
Abstract
Epidemiological studies have identified prior traumatic brain injury (TBI) as a risk factor for developing Alzheimer's disease (AD). Neurofibrillary tangles (NFTs) are common to AD and chronic traumatic encephalopathy following repetitive mild TBI. However, it is unclear if a single TBI is sufficient to cause accumulation of NFTs. We performed a [18F]MK-6240 positron emission tomography (PET) imaging study to assess NFTs in patients who had sustained a single TBI at least 2 years prior to study inclusion. Fourteen TBI patients (49 ± 20 years; 5 M/9 F; 8 moderate-severe, 1 mild-probable, 5 symptomatic-possible TBI) and 40 demographically similar controls (57 ± 19 years; 19 M/21 F) underwent simultaneous [18F]MK-6240 PET and magnetic resonance imaging (MRI) as well as neuropsychological assessment including the Cambridge Neuropsychological Test Automated Battery (CANTAB). A region-based voxelwise partial volume correction was applied, using parcels obtained by FreeSurfer v6.0, and standardized uptake value ratios (SUVR) were calculated relative to the cerebellar gray matter. Group differences were assessed on both a voxel- and a volume-of-interest-based level and correlations of [18F]MK-6240 SUVR with time since injury as well as with clinical outcomes were calculated. Visual assessment of TBI images did not show global or focal increases in tracer uptake in any subject. On a group level, [18F]MK-6240 SUVR was not significantly different in patients versus controls or between subgroups of moderate-severe TBI versus less severe TBI. Within the TBI group, One Touch Stockings problem solving and spatial working memory (executive function), reaction time (attention), and Mini-Mental State Examination (MMSE) (global cognition) were associated with [18F]MK-6240 SUVR. We found no group-based increase of [18F]MK-6240 brain uptake in patients scanned at least 2 years after a single TBI compared with healthy volunteers, which suggests that no NFTs are building up in the first years after a single TBI. Nonetheless, correlations with cognitive outcomes were found that warrant further investigation.
Introduction
Several epidemiological studies have identified prior traumatic brain injury (TBI) as an important risk factor for the development of dementia and Alzheimer's disease (AD). 1 –4 Whereas earlier research linking TBI to AD was mostly based on clinical evaluations of AD, today AD is biologically defined by means of biomarkers for the presence of amyloid plaques, tau neurofibrillary tangles (NFTs), and neurodegeneration (amyloid/tau/neurodegeneration [ATN] framework). 5 Post-mortem studies have shown that repetitive (mild) TBI can lead to the widespread accumulation of NFTs and the development of chronic traumatic encephalopathy (CTE). 6 The NFTs found in CTE after repetitive TBI are predominantly located in the depths of cerebral sulci, around small cerebral blood vessels, 7 –16 whereas in AD, an NFT-specific hierarchical progression pattern has been demonstrated by Braak and Braak. 17
As for pathological changes after a single TBI, conflicting results have been reported. Johnson and coworkers reported NFTs in post-mortem brains from long-term survivors of a single TBI, although significance compared with healthy controls (HC) was only reached for the subset of subjects <60 years of age. 18 Using tau positron emission tomography (PET), some studies have shown increased tracer uptake after a single TBI compared with HC, 19,20 albeit by using first-generation tau PET tracers that also exhibit off-target binding to monoamine oxidase (MAO)-B and α-synuclein. 21 Different studies using the same tau PET tracer reported conflicting outcomes with some demonstrating increased [ 18 F]Flortaucipir uptake after a single TBI, 22,23 whereas others failed to do so. 24 Hicks and coworkers recently investigated [ 18 F]MK-6240 uptake in a large sample of patients who sustained a single moderate-to-severe TBI at least 10 years prior to study inclusion and found no significantly higher tracer uptake in comparison with HC. 25 Taken together, all available evidence suggests that NFTs can develop after a single TBI, although 10 years after the event, NFT-binding tracers such as [ 18 F]MK-6240 do not seem to show group differences compared with HC. It is unclear if at 10 years post- injury, NFTs are either not yet formed or may have already been cleared from the brain through tau clearance mechanisms such as proteasomal degradation and autophagy. 26,27
This study aims to investigate the presence of NFTs using [ 18 F]MK-6240 PET-magnetic resonance (MR) in subjects at least 2 years after a single TBI as compared with HC. Moreover, we explored the correlation of [ 18 F]MK-6240 binding with time since injury and with cognitive outcome as assessed by a neuropsychological test battery.
