
Abstract
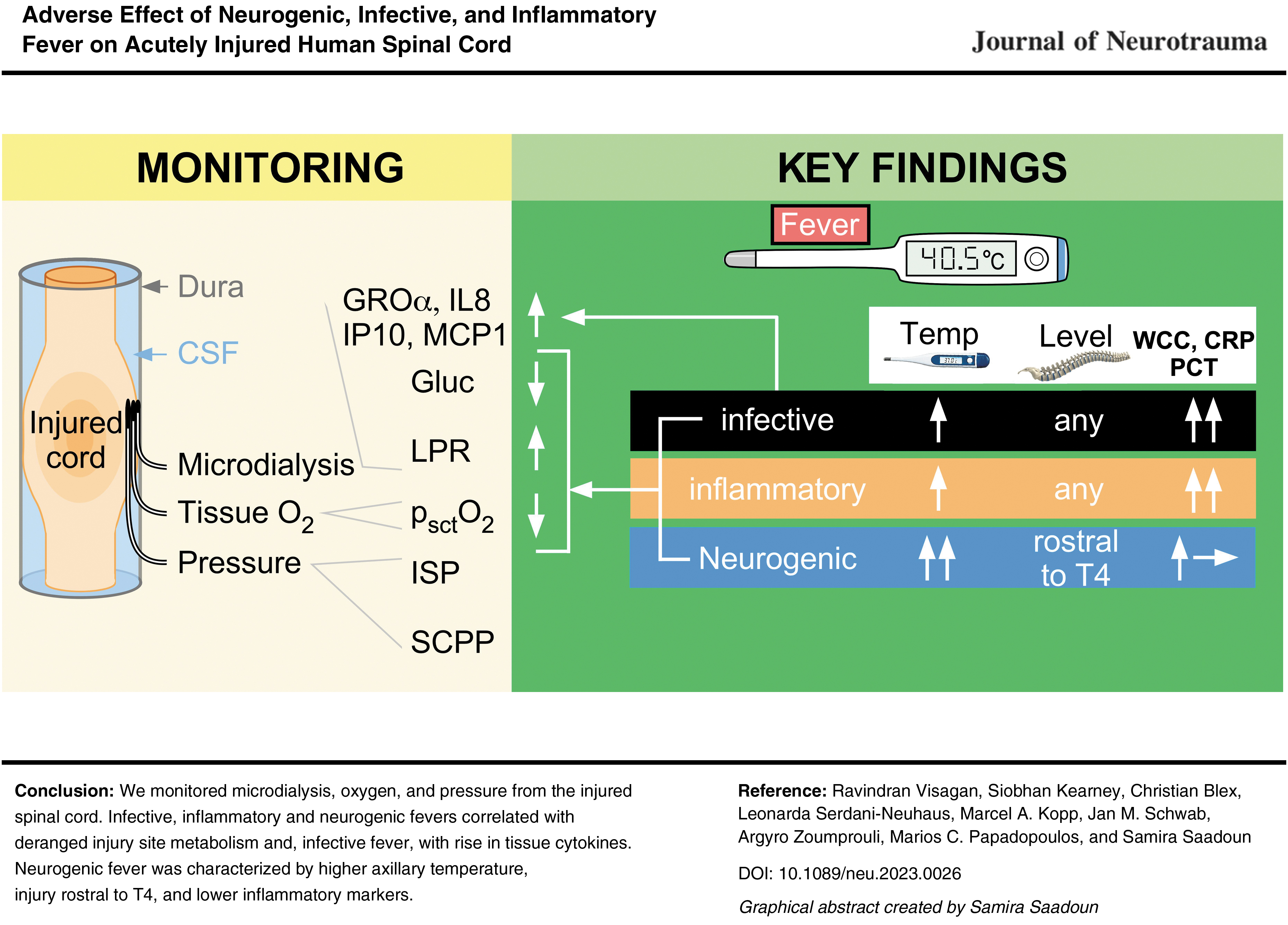
This study aims to determine the effect of neurogenic, inflammatory, and infective fevers on acutely injured human spinal cord. In 86 patients with acute, severe traumatic spinal cord injuries (TSCIs; American Spinal Injury Association Impairment Scale (AIS), grades A–C) we monitored (starting within 72 h of injury, for up to 1 week) axillary temperature as well as injury site cord pressure, microdialysis (MD), and oxygen. High fever (temperature ≥38°C) was classified as neurogenic, infective, or inflammatory. The effect of these three fever types on injury-site physiology, metabolism, and inflammation was studied by analyzing 2864 h of intraspinal pressure (ISP), 1887 h of MD, and 840 h of tissue oxygen data. High fever occurred in 76.7% of the patients. The data show that temperature was higher in neurogenic than non-neurogenic fever. Neurogenic fever only occurred with injuries rostral to vertebral level T4. Compared with normothermia, fever was associated with reduced tissue glucose (all fevers), increased tissue lactate to pyruvate ratio (all fevers), reduced tissue oxygen (neurogenic + infective fevers), and elevated levels of pro-inflammatory cytokines/chemokines (infective fever). Spinal cord metabolic derangement preceded the onset of infective but not neurogenic or inflammatory fever. By considering five clinical characteristics (level of injury, axillary temperature, leukocyte count, C-reactive protein [CRP], and serum procalcitonin [PCT]), it was possible to confidently distinguish neurogenic from non-neurogenic high fever in 59.3% of cases. We conclude that neurogenic, infective, and inflammatory fevers occur commonly after acute, severe TSCI and are detrimental to the injured spinal cord with infective fever being the most injurious. Further studies are required to determine whether treating fever improves outcome. Accurately diagnosing neurogenic fever, as described, may reduce unnecessary septic screens and overuse of antibiotics in these patients.
