
Abstract
Higher psychological resilience is correlated with less severe post-concussion symptoms (PCS) after mild traumatic brain injury (mTBI) in children, but the directional nature of this relationship remains uncertain. Although traditionally regarded as a stable, trait-like construct, resilience may be malleable and potentially influenced by mTBI and post-concussive symptoms. The current study sought to examine the stability of resilience, elucidate the dynamic nature of the resilience-PCS relation, and determine whether resilience-symptom associations are specific to mTBI or applicable to traumatic injury in general. Participants were children aged 8–16.99 years with either mTBI (n = 633) or orthopedic injury (OI; n = 334) recruited to participate in a prospective cohort study after presenting acutely to five Canadian pediatric emergency departments (EDs). Symptoms and psychological resilience were assessed at 1 week, 3 months, and 6 months post-injury. Group differences in resilience over time were examined using a mixed linear model, and associations between resilience and symptoms over time were examined using random intercepts cross-lagged panel modeling (RI-CLPM). The mTBI group reported significantly lower resilience than the OI group, but the difference was significantly larger 1 week post-injury (d = 0.50) than at 3 months (d = 0.08) and 6 months (d = 0.10). Cross-lagged panel models indicated that resilience had both stable and dynamic aspects, and both affected and was affected by PCS, although their association varied by time post-injury, symptom measure, and reporter (parent vs. child). Higher parent-reported cognitive symptom severity at 1 week was significantly associated with higher resilience at 3 months (β = 0.23, p = 0.001). Higher resilience at 3 months was associated with lower levels of parent-reported somatic symptom severity (β = −0.14, p = 0.004) and fewer total symptoms (β = −0.135, p = 0.029) at 6 months. Higher resilience at 3 months was associated with fewer child-reported symptoms at 6 months (β = −0.11, p = 0.030) and, reciprocally, fewer child-reported symptoms at 3 months were associated with higher resilience at 6 months (β = −0.22, p = 0.001). Notably, injury group was not a significant moderator in cross-lagged models, suggesting that resilience-symptom associations are not specific to mTBI. Psychological resilience and symptoms have bidirectional relationships after injury. Interventions designed to foster resilience have the potential to promote recovery after mTBI specifically and injury more generally.
Introduction
Mild traumatic brain injury (mTBI) involves a traumatic insult that results in an alteration in brain function, typically reflected in a transient disturbance of mental status but not necessarily loss of consciousness. 1 mTBI is a significant public health concern, with a worldwide incidence rate of 55 million annually, and the Centers for Disease Control and Prevention estimate that 65% of mTBIs involve children and adolescents. 2,3 Although most youth demonstrate symptom resolution within 4 weeks, upward of 35% of children with mTBI demonstrate persistent post-concussive symptoms (PCS) lasting beyond that point. 4 –8 For that reason, identifying modifiable factors implicated in persistent PCS has important consequences for clinical management and outcomes.
Several reviews have suggested that psychological factors are significant predictors of PCS after mTBI, 9 –11 including psychological resilience. Resilience refers to the capacity of individuals to adapt to and overcome adversity. 12 The association between resilience and PCS is intuitive; resilience may help in managing the adversity represented by traumatic injury. Studies have consistently found that higher resilience is associated with less severe or fewer PCS. 13 –18 Among these studies, however, only two have specifically examined the role of resilience in pediatric mTBI. 13,14
A key shortcoming of the existing research is that the relation between resilience and PCS has been examined only correlationally. The directionality of the association between resilience and PCS has not been explored. This may be in part because resilience is often assumed to be a stable, trait-like psychological construct. This assumption has been challenged, however, by research suggesting that resilience is malleable, sometimes changing in response to adversity itself. 19 –22 Further, existing research is primarily cross-sectional, precluding assessment of directionality because changes in resilience and PCS cannot be measured or related to one another. Finally, the limited longitudinal research has not applied a robust statistical approach that can assess dynamic relationships between resilience and symptoms over time, likely because of limitations in sample size.
The current study sought to address these issues using data from the Advancing Concussion Assessment in Pediatrics (A-CAP) study, 23 which recruited a large sample of children with mTBI or orthopedic injury (OI) prospectively and followed participants longitudinally for 6 months post-injury. Specifically, the study examined the dynamic nature of resilience across time in two distinct respects. One was to test whether resilience changes over time after injury, and the other was to examine the directionality of the relation between resilience and PCS and whether it changes over time post-injury.
Thus, the first aim was to examine group differences in resilience over time in children with mTBI relative to those with OI. We predicted resilience would increase over time in both groups as the adverse effect of injury dissipated, but we had no a priori hypothesis about the extent or direction of group differences in resilience. The second aim was to examine the directionality of the association between resilience and PCS across time, using random intercepts cross-lagged panel modeling (RI-CLPM), which can parse out the directionality of associations between variables from longitudinal data by testing for within-person associations across time while statistically controlling for stable between-person differences. 24 We expected resilience and PCS to demonstrate bidirectional influences. As part of the RI-CLPM modeling, we tested the invariance of the associations between resilience and PCS across injury groups, to determine whether the relations were specific to mTBI or characteristic of injuries more generally. The results were expected to help clarify whether resilience is a relevant target for promoting recovery after pediatric mTBI.
Methods
Study design
This study uses data from A-CAP, 23 which was a prospective, longitudinal cohort study of children with mTBI or OI aged 8–16.99 years recruited from five pediatric emergency departments (EDs) within the Pediatric Emergency Research Canada (PERC) network. 25 The OI group was included to control for the general effects of trauma and the non-specific nature of PCS. Children and one of their parents were asked to return at 1 week, 3 months, and 6 months post-injury for follow-up-assessments. Recruitment started in September 2016 and ended in December 2018, and all follow-up assessments were completed by July 2019. The A-CAP study was approved by the research ethics boards at all participating institutions. All participants provided written assent and parents provided written informed consent.
Participants
Children were eligible for the mTBI group if they sustained a blunt head trauma resulting in at least one of the following three features, consistent with the World Health Organization (WHO) definition of mTBI 26 : 1) an observed loss of consciousness; 2) a Glasgow Coma Scale (GCS) score of 13 or 14; or 3) at least one acute sign or symptom of concussion as noted by ED medical personnel on a standard case report form (i.e., post-traumatic amnesia, focal neurological deficits, skull fracture, post-traumatic seizure, vomiting, headache, dizziness, other mental status changes). Children with OI were eligible if they sustained an extremity fracture, sprain, or strain caused by physical trauma that scored 4 or less on the Abbreviated Injury Scale, 27 which was established as a cutoff to help ensure exclusion of children with severe injuries. Detailed inclusion and exclusion criteria along with complete study procedures can be found in the published study protocol. 23
Procedures and measures
Ratings of resilience and PCS were collected at the three post-injury assessments. Resilience was rated by the participating child all three times. PCS were rated by both the participating child and one of their parents all three times; additionally, parents provided retrospective ratings of pre-morbid symptoms at the 1-week post-injury assessment.
