
Abstract
Emerging evidence suggests that advanced neuroimaging modalities such as arterial spin labelling (ASL) might have prognostic utility for pediatric concussion. This study aimed to: 1) examine group differences in global and regional brain perfusion in youth with concussion or orthopedic injury (OI) at 72 h and 4 weeks post-injury; 2) examine patterns of abnormal brain perfusion within both groups and their recovery; 3) investigate the association between perfusion and symptom burden within concussed and OI youths at both time-points; and 4) explore perfusion between symptomatic and asymptomatic concussed and OI youths. Youths ages 10.00-17.99 years presenting to the emergency department with an acute concussion or OI were enrolled. ASL-magnetic resonance imaging scans were conducted at 72 h and 4 weeks post-injury to measure brain perfusion, along with completion of the Health Behavior Inventory (HBI) to measure symptoms. Abnormal perfusion clusters were identified using voxel-based z-score analysis at each visit. First, mixed analyses of covariance (ANCOVAs) investigated the Group*Time interaction on global and regional perfusion. Post hoc region of interest (ROI) analyses were performed on significant regions. Second, within-group generalized estimating equations investigated the recovery of abnormal perfusion at an individual level. Third, multiple regressions at each time-point examined the association between HBI and regional perfusion, and between HBI and abnormal perfusion volumes within the concussion group. Fourth, whole–brain one-way ANCOVAs explored differences in regional and abnormal perfusion based on symptomatic status (symptomatic vs. asymptomatic) and OIs at each time-point. A total of 70 youths with a concussion [median age (interquartile range; IQR) = 12.70 (11.67-14.35), 47.1% female] and 29 with an OI [median age (IQR) = 12.05 (11.18-13.89), 41.4% female] were included. Although no Group effect was found in global perfusion, the concussion group showed greater adjusted perfusion within the anterior cingulate cortex/middle frontal gyrus (MFG) and right MFG compared with the OI group across time-points (ps ≤ 0.004). The concussion group showed lower perfusion within the right superior temporal gyrus at both time-points and bilateral occipital gyrus at 4 weeks, (ps ≤ 0.006). The number of hypoperfused clusters was increased at 72 h compared with 4 weeks in the concussion youths (p < 0.001), but not in the OIs. Moreover, Group moderated the HBI-perfusion association within the left precuneus and superior frontal gyrus at both time-points, (ps ≤ 0.001). No association was found between HBI and abnormal perfusion volume within the concussion group at any visits. At 4 weeks, the symptomatic sub-group (n = 10) showed lower adjusted perfusion within the right cerebellum and lingual gyrus, while the asymptomatic sub-group (n = 59) showed lower adjusted perfusion within the left calcarine, but greater perfusion within the left medial orbitofrontal cortex, right middle frontal gyrus, and bilateral caudate compared with OIs. Yet, no group differences were observed in the number of abnormal perfusion clusters or volumes at any visit. The present study suggests that symptoms may be associated with changes in regional perfusion, but not abnormal perfusion levels.
Introduction
Pediatric concussion is a serious health concern, as up to 35% of children experience persisting symptoms after concussion (PSAC) beyond 1 month after the injury. 1,2 These symptoms include somatic, physical, emotional, and sleep symptoms, which can significantly impact normal activities and quality of life. 3 The pathophysiology underpinning concussion recovery and symptom resolution is not fully understood; however, emerging evidence suggests that advanced neuroimaging modalities may have prognostic utility for pediatric concussion, one of which is arterial spin labeling (ASL). ASL is a non-invasive magnetic resonance imaging (MRI) technique that measures perfusion without the need for the injection of contrast agents. 4 ASL is quantitative and reproducible, and therefore is particularly suitable for longitudinal study designs. Brain perfusion has been suggested as a possible biomarker of concussion 5 ; however, there is still limited research on longitudinal changes in perfusion from acute (< 72 h) to subacute stages (e.g., 4 weeks) and how these changes relate to symptom presentation (as highlighted by a recent systematic review). 6
Brain perfusion alterations are well documented in more severe traumatic brain injuries (TBIs) and animal models, 7,8 but are not well described in concussions and less so in pediatric patients with PSAC. In moderate-to-severe forms of TBI, hypoperfusion is observed on the first day, followed by a 1- to 3-day period of hyperemia (i.e., hyperperfusion), then another hypoperfusion phase that lasts days to weeks. 9,10 Studies using ASL following concussions, especially pediatric concussions, are limited but generally suggest hypoperfusion in the acute stage (i.e., ≤72 h of injury). 11 –15
Symptoms are assumed to indirectly reflect the pathophysiological changes that occur in the brain following concussion, yet limited research has examined the association between symptoms and the neurobiological mechanisms of concussion. Some studies have found no associations between global perfusion and symptom severity within 7 days of injury 16 or on Day 13 post-injury in adults. 17 or between regional perfusion and symptom severity months to years post-concussion in pediatrics. 11,18 A recent study has not observed differences in global gray and white matter perfusion between symptomatic and asymptomatic children at 2 weeks post-concussion. 19 On the contrary, other studies have found an association between regional and global brain perfusion and symptom severity within a week 20 and a month post-injury in adults, 14 and in children and adolescents at 1 month post-injury. 21 Specifically, children and adolescents who remained symptomatic at 1 month post-concussion had significantly increased brain perfusion when compared with those who clinically recovered from their concussion and healthy controls. 21
In contrast, asymptomatic concussed children and adolescents had lower brain perfusion when compared with healthy controls. 21 A follow-up study including only children and adolescents with PSAC showed significant differences in global perfusion at 1 month post-concussion in those who recovered by 8-to-10-weeks compared with those who failed to recover. 18 Overall, these studies suggest that youth differed significantly in their brain perfusion patterns depending on their symptom recovery trajectories.
Importantly, previous studies examining brain perfusion post-concussion lack prospective or longitudinal data, 11,16,20 –23 have small sample sizes, 12,14 –16,23,24 focus only on sport-related concussions 12,15,16,18,20,22,24 and adult samples, 14 –16,18,20,22,23 have no, small, or inadequate comparison groups, 12,15,16,18,20,22 –24 or do not control for important covariables such as age and sex. 11,23 Moreover, existing ASL concussion studies focus on group differences rather than the single-subject level, assuming that abnormalities consistently manifest in the same brain regions (i.e., high spatial overlap). As such, traditional neuroimaging analyses such as voxel-wise and region of interest (ROI) analyses may not sufficiently account for the heterogeneous nature of concussive injuries or accurately assess recovery. 25 Incorporating subject-specific abnormalities analyses can complement traditional approaches and offer additional insights into neural correlates of concussion. Finally, some of these studies 18,21,24 examining brain perfusion and symptomatic status have used methods to classify symptomatic and asymptomatic participants that overestimate PSAC prevalence. 26 -28 Given the limited data and discrepancies of ASL findings, research investigating the longitudinal changes of brain perfusion from the acute to subacute stages of concussion and their relation to symptoms in pediatric samples is needed to shed light on the neuropathological underpinnings of poor concussion outcomes.
The primary objective of this study was threefold: 1) examine brain perfusion changes, both globally and regionally, in youth with a concussion compared with youth with an orthopedic injury (OI) at 72 h and 4 weeks post-injury; 2) examine patterns of abnormal brain perfusion (i.e., number of clusters of abnormal hyperperfusion and hypoperfusion, and corresponding perfusion volumes) in both groups at 72 h and 4 weeks post-injury; and 3) investigate the association between brain perfusion and symptom burden within concussed youth with a concussion and with an OI at 72 h and 4 weeks post-injury. We hypothesized that those with a concussion would show decreased brain perfusion in the acute phase and increased perfusion in the subacute phase relative to those with an OI. We also hypothesized that both adjusted regional brain perfusion at a group level and abnormal brain perfusion at an individual level would be associated with symptom burden. The secondary objective was to compare brain perfusion patterns in symptomatic concussed participants, asymptomatic concussed participants, and OIs at 72 h and 4 weeks post-injury. We hypothesized that youth with ongoing concussion symptoms would show distinct brain perfusion patterns compared with both those clinically recovered (i.e., asymptomatic) from their concussion and those with an OI.
Methods
Study design and setting
This study is a planned secondary analysis of the randomized clinical trial Pediatric Concussion Assessment of Rest and Exertion+MRI (PedCARE+MRI) completed at CHEO from May 2018 to February 2020, an adjunct study to the PedCARE study. 29,30 CHEO's Research Ethics Board approved this study. The primary objective of the PedCARE+MRI study was to investigate whether early resumption of physical activity at 72 h post-concussion would lead to improved neurophysiological outcomes. During their emergency department (ED) visit, participants with a concussion were randomized into two groups: 1) early resumption of physical activity; 2) rest until asymptomatic. Before conducting statistical analyses for the present study, the two randomization groups were compared on the amount of moderate-to-vigorous physical activity completed within the first 2 weeks of concussion. Similar to previous work, 30 randomization groups showed similar physical activity patterns and thus were combined for the current analysis. See the Supplementary Materials for details. Comparison group participants, who sustained an OI, were also recruited but not randomized to either treatment group. The OI group served only as an observational comparison group for the neuroimaging component.
