by a blinded central neuroradiologist. Each imaging CRF included 70 imaging biomarkers per patient.
Covariates and outcomes
For the purposes of the present analyses, the ProTECTIII data were applied to identify predictive markers of death and poor outcome. Poor functional outcome was defined as DRS ≥6 or GOS-E ≤5. Data on clinical and imaging characteristics, ICP, and surgical intervention (craniotomy, hemicraniectomy, or external ventricular drain placement) were assessed.
The predictive value of physiological variables including ICP has been described previously. 13 For example, a recorded ICP “transgression” is defined as an instance of ICP ≥20 mm Hg that persists for at least 10 min duration. The threshold of 20 mm Hg was selected based on past analyses of the ProTECTIII dataset. 13 The proportion of time with elevated ICP is computed as the proportion of hours during which at least one such transgression was recorded, divided by the total number of hours over which ICP recordings were maintained. Maximum ICP is the greatest absolute ICP value measured during any transgression. Analysis of correlation between CT data and ICP recordings is limited to those patients in whom invasive monitoring was performed (GCS ≤8, n = 354).
Imaging variables extracted for use in the present analysis include five signs of elevated ICP (sulcal obliteration, lateral ventricular compression, compression of the third ventricle, presence of midline shift, and visualized herniation). Visualized herniation was itself a composite metric that included transtentorial, uncal, tonsilar, or upward herniation present on head CT. Phenotype of lesions include subdural hematoma (SDH), EDH, SAH, intraparenchymal hemorrhage (IPH), multi-focal contusion, IVH, and DAI. Location of lesion is defined as: lobar, basal ganglia, or infratentorial hemorrhage. Presence of lesions ≥30 cc based on volume is assessed; volumes were measured using methods of semi-automated lesion segmentation and volume estimation published previously by these authors. 3
Statistical analysis
Data analyses were performed using R (R 4.0.5 and R Studio 1.4). Multi-variate logistic regressions were applied to evaluate the association of clinical covariates, such as signs of increased ICP or phenotype/location of traumatic hemorrhage, with binary response variables, defined as death and poor functional outcome. To analyze continuous response variables, such as maximum ICP, average ICP, and time until death, multiple linear regressions and analysis of effect size were used. The proportion of time spent with ICP ≥20 mm Hg of the total time over which ICP measurements were recorded, was also considered as a separate continuous response variable. Number of CT biomarkers of elevated ICP was assessed as a categorical predictor.
Statistical significance (p value) was calculated by using Wald test and F test under assumption of logistic regression and linear regression, respectively, with 95% confidence interval (CI) and p < 0.05 utilized to define statistical significance. Odds ratios (ORs) and CIs for regression coefficients were calculated.
Receiver operating characteristic (ROC) curves assessing accuracy of the composite number of signs of elevated ICP on CT, Marshall score, and Rotterdam scores as three potential predictors of patient outcome (death and poor six-month functional outcome) were calculated and compared. Calculations were based on 100 iterations of logistic regression with an 80/20 training/testing split. Areas under these curves (AUC) values were subsequently calculated and reported with the 95% CI displayed.
Results
Of 882 subjects enrolled in ProTECTIII, 881 were included in this analysis. One patient was excluded because of lack of baseline head CT; 700 (79.5%) were male and 181 (20.5%) were female. At time of enrollment, median age was 35 years (range 17–94). Eighteen patients were further excluded because of loss to follow-up before completion of outcome assessment. There were 354 (40.2%) patients treated with invasive ICP monitoring, of whom 118 (13.4%) were noted to have elevation of ICP ≥20 mm Hg (defined as ICP “transgression”). Duration and magnitude of ICP transgression were included in the analyses of the ICP covariate.