Introduction
Traumatic spinal cord injury (TSCI) is a catastrophic event with global incidence of about 10.5/100,000 persons, resulting in 768,473 new cases annually worldwide. 1 TSCI causes substantial disability (paralysis, sensory loss, urinary/fecal incontinence, loss of sexual function, hypotension, and poikilothermia), 2 comorbidity (renal failure, decubitus ulcers, pneumonia, and urosepsis), 2 and distress (anxiety, depression, and chronic pain). 3
The mechanisms of neuronal damage in TSCI are identical to those in traumatic brain injury (TBI); in addition to the primary injury, secondary damage is caused by edema, hypotension, hypoxia, metabolic insult, and inflammation. 4 Despite such similarities, the managements of TBI and TSCI differ substantially; in severe TBI, we monitor intracranial pressure (ICP), cerebral perfusion pressure (CPP), and, in some neuro intensive care units (neuro ICUs), brain tissue oxygen (pbtO2) and tissue metabolism (by microdialysis [MD]) to mitigate secondary damage by detecting treatable deleterious factors, for example, high ICP, low CPP, and low pbtO2. Our group developed analogous injury-site monitoring after TSCI. After severe TSCI, we insert pressure, oxygen, and MD probes at the injury site to record intraspinal pressure (ISP), spinal cord perfusion pressure (SCPP), spinal cord tissue oxygen (psctO2), 5 and tissue metabolism. ISP, SCPP, and psctO2 are clinically important parameters that correlate with injury site metabolism 5 –7 and long-term outcome. 8 Increasing SCPP improves somatosensory 9 and motor-evoked responses 10 at the injury site, increases limb power, 6,10 lowers the sensory level, 11 improves urinary 12 and anal 13 functions, and increases psctO2. 7 Monitoring is safe; risks are cerebrospinal fluid (CSF) leak and probe displacement. 7,14,15
In the first 2 weeks after TSCI, up to 71% of patients have fever, 16 associated with cord metabolic stress (low tissue glucose, high glutamate, high lactate to pyruvate ratio [LPR]) and impaired recovery. 17 Previous studies do not distinguish between different types of fever. Fever may be infective, inflammatory (peripheral trauma, surgery without infection, venous thrombosis, drug reaction) or neurogenic. After acute TSCI, neurogenic fever is a distinctive and commonly encountered feature that has been poorly characterized. Here, we used our monitoring techniques to determine the effect of these different types of fever on the injured spinal cord and to identify clinical features that distinguish neurogenic from non-neurogenic fever.
Methods
Institutional research board approvals
Patients were recruited as part of the Injured Spinal Cord Pressure Evaluation (ISCoPE) clinical study at St. George's Hospital, London, UK. Approvals for ISCoPE, including consent form and patient information sheet, were obtained from the St. George's, University of London Joint Research Office, and the National Research Ethics Service London–St. Giles Committee (no. 10/H0807/23). The study was performed in accordance with ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all participants included in the study or their family members. ISCoPE is registered at
Inclusion and exclusion criteria
We included all patients with TSCI recruited into ISCoPE between September 2016 and December 2021 with viable ISP, SCPP, MD, and psctO2 monitoring signals. Inclusion criteria were: 1) severe TSCI defined as American Spinal Injury Association Impairment Scale (AIS) grade A, B, or C; 2) age 18–70 years; and 3) timing between TSCI and surgery within 72 h. Exclusion criteria were: 1) patient unable to consent; 2) other significant comorbidities; and 3) penetrating TSCI.
Neurosurgical management and probe placement
All patients were admitted to the neurosurgical unit at St. George's Hospital and underwent International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) assessments by a trained neurosurgical resident, which were repeated prior to discharge to the rehabilitation unit (2–3 weeks post-TSCI) and at follow-up. Surgical decompression and spinal instrumentation were performed by a neurosurgeon. The type of surgery was based on clinical indication and surgeon preference and included posterior approach with lateral mass (cervical), pedicle screw (thoracic), and rod fixation (Stryker Oasys for cervical and Stryker Xia for thoracic; Stryker UK, Newbury, Berkshire, England).
At the end of posterior surgery to decompress the spinal cord and fix the spine, a pressure probe (Codman Microsensor Transducer®, Depuy Synthes, Leeds, UK), an MD catheter (CMA61, CMA Microdialysis AB, Solna, Sweden), and an O2 electrode (Licox CC1P1, Integra, Sophia-Antipolis, France) were inserted intradurally under the operating microscope, were positioned on the surface of the injured cord at the site of maximal cord swelling, and were secured to the skin using silk sutures. This setup allows multi-modality monitoring (ISP, SCPP, psctO2, tissue glucose, tissue LPR) from the injury site (Fig. 1). The patients received antibiotics at induction (cefuroxime 1.5 g intravenously if no penicillin allergy) and 48 h of vancomycin and gentamicin post-operatively according to body weight as standard protocol. Pre-operative computed tomography (CT) and magnetic resonance imaging (MRI) of the spine were performed, then post-operative CT of the spine, typically within 2 days, and post-operative MRI of the spine, typically within 1 week after probe removal.
