
Abstract
Rapid technology advances have led to diverse assistive technology (AT) options for use in memory rehabilitation after traumatic brain injury (TBI). This systematic review aimed to evaluate the efficacy of electronic AT for supporting phases of memory in daily life after TBI. A secondary aim was to examine user perspectives on the utility of AT and factors influencing uptake or use. A systematic search of PsycINFO, MEDLINE, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Excerpta Medica database (Embase), Scopus, and Cochrane Library was conducted from database inception to June 13, 2022, to identify eligible studies. Methodological quality was assessed by two independent reviewers. Nineteen eligible articles involving a total of 311 participants included four randomized controlled trials (RCTs; Class I), five single-case experimental designs (Class II), and 10 pre-post group (n
Introduction
Assistive technology (AT) refers to products, systems, and services used to maintain or enhance the functional capabilities of its user. 1 These include a range of devices, from low-tech (e.g., glasses, walking cane) to high-tech equipment, including mobile phones and home automation systems. AT has been shown to support diverse aspects of physical, cognitive, social, and behavioral functioning after traumatic brain injury (TBI). The advancement of digital and electronic technologies has enabled the increased use of AT in rehabilitation after TBI to deliver interventions (e.g., through iPads and virtual reality), support individuals' adjustment to their functional impairments, and promote independence in the home and community. 2 Although AT may support diverse aspects of physical, cognitive, social, emotional, and behavioral functioning after TBI, due to the prevalence and consequences of memory impairment there has been considerable research focus on technological aids to support memory function. 3
Memory entails dynamic processes related to the encoding, storage, and retrieval of information, enabling individuals to retain knowledge of their prior experiences, draw upon these in the present, and act upon future intentions and goals. 4 Damage to fronto-temporal pathways following TBI commonly results in the impaired ability to learn new information and perform timely actions in the future (i.e., prospective memory). Such difficulties are a major source of frustration for individuals with TBI and their caregivers, impacting independence and vocational functioning. 5,6 Memory processes are vital to link one's past, present, and future selves. 7 The inability to recall one's life experiences, hold in mind current intentions, and carry out goal-relevant actions can negatively impact individuals' self-identity. 8
Improving memory function or individuals' ability to cope with memory impairment is a major focus of cognitive rehabilitation after TBI. Rehabilitation approaches can be broadly classified into remediation, or targeted training to improve cognitive processes underlying memory, and compensatory approaches that aim to mitigate the impact of memory impairment through strategy use. 6 In terms of the former, despite some evidence of effectiveness of remedial approaches (e.g., computerized training) for improving performance on training tasks or those similar to training, there is little evidence that such gains generalize to the ability to recall information in daily life. 9 –11
Compensatory approaches to memory rehabilitation typically focus on environmental supports (e.g., caregiver education, daily routines, and environmental organization) and use of internal and external memory aids. The latter approach aims to improve individuals' understanding of the benefits of memory aids, ability to recognize and anticipate memory problems in daily life, and training in the effective use of strategies. Systematic reviews support the benefits of internal memory aids including instructional and/or metacognitive strategies (e.g., visualization/visual imagery; Preview, Question, Read, Summarize & Test [PQRST]; self-generation; retrieval practice), particularly for individuals with mild to moderate memory impairment with preserved executive functioning. 10,12 For individuals with more severe memory impairments, external memory aids and environmental supports (e.g., diaries/notebooks, mobiles/smartphones, paging systems, whiteboards) are found to be more beneficial than internal memory strategies. 12
In a study investigating self-reported use of memory strategies and predictors of use after brain injury, Jamieson and colleagues 13 found that the most used strategies included: leaving objects in noticeable places (86%), calendars (79%), reminders from significant others (78%), lists (78%), mentally retracing one's steps (77%), and diaries (77%). AT devices such as mobile phones for reminders (38%) and alarms/timers (38%) were less common, although more frequent in younger adults who were familiar with technology prior to their injury.
Over the last few decades, rapid developments in technology have increased the accessibility and availability of electronic AT to support individuals' independence in the home and community. 14 Two broad types of AT relevant to memory function are important to distinguish, namely, micro-prompting systems designed to support task performance within a specific context, and devices that can be flexibly employed to compensate for a broad range of everyday memory demands. Micro-prompting systems, such as the Cognitive Orthosis for coOKing (COOK) 15 and navigation systems, 16 provide step-by-step prompting to ensure successful task execution. Often referred to as cognitive orthoses, these systems provide high-level support across all phases of task execution, including planning, organization, decision-making, memory, and sequencing, in specific contexts (e.g., cooking select meals in a specific kitchen, finding a specific route). Although such cognitive support systems can improve safety and reduce supervision needs, 15,16 these need to be adapted or reprogrammed for different tasks and/or settings and are not designed to improve individuals' self-regulation skills or flexible use of memory strategies across multiple everyday contexts.
Training individuals with TBI to use AT to support memory function across a broad range of daily contexts has the potential to improve independence, occupational functioning, and psychological well-being. AT can support both retrospective (e.g., autobiographical memory) and prospective (e.g., time-, event-, and or activity-based) remembering. This may include supporting individuals to record salient life experiences or important information for later retrieval, setting timely reminders or alerts to perform a task (e.g., take medication) during an ongoing activity, and future reminding of goal-directed actions (e.g., attend appointments and social events). Successful use of a memory aid requires both the input and output phases. 17 In line with theories of prospective memory, 18 these phases can be further distinguished as: intention formation and encoding (registering an intention for future action), retention (storing the content of the intention over time and maintaining it in mind while engaged in an ongoing task), retrieval (recognizing the cue and recalling the intention at the appropriate time or event), execution (ceasing or switching from the ongoing activity to carry out the intention), and evaluation (confirmation of outcome).
There is an extensive body of literature on the efficacy of remedial or restorative approaches and internal and external compensatory aids for addressing memory impairment after brain injury. 10,12 The most robust support, or Level I evidence (i.e., at least one meta-analysis, systematic review, or randomized controlled trial (RCT) of appropriate size with a relevant control group), is for the efficacy of external compensatory memory aids. However, relatively few reviews have focused on the efficacy of electronic AT for improving memory-related functioning after TBI.
In an early review focused on electronic AT for cognition for diverse clinical populations, Gillespie and associates 19 identified that technology has been used to support memory, attention, calculation, emotion, experience of self in the environment (e.g., navigation), and higher-order cognitive functions (e.g., time management and planning). Seven studies reported on AT for supporting memory function, including cameras (SenseCam) and multi-media reminiscence devices. Notably, most studies were descriptive and reported on the design or development of the AT and hence empirical support for use of AT to support memory function is limited.
In a systematic review and meta-analysis of cognitive prosthetic technology for memory after acquired brain injury (ABI), Jamieson and colleagues 3 identified 32 single-case experimental designs (SCEDs; 17 reporting data for non-overlap of all pairs analysis) and 11 group studies, 7 of which were included in the meta-analysis. The meta-analysis revealed a large effect size supporting the efficacy of cognitive prosthetic technology. For the SCEDs, the effect of intervention was medium overall, with stronger effects evident for micro-prompting than prospective prompting devices. Notably, their review included study samples involving any type of brain injury or neurological/degenerative disease and approximately one-third of studies evaluated micro-prompting systems. Due to the heterogeneity of injury etiology (e.g., stroke, trauma, encephalitis, multiple sclerosis, dementia), the efficacy of AT for supporting memory function after TBI was not able to be ascertained.
In a review of electronic portable assistive devices for people with ABI, Charters and co-workers 20 identified insufficient evidence to recommend the use of these devices as a practice standard due to the lack of well-designed RCTs. Most studies employed case control, single-case experimental methodology or pre-post designs. Based on these designs, there was sufficient evidence to recommend use of electronic reminder systems (e.g., personal digital assistants, smartphone, voice recorders) to support everyday memory as a practice guideline.