Inclusion and exclusion criteria
Concussion Group
Patients ages 10.00-17.99 years presenting to the ED within 48 h of a head injury and diagnosed with a concussion according to the Berlin consensus statement definition 31 were invited to participate. The concussion diagnosis was confirmed using physician judgment and an adapted version of the Centers for Disease Control and Prevention tiered framework. 32 At least one symptom from the “highest level of certainty” tier had to be present (e.g., dazed/confused/foggy, loss of consciousness, memory problems), or at least two from the “higher level of certainty” tier (e.g., nausea or vomiting, headache, vision changes, etc. immediately or within an hour post-injury).
Exclusion criteria were: 1) not fluent in English; 2) Glasgow Coma Scale score ≤13; 3) any abnormal neuroimaging findings, including positive head computed tomography (CT) findings (neuroimaging was not required, but may have been performed when clinically indicated); 4) required neurosurgery, intubation or intensive care; 5) multi-system injuries with treatment that required hospital admission, operating room, or procedural sedation in the ED (hospital admission for observation or management of ongoing concussion symptoms was not exclusionary); 6) severe pre-existing neurological condition preventing adequate communication; 7) intoxication in the ED; 8) no clear history of trauma as primary event (e.g., seizure, syncope, or migraine); 9) inability to resume physical activity; 10) inability to obtain consent or assent or if a legal guardian was not present; 11) previous neurological or neurodevelopmental disorder such as epilepsy, intellectual disorder/mental retardation, autism (history of attention deficit hyperactivity disorder, learning disability, or Tourette's syndrome was not exclusionary); 12) intoxication at time of ED or MRI presentation as per clinician or research assistant judgment; 13) previous hospitalization for psychiatric disorders; 14) administration of sedation medication prior to or during ED visit (e.g., propofol, ketamine, nitrous oxide, midazolam, benzodiazepines, fentanyl); 15) inability to be present at the 72 h (± 48 h) and 4 weeks (± 5 days) MRI follow-ups; and 16) MRI contraindications (e.g., pregnancy, pacemakers, metal implants, dental braces/spacers, claustrophobia).
OI Group
Patients ages 10.00-17.99 years presenting to the ED within 48 h of an isolated upper extremity injury due to blunt force or physical trauma (e.g., sprain, fracture, strain) that may require immobilization constituted the OI group. Exclusion criteria were the same as for the concussion group and included 1) closed reduction procedural sedation required; 2) surgical management; and 3) history of concussion or traumatic brain injury within the previous year. OI participants were also screened for concussion during the ED visit.
Concussion Group
Patients ages 10.00-17.99 years presenting to the ED within 48 h of a head injury and diagnosed with a concussion according to the Berlin consensus statement definition 31 were invited to participate. The concussion diagnosis was confirmed using physician judgment and an adapted version of the Centers for Disease Control and Prevention tiered framework. 32 At least one symptom from the “highest level of certainty” tier had to be present (e.g., dazed/confused/foggy, loss of consciousness, memory problems), or at least two from the “higher level of certainty” tier (e.g., nausea or vomiting, headache, vision changes, etc. immediately or within an hour post-injury).
Exclusion criteria were: 1) not fluent in English; 2) Glasgow Coma Scale score ≤13; 3) any abnormal neuroimaging findings, including positive head CT findings (neuroimaging was not required, but may have been performed when clinically indicated); 4) required neurosurgery, intubation or intensive care; 5) multi-system injuries with treatment that required hospital admission, operating room, or procedural sedation in the ED (hospital admission for observation or management of ongoing concussion symptoms was not exclusionary); 6) severe pre-existing neurological condition preventing adequate communication; 7) intoxication in the ED; 8) no clear history of trauma as primary event (e.g., seizure, syncope, or migraine); 9) inability to resume physical activity; 10) inability to obtain consent or assent or if a legal guardian was not present; 11) previous neurological or neurodevelopmental disorder such as epilepsy, intellectual disorder/mental retardation, autism (history of attention deficit hyperactivity disorder, learning disability, or Tourette's syndrome was not exclusionary); 12) intoxication at time of ED or MRI presentation as per clinician or RA judgment; 13) previous hospitalization for psychiatric disorders; 14) administration of sedation medication prior to or during ED visit (e.g., propofol, ketamine, nitrous oxide, midazolam, benzodiazepines, fentanyl); 15) inability to be present at the 72 h (± 48 h) and 4 weeks (± 5 days) MRI follow-ups; and 16) MRI contraindications (e.g., pregnancy, pacemakers, metal implants, dental braces/spacers, claustrophobia).
OI Group
Patients ages 10.00-17.99 years presenting to the ED within 48 h of an isolated upper extremity injury due to blunt force or physical trauma (e.g., sprain, fracture, strain) that may require immobilization constituted the OI group. Exclusion criteria were the same as for the concussion group and included 1) closed reduction procedural sedation required; 2) surgical management; 3) history of concussion or traumatic brain injury within the previous year. OI participants were also screened for concussion during the ED visit.
Outcome measures
MRI acquisition
Acquisition of the MRI scans took place at 72 ± 48 h post-injury (Time 1) and 4 weeks ±5 days post-injury (Time 2). Participants were scanned at the Brain Imaging Centre at the Royal Ottawa Mental Health Centre on a 3 Tesla MRI system (Magnetom Biograph mMR, Siemens, Erlangen, Germany) using a standard 12-channel head receiver coil. Structural scanning included three-dimensional T1-weighted Multi-Echo Magnetization Prepared Rapid Acquisition Gradient Echo imaging (MEMPRAGE) 33 : inversion time (TI)/echo time (TE)/repetition time (TR) = 1160/2.21;4.09;5.97;7.85/2300 msec, flip angle (FA) = 8°, 192 transversal slices with field of view (FOV) = 230 × 230 mm, 256 × 256 pixel matrix, 1 mm slice thickness, 0.9 × 0.9 mm in-plane resolution, with bandwidth (BW) = 650 Hertz per pixel (Hz/px) for all four contrasts.
ASL was performed using a 3D GRASE pulsed ASL (PASL) sequence with FAIR QII (Quantitative Imaging of Perfusion using multi-inversions) and background suppression pulses. The following parameters were applied: resolution: 1.8 × 1.8 × 5.0 mm; slices = 28, slice thickness of 5 mm; FOV = 230 × 230 mm2; TR = 4600 msec; TE = 15.56 msec; bolus = 700 msec; 12 inversion time (msec) = 860, 1060, 1260, 1460, 1660, 1860, 2060, 2260, 2460, 2660, 2860, 3060; averages = 1. The ASL sequence was 5 min and 37 sec. Subsequently a single calibration image and 12 tag-control image pairs were acquired (acquisition time = 54 sec).
Symptoms assessment
Pre-injury and post-injury (ED, 72 h, and 4 weeks) symptoms were measured using the Health and Behavior Inventory (HBI; post-injury symptoms) and retrospective HBI (pre-injury symptoms). 34 The HBI is a 20-item self-report questionnaire rated on a 4-point rating scale based on how often a symptom was experienced in the previous week (0 = not at all/never, 3 = a lot/often; range = 0-60; higher scores reflect greater symptom burden). The retrospective HBI is similar in structure to the HBI and is completed by a parent/guardian. The HBI is a validated and reliable assessment for children and adolescents, 34,35 and is recommended as a common data element for concussion by the National Institutes of Health. 36 Symptoms were assessed two ways: symptom burden (post-concussion HBI total score) and symptomatic status (symptomatic vs. asymptomatic). Symptomatic status at each visit was determined by reliable change z-scores, using the following formula: 26
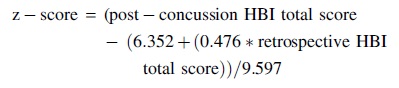
For the present study, z-scores ≥1.28 (>10th percentile) were considered as a significantly greater-than-expected increase in symptom burden post-concussion relative to retrospective ratings (i.e., symptomatic).