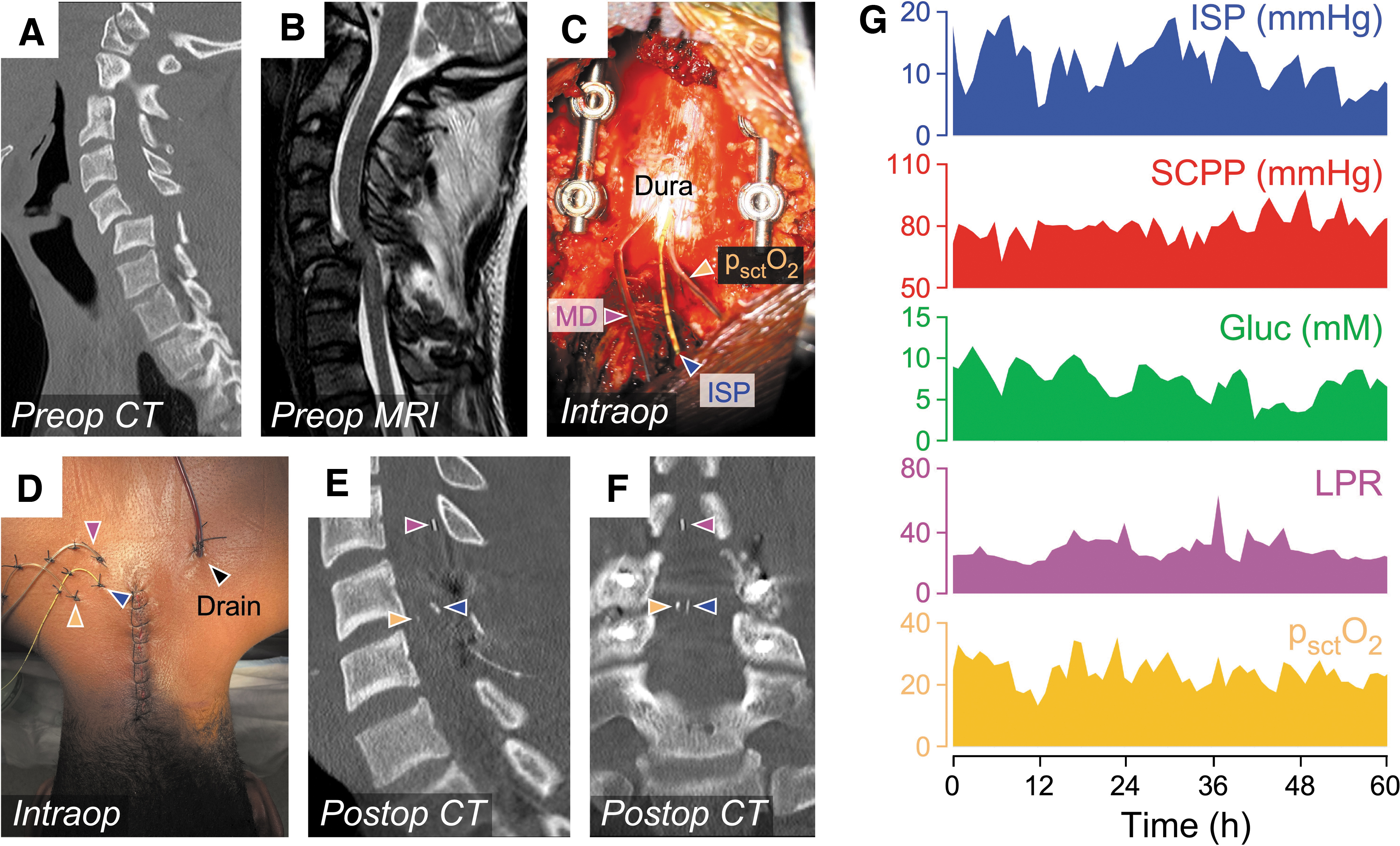
Monitoring setup.
Neuro ICU management
Post-operatively, all patients were admitted to the neuro ICU where they were reviewed daily by neuro ICU and neurosurgery teams. Each patient's ventilation was supported as appropriate with corresponding sedation, dependent on the level and severity of TSCI. This may have included timely extubation post-operatively or early tracheostomy. The surgical wound was reviewed daily, a post-operative drain was kept on gravity, and the patient was turned in bed to avoid pressure sores. To prevent venous thromboembolism, we used a standard protocol of Flowtrons® plus prophylactic low-molecular-weight heparin started at 48 h. To date, we have not observed post-operative hemorrhage in our patients with TSCI using this protocol. 18 Vasopressor support (norepinephrine) was provided as required without set SCPP parameters. Neuro ICU physicians did not act on ISP, SCPP, psctO2, or MD values in line with the observational nature of the study. The ISP, MD, and psctO2 probes were removed within 1 week, and the probe skin exit sites were sutured using nylon.
ISP and SCPP monitoring
The ISP probe was connected to a Codman ICP box linked via a ML221 amplifier to a PowerLab data acquisition hardware device, in turn linked to a laptop running the data acquisition and analysis software LabChart v.8 (ADInstruments, Oxford, UK). Arterial blood pressure (ABP) was recorded from a radial artery catheter connected to a Philips Intellivue MX800 bedside monitor (Philips, Guildford, UK ) and then to the PowerLab system or ICM+. The ISP and ABP signals were sampled at 1 kHz and used to compute SCPP as mean arterial pressure (MAP) – ISP. ISP is the same as intraparenchymal cord pressure at the injury site, 19 which is different from CSF pressure measured above or below the injury because the swollen, injured cord is compressed against the dura, thus compartmentalizing the intrathecal space as described in earlier publications. 10,14,20
Microdialysis monitoring
MD was started post-operatively in the neuro ICU as described. 15,17,21 Central nervous system fluid (CMA Microdialysis AB) was perfused at 0.3 μL/min using the CMA106 pump (CMA Microdialysis AB). MD vials were changed hourly and analyzed using ISCUS Flex (CMA Microdialysis AB) for glucose, lactate, and pyruvate. The LPR was calculated. The first two samples from each patient were discarded to allow priming of the MD catheter and stabilization of the metabolite concentrations. One-hundred-fold changes in metabolite concentration, compared with the preceding hour, were excluded from the analysis, assumed to be errors in measurement. Our MD method measures spinal cord surface metabolism at the injury site, which correlates with intraparenchymal injury site metabolism, but is different from metabolites measured from lumbar CSF. 15,17,21
Tissue oxygen monitoring
The O2 electrode was connected to a Licox PtO2 Monitor (Integra), in turn linked to a Philips Intellivue MX800 bedside monitor (Philips), which was connected to the PowerLab system. The Licox signal was sampled at 1 kHz.