Most patients (n = 706) were noted to have positive initial head CT demonstrating traumatic lesions within 4 h of TBI. These include 582 patients (66.1%) with traumatic SAH, 424 (48.1%) with SDH, 352 (40.0%) with contusions, 247 (28.0%) with diffuse axonal injury, 193 (21.9%) with IVH, 126 (14.3%) with EDH, and 42 (4.8%) with solitary IPH. In terms of individual CT signs of elevated ICP: 211 patients (24.1%) demonstrated third ventricle compression, 205 (23.3%) lateral ventricle compression, 196 (22.2%) sulcal obliteration, 190 (21.6%) midline shift, and 158 (17.9%) visualized herniation; 612 patients (69.5%) had none of these five findings identified, while 99 (11.2%) were noted to have all five signs of increased ICP present.
Among the cohort of patients with ICP recordings available for analysis, 236 (66.7%) had none of these five signs present on baseline CT, similar to the proportion in the overall study population. Additional descriptive and radiographic patient characteristics are presented in Table 1.
Descriptive Table Summarizing Population Characteristics
SD, standard deviation.
Relationship between CT biomarkers of increased ICP and patient morbidity and death
Patients with no signs of increased ICP on initial CT scan were less likely to die than patients with signs of increased ICP (OR = 0.183, 95% CI [0.126, 0.266], p < 0.001). As the number of defined signs of increased ICP increased on a patient's initial head CT (n = 1-5), so did the patient's odds of both death and poor functional outcome (Table 2).
Multi-Variate Regressions Assessing Relationship of Cumulative Number of Computed Tomography Signs of Elevated Intracranial Pressure With Patient Outcomes and Proportion of Time in Intracranial Pressure Transgression
Time to death was significantly related to number of CT biomarkers of increased ICP: time to death was shorter in patients with all five CT biomarkers (mean difference -17.022 days, 95% CI [-30.735, -3.309], p = 0.015), and significantly longer in those with none of the five CT biomarkers (mean difference 14.363 days, 95% CI [2.688, 26.037], p = 0.016). Further, having four or five of these biomarkers was significantly associated with increased odds of poor six-month functional outcome (OR = 2.648, 95% CI [1.508, 4.650], p < 0.001; OR = 5.644, 95% CI [3.270, 9.744], p < 0.001). Time until death was also longer with greater number of days with recorded ICP ≥20 (effect size 3.424 days, 95% CI [1.500, 5.439], p < 0.0001; Table 4)
ICP measurement ≥20g is correlated with specific biomarkers on baseline head CT
Of the five CT biomarkers of elevated ICP intracranial pressure assessed in a binary fashion (Fig. 1), several were also correlated with trends in subsequent ICP transgression during hospitalization in the subset of 354 patients with recorded ICP monitoring data (Table 3). Specifically, higher maximum ICP was predicted by sulcal obliteration (mean 41.418 mm Hg, 95% CI [37.592, 45.244], p = 0.029) and third ventricle compression (mean 41.403 mm Hg, 95% CI [37.377, 45.429], p = 0.039), but not by lateral ventricle compression (mean 39.358 mm Hg, 95% CI [36.155, 42.561], p = 0.135), midline shift (mean 39.200 mm Hg, 95% CI [35.369, 43.031], p = 0.454), or visualized herniation (mean 41.274 mm Hg, 95% CI [36.467, 46.081], p = 0.855). Patients with sulcal obliteration also tended to spend a greater proportion of monitored hours in ICP transgression (0.263, 95% CI [0.226, 0.299], p = 0.007) than patients without sulcal obliteration. This was not true of the other four CT biomarkers of elevated ICP (Table 3).