MRI data processing
The MRI data were assessed using FMRIB Software Library v6.0 (FSL), 37 Statistical Parametric Mapping 12 (SPM12) software, 38 Matlab 2016a (The MathWorks Inc., United States) and R version 4.1.3. 39 Structural scans were individually reviewed for motion, using the methods described by Backhausen and colleagues. 40 Image sharpness, ringing, contrast-to-noise ratio of subcortical structures, and contrast-to-noise ratio of gray matter and white matter were all taken into consideration. Images were given a pass or fail rating: any scans that failed were automatically excluded. Scans were also excluded if a radiologist determined that significant incidental findings were present (e.g., tumor).
Weighted perfusion was reviewed for motion artifacts and to ensure adequate contrast from gray and white matter. Analysis of Functional Neuroimages (AFNI) 3dvolreg command 41 was used to assess motion in the ASL data before and after motion correction. Motion correction was performed using mcflirt 37 on both the calibration and ASL data. Framewise displacement (FD) calculations, 42 involving the combination of six different head motion parameters, were conducted to yield a single scalar value for participants head motion. The decision to exclude participants based on motion considered both motion correction using mcflirt 37 and visual inspection of the ASL and structural images.
The structural and ASL data was processed using FSL. 37 Reorientation, cropping, bias-field correction, registration to standard space, brain extraction, tissue-type segmentation, and subcortical structure segmentation were all performed on the structural images using the fsl_anat command. 37 Voxel-wise perfusion estimates were calculated in units of mL/100 g/min from the mean difference of all tag–control pairs, using a kinetic modeling approach from FSL oxford_ASL toolbox. 43 The perfusion images were co-registered into a common template space by computing the rigid-body transform of each participant's mean functional volume to their T1 image coupled with a non-linear registration of the structural image to the MNI152 template.
z-score maps. The z-score perfusion maps were generated for each participant with concussion and OI at both assessment time-points using the distribution-corrected z-scores (DisCo-Z) method, 44 -46 and subsequent voxel-based analyses were conducted.
Specifically, the z-maps were computed relative to the voxel-based mean and standard deviation (SD) of the pooled relative cerebral blood flow data from all OI participants. Voxels of abnormal hyperperfusion or hypoperfusion were identified based on adjusted z-threshold that accounted for the distributional properties of the transformed concussion and OI data (preset threshold of z-score ≥2.5 or ≤ -2.5, respectively, similar to a TBI study using a subject-specific abnormalities approach). 25 A criterion of five contiguous voxels (40 mm3) was applied to mitigate the presence of false extrema. For each participant at both study time-points, the number of clusters exhibiting abnormal perfusion, including hypoperfusion and hyperperfusion, along with the corresponding abnormal volume for each perfusion category, was calculated.
Statistical analysis
Frequencies and descriptive statistics were used to summarize participants' baseline characteristics for the total PedCARE+MRI sample and final sample included in the study. Independent t-tests or chi-squared tests were performed to compare the concussion and OI groups on demographic variables as appropriate. Moreover, symptomatic and asymptomatic concussed participants at each time-point were compared on demographic variables. These group comparisons were performed using SPSS version 22.0 (IBM Corp, United States). Partial-η 2 are reported as the effect size for the ANCOVAs using the following guidelines: η 2 < 0.06 = small; η 2 = 0.06-0.14 = medium; η 2 > 0.14 = large. 47
Analysis 1: Comparing global and adjusted perfusion by group and time-points
First, a 2 (Concussion vs. OI) × 2 (72 h vs. 4 weeks) within-subjects and between-groups mixed ANCOVA was conducted to investigate the Group × Time interaction on global perfusion within the whole–brain, gray matter, and white matter, with Power's FD values, age, and sex as covariates. A Bonferroni correction was applied (p < 0.05/3).
Second, a 2 (Concussion vs. OI) × 2 (72 h vs. 4 weeks) ANCOVA was conducted to investigate the Group × Time interaction for regional perfusion at the whole–brain level. Preprocessed perfusion maps of the two groups at both time-points were included in the model. Global gray matter perfusion, age, sex, and Power's FD values were controlled to examine adjusted perfusion to reduce the confounding effect of individual differences. Thresholds were set as uncorrected p < 0.001 at the whole–brain level, and false discovery rate (FDR) corrected p < 0.05 at the cluster level. Post hoc regions of interest (ROIs) analyses were performed in the regions showing significant main effects or interaction effects in the whole–brain ANCOVA analysis.
Analysis 2: Patterns of abnormal brain perfusion within groups
Within-group series of generalized estimating equations with negative binomial distribution were conducted to investigate the recovery of number of clusters of hyperperfusion and hypoperfusion, and corresponding perfusion volumes, between the 72-h and 4-week time-points. Age, sex, and Power's FD values were included as covariates. A Bonferroni correction was applied (p < 0.05/4).
Analysis 3: Association between perfusion and symptom burden at each time-point
First, a regression analysis between HBI total scores and adjusted perfusion was performed using preprocessed perfusion maps of the two groups at both time-points included in the model as dependent variables, with Group and HBI total as the covariates of interests. The Power's FD values, mean perfusion values in global gray matter, age, and sex were treated as covariates. We focused on the Group × HBI interaction to compare the HBI-perfusion association differences between concussion (n = 69) and OI (n = 29) groups in both time-points. Thresholds were set as uncorrected p < 0.001 at the whole–brain level, and family-wise error (FWE) corrected p < 0.05 at the cluster level. Post hoc ROI analyses were performed in the regions showing significant interaction effects in the whole-brain regression analysis.
Second, a series of regression analyses between HBI total scores and abnormal perfusion (hypoperfusion, and hyperperfusion) volumes was performed at both time-points, with HBI total score as dependent variables (either 72 h or 4 weeks), and abnormal perfusion volumes (either hyperperfusion or hypoperfusion), age, sex, and Power's FD values as predictors. A Bonferroni correction was applied across time-points (p < 0.05/2).
Analysis 4 (exploratory): Comparison in perfusion between symptomatic and asymptomatic concussed participants, and OI
First, whole–brain level one-way ANCOVAs were conducted for each time-point to explore group differences (symptomatic, asymptomatic, and OI) in adjusted perfusion. Power's FD values and mean perfusion values in global gray matter were treated as covariates. Post hoc ROI analysis was conducted when a Group effect was significant at the whole–brain level. Pairwise ANCOVA analyses were conducted if no group effect was found. Thresholds were set as uncorrected p < 0.001 at the whole–brain level, and family-wise error (FWE) corrected p < 0.05 at the cluster level.
Second, one-way ANCOVAs were conducted at each time-point to explore group differences (symptomatic, asymptomatic, and OI) in the number of abnormally hyperperfused and hypoperfused clusters and in the corresponding volumes. Power's FD values were treated as covariates. Post hoc ROI analyses were conducted even in the absence of a Group effect. A Bonferroni correction was applied across time-points (p < 0.05/2).
Results
Participants
A total of 70 youth with concussion [median age (interquartile range; IQR) = 12.70 (11.67-14.35) years, 47.1% female] and 29 with OI [median age (IQR)=12.05 (11.18-13.89) years, 41.4% female] were included (see Supplementary Fig. S1 in the Supplementary Materials for enrollment breakdown of the concussion and OI groups). Concussion and OI groups did not differ in age, sex, mechanism of injury, or prevalence of co-morbid developmental and psychiatric disorders (Table 1). However, time from injury to the first MRI was significantly shorter in the concussion group than in the OI group [Concussion median (IQR) = 75.13 (52.12-89.50) h; OI median (IQR) = 117.00 (70.25-121.13) h; p = 0.003].
Participant Demographics
Significant at p = 0.003. One participant did not complete the HBI questionnaire at 4 weeks. 1Social (Pragmatic) Communication Disorder, Language Processing Disorder, Autism Spectrum Disorder; 2One missing value; 3Social (Pragmatic) Communication Disorder and Language Processing Disorder; 4Language Processing Disorder; 5Not enough details to ascertain the type of injury (i.e., thrown on the ground, kicked in the head). It could be assault or sport/recreational play.
PedCARE+MRI, Pediatric Concussion Assessment of Rest and Exertion+MRI; OI, orthopedic injury; SD, standard deviation; ADHD, attention deficit/hyperactivity disorder; ED, emergency department; IQR, interquartile range; MRI, magnetic resonance imaging.
Analysis 1: Comparing global and adjusted perfusion by group and time-points
Global perfusion by group and by time-points
Global perfusion analyses revealed significant Time effects for gray matter [F(4,64) = 6.612, p = 0.012, white matter, F(4,94) = 5.804, p = 0.016] and whole–brain [F(4,94) = 6.612, p = 0.12; Table 2] with perfusion being increased at 4 weeks relative to 72 h. Specifically, the concussion group showed increased global perfusion in gray and white matter and whole–brain at 4 weeks relative to 72 h [ts(69) ≥ 2.167, ps ≤ 0.013], while the OI group did not show perfusion differences between the two time-points [ts(28) ≤ 0.498, ps ≥ 0.622; Table 3]. While the Time effect was mainly driven by the concussion group, no Group effect or interaction of Group × Time survived Bonferroni correction (ps ≥ 0.035; Fig. 1).