Patient assessments
Patients had an ISNCSCI examination on admission, at about 2 weeks post-operatively, and at 6-month follow-up. A pre-operative CT spine and MRI scan were performed. Following surgery, patients underwent regular motor limb assessments on the neuro ICU. A CT scan of the spine was performed typically within 48 h of surgery. Post-operatively, arterial blood gases were measured, initially 4–6 hourly, then at the discretion of the neuro ICU staff. Venous blood tests including white cell count (WCC; normal 4–11 cells/μL), C-reactive protein (CRP; normal 0–20 mg/L), and procalcitonin (PCT; normal <0.49 μg/L) were performed daily.
Temperature recordings
Our neuro ICU staff monitored peripheral temperature every 1–4 h by placing a SureTemp Plus (WelchAllyn, Aston Abbotts, UK) thermometer in the axilla for 12–15 sec. Temperature readings were paired with ISP and MAP readings for 30 min before and after the reading and with the chronologically nearest arterial or venous blood samples. Use of axillary temperature was a pragmatic choice because not all patients had monitoring of central temperature.
Fever definitions
We defined normothermia as 36.5–37.4°C, low fever as 37.5–37.9°C, and high fever as
Only fever episodes occurring in the post-operative, multi-modality monitoring period (up to 7 days) were included in the analysis. A few delayed infections during the hospital episode are reported in the section Complications (see also Table 1). Further, not all infections manifested in high grade fever, that is, non-pyrogenic, and so are reported in Table 1 but not the high-grade fever analysis. This accounts for the discrepancy between reported fever episodes and reported infective complications.
Complications of Monitoring
CSF, cerebrospinal fluid.
Cytokine/chemokine analysis
We measured the concentrations of cytokines/chemokines in the MD fluid collected from the injury site. These molecules were selected because they have been implicated in the pathophysiology of TSCI; they are <30 kDa (i.e., cross the MD membrane) and are part of our multi-plex electrochemiluminescence assay panel. For each patient, MD vials were collected during normothermia and during high fever. MD vials, each containing ∼10 μL, were stored at −80°C and analyzed in a blinded fashion at Charité-Universitätsmedizin Berlin by multi-plex electrochemiluminescence assays (Meso Scale Discovery, Rockville, MD, USA) using the following antibody sets from the U-PLEX Biomarker Group 1 Human Assays panel (K15067M): interleukin (IL)-4, IL-8, IL-10, IP-10, GRO-α, MCP-1, MIP-1α, and MIP-1β. If necessary, the MD samples were diluted to the minimum required volume for a single determination (25 μL) or analyzed directly according to the manufacturer's protocol. Ninety-six-well plates including samples, blanks, and recombinant standard concentrations were measured and unknown concentrations calculated, using the MESO QuickPlex SQ 120 Reader and the MSD DISCOVERY WORKBENCH software version 4.0 (Meso Scale Discovery, Rockville, MD, USA), respectively.
Serum procalcitonin (PCT) measurement
PCT was measured pre-operatively and daily during the period of monitoring. For the first 26 patients, PCT was measured using a portable analyser (Biopanda BR G800 PCT immunoassay, Belfast, UK) In subsequent patients, we measured PCT levels at the St. George's Hospital biochemistry laboratory as part of the daily blood tests done in the neuro ICU.
Neuro ICU response to fever
During fever, blood, sputum, line, urinary catheter, and wound swabs were cultured. A chest radiograph was performed. There was daily neuro ICU review by clinical microbiology physicians who may request repeat cultures depending on the clinical picture and laboratory findings. Antipyretics administered were typically paracetamol 1 g 4 times a day and, either diclofenac infusion 150 mg daily, or ibuprofen orally 400 mg 3 times daily. On rare occasions when fever was refractory to pharmacotherapy, active surface cooling to normothermia was employed.
Vasopressors
Vasopressors were administered at the discretion of the neuro ICU. In general, a minimum MAP of 80 mmHg was advised. The neuro ICU team were blinded to the ISP, SCPP, psctO2, and MD measurements. Intravenously administered norepinephrine (4 mg/50 mL, 5% dextrose) via a central venous catheter was the preferred inotrope. In some patients, metaraminol (10 mg/20 mL, 0.9% saline) was used initially. Vasopressor dose administered was recorded hourly by the neuro ICU nurses.
Statistical analysis
For each fever type, percentage of hours at high fever versus temperature and versus day after TSCI were compared by two-way analysis of variance (ANOVA). Number of cases of each fever type at or above vertebral level T3 versus below T3 (the expected level of neurogenic temperature dysregulation) were compared by Fisher's exact test. Change in the level of an injury site physiological variable (e.g., LPR) may precede the onset of fever or may be caused by an insult unrelated to fever (e.g., drop in SCPP). Thus, to determine the effect of fever on each injury site physiological variable, we assessed trends related to episodes of normothermia then fever then normothermia, rather than plotting the level of the injury site physiological variable during normothermia versus fever. The number of times that ISP, SCPP, tissue glucose, tissue LPR, and tissue psctO2 increased, remained constant, or decreased during fever versus normothermia, during short (1 h) versus prolonged (>1 h) fever, or during pre-fever versus normothermia were compared using Fisher's exact test. Chemokine/cytokine levels during fever versus baseline were compared using the paired Mann-Whitney U test. Statistical tests are two-tailed. The data mining freeware Orange 3.34.0 was used to classify fever as neurogenic versus non-neurogenic using Tree, Stochastic gradient descent, Neural network, Logistic regression, and CN2 rule induction classifiers with leave-one-out cross-validation to compute Area Under Curve, Classification Accuracy, F1 score, Precision, and Recall.