Resilience was assessed using the 10-item Connor-Davidson Resilience Scale (CD-RISC 10). 28 Total possible scores range from 0 to 40, with higher scores indicative of greater resilience. The CD-RISC has demonstrated acceptable reliability and validity in previous research, including significant correlations with PCS in children with a history of concussion. 13,14,29,30 In the current sample, Cronbach's alpha for the CD-RISC ranged from 0.84 to 0.92 in the two groups across the three assessments.
PCS were measured using two rating scales. The first was the Health and Behavior Inventory (HBI). 31,32 The HBI is a 20-item, factor analytically derived rating scale of PCS frequency that generates somatic (e.g., headache, dizziness) and cognitive (e.g., memory deficits, attention deficits) subscale scores ranging from 0 to 27 and 0 to 33, respectively. The second measure was the Post-Concussive Symptom Interview (PCS-I), which asks respondents to report on the presence/absence of 15 specific symptoms. The PCS-I is administered orally in a face-to-face interview. On both measures, higher scores indicate more severe PCS. Both scales have adequate psychometric properties and have been validated in children with mTBI. 33 –35
Statistical analyses
To address the first study aim, we used a linear mixed model (LMM) to examine changes in resilience across time. Group (mTBI vs. OI), time (post-acute, 3-month follow-up, 6-month follow-up), and their interaction were included as model predictors. An unstructured covariance matrix was used because no assumptions were made about the nature of how resilience may change over time. Post hoc simple effects contrasts were used to explore significant interactions between injury group and time. Maximum likelihood estimation (MLE) was used to adjust for missing data.
To address the second and third study aims, six RI-CLPMs were tested to examine the directionality of the associations between resilience and each of the six symptom measures (i.e., HBI cognitive and somatic scales and PCS-I total score, for parent and child). Parents' retrospective ratings of pre-injury symptoms were treated as covariates. An article published by Hamaker and colleagues introduced the random intercepts component of the CLPM, which has the benefit of adjusting for stable, between-subject variability in the autoregressive parameters of the model that reflects stable associations between predictors. 24 MLE was used to produce model estimates in the RI-CLPM to adjust for missing data.
The focus of RI-CLPM is the cross-lagged relationships between predictors (i.e., resilience and PCS). Although RI-CLPM determines whether a cross-lagged parameter significantly differs from the null hypothesis of no cross-lagged effect, the finding of a significant cross-lagged parameter is not sufficient to declare unidirectionality in the relationships between variables. In all models with a significant cross-lagged effect, an additional direct comparison of cross-lagged parameters across a given interval was completed to establish directionality. In the current study, injury group (i.e., mTBI or OI) was treated as a moderator such that the RI-CLPMs for mTBI and OI were nested in the same model and compared to determine whether associations between resilience and PCS were specific to mTBI or characteristic of injuries more generally.
IBM SPSS version 28 was used to conduct descriptive analyses and the LMM (IBM SPSS Statistics, 2021). MPlus version 8.5 was used to conduct the RI-CLPM. 36,37
Results
Sample characteristics
Participant recruitment and retention is summarized in Figure 1. A total of 967 parent-child dyads consented to participate in the study, 633 with mTBI and 334 with OI. Of those, 423 with mTBI and 218 with OI attended all three post-ED visits, and 136 with mTBI and 69 with OI attended one or two post-ED visits but not all three. All participants with resilience data from at least one post-ED assessment (549 with mTBI; 278 with OI) were included in the LMM that examined group differences in resilience over time. Children who attended at least one post-ED assessment did not differ significantly from those who were only seen in the ED on either demographic or clinical characteristics (i.e., age, sex, race/ethnicity, parental education, neighborhood material and social deprivation, retrospective pre-injury symptom scores, total symptoms reported in ED, 5P study clinical risk score for predicting persisting symptoms 7 ). Moreover, among children attending at least one post-ED assessment, those who attended one versus two versus three follow-up visits differed significantly only in race/ethnicity, because of a high rate of attrition among the small group of indigenous participants. Children did not differ on any other demographic or clinical variables based on the number of attended follow-up visits.
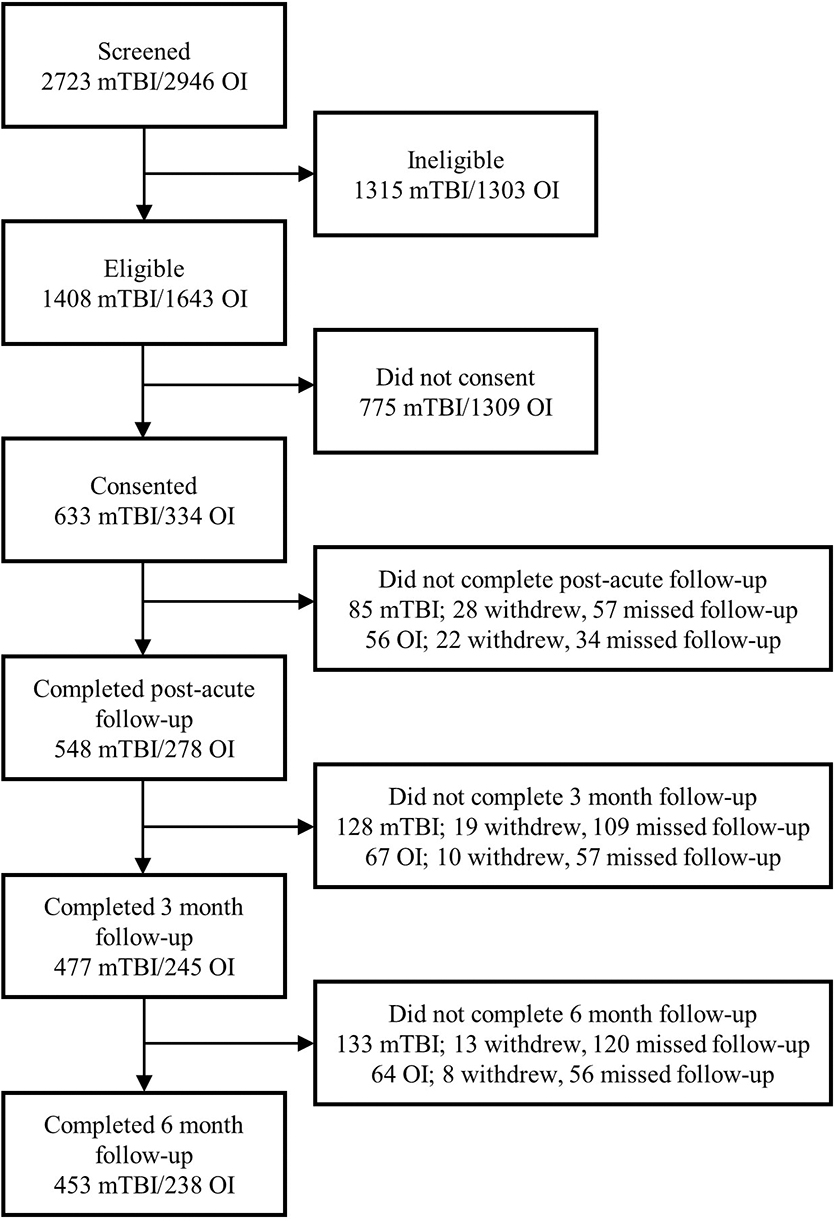
Screening, recruitment, and retention of children with mTBI and OI. mTBI, mild traumatic brain injury; OI, orthopedic injury.
