
Abstract
Mild traumatic brain injury (mTBI) affects 42 to 56 million individuals worldwide annually. Even more individuals are affected by sub-concussive repetitive head impacts (SRHIs). Such injuries may result in significant acute and chronic symptoms. A study of how individuals may adjust or augment their nutritional and dietary habits to prevent cumulative neurotrauma and promote post-injury recovery is necessary. The objective of the current study is to systematically review nutritional and dietary interventions for neurotrauma prevention and mTBI recovery to direct clinical decision-making and identify future areas of research. This systematic review, without a specified time-period, was performed in PubMed, Scopus, Cochrane, CINAHL, and Web of Science followed by a manual search of references. Search strings were generated by a research librarian. Studies were included if they: 1) investigate human subjects with mTBI or SRHI; 2) investigate a supplement/ingredient of dietary supplement sold in the U.S. or dietary intervention without classification as a drug or prohibitive statement against use by the U.S. Food and Drug Administration (FDA); 3) assess a quantifiable outcome; and 4) are published in English in a peer-reviewed journal with an accessible full-length article. Studies were excluded if: 1) the study included non-mTBI or SRHI subjects (e.g., moderate/severe TBI, stroke); 2) mTBI is not assessed separately from moderate/severe mTBI; or 3) the studies that required intracranial hemorrhage. Fifteen studies from 12 unique subject populations met inclusion and exclusion criteria. A total of 1139 mTBI or SRHI subjects were enrolled across intervention arms in the study populations. A total of eight intervention were studied. Omega-3 fatty acid (n-3FA), melatonin, and Pinus radiata were the only interventions examined in multiple studies. Studies included 10 randomized-control trials, three prospective observational studies, and two retrospective observational studies. Seven of the 15 studies had a low risk of bias. Eleven studies reported benefit of the intervention. Strongest evidence supports n-3FA utility for neurotrauma prevention in athletes exposed to SRHI. Both Pinus radiata and melatonin may have benefit for persistent post-concussion symptoms; however, additional multi-center studies are necessary prior to making a definitive conclusion on these supplements' efficacy. Future studies should continue to assess both novel interventions and additional interventions examined in this review to bring additional evidence to the burgeoning field of nutritional and dietary interventions for SRHI and mTBI.
Introduction
With an estimated 42-56 million occurrences worldwide annually, mild traumatic brain injury (mTBI), including concussion, is a public health crisis. 1 -3 A large number of mTBIs occur in the context of sport or military activities, where participants are also at risk of sub-concussive repeat head impacts (SRHIs), neurotrauma below the threshold to elicit any signs of a concussion. 4 -6 Importantly, both mTBI and SRHI have been shown to result in acute and chronic changes in brain structure and function, 7 and may be associated with long-term neurodegenerative conditions such as Alzheimer's disease, amyotrophic lateral sclerosis, and chronic traumatic encephalopathy. 2,8,9 Despite the known risks of mTBI and SRHI, there is a dearth of literature with recommendations for mTBI and SRHI prophylaxis or treatment.
The lack of effective interventions for mTBI and SRHI in part reflects the multiple secondary mechanisms of injury that result from the initial mechanical trauma, including excitotoxicity, oxidative stress, edema, neuroinflammation, and cell death. 10 -12 To date, most drugs aimed at selected pathways of injury have failed to demonstrate efficacy in clinical TBI trials. It therefore stands to reason that a successful prophylactic or post-injury treatment may have to simultaneously address multiple secondary injury mechanisms. Nutritional interventions, such as dietary changes and nutritional supplements, may offer an opportunity to investigate therapeutic interventions with broader, pleiotropic effects. 11 Further, food products or dietary interventions are often cheaper, more accessible, with fewer potential adverse effects compared with pharmaceutical interventions. 13
Given the risks of mTBI and SRHI, there is a growing body of research investigating nutritional interventions for mTBI and SRHI. Such research has given rise to a new term, nutraceuticals, which refers to nutritional supplements, herbal products, beverages, and dietary modifications that can be used for illness prevention or recovery. 14 However, nutraceuticals do not have as rigorous approval standards as pharmaceutical drugs; nonetheless, many manufacturers claim their nutraceuticals improve or prevent damage associated with neurotrauma without sufficient clinical evidence. 15 -17
Since the regulatory environment of dietary modifications and nutraceuticals does not require a rigorous assessment of their beneficial effects, it is pertinent to assess the efficacy of the major components of such interventions with respect to prophylaxis and treatment of head injury sequalae. Despite the growing interest in nutraceutical treatments for mTBI and SRHI, we found no systematic reviews that examine such mTBI and SRHI interventions in human populations. However, there exists at least one systematic review that examined nutritional interventions of mTBI in animal models and another assessing pharmacologic interventions of mTBI. 11,18 Therefore, the current systematic review examines the state of dietary and nutritional interventions in the prevention and treatment of mTBI and SRHIs sequalae. This review could inform clinical decision-making as well as probe areas for additional research with respect to specific nutritional and dietary interventions in the head trauma field.