Results
Participants
We recruited 86 consecutive patients with TSCI who contributed 5591 h of monitoring data in total. All subjects and family members approached agreed for the patients to participate. Table 2 shows demographic information. Most (80.2%) were males, and most (84.6%) were younger than age 60 years. There were 59.3% cervical, 34.8% thoracic, and 5.8% conus injuries. On admission, 59.3% of the patients were AIS grade A, 16.3% grade B, and 24.4% grade C. Most patients (82.6%) had posterior surgery only, and the rest (17.4%) had combined anterior + posterior. AIS grade at follow-up (on average 2.7 years) improved in 40.2%, stayed the same in 56.1%, and deteriorated in 3.7%.
Patient Characteristics
AIS, American Spinal Injury Association Impairment Scale; ISP, intraspinal probe; MD, microdialysis; psctO2, tissue oxygen; SCPP, spinal cord perfusion pressure; SEM, standard error of the mean.
Complications
Table 1 lists complications. Of the patients, 11.6% had CSF leak from probe exit site(s), successfully managed by placing extra skin sutures at the bedside. On the 2-week post-operative MRI, 34.9% of patients had non-compressive pseudomeningocele, all conservatively managed. Of these, 50% had an MRI at 6–12 months, showing near-total or total resolution of the pseudomeningocele in 80%. Of the patients, 1.2% had positive wound swabs and drain fluid culture with neck stiffness reported as a “serious adverse event,” successfully managed with antibiotics for possible central nervous system (CNS) infection. There was no probe-related hematoma or spinal cord damage based on neurological function and MRI. Of the patients, 4.7% had wound infections: the one patient requiring a wound washout had poorly controlled diabetes, primary Escherichia coli urosepsis and subsequent wound infection.
Fever characteristics
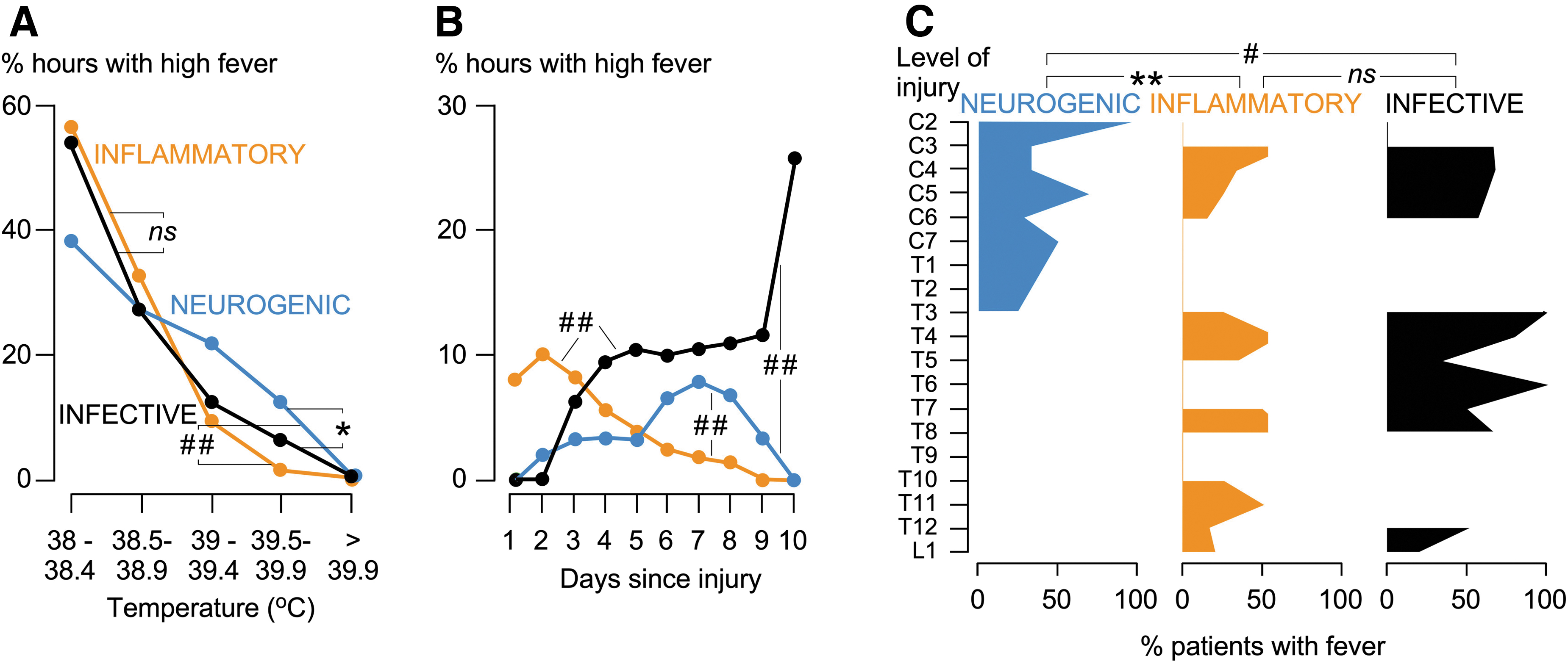
High fever (axillary temperature
Characteristics of different fevers.
Incidence of High Fever (
Figures represent fever episodes from pyrogenic infections. Non-pyrogenic infections and/or delayed infections outside the multi-modality monitoring period in Table 1.
Total number of hourly temperature recordings, of which 2864 h had accompanying monitoring data.
Inflammatory fever source attributed as “Unknown” when criteria not met for other causes.
Wound sepsis accounted for high fever in 1 patient; however, four cases presented in Table 1: Complications because the remainder did not manifest with fever.
Moderate index of suspicion but no corresponding positive culture; see the Methods section.
DVT, deep venous thrombosis; PE, pulmonary embolism.
Effect of fever on injury site physiology and metabolism
We asked if the three types of fever are associated with metabolic stress at the injury site. Five parameters monitored from the injured cord were studied: ISP, SCPP, glucose, LPR, and psctO2. We determined how often each parameter increases, is unchanged, or decreases during fever and compared with the corresponding frequencies for normothermia (Fig. 3). None of the three fever types affect ISP or SCPP (not shown), but all three are associated with low glucose, high LPR, and low psctO2 (the changes in psctO2 did not reach significance for inflammatory fever). We conclude that all three fever types are associated with metabolic stress at the injury site.