Kettlewell and colleagues 21 evaluated the efficacy of “personal smart technologies” for improving independence, goal attention, fatigue, or quality of life after ABI. Although the focus was not on memory specifically, the devices included AT commonly used for prospective remembering (e.g., personal digital assistant, smartphone application, mobile messaging). The authors evaluated six RCTs rated as having high methodological quality on the Physiotherapy Evidence Database (PEDro) 22 and conducted a meta-analysis on four of these studies. Sample characteristics were broad in terms of etiology, with studies including individuals with TBI, stroke, anoxia, infection, and brain tumor. Overall, they found no significant effect of personal smart technology on outcomes and concluded that there is presently insufficient evidence to support the clinical benefits. They noted that most devices were not selected or tailored to individuals' needs, potentially due to the uniform approach employed in controlled group trials.
Considered together, previous reviews provide mixed evidence of the efficacy of electronic AT for supporting memory-related function in individuals with ABI. Notably, reviews to date have not evaluated whether the evidence of efficacy varies according to individuals' level of involvement in the encoding (input) and retrieval and execution (output) phases of memory aid use, which has key implications for their independence and support needs in daily life. Further, there has been little emphasis placed on user perspectives of AT in terms of usability or ease of use. Velikonja and associates 10 highlight the need for an individual's characteristics, preferences, and lifestyle to be taken into account when recommending and training use of memory strategies. Similarly, research on acceptance of technologies in brain injury rehabilitation 23,24 has demonstrated how user perspectives influence the likelihood of adoption in daily life. The importance of end-user input and evaluation of AT is increasingly recognized in the rehabilitation field to inform personalized technology solutions and increase uptake. 25
Given the rapid technological developments in the field and mixed findings of previous reviews, the main aim of this systematic review was to evaluate the efficacy of electronic AT used by individuals with TBI to support memory function in daily life. As a novel approach, we sought to determine whether the evidence of efficacy varies according to participants' level of independence in using the AT to support phases of memory. A secondary aim was to examine user perspectives on the utility of electronic AT and factors influencing uptake or use.
Methods
The protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42021290916). The methods and reporting were guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines (PRISMA). 26
Search strategy
Potentially eligible articles were identified through title and abstract searches of the following six databases: MEDLINE, Excerpta Medica database (Embase), PsychINFO, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Scopus, and Cochrane Library. In line with the PICO framework, 27 three sets of search terms were used in each database, which related to the population (e.g., TBI, brain injury, head injury, head trauma), intervention (e.g., AT, technology, memory aid, digital, smartphone), and outcome (e.g., memory, remind, remember, cognition; see Supplementary Table S1). Comparator terms (e.g., usual care, wait-list) were not used in the search because designs relevant to this review included those without a control or comparator condition, for example, pre-post group studies.
Searches were restricted to articles on human subjects, written in or translated into English, published in peer-reviewed journals, and with full-text available. Databases were initially searched from their inception to November 26, 2021, with an updated search performed on June 13, 2022. In addition, backward and forward citation searches were conducted on all eligible articles.
Study selection
The screening of articles was facilitated by the web-based software platform Covidence.
28
Following initial screening of articles based on title and abstract, two authors (JM and TO) independently assessed the eligibility of peer-reviewed full-text articles according to the following criteria: The sample was comprised of adults (minimum age 18 years) with TBI. In samples with mixed causes of brain injury, at least 50% of participants had a TBI diagnosis. Where etiology was not specified, authors were contacted for further information (note: attempts were made to contact authors of four articles; one responded). The study evaluated the efficacy of AT used by individuals (with or without support during the input or encoding phase) to support memory-related functioning in daily life. That is, participants were expected to be independent in using the AT for at least one distinct memory phase, such as programming reminders and/or retrieving and executing tasks or memory-related actions. This included AT designed to support retrospective and/or prospective remembering, including keeping a diary and scheduling timely reminders and alerts to support goal-relevant actions (e.g., daily medication, appointments). Outcomes were assessed related to participants' self-reported memory function or performance relevant to memory functioning (e.g., target memory behaviors, task completion, goal recall or attainment, rate of forgetting, frequency of memory reminder set or usage of the AT, number of reminders/prompts needed, activities of daily living [ADLs], independence) based on pre- versus post-intervention comparisons or post-intervention changes relative to a control/alternative treatment condition. The study design was an RCT, quasi-RCT, comparative non-randomized intervention with concurrent controls, single-arm (e.g., within-subjects, pre-post design) with a minimum of 10 participants, or single-case methodology with sufficient baseline phase (3 or more data points) prior to the treatment phase. Group studies (
Studies were excluded if individuals with TBI were not responsible for using the AT for memory-related tasks themselves (e.g., technology was solely under clinician or caregiver control for both entering reminders and retrieving information) or if the technology was used by clinicians to deliver therapy. 29 Similarly, studies focused on evaluating different approaches to training, 30 rather than the efficacy of AT for supporting memory-related functioning, were excluded. Studies evaluating the efficacy of micro-prompting technology 31 to support step-by-step completion of specific tasks were not eligible. Studies were also ineligible if they outlined the conceptual development or design of AT without data to support efficacy. Further exclusion criteria included case studies without sufficient data (e.g., <3 baseline data points), group studies not reporting the statistical significance of pre-post changes or between-group differences, and studies reporting on outcomes not relevant to memory functioning. Conference abstracts, commentaries, letters, editorials, review articles, qualitative studies, study protocols, and non-peer-reviewed material were also excluded from the review. Any disagreements regarding eligibility of articles were resolved through discussion with a third author (CS) to reach consensus.
Data from eligible studies were extracted by one author (JM) and checked with another author (TO). Data extracted included: author(s) and year of publication, sample characteristics, study design, AT features and functions, the AT intervention (e.g., duration/frequency/intensity) and support with use of devices, outcome measures, statistical analytic approaches, and findings related to the review questions.
Quality assessment
Studies were initially classified according to the class levels used in reviews of evidence-based cognitive rehabilitation. 12 Class I studies were well designed, prospective, RCTs. Within this category, Class Ia studies consisted of prospective designs with quasi-randomized assignment to treatment conditions (e.g., allocation to alternating conditions or crossover designs). Class II studies included prospective, non-randomized cohort studies; retrospective, non-randomized case-control studies; or clinical series with well-designed controls such as multiple-baseline or alternating treatments SCED, as defined by Tate and Perdices. 32 Class III studies referred to clinical series without concurrent controls (single-arm, pre-post studies), or single-case methodology without multiple baselines or experimental control (i.e., AB designs).
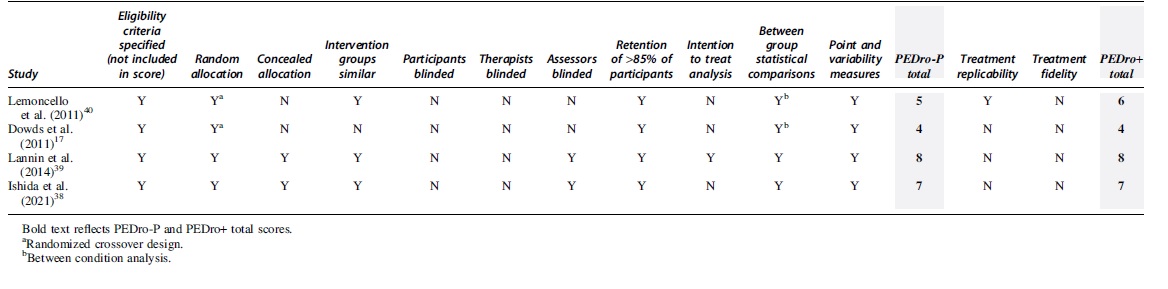
Class I studies were further appraised by two authors (JM and TO) using the PEDro-P
22
and PEDro+
33
scale. According to authors of the PEDro scale, scores of 6–8 constitute “good” methodological quality, whereas scores of 9–10 constitute “excellent” quality. In line with a review of digital health by Avramovic and co-workers,
34
we included the two additional items developed by Cherney and colleagues
33
to assess treatment replicability and treatment fidelity (PEDro+). The 11-item PEDro scale assesses: eligibility criteria (not included in score), random allocation, allocation concealment, similarity of intervention groups, blinding (of subject, therapists, and assessor), retention of
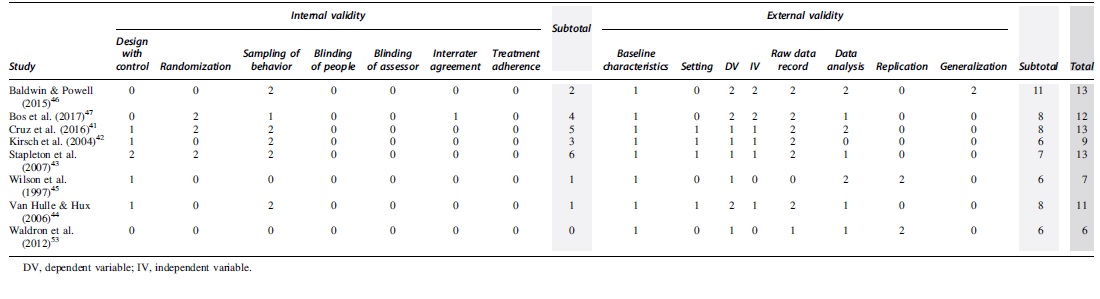
Class II and III single-case studies were further appraised using the 15 items of the risk of bias in N-of-1 Trials (ROBiN-T) Scale. 32,35 Seven items relating to internal validity include: design with control, randomization, sampling of behavior, blinding of patient/therapist, blinding of assessors, interrater reliability, and treatment adherence. The eight external validity and interpretation items include: baseline characteristics, setting, dependent variable, independent variable, raw data record, data analysis, replication, and generalization. As per guidelines by Tate and Perdices 32 and by Tate and colleagues, 35 a 3-point scale (0, 1, 2) was used to rate each item. Any disagreements were resolved through discussion to reach consensus.