Methods
The systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol guidelines 19 (Supplementary PRISMA Checklist; Supplementary PRISMA Flowchart) and was registered with PROSPERO, [CRD42022334011]. 20 Search strings were generated in concert with a research librarian (CC). Search strings were peer reviewed by research librarians at UMass Chan Medical School. Databases searched on May 27, 2022, included PubMed, Scopus, Cochrane, CINAHL, and Web of Science (Supplementary Appendix S1). To be included in the review, studies were required to: 1) investigate healthy human subjects who incurred an mTBI or SRHI; 2) investigate a supplement/ingredient of dietary supplement sold in USA or dietary intervention without classification of drug or statement to prohibit use by FDA; 3) assess a quantifiable outcome; and 4) be published in English in a peer-reviewed journal with an accessible full-length article. Exclusion criteria were: 1) non-mTBI or SRHI subjects (e.g., moderate/severe TBI, stroke); 2) mTBI not assessed separately from moderate/severe mTBI; or 3) studies that required intracranial hemorrhage.
Total number of studies collected were 4643. After de-duplication, 3617 unique studies were screened by one reviewer (CF) to identify which studies met criteria for full-article review. Next, two reviewers (CF and KM) assessed for inclusion or exclusion of full-length articles. Disagreements were reconciled through consensus. Supplementary Figure S1 represents the complete PRISMA protocol process.
Data extraction and bias assessment was performed by two reviewers (CF and DJ). Disagreement over bias level was addressed with discussion and consensus. For randomized-controlled trials, this systematic review used the Revised Cochrane Risk-of-Bias tool for Randomized Trials, RoB 2. 21 For non-randomized controlled trials, this systematic review used the Cochrane Risk of Bias in Non-Randomized Studies–of Interventions tool (ROBINS-I; Fig. 1). 22 Strength of evidence was determined by Oxford Centre for Evidence-based Medicine rating scale (Table 1). 23

Representation of bias assessment for randomized control trials and non-randomized control trials.
Cumulative Summaries of Treatments with Strength of Evidence
GI, gastrointestinal; SRHI, sub-concussive repetitive head impact; mTBI, mild traumatic brain injury; fMRI functional magnetic resonance imaging.
Results
A total of 15 studies from 12 unique study populations were included in this systematic review. The studies assessed the potential of eight unique interventions as a prophylactic or treatment for mTBI or SRHI across 1139 subjects. No studies assessed multiple interventions. The most studied interventions were omega-3 fatty acids (n-3FA) and melatonin, each examined in four studies. Pinus radiata, manufactured and named Enzogenol©, was examined in two studies. No other intervention was assessed in more than one study. Proportional representations of common study characteristics are represented in Figure 2A-D.