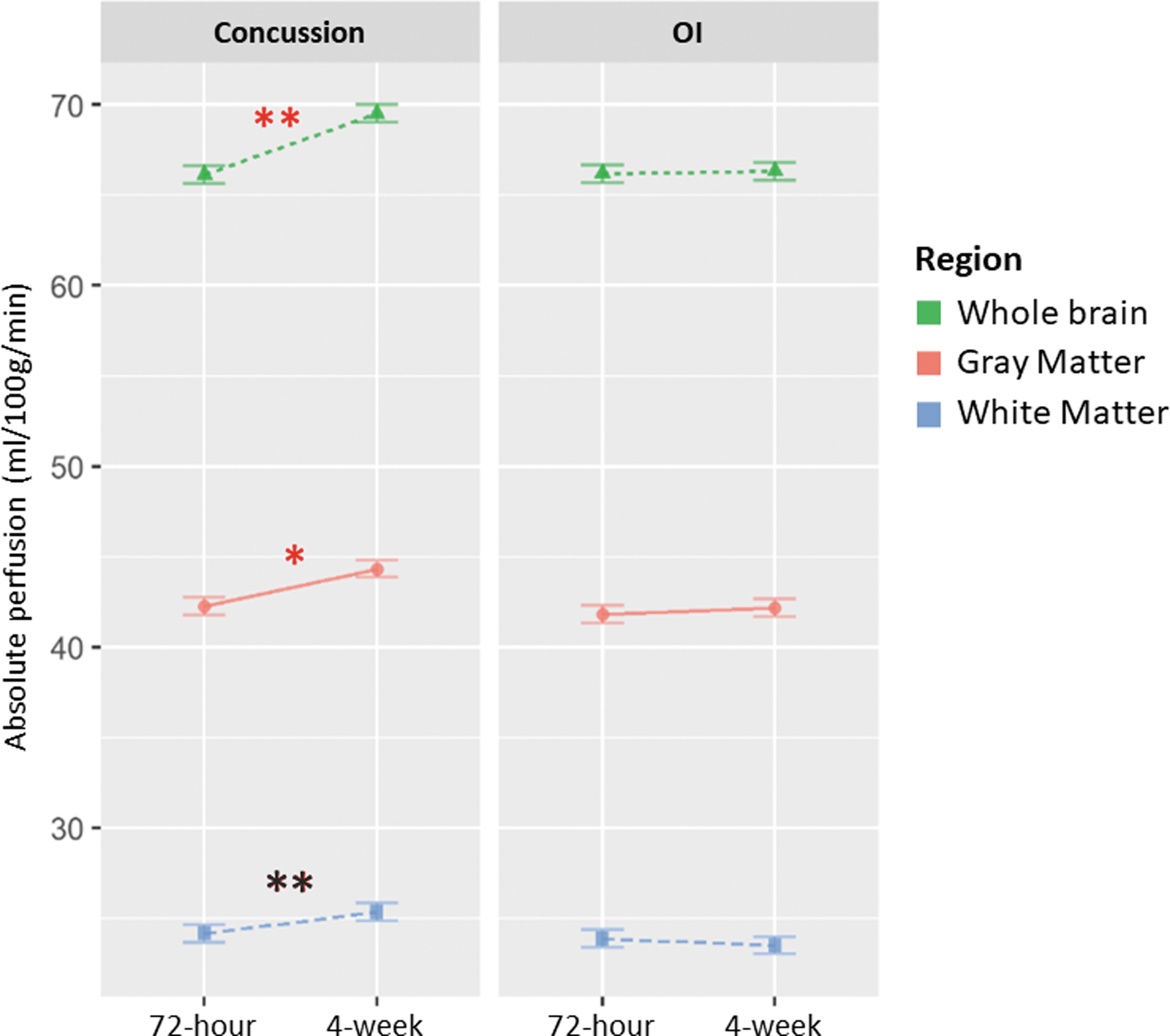
Main Time effect in Absolute Global perfusion within the gray matter (GM), whole–brain, and white matter (WM) in the Concussion and the Orthopedic Injury groups at the 72 h and 4 weeks post-injury time-points.
Group Effects, Time Effects, and Group × Time Interaction on Global Perfusion in Gray Matter, White Matter, and Whole–Brain in Concussion and Orthopedic Injury Groups at 72 h and 4 Weeks Post-Injury
The significance was p < 0.016 (.05/3) after the Bonferroni correction. Bold font denotes significance.
GM, gray matter; WM, white matter.
Post Hoc Time Effects of Global Perfusion in Concussion and Orthopedic Injury Groups
Bold font denotes significance.
GM, gray matter; WM, white matter.
Changes in adjusted perfusion by group and by time-point
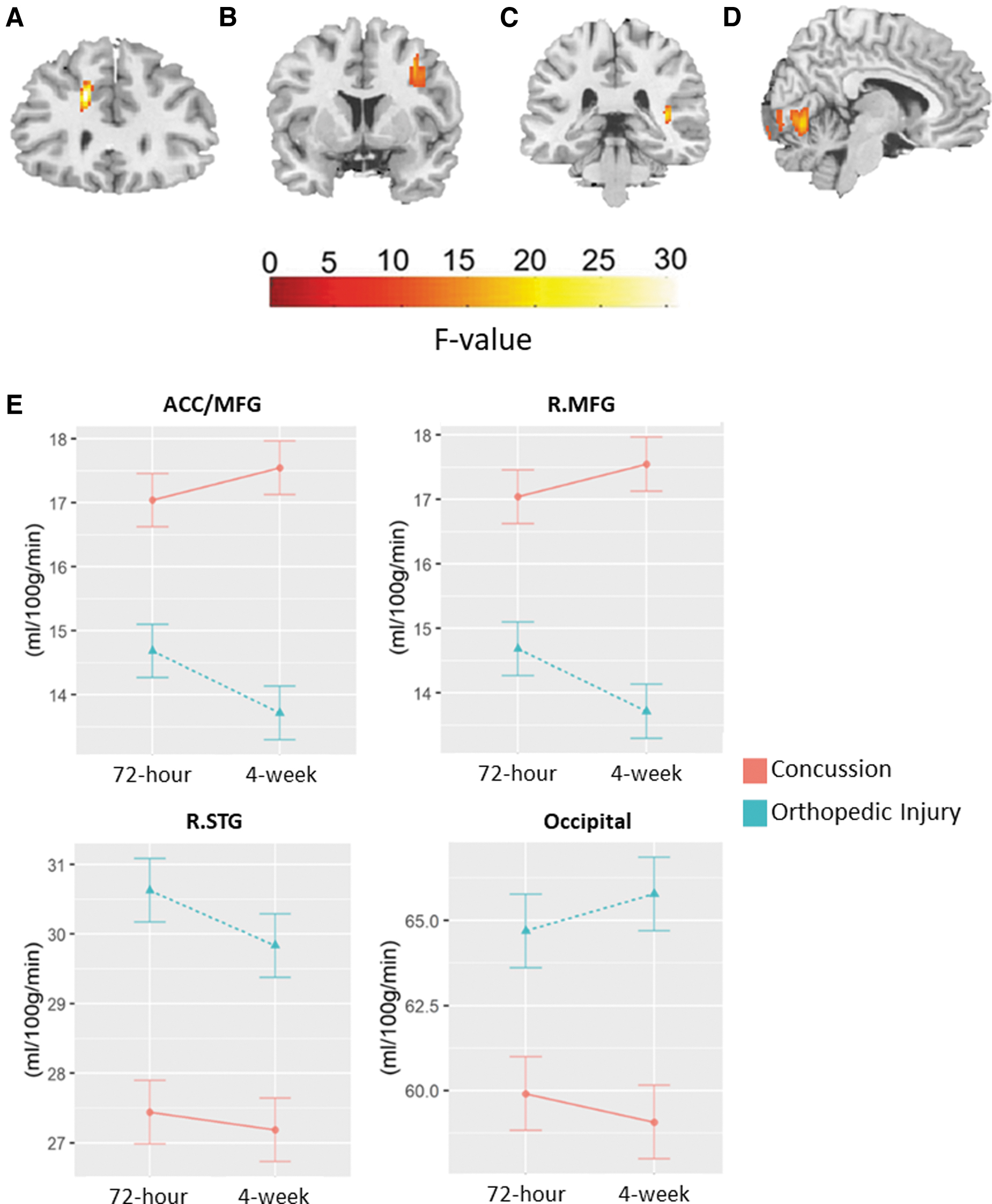
No significant Group × Time interaction was found in adjusted perfusion; however, the whole–brain analysis of regional perfusion showed significant Group effects within the anterior cingulate cortex/middle frontal cortex (ACC/MFC; Fig. 2A), right middle frontal gyrus (R.MFG; Fig. 2B), right superior temporal gyrus (R.STG; Fig. 2C) and left and right occipital lobe (Fig. 2D; Table 4; ps ≤ 0.0.038).
