
Abstract
Although there is significant variability in the manifestations of persisting post-concussive symptoms (PPCS), autonomic dysfunction has been reported to contribute to PPCS and could serve as a biomarker of recovery. The objective of this study was to evaluate cardiac autonomic reflexes and autonomic function after concussion injury comparing those with prolonged concussion symptoms to those without. This is a case-control study where a non-referred population of concussed children or adolescent participants were enrolled from the Emergency Department (ED) of the Stollery Children's Hospital, a tertiary pediatric hospital in Edmonton, Alberta, Canada. Children and adolescents 8 through <18 years of age who presented with mild traumatic brain injury were diagnosed with concussion. Our study reported concussion symptoms and standardized clinical cardiac autonomic reflex testing at 4 and 12 weeks after injury. Our findings showed that 28 participants with concussion completed the 4-week follow-up questionnaires, and that 17 (61%) were diagnosed with PPCS. Difficulty concentrating, fatigue, noise sensitivity, light sensitivity, and headache were most commonly reported at baseline among those who were later diagnosed with PPCS. The mean change in heart rate (HR) with head-up tilt was 44.2 bpm (standard deviation [SD] 9.1) in the non-PPCS group and 46.6 bpm (SD 14.1) in the PPCS group at 4 weeks and was not significant in the unadjusted (p = 0.2) or adjusted analysis for age and female sex (p = 0.2). Overall, 70% (19/27) had significant orthostatic tachycardia >40 bpm, but PPCS and non-PPCS groups were similar. Similar results were observed among 23 participants at 12-week follow-up. The median maximum decrease in systolic blood pressure (SBP) with head-up tilt was -26.9 mm Hg (interquartile range [IQR] -32.6, -22.3) in the non-PPCS group and -25.1 mm Hg (IQR -32.2, -18.2) in the PPCS group, and was not significantly different in the unadjusted (p = 0.8) or adjusted (p = 0.8) analysis. Overall, 19 of 26 participants (73%) demonstrated orthostatic hypotension (SBP change >20 mm Hg) with no significant difference between the PPCS and non-PPCS groups. Similar results were observed at 12-week follow-up. In conclusion, cardiac autonomic reflex responses are abnormal in most children and adolescents with a concussion injury at 4- and 12-week follow-up and may reflect ongoing autonomic dysfunction. However, autonomic function did not differentiate PPCS, indicating that reported symptoms are not sensitive to autonomic abnormalities.
Introduction
Persisting post-concussive symptoms (PPCS), often defined as concussion symptoms lasting >4 weeks, present a significant diagnostic and management challenge. 1 Although there is significant variability in the manifestations of PPCS, headache, dizziness or lightheadedness, and cognitive impairment are those most reported. 2 Although symptoms of dizziness may represent vestibular dysfunction, many report lightheadedness with postural changes such as standing up, 3 suggesting the presence of autonomic dysregulation.
Disturbance of normal autonomic dysfunction has long been implicated in concussion and may contribute to the persistence of post-concussion symptoms. 4 Autonomic dysfunction may underlie a number of concussion symptoms including headache, anxiety, cognitive impairment, mood disorders, and sleep disturbances. 5 Although studies have explored the relationship between concussion and autonomic nervous system (ANS) dysfunction using methods such as heart-rate variability, 6 few studies have employed a standard clinical autonomic testing paradigm, and even fewer have explored whether normalized autonomic function correlates with symptom improvement. In one clinic referral population of patients with persistent concussion symptoms and lightheadedness, head-up tilt was abnormal in 24 of 34 (70%) participants. 7 Among those with abnormal results on the head-up tilt test, 14 were observed to have significant postural orthostatic tachycardia >40 beats per minute, and a reduction in postural tachycardia was associated with reduced concussion symptoms.