All participants with resilience and symptom data from at least two post-ED visits were included in the RI-CLPMs (502 with mTBI; 260 with OI). Sample characteristics for children included in the RI-CLPM analyses are summarized in Table 1. The OI and mTBI groups did not differ in age, sex, material or social deprivation, 38 race/ethnicity, or parental education. They differed significantly on days to the 1-week follow-up, with a slightly longer mean interval for the OI group, but not on days to the 3-month or 6-month follow-ups. When days to the 1-week follow-up was included as a covariate in the analyses reported below, it was not significant, and its inclusion did not alter any of the results.
Descriptive Chracteristics and Comparisons of the Mild Traumatic Brain Injury and Orthopedic Injury Groups
mTBI, mild traumatic brain injury; OI, orthopedic injury; SD, standard deviation.
Group differences in resilience
Model estimates of resilience as a function of group over time are plotted in Figure 2. The main effects of both group (i.e., injury type), F(1, 828.26) = 21.93, p < 0.001, and time, F(2, 727.74) = 13.18, p < 0.001, were significant, as was the interaction of group and time, F(2, 727.74) = 9.33, p < 0.001. Simple effects contrasts showed that resilience increased significantly across time among children with mTBI, F(2, 732.39) = 29.54, p < 0.001, but did not change among those with OI, F(2, 729.47) = 2.00, p = 0.136. Group differences were largest at the 1-week assessment, such that resilience was significantly lower in the mTBI group than the OI group, with a large effect size, (ψ = −3.82, SE = 0.53) t(842.35) = −7.16, p < 0.001, d = 0.50. Children with mTBI also had significantly lower resilience at 3 months but with small effect sizes, (ψ = −1.42, SE = 0.65), t(776.30) = −2.18, p = 0.030, d = 0.08, and 6 months, (ψ = −1.79, SE = 0.65), t(762.95) = −2.76, p = 0.006, d = 0.10.
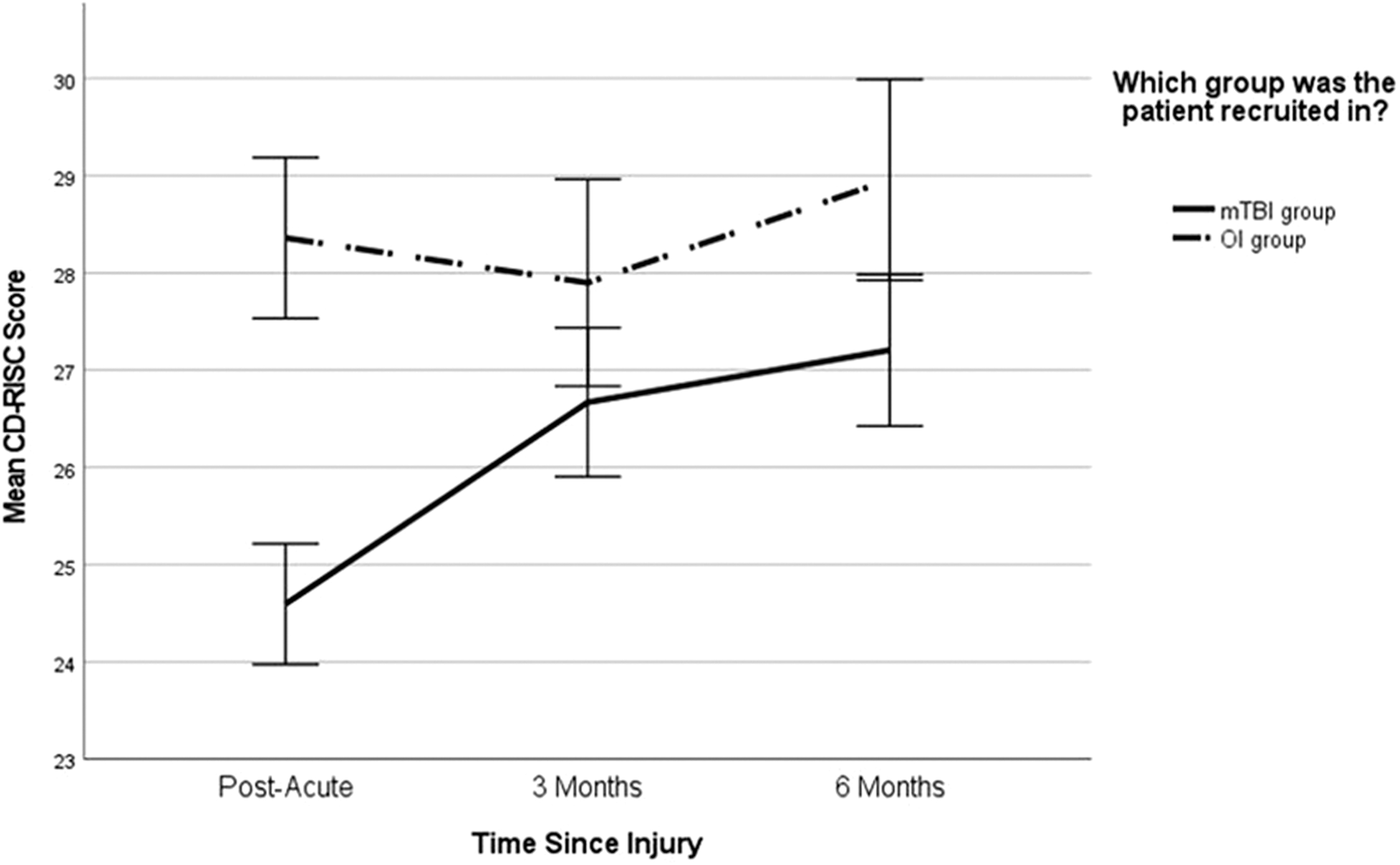
Linear mixed model of mean resilience (CD-RISC) scores over time stratified by injury group, mTBI and OI. Bars represent 95% CIs. CD-RISC, Connor-Davidson Resilience Scale; CI, confidence interval; mTBI, mild traumatic brain injury; OI, orthopedic injury.
Reciprocal modeling of resilience and PCS
Of the six RI-CLPMs, four showed significant cross-lagged coefficients and are presented in more detail here. The models are not stratified by injury group because type of injury did not have a significant moderating effect in any model.