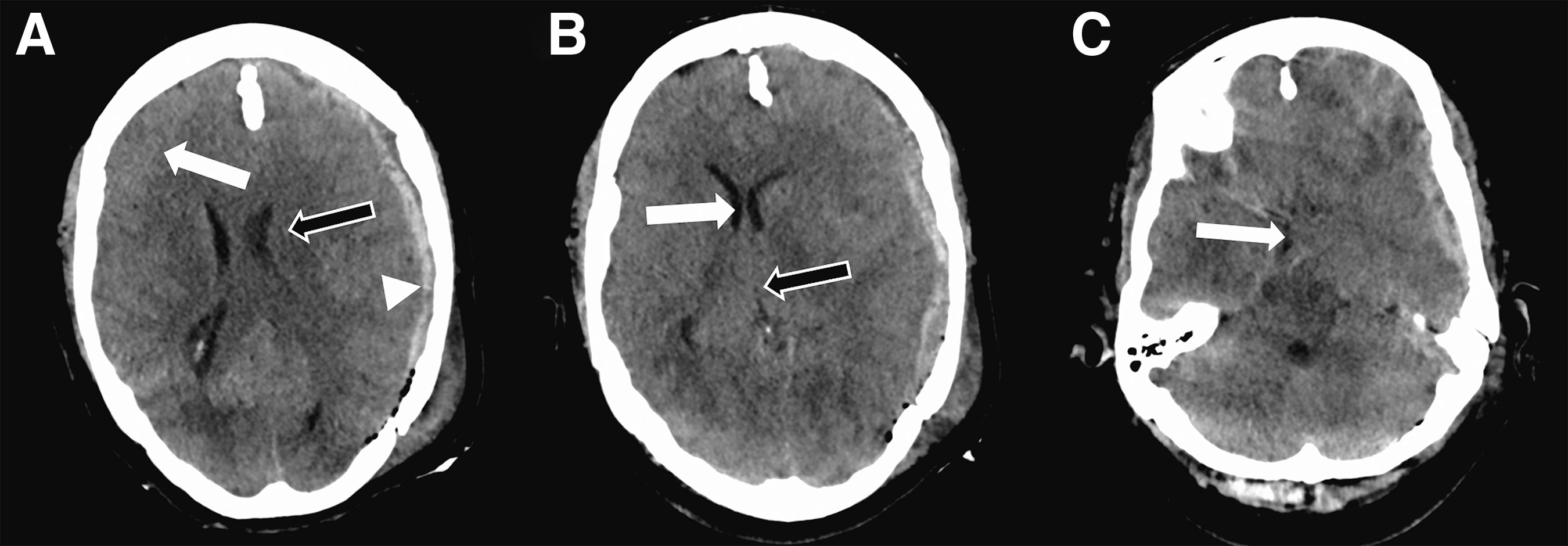
Example of baseline head CT axial images from the ProTECTIII cohort demonstrating (
Multi-Variate Regressions Assessing Relationship of Individual Computed Tomography Signs of Elevated Intracranial Pressure With Patient Outcomes and Proportion of Time in Intracranial Pressure Transgression
ICP, intracranial pressure.
Relationship between ICP, baseline CT findings, and patient morbidity and death
Including only those 354 patients with recorded ICP monitoring data, we conducted a multi-variate logistic regression with covariates including the number of signs of elevated ICP, measured ICP characteristics (maximum ICP, number of days with ICP ≥20, and proportion of hours with ICP ≥20), and hemorrhagic lesion characteristics including size, phenotype, and location. Several variables were found to independently predict death, poor functional outcome at six months, and time until death (Table 4). In particular, odds of death were lower with more days spent in ICP transgression (OR = 0.843, 95% CI [0.761, 0.926], p = 0.001), higher with greater maximum reported ICP (OR = 1.025, 95% CI [1.004, 1.047], p = 0.021), and higher proportion of monitored hours positive for ICP transgression (OR = 6 4.99 95% CI [7.731, 635.51], p < 0.001).
Multi-Variate Regression Assessing Number of Computed Tomography Findings of Elevated Intracranial Pressure, Measured Intracranial Pressure, Hemorrhage Locations, Hemorrhage Phenotypes With Patient Outcomes
ICP, intracranial pressure; DAI, diffuse axonal injury.
Notably, measured ICP transgression variables were not associated with odds of poor functional outcome (Table 4). Conversely, in terms of CT biomarkers, having all five signs of elevated ICP remained associated with greater odds of poor functional outcome on multi-variate regression (OR = 4.44, 95% CI [1.514, 14.183], p = 0.009), but not death (OR = 2.133, 95% CI [0.755, 5.978], p = 0.149). Taken together, results suggest that measured ICP transgression patterns better predicted patient death, but not poor functional outcome.