Main Group effects (Concussion vs. Orthopedic Injury) in adjusted regional perfusion within the
Main Group Effects (Concussion vs. Orthopedic Injury) in Adjusted Regional Perfusion
Power's framewise displacement values, mean perfusion values in global gray matter, age, and sex were treated as covariates. Thresholds were set as uncorrected p < 0.001 at the whole–brain level, and false discovery rate corrected p < 0.05 at the cluster level. Bold font denotes significance.
FWE, family-wise error; ACC, anterior cingulate cortex; MFC, middle frontal cortex; R, right; MFG, middle frontal gyrus; STG, superior temporal gyrus; L, left.
Post hoc ROI analyses revealed that the concussion group showed greater perfusion within the ACC/MFG and R.MFG compared with the OI group at both time-points. Further, the concussion group showed lower perfusion within the R.STG at 72 h and within the occipital at 4 weeks (Table 5; Fig. 2E). Absolute perfusion results are presented in the Supplementary Materials.
Post hoc Region of Interest Analyses of Group Differences (Concussion vs. Orthopedic Injury) in Adjusted Regional Perfusion
Power's framewise displacement values, mean perfusion values in global gray matter, age, and sex were controlled for as covariates. The significance was p < 0.01 (0.05/5) after the Bonferroni correction. Bold font denotes significance.
ACC, anterior cingulate cortex; MFG, middle frontal gyrus; CC, concussion; OI, orthopedic injury; R, right; STG, superior temporal gyrus.
A significant Time effect was found within the left postcentral gyrus (L.PostCG: -60, -12, 26, cluster size = 188 voxels, F = 32.31, pFDR < 0.001 (Fig. 3A). Post hoc analyses revealed that the perfusion was lower at 72 h than at 4 weeks within the L.PostCG (t = -3.60, p < 0.001). Both the concussion (t = -2.81, p = 0.006), and the OI (t = -2.26, p = 0.028) groups showed this Time effect (Fig. 3B).
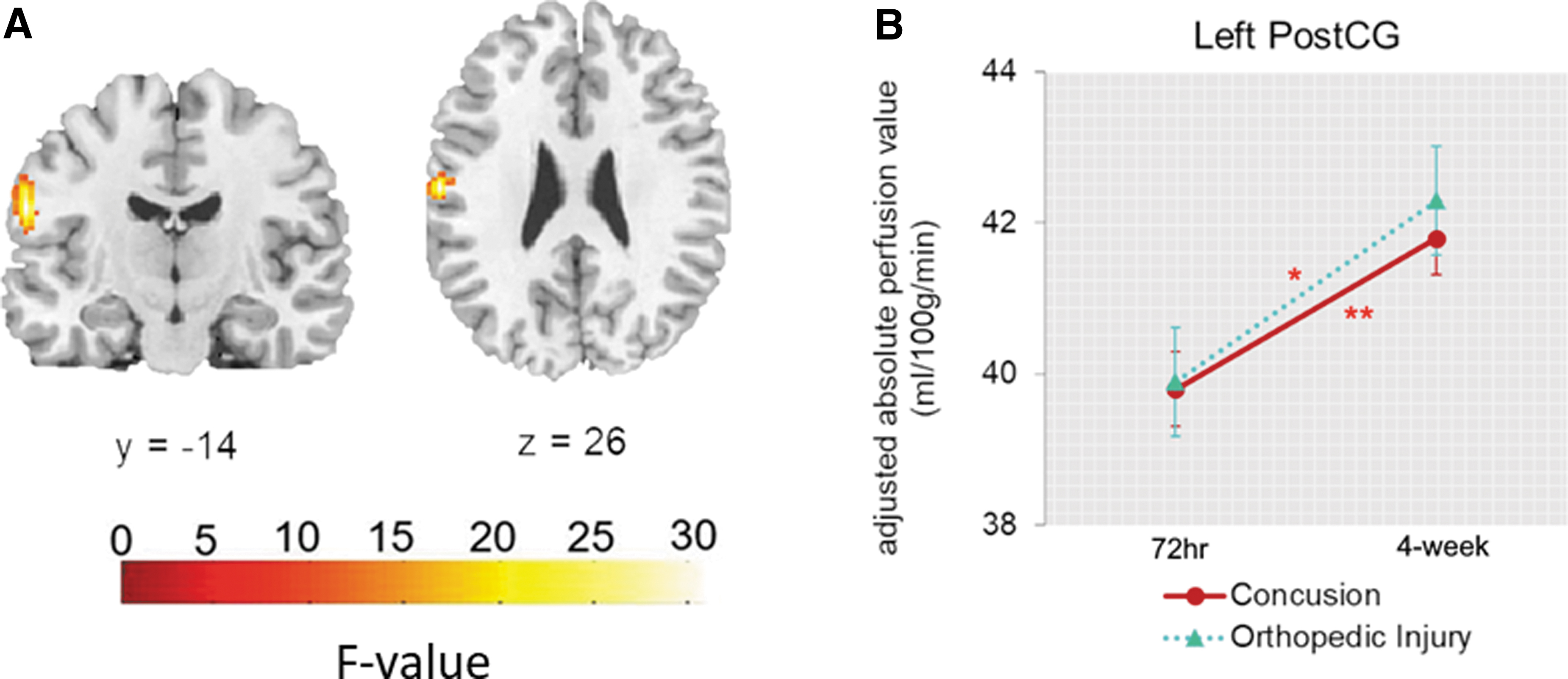
Main Time effects (72 h vs. 4 weeks) in adjusted regional perfusion within the left postcentral gyrus (PostCG). Power's framewise displacement (FD) values, mean perfusion values in global gray matter, age, and sex were treated as covariates
Analysis 2: Patterns of abnormal brain perfusion within group
s
Descriptives for the voxel-based z-scores analyses can be found in Table 6. Detailed results are presented in Supplementary Tables S1 and S2 in the Supplementary Materials.
Descriptive of Voxel-Based z-Scores Analyses
Data are presented as median [interquartile range].
OI, orthopedic injury.