Results
Study characteristics
The initial search yielded 4801 articles, which reduced to 2774 once duplicates were removed. A further 2721 articles were excluded by the title and abstract, leaving 53 articles to be screened as full texts. There was 94% agreement between two authors concerning the inclusion or exclusion of the 53 studies. Initial disagreement regarding eligibility of three studies was resolved through discussion with a third author. This process identified 19 articles eligible for review (see Fig. 1). The list of 34 excluded articles and reasons for exclusion are summarized in Supplementary Table S2. Citation searching resulted in a review of 7 further articles screened as full texts, none of which were eligible. Two articles by Wright and associates 36,37 represent an original study and subsequent replication study of the same AT intervention with different samples. A summary of the study samples, designs, AT, interventions, primary outcomes, and key findings is presented in Table 1.
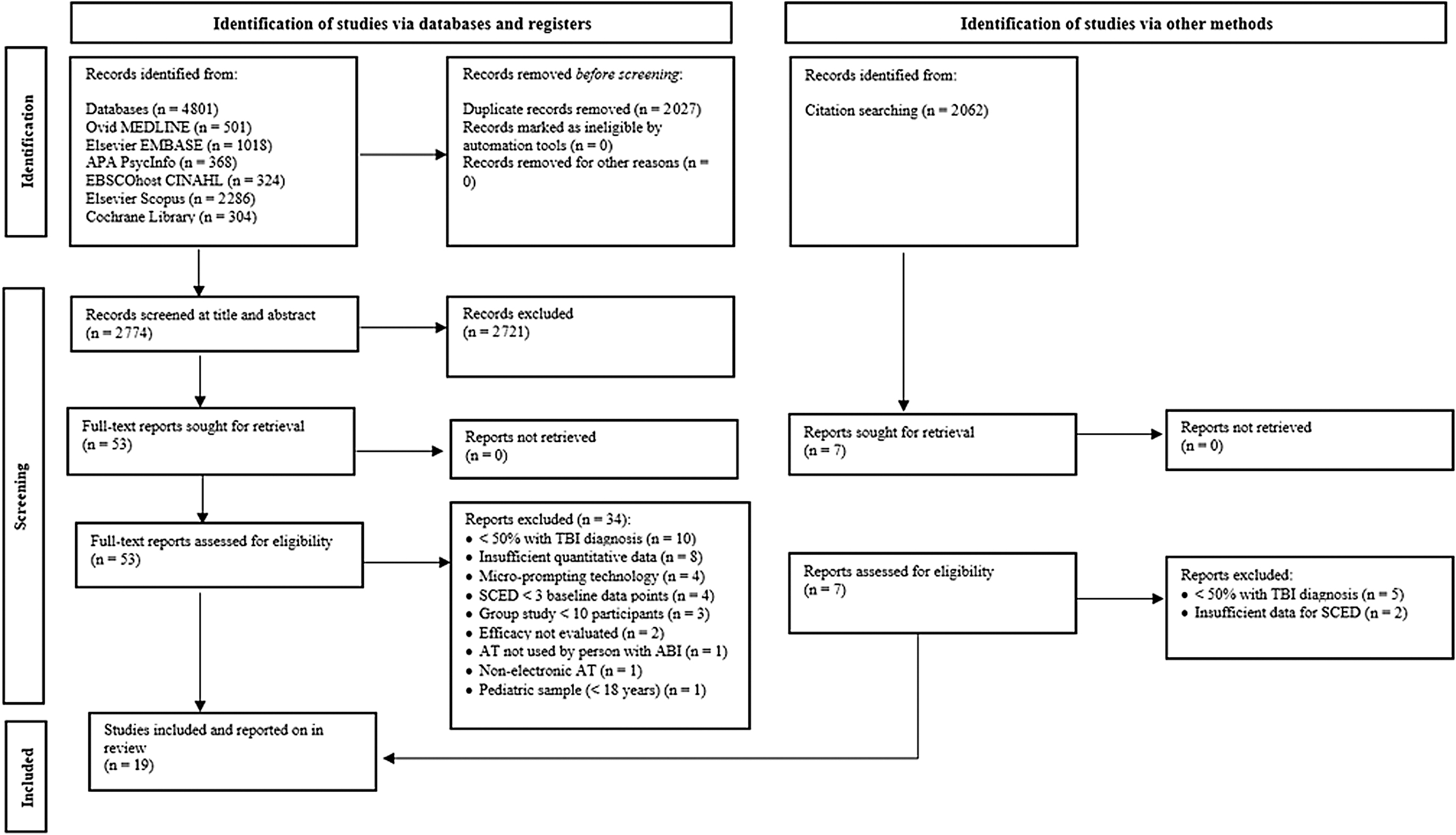
PRISMA flow diagram 26 and search outcomes. AT, assistive technology; SCED, single-case experimental design; TBI, traumatic brain injury.
Summary of Study Sample, Design, AT Devices and Applications, Intervention Characteristics, Outcomes, and Key Findings
Effect sizes calculated according to guidelines by Morris and DeShon. 66
Effect size could not be calculated based on data reported. 66
ABA, acquired brain injury; AT, assistive technology; CHART–Revised, Craig Handicap Assessment and Rating Technique–Revised; d, Cohen's d (0.20 = small, 0.50 = medium, 0.80 = large); COPM, Canadian Occupational Performance Measure; EMC, Everyday Memory Checklist; Google Calendar, free online calendar that synchronises with the user's mobile phone and sends notifications about events; h, hour; M, mean; NAP, nonoverlap of all pairs; ns = not significant; PDA, personal digital assistant; PMQ, Prospective Memory Questionnaire; RCT, randomized controlled trial; SCED, single-case experimental design; SD, standard deviation; TBI, traumatic brain injury; TSI, time since injury; yrs, years.
Quality of methodology
There were 2 Class I studies,
38,39
2 Class Ia studies,
17,40
5 Class II studies
41
–45
and 10 Class III studies
36,37,46
–53
(see Table 1). In the quality appraisal of the 4 Class I studies (see Table 2), there was substantial interrater agreement concerning PEDro-P and PEDro+ scores (κ = 0.88, p < 0.001), with disagreement resolved through discussion to yield final ratings. PEDro-P and PEDro+ scores ranged from 4 to 8. The comparator conditions for the Class I studies involved wait-list control,
38
usual care or practice,
39,40
and paper-based aids.
