
Abstract
Evaluating large data sets precludes the ability to directly measure individual experiences, instead relying on proxies to infer certain constructs. Blast exposure is a construct of study currently in its infancy, resulting in diverse definitions and measurements across studies. The purpose of the present study was to validate military occupational specialty (MOS) as a proxy for blast exposure in combat veterans. A total of 256 veterans (86.33% male) completed the Salisbury Blast Interview (SBI) and Mid-Atlantic Mental Illness Research Education and Clinical Center (MIRECC) Assessment of Traumatic Brain Injury (MMA-TBI). MOS was collected through record review and categorized into low and high risk for blast exposure. Chi-square analyses and t tests compared SBI metrics between MOS categories. Receiver operating characteristic (ROC) analyses evaluated the diagnostic accuracy of MOS category in determining blast exposure severity. Veterans in high-risk MOS were more likely to have experienced blast and deployment TBI (ps < 0.001) than were those in low-risk MOS. ROC analyses indicated good specificity (81.29–88.00) for blast and deployment TBI outcomes, suggesting that low-risk MOS is generally associated with an absence of blast and deployment TBI outcomes. Sensitivity was low (36.46–51.14), indicating that MOS risk level was not a good predictor of the presence of these outcomes. Results demonstrate that high-risk MOSs will identify individuals with blast exposure and deployment TBI history whereas low-risk MOSs will capture a highly variable group. Accuracy of MOS categorization was not acceptable for diagnostic-level tests; however, results support its use as a screening measure for a history of exposure to blast, use in epidemiological studies, and considerations for military policy.
Introduction
Despite advances in the conceptualization of blast exposure, the ideal way to measure blast exposure has not been established. A recent review 1 highlighted the measures currently available to characterize low-level blast (LLB) (overpressure from outgoing munitions) exposure, most of which are instruments that quantify the frequency of an individual's exposure to specific munitions and occupational events. Though these are effective at estimating potential cumulative exposure to non-concussive overpressure across a military career, these instruments are largely restricted to quantifying frequency of LLB and do not evaluate the overall experience of the blast itself (e.g., characteristics of the exposure) from both LLB and high-level blast (HLB; overpressure as a result of incoming munitions) exposures. Unique from other measures, the Salisbury Blast Interview (SBI) 2 is a comprehensive interview that evaluates lifetime blast exposures, from outgoing munitions to incoming munitions (e.g., improvised explosive devices [IED]). The SBI captures frequency as well as individual experiences of blast, including physical experience (e.g., pressure, wind, debris) of the blast itself and other outcomes resulting from the blast (e.g., lacerations from tertiary exposure). Although it is more comprehensive than the other featured measures, it is not always feasible to include a clinical interview in research studies with time restrictions or direct care provisions.
In contrast to structured clinical interviews, a promising approach to evaluating blast exposure history is the use of military occupational specialty (MOS) (i.e., a service member's job in the military) from existing records to approximate the level of repeated occupational overpressure exposure. 3 Although not specific to individual experiences, using a proxy such as MOS allows for large-scale or population-based investigations into military-related blast exposures that would not be feasible to execute by gathering data prospectively. Because MOS is likely to be present in most databases, including medical records, it is valuable for use with existing large data sets and can thus help address sample bias limitations inherent in studies using other methodologies.
Epidemiological investigations have used MOS as a proxy to investigate the adverse health outcomes associated with LLB. For example, Belding and coworkers (2020) 3 systematically categorized MOS as low, moderate, or high risk of low-level occupational blast exposure, and demonstrated that Marines in a high-risk MOS were more likely to experience a blast during deployment and more likely to sustain a TBI during deployment. 3 The relationship with TBI was similar in an Army cohort 4 and across Services, 5 particularly among Service Members who have spent more time in service and therefore have had more cumulative exposure to LLB. Further, occupational risk of LLB (using MOS as a proxy) has been shown to exacerbate the effects of mild TBI on subsequent symptom presentation. 5 –7
Despite the growing epidemiological evidence of the adverse health outcomes associated with LLB, no publications to date have compared MOS with dedicated interview measures of blast exposure. Further, the use of MOS to infer occupational blast exposure history has not been evaluated in a Veteran cohort. The purpose of the present research was to leverage a detailed and comprehensive assessment that can be conducted on an individual basis to improve understanding of analyses utilizing large operational data sets. First, we evaluated the agreement between MOS risk categorizations derived from available medical records and blast characteristics obtained prospectively from veterans in a research study. Second, diagnostic accuracy was calculated to objectively determine how well MOS classified high- and low-risk blast exposure categories.