Methods
Participants
Eligible patients were at least 18 years old and had sustained a single TBI at least 2 years prior to study inclusion. Patients were referred by either neurosurgical or psychiatric centers. Severity was assessed according to the Mayo Classification.
28
Main exclusion criteria were history of neurodegenerative disorders prior to the head trauma and contraindication for magnetic resonance imaging (MRI). HC between 18 and 85 years old were recruited through local newspapers and Internet advertisements. Physical and mental health were thoroughly assessed. Exclusion criteria for HC were history of major neurological, psychiatric, or internal pathology; history of alcohol or other drug abuse; and MR abnormalities including brain white matter disease Fazekas 3. All subjects underwent cognitive screening consisting of a neuropsychological test battery with following subtests of the Cambridge Neuropsychological Test Automated Battery (CANTAB)
29
: Reaction Time (RTI), Paired Associates Learning (PAL), Spatial Working Memory (SWM), Multitasking Test (MTT), and One Touch Stockings of Cambridge (OTS). A detailed description of these tests can be found at
The study was approved by the local ethics committee and was conducted according to the latest version of the Declaration of Helsinki. Written informed consent was signed by all participants prior to study inclusion. This study is part of a larger, multimodal, multi-tracer imaging study that also included other patient populations (
Data acquisition
[ 18 F]MK-6240 was synthesized as previously described. 30 All subjects underwent a 30-min PET-MR scan, acquired 90–120 min post-injection of 100-150 MBq [ 18 F]MK-6240. All scans were performed on an integrated time-of-flight 3T PET-MR scanner (Signa, GE Healthcare, Milwaukee, WI, USA). [ 18 F]MK-6240 PET acquisitions were re-binned into six frames of 5 min and reconstructed using an ordered subset expectation maximization (OSEM) algorithm (4 iterations and 28 subsets), with corrections for scatter, random coincidences, dead time, and radioactive decay. Attenuation correction was zero-echo time (ZTE) MR-based as reported previously. 31 Three-dimensional isotropic 4 mm Gaussian smoothing was applied to reduce image noise.
Simultaneously with the PET scan, three-dimensional (3D) T1-weighted MR images [(plane: sagittal; echo time [TE]: 3.2 ms; repetition time [TR]: 8.5 ms; inversion time [TI]: 450 ms; flip angle: 12 degrees; receiver bandwidth: 31.25 kHz; number of excitations [NEX]: 1; voxel size: 1 x 1 x 1 mm) as well as 3D T2-weighted fluid-attenuated inversion recovery (FLAIR) images (plane: sagittal; TE: 137 ms; TR: 8500 ms; TI: 2298 ms; receiver bandwidth: 31.25 kHz; NEX: 1; voxel size: 0.7 x 1 x 1 mm) were acquired using a vendor-supplied 8-channel or 32-channel brain phased array head coil.
Subjects >50 years of age also underwent an amyloid [ 18 F]NAV4694 or [ 11 C]Pittsburgh compound B ( 11 C-PiB) PET scan on the same PET-MR scanner or on a PET-computed tomography (CT) scanner (Biograph TruePoint, Siemens, Erlangen, Germany), respectively. [ 18 F]NAV4694 and [ 11 C]PiB scans were reconstructed using an OSEM algorithm, and 3D isotropic 4.5 mm and 2 mm Gaussian smoothing were applied, respectively. Amyloid status was visually assessed and classified as positive or negative by an expert nuclear medicine physician (K.V.L.).