17
In an RCT with multiple crossover design by Dowds and colleagues,
17
four intervention conditions were evaluated, including usual approach or memory aids (baselines week 1 and 5), and three active conditions of a paper-based organizer and two types of personal digital assistant (PDA) in randomized order between baselines. All four studies reported eligibility criteria, random allocation,
In the quality appraisal of the eight single-case studies (see Table 3), interrater agreement was also high (κ = 0.85, p < 0.001), with disagreement resolved through discussion to yield final ratings. The mean ROBiN-T rating for internal validity was 2.75/14 (range: 0–6) and mean external validity rating was 7.5/16 (range: 6–11). The total mean rating was 10.5/30 (range: 6–13). Most single-case studies (
Sample characteristics
A total of 311 participants with brain injury were involved across 19 studies (M = 16, range: 1–78). Four studies included only individuals with severe TBI,
42,44,46,50
whereas four involved participants with moderate to severe TBI
47,51
or mild to severe TBI.
41,43
Injury severity was not specified for the TBI-only sample employed by Dowds and colleagues.
17
The remaining studies included participants with mixed ABI etiology (
Studies typically measured severity of memory impairment using objective indices (e.g., Rivermead Behavioral Memory Test), although this was not always an eligibility criterion for participation, with some studies including participants who performed in the normal range on memory testing. 41,52 The Class I studies by Ishida and associates 38 and Lannin and co-workers 39 only included participants who demonstrated impairment on objective memory tests, whereas other studies recruited participants with subjective memory complaints or those demonstrating functional difficulties.
Types of AT
Most studies (74%) used commercially available devices and software that were not designed specifically for people with brain injury. Devices included PDA, pocket computer and alarm, tablet, pager, smartphone, wristwatch, voice recorder or voice organizer, and television. Participants' own mobile phone was used in three studies. 41,46,48 Software included alarm, calendar, agenda, notebook, and to-do-list applications, some of which were linked to text or SMS functions. Two purpose-designed systems included NeuroPage, a portable alphanumeric pager, 45 and television-assisted prompting, a set-top device and computer connected to participants' home televisions. 40 Scheduling and reminding software were purpose-designed for a pocket computer, 36,37 tablet, 38 and pager. 42
Focus of AT interventions
Table 4 summarizes participants' involvement or independence in using the AT and evidence of efficacy of each intervention. Two studies by Wright and associates 36,37 focused on use of the AT (pocket computer) for the encoding phase only, with participants taught to make new entries and edit entries as needed. Nine studies involved the researchers externally programming reminders into the AT device, with the interventions focused on participants' use of devices to retrieve intentions and execute memory tasks. 40,42 –46,48,51,52 In three studies, 17,41,47 participants were cued and supervised to enter task reminders into the AT, with the evaluation focusing on their ability to retrieve and execute tasks. Five studies evaluated participants' more independent use of AT to support encoding, retrieval, and execution phases, 38,39,49,50,53 although none of these five studies verified that reminders were entered in the AT device.
Summary of AT Intervention Studies According to Participants' Independence or Phase of Memory Supported, Memory-Related Outcomes Assessed, and Evidence of Efficacy
Objective refers to behavioral outcomes verified by researchers as opposed to self-reports from participants, or memory functioning rated by family caregivers or staff.
AT, assistive technology; PDA, personal digital assistant; TAP, television-assisted prompting.
Memory-related outcomes
Most studies (63%) evaluated the efficacy of the AT intervention using at least one objective behavioral outcome that could be verified by researchers. As summarized in Table 4, these outcomes included frequency of use of the AT or entries made, 36,37 tested recall of information from reminders, 48,51 entries made in a daily planner, 42 and completion of experimental tasks devised by researchers (e.g., posting a postcard, sending an e-mail or text message, calling a voice mail). 17,40,47,49,52 Ishida and associates 38 used standardized tests of memory functioning as a secondary outcome. In addition to experimental tasks, Dowds and colleagues 17 devised personalized tasks in which participants were required to contact researchers to report on task completion, although task completion was not verified. Caregiver or residential care staff reports of task completion were used in several studies, 38,39,41,44,45,46 whereas self-reports of improvement in functioning was the sole approach used by Gentry and associates. 50 Lannin and co-workers 39 used Goal Attainment Scaling to assess achievement of personal memory goals.
User perspectives on the utility of AT devices
Nine studies (47%) assessed user perceptions of feasibility, acceptability, and/or utility of the AT and features. 36 –38,40,41,46,48,51,52 This included obtaining quantitative ratings of “user friendliness,” 52 ease of use, usefulness, frequency of use, and preference for keeping different styles of AT or likelihood of continuing to use or purchasing in the future. 36 –38,40,51,52 Lemoncello and colleagues 40 additionally asked participants questions (Yes/No) regarding whether or not they found the AT helpful for completing tasks, if it impacted their daily function, and if they would continue to use or recommend it to others. Some studies interviewed participants to obtain feedback regarding their satisfaction and experiences of use with the AT (e.g., problems encountered) and suggested modifications. 40,41,48,51 Dowds and colleagues 17 recorded which PDA device participants chose to retain at the end of the study, but without exploring reasons for the choice. Lannin and co-workers 39 recorded whether caregiver support was needed for participants to learn or remember to use the AT and reported the proportion of participants still using the device at 8-week follow-up; however, user perceptions were not obtained.
AT interventions for encoding of memory intentions
Two Class III studies by Wright and associates 36,37 evaluated individuals' ability (n = 12) to independently use a pocket computer with a purpose-designed interface for diary, alarm, notebook, and to-do list functions. Two different styles of pocket computers were examined, one with and one without a physical keyboard, with training for each provided prior to use. Participants were given each computer for 2 months (in counter-balanced order) with a 1-month break between use. The key outcomes were use of pocket computer functions and reminders set, as indicated by a computer file log, and perceived ease of use and usefulness. In the first study, 36 all participants demonstrated successful use of both computers and 83% rated these as useful. The diary function was rated as significantly more useful than the notebook function. There were no differences in number of entries made, rating of usability, or preference for keeping each computer style. High-frequency users made a similar number of entries across each computer style, whereas low-frequency users made fewer entries in the one without the physical keyboard.
The second study 37 sought to replicate the first study in a different sample (n = 12) using the same AT and intervention procedures, but also added a to-do-list and game functions to the interface of both pocket computer styles. Consistent with the original study, all participants demonstrated successful use of the memory aid functions and most (83%) reported these as very useful. The diary function was rated as more useful than the notebook and to-do-list functions. There was no significant difference in frequency of use of the two different computer styles. Number of diary entries was significantly higher for individuals with greater prior use of memory aids.
AT interventions with pre-programmed reminders
One Class Ia, 40 four Class II, 42 –45 and four Class III studies 46,48,51,52 evaluated participants' ability to carry out memory-related tasks that had been pre-programed by a researcher, clinician, or family member.
Using a randomized crossover design (Class Ia), Lemoncello and colleagues 40 evaluated utility of Television Assisted Prompting (TAP) in 23 participants with ABI. Participants were randomly allocated to the TAP or “typical practice” conditions, with the latter entailing individuals' use of their usual memory strategies. Participants experienced two 2-week periods of both the TAP and typical practice conditions over an 8-week intervention period. TAP provided audiovisual reminders on the person's home television at scheduled times. The system was devised to allow prompts to be entered from any computer, with the television turning on automatically to deliver prompts at pre-scheduled times. Reminders remained on the screen for up to 1 h (with audio prompts) until the user confirms task completion or elects to refuse or postpone the task (using buttons on the device). Researchers entered the prompts based on individual preferences for the content and timing of delivery. Outcomes included task completion on preferred and non-preferred tasks selected by participants, with completion recorded using a home log, and two experimental tasks devised by researchers to enable objective verification.
Overall, the TAP condition was associated with significantly higher task completion (72%) as compared with the control condition (43%). All participants perceived that TAP helped them to complete tasks, whereas 72% indicated they would continue to use a system like TAP. Strengths of the study included participant retention (92%), use of an objective index of task completion, and treatment replicability. Weaknesses included lack of allocation concealment, blinding, intention-to-treat analysis, and treatment fidelity (PEDro-P = 5; PEDro+ = 6).