Resilience and parent-reported cognitive symptom severity. The reciprocal effects of resilience and parent-reported cognitive symptoms on the HBI are summarized in Figure 3. The only significant cross-lagged parameter in this model was the positive effect of cognitive symptoms at 1 week on resilience at 3 months, β = 0.23, p = 0.001. However, direct comparison of the cross-lagged parameters over this interval indicated they were not significantly different, t(818) = −0.411, p = 0.086. None of the other cross-lagged parameters were significant, all βs ≤ 0.22 and all ps ≥ 0.090.
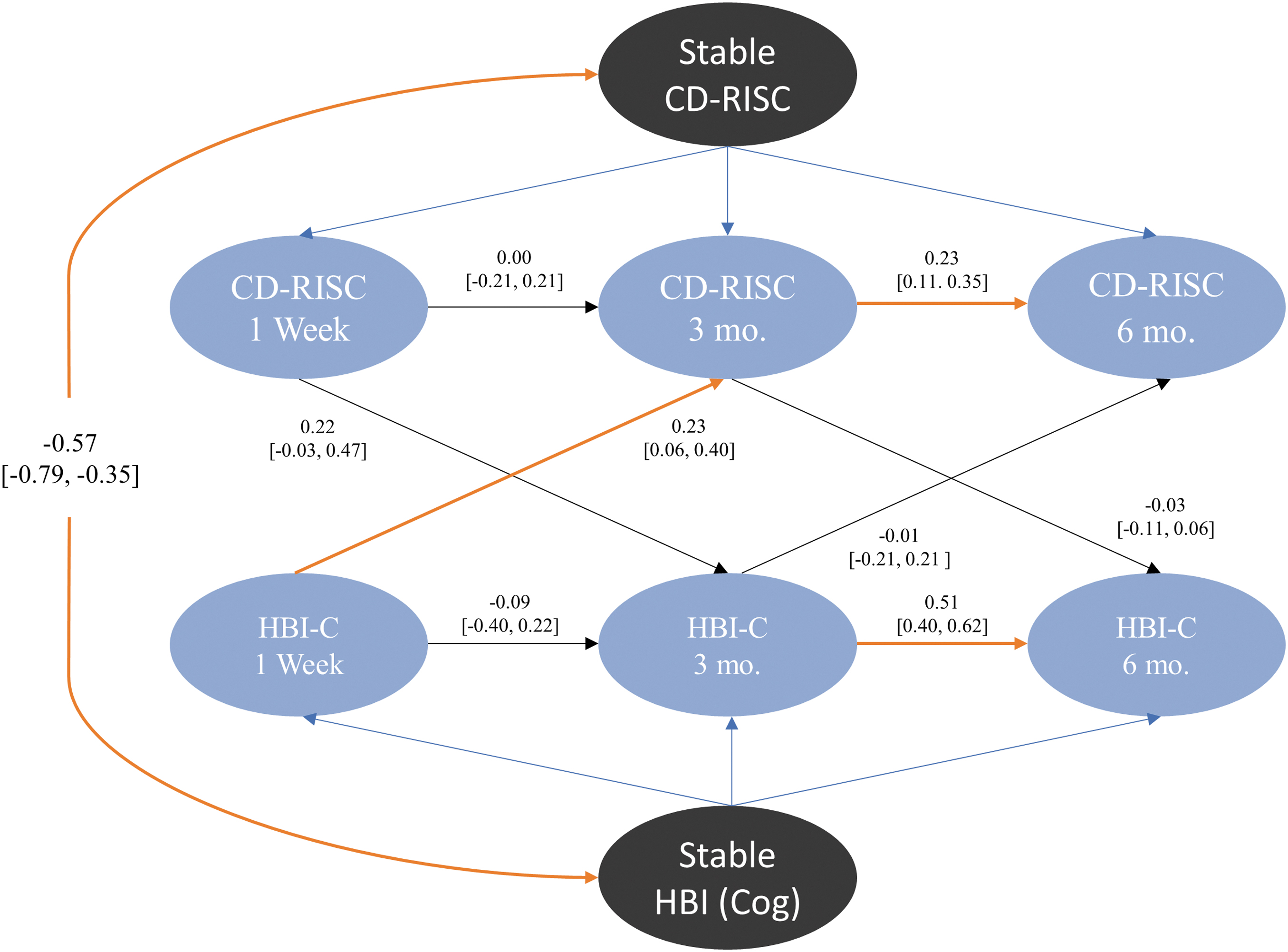
Random intercept cross-lag panel model of parent-reported cognitive symptom severity (HBI-C) and self-reported resilience (CD-RISC) over 6 months (blue). The stable components of resilience and parent-reported cognitive symptom severity are represented by the black ovals. Orange arrows indicate a significant model parameter. Model parameters are indicated alongside their corresponding arrows; brackets indicate the lower and upper bounds of the 95% CI of each model parameter. CD-RISC, Connor-Davidson Resilience Scale; CI, confidence interval; HBI, Health and Behavior Inventory.
Resilience and parent-reported cognitive symptoms both had significant autoregression parameter estimates from the 3-month to 6-month follow-up, β = 0.23, p < 0.001, and β = 0.51, p < 0.001, respectively. However, the autoregression parameter estimates from the 1-week to the 3-month follow-up were not significant, β = 0.00, p = 0.994, and β = −0.09, p = 0.565.
Stable, between-group parameter estimates accounted for statistically significant amounts of variance in both resilience and parent-reported cognitive concussion symptoms, all βs ≥ 0.427 and all ps < 0.001 for resilience, and all βs ≥ 0.633 and all ps < 0.001 for symptom scores. Further, the stable association between the random intercepts of resilience and parent-reported cognitive symptoms was significant, β = −0.569, p < 0.001.
Resilience and parent-reported somatic symptom severity. The reciprocal effects of resilience and parent-reported somatic symptoms on the HBI are summarized in Figure 4. The only significant cross-lagged parameter estimate was the negative effect of resilience on somatic symptoms from the 3-month to 6-month follow-up, β = −0.14, p = 0.004. However, the cross-lagged parameters between 3-month and 6-month follow-ups did not differ from each other, t(832) = 0.16, p = 0.255. None of the other cross-lagged parameters were significant, all βs ≤ 0.12 in magnitude and all ps ≥ 0.127.