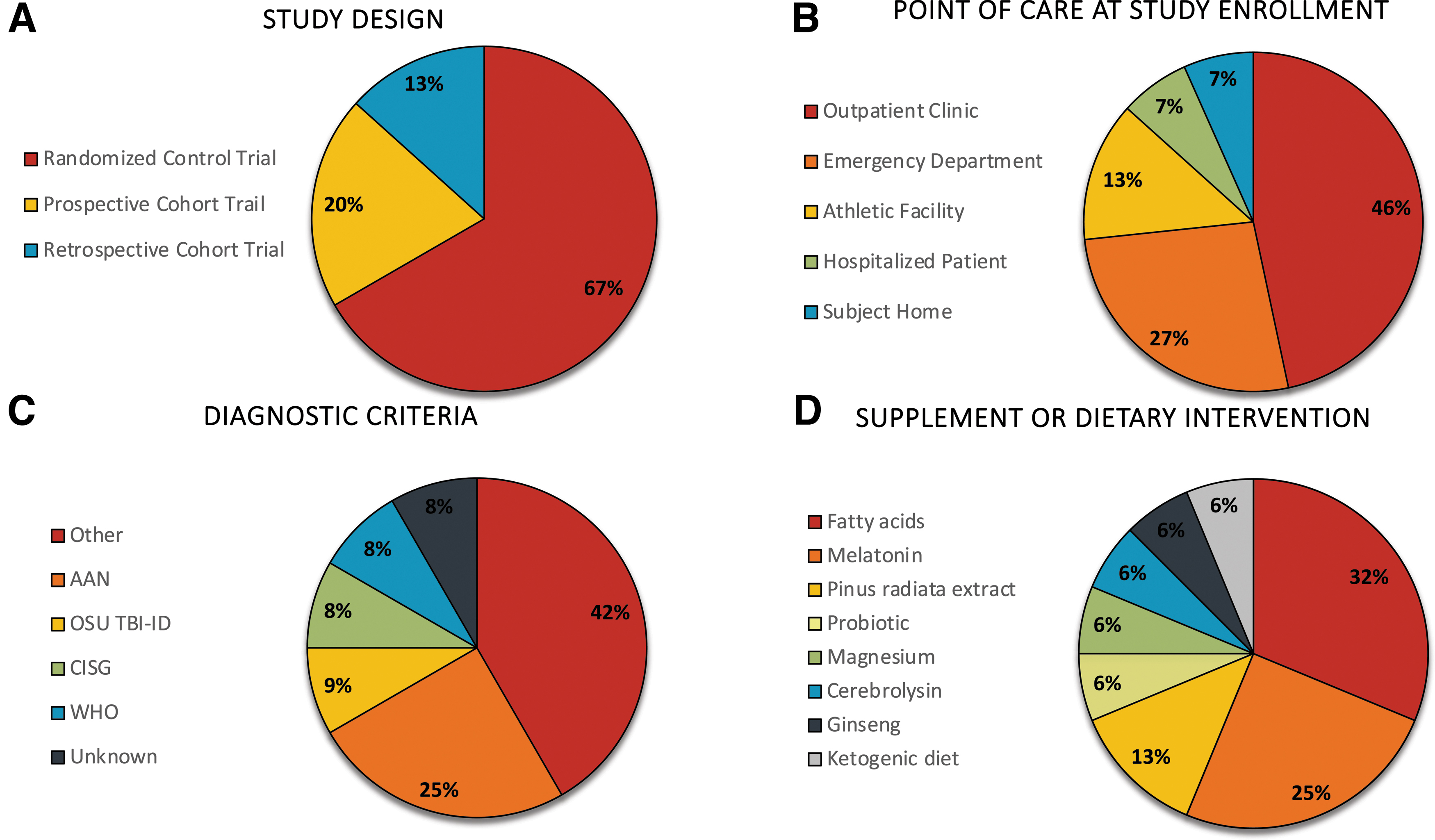
Proportional representation of key figure elements.
Of the 12 study populations, three populations were administered intervention before an athletic season to examine the intervention's utility to prevent SRHI-related neurotrauma. Four populations were enrolled, on average, between 48 h and 1 week post-mTBI, and five were enrolled after reporting persistent-post concussion symptoms (PPCS), defined as lasting more than 1 month post-mTBI. Of these study populations, three populations included only pediatric subjects (maximum age 18 years old), and eight study populations included only adult subjects, of which three exclusively enrolled collegiate football players. One study did not specify a study population with a discernable age range (Fig. 3). 24
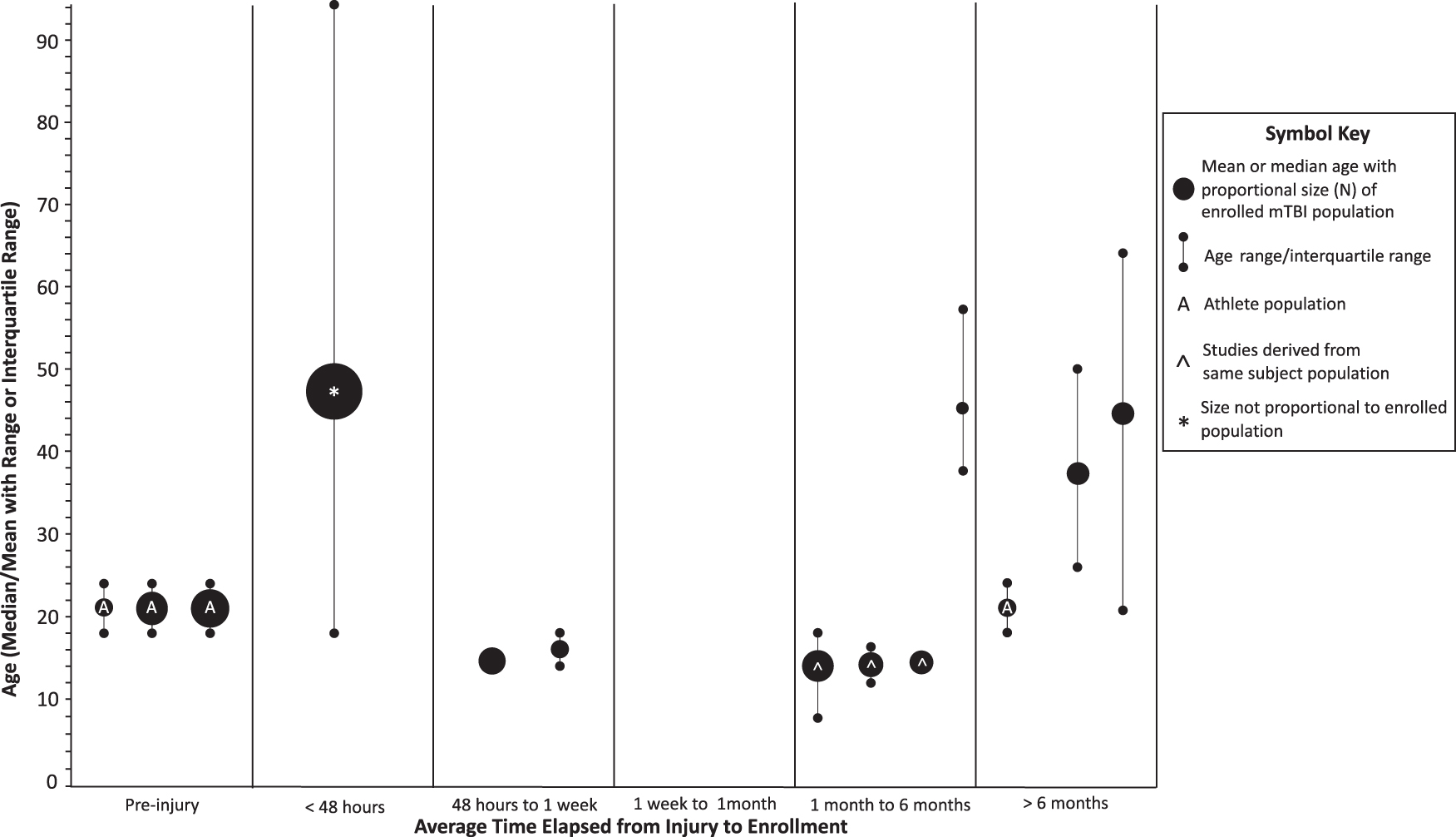
Representation of subject age and age range plotted against time elapsed from mTBI to intervention. Standiford and colleagues 2021 nor Korshnyak and colleagues 2022 were not included as they did not specify a median or mean age for their study population. ⌃Barlow and colleagues 2021, Barlow and colleagues 2020, and Iyer and colleagues 2020 used separate sub-populations from a single gross study population. *Muresanu and colleagues 2015's total mTBI population was 5532 subjects. A: Heileson and colleagues 2021, Mullins and colleagues 2022, Oliver and colleagues 2016 and Walter and colleagues 2017 all drew from either professional or collegiate athlete populations.
Eleven of the 15 studies received funding or indicated financial support from an organization. The most common funding sources included the Canadian Institute for Health Research (CIHR) and Enzo Nutraceuticals©. One study did not explicitly state that it received funding from a private organization, however it did state that supplements were provided by Korean Ginseng Corporation, indicating an affiliation with the organization. 25 Of the funded studies, six received funding from either academic institutes or federal funding, while five studies received funding from private corporations. All privately funded studies reported statistically significant results in support of the studied interventions (100%), while the non–privately funded studies reported statistically significant findings in 60% of the studies.
Bias assessment using RoB 2 (10 studies) and ROBINS-I (five studies) showed that of the 15 studies, eight received evidence of bias (EOB) ratings of at least some concern for bias. Of these eight studies, four EOB ratings indicated either serious or critical levels of bias. Of the randomized control trials rated by RoB 2, 60% had low concern for bias. In comparison, only 20% of the non-randomized control trials had low concern for bias and 40% had a critical level of bias (Fig. 2). A representation of each trial design (Fig. 4) and an evidence table of key study variables (Table 1) was included in this study.