Method
Participants
Data from the Chronic Effects of Neurotrauma Consortium Study 34 (CENC-34) were used for the present analyses. The purpose of CENC-34 was to evaluate how primary blast exposure affected the brain and behavior of post-9/11 United States combat Veterans. Inclusion criteria were being ≥18 years of age or deployment to a combat zone after 9/11/2001. Exclusion criteria were: lifetime history of moderate to severe TBI or penetrating brain injury; TBI outside of deployment with loss of consciousness; history of major neurological disorder (e.g., stroke, seizure, spinal cord injury); history of serious mental illness (e.g., bipolar disorder, schizophrenia); current neurocognitive disorder, substance use disorder, or psychosis. Neuroimaging was conducted as part of the broader project and additional exclusion criteria related to these study activities were pregnancy, presence of ferrous metal in the body, and implanted electrical stimulation devices (e.g., pacemaker).
A total of 341 participants were enrolled into the study. After enrollment, 26 participants were determined to have a history of moderate to severe TBI and were excluded from analyses. An additional 47 were excluded for symptom validity failure based on the Structured Inventory of Malingered Symptoms (SIMS 8 ) scores >23. 9 After categorizing participants into risk groups (see MOS classification in the next section), the number of participants in the moderate group was determined to be too low (n = 12) for meaningful analyses. These individuals were removed listwise from the sample. The final sample size for analyses was 256.
Measures
MOS classification and blast risk categorization
MOS was collected from participant military records (e.g., DD Form 214, DD Form 2796/Post Deployment Health Assessment [PDHA]). Participants were categorized into those at low, moderate, or high risk of blast exposure using occupational categorization schemes developed by Belding and coworkers. 3 The highest MOS risk level was retained per participant.
Salisbury Blast Interview
The SBI 2 is a blast interview that characterizes experiences of blast across the lifespan. Information is collected about each blast event, including a narrative, munition, date, distance, environment (e.g., deployment), protective factors (e.g., behind cover), experienced blast characteristics (e.g., pressure, wind, debris), and additional physical injury. Blast events can be paired with a TBI interview if symptoms congruent with a TBI are experienced at the time of a blast. Although several metrics of blast characteristics can be derived from the SBI for analysis, the original investigation 2 identified blast pressure severity as the best predictor of more severe outcomes (e.g., TBI). The most severe reported lifetime blast pressure represented blast exposure severity for the present analyses. This variable is scored on a behaviorally anchored Likert scale from 0 (none) to 5 (strongly, resulted in greater than minor injury).
Mid-Atlantic Mental Illness Research Education and Clinical Center MIRECC Assessment of TBI (MMA-TBI) 10
The MMA-TBI is a structured lifetime TBI interview that determines the presence and severity of TBI across the lifespan. The associated algorithm assigns TBI diagnosis and severity based on the Veterans Administration/Department of Defense (VA/DoD) Clinical Practice Guideline for TBI. 11,12 The MMA-TBI evaluates TBI cause, presence and duration of loss of consciousness, alteration of consciousness, and post-traumatic amnesia, as well as the presence and duration of common post-concussive symptoms (e.g., headache, dizziness, vision problems) following each occurrence. We specifically evaluated deployment TBI for the present analyses because of its salience to outcomes in this population. 13,14 Deployment TBI was represented dichotomously (0 = absent) in analyses and was considered present if a participant had experienced at least one TBI in a deployment environment. Blast TBI was also evaluated as an outcome in analyses and is defined as a deployment TBI caused by primary blast forces.