In the same models, patterns of traumatic hemorrhage location, size, and phenotype were associated with death and poor functional outcome, respectively, but not with time until death. Predictors of death included hemorrhage location in the posterior fossa (OR = 3.208, 95% CI [1.12, 9.188], p = 0.029) and basal ganglia (OR = 3.079, 95% CI [1.178, 8.077], p = 0.021), but not hemorrhage phenotype including EDH (OR = 0.565, 95% CI [0.236, 1.283], p = 0.185) or SDH (OR = 1.13, 95% CI [0.515, 2.503], p = 0.761). Presence of a hematoma >30 cc in volume was associated with death (OR = 3.702, 95% CI [1.575, 8.956], p = 0.003). Poor functional outcome at six months was significantly associated with hemorrhage in the frontal lobe (OR = 2.951, 95% CI [1.265, 7.067], p = 0.013), SAH (OR = 2.231, 95% CI [1.067, 4.717], p = 0.034), and with IVH (OR = 2.249, 95% CI [1.159, 4.508], p = 0.019).
These analyses were controlled for application of neurosurgical intervention including external ventricular drain (EVD), hemicraniectomy, and/or craniotomy, although these features were not found to independently predict any of the three outcome variables studied. Additional results detailing associations of hemorrhage phenotype and location variables without the ICP variables included in this model have been published previously as conference proceedings. 16
Death and functional outcome based on surgical intervention
Of the 881 patients, 28 (3.2%) required craniotomy, 36 (4.1%) required decompressive hemicraniectomy, and 153 (17.4%) required EVD placement (Table 5). Cumulatively, 143 (16.2%) patients received one of these interventions, 28 (3.2%) received two, and six (0.7%) received all three interventions. Patients were more likely to die if they required craniotomy (OR = 4.318, 95% CI [1.33, 16.03], p = 0.019) or hemicraniectomy (OR = 2.993, 95% CI [1.109, 8.482], p = 0.031), but death was not associated with EVD placement (OR = 1.513, 95% CI [0.844, 2.719], p = 0.164). Odds of death increased with the number of interventions required (p = 0.008); OR = 4.219 (95% CI [1.528, 11.826] for patients needing two interventions (p = 0.005).
Multi-Variate Logistic Regression Assessing Relationships Between Specific Intervention Variables and Cumulative Number of Interventions Performed with Patient Outcomes
Intervention-related covariates, including craniotomy, craniectomy, EVD, and time to surgery, were not significantly associated with time to death in these analyses (Table 5). In this cohort, time to surgical intervention was also not significantly associated with mortality or functional outcome.
CT composite biomarkers of increased ICP compared with Marshall and Rotterdam scores
Building on the above analyses, we assessed how composite number of signs of elevated ICP on baseline head CT compared as a predictive marker to the established, multi-factorial Marshall and Rotterdam scoring systems in this study cohort. Results of ROC curve analysis are displayed in Figure 2. All three metrics were significantly better predictors of death than poor functional outcome (composite number of CT signs of elevated ICP, AUC = 0.714 [0.694, 0.734] vs. AUC = 0.624 [0.611, 0.637]; Marshall score, AUC = 0.754 [0.733, 0.744] vs. AUC = 0.637 [0.623, 0.651]; Rotterdam score, AUC = 0.720 [0.695, 0.744] vs. AUC = 0.647 [0.631, 0.663]). None of the three metrics was statistically better than any other in terms of predicting outcome.

Receiver operating characteristic (ROC) curves demonstrating accuracy of composite number of computed tomography (CT) signs of elevated intracranial pressure versus Marshall and Rotterdam scores for predicting (
Discussion
The present study includes a comprehensive, multi-variate assessment of how imaging and longitudinal ICP monitoring data relate to patient death and functional outcome after moderate to severe TBI. Further, we underscore how image-based biomarkers of elevated ICP are individually related to ICP monitoring data in a sizable prospective cohort, present a composite imaging biomarker based on five distinct findings, and compare overall performance of this biomarker against pre-existing predictive scores. While many of the individual trends found have been reported previously, we believe this is the first attempt to derive a combined and fully integrated model across imaging and longitudinal physiological data. Curation of these data would only be possible in the context of a multi-center clinical trial or prospective registry tracking patients closely on a day-to-day basis during the post-injury inpatient stay.