PET analysis
Reconstructed [ 18 F]MK-6240 images were corrected for motion artifacts with PMOD software (v4.1, PMOD Inc. Zurich, Switzerland) using a rigid frame-by-frame co-registration to the first frame. Subsequently, all motion-corrected frames were averaged and rigidly co-registered to the corresponding T1-weighted MRI. Also, T2-weighted FLAIR images were co-registered to the corresponding T1-weighted MRI. FreeSurfer v6.0 (Laboratory for Computational Neuroimaging v6.0, Boston, MA, USA) was used for T1- and T2 FLAIR-based MR segmentation and automated parcellation of the volumes of interest (VOIs). 32 –34 A region-based voxelwise (RBV) partial volume correction was applied to the standardized uptake value (SUV) maps, 35 where the PET resolution was modeled as a 3D isotropic Gaussian kernel with a full width at half maximum (FWHM) of 5 mm. Next, SUV ratios (SUVR) were calculated using the full cerebellar cortex as a reference region. 36 Based on regions with increased tau as obtained by other PET studies in TBI, 18 –20,22,23 eight composite, bilateral gray matter (GM) VOIs were a priori defined and derived from the FreeSurfer parcellation: frontal, parietal, occipital, temporal, mesotemporal (entorhinal cortex, parahippocampal gyrus, hippocampus, and amygdala) (MTL), and anterior cingulate cortex, as well as the insula and thalamus.
For the voxel-based analyses, SUVR maps were spatially normalized to Montreal Neurological Institute (MNI) space using a non-linear registration as obtained by the CAT12 toolbox of Statistical Parametric Mapping (SPM12; Welcome Trust Centre for Neuroimaging, University College, London, UK) and smoothed using an isotropic Gaussian kernel with 8 mm FWHM (voxel size: 1.5 x 1.5 x 1.5 mm).
Statistical analysis
Statistical analyses were performed in GraphPad Prism version 9 (GraphPad Software, La Jolla, CA, USA). Data are presented as mean ± standard deviation (SD) unless otherwise specified. Normality of the data distributions was assessed by Shapiro–Wilk tests (α = 0.05). Demographic characteristics were compared between groups using an unpaired Student t test, unpaired Mann–Whitney U test, Fischer's exact test, χ 2 test, or χ 2 test for trend as appropriate.
Using spatially normalized and smoothed images as described, voxel-based z-score maps were generated for each patient versus the HC group. Additionally, for each HC, a voxel-based z-score map was calculated versus the remainder of the HC group. A z-score of >2.5 was considered positive.
For the VOI-based analysis, mean regional [ 18 F]MK-6240 SUVRs were compared between TBI and HC using an unpaired Student t test or Mann–Whitney U test as appropriate at a significance level of α = 0.006 (Bonferroni corrected for 8 VOIs).
The voxel-based group comparison was performed using an unpaired t test in SPM with thresholds for cluster height, voxel height, and cluster extent of p < 0.05 (familywise error [FWE] corrected), p < 0.001 (uncorrected), and kext > 200 voxels, respectively. To exclude extracerebral clusters, a binary GM mask was applied. Correlations between [ 18 F]MK-6240 SUVR and time since injury were assessed within the TBI group and correlations between [ 18 F]MK-6240 SUVR and neuropsychological test scores were assessed within the combined cohort of TBI patients and HC, both by Pearson or Spearman correlation coefficients as appropriate at a significance level of α = 0.05. As this was an exploratory analysis, no correction for multiple comparisons was applied for this correlation analysis.
Results
Participants and neuropsychological evaluations
Fourteen patients with moderate-to-severe (n = 8), mild probable (n = 1), or symptomatic possible (n = 5) TBI were included and received a [ 18 F]MK-6240 PET-MR scan on average 5.6 ± 2.9 years (range 2.0–10.8) post injury. Patient characteristics are summarized in Table 1.
Patient Characteristics
Patient labels as shown in Figure 1.
PET, positron emission tomography; MRI, magnetic resonance imaging; DAI, diffuse axonal injury; Mild/prob TBI = mild probable traumatic brain injury; Mod/sev TBI = moderate/severe TBI; n/a = not available; Neg = negative; Pos = positive; Sympt/poss TBI = symptomatic possible TBI; TA = traffic accident.
For comparison, a demographically similar group of 40 HC was included. Injected activity was 121 ± 15 MBq (specific activity of 584 ± 250 GBq/μmol) and 138 ± 26 MBq (specific activity of 593 ± 464 GBq/μmol) for TBI patients and HC, respectively. Group characteristics are shown in Table 2.
Demographic Information on Healthy Control and TBI Groups
Data are presented as mean ± standard deviation (SD) when appropriate.
Significant findings are indicated in bold.
BDI, Beck Depression Inventory; CANTAB, Cambridge Neuropsychological Test Automated Battery; MMSE, Mini-Mental State Examination; MTT, Multitasking Test; OTS, One Touch Stockings of Cambridge; PAL, Paired Associates Learning; RTI, Reaction Time; SCL-90, 90-item Symptoms Checklist; SWM, Spatial Working Memory; TBI, traumatic brain injury.