To explore the relationship between concussion and PPCS, we undertook a study to evaluate a non-referred population of concussed children or adolescents with and without persistent concussion symptoms. We also explored in follow-up whether PPCS correlated with autonomic function over time. We hypothesized that those with PPCS would demonstrate more evidence for autonomic dysregulation than those who did not exhibit prolonged symptoms 4–12 weeks after their injury. A better understanding of the underlying mechanisms associated with PPCS may suggest new opportunities for management or inform return to activity advice.
Methods
Study objectives
Our primary objective was to evaluate the regulation of heart rate (HR) and blood pressure (BP) in response to head-up tilt and other provocative maneuvers to measure cardiovascular autonomic function in children and adolescents with a history of concussion. All participants were diagnosed with concussion and in the emergency department (ED) at the time of diagnosis. Participants were evaluated at 4 and 12 weeks after their concussion and separated into two cohorts with and without PPCS. Secondary objectives included: (1) to assess the relationship between postural dizziness or lightheadedness (i.e., orthostatic intolerance) as a specific concussion symptom and physiologic changes in HR and BP and (2) to objectively assess other cardiac autonomic reflexes including Valsalva and HR variability (HRV) in response to respiration as well as quantitative measures of post-ganglionic sympathetic sweat function.
Inclusion and exclusion criteria
Participants were enrolled from the Stollery Pediatric ED, a tertiary referral pediatric hospital in Edmonton, Alberta, Canada. Children and adolescents 8 through <18 years of age presenting with mild traumatic brain injury and diagnosed with concussion as defined by the Zurich consensus statement 2012 8 were eligible and invited to participate. The Post-Concussion Symptom Inventory (PCSI) was collected at the time of enrolment and then again at 4- and 12-week follow-up. PPCS were defined as an increase from pre-concussion baseline of three or more symptoms on the validated PCSI at 4 weeks (consistent with the International Classification of Diseases, 10th Revision [ICD-10] definition of PPCS). All participants had sustained a concussion, and we compared those with PPCS at 4 weeks after their injury with those without PPCS.
Participants were required to be proficient in English. Children or adolescents with the following criteria were excluded: (1) other clinically significant neurological disease that may affect the autonomic nervous system (i.e., structural cerebral abnormalities, cerebral palsy, congenital central hypoventilation, Prader-Willi syndrome, Riley-Day syndrome, spinal cord lesion, or other peripheral neuropathy); (2) concomitant use of medications known to interfere with HR and BP responses that may affect the autonomic nervous system) if these medications could not be discontinued for at least 1 week prior to cardiac autonomic reflex testing; and (3) inability to stand on tilt table or understand testing procedures and instructions.
Concussion was defined as: (1) a direct blow to the head, face, neck, or elsewhere on the body with an impulsive force transmitted to the head, resulting in one or more of the symptoms in one or more of the following clinical symptom domains (which may or may not have involved loss of consciousness) within the past 48 h; (2) somatic symptoms (e.g. headache, nausea, loss of balance, dizziness, sensation to light or noise, visual problems, and clumsiness); (3) cognitive symptoms (e.g., feeling as if in a fog, difficulty concentrating or remembering, answering questions more slowly and being confused with directions/task); (4) emotional/behavioral symptoms (e.g. being irritable, sad, or nervous or experiencing emotional lability), physical signs (e.g. loss of consciousness and amnesia); or (5) sleep disturbance (e.g. sleeping more, or experiencing fatigue, drowsiness, and insomnia).
Study Design
The protocol was developed as a sub-study of the Predicting Persistent Post-Concussive Problems in Pediatrics (5P study), 1 in which the primary objective was to derive a decision rule to predict PPCS at 4 weeks after presenting to the ED with concussion. Eligible participants presenting to the ED and diagnosed with concussion were approached for participation in the parent study and this sub-study, and those who agreed to participate and signed informed consent and assent were scheduled for cardiac autonomic reflex testing in the Pediatric Autonomic Function Laboratory at the Stollery Children's Hospital 4–6 weeks following their concussion injury. Baseline demographic data were collected in the ED as well as the parent and participant PCSI.