Combat exposure
Combat exposure was evaluated using the Deployment Risk and Resiliency Inventory part D (DRRI-2-D). The DRRI-2-D is a 17-item measure of exposure to different combat experiences with a total possible score of 17–102. Greater scores represent greater combat exposure.
Post-traumatic stress disorder (PTSD) diagnosis
The Clinician Administered PTSD Scale for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (CAPS-5) was administered to all participants by clinically supervised and trained masters or doctoral level staff. The CAPS-5 informed current and lifetime PTSD diagnosis, represented dichotomously (0 = absent) in analyses.
Statistical analysis
Analyses were conducted in SAS Enterprise Guide version 8.3 and STATA/MP version 17. Sample characteristic analyses were conducted using χ2 or independent samples t tests as indicated. Analyses comparing continuous SBI outcomes between MOS risk levels were conducted with independent samples t tests. The Satterthwaite approximation was used when variances between sample sizes were unequal; the pooled variance was used in all other instances. Diagnostic accuracy was calculated using the roctab procedure in STATA/MP. Criteria included blast exposure (0 = SBI pressure score of 0; 1 = SBI pressure score ≥1) defined as experiencing any pressure severity as a result of a blast, and greater severity blast exposure (0 = SBI pressure score 0–2; 1 = SBI pressure score ≥3) defined as experiencing a blast with a pressure gradient that resulted in minor pain or alteration in function (SBI pressure score = 3) to resulted in greater than minor injury (SBI pressure score = 5).
Results
Descriptive information about the sample and measures is presented in Table 1. Participants were 256 combat Veterans, 86.33% male (n = 221) between the ages of 23-71, mean (M) = 41.56, standard deviation (SD) = 10.00, who deployed in support of the wars in Iraq and Afghanistan. Most participants were white (n = 150, 58.59%) or black (n = 96, 37.50%) United States Army (n = 182, 71.09%) veterans. Average number (M) of total deployments was 2.73 (SD = 3.66, range = 1–50), and time since most recent combat deployment was M = 9.76 years (SD = 3.53, range = 1.25–16.70). Most participants (n = 181, 70.70%) experienced at least one blast with some detectable pressure gradient (SBI pressure scale ≥1). Most participants in the sample had an MOS that was categorized as low-risk, n = 181, 70.70%. The most common MOS among the sample was 88M (transportation; n = 27), followed by 11B (infantry; n = 14) and 91W (expeditionary medical services; n = 11).
Sample Characteristics (n = 256)
Categories are not mutually exclusive.
P values are provided from χ2 analyses or independent samples t tests. Combat exposure is represented by the total score of the Deployment Risk and Resiliency Inventory, Second Edition, Section D (DRRI-2-D); Blast exposed is positive if subject experienced a blast with pressure of ≥1. Greater severity blast exposed is positive if subject experienced a blast with pressure of ≥3. MOS, military occupational specialty; M, mean; SD, standard deviation; TBI, traumatic brain injury; deployment TBI, history of experiencing a TBI during a deployment; blast TBI, deployment TBI caused by primary blast forces; PTSD, post-traumatic stress disorder.
Characteristics of blast by MOS risk
Analyses comparing MOS risk levels across primary SBI outcomes and self-reported symptom outcomes are presented in Table 2. There were significant differences between MOS levels across all metrics of blast severity. Specifically, the high-risk MOS group had greater mean scores for highest wind (p = 0.002), debris (p < 0.001), pressure (p < 0.001; see Fig. 1), temperature (p = 0.001), ground shaking (p < 0.001), sound (p < .001), and shorter minimum distance from a blast (p < 0.001) than the low-risk MOS group. There were no differences between MOS levels for metrics of blast frequency (i.e., number of blasts with pressure ≥1; number of blasts with pressure ≥3). Comparisons across MOS categories indicated a higher likelihood of having experienced a blast (p < 0.001), greater severity blast (p < 0.001), deployment TBI (p < 0.001), and blast TBI (p < 0.001) in the high-risk MOS category. Notably, of the 75 individuals in the high-risk MOS category who experienced greater severity blast, only 44 (58.67%) reported a greater-severity blast occurring during combat.