Six TBI patients and 26 HC received amyloid PET scans of which two and four were A positive, respectively. Groups did not significantly differ concerning age, sex, or education. TBI patients showed significantly lower scores on MMSE and had significantly higher BDI and SCL-90 scores. No significant differences in CANTAB domains were observed.
[ 18 F]MK-6240 in individual patients with TBI
[ 18 F]MK-6240 images are shown for all TBI patients in Figure 1. Visually, none of these patients showed a clear focal increase in tracer uptake in GM areas. Two patients (panels D and L) showed slightly increased global tracer uptake. Amyloid-positive TBI patients were those in panels C and L. For comparison, panel O shows an [ 18 F]MK-6240 SUVR image of a healthy control. As for a semiquantitative voxel-based analysis, all SUVR images were z-score transformed and a z-score of 2.5 was considered positive. As a result, in the TBI group a median of 2098 voxels (interquartile range [IQR]: 242–10524) were positive at this threshold whereas in the HC group, a median of 1024 voxels (IQR: 279–3407) were positive (p = 0.53).

[ 18 F]MK-6240 standardized uptake value ratios (SUVR) images from traumatic brain injury (TBI) patients and a healthy control. This figure shows lack of increased tracer uptake in TBI patients. Corresponding information is shown in Table 1. Amyloid positive TBI patients are shown in panels C and L. A healthy volunteer is shown in panel O. Images are shown in radiological convention.
[ 18 F]MK-6240 SUVR in TBI versus HC
Results of the VOI-based group comparison are shown in Figure 2. [ 18 F]MK-6240 SUVR was not significantly different between TBI patients and HC in any of the assessed VOIs (Table S2), nor between subgroups of moderate-severe TBI versus less severe TBI (Table S3). Voxel-based analysis indicated a cluster with higher [ 18 F]MK-6240 SUVR in the left cerebellum (according to automated anatomical labeling [AAL] atlas) in TBI patients than in HC (cluster pFWE = 0.049, kext = 1261 voxels).

[ 18 F]MK-6240 standardized uptake value ratios (SUVR) volume of interest (VOI)-based group comparison. This figure shows the results of the [ 18 F]MK-6240 SUVR VOI-based group comparison between healthy controls (HC) (shown in blue) and traumatic brain injury (TBI) patients (shown in red). Amyloid status of TBI patients is indicated as unknown (square), negative (open triangle), or positive (full triangle). HC subject with high mesotemporal [ 18 F]MK-6240 SUVR was amyloid negative.
Association with time since injury and clinical outcome
Time since injury was not significantly associated with [ 18 F]MK-6240 SUVR in the TBI group (Table S4).
Additionally, in the combined cohort of TBI patients and HC, RTI median five-choice movement time, SWM strategy, MMSE, BDI, and SCL-90 were not significantly associated with [ 18 F]MK-6240 SUVR in any of the assessed VOIs. On the other hand, OTS problems solved on first choice was significantly associated with [ 18 F]MK-6240 SUVR in the anterior cingulate VOI (rs = -0.38 ; p = 0.004; Fig. 3), mesotemporal VOI (rs = -0.38; p = 0.005), and thalamus VOI (rs = -0.34; p = 0.01) but not in any of the other assessed VOIs. PAL first attempt memory score was significantly associated with [ 18 F]MK-6240 SUVR in the anterior cingulate (rs = -0.30; p = 0.03; Fig. 3) but not in any of the other assessed VOIs. MTT multitasking cost was significantly associated with [ 18 F]MK-6240 SUVR in the frontal VOI (rs = -0.36; p = 0.008) (Table S5). Of note, upon outlier exclusion MTT multitasking cost remained significantly associated with [ 18 F]MK-6240 SUVR in the frontal VOI (rs = -0.35; p = 0.009). These correlations were also assessed within the TBI group separately. Here, RTI median five-choice movement time was significantly associated with [ 18 F]MK-6240 SUVR in the mesotemporal VOI (rs = 0.64; p = 0.02) and anterior cingulate (rp = 0.57; p = 0.03). SWM strategy was significantly associated with [ 18 F]MK-6240 SUVR in the mesotemporal VOI (rs = 0.58; p = 0.03). OTS problems solved on first choice was significantly associated with [ 18 F]MK-6240 SUVR in the anterior cingulate VOI (rp = -0.63; p = 0.02), and MMSE was significantly associated with [ 18 F]MK-6240 SUVR in the insula VOI (rs = -0.61; p = 0.02) (Table S6).