Patient prognostication in moderate to severe TBI
While many past studies have been performed to evaluate predictors of outcome after TBI, these have fallen short of incorporating all pertinent variables into the same model and have largely been unable to identify meaningful correlations with functional outcome. In a study in Latin America, hospital deaths rose and functional outcome decreased, with Marshall grade of injury, SDH, IVH, and intracerebral hemorrhage, as well as elevated initial ICP. 20 Midline shift and cisternal effacement on imaging independently correlated with poor outcome while EDH had a more favorable outcome. 20 Others report that age, ambient and crural cistern effacement, hypodensities seen on post-decompressive hemicraniectomy scans, initial GCS score, and Abbreviated Injury Severity (AIS) score, and contrast extravasation on CTA together correlate with worse outcome. 21 –23
In data collected for the CLEAR-III trial (non-traumatic ICH/IVH), single events of sustained ICP >18 mm Hg and >30 mm Hg (studied separately) were predictors of short-term death. Successive ICP >20 mm Hg for any amount of time was predictive of long-term death. 24 While a threshold of ICP ≥20 was also found to be significantly related to outcome in the ProTECTIII trial data, 13 others have more recently suggested a threshold of ICP ≥22 as a potential cutoff. 14,15 In clinical practice, an ICP and CPP thresholds should be guided on an individualized basis by real-time assessment of physiological response, whenever possible.
Along these lines, it has been challenging to account for the evolving pathophysiology of TBI over the time after injury and heterogenous injury types collectively categorized as TBI on past analyses. Modern multi-modal physiological monitoring in the ICU offers the opportunity to study longitudinal covariates, such as sustained elevations in increased ICP, 1,13,25 and direct measurement of cerebral oxygenation. 1,13,25,26 The opportunity to leverage some of these data available from the ProTECTIII cohort was a major motivation for the present study and could help underpin more individualized treatment guidelines.
The IMPACT/CRASH score has been studied extensively and is an excellent tool to discriminate across large cohorts of patients. Numerous studies have been conducted to validate the scoring tool with outcomes varying widely based on inclusion criteria. 27 The lack of continuous ICP and other detailed physiologic data, however, remains a potential limitation of the IMPACT tool.
Elevated ICP has long been accepted as a predictor of death and poor neurological outcome, and direct measurement of ICP is a standard of goal-directed therapy for severe TBI. 11,13,28 -30 Previous studies have demonstrated that positive baseline head CT in combination with subsequent sustained ICP is associated with poor outcome, a finding in both adult and pediatric patient populations. 31,32 Therefore, it is reasonable to hypothesize that modern predictive tools may benefit from inclusion of ICP transgression measurement alongside detailed characterization of structural pathology observed on imaging. The inclusion of additional physiological covariates, such as hemoglobin, mean arterial pressure, and coagulation parameters, could be of even further utility in this regard. 13,33 -37
Toward a unified model combining CT biomarkers and ICP monitoring data
Building on this previous literature, we present the first comprehensive integration of imaging and longitudinal ICP measurement data in a large, prospective, multi-center study of patients with moderate to severe TBI. We demonstrate a multi-variate model that identifies maximum ICP, proportion of time with elevated ICP, hemorrhage volume >30 mL, and hemorrhage locations in the basal ganglia and posterior fossa as significant independent predictors of patient death. The SAH, IVH, and frontal lobe hemorrhage were identified as independent predictors of patient six-month functional outcome (Table 4).
Focusing on direct ICP measurements during the index hospitalization, we demonstrate that higher maximum ICP is best predicted specifically by sulcal effacement and compression of the third ventricle, while lateral ventricle compression, third ventricle compression, and visualized herniation (including transtentorial, uncal, tonsilar, or upward herniation) are related to higher average ICP value (Table 3).