Maximum blast exposure by military occupational specialty (MOS) risk group. The percentage of participants reporting each maximum blast exposure rating by MOS risk category. Maximum blast exposure severity rating is represented by Salisbury Blast Interview (SBI) maximum pressure rating (0 = unexposed).
MOS Risk Level Comparison on SBI Blast Characteristics (n = 256)
Blast and traumatic brain injuries (TBI) characteristics are from ratings on the Salisbury Blast Interview (SBI). Frequency 0 pressure refers to the absence of exposure to blast or number of exposures to blast in which no pressure was felt. Frequency ≥1 pressure and frequency ≥3 pressure refer to the total number of lifetime blast exposures in which the pressure felt met or exceeded the specified threshold.
Degrees of freedom (df) adjusted per Satterthwaite approach used because unequal variances.
MOS, military occupational specialty; M, mean; SD, standard deviation.
Diagnostic accuracy of MOS risk
Results of the diagnostic accuracy analysis evaluating sensitivity and specificity of MOS categories predicting experienced blast and TBI are presented in Table 3. Specificity levels for blast and TBI outcomes were relatively high, suggesting that being in a low-risk MOS is generally associated with an absence of the criteria examined. However, sensitivity levels for these outcomes were relatively low, indicating that MOS risk level was not a good predictor of the presence of these outcomes (see Fig. 2). The mix of higher specificity and lower sensitivity is reflected in generally low area under the curve (AUC) values.
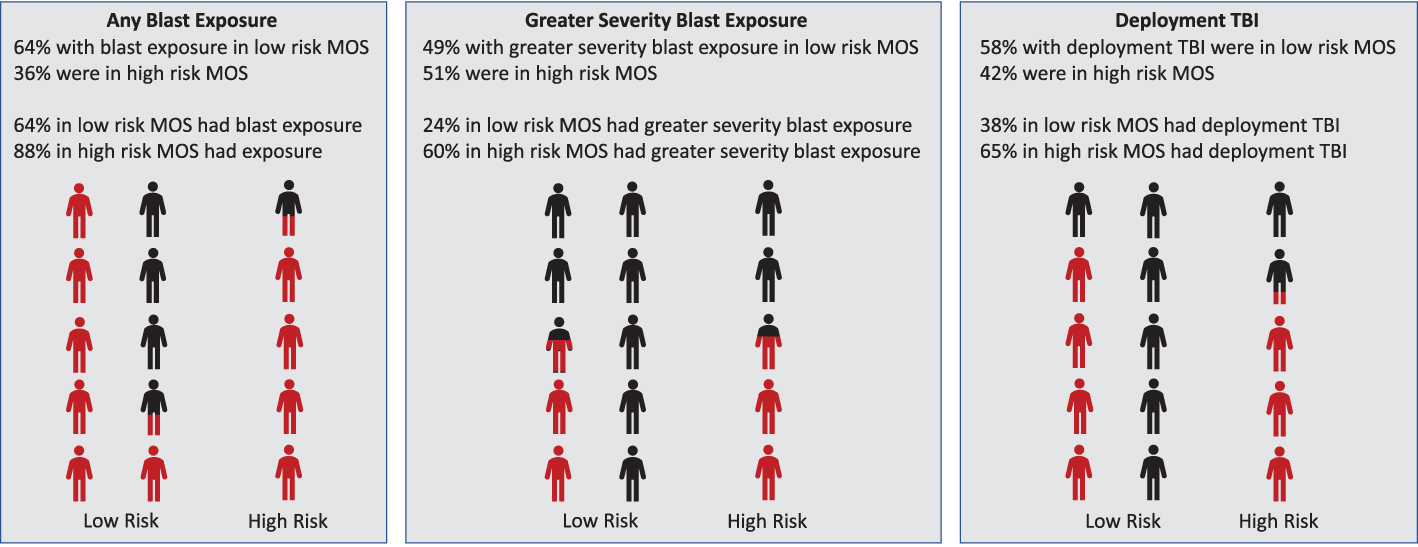
Illustration of receiver operating characteristic (ROC) analyses demonstrating proportions across military occupational specialty (MOS) categories. Red color indicates positive cases. High risk MOS categories consisted of a higher proportion of individuals with any (pressure ≥1) or greater (pressure ≥3) severity blast exposure or deployment traumatic brain injury (TBI) history; however, this did not capture all individuals with blast exposure or deployment TBI history. Low risk MOS categories contained most individuals without a history of blast exposure or deployment TBI history, but were also composed of a large proportion of individuals who did have blast exposure or TBI history.