A Class II study by Stapleton and co-workers 43 employed an ABAB multiple baseline-across-participants design to investigate use of reminder functions on mobile phones for five individuals with TBI. Individuals were randomly allocated to baseline length (2, 3, or 4 weeks of daily tallies) followed by a 7-week intervention, 2-week baseline, and 2-week second intervention phase. Participants and/or caregivers recorded daily completion of target behaviors. For the intervention periods, participants were trained to use new mobile phones that were programmed by researchers to deliver timely reminders relevant to individuals' memory goals. The analysis indicated a significant increase in target behaviors between the baseline and intervention phases for Participants 1 (51–95%) and 5 (58–88%), who also demonstrated learning of some routines in the second baseline. Target behaviors did not increase significantly for Participants 2, 3, and 4, who demonstrated more severe memory and executive impairment and required 24-h care. User perceptions were not assessed. Key strengths related to the design control, randomization, and behavior sampling. Weaknesses included lack of examination of interrater agreement, replication, and generalization (SCED: 13/30).
Kirsch and associates 42 employed an ABA single-case design (Class II) to evaluate the efficacy of an “in-house” alphanumeric paging system for a male with severe TBI. The paging system was designed to cue him to use a daily planner to record information related to speech therapy sessions for evening discussions with a family member. During the baseline (32 days) he received reminders from his therapist at the start of the session to record information in his daily planner at the end of the session. During the 24-day intervention the therapist additionally scheduled prompts from the pager to occur 5 min prior to the end of session to remind the participant to write in his daily planner. Overall, daily planner entries increased from 22% to 94% during the intervention period and decreased to 49% when the pager was withdrawn. User perceptions were not assessed. In addition to lack of examination of interrater agreement, replication, and generalization, there was considerable within-phase variability that was not examined or controlled for using statistical methods (SCED: 9/30).
Wilson and colleagues 45 used an ABA group design (Class II) with 15 participants to evaluate the use of NeuroPage, a portable paging system. Target behaviors were selected in collaboration with participants and their caregivers. Memory failures were recorded by caregivers over a 2–6 week baseline that varied for each participant due to the nature of their memory problems and stability of baseline data. During the 12-week intervention period, the NeuroPage service programmed delivered timely reminders. In the 3-week post-treatment phase, the pager was withdrawn. An odds-ratio test accounting for varying success rates for each target behavior indicated that all participants significantly benefited from the pager. Task success increased on average from 37% during the baseline to 85% during treatment. Mean success in the post-treatment phase (74%) indicated some ongoing benefits in terms of learning routines. User perceptions of AT were not assessed. Key strengths included the systematic data analysis and replication, whereas weaknesses included lack of randomization, insufficient details of the intervention and approach to training, and lack of examination of interrater agreement (SCED: 9/30).
Using an ABACA design, a Class II study by Van Hulle and Hux 44 evaluated the utility of two types of AT, a wristwatch alarm with vibration function and a digital voice recorder and alarm system, for supporting three individuals with severe TBI to take medication. During each 2-week baseline (A) phase, participants received written reminders (medication schedules). The first treatment (B) phase entailed the use of one AT device along with written reminders. Data collection ceased when participants achieved 100% independence with medication across multiple days. Participant 1 improved from 56% to 75% success during baseline and treatment (wristwatch alarm) and improved to 100% in the second baseline with the watch withdrawn. Participant 2 did not achieve 100% success across any of the phases, including the two AT treatment phases, and continued to require verbal reminders from staff. A third participant achieved 100% success during his initial baseline period and therefore AT was not introduced. User perceptions were not assessed. Key strengths included the lengthy baseline with specified criterion for success, whereas the lack of randomization to order of AT, generalization, replication, and details of training were weaknesses (SCED: 11/30).
A Class III study by Hart and associates 51 evaluated the efficacy of a portable voice organizer for supporting individuals' (n = 10) recall of therapy goals and plans. Six goal statements were generated by clinicians, with three randomly selected to be recorded on a voice organizer. Goals included broad statements regarding reasons for treatment and more focused personal goals and were recorded by clinicians. Participants selected three times each day to listen to recorded goals, as prompted by an alarm. They wore the voice organizer attached to a belt or purse strap. Recall for therapy goals was tested under two conditions: free recall (no cues) and cued recall (key words for goals provided). Following the 1-week intervention, participants demonstrated significantly better recall of recorded goals than unrecorded goals in both free recall and cued recall conditions. Compliance to listening to the recording was generally high, and 6 out of 10 participants perceived improvement in their memory for therapy goals. Nevertheless, two participants expressed frustration regarding the alarm or functions to play the recorded message.
Following similar procedures to and associates, 51 the Class III study by Culley and Evans 48 tested the efficacy of SMS text messaging for improving recall of rehabilitation goals. Eleven participants were sent SMS texts on their personal mobile phones that related to three randomly selected personal rehabilitation goals out of six, three times each day for 14 days. There were no differences in free or cued recall (cue words given for goal) for these goals at baseline. However, at 7 and 14 days both free recall and cued recall was significantly higher for the goals participants received text messages for as compared with the goals without reminders. The magnitude of difference was greater from baseline to 7 days than from 7 days to 14 days, suggesting that the text messages had the greatest benefit for learning goals in the first 7 days. All participants provided positive feedback regarding the benefits of receiving text messages for supporting their memory, including improved alertness, motivation, and ability to remember and carry out goals.
Baldwin and Powell 46 employed an AB design (Class III) to evaluate the efficacy of using Google Calendar on a personal mobile phone for improving task completion. A man with severe TBI and his wife selected the type and timing of prompts (five spaced alerts per event), whereas the researcher entered the events externally. The man's wife kept a log of task completion for three target behaviors and three control behaviors for the 6-week baseline (Weeks 1–6) and 6-week intervention (Weeks 8–13). Week 7 was a training week in which the man was taught to respond to task alerts. Using non-overlap of all pairs, the analysis showed a 90% reduction in forgetting for target memory behaviors, whereas no change was evident for two of the three control behaviors. A comparison of pre- and post-intervention ratings on self-report measures indicated improvements in the man's subjective memory and an increase in personal control and treatment control beliefs, whereas inappropriate beliefs and threat appraisals about use of memory aids decreased. Key strengths of the study included the 6-week baseline, in-depth sampling of behavior, and assessing generalization. Weaknesses related to the AB design, randomization, replication, or examination of interrater agreement or treatment adherence (SCED = 13/30).
A Class III study by Thöne-Otto and Walther 52 examined the utility of two memory aids, a palm organizer and a mobile phone with agenda function. They employed an ABAC design with group-level data (n = 12). During each 2-week phase, participants were required to perform 20 experimental memory tasks. The order of memory aids was counterbalanced, and participants received 5 h of training per device. Based on progress during training, six participants were classified as slow learners and six as fast learners. Overall, improvement in memory performance was not significant for either device. Only fast learners spontaneously used the devices and were more likely to report the desire to continue using the device, particularly the palm organizer. Various disadvantages related to the number of menu steps, interface (key and touch panel size), and alarm were reported.
AT interventions with cued encoding and independent retrieval and execution
A Class Ia study 17 and two single-case studies (Class II, 41 Class III 47 ) evaluated AT interventions in which participants were cued and supervised to enter reminders into a device. Dowds and colleagues 17 examined the efficacy of automated reminders from two PDA-type devices in 36 people with TBI with self-reported memory problems. The palmtop-sized computers were a Palm device and a Microsoft device. A randomized multiple crossover design was employed over an 8-week period with four conditions: baseline, pen and paper memory, aid and two PDAs. Memory aid condition changed each week in a randomized order, with training occurring just prior to use. Participants were supported to enter reminders into each memory aid when receiving their weekly assignments. The main outcome was timely task completion based on researcher-assigned tasks (daily calls to an answering machine or office) and time-related personalized tasks selected in collaboration with participants. Use of either PDA was associated with significantly higher task completion rates as compared with baseline (27%) and paper memory aids (26%). The Palm PDA was associated with significantly higher completion rates (56%) than the Microsoft PDA (38%), which authors attributed in part to the louder alarm for the Palm device. Most participants (75%) chose to retain the Palm PDA after the study, although user perceptions were not assessed. Strengths included high retention (92%) and use of an objective index of task completion. Weaknesses included lack of allocation concealment, blinding, intention-to-treat analysis, treatment fidelity, and replicability (PEDro-P = 4; PEDro+ = 4).