At 4–6 weeks and 12–14 weeks after the injury, participants completed the PCSI and the Autonomic Symptom Profile (Supplementary Appendix A) with the help of their parents. Cardiac autonomic reflex testing (which will be described) was performed at both time points. Autonomic testing was performed in the mornings in a quiet room with a room temperature between 21 and 22°C. The participants were asked to get a good night's rest before the procedure and eat a normal breakfast and drink their usual volume of fluids.
The PCSI and Autonomic Symptom Profile assess many symptoms commonly observed in disorders of autonomic function. The Autonomic Symptom Profile was collected at 4- and 12-week follow-up. The frequency of symptoms commonly associated with autonomic dysfunction is reported on an ordinal scale as follows: 0 ∼ Never, 1 ∼ 1–5 times per month, 2 ∼ 6–15 times per month, 3 ∼ 16–20 times per month, and 4 ∼ daily. Data are presented as a visual heat map illustrating the median of the ordinal scale for each symptom comparing both groups.
Cardiac autonomic reflex testing
Standardized clinical cardiac autonomic reflex tests were performed, including Valsalva maneuver (assessing the ratio of the greatest HR during Valsalva and lowest HR after Valsalva; a measure of cardiovagal function), deep breathing at six breaths per min (assessing the mean difference in HR with each respiration; a measure of cardiovagal function), head-up tilt to 70 degrees (assessing change in HR and BP; a measure of cardiovagal and sympathetic function), and sudomotor/sweat function (assessing small fiber nerve function to sweat glands). Continuous single-lead electrocardiogram, non-invasive continuous blood pressure (Finapres®, Amsterdam, The Netherlands), and integrated digital signal-recoding platform (WR TestWorks®, Stillwater, Minnesota and LabChart®, Powerlab, ADInstruments, Colorado Springs, CO) were used. The standard procedures performed on each participant while supine included deep breathing at six breaths per min for 10 breaths followed by the Valsalva maneuver with a pressure of 40 mm Hg held for 10 sec with a minimum 5-min rest period in the supine position before or between each maneuver. The head-up tilt to 70 degrees for 10 min was performed next using a mechanized tilt table while continuously recording HR and BP. The final procedure performed on each participant was Quantitative Sudomotor Axon Reflex Test (QSART) to quantitate the sudomotor (i.e., sweat) response to acetylcholine, which provides a measure of post-ganglionic sympathetic nerve function. The QSART device (Q-Sweat, WR Medical Inc., Stillwater, MN) recorded the sudomotor response in four sites (forearm, proximal leg, distal leg, and foot) on the same side simultaneously. 9
Primary outcomes and sample size estimate
Participants diagnosed with PPCS at 4 weeks were compared with those without PPCS at 4 weeks. The primary outcome variables were the change in HR and systolic BP (SBP) in response to 70 degree head-up tilt. Whereas a change in HR of 30 bpm with head-up tilt is considered abnormal in adults, a change of 40 bpm is considered abnormal in adolescents (13–17 years) and children (6–12 years) based on population-based data and consensus opinion. 10,11 A sustained decrease in SBP with head-up tilt of >20 mm Hg is defined by consensus as orthostatic hypotension. 12,13 A difference >20 bpm in the HR change with head-up tilt was considered a clinically meaningful difference between groups with and without PPCS at 4 weeks. The standard deviation (SD) of HR changes within 3 min of head-up tilt observed in our laboratory is 18. A difference of 15 mm Hg between groups was considered a clinically meaningful difference for the reduction in SBP with head-up tilt, and our laboratory SD for this measure is 13. With these parameters, a total sample size of 22 (i.e., 11 cases and 11 controls) was estimated to provide 80% power to detect the estimated clinically meaningful differences between groups. In anticipation that some patients would be lost to follow-up or would not complete the testing, we planned to enroll a total of 30 participants which would provide 90% power to detect a difference between groups as defined.