Diagnostic Accuracy of MOS Risk Level for Military-Relevant Outcomes (n = 256)
Blast exposed = Salisbury Blast Interview (SBI) pressure rating ≥1; blast exposed severe = SBI pressure rating ≥3. Traumatic brain injury (TBI) diagnosis and mechanism were determined using the Mid-Atlantic Mental Illness Research Education and Clinical Center (MIRECC) Assessment of Traumatic Brain Injury (MMA-TBI). Post-traumatic stress disorder (PTSD) diagnosis (lifetime) was determined using the Clinician Administered PTSD Scale for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (CAPS-5).
MOS, military occupational specialty; AUC, area under the curve.
Post-hoc analyses
To probe the low sensitivity outcome (i.e., heterogeneity in the low-risk MOS group), we compared deployment characteristics of low/no (i.e., blast pressure 0–2) and high (i.e., blast pressure 3–5) blast pressure groups within the low-risk MOS group. Specifically, we wanted to determine if greater opportunity to be exposed to blast explained the heterogeneity within the low-risk MOS group. Independent samples t tests were conducted to evaluate differences in (1) total number of deployments and (2) total months deployed across deployments. Although low-risk MOS individuals with more severe blast exposure had a greater average number of deployments (M = 3.52, SD = 7.30) and a greater average total months deployed (M = 21.84, SD = 11.57) than the low/no blast exposure group (M = 2.63, SD = 2.51; M = 20.86, SD = 13.89, respectively), these differences were not significant between groups (p = 0.429, p = 0.673, respectively).
Discussion
Despite growing recognition of the adverse outcomes associated with blast exposure among military personnel in training and operational environments, much work still needs to be done to improve methods to assess blast exposure for research and operations purposes. A variety of methods to measure blast exposure are necessary for robust analyses using different study designs (e.g., epidemiological studies of archival data, survey-based studies, imaging studies), yet no study to date has directly compared different methods. The present research sought to fill this gap by comparing MOS (which has been used as a proxy for blast exposure in population-based epidemiological studies) with blast exposure identified by the SBI (a structured interview administered by trained clinical providers). Broadly speaking, two key findings emerged: first, the SBI validated MOS as a proxy for blast exposure; and second, MOS is a specific but not a sensitive measure of blast exposure and TBI history.
Research on the adverse outcomes associated with LLB was reinvigorated in the early 2000s following reports from service members, particularly instructors at certain training programs (e.g., breaching), describing neurological symptoms following chronic exposure to certain weapon systems. 15 –17 To address limitations associated with small sample size when surveilling exposures sustained in these training courses, 15 epidemiological research on LLB using archival population-level databases commenced and relied on MOS as a proxy for LLB based on the idea that the use of certain weapon systems would be more likely among warfighters in some occupations compared with others. 3 –7 Although previous research suggests associations between MOS and blast exposure, 18 no research to date has directly compared MOS as a proxy with other methods to assess blast exposure (e.g., structured interviews). The current project extends previous findings by using structured clinical interviews to evaluate blast and TBI history, which allows for a comprehensive individualized history of blast and TBI to be compared with MOS risk levels.
Results confirmed the hypothesis that service members working in high-risk occupations were, in structured interviews, more likely to report exposure to blast. Although findings did not show differences in frequency of exposure to blast as a function of occupational risk of blast exposure, findings reported herein suggest that those who worked in high-risk occupations were significantly more likely to report closer physical proximity to the blast origin and corresponding metrics of intensity (e.g., wind, debris). Further, those who worked in high-risk MOSs were more likely to report deployment-related mild TBI, congruent with previous research evaluating TBI screens in the medical record. 3 –5 However, it is important to reiterate that just over half (58.6%) of these individuals reported greater severity blast during combat, which highlights the overall risk of blast exposure associated with other occupational duties. Together, these results replicate epidemiological findings documenting adverse outcomes of occupational risk of LLB exposure using a more precise measure of blast exposure.