A Class II study by Cruz and colleagues 41 evaluated the efficacy of Google Calendar with text messages on personal mobile phones for improving prospective memory in two participants with a mild or severe TBI. Using a multiple baseline across target behaviors design, the onset of reminders for each activity was randomly assigned (minimum baseline of 5 data points). Reminders were entered by participants during rehabilitation sessions with therapist support. The main outcome was activity completion as recorded by the participant or caregiver. Non-overlap of all pairs analysis for Participant 1 indicated significant improvement for one out of three tasks, along with generalization to a new activity. Participant 2 demonstrated significantly improved performance on one out of two tasks. User feedback indicated that the content of reminders and nature of the activity influenced effectiveness of the prompts, and that additional strategies were often required. Key strengths related to the randomization of reminder onset, length of baseline, and data analysis. Weaknesses included lack of examination of interrater agreement, replication, and generalization (SCED: 13/30).
Bos and associates 47 evaluated the use of a smartphone relative to baseline and memory notebook conditions (AB1B2; n = 2) or relative to baseline only (AB; n = 5). Participants were randomly allocated to a baseline length of 3–7 weeks. Training for each memory aid was provided prior to the 8-week intervention period. Researchers cued participants to enter reminders for memory tasks during weekly appointments. Tasks entailed sending text messages with specified content and posting a postcard. For individuals receiving both memory aids, task performance improved between baseline and notebook use, but additionally improved during the smartphone condition for two out of three memory tasks. For individuals receiving the smartphone after baseline, results were mixed. Three participants showed clear improvement in task performance on two or three of the tasks, one participant showed better performance on the texting task and a decline on the postcard task, and one participant showed a decline in performance across all tasks when using the smartphone relative to baseline. The mixed findings were attributed to participants' variable motivation and attitude toward using smartphones, severity of memory impairment, and lack of personalization of memory tasks. However, user perceptions were not assessed. Strengths included randomization of baseline length, in-depth data record, and objective indices of task performance, whereas weaknesses included lack of experimental control, replication, and generalization (SCED: 12/30).
Interventions promoting independent use of AT to support memory
Two Class I studies 38,39 and three Class III studies 49,50,53 examined the efficacy of AT used independently by participants to enter information (encoding), retrieve, and execute tasks.
Lannin and co-workers 39 conducted an RCT to evaluate the efficacy of a PDA for achieving memory and organization goals relative to standard occupational therapy without electronic memory aids. Forty-two individuals with ABI who demonstrated objective memory deficits were recruited. Individuals allocated to the PDA condition chose between a Windows or Macintosh device, both of which had alarm, calendar, address book, and camera features. Training and support to use the PDA was conducted during occupational therapy sessions over 8 weeks (mean therapy = 7 h; range = 6–21 h) and entailed five modules focused on: choosing personally meaningful activities to increase independence with caregiver input, self-awareness training, training in basic skills to use the PDA, learning to use the PDA to schedule and act on reminders, and generalization of strategy use outside of therapy. Individuals in the PDA condition demonstrated significantly greater achievement of memory goals and reduction in caregiver reports of forgetting. There were no significant differences in participants' subjective memory functioning. Caregiver support to use or remember to use the PDA was required for 19%, and nearly one-third required further support from caregivers between therapy sessions.
At the 8-week follow-up assessment, 67% of those who received the intervention reported that they continued to use the PDA daily, whereas 14% had ceased using the PDA. User perceptions or reasons for discontinued use were not assessed. Strengths of the study included allocation concealment, blinded assessment, participant retention (100%), and intention-to-treat analysis (PEDro-P = 8; PEDro+ = 8). Limitations included the lack of evaluation of treatment fidelity and varying intensity of therapy hours involved in the intervention, which impacts treatment replicability.
A Class I study by Ishida and associates 38 used a wait-list control design to examine the efficacy of tablet computer software for improving memory function in 78 participants with ABI. The intervention entailed an initial 2-week training period during which therapists taught participants how to operate a 7-inch tablet PC, with practice to ensure they could use event scheduling, reminders, memo notes, and timer functions. The schedule function included a checklist to confirm actions were completed. Participants used the tablet independently over 3 months to manage their daily schedule, with additional support from therapists as needed. There were no significant effects of intervention for self -and caregiver-reported memory function (primary outcome), caregiver burden, or psychosocial functioning. However, the intervention was associated with better performance on an objective memory test (Rivermead Behavioral Memory Test) and improved general self-efficacy relative to the wait-list condition. Subjective reports indicated that the daily schedule with voice reminder and diary functions were most frequently used (35–41%); however, 78% reported the tablet was moderately difficult or difficult to use, mainly due to the size (portability) and managing message sounds. Strengths included allocation concealment, high retention (98%), and assessor blinding. Weaknesses included the lack of intention-to-treat analysis, analysis of treatment fidelity, and details to support treatment replicability (PEDro-P = 7; PEDro+ = 7).
A Class III study by Gentry and associates 50 evaluated the effectiveness of PDAs for improving occupational performance in 23 individuals with severe TBI. The training was conducted in each participant's home during three to six 90-min sessions. No information was provided regarding PDA selection or allocation. Participants were given a PDA to use independently over 8 weeks. Approximately one-third contacted researchers during the intervention for support to use the PDA. A comparison of pre- and post-intervention functioning indicated significant improvement in self-perceived occupational performance on personally relevant tasks (e.g., remembering appointments, time and task management, medication management) and self-rated cognitive independence, mobility, and occupations. User perceptions were not assessed. Key limitations of this study related to the sole reliance on self-reported functioning and lack of experimental control.
A Class III study by Evald 49 evaluated the effectiveness of a smartphone combined with Internet-based calendar for improving memory performance in 13 individuals with TBI. Participants received an initial individual session focused on phone and Internet set-up and synchronization followed by five group sessions in which they learned to use the AT to enter appointments, contacts, and memory assignments through smartphone applications. Self-reported memory function and daily achievement of target behaviors (daily memory log, e-mail reporting task) was assessed at pre-intervention, post-intervention, and 2-month follow-up assessment. Overall, there was no significant improvement in performance on the assigned memory tasks at post-intervention or follow-up; however, participants reported significantly fewer memory problems at both time-points relative to pre-intervention. Most participants (77%) continued to use the smartphone for memory compensation at 2-month follow-up, although user perceptions were not assessed.
A Class III study by Waldron and colleagues 53 evaluated the efficacy of an intervention for teaching five participants with ABI (60% TBI) to program a PDA to provide reminders to complete seven personally relevant memory tasks. All tasks could be objectively verified as completed. An AB quasi-experimental design with usual memory aids only (3-week baseline) and PDA strategy phases was employed. Participants were trained to use the PDA in three weekly 90-min group sessions. Individual and group level analysis indicated that rates of task completion significantly improved between baseline (M = 59%) and PDA strategy phases (M = 90%). User perceptions of the AT were not assessed. Strengths included replication of findings and objective indices of task performance, whereas weaknesses included lack of experimental control, randomization, interrater agreement, and generalization (SCED: 6/30).
Discussion
Technology is increasingly being used in TBI rehabilitation to deliver interventions, support individuals' adjustment to their functional impairments, and promote independence in the home and community.
2,34
This systematic review aimed to evaluate the efficacy of AT used by individuals with TBI to support memory-related functioning and determine whether evidence of efficacy varies according to the phases of memory supported. Overall, from a total of 19 studies, there was evidence from 12 studies (3 Class I; 2 Class II; and 7 Class III) to support the efficacy of AT for improving memory-related functioning. Although the quality of methodology was variable, 2 of the Class I studies were well-designed RCTs (PEDro+:
Ishida and associates 38 did not find intervention effects for self-reported memory functioning, although they reported significant effects on an objective memory test and for self-reported self-efficacy. Lemoncello and colleauges 40 reported significant improvement in task completion based on both a home log (self-reported) and experimental tasks (objective). Dowds and colleagues 17 also found improvement in task completion for both researcher-assigned (objective) and personalized tasks (self-reported).
However, the evidence of efficacy was found to vary according to the phase/s of memory function supported, with the evaluation of AT interventions focusing on: 1) encoding or entering memory reminders (n = 2); 2) pre-programmed AT to support retrieval and task execution phases (n = 9); 3) cuing person to enter reminders to support retrieval and execution (n = 3); and 4) independent use of AT across memory phases (n = 5). In relation to the secondary aim, the utility and uptake of AT was found to be impacted by various user-related factors and design features.