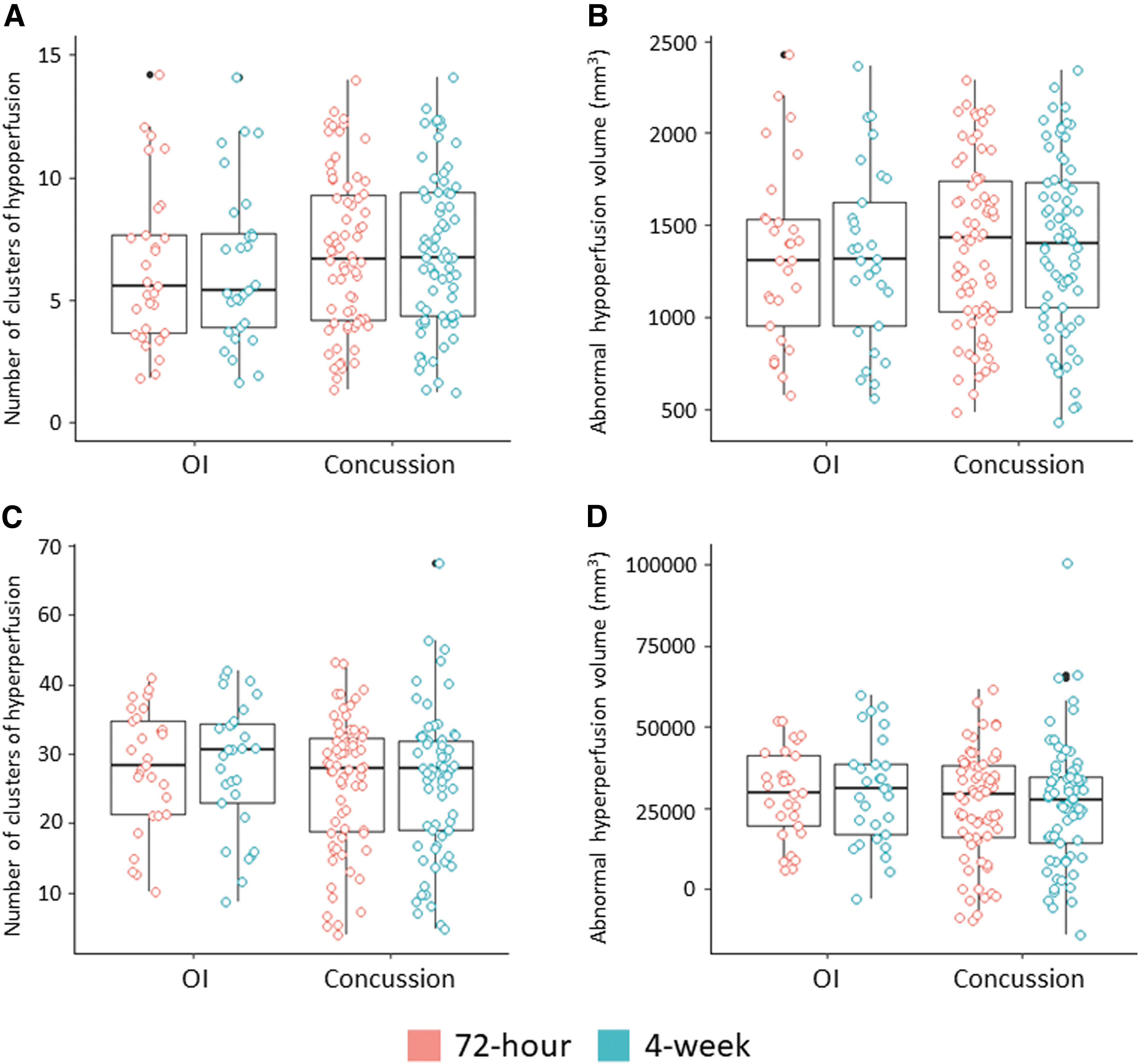
Within the concussion group, a significant Time effect was found for the number of hypoperfused clusters [Wald χ 2 (1) = 18.23, p < 0.001], with an increased number of hypoperfused clusters at 72 h compared with 4 weeks post-concussion (Fig. 4A). The analyses did not reveal a statistically significant Time effect for abnormal hypoperfusion volume after applying the Bonferroni correction [p < 0.0125; Wald χ 2 (1) = 6.19, p = 0.013], although they suggested higher abnormal volume at 72 h compared with 4 weeks (Fig. 4B). No Time effects were observed for number of hyperperfused clusters or abnormal hyperperfusion volume [Wald χ 2 (1) ≤ 0.44, ps ≥ 0.508; Fig. 4C, 4D].
Patterns of abnormal brain perfusion within the Concussion and the Orthopedic Injury groups at 72 h and 4 weeks on
Within the OI group, no time effects were observed for abnormal cluster numbers or volumes in hyperperfusion or hypoperfusion [Wald χ 2 (1) ≤ 1.12, ps ≥ 0.291].
Analysis 3: Association between perfusion and symptom burden
Association between adjusted perfusion and symptom burden
Perfusion levels in the left precuneus (L.Pcu: -14, -60, 42; clusters size = 115 voxels, F = 17.13, p FWE = 0.05) and left superior frontal gyrus (L.SFG: -22, 56, 14, cluster size = 108 voxels, F = 26.05, p FWE = 0.008) were associated with symptom burden (Supplementary Fig. S2 in the Supplementary Materials).
Post hoc ROI analyses showed significant HBI × Group interactions at both time-points, indicating that the concussion and the OI groups had different HBI-perfusion associations, adjusted for Power's FD, global gray matter perfusion, age, and sex. Specifically, at both time-points, the concussion group showed a positive association between HBI and L.Pcu, while the OI group showed a negative one. Moreover, at both time-points, the concussion group showed negative associations between HBI and L.SFG perfusion, while the OI group showed positive associations (Table 7). Absolute perfusion results are presented in the Supplementary Materials.
Post-Hoc Region of Interest Analysis (ROI) Between Symptom Burden and Adjusted Regional Perfusion
L = Left; HBI = Health Behavior Inventory, measures symptom burden; Pcu = Precuneus; SFG = Superior Frontal Gyrus. Power's FD values, mean perfusion values in global gray matter, age, and sex were treated as covariates. The significance was p adj < .05 after Bonferroni correction. Bold font denotes significance.
Association between abnormal volumes of perfusion and symptom burden within the concussion group
HBI total scores were not a significant predictor of abnormal perfusion volumes (neither hyperperfusion nor hypoperfusion) at 72 h or 4 weeks post-concussion after accounting for Power's FD values, age, and sex (ps ≥ 0.047; Table 8). The association between HBI total scores and abnormal hyperperfusion at 4 weeks did not survive the Bonferroni correction (p < 0.025). Detailed results are presented in Supplementary Table S3 in the Supplementary Materials.
Association Between Symptom Burden and Volume of Abnormal Perfusion Within the Concussion Group Within 72 Hours and 4 Weeks of injury
Symptom burden was measured with the total scores of the Health Behavior Inventory (HBI). Volumes are in mm3. Power's FD, age, and sex were treated as covariates. Only the predictor of interest (total score on the HBI completed at the same timepoint) is presented here. The full models can be found in Supplemental Materials. The significance was p < .025 (.05/2) after the Bonferroni correction.
Analysis 4 (exploratory): Comparison in CBF between symptomatic and asymptomatic concussion, and OI groups
Comparison of adjusted perfusion
At 72 h, 32 concussed participants were reliably symptomatic, while 38 were asymptomatic. Neither the omnibus one-way ANCOVA nor the pairwise comparisons showed Group effects in perfusion between symptomatic concussion, asymptomatic concussion, and OI groups.
At 4 weeks, 10 concussed participants were still symptomatic, while 59 were asymptomatic (one missing HBI at 4 weeks). The one-way ANCOVA did not show group differences, yet the pairwise comparisons showed lower adjusted perfusion for the symptomatic group within the right cerebellum (24, -38, -44; t = 4.45, p FWE = 0.013, cluster size = 113 voxels) and right lingual gyrus (6, -72, 4; t = 4.12, p FWE = 0.001, cluster size = 161 voxels) relative to the OI group (Fig. 5A). In addition, the asymptomatic group showed lower adjusted perfusion within the bilateral calcarine (R: 12, -82, 8; t = 4.45, p FWE = 0.036, cluster size = 93 voxels; L: -10, -88, 0; t = 4.54, p FWE < 0.001, cluster size = 307 voxels; Fig. 5B) relative to the OI group, and greater adjusted perfusion within the left medial orbitofrontal cortex (-14, 36, -10; t = 5.15, p FWE < 0.001, cluster size = 220 voxels), R.MFG (30, 8, 28; t = 4.42, p FWE = 0.036, cluster size = 93 voxels), and bilateral caudate (R: 18, 26, 4; t = 3.34, p FWE = 0.005, cluster size = 139 voxels; L: -18, 24, 2; t = 3.90, p FWE < 0.001, cluster size = 220 voxels; Fig. 5C).