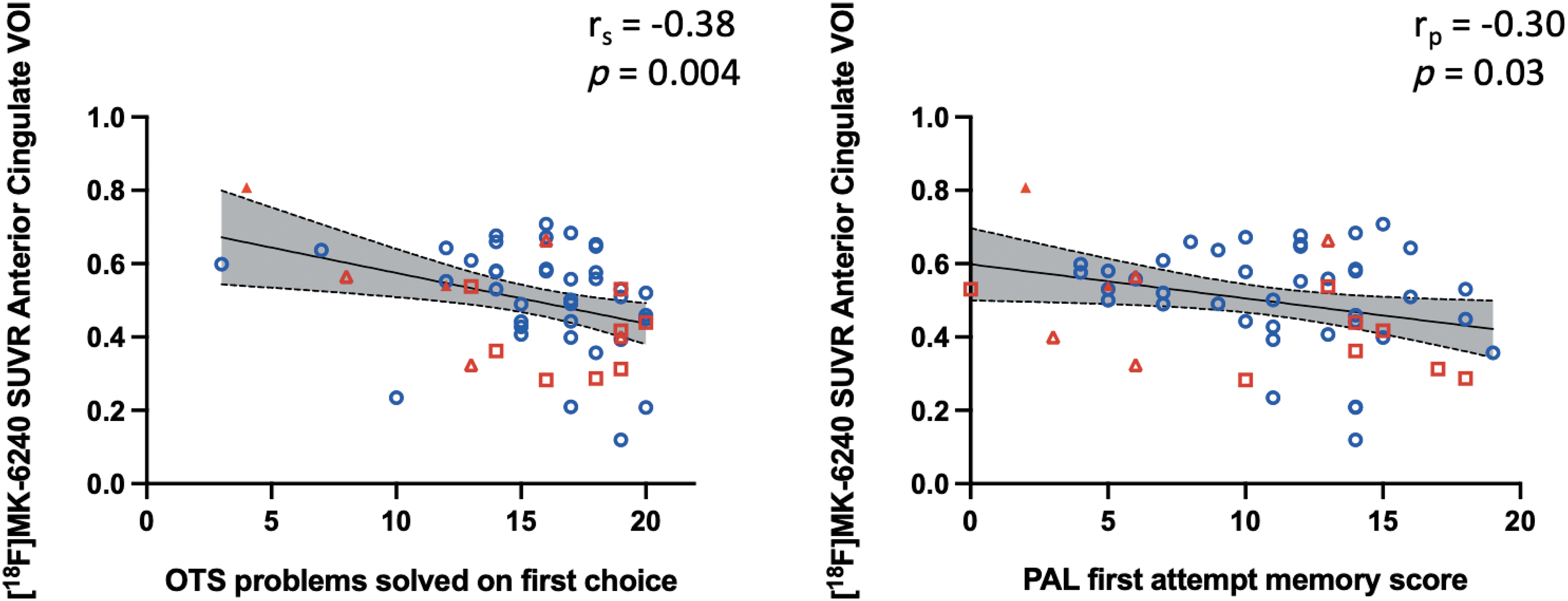
[ 18 F]MK-6240 standardized uptake value ratios (SUVR) volume of interest (VOI)-based correlations with neuropsychological test scores. This figure shows the significant correlations of [ 18 F]MK-6240 SUVR with neuropsychological test scores One Touch Stockings of Cambridge (OTS) problems solved on first choice and Paired Associates Learning (PAL) first attempt memory score. Correlation coefficients and p values denote correlation analysis within the combined cohort of traumatic brain injury (TBI) patients and healthy controls. Healthy controls are indicated in blue and TBI patients are indicated in red. Amyloid status of TBI patients is indicated as unknown (square), negative (open triangle), or positive (full triangle).