Representation of study design including study time frame and outcome measurements. Representation of each study design for all beginning with time 0 representing study enrollment. If the intervention period had a variable timeframe, the lined bar represents the duration of the longest reported intervention period. If a study reported outcome measured in a variable timeframe, outcome measurements were taken at different time points relative to treatment initiation for subjects. ⌃Staniford and colleagues 2021 collected outcome measures at enrollment as well as 1 h, 48 h and 120 h after enrollment. Korshnyak and colleagues 2022 and Rippee and colleagues 2020 collected daily urinary samples throughout intervention period. Brenner and colleagues 2020 subjects reported daily GI symptoms in a diary for 2 weeks prior to intervention initiation. Color image is available online.
Omega-З fatty acids
Four studies assessed n-3FA supplementation and neurotrauma prevention or recovery. Three studies examined n-3FA interventions for the prevention of neurotrauma from SRHI in collegiate athletes over the course of a football season, using a blood biomarker proxy for brain injury. 26 -28 Oliver and colleagues 2016 (EOB: some concerns; funding: DSM Nutritional Products; intervention n = 62 SRHI) reported on a three-arm trial of DHA supplementation (2 g/day, 4 g/day, or 6 g/day) provided to collegiate football players over the course of a 27-week athletic season. This study reported that, compared with placebo, n-3FA supplementation prevented changes in the blood biomarker neurofilament light chain (Nfl) after an athletic season. 28 A more recent study, Heileson and colleagues 2021 (EOB: serious concern; funding: STRUCT Nutrition; intervention n = 49 SRHI), followed a similar study design; providing 2.9 g/day of combined DHA, EPA, and DPA to NCAA football players over the course of an athletic season. This study reported that the n-3FA regimen prevented Nfl elevation at each measurement interval throughout the football season except for baseline measures as compared with placebo. 26 Mullins and colleagues 2021 (EOB: some concerns; funding: National Institutes of Health; intervention n = 19 SRHI) contradicted the findings of both Oliver and colleagues 2016 and Heileson and colleagues 2021. Mullins and colleagues 2021 reported Nfl levels were not significantly different at any measurement interval between a group of collegiate football players supplemented with 3.5 g of a DHA and EPA supplement five times per week and a control group of players. 27
Miller and colleagues 2022, (EOB: low; funding: none; intervention n = 20 mTBI) examined how 2 g/day DHA supplementation within 4 days of injury effected recovery in pediatric mTBI. This study found that subjects taking DHA supplementation experienced a 5-day reduction in time from injury to the subject reporting no symptoms on the Sport Concussion Assessment Tool 3 questionnaire compared with placebo group. This resulted in quicker return to play than a placebo group. 29
Mullins and colleagues 2021, Oliver and colleagues 2016 and Miller and colleagues 2022 reported on adverse effects attributable to n-3FA supplementation. Adverse effects attributed to supplementation included GI distress (n = 8), halitosis or erucation (n = 5), and acne (n = 2). No serious adverse effects were reported. Heileson and colleagues 2021 did not comment on adverse effects.
Melatonin
Four studies from two separate study populations assessed the effect of melatonin on mTBI recovery in pediatric populations. Barlow and colleagues 2020 (intervention n = 63 mTBI), Barlow and colleagues 2021 (intervention n = 50 mTBI) and Iyer and colleagues 2020 (intervention N = 44 mTBI) utilized the same design and study population (EOB: low; funding: CIHR) to compare the effect of either 3 mg or 10 mg melatonin supplementation after a month of PCS. These studies combined to find that either 3 or 10 mg melatonin supplementation for four weeks corresponded with improved functional magnetic resonance imaging (fMRI) findings and improved subjective sleep; the 3 mg arm even reported reduced depression severity. 30 -32 Howell and colleagues 2021 (EOB: some concerns; funding: none; intervention n = 29 mTBI) found no significant improvement in subjective sleep reports in a population of mTBI subjects presenting within 14 days of injury reporting sleep disturbances post-injury. 33
Barlow and colleagues 2020 and Barlow and colleagues 2021 reported seven instances of adverse effects possibly attributable to intervention including fatigue (n = 2), insomnia (n = 2), cognitive complaint (n = 1), nausea (n = 1), and behavioral change (n = 1). No serious adverse effects were reported. Iyer and colleagues 2020 did not comment on adverse effects; however, it is comprised of a subset of Barlow and colleagues 2020 subjects. Howell and colleagues 2021 did not commented on adverse effects.