In terms of AT interventions for supporting encoding of memory intentions, Wright and associates 36,37 demonstrated that individuals were able to learn to use two different styles of pocket computers to enter and edit memory reminders. Use of these devices was sustained over 2 months, with the appointment diary and auditory alarm rated as most useful. Individuals who used aids to assist memory before their injury made more diary entries. These studies did not determine whether use of the pocket computers improved recall or successful task completion or assess the impact of cognitive impairment on ability to learn to use the devices. Nonetheless, the findings support individuals' ability to use AT for the intention formation and encoding phase (i.e., entering reminders), which is an integral part of memory aid use.
Nine studies evaluated the efficacy of AT interventions with pre-programmed reminders for supporting memory retrieval and task execution. Of these, six studies (one Class Ia, 40 two Class II, 42,45 and three Class III 46,48,51 ) supported the efficacy of these interventions, whereas three studies (two Class II 43,44 and one Class III 52 ) provided mixed or no support. The Class I study by Lemoncello and colleagues 40 supported the benefits of scheduled audiovisual reminders delivered via participants' home televisions. As a novel feature, the reminders remained on the television until participants confirmed task completion, thus reflecting the evaluation phase of memory. With caregiver support to program reminders, this AT system may have utility for supporting memory function in the home. Other smart home devices that show promise for providing timely reminders include smart speakers and voice assistants, 54 although pilot research indicates some barriers to using speech-based systems for clients with severe cognitive and linguistic impairments.
Five other studies highlighted the benefits of electronic AT with pre-programmed reminders for portable devices to support home and community functioning. These included a voice organizer, 51 SMS text messaging, 48 paging systems, 42,45 and PDAs. 46 Two of these studies targeted participants' episodic memory for therapy goals, 48,51 with thrice daily messages supporting participants to later recall their goals under both cued and free recall conditions. The AT in the other three studies cued participants to remember to record information on therapy 42 or perform memory tasks at a set time. 30,46 There was evidence from the study by Wilson and colleagues 45 that use of a pager over 12 weeks helped participants to learn task routines after the AT was withdrawn.
However, in three studies evaluating the use of AT with pre-programmed reminders there was mixed support or non-significant results. 43,44,52 Notably, in studies by Thöne-Otto and Walther 52 and Van Hulle and Hux 44 memory tasks were both selected and pre-programmed by researchers or caregivers. As noted by Ellis, 18 intention formation is a key part of the encoding phase whereby individuals' own memory goals inform selection of tasks to be remembered. In the Van Hulle and Hux 44 study, AT devices (wristwatch alarm and digital phone recorder) were used to improve medication compliance to reduce staff workload rather than reflecting individuals' own goals. Thöne-Otto and Walther 52 found that participants' perceptions of design features such as menu steps, touch panel interface, and alarm impacted their use of a PDA and mobile phone. The mixed support for the efficacy of AT in the study by Stapleton and co-workers 43 appeared to be related to the severity of participants' cognitive impairment. Although all five participants selected their own memory goals, the two participants who benefited from pre-programmed mobile phone reminders had mild to moderate memory impairment, whereas the three who did not benefit had severe memory and executive function impairments warranting 24-h care.
In line with the multi-process model of prospective memory, 55 prospective remembering relies on various cognitive processes mediated by the frontal and temporal lobes, such that even with an external prompt, successful execution still requires the individual to successfully attend to and process the cue, inhibit participation in the ongoing task, and flexibly shift their attention to execute the intention. 4 More severe cognitive impairment is also associated with apathy, 56 which may reduce individuals' capacity to act upon memory prompts even when these reflect personal goals.
Three studies evaluated the efficacy of AT interventions with cued or assisted encoding of reminders. In the Class Ia study by Dowds and colleagues, 17 participants were “assisted as much as needed” (p. 345) to enter reminders into the PDAs at the time they received their weekly assignments. The PDAs were effective for supporting individuals' retrieval and execution of both researcher-assigned and personalized tasks selected by participants. The PDA with a louder alarm was associated with higher task completion (56% vs. 38%) and was chosen by 75% participants to retain at the end of the study. The single-case studies by Cruz and colleagues 41 and Bos and associates 47 highlighted some potential barriers influencing effectiveness of AT. Cruz and colleagues 41 identified that the content of reminders entered in Google Calendar was often insufficient to cue required actions for task completion. Bos and associates 47 attributed their mixed findings to participants' variable motivation for completing researcher-assigned tasks, attitudes toward using a smartphone, and severity of cognitive impairment. Therefore, despite individuals receiving support to ensure the accuracy of encoding memory intentions, various barriers can impact their ability and motivation to retrieve and execute memory tasks.
The final study type evaluated the efficacy of AT interventions that taught participants to enter memory intentions and retrieve and execute tasks independently. The well-designed Class I study by Lannin and co-workers 39 and two Class III studies by Gentry and associates 50 and Waldron and colleagues 52 supported the efficacy of interventions involving PDAs to achieve memory-related tasks, whereas studies by Ishida and associates 38 and Evald 49 provided mixed support. In each study, participants received several training sessions to learn to schedule, retrieve, and act upon reminders.
Over an 8-week intervention, Lannin and co-workers 39 found that nearly one-third of participants required caregiver support to use PDAs in the home. Two months after the intervention, approximately two-thirds were continuing using the PDA daily, although level of ongoing caregiver support was not specified. Gentry and associates 50 similarly found that one-third of their sample with severe TBI contacted researchers for support to use the PDA after receiving 3–6 training sessions. The Class I study by Ishida and associates 38 provided mixed support for the efficacy of a tablet with customized software. Participants received training of varied intensity (several hours to several days) to learn device functions and then used the tablet independently over a 3-month interval. There were no significant differences in the primary outcome of self- and caregiver-rated everyday memory relative to wait-list controls, although participants' objective memory performance on a functional memory test and general self-efficacy improved to a greater extent than controls. However, most participants (78%) perceived the tablet as moderately difficult or difficult to use due to the large size (7-inch) and difficulty managing message sounds. Notably, none of these studies evaluated participants' success with the input phase of memory aid use. Hence, it is unclear if memory-related functioning did not improve because memory intentions were not successfully entered in the device, or if participants failed to respond to or act upon reminders.
In relation to the second aim of the review, various factors were found to influence user perceptions of the utility of the AT and uptake or frequency of use. Based on these findings, a framework was developed (see Fig. 2) to guide the personalization of AT and design features in practice. In this framework, general factors influencing uptake and effectiveness of AT include individuals' prior memory aid use, 37 attitude toward the AT device 46,47 and design features, 38,52 severity of cognitive impairment or learning capacity, 43,47,52 and availability of support to use the device in the community. 39 Baldwin 57 identified “lifestyle fit” as a key predictor of memory aid use, highlighting the need for AT to reflect individuals' values, lifestyle, and sense of self. This might partly account for the positive outcomes of Baldwin and Powell 46 and Culley and Evans 48 in which pre-programmed reminders were received through participants' own mobile phones.

Factors influencing the uptake and effectiveness of AT for supporting memory-related function. AT, assistive technology.