Discussion
In this study, we investigated NFT deposition at least 2 years after a single TBI using [ 18 F]MK-6240 PET. Our data showed no group differences in tracer uptake between TBI and HC, neither in terms of individual z-scores deviation volume, nor in a direct VOI-based or voxel-based group comparison. Our results are in agreement with a recent Australian study by Hicks and coworkers indicating no increased [ 18 F]MK-6240 binding at least 10 years after a single TBI. 25 Whereas Weiner and coworkers investigated tau changes in a mixed group of single and multiple TBI and found no significantly higher tau [ 18 F]Flortaucipir PET deposition compared with HC, 24 another study by Clark and coworkers also examined a mixed single/multiple TBI group and found an increase in cerebrospinal fluid (CSF) phospho-tau (p-tau) and total-tau (t-tau). 37 It has been shown in AD patients that CSF p-tau starts deviating from normal values before tau PET uptake increases, 38 which might also explain the discrepant findings between PET imaging and CSF measures in these mixed TBI cohorts. Interestingly, Wooten and coworkers assessed [ 18 F]Flortaucipir uptake across the frequency spectrum of TBI and found tracer uptake to be the highest in a patient who had sustained a single severe TBI 2.5 years prior to PET, whereas tracer uptake in most former contact sports athletes who sustained multiple TBIs was comparable to that in controls. 39 Therefore, severity of TBI might also be an important variable next to TBI frequency in subsequent tau accumulation after TBI.
The lack of increased [ 18 F]MK-6240 uptake after TBI in our study sample could be explained by several hypotheses. First, it could be caused by the true absence of NFTs where either no NFTs accumulated after a single TBI, NFTs were not formed yet, or the formed NFTs were already cleared. Little is known about the rate at which NFTs are formed. However, it has been shown that local replication, as opposed to spreading across brain regions, is the predominant process controlling the global rate of tau accumulation in AD. 40 As such, it might be possible that an NFT conformation is not (yet) formed but that toxic, soluble tau oligomers are present. However, a contribution of such tau oligomers cannot be investigated using [ 18 F]MK-6240 PET, because this tracer binds selectively to NFTs. 41 More specifically, [ 18 F]MK-6240 binds to 3R/4R NFTs as found not only in AD but also in CTE. 15 Therefore, if NFTs were formed after TBI in high concentration, they should have been visualized by the tracer. In addition, it is still unclear which factors such as TBI severity or location of the impact are crucial for the formation of NFTs after TBI. Concerning the hypothesis that NFTs were already removed, it has been demonstrated that clearance of tau oligomers and NFTs is mediated by proteasomal degradation and autophagy. 26,27 It is known that these clearance mechanisms are impaired in AD, but their functioning in CTE is yet to be elucidated and the rate at which tau clearance takes place is still unclear. Because a lack of increased tracer uptake at least 10 years after a single TBI was also shown by Hicks and coworkers, 25 it is unlikely that NFTs will still be formed during the years after the 2–10 year range that we examined here. Although this seems unlikely based on previous literature findings and suggested mechanisms, we cannot fully rule out the possibility that NFTs were formed early and in small quantities, but may have been cleared within the first 2 years after the injury.
Second, tracer uptake was quantified by means of SUVR. Therefore, perfusion changes are not considered in the quantification. We used the cerebellar cortex as a reference region as was previously validated in HC and AD, 36 and did not find a significant difference in partial volume corrected SUV in the cerebellar cortex between both groups (data not shown). Nonetheless, the validation of this reference region in TBI was not yet performed. It is of note that neuronal loss and sparse NFTs have been reported in the cerebellum in relation to CTE. 4,7 Although NFTs in the cerebellum in CTE are unlikely to confound PET analysis, to exclude the possibility that our findings were driven by our choice of reference region, we also quantified the images using pons as a reference region. 42 Results did not change and confirmed that no significant differences in tracer uptake could be found between the TBI and HC groups in any of the VOIs (data not shown).
Experimental animal studies have shown toxic tau oligomers shortly after a single TBI, 43 but to the best of our knowledge, tau imaging shortly after TBI has yet to be performed in humans. Importantly, disruption of the blood–brain barrier (BBB) can occur as a result of TBI, 4 which implicates that polar tracer metabolites can interfere with the PET signal, 44 making interpretation of such results challenging.