Taken together, these findings highlight specific patterns of CT findings that may enable earlier prognostication and ultimately guide treatment decision making. Whether changes in clinical decisions made based on better understanding of patient prognosis would enable more targeted ICP control after severe TBI is yet to be seen, limited significantly by the potential collinearity of several of the variables included in our model. Further, the addition of ICP spikes and derived duration of ICP ≥20 mm Hg may offer improvement in predictive capability for individual patients (Table 4). 24
Despite these findings, it should be noted that our results also highlight that approximately 67% of patients for whom ICP monitoring was implemented in the ProTECTIII trial did not have any of the five signs of elevated ICP we studied present on baseline head CT. This is a principle entrenched in the BTF guidelines: while CT findings of elevated ICP may augment prognostication models, these findings alone should not be relied on for deciding whether to intervene on clinically suspected ICP elevation. 29 In fact, it is entirely possible that early intervention may have contributed to effective ICP management in a subset of our cohort, an interaction that we did not specifically study.
A new composite imaging biomarker was defined as the number of CT signs of elevated ICP and was found to be predictive of patient outcome (Table 2). We compared this individual metric with more established imaging-based scoring systems (Marshall, Rotterdam). In terms of both death and six-month morbidity across our cohort of 881 subjects, neither the Marshall nor Rotterdam scoring system better predicted patient outcome than number of CT signs of elevated ICP alone (Fig. 2). This same metric was interestingly an independent predictor of six-month functional outcome on our multi-variate analysis, while the physiological monitoring data was not (Table 4).
For prediction of death, the reciprocal was true: ICP monitoring data significantly and independently predicted death, while their CT-derived correlates did not. While death prediction has been more extensively and successfully studied, our analysis identified several biomarkers abstracted from baseline non-contrast head CT that predict poor functional outcome six months after injury—namely, presence of all five radiographic signs of elevated ICP, presence of frontal lobe hemorrhage, and presence of traumatic subarachnoid and/or intraventricular hemorrhage.
The Marshall and Rotterdam scores focus on some critical imaging findings as predictors of death, but do not incorporate imaging variables that are demonstrably important for patient functional outcome as evidenced through the present study, such as hemorrhage phenotype and volume quantification. 3,10,16 While useful for initial evaluation, these scores lack the refinement and updated prognostic value of continued serial data beyond primary injury and into the secondary injury phases, at which point an updated prognostication may be warranted in light of new information that arises during the patient's critical care course. 13 Our results strengthen the idea that detailed radiographical information could be combined with measured ICP trends to achieve progressively improved prediction of functional outcome at the earliest possible point during the course of care.
Implications and future directions
Overall, this study provides essential data regarding the relationship between baseline imaging, monitored ICP transgression, and six-month patient outcome that will subserve the formulation of a multi-modal TBI outcomes predictor based on coupled radiographical findings and physiologic monitoring. Here, we focus on the addition of time spent above threshold ICP ≥20 mm Hg over the course of inpatient ICP monitoring.
Many of the findings in this analysis contribute to the framework established by previous generations of predictive models that collectively aim to better inform clinicians and families as they make critical decisions regarding long-term care planning and interventions. Future studies should seek to incorporate additional physiological and biomarker data toward improved prognostication and should perhaps consider subsets of this heterogenous population as distinct entities (e.g., patients with primarily intra- vs. extra-axial traumatic pathology). Goal-directed therapy, including ICP, PbtO2, CPP management, and other physiological and serum biomarker data, may enable increasingly precise patient prognostication.