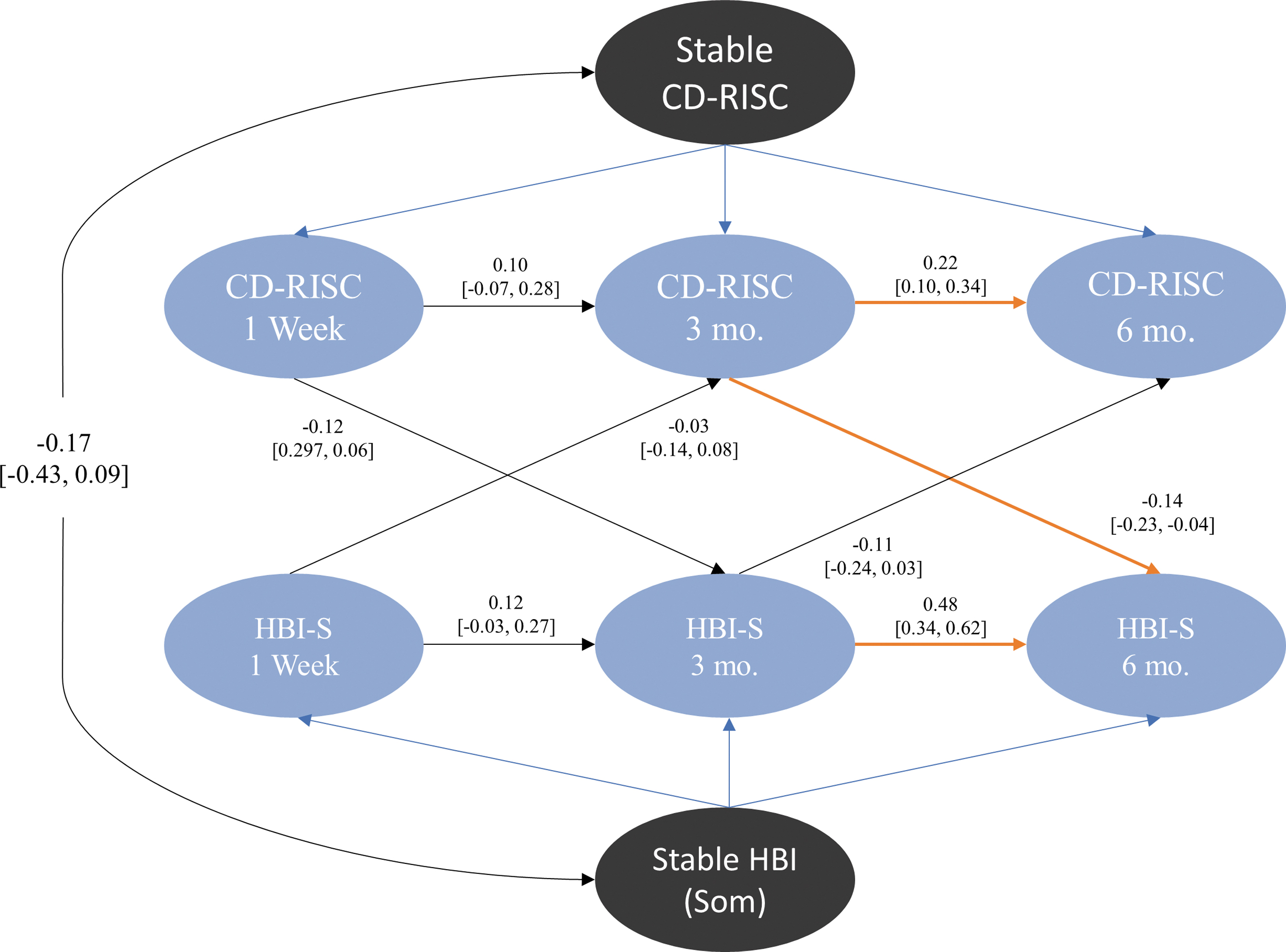
Random intercept cross-lag panel model of parent-reported somatic symptom severity (HBI-S) and self-reported resilience (CD-RISC) over 6 months (blue). The stable components of resilience and parent-reported somatic symptom severity are represented by the black ovals. Orange arrows indicate a significant model parameter. Model parameters are indicated alongside their corresponding arrows; brackets indicate the lower and upper bounds of the 95% CI of each model parameter. CD-RISC, Connor-Davidson Resilience Scale; CI, confidence interval; HBI, Health and Behavior Inventory.
Parent-reported somatic symptoms and resilience both showed significant positive autoregression from the 3-month to 6-month follow-up, β = 0.48, p < 0.001, and β = 0.22, p < 0.001, respectively. However, the autoregression parameter estimates were not statistically significant from the 1-week to the 3-month follow-up for either parent-reported somatic symptoms or resilience, β = 0.12, p = 0.107, and β = −0.10, p = 0.260, respectively.
Stable, between-group parameter estimates accounted for statistically significant variance in both resilience and parent-reported somatic concussion symptoms, all βs ≥ 0.64, all ps < 0.001 for resilience, and βs ≥ 0.31, all ps < 0.001 for somatic symptoms. However, the stable association between the random intercepts of resilience and parent-reported somatic concussion symptoms was not significant, β = −0.17, p = 0.200.
Resilience and parent-reported symptom count. The model of resilience and parent-reported concussion symptom total on the PCS-I is presented in Figure 5. The only significant cross-lagged parameter estimate was the negative effect of resilience on total symptom count between the 3-month and 6-month follow-ups, β = −0.135, p = 0.029. The cross-lagged parameters between the 3-month and 6-month follow-ups were not significantly different, t(818) = 0.147, p = 0.436. None of the other cross-lagged parameters were significant, all βs ≥ −0.07 and all ps ≥ 0.221.