Statistical methods
Descriptive statistics were used to summarize the patient characteristics and clinical presentation. Initially, Wilcoxon tests were applied to provide an unadjusted comparison of study outcomes at weeks 4 and 12 between exposure groups (PPCS vs. no PPCS). Then multi-variable linear regressions were fitted to estimate group differences in outcomes while adjusting for age and sex, and to enable comparison of estimated outcome means (for each sex/group combination, with age set to its mean) against normative value (as null). Finally, a series of Wilcoxon tests were performed to examine the cross-sectional relationship between our study outcomes (autonomic measure) and five specific PCSI items (headache, balance, dizziness, nausea, general difference) at week 4. All statistical analyses were performed with R software (version 4.0.5).
Results
Participant characteristics
In total, 30 participants consented to participate in the study. Two withdrew from the study before completing any study procedures at 4 weeks. Twenty-eight participants completed the 4-week follow-up questionnaires, of which 17 were diagnosed with PPCS and 11 did not have PPCS. Primary outcome data was available for 27 participants at the 4 week follow-up and 23 participants at 12 week follow-up. Baseline characteristics comparing groups with and without PPCS are presented in Table 1. As was observed in the 5P study, a greater proportion of females were later diagnosed with PPCS. 1 A subset of PCSI symptoms is listed and presented as a heat map in Figure 1, comparing groups diagnosed with PPCS at baseline, and at 4- and 12-week follow-up. The heat map provides a visual representation of greater symptom burden at baseline among participants who were later diagnosed with PPCS at 4 weeks. To a lesser degree, the greater symptom burden persisted at 4 and 12-week follow-ups.
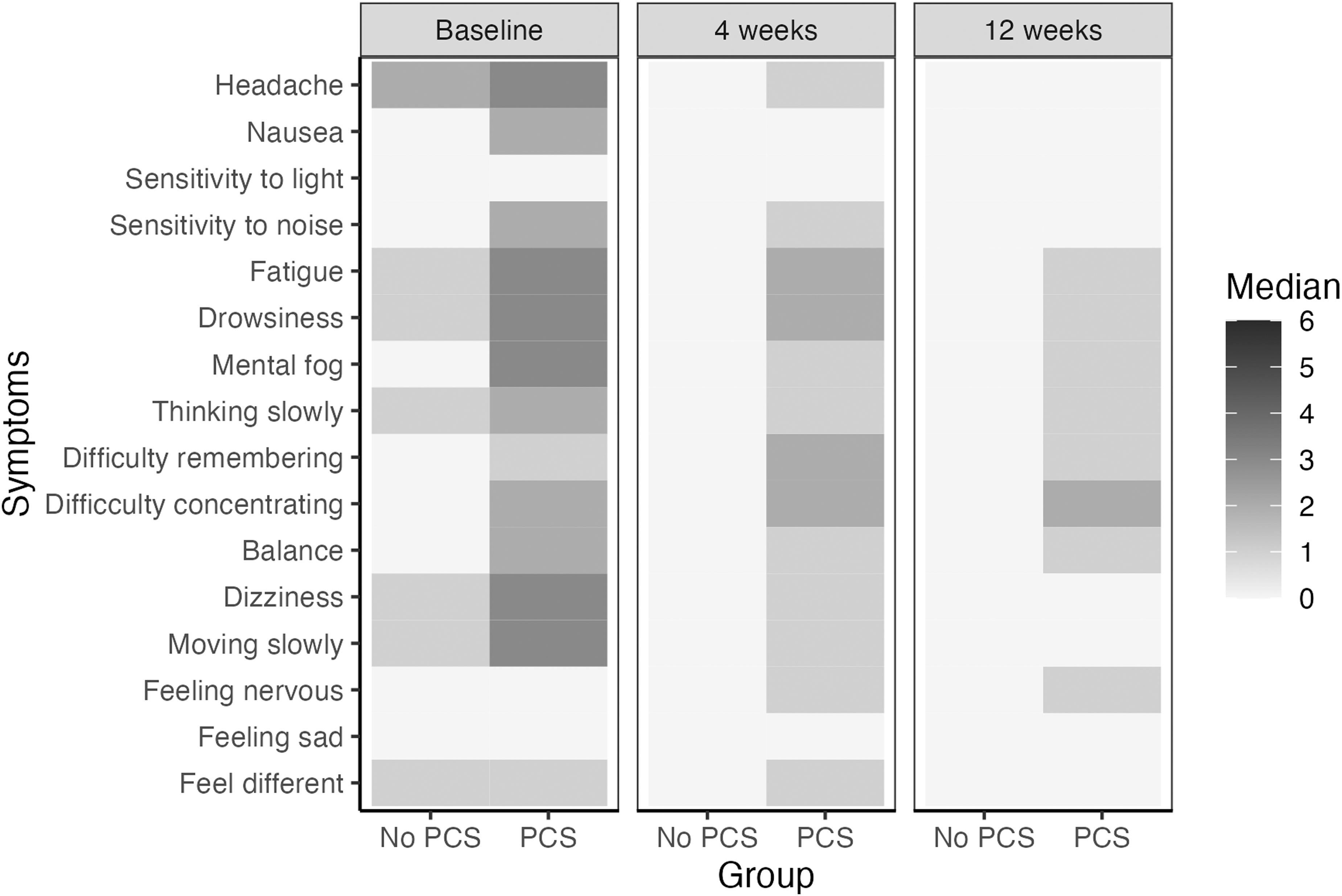
Median reported levels presented as a heatmap on selected symptoms reported in the Post-Concussion Symptom Inventory (PCSI) at baseline, 4-weeks, and 12-weeks follow-up. Symptoms are reported on an ordinal scale from 0 to 6 with 0 = Not a problem, 3 = Moderate problem, and 6 = Severe problem.
Baseline Characteristics of Children or Adolescents With and Without Persistent Concussion Symptoms at 4 Weeks Post-Injury
n (%)
Fisher's exact test
PPCS, persisting post-concussive symptoms
Figure 2 visually illustrates the group differences in the median frequency of reported symptoms on the Autonomic Symptom Profile using an ordinal scale at each time point and presented as a heatmap. Our study was not powered to detect group differences among individual reported symptoms. Using a conservative simple Bonferroni correction for multiple comparisons (n = 16) we observed that difficulty concentrating, sensitivity to noise, and sensitivity to light were more commonly reported symptoms at baseline among those who were later diagnosed with PPCS, each with a significance level of p ≤ 0.003 on a heatmap of the Autonomic Symptom Profile.