Pinus radiata extract (Enzogenol)
Two studies assessed the effect of a 1 g/day for 6 weeks or 12 weeks of Pinus radiata regimen on subjects with PPCS. 34,35 Theadom and colleagues 2013 (EOB: low; funding: ENZO nutraceutical; intervention n = 29 mTBI) reported that subjects 3-12 months post-mTBI with PPCS demonstrated reduced self-reported cognitive failures (CFQ scores) post–12-week regimen as compared with placebo. Walter and colleagues 2017 (EOB: some concerns; funding: ENZO nutraceutical; intervention n = 42 mTBI) reported that subjects 6-36 months post-mTBI with PPCS had improved cognitive function, specifically in Stroop Color-Word testing, and improved physical discomfort after a 6-week regimen compared with placebo.
Theadom and colleagues 2013 reported headache (n = 2) and sleep disturbances (n = 1) in the Enzogenol arm. Such adverse effects did not statistically differ from the placebo group, which also reported similar adverse effects of headache (n = 2) and sleep disturbances (n = 2). Walter and colleagues 2017 did not comment on adverse effects attributed to Pinus radiata supplementation.
Cerebrolysin
Muresanu and colleagues 2015 (EOB: serious; funding: none; intervention n = 745 mTBI) reported that cerebrolysin (20 mL/day or 30 mL/day) administered within 48 h of mTBI improved 10-day but not 30-day symptom recovery outcomes. This indicated that acute stage intervention with cerebrolysin may alleviate short-term symptoms. 36 This study did not comment on adverse effects attributed to cerebrolysin supplementation.
Red Korean Ginseng
Korshnyak and colleagues 2022 (EOB: critical; funding: Korean Ginseng Corporation; intervention N = 42 mTBI) reported that 4-week trial of ginseng supplementation in subjects 4 to 6 years post-mTBI with continued PPCS resulted in normalized physiologic parameters including melatonin and sympathetic activity and improved symptom severity. 25 No adverse effects or serious adverse effects were reported by subjects.
Ketogenic diet with MCT supplement
Rippee and colleagues 2020 (EOB: low; funding: University of Kansas Medical Center/Center for Concussion and Heads Up Foundation; intervention n = 14 mTBI) reported that an 8-week trial of ketogenic diet and medium chain triglyceride (MCT) supplement in a PPCS population resulted in statistically significant memory improvement and a non-statistically significant trend toward improvement in total PCSS. 37
Rippee and colleagues 2020 also reported diarrhea post-medium chain fatty acid supplementation (n = 1) and nausea and fatigue while dieting (n = 1). No serious adverse effects were reported.
Magnesium
Standiford and colleagues 2015 (EOB: serious; funding: none; intervention n = 9 mTBI) reported that 400 mg magnesium (combined with 500 mg acetaminophen) taken within 48 h of mTBI twice a day resulted in improved PCSS scores within 2 days post-intervention initiation compared with placebo. However, the improvement in PCSS scores returned to a non-significant value 5 days after intervention initiation. This indicated that the intervention may alleviate short-term symptoms post-mTBI. 24 Standiford and colleagues 2015 did not comment on presence of adverse effects attributable to magnesium supplementation.
Probiotic
Brenner and colleagues 2020 (EOB: low; funding: Department of Veterans Affairs; intervention n = 16 mTBI) reported no significant improvement of PPCS after a 6-to-10-week trial of daily probiotic. 38 No adverse effect or serious adverse effects were reported by subjects.
Discussion
This systematic review assessed the efficacy of nutritional supplements and dietary interventions for mTBI or neurotrauma prevention and recovery. This is the only systematic review to examine the effects of nutraceuticals on neuroprotection and recovery in a patient population subjected to SRHI or mTBI. In total, eight unique interventions assessed by 15 studies targeted a wide range of potential protective mechanisms, detailed in Figure 5. While the majority of studies (73.3%) demonstrated some utility of nutraceutical intervention in symptom amelioration, functional performance, or blood biomarker expression, none of the interventions represented in this review have yet garnered sufficient evidence to justify their use as first-line therapeutic interventions in a clinical setting. Importantly, only 60.0% of the studies assessed adverse reactions.