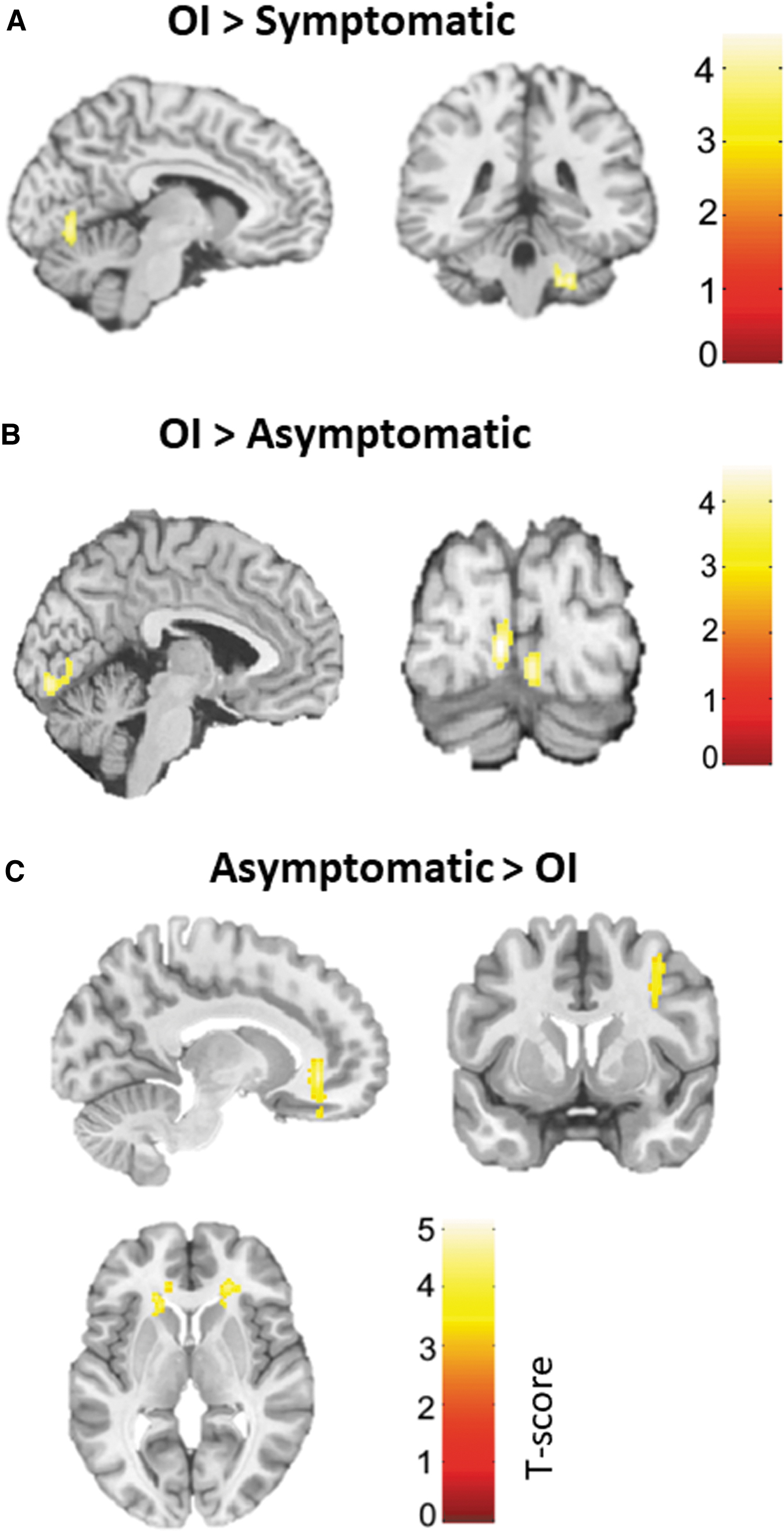
Pairwise comparison among Symptomatic Concussion, Asymptomatic Concussion, and Orthopedic Injury groups in adjusted regional perfusion within the
Comparison of abnormal perfusion
Neither the omnibus one-way ANCOVA nor the pairwise comparisons showed Group effects in the number of abnormally perfused clusters (hyperperfused or hypoperfused; Supplementary Fig. S3 in the Supplementary Materials) or hyperperfusion or hypoperfusion volume (Fig. 6) between symptomatic concussion, asymptomatic concussion, and OI groups at 72 h or 4 weeks (ps ≥ 0.209).

Comparison of abnormal perfusion at 72 h and 4 weeks between participants who remained symptomatic at 4 weeks, who were clinically recovered (i.e., asymptomatic) at 4 weeks, and who had an orthopedic injury (OI) in terms of hyperperfusion
Discussion
In this prospective longitudinal neuroimaging study, differences in regional perfusion between concussion and OI group were found in both the acute (i.e., 72 h post-injury) phase of injury and at 4 weeks post-concussion within brain regions associated with higher cognition, multisensory integration, vision, and language processing. These regional differences were observed in the absence of group differences in global perfusion. Significant associations between perfusion within the left precuneus and left SFG and symptom burden were observed, and these associations were moderated by group at both time-points. When the concussion group was further divided into symptomatic and asymptomatic subgroups and compared with the OI group, different brain perfusion profiles were observed 4 weeks post-injury. Importantly, youth who had clinically recovered from their concussion (i.e., asymptomatic) exhibited differences in perfusion within several brain regions compared with the youth with OI, suggesting that the brain may not have fully physiologically recovered.
In the present study, global perfusion did not differ between concussion and OI groups over time, yet regional perfusion changes were found despite no group difference in global perfusion, similar to previous studies. 11,16,22 Specifically, when compared with the OI youth, concussed participants exhibited both hypoperfusion and hyperperfusion at 72 h and 4 weeks in several brain regions, suggesting an incomplete regional neurophysiological recovery.
Interestingly, among those with a concussion, we observed an increased number of abnormal hypoperfused clusters at 72 h post-injury compared with 4 weeks, with the hypoperfusion volume nearing statistical significance. However, unlike our regional results, abnormal hyperperfusion clusters and volume did not differ over time. As expected OI groups were stable through time. In contrast, an adult TBI study showed significantly higher volumes of abnormally hyperperfused and hypoperfused tissue in subacute TBI participants (median = 17 days) compared with controls. 25 Further, in that study, while not statistically significant, there was a higher number of hypoperfused clusters. A small subset of participants also underwent a scan at 6 months post-injury, showing a decrease in abnormal hypoperfusion volume between the two assessments. The discrepancies in findings concerning hyperperfusion may be attributed to differences in sample characteristics (age, injury severity, time since injury to MRI) and methodologies (DisCo-z vs. leave-one-out method, adjustment for confounding variables, and statistical tests). Taken together with previous studies, the present findings suggest that perfusion recovery in concussion may occur regionally rather than globally. 48 Further, the presence of hypoperfusion abnormalities at 72 h post-concussion, which subsequently resolved by 4 weeks, suggests recovery.
This study also provides evidence that post-concussion symptoms may reflect the neurometabolic cascade stemming from the concussive injury. First, significant associations were found between symptom burden and regional brain perfusion. These associations were present at 72 h and persisted at 4 weeks, and were moderated by group (i.e., associations were in opposite directionality). Specifically, the greater the symptom burden, the greater the left precuneus perfusion in the concussion group, whereas the opposite was observed within the OI group. In the left SFG, the opposite pattern was observed: the lower the symptom severity, the greater the perfusion within the concussion group. These findings are partially consistent with those from previous studies in adults. In university athletes within 7 days of a sports concussion, greater symptom severity was associated with increased posterior cortical perfusion. 20 Further, in older adults, the severity of dizziness symptoms was correlated with higher perfusion in the frontal lobes. 14 The current study suggests that associations between symptom severity and perfusion are also present in pediatric populations, yet they might differ from those observed in adults.
Second, different brain perfusion profiles were observed based on the symptomatic status of concussed participants at 4 weeks. Concussed participants who were still symptomatic 4 weeks post-injury displayed higher regional perfusion than youth with OI within the right cerebellum and lingual gyrus. Findings of increased perfusion in children and adolescents who remained symptomatic in the subacute stage of concussion when compared with the OI group are consistent with previous studies, although the regions where these group differences were observed are different. 21,24 This may reflect heterogeneity in the mechanism of injury, localization of concussive impact or presence of coup-contre-coup injuries, analytic methods, or other premorbid factors.
Importantly, the current study revealed differences between asymptomatic concussed participants and OI youth within some brain regions, with both hypoperfusion and hyperperfusion being observed. Hyperperfusion in asymptomatic participants may represent a compensatory mechanism reflecting the high metabolic demand needed for recovery, while hypoperfusion might be related to local damage to microvasculature. 49 Similar to the present study, a previous study showed increased perfusion within the left dorsal anterior cingulate cortex in adolescent athletes who reported symptoms 6 weeks after their concussion compared with asymptomatic concussed athletes and athletes who never sustained a concussion. 24 Another study found differences between asymptomatic concussed participants and OI participants at 40 days post-concussion, but in this case, it involved lower regional perfusion in several areas. 21
Taken together with the present results, the collective findings suggest that neurophysiological recovery does not always align with post-concussion symptom resolution. Collapsing results across symptomatic status might lead to inaccurate conclusions regarding recovery because of differential perfusion patterns. However, the changes in brain perfusion may not be solely attributable to symptomatology. Indeed, significant differences in brain perfusion were observed between concussed participants who were not reporting symptoms and OI participants at 4 weeks post-injury, suggesting that the alterations in brain perfusion observed following a concussion are not due only to symptoms. Whether these changes have a significant impact on the safe return to daily activities, such as school, work, or sports, requires further exploration.
However, within the concussion group, symptom burden was not associated with abnormal perfusion levels at either the 72-h or 4-week post-concussion time-points. Results indicated a trend towards higher symptom burden being associated with increased levels of abnormal hyperperfusion at 4 weeks. This potential association may become statistically significant with a larger sample size and a distribution that is less skewed toward zero. Further, no statistical differences were observed between the symptomatic, asymptomatic, and orthopedic injury (OI) participants at 72 h and 4 weeks post-injury in terms of the number of abnormally perfused clusters and their corresponding volumes. Age and sex were not adjusted for in the analyses, despite prior research having identified them as moderators of both concussion and perfusion separately. The sample size of the symptomatic subgroup was not large enough to adequately control for important confounding variables, highlighting the exploratory nature of the analysis. As a result, the findings should be interpreted cautiously. Third, it is important to recognize that regional perfusion and abnormal perfusion are computationally and clinically distinct.