Physiology and metabolism of injured cord during fever. ), no change ( ), or decrease (
), or decrease ( ) in GLUC, tissue LPR, and psctO2. P < 0.05*, 0.005***, 0.0001###. GLUC, tissue glucose; LPR, lactate to pyruvate ratio; psctO2, tissue oxygen.
) in GLUC, tissue LPR, and psctO2. P < 0.05*, 0.005***, 0.0001###. GLUC, tissue glucose; LPR, lactate to pyruvate ratio; psctO2, tissue oxygen.
Our next hypothesis was that prolonged (>1 h) fever is associated with more metabolic stress at the injury site than brief (≤ 1 h) fever. Supplementary Figure S2 shows that the duration of each of the three fever types had no impact on ISP or SCPP. However, compared with brief fever, prolonged fever is associated with lower tissue glucose (neurogenic fever), higher LPR (inflammatory and infective fevers), and lower psctO2 (neurogenic, inflammatory, and infective fevers). We conclude that, for all three fever types, prolonged fever is associated with more metabolic stress at the injury site than brief fever.
We then investigated whether the spinal cord metabolic derangement precedes the fever by examining the 5 h before fever onset (Supplementary Fig. S3). Changes in ISP, SCPP, glucose, LPR, and psctO2 before neurogenic or inflammatory fever are no different than during normothermia. However, significant decrease in glucose, significant increase in LPR, and non-significant decrease in psctO2 occur before the onset of infective fever. We conclude that spinal cord metabolic derangement precedes the onset of infective, but not neurogenic or inflammatory, fever by at least 4 h.
Injury site cytokines/chemokines
We asked whether fever is associated with increased cord inflammation, quantified as changes in the levels of cytokines/chemokines at the injury site during fever versus baseline. Figure 4 shows that neurogenic and inflammatory fevers are not associated with significant changes in any assayed cytokines/chemokines, although wide variability between patients is observed. Infective fever is associated with significantly elevated levels of pro-inflammatory cytokines/chemokines (GROα, IL-8, IP-10, MCP-1, MIP-1β), but no significant change in the levels of anti-inflammatory cytokines/chemokines (IL-4, IL-10). These findings suggest that infective, but not neurogenic or inflammatory, fever is associated with increased injury site inflammation.

Cytokines in injured spinal cord during fever. Percentage of change in the levels of GROα, IL-8, IP-10, MCP-1, MIP-1α, MIP-1β, IL-4, and IL-10 in microdialysates collected from the injury site during high fever (≥ 38°C) versus normothermia. Neurogenic (blue), inflammatory (orange), or infective (black) fever. Dots are fever episodes; lines are medians, logarithmic scale; ns, not significant; P < 0.05*, 0.005***.
Neurogenic fever predictor
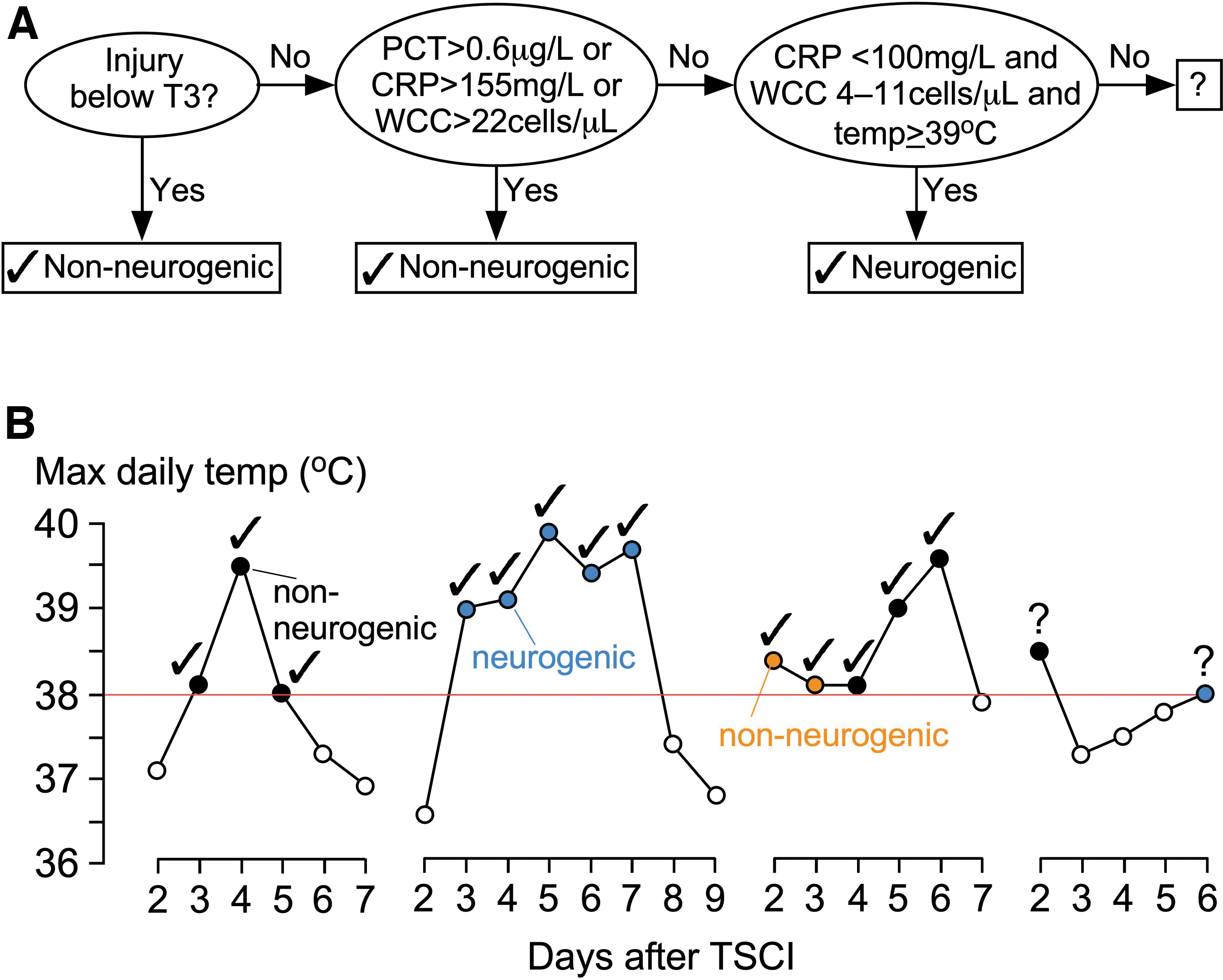
We hypothesised that it is possible to reliably distinguish neurogenic from non-neurogenic high fever by simple clinical tests. Patient characteristics (age, sex, level of injury, severity of injury) and daily fever characteristics (day from injury, maximum temperature, WCC, CRP, PCT) were entered into logistic regression, neural network, tree, stochastic gradient descent, and CN2 rule induction algorithms with accuracy assessed by leave-one-out cross-validation. All classifiers performed well in various evaluation metrics; in general, the classifiers employed five key discriminating features, including level of injury, WCC, CRP, PCT, and maximum daily temperature (Supplementary Fig. S4). Five simple clinical rules, based on these characteristics, allow 59.3% of high fever episodes to be classified with 100% accuracy, as neurogenic or non-neurogenic; the remaining 40.7% high fever episodes cannot be reliably classified (Supplementary Table S1). Figure 5 shows a simple flow chart to distinguish neurogenic from non-neurogenic fever with examples of fever episodes.
Distinguishing neurogenic from non-neurogenic fever.
Discussion