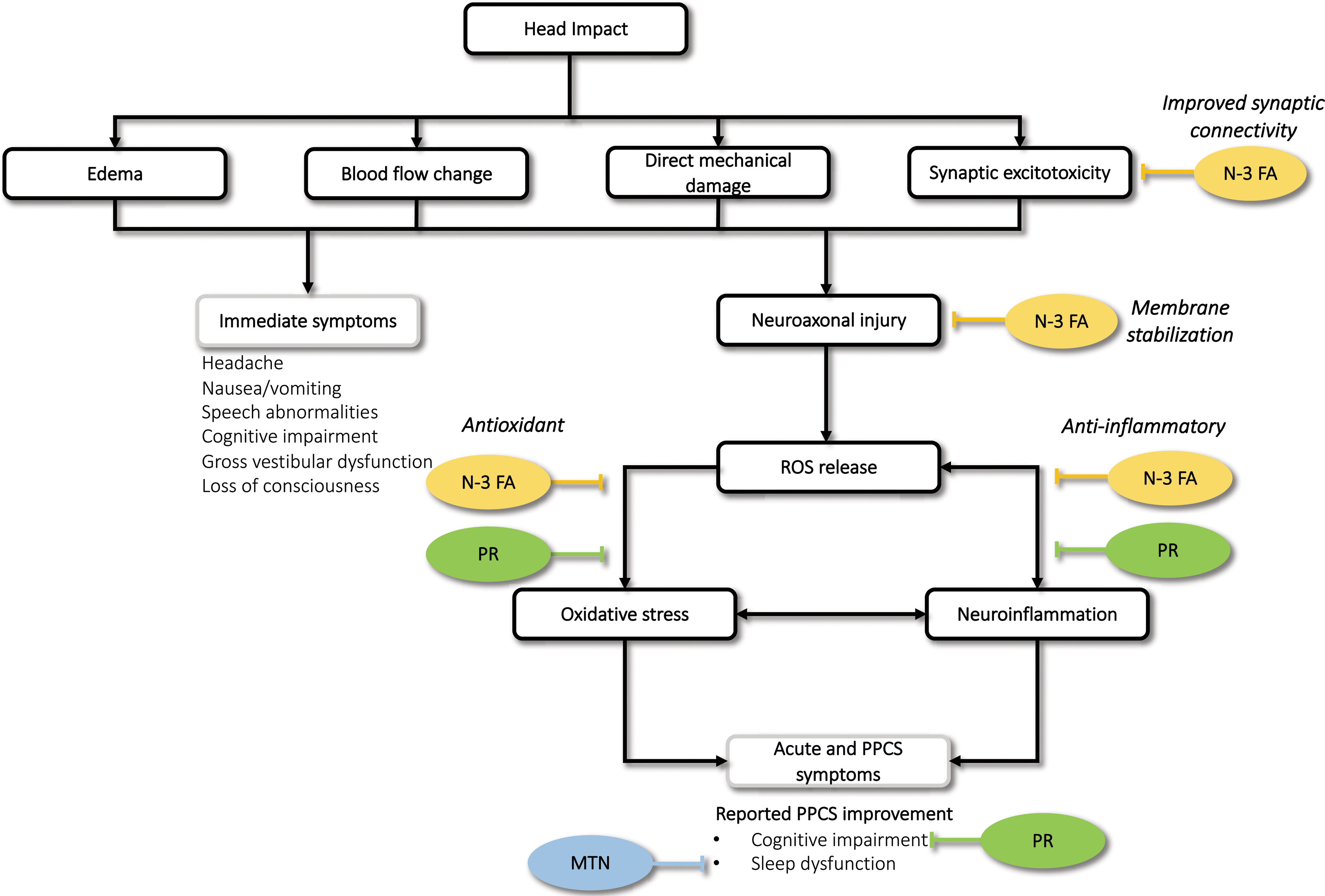
Proposed mechanism of intervention with significant subclinical or clinical benefit in two or more studies. Included interventions includes omega-3 fatty acid (n-3FA) melatonin (MTN), and Pinus radiata. Color image is available online.
Of the nutraceuticals included in this review, n-3FAs are perhaps the most widely studied. Two of three studies concluded that n-3FA prevented serum elevations of Nfl, a neuronal cytoplasmic protein and known biomarker of neuroaxonal injury, in football players and an additional study showed that it improved recovery time post-mTBI. 39 One study failed to demonstrate a statistically significant attenuation of serum Nfl over the course of the season in n-3FA-treated athletes, although it attributed the lack of statistical significance to a small sample size. 27 Further, no serious adverse effects were reported in any of the studies. Therefore, n-3FA supplementation proved to be a safe and effective supplement for protection against neurotrauma recovery for American collegiate football players and may promote faster recovery times when mTBI occurs. 26 –29
Other than n-3FA, two interventions showed clinical and/or sub-clinical evidence for utility in mTBI recovery: melatonin and Pinus radiata extract. Melatonin corresponded with improvement in post-mTBI sleep disturbances or structural neurological improvement as measured by fMRI in two of four studies across two pediatric patient populations. 31,32 Prior studies documented an association between circadian rhythm dysfunction resulting in sleep disturbances post-TBI and endogenous melatonin dysregulation. 40,41 Despite normal physiological expectations and a study in this review demonstrating improved fMRI signaling following melatonin supplementation following mTBI, it remains unclear whether melatonin supplementation produces clinically relevant improvements in mTBI-related sleep impairment. Of note, melatonin supplementation resulted in the side effects of insomnia and daytime fatigue, which are also indications to initiate melatonin treatment after concussion. Nonetheless, given the non-addictive properties of melatonin and minimal side effect profile, 3 mg to 10 mg melatonin may be considered for pediatric mTBI patients. 30 –33,42 More evidence is necessary for adult populations.