Limitations
As a secondary analysis of the original trial data, the study was not powered for significance across all variables assessed. Further, our analyses relied on previously defined thresholds utilized in past studies of the ProTECTIII dataset t that have been found to be related to patient outcome, including an ICP threshold of ≥20 mm Hg and an unfavorable GOSE ≤5. Understanding of optimal thresholds for these and other metrics, in research and clinical practice, continues to evolve. 13 -15,38,39
More broadly, the applicability of our findings may be limited by practice- and setting-dependent variation in the adoption of guideline-based ICP monitoring in moderate to severe TBI, although we believe including ICP measurements in models such as ours at this stage of understanding is well evidenced. 11,30,40 We did not include the effect of cerebral autoregulation status within the regression model, although future research should incorporate these data. 41 We do not consider the other sets of physiological covariates compiled within the ProTECTIII trial dataset, 13 although future investigations will be undertaken to assess these data, as well as serum biomarker data. 42,43 Further, while the patients included in the present post-hoc analysis of the ProTECTIII trial dataset were randomized initially to one of two treatment groups, previous work has demonstrated that randomization had no impact on physiological transgression data including ICP. 13
Future prospective studies are needed to develop and validate a cohesive outcomes score based on the presented regression results and to clarify cut-off percentages for risk of death and poor functional outcome. Such a study may draw on the statistical relationships defined in the present study (e.g., using ORs reported in our data tables to weight various variables accordingly) to build the model, but should ultimately evaluate the model using an independent patient cohort that includes some or all of the multi-modal data available for the ProTECTIII trial cohort.
Conclusions
Sulcal obliteration and third ventricular compression are radiographic signs of elevated ICP associated with directly measured ICP ≥20 mm Hg. These radiographic biomarkers are associated with patient outcome and might be incorporated into prognostic models along with other imaging biomarkers and directly measured ICP elevation. Further investigation should study the potential utility of such combined models in contributing to outcomes-focused prognostication after moderate to severe TBI.
Footnotes
Acknowledgments
Portions of the data presented in this article were previously presented as oral and/or poster presentations at the Society for Critical Care Medicine (2020) and National Neurotrauma Society (2022) annual meetings.
Authors' Contributions
Tyler J. Harder: Formal analysis, Conceptualization, Investigation, Data Curation, Writing – Original Draft, Writing – Review & Editing; Owen P. Leary: Formal analysis, Conceptualization, Investigation, Data Curation, Project administration, Writing – Original Draft, Writing – Review & Editing; Zhihui Yang: Formal analysis, Methodology, Investigation, Writing – Review & Editing; Brandon Lucke-Wold: Conceptualization, Investigation, Writing – Original Draft, Writing – Review & Editing; David D. Liu: Formal analysis, Methodology, Investigation, Writing – Review & Editing; Megan E. H. Still: Writing – Original Draft, Writing – Review & Editing; Miao Zhang: Formal analysis, Investigation, Writing – Review & Editing; Sharon D. Yeatts: Methodology, Investigation, Writing – Review & Editing; Jason W Allen: Data Curation, Methodology, Investigation, Writing – Review & Editing; David W. Wright: Conceptualization, Investigation, Resources, Writing – Review & Editing; Derek Merck: Methodology, Investigation, Resources, Project administration, Writing – Review & Editing; Lisa H. Merck: Conceptualization, Investigation, Resources, Project administration, Writing – Review & Editing.
Funding Information
The ProTECTIII clinical trial and collection of data used for this study was supported by grants from the National Institutes of Health and National Institute of Neurological Disorders and Stroke (NS062778, 5U10NS059032, and U01NS056975) and the National Center for Advancing Translational Sciences of the National Institute of Health (UL1TR000454), and by the Emory Emergency Neurosciences Laboratory in the Department of Emergency Medicine, Emory School of Medicine, and Grady Memorial Hospital.
Detailed annotation and curation of the ProTECTIII clinical trial baseline imaging data completed as part of this study was supported by grant funding from the National Institutes of Health and National Institute of Neurological Disorders and Stroke (5U01N2O62778-05REV, Sub-award T129489), and by the Brown Emergency Neurosciences Research Division in the Department of Emergency Medicine and the 3D Laboratory in the Department of Diagnostic Imaging, Warren Alpert Medical School of Brown University, and Rhode Island Hospital.
Author Disclosure Statement
No competing financial interests exist.