Phase-relevant factors refer to user and design features that may impact the success of the AT for supporting different phases of memory. The personal salience of the memory goal and individuals' involvement in specifying the timing and content of the reminder may influence use of the AT device regardless of whether they physically enter their own reminders. 44,46,52 Wright and associates 36,37 showed that individuals can learn to independently set reminders; however, some may need ongoing prompting to set these. Although not examined by studies in this review, research by Jamieson and colleagues 58 highlighted potential benefits of automated “push notifications” (e.g., “Do you need to set any reminders?”) to cue people to initiate task scheduling, reducing reliance on carers. For the retention phase, some AT device functions (e.g., calendars) enable individuals to preview and edit upcoming memory tasks, 36 –38 which may support monitoring functions of prospective memory. 55 This is not the case for pagers such as the NeuroPage 45 or other messaging systems. 48,51 Nonetheless, spaced alerts can be programmed for calendar and messaging systems, with the repetition of cues supporting individuals to learn the content of messages 48,51 and prepare for future task completion. 46
In terms of retrieval, the nature of alerts (e.g., volume of alarm) and content of reminder needs to be sufficient to cue relevant actions, 17,41 yet not cause frustration or embarrassment. 46,51 Once retrieval cues are detected, the ability to execute the memory task is reliant upon goal-directed behavior and executive skills such as inhibition, switching, and initiation. Poor initiation or apathy may pose a barrier to ongoing task completion despite individuals' initial motivation. 43 Studies in this review did not examine the effects of co-administration of pharmacological agents (e.g., antidepressants or stimulants) on intervention outcomes. Given the potential effects of these agents on initiation or apathy, this warrants further research. Finally, the evaluation phase refers to confirmation of task completion through a specific action. NeuroPage was designed to include a “closing the loop” function, whereby users call a number when they have carried out actions to cancel ongoing reminders. 59 This requirement may be impractical for all scheduled reminders and hence automated prompting for individuals to confirm whether actions were completed, postponed, or cancelled may be a useful feature 40 combined with environmental strategies (e.g., checking medication dispensers).
Limitations
Several limitations of this review need to be considered when interpreting the evidence of efficacy of electronic AT interventions and factors influencing uptake. First, the findings are largely based on Class II or Class III studies, which, according to guidelines on evidence-based cognitive rehabilitation, 12 indicate “possible effectiveness.” Of the four Class I studies, none examined treatment fidelity and only two 38,39 employed blinding of assessors. Although it is challenging to blind participants and therapists in behavioral interventions, in trials involving comparison of two or more active interventions, the hypotheses regarding intervention efficacy could be concealed from participants and therapists to minimize potential bias. Notably, only one RCT in the present review used an active control condition, which involved a paper-based organizer. 17 Nonetheless, there was evidence for the effectiveness of AT interventions for supporting memory-related function as a practice standard, based on at least one well-designed Class I study 39 with additional support from two Class Ia, 17,40 two Class II, 44,45 and seven Class III 36,48 –53 studies.
Second, evidence in this review was combined for a wide range of technologies. Although the focus was on the phase of memory supported, it is important to acknowledge that individuals' experience and use of AT most likely varied for different devices. For example, in several studies participants used their own smartphone, 41,46,48 television, 40 or computer, 50 which are likely to have been used for other various purposes. In other studies, devices were supplied for the purpose of the study and were only used for reminding. Hence, participants' prior use of and familiarity with the device may have impacted the effectiveness of the intervention. Many studies attempted to address the lack of familiarity through training 17,38,39, 41,43,46,47,49 –53 or supporting the use of AT throughout the trials, 39,50 but their effect on outcomes is unclear. The influence of familiarity and prior use of AT devices and features on intervention outcomes requires further research.
Third, there was considerable variability in the memory-related outcomes assessed across the studies (see Table 4). Seven studies employed self-report or caregiver-reported outcomes that were not verified by researchers. More subjective indices may be more prone to bias, which is not addressed by the PEDro-P 22 or PEDro+ 33 scales and is accounted for by one item on the RoBiNT scale. 32,35 In the measurement of memory-related functioning, it can be challenging to employ ecological tasks that are meaningful to participants while minimizing potential bias. Reliance on participants with memory impairment to record their own task success or memory failures has questionable reliability and such actions during the baseline period could inadvertently support memory and reduce the chances of detecting an intervention effect. Some studies aimed to personalize performance-based tasks according to the nature of participants' typical memory failures or memory goals. 48,51,53 For example, Waldron and colleagues 53 asked individuals with TBI and family members to describe typical memory failures experienced and devised seven related ecological tasks for which outcomes could be objectively verified.
Fourth, long-term follow-up and investigation of factors influencing ongoing use of AT beyond the intervention was a major gap in the studies reviewed. In the studies that provided novel technology to participants, the device was typically withdrawn at the end of the intervention. As an exception, two studies, by Lannin and co-workers 39 and Dowds and colleagues, 17 gave participants a PDA to keep at the end of the study; however, only Lannin and co-workers examined continued use at 8-week follow-up, based on self-report. In the three studies in which participants used their own smartphones, 41,46,48 none examined long-term maintenance or ongoing use of the AT functions taught during the intervention.
Finally, due to the primary focus on evidence of efficacy, user perspectives of utility reflect only those gained following the AT intervention, rather than during earlier design or piloting phases. As noted by Aldrich, 60 it is optimal to request feedback from potential users at frequent intervals rather than solely at the end of a trial period of use. Aldrich further highlighted likely benefits of direct observation of individuals engaging with the AT to gauge their reactions and immediate feedback, rather than relying on individuals' recall of experiences in a later interview. For example, Wallace and colleagues 61 reported user-centered development of an external memory aid (EyeRemember), in which ongoing feedback was sought from people with brain injury, their caregivers, and clinicians through focus groups, sit-by demonstrations, and prototype testing.
Future research directions
In future research, it is recommended that well-designed clinical trials focus on comparing the efficacy of AT interventions providing varied levels of support with encoding (e.g., self-initiated, cued, and pre-programmed reminders) and factors moderating outcomes (e.g., severity of cognitive impairment, caregiver support). For studies evaluating individuals' independent use of AT, it is optimal to verify device use (i.e., reminders entered) and task completion using objective indices. Further research is also needed to support the preliminary framework (Fig. 2) of general and phase-specific factors influencing utility and uptake of AT for memory in practice. Notably, recent experimental research by Jamieson and colleagues 62 compared the effect of narrow-deep (i.e., more screens with less information displayed per screen) and broad-shallow (i.e., fewer screens but more information displayed per screen) user interfaces when teaching people with ABI to use a custom designed reminding application (ApplTree 58 ). Participants made more errors and omitted more information when using the broad-shallow interface as compared with the narrow-deep one. However, preferences for user interface varied and influenced perceptions of ease of use.
Understanding user preferences for the type of AT device and design features is integral to patient-centered care and is best facilitated through co-design with intended technology users. 61,63 Research also shows that the approach used to train individuals to use AT for memory can influence learning outcomes, although there are mixed findings concerning the relative efficacy of systematic instruction, errorless learning, and trial-and-error learning. 30,64 Outcomes of training may vary according to participants' preferred learning style and severity of cognitive impairment. 65 Evaluating the efficacy of training approaches and the influence of user characteristics remains an important focus for future research. Given the lack of studies evaluating long-term use of AT, there is also a need for research to investigate long-term uptake or sustained use of AT following interventions and factors influencing long-term use.
Conclusions
Overall, this review identified that 12 of the 19 studies supported the efficacy of AT interventions for improving memory-related functioning in individuals with TBI. There was the most empirical support for the efficacy of AT for facilitating retrieval and execution phases of memory (i.e., supported by 6/9 studies) with pre-programmed reminders. However, further controlled studies are needed to evaluate the efficacy of AT according to level of support provided for different phases of memory, and to examine the moderating effects of user characteristics. Such research will have important clinical implications for enhancing uptake of AT to improve individuals' independence and quality of life after TBI.
Footnotes
Transparency,Rigor,and Reproducibility Summary
The protocol for this systematic review was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42021290916). The methods and reporting were guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines (PRISMA). The screening of articles was facilitated by the web-based software platform Covidence. Six databases, namely, MEDLINE, Excerpta Medica database (Embase), PsychINFO, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Scopus, and Cochrane Library, were initially searched from their inception to November 26, 2021, with an updated search performed on June 13, 2022. Following initial screening of articles based on title and abstract by a single author (JM), two authors (JM and TO) independently assessed the eligibility of peer-reviewed full-text articles. Data on the 19 included articles has been comprehensively reported in the manuscript. Articles excluded at the full-text review stage and reasons for exclusion are summarized in Supplementary Table S2. For other details concerning the search process and outcomes, please contact the lead author.
Acknowledgments
The authors gratefully acknowledge the support of the Motor Accident Insurance Commission and Advance Queensland Industry Research Fellowship.
Funding Information
Funding was provided by the Motor Accident Insurance Commission, and by an Advance Queensland Industry Research Fellowship awarded to Dr. Shirota.
Author Disclosure Statement
No conflicting financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.