Two separate studies reported an improvement in cognitive and/or physical symptoms in PPCS populations when supplemented with a 6-12-week regimen of Enzogenol, a nutraceutical composed of Pinus radiata. 34,35 Pinus radiata primarily contains proanthocyanins (up to 84%), taxifolin (1-2%), and other flavonoids (8%); ingredients associated with antioxidant properties. 43 Both studies hypothesized that Enzogenol's cognitive benefit is derived from the supplement's protection against oxidative stress and neuroinflammation that may persist for years post-mTBI. 34,35 However, in a recent systematic review by Robertson and colleagues (2020) on therapeutic utility of the Pinus spp. in chronic disease populations, efficacy and safety testing was inconclusive. Further, 75% of clinical trials of Pinus sp. are funded by manufacturers with financial stake in the trials' outcomes. 44 Thus, additional non-privately funded studies are warranted to validate significant cognitive improvements in PPCS reported in these two studies.
Magnesium, probiotics, ketogenic diet, cerebrolysin, and ginseng supplementation were each assessed by a single study. Four of the five studies identified a statistically significant benefit from the intervention and all five found little to no adverse effect from the intervention. 24,25,36 -38
This review is not without limitations. First, bias and funding may undermine some of the significant findings: 53.3% of included studies contained at least some concern of bias, with 20% of all studies being identified as high or critical levels of bias. Further, all industry sponsored studies reported findings supporting the studied intervention while 60% of non-industry sponsored or non-funded studies reported findings supporting supplement benefits. 25,26,28,34,35 Industry financial pressure and bias in reporting significant findings limits our ability to gather information that opposes beneficial effects of interventions. 45,46
Second, this study is limited by the variability in classification of food versus drug by ambiguous FDA standards and lack of an international classification consensus. 47 This study excluded two interventions because they were classified as a drug or specifically prohibited by the U.S. FDA despite being an active ingredient in supplement formulations sold either domestically, internationally or both (e.g., N-acetyl-cysteine, piracetam). 48,49 However, cerebrolysin, which is not classified as a food product by the FDA, is an ingredient of nootropic supplement formulations sold in the United States that was included in this review. 36 Given the burgeoning nature of nutraceutical intervention and ambiguity of supplement classifications, strong criteria are needed to determine which formulations should be considered “drug” versus “non-drug” for future studies. Further, any study examining the effect of a nutraceutical or nutraceutical ingredient on a SRHI or mTBI population should include “nutraceutical,” “supplement,” or “diet,” as well as “mTBI,” “concussion,” or “head impacts” in the publication MeSH terms to promote searchability.
Finally, the variability within diagnostic criteria, reporting age of participants, percentage of male and female subjects, duration of treatment, and outcome measures precludes this systematic review from including a meta-analysis. Further, the lack of a singular mTBI diagnostic criteria may confound a consensus on the utility of an intervention. Therefore, standardized measures and subject data should utilize those outlined in the National Institute of Neurological Diseases and Department of Defense (2018). 50
Conclusion
This study collected and reviewed more than 3600 unique studies, of which 15 were included in this systematic review. The included studies assessed the efficacy of eight unique supplements or dietary interventions for recovery post-mTBI and n-3FA efficacy in preventing neurotrauma in subjects exposed to SRHI. While most of these interventions require additional large, randomized control trials to assess their efficacy and side effect profile, n-3FA does appear to provide neuroprotection or improved recovery acutely post-mTBI with minimal side effect profile. Further research must focus on novel nutraceutical formulations claiming utility for mTBI prevention and recovery as well as assessment of efficacy, dosing and duration parameters for interventions examined within this review.
Access to Data and Data Analysis
Charles Feinberg and Dr. Rebekah Mannix had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding Information
No funding.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix S1
Supplementary PRISMA Checklist
Supplementary PRISMA Flowchart
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.