Given these considerations, the results of this analysis are best interpreted as serving an exploratory and hypothesis-generating role. They offer a foundation for potential future investigations that aim to refine our understanding of the relationships between concussion, symptom burden, and abnormal perfusion patterns. Subsequent studies could explore the optimal z-score threshold for differentiating concussion samples from comparison groups, including OIs and typically developing children ("healthy controls").
The present study provides valuable insights into the relationship between brain perfusion and symptoms; however, the mechanism underlying the altered brain perfusion is still unknown. Studies have highlighted that cerebrovascular reactivity (CVR) offers a unique perspective on cerebral vascular functioning by assessing changes in the hemodynamic response when vasodilatory agents (e.g., CO2) are introduced. 50 -52 Functional MRI combined with a respiratory challenge has shown promise in investigating CVR following concussion. Recent studies on concussed university athletes found that greater symptom severity 16,53 and prolonged recovery 53 were associated with CVR alterations during a breathing challenge. In adolescents, CVR alterations during a hypercapnia challenge were observed to persist beyond resting perfusion alterations, 54,55 suggesting either that CVR is more sensitive than ASL to the subtle changes occurring after concussion or that the concussion-related deficits are only apparent under the influence of an additional stressor. However, the CVR alterations were not associated with post-concussion symptoms, 54,55 behaviors, or quality of life 55 in the subacute phase of concussion. Future studies employing CVR and ASL techniques in conjunction will provide a more comprehensive assessment of blood flow after pediatric concussion.
To the best of our knowledge, the present study is among the first to not only conduct MRI scans in the acute phase (i.e., 72 h) following concussion, but also longitudinally with a relatively large sample size. The conservative approach to adjusting for multiple comparisons in regional perfusion analyses implemented herein reduced the possibility of false positives. Further, the inclusion of an OI comparison group is a strength, as it allowed for control of injury-related characteristics (e.g., pain, post-traumatic stress, medical treatment) 56 that would not be present in a healthy sample, strengthening the internal validity of the findings. The stability of global perfusion findings within the OI group across time suggests that the OI group is a suitable comparison group.
Despite the numerous strengths of this study, the findings must be interpreted considering some methodological limitations. First, the participants were recruited in the emergency department and, thus, the injuries might represent more severe concussions. However, sports concussions are over-represented in the literature, limiting the generalizability of the previous findings. Including a variety of mechanisms of injury may also be viewed as a strength as generalizability is increased. Second, while the OI group is viewed as a strength, the addition of a healthy comparison group of typically developing children would allow further control of injury-related variables. Third, the present study does not allow for determination of resolution time for the observed brain perfusion alterations. Future prospective, longitudinal ASL studies might consider including later time-points (e.g., 2 and 3 months) to determine the natural progression of neurophysiological recovery.
Fourth, the small sample and the low rate of comorbidities did not allow for examination of the possible relationships between pre-existing neurodevelopmental or psychological disorder and brain perfusion after pediatric concussion. Fifth, the present study employed a measure of overall symptom burden that encompassed both cognitive and somatic symptoms. This measure captured a broad range of symptoms related to the complex nature of concussion. While the measure captured a broad range of symptoms, it did not allow the exploration of the potential influence of other maladaptive phenotypes (e.g., pain, mood and sleep disturbances, cognitive fatigue) on brain perfusion recovery. Finally, treatment (early resumption of physical activity vs. rest until asymptomatic) was not controlled for in the analyses for several reasons: no randomization of the OI group, as it served as a reference for the neuroimaging component, and lack of accelerometer data for the OI group.
Conclusions
The present findings show differential regional perfusion patterns at 72 h that persisted at 4 weeks between concussion and OI participants, even in clinically recovered concussed participants, suggesting an incomplete physiological recovery. Within the concussion group, hypoperfusion abnormalities were observed at 72 h and resolved by 4 weeks, suggesting recovery. Further, the findings indicate that pediatric concussion symptomatology is related to brain perfusion at a group level, but not to subject-specific abnormal perfusion levels. While previous concussion research of brain hemodynamics is variable in study design and findings, brain perfusion along with symptoms may be a promising biomarker for pediatric concussion.
Transparency, Rigor, and Reproducibility Summary
This is a substudy of a larger randomized clinical trial. The parent study Pediatric Concussion Assessment of Rest and Exertion (PedCARE) study was pre-registered at
Footnotes
Acknowledgments
We would like to acknowledge the contribution of the Royal Brain Imaging Center, specifically Reggie Taylor and Katie Dinelle. We would like to thank Andrew Dodd for his methodological input on subject-specific abnormalities approaches.
Partial results from this study were presented at the 2nd Meeting of the Canadian Concussion Network in Montreal, QC in June 2022. The conference proceeding was published in the Journal of Head Trauma Rehabilitation. 58 Results as presented herein were presented at an internal conference at the University of Ottawa Brain and Mind Research Institute Research Day in Ottawa, Canada in December 2023. Abstracts were not published. Results were presented at the 14th World Congress of Brain Injury in Dublin, Ireland in March 2023. The conference proceeding was published in Brain Injury.
Portions of this manuscript are available online (doi: 10.22215/etd/2022-15254) as a thesis for Rachel Kardish, MSc, submitted to the Faculty of Graduate and Postdoctoral Affairs of Carleton University, Ottawa, Ontario, Canada, as a requirement for the degree of Master of Science in Neuroscience obtained in 2022. The thesis is available online on the Carleton University Institutional Repository (
Authors' Contributions
Veronik Sicard: Conceptualization (lead), formal analysis (equal), writing—original draft (lead), visualization (equal). Zhuo Fang: Formal analysis (equal), writing—review and editing, visualization (equal). Rachel Kardish: Conceptualization (equal), formal analyses (supporting), writing—original draft (supporting). Katherine Healey: Investigation (lead), formal analyses (supporting), methodology (supporting), writing—review and editing, project administration (equal). Andra Smith: Conceptualization (supporting), methodology (supporting), writing—review and editing. Sarah Reid: Investigation (supporting), writing—review and editing. Greg O. Cron: Conceptualization (supporting), methodology (supporting), writing—review and editing. Gerd Melkus: Conceptualization (supporting), methodology (supporting), writing—review and editing. Nishard Abdeen: Conceptualization (supporting), methodology (supporting), writing—review and editing. Keith Owen Yeates: Conceptualization (supporting), methodology (supporting), writing—review and editing. Gary Goldfield: Conceptualization (supporting), writing—review and editing. Nick Reed: Conceptualization (equal), methodology (equal), writing—review and editing. Roger Zemek: Conceptualization (equal), methodology (equal), investigation (lead), funding acquisition (lead), writing—review and editing. Andrée-Anne Ledoux: Project administration (lead), conceptualization (lead), methodology (lead), formal analyses (lead), investigation (lead), funding acquisition (lead), writing—review and editing, supervision (lead).
Funding Information
This work was supported by the IMPACT OSSU Award; the PSI Foundation; and graduate student funding from the Canadian Institutes of Health Research (CIHR).
Authors Disclosure Statement
VS receives royalties for the sales of a concussion book (Commotions Cérébrales) by Flammarion Québec.
RLZ's research program has received financial support through competitively funded research grants from Canadian Institutes of Health Research (CIHR), Ontario Neurotrauma Foundation (ONF), Physician Services Incorporated (PSI) Foundation, CHEO Foundation, Ontario Brain Institute (OBI), National Football League (NFL), Ontario Ministry of Health (MOH), Public Health Agency of Canada (PHAC), Health Canada, Parachute Canada and Ontario SPOR Support Unit (OSSU). RZ is also supported by a Tier 1 Clinical Research Chair in Pediatric Concussion from University of Ottawa. All grant funding goes directly to the institution. RZ sits on the board of directors for North American Brain Injury Society (NABIS) which is an unpaid volunteer role. Finally, RZ is a founding partner and a minority shareholder of 360 Concussion Care (a learning health system and network of interdisciplinary concussion clinics in Ontario); no proceeds have been transferred to RZ.
NR is a holder of a Canada Research Chair (Tier 2) in Pediatric Concussion and reports receiving grants and research funding from the Canadian Institutes of Health Research (CIHR), Ontario Neurotrauma Foundation (ONF), Public Health Agency of Canada (PHAC), Parachute Canada, Special Olympics Canada, Greater Toronto Hockey League, Dr. Tom Pashby Sport Safety Fund, Holland Bloorview Kids Rehabilitation Hospital and Scotiabank. NR is an investigator in a multi-center study funded by the National Football League (NFL) Scientific Advisory Board. NR is an executive board member for the International Pediatric Brain Injury Society (IPBIS) which is an unpaid volunteer role.
For the other authors, no competing financial interests exist.
Supplementary Material
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.