The second aim of the present research was to identify the sensitivity and specificity of MOS as an indicator of blast exposure. Findings suggest that specificity of MOS risk categories was adequate for both TBI and blast histories. Individuals who were not blast exposed or did not have deployment TBI history were primarily in the low-risk category, as expected. However, sensitivity levels of the MOS categories were lower than expected, indicating that the number of individuals who were positive for greater severity blast exposure or TBI history tended to be similar across risk categories. This is because of differences in the size of the MOS risk categories (i.e., a greater number of participants worked in low versus high-risk occupations). Similar discrepancies occur for the other blast exposure and TBI history groups. The difference in proportion drives statistical differences between groups, but the higher number of individuals in the low-risk MOS category reduces sensitivity. This is congruent with recent work that indicates homogeneity within occupations for LLB, but significant heterogeneity for HLB within occupations that may differ as a result of unique experiences during deployment. 18
These results support the use of MOS risk categories as an indicator of blast exposure history in large data sets as well as in consideration for potential policy recommendations, and have clear implications to guide future use and interpretation. For example, high-risk MOS categories will consist of a high proportion of individuals with blast exposure or deployment TBI history; however, this does not capture all individuals with blast exposure or deployment TBI history. In addition, the blast exposure experienced by individuals in high-risk MOS is more likely to be of a higher severity than that experienced by individuals in low-risk MOS. In contrast, low-risk MOS categories will contain the vast majority of individuals without a history of blast exposure or deployment TBI history but will also contain a large proportion of those individuals who do have blast exposure or TBI history. Understanding how deployment TBI and blast exposure history vary across MOS risk categories will improve interpretation of analyses based on these categorizations. Although the data for these analyses may be limited in representativeness to the broader military population, these results suggest that, among service members who deploy to a combat zone, protective measures implemented for high-risk MOS categories will primarily affect individuals likely to experience blast exposure. However, this will represent less than half of those individuals who will actually experience blast exposure. In contrast, implementing protective measures in low-risk MOS categories will primarily affect individuals unlikely to experience blast exposure.
These results also raise important questions regarding how outcomes of blast exposure and TBI may differ across risk categories. The difference in severity of blast exposure suggests the possibility that differences in actual blast characteristics may result in poorer outcomes for individuals in high-risk MOS. The severity of blast exposure has previously been shown to be associated with increased psychiatric symptom report, higher likelihood of TBI, poorer cognitive performance, and alterations to brain structure and function. 2,19 –24 In addition, blast exposure is frequently a traumatic experience when it results from combat exposure to enemy munitions. Individuals in high-risk MOS may be better prepared for these experiences than individuals in low-risk MOS. This difference in preparedness could result in differences in outcomes based on the traumatic nature of the experience (e.g., increased post-traumatic stress responses). Exploratory analyses in this sample indicated that deployment duration and/or number of deployments, and therefore greater opportunity for blast exposure, did not explain the heterogeneity in the low-risk MOS group. Further research is needed to fully understand the potential interactions among MOS risk level, blast exposure, and functional outcomes for service members and veterans.
These findings should be considered in the context of several limitations. First, the SBI evaluates blast regardless of whether the blast exposure sustained is the result of incoming or outgoing munitions (i.e., HLB or LLB). Whereas MOS is presumed to be a proxy for LLB only, the SBI measures both HLB and LLB. Therefore, findings cannot be attributed purely to LLB. Future work will be necessary to determine the exact relationship between MOS categories and LLB/HLB exposure. An evaluation of incoming versus outgoing exposures or the inclusion of a measure of strictly occupational exposures such as the Blast Exposure Threshold Survey (BETS) 25 or Blast Ordnance and Occupational Exposure Measure (BOOM) 26 may be helpful. Second, the current sample was composed primarily of veterans enrolled, on average, a decade after a combat deployment. These considerations may affect interpretation of the results.