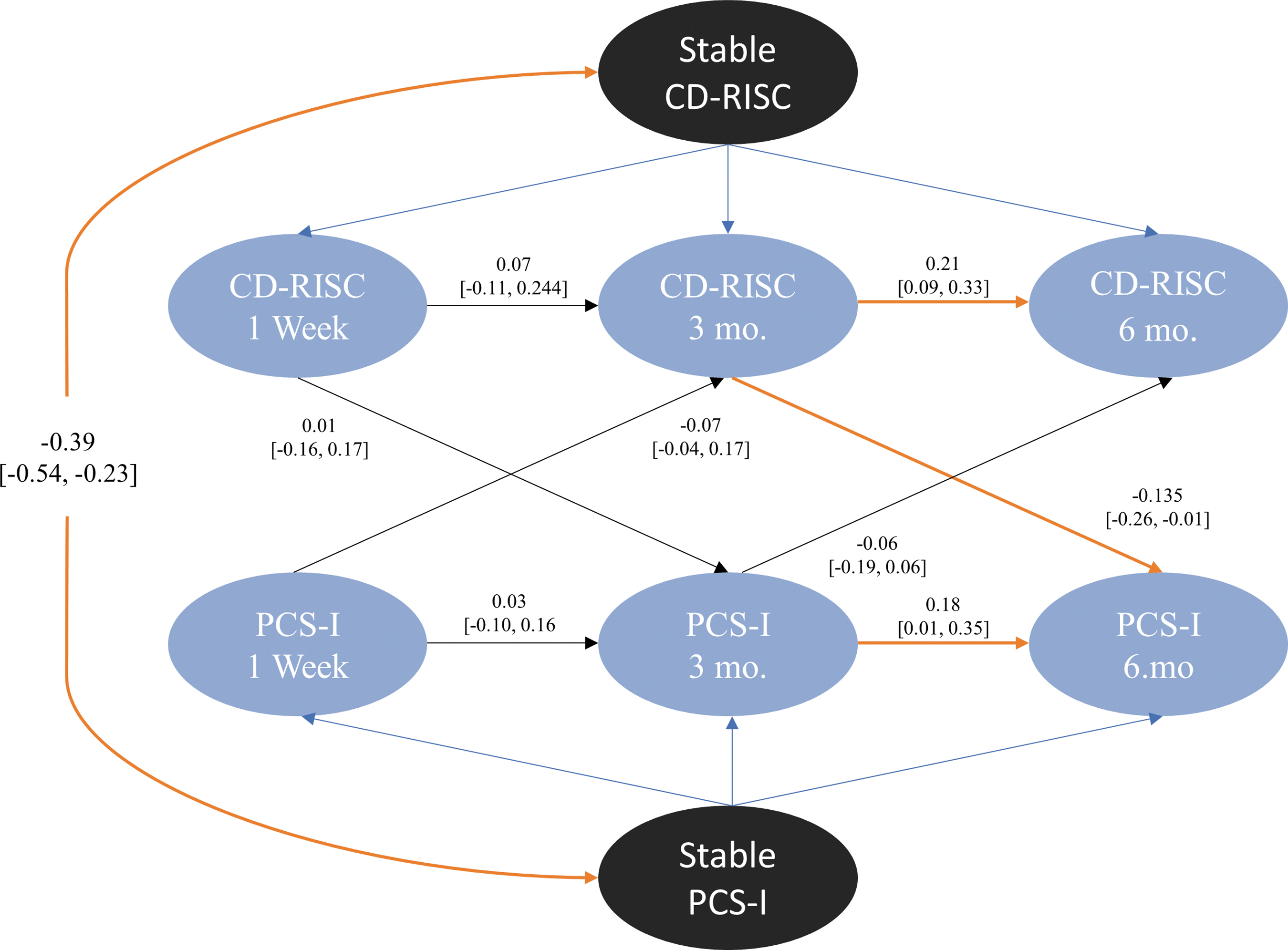
Random intercept cross-lag panel model of parent-reported concussion symptom count (PCS-I) and self-reported resilience (CD-RISC) over 6 months (blue). The stable components of resilience and parent-reported concussion symptom count are represented by the black ovals. Orange arrows indicate a significant model parameter. Model parameters are indicated alongside their corresponding arrows; brackets indicate the lower and upper bounds of the 95% CI of each model parameter. CD-RISC, Connor-Davidson Resilience Scale; CI, confidence interval; PCS-I, Post-Concussive Symptom Interview.
Both total symptom count and resilience demonstrated significant autoregression from 3-month to 6-month follow-ups, β = 0.18, p = 0.04, and β = 0.21, p = 0.001, respectively. However, autoregression parameter estimates were not statistically significant from the 1-week follow-up to the 3-month follow-up for either total symptom count or resilience, β = 0.03, p = 0.660, and β = −0.07, p = 0.438, respectively.
Stable, between-group parameter estimates accounted for statistically significant variance in both resilience and symptom count, all βs ≥ 0.66, all ps < 0.001 for resilience, and all βs ≥ 0.50, all ps < 0.001 for symptom count. Additionally, the stable association between the random intercepts of resilience and concussion symptom count was significant, β = −0.386, p < 0.001.
Resilience and child-reported symptom count. Figure 6 portrays the model of resilience and child-reported total symptom count on the PCS-I. Both cross-lagged parameter estimates were significant from the 3-month to 6-month follow-ups, including a negative effect of resilience on total symptom count, β = −0.11, p = 0.03, and a negative effect of total symptom count on resilience, β = −0.22, p = 0.001. The cross-lagged parameters between the 3-month and 6-month follow-ups differed significantly, t(818) = 0.52, p = 0.002, being higher for the effect of symptom count on resilience. The cross-lagged parameters between the 1-week and the 3-month follow-ups were not significant.
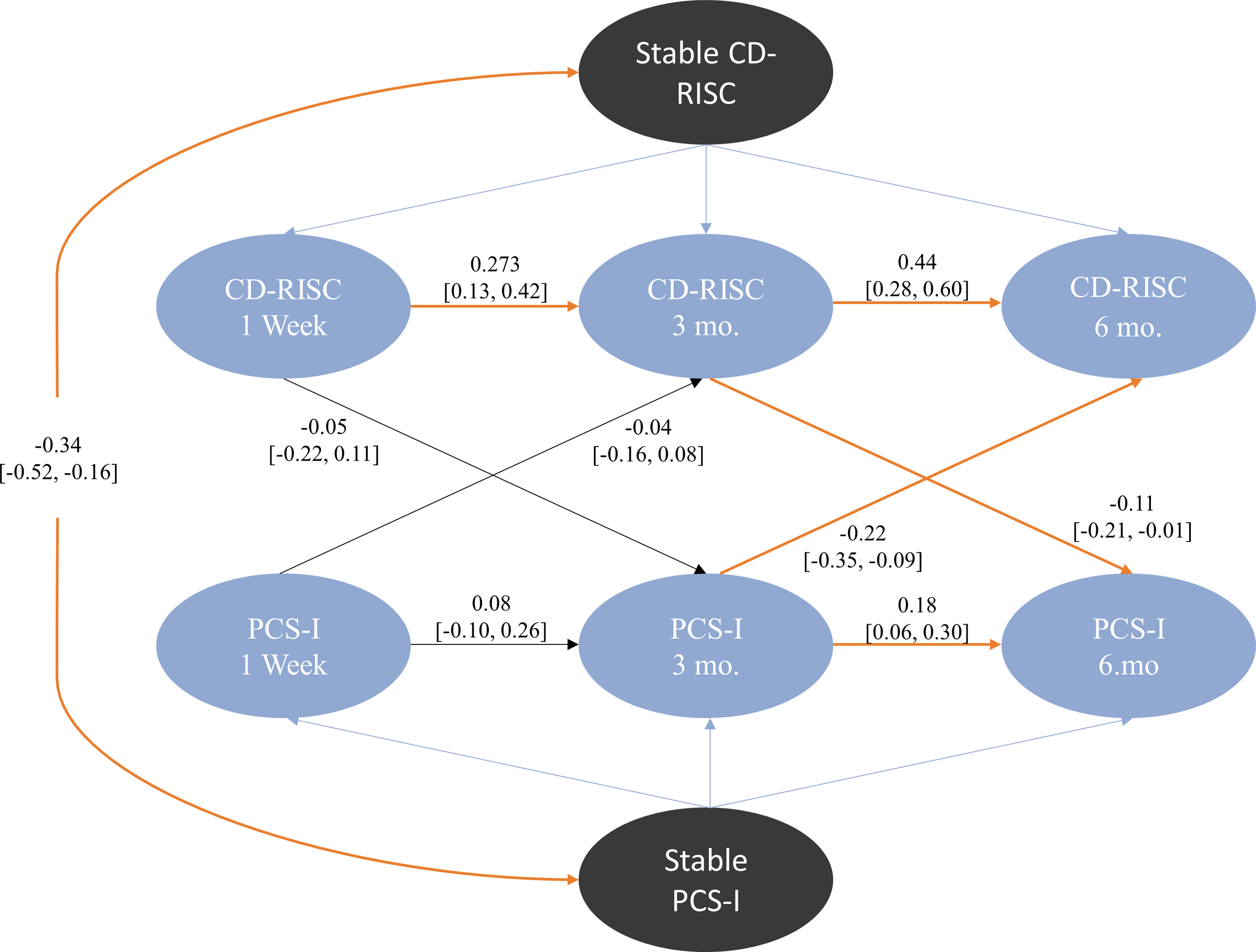
Random intercept cross-lag panel model of self-reported concussion symptom count (PCS-I) and self-reported resilience (CD-RISC) over 6 months (blue). The stable components of resilience and child-reported concussion symptom count are represented by the black ovals. Orange arrows indicate a significant model parameter. Model parameters are indicated alongside their corresponding arrows; brackets indicate the lower and upper bounds of the 95% CI of each model parameter. CD-RISC, Connor-Davidson Resilience Scale; CI, confidence interval; PCS-I, Post-Concussive Symptom Interview.