Within the combined cohort of TBI patients and HC, the scores of neuropsychological tests covering domains of executive functioning (OTS, MTT) and memory (PAL) were significantly associated with [ 18 F]MK-6240 SUVR. However, none of these associations remained significant after correction for multiple comparisons. Whereas many studies have shown significant correlations of the tau PET signal with cognitive outcomes in mild cognitive impairment or AD, 45 –48 these correlations were consistently lacking when examining TBI cohorts. 19,23 Additionally, CSF p-tau and t-tau were not associated with measures for executive functioning, verbal learning, or memory in a mixed single-multiple TBI cohort. 37 Moreover, the correlation we found between [ 18 F]MK-6240 SUVR and MTT multitasking cost (rs = -0.36; p = 0.008) is negative, whereas a positive correlation was expected because an increase in MTT multitasking cost scores indicates worse multitasking and was assumed to be correlated with increased [ 18 F]MK-6240 SUVR. This highlights the need for further investigation of the correlations of [ 18 F]MK-6240 SUVR with neuropsychological test scores in larger TBI samples.
This study comes with a number of limitations. The sample of TBI patients was quite small and heterogeneous, which might have resulted in insufficient power to demonstrate differences on the group level. However, our z-score analysis together with a thorough visual inspection of the images supported our group-level findings that are concordant with the results obtained by Hicks and coworkers. 25 Because of the small subset of patients who received an amyloid PET scan, the influence of amyloid plaques on tau deposition as measured by [ 18 F]MK-6240 could not be evaluated and requires further investigation. However, both patients with positive amyloid PET were >60 years of age, so the chance of amyloid positivity as part of the normally increased incidence with ageing is possible. 49 In addition, genotyping for apolipoprotein E (ApoE), of which the presence of the ApoE ɛ4 allele increases the risk of developing sporadic AD, 50 was not performed. It has been hypothesized that for subjects who are genetically predisposed to develop AD pathology, sustaining a TBI could increase susceptibility to developing NFTs, 13,51 although this was contradicted by others. 7,52 Last, as mentioned, tracer quantification was performed using SUVR, which does not account for tracer influx and washout and can therefore be influenced by perfusion changes. Nonetheless, it was previously demonstrated that late-time point [ 18 F]MK-6240 SUVR is closely correlated to full dynamic tracer quantification, 36 and that perfusion changes of ±25% only slightly influence [ 18 F]MK-6240 SUVR quantification. 53 Moreover, as patients were scanned at least 2 years after their TBI, changes in BBB permeability at this time point are unlikely.
Conclusion
In conclusion, we found no group-based increase of [ 18 F]MK-6240 brain uptake in patients scanned at least 2 years after a single TBI compared with healthy volunteers, which suggests that no NFTs are building up in the first years after a single TBI. However, significant correlations with cognition scores were found that warrant further investigation in a larger sample.
Transparency, Rigor, and Reproducibility Summary
The study was pre-registered at
Footnotes
Acknowledgments
We thank all the participants for their willingness to participate in this study. We are grateful to the PET-MR technologists, in particular Kwinten Porters and Jef Van Loock for their contribution in data acquisition. We also thank the PET radiopharmacy team and nuclear medicine medical physics team for their skilled contributions.
Authors' Contributions
K.V.L., M.V., R.L., G.V., and L.M. contributed to study concept and design. K.V.L. and M.V. supervised the study progression. G.V., L.M., B.D., J.V.W., and D.L. recruited study participants. G.V. and L.M. contributed to data acquisition. G.V., L.M., M.K., M.V., and K.V.L. contributed to data analysis and interpretation. K.V.L., R.L., and M.V. obtained funding. G.V. and K.V.L. drafted the manuscript. Manuscript revision was performed by all authors.
Funding Information
This study was supported by a Fonds Wetenschappelijk Onderzoek (FWO) grant (FWO/G093218N) and by KU Leuven internal C2 funding (C24-17-063).
Author Disclosure Statement
K.V.L. and R.L. performed this study as senior investigators of FWO Flanders. K.V.L. is an advisory board member of Cerveau and has received fees through KU Leuven for consultancy activities for GE Healthcare. K.V.L. and M.K. have performed contract research through KU Leuven for Merck, Janssen Pharmaceuticals, UCB, Cerveau, Syndesi, Eikonizo, GE Healthcare, Cerevel, BMS, and Curasen. No other potential conflicts of interest relevant to this article exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.