Conclusion
The presented research validated the use of MOS as a proxy for blast exposure and demonstrated an association with TBI history. Using structured clinical interviews conducted with a sample of combat Veterans, results highlighted that high-risk MOSs will likely capture a subgroup of individuals with blast exposure and TBI history. Conversely, low-risk MOS will likely capture a large proportion of individuals without blast exposure or TBI history, but this group will also include a proportion of individuals with such history, creating a highly variable group. The current study suggests that the accuracy of MOS categorization does not reach levels considered acceptable for diagnostic tests; however, these results do support its use as a screening measure for a history of exposure to blast and therefore potentially to TBI, as well as for use in epidemiological studies and considerations for military policy.
Transparency, Rigor, and Reproducibility Summary
This is a cross-sectional observational study. This study was not formally registered. Because this is a secondary analysis, the analysis plan was not formally pre-registered. Sample was composed of 341 human subjects ≥18 years of age who experienced combat during a military deployment as measured by the DRRI-2 section D. Participants were enrolled between March 2016 and March 2019. A total of 803 potential participants were screened, 341 were enrolled, and adequate data were obtained from 338. Participants were excluded from present analyses if they had a history of greater than mild TBI or did not pass symptom validity screening. The number of participants in the moderate risk MOS group was determined to be too low for meaningful analyses. These individuals were removed listwise from the sample. Actual sample size for analyses was 256 subjects with 75 in the high-risk MOS group and 181 in the low-risk MOS group. Participants completed all procedures, including providing informed consent and self-report measures, undergoing neuropsychological assessment, and participating in validated diagnostic clinical interviews. Interviews and neuropsychological assessment were conducted by trained masters- or doctoral-level staff under direct supervision of doctoral level neuropsychologists, with ongoing consultation. Self-report measures were collected using an electronic data capture system with alerts for missing or incorrect data (e.g., out of range). There was no therapeutic intervention as part of this study. De-identified data from this study are available in the Federal Interagency Traumatic Brain Injury Research (FITBIR) Informatics System (
Footnotes
Acknowledgments
We thank the Veterans and Service Members who participated in this research. We also thank Mary Peoples, David J. Curry, MSW, Alana M. Higgins, MA, Christine Sortino, MS, and G. Melissa Evans, MA, for their contributions to this project.
Authors' Contributions
Sarah Martindale was responsible for conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing – original draft, and writing – review & editing; Jennifer Belding was responsible for conceptualization, methodology, writing – original draft, and writing – review & editing; Cameron Crawford was responsible for data curation, writing – original draft, and writing – review & editing; and Jared Rowland was responsible for conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing – original draft, and writing – review & editing.
Please contact the corresponding author for a comprehensive list of publications from the present study.
Disclaimer
The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as representing an official United States Department of Veterans Affairs or United States Department of Defense position, policy, or decision, unless so designated by other official documentation.
Study Protocol
The study protocol was approved by the W.G. (Bill) Hefner VA Healthcare System Institutional Review Board in compliance with all applicable federal regulations governing the protection of human subjects. Research data were derived from an approved W.G. (Bill) Hefner VA Healthcare System Institutional Review Board protocol, number #15-008.
Naval Health Research Center (NHRC) Disclaimer/Jennifer Belding
I am a military service member or employee of the United States government. This work was prepared as part of my official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the United States government. Title 17, U.S.C. §101 defines a United States government work as work prepared by a military service member or employee of the United States government as part of that person's official duties. This work was supported by the United States Army Medical Research and Materiel Command under work unit no. 1518. The views expressed in this work are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States government.
Funding Information
This work was supported by grant funding from Department of Defense, Chronic Effects of Neurotrauma Consortium (CENC) Award W81XWH-13-2-0095 and Department of Veterans Affairs CENC Award I01 CX001135. This work was also supported by resources of the Salisbury Veterans Affairs Medical Center and the Mid-Atlantic Mental Illness Research Education and Clinical Center (MIRECC).
Author Disclosure Statement
No competing financial interests exist.