Resilience and child-reported total symptom count both demonstrated significant autoregression from the 3-month to 6-month follow-up, β = 0.44, p < 0.001, and β = 0.18, p = 0.003, respectively. Further, autoregression from the 1-week to the 3-month follow-up also was significant for total symptom count, β = 0.27, p < 0.001. Autoregression for resilience from the 1-week to the 3-month follow-up was not significant, β = 0.08, p = 0.402.
Stable, between-group parameter estimates accounted for statistically significant amounts of variance in both resilience and child-reported symptom counts, all βs ≥ 0.628 and all ps < 0.001 for resilience, and all βs ≥ 0.474 and all ps < 0.001 for symptom counts. Further, the stable association between the random intercepts of resilience and symptom counts was significant, β = −0.338, p < 0.001.
Discussion
The current study sought to examine the association between resilience and PCS in children with mTBI. The first aim was to examine changes in resilience over time in children with mTBI relative to children with OI. Resilience increased significantly over time in children with mTBI but did not change significantly over time among children with OI; moreover, resilience was significantly lower in children with mTBI compared with those with OI at all three time-points, but particularly at the post-acute assessment. These results may suggest that mTBI results in a unique post-acute decrement in psychological resilience, distinct from injuries broadly, with subsequent increases in resilience as recovery from concussion proceeds. However, pre-injury resilience was not measured, so we cannot be certain that the mTBI and OI groups were equivalent before their injuries.
Although mean resilience differed between groups and over time in the mTBI group, individual differences in resilience showed significant stability. In the RI-CLPM models, the autoregression of resilience over time was consistently significant between 3 and 6 months for both groups, indicating considerable stability in individual differences in resilience across that interval. The RI-CLPM models also indicated stable associations between resilience and PCS independent of injury group. Together, these findings suggest considerable stability to individual differences in resilience across injury recovery in both groups. On the other hand, the RI-CLPM models were not entirely supportive of a static model of resilience. Resilience only showed significant autoregression from 1 week to 3 months in one of six models. Further, autoregression coefficients never exceeded 0.5, indicating that less than half of the variance in resilience at a given time could be explained by prior measures of resilience. Finally, in three models, PCS had a significant cross-lagged effect on resilience. Thus, although resilience shows moderate stability, it is also dynamic in the context of injury recovery. Indeed, the findings suggest that the traditional view of resilience as a static trait is likely incorrect, and are consistent with a growing body of research suggesting that resilience should be considered a dynamic construct. 39
The second study aim was to elucidate the longitudinal, dynamic relationship between resilience and PCS. We found that most directional influences between resilience and PCS were apparent from 3 to 6 months, and generally involved the expected negative association between PCS and resilience. The only exception to this was an unexpectedly positive relationship from 1 week to 3 months, with higher parent-reported cognitive symptoms leading to higher resilience. Taken together, these findings may suggest, first, that injury can temporarily disrupt the typical causal relationships between resilience and PCS, and, second, that in some cases greater PCS may promote greater resilience. This is consistent with other studies suggesting that adversity can, in some circumstances, build resilience. 20,40
The results of the RI-CLPM models also suggest that the directionality of associations between resilience and PCS may be both reporter and scale dependent. Resilience tended to predict PCS but not vice versa when considering parent ratings of PCS, whereas bidirectional relationships between resilience and PCS were only found for child ratings of PCS. Because resilience was rated by children, shared method variance may help account for this latter finding. The findings also suggest that the PCS-I may be more sensitive than the HBI subscales to the dynamic relations between resilience and PCS when examining children's ratings of symptoms, whereas directional relationships were found for both models that used parent ratings on the HBI. The yes/no question format of the PCS-I may be easier for children to complete, whereas the granular nature of the HBI may be more sensitive for parents. Parent and child ratings of PCS generally demonstrate modest agreement, 31,41 so differences between RI-CLPM models based on their ratings are not unexpected.
Of the four models with significant cross-lagged parameters, only one conclusively demonstrated bidirectionality, with both cross-lagged parameters from 3 to 6 months being significant; in that model, the two cross-lagged parameters were significantly different, such that the influence of PCS on resilience was stronger than vice versa. In two other models, resilience at 3 months negatively influenced symptoms at 6 months, whereas symptoms did not significantly influence resilience; in those models, however, the cross-lagged coefficients did not differ significantly. Overall, the evidence suggests that resilience and PCS likely have bidirectional effects that become more apparent with time post-injury, consistent with other research suggesting that non-injury related factors assume growing importance as predictors of PCS after concussion. 42
Given findings indicating that resilience is to some extent dynamic and reciprocally affects injury outcomes such as PCS, future research might target resilience for clinical interventions to help prevent or ameliorate persistent symptoms in the context of both mTBI specifically and injury recovery more generally. Resilience has been a focus of randomized controlled trials (RCTs) designed to benefit a range of other clinical populations, including individuals who have suffered traumatic injury. 43,44 However, these RCTs have been limited to adult populations, and their results may not translate to a pediatric population. Further, the treatment protocols within these RCTs were multi-modal and therefore could not isolate the specific impact of resilience on injury outcomes. However, one RCT targeted psychological resilience specifically in adult participants with mTBI and found that the treatment group had fewer PCS after treatment compared with the control group. 45 Thus, the evidence to date suggests that targeting resilience can potentially produce significant clinical improvement within the context of mTBI and injury more broadly. Further research is needed to understand the mechanisms by which resilience influences injury outcomes and vice versa, and to develop an effective treatment protocol within the pediatric population.