We reported previously that, after acute TSCI, fever (axillary temperature ≥38°C) is associated with cord metabolic stress and impaired neurological recovery. 17 Here, we refined our analysis to show that deranged injury site metabolism is a feature of all three major types of fever (neurogenic, inflammatory, infective) and, therefore, all three types of fever are probably harmful. Infective fever seems the most detrimental to the injured cord because it is also associated with elevated spinal cord levels of pro-inflammatory cytokines/chemokines. The three types of fever have different features that can be exploited to distinguish neurogenic from non-neurogenic fever with confidence.
The following mechanism may explain how fever causes metabolic stress at the injury site. Evidence from patients with TSCI, 7,22 –24 rodents, 25,26 and pigs 27 –29 suggest that the injured cord is ischemic. By increasing the metabolic rate, 30 fever increases glucose and oxygen consumption, which accounts for the reduction in tissue glucose and psctO2 at the injury site that we detected during fever; these changes cannot be explained by reduced cord perfusion because fever does not affect SCPP or ISP. Tissue oxygen depletion during fever then exacerbates cord ischemia evidenced by rising LPR at the injury site. It follows that more prolonged fever is associated with more metabolic stress at the injury site. This mechanism may apply to all types of fever and all CNS ischemic pathologies, for example, fever worsens outcome in patients with TSCI, 31 –35 patients with TBI, 36,37 and rodent TBI models 38,39 ; fever also increases infarct size and mortality, and worsens outcome in patients with stroke. 40,41 Together, these findings suggest that prompt treatment of fever may improve outcome after TSCI.
Unlike other fevers, infective fever is linked to additional harmful effects. Infective fever is associated with elevated spinal cord levels of chemoattractants and activators of leukocytes including GROα and IL-8 (neutrophils 42 ) as well as IP-10, MCP-1, and MIP-1β (microglia, 43,44 macrophages 45 –47 ), without changes in IL-4 or IL-10, which are anti-inflammatory. 48 Neutrophils, microglia, and macrophages are abundant in acutely injured human 24 and rat 49,50 spinal cord; their activation may cause further tissue damage. 51 Our finding that cord metabolic stress precedes the onset of infective fever suggests detrimental factors other than temperature, likely to be leukocytes. The clinical implication is that treating fever without addressing the leukocytes is unlikely to eliminate the detrimental effect of infective fever.
The three types of fever have different characteristics: Temperature: Infective and inflammatory fevers may be mediated by prostaglandins,
52
–54
but neurogenic fever is caused by interruption of thermoregulatory spinal cord pathways.
55
Neurogenic fever is thus poorly responsive to cyclooxygenase inhibition by paracetamol/non-steroidal anti-inflammatory drugs
56
; this may explain why neurogenic fever is higher than non-neurogenic. Time course: Neurogenic fever starts soon after TSCI and peaks at 1 week, likely related to evolving changes within the cord, for example, cord edema. Inflammatory fever is primarily from trauma to other organs/surgery and thus peaks early. Infection takes time to develop, which may explain why infective fever starts >48 h after TSCI. Level of injury: Neurogenic fever is confined to injuries above vertebral level T4. This coincides with the level for temperature dysregulation in chronic TSCI
57
and autonomic dysreflexia.
58
The mechanism of neurogenic fever may be interruption of sympathetic supply to skin (trunk, legs) and internal organs thus disrupting vasoconstriction/dilation, which has a major impact on heat elimination. Alternatively, cervical interneurons (propriospinal neurons), which are major contributors to the plastic reorganization of spinal neuronal circuitry after cervical TSCI, for example, to sustain breathing, may play a role.
59
In contrast, inflammatory and infective fevers are not linked to the level of injury. Peripheral sepsis: Unlike neurogenic fever, infective and inflammatory fevers are associated with more marked peripheral inflammation (higher WCC, CRP, PCT).