The current study has several limitations. Given only three measurement occasions, an impulse response analysis was not possible. The RI-CLPM models were constrained to examining how one variable at an immediately preceding time-point is related to another variable at the next time. Impulse response analyses allow for examination of how variables at more distant time-points are associated with later variables. Models that allow for impulse response analyses (e.g., the general cross-lagged model) require at least four time-points to have sufficient degrees of freedom to estimate the required parameters. 46 Future studies are needed to determine whether resilience has delayed effects on PCS or vice versa.
Another limitation of the current study is its temporal resolution, given that measures of resilience and PCS were collected at 3-month intervals. Longer intervals between measurements have the benefit of capturing enduring cross-lagged effects but have limited ability to parse how cross-lagged terms may change over time. Greater temporal resolution would also provide clarity about when non-injury factors such as resilience may begin to influence PCS. Future studies should measure resilience and PCS more frequently.
Because our sample was limited to children aged 8 to 16.99 years, the findings cannot be generalized to younger children and older adolescents. Although the sample was representative of the broader Canadian population in terms of sex and race/ethnicity, it was relatively high in socioeconomic status (SES). The higher SES of our sample may reflect greater resources for promoting recovery, and hence may have influenced PCS over time. Generalizability was also limited due to our sample being recruited from EDs. Our results may not generalize to children who seek care outside the ED or who do not seek care at all. Differences between those who agreed to participate versus those who declined, as well as between those who returned for follow-up visits versus those who did not, may also have introduced bias, although we found few differences as a function of retention. Finally, the A-CAP study was conducted from September 2016 to July 2019; the current findings may not extend to current cohorts.
Conclusions
The results of this study provide greater clarity regarding the association between psychological resilience and PCS after mTBI. Where previous studies have assumed resilience to be a predictor of injury recovery, the present study provides evidence for a reciprocal, dynamic relationship between resilience and symptoms that becomes stronger over time and is true of injury in general and not specific to mTBI. Given the reciprocal influences between resilience and symptoms, clinicians may wish to assess resilience when working with children with mTBI, especially if they report persistent PCS. Because resilience appears to be malleable, clinicians may also consider implementing interventions designed to promote resilience as a means of promoting recovery after mTBI and other injuries. However, RCTs of such interventions are needed to confirm their efficacy specifically in children with mTBI or injuries more generally.
Transparency, Rigor, and Reproducibility Summary
The study protocol was published shortly after the A-CAP study began. 23 The study protocol included a general analytic plan, but the specific analysis plan for this article was not formally pre-registered. A sample size of 700 in the mTBI group and 300 in the OI group was planned to provide adequate power to detect small effect sizes. A total of 6449 children were screened in the ED, 3051 were eligible, and 979 were consented and enrolled, of whom 12 withdrew or were later determined to be ineligible. The final sample included 967 children, 633 in the mTBI group and 334 in the OI group. Of those, 829 completed at least one post-ED assessment, and 762 completed at least two post-ED assessments. Key inclusion criteria were based on an established definition. Data were collected by research staff blind to relevant characteristics of the participants. Participants were not informed of their scores on the measures used in the current analyses.
All surveys and questionnaires used in the study are available from the authors. The primary measures used in the current analyses have demonstrated acceptable psychometric characteristics. Missing data were handled using maximum likelihood estimation, as reported in the text. De-identified data from this study are not available in a public archive but can be made available upon reasonable request from any qualified investigator, subject to a signed data access agreement and as allowable according to institutional ethics board standard, by e-mailing the senior author (KOY). Analytic code used to conduct the analyses presented in this study are not available in a public repository but may be available by e-mailing the corresponding author. The authors agree to provide the full content of the manuscript on request by contacting the senior author (KOY).
Footnotes
Acknowledgments
The authors thank the research and hospital staff for their help in collecting patient data. Gratitude is owed to Cherry Zhang, MSc, for assistance in data transformation and cleaning. We are grateful to the parents of participants and the participants themselves, without whom this research would not be possible.
Authors' Contributions
Ali Hassan: conceptualization, methodology, formal analysis, writing–original draft, visualization; Brian L. Brooks, Miriam H. Beauchamp, Roger Zemek, William Craig, Quynh Doan: conceptualization, methodology, investigation, writing–review and editing; Brae Anne McArthur: formal analysis, writing–review and editing; Keith O. Yeates: conceptualization, methodology, investigation, supervision, project administration, funding acquisition, writing–review and editing.
Funding Information
The Advancing Concussion Assessment in Pediatrics (A-CAP) study was supported by a Foundation Grant (FDN-143304) from the Canadian Institutes for Health Research (CIHR) to the University of Calgary (K. Yeates, PI).
Author Disclosure Statement
Brian L. Brooks declares the following conflicts of interest: royalties for the sales of the Pediatric Forensic Neuropsychology textbook (2012, Oxford University Press); royalties for the sales of three pediatric neuropsychological tests (Child and Adolescent Memory Profile [ChAMP]; Sherman and Brooks, 2015, PAR, Inc.), Memory Validity Profile (MVP; Sherman and Brooks, 2015, PAR, Inc.), and Multidimensional Everyday Memory Ratings for Youth (MEMRY; Sherman and Brooks, 2017, PAR, Inc.); grants for concussion/MTBI research; reimbursement for talks on concussion/MTBI; consulting neuropsychologist to the Calgary Flames for the NHL Concussion Program; and private practice work with people with concussion/MTBI.
Roger Zemek has competitively funded research grants from CIHR, Ontario Neurotrauma Foundation (ONF), Physician Services Incorporated (PSI) Foundation, CHEO Foundation, Ontario Brain Institute (OBI), Ontario SPOR Support Unit (OSSU), and the National Football League (NFL) Scientific Advisory Board. Roger holds the Clinical Research Chair in Pediatric Concussion from University of Ottawa, he and has been on the Concussion Advisory Board for Parachute Canada (a non-profit injury prevention charity) and the Board of Directors for North American Brain Injury Society (volunteer position). Roger is the co-founder, Scientific Director and a minority shareholder in 360 Concussion Care, an interdisciplinary concussion clinic.
Keith Owen Yeates receives an editorial stipend from the American Psychological Association. He is an unpaid member of the Scientific Advisory Committee for Brain Injury Canada. He is principal investigator on grants from CIHR and is a co-investigator on research grants from CIHR, the U.S. National Institutes of Health (NIH), Brain Canada Foundation, and National Football League Scientific Advisory Board. He receives book royalties from Guilford Press and Cambridge University Press. He has received travel support and honorarium for presentations to multiple organizations. He receives honorarium for serving on the following groups: Independent Data Monitoring Committee (IDMC), Care for Post-Concussive Symptoms Effectiveness (CARE4PCS-2) Trial, National Institute for Child Health and Human Development; Observational Study Monitoring Board (OSMB), Approaches and Decisions in Acute Pediatric TBI (ADAPT) Trial, National Institute of Neurological Disorders and Stroke; National Research Advisory Council, National Pediatric Rehabilitation Resource Center, Center for Pediatric Rehabilitation: Growing Research, Education, and Sharing Science (C-PROGRESS), Virginia Tech University.