The three types of fever have different managements. Infective fever requires source identification and septic screening and is treated with antibiotics but may require additional measures, for example, change of peripheral line or urinary catheter, chest physiotherapy, or surgical lavage. 34,60 Inflammatory fever is multi-factorial, driven by systemic inflammatory response to polytrauma, surgery, venous thromboembolism, or blood transfusion; management is supportive. 61,62 Neurogenic fever, a unique and prominent feature in acute TSCI, is non-inflammatory but difficult to diagnose because of concomitant peripheral inflammation. 63,64 Therefore, neurogenic fever is often managed as infective with unnecessary septic screens and overuse of antibiotics.
We showed that neurogenic fever has simple distinguishing features: TSCI above T4, higher temperature, and less peripheral inflammation (WCC, CRP, PCT). Using these, neurogenic fever can be confidently distinguished from non-neurogenic more than 50% of the time. Early and accurate diagnosis of neurogenic fever may reduce over-investigation and over-treatment with antibiotics that may, in turn, limit the emergence of antibiotic resistance. There is no treatment for neurogenic fever after TSCI; bromocriptine merits investigation, based on reports of its effectiveness in eliminating neurogenic fever after TBI. 65,66 Table 4 compares the pathological basis, diagnosis, and management of infective, inflammatory, and neurogenic fevers in patients with TSCI.
Comparison of the Pathological Basis, Diagnosis, and Management of Infective, Inflammatory, and Neurogenic Fevers in Patients With TSCI
CRP, C-reactive protein; DVT, deep venous thrombosis; NLI, neurological level of injury; NSAID, non-steroidal anti-inflammatory drug; PCT, procalcitonin; TSCI, traumatic spinal cord injury; WCC, white cell count.
Our conclusions are supported by many hours of monitoring, but there are limitations. We show associations, not causality, and thus we cannot prove that treating fever will improve outcome; a randomized, controlled trial is needed. It is also unclear if the cytokines/chemokines are produced locally, for example, by microglia, 67 or enter the cord from the circulation; simultaneous assays using serum and injury site MD may help resolve this. Finally, the method of distinguishing neurogenic from non-neurogenic fever needs external validation. Our patient cohort is typical of the TSCI population with comparable demographics, 68 –70 fever, 16,31,71 complications, 69,72 and outcomes. 69,72,73
This study shows how monitoring from the injured spinal cord may help with clinical management in patients with acute, severe TSCI. Inserting probes intradurally is invasive and can only be done intra-operatively (posterior approach) under direct vision. To date, at St. George's Hospital, we have monitored using one (ISP), 10 two (ISP, MD), 15 or three (ISP, MD, Licox) 7 probes in more than 90 patients with TSCI. The monitoring technique does not increase the risk of neurological deterioration or wound infection, and the long-term neurological outcomes of our patients are comparable to those of other centers. 74
Conclusions
Our study provides evidence that fever may cause secondary damage after acute TSCI and illustrates how injury site monitoring may be used to determine how the spinal cord responds to injury to guide patient management. Further studies are required to determine if treating fever improves neurological outcome.
Transparency, Rigor, and Reproducibility Summary
The study was pre-registered at
Quantitative test-retest reproducibility was not required, because established and validated monitoring techniques in routine clinical use were employed: pressure probe (Codman), tissue oxygen catheter (Licox), MD (Solna, Sweden), and PCT. The test-retest reliability of the clinical outcome measures was not formally determined. Inclusion and exclusion criteria for ISCoPE are listed in the Methods section. The primary outcome measures (tissue glucose, tissue LPR, tissue cytokines, ISP, SCPP, and psctO2) are not yet established standards in the field. AIS assessment is standard in the field. Future validation warrants a randomized control trial comparing groups of patients with TSCI with (1) continuous cord monitoring and perfusion targeted therapy versus (2) non-monitored patients. The other clinical outcome measure, PCT, as a differentiator of fever type is an emerging standard in the field. Normality, homogeneity of variances, and independence were assumed. When not met, non-parametric tests were considered. Adjusting for multiple comparisons was performed using logistic regression. Replication of the monitoring methods and evaluation of the study group was previously validated in an independent TSCI cohort.
De-identified data from this study are not public, however anonymized data, and the manuscript can be made available (subject to institutional ethical standards) by emailing the corresponding author. There is no analytic programming code associated with this study. The authors agree to provide the full content of the manuscript on request by contacting the corresponding author.
Footnotes
Acknowledgments
We thank the neurosurgeons at St. George's Hospital who helped recruit patients. The neuroanesthesia, neuro ICU, and operating theater staff at St. George's Hospital helped with data collection.
Authors' Contributions
The authors contributed as follows. Ravindran Visagan: methodology, formal analysis, investigation, data curation, visualization. Siobhan Kearney: investigation. Christian Blex: investigation. Leonarda Serdani-Neuhaus: investigation. Marcel A. Kopp: investigation, resources, writing–review and editing. Jan M. Schwab: resources, writing–review and editing. Argyro Zoumprouli: methodology, investigation, resources, writing–review and editing, project administration. Marios C. Papadopoulos: conceptualization, methodology, investigation, resources, writing–review and editing, project administration, funding acquisition. Samira Saadoun: conceptualization, methodology, formal analysis, resources, writing–original draft, writing–review and editing, visualization, supervision, project administration, funding acquisition.
Funding Information
Funded was provided by the Wings for Life Spinal Cord Research Foundation (research grant; SS, MCP), Neurosciences Research Foundation (McKissock Fellow; RV), Royal College of Surgeons of England (Research Fellow; RV), and National Institute for Health and Care Research (NIHR) Clinical Research Network (SK).
Author Disclosure Statement
SS and MCP are principal investigators on a Wings for Life research grant awarded to St. George's, University of London. Salary support for RV was from Wings for Life and the Royal College of Surgeons of England. RV was a McKissock research fellow supported by the Neurosciences Research Foundation. The salary for SK was from the NIHR Clinical Research Network.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.