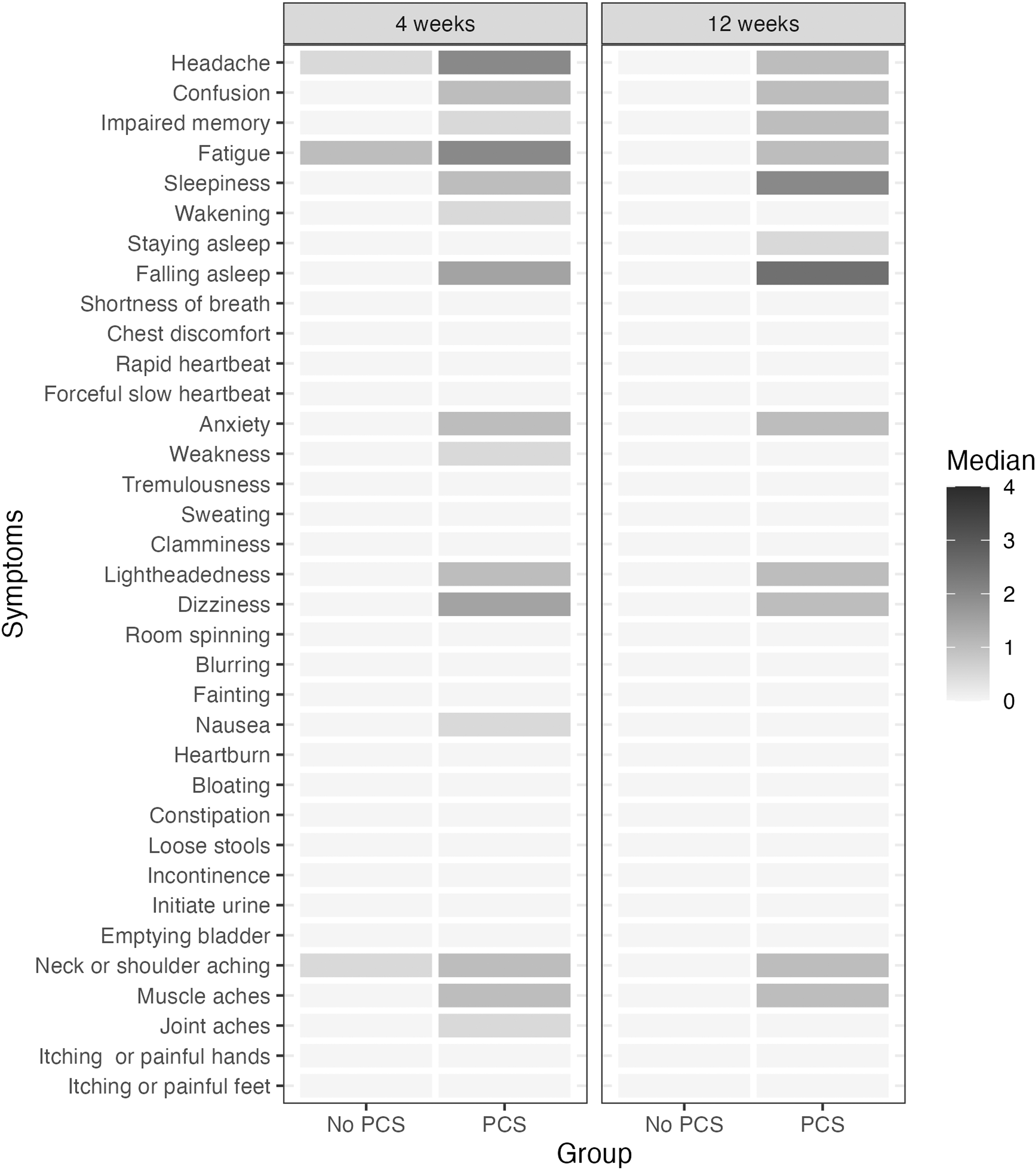
Median reported levels presented as a heatmap on symptoms reported in the Autonomic Symptom Profile with the frequency of symptoms reported as 0 = Never, 1 = 1–5 times per month, 2 = 6–15 times per month, 3 = 16–20 times per month, and 4 = daily.
Visually there appeared to be a higher frequency of autonomic-related symptoms among those diagnosed with PPCS at 4 weeks versus those who were not, and this persisted at the 12-week follow-up.
Change in HR with head-up tilt at 4- and 12-weeks post-concussion
The mean change in HR with head-up tilt is presented in Figure 3a. A normal change in HR with head-up tilt in children or adolescents is <40 bpm as depicted in the figure. The mean increase in HR with 70 degree head-up tilt was 44.2 bpm (SD 9.1) in the non-PPCS group and 46.6 bpm (SD 14.1) in the PPCS group at 4 weeks after the concussion injury. The was no significant difference between groups for the unadjusted analysis (p = 0.2). In the adjusted analysis controlling for age (years) and female sex using simple linear regression, there was also no significant difference between groups (p = 0.2). However, the overall mean change in HR in both groups was 45.8 bpm (95% confidence interval [CI] 40.9–50.7) and was significantly greater than 40 bpm (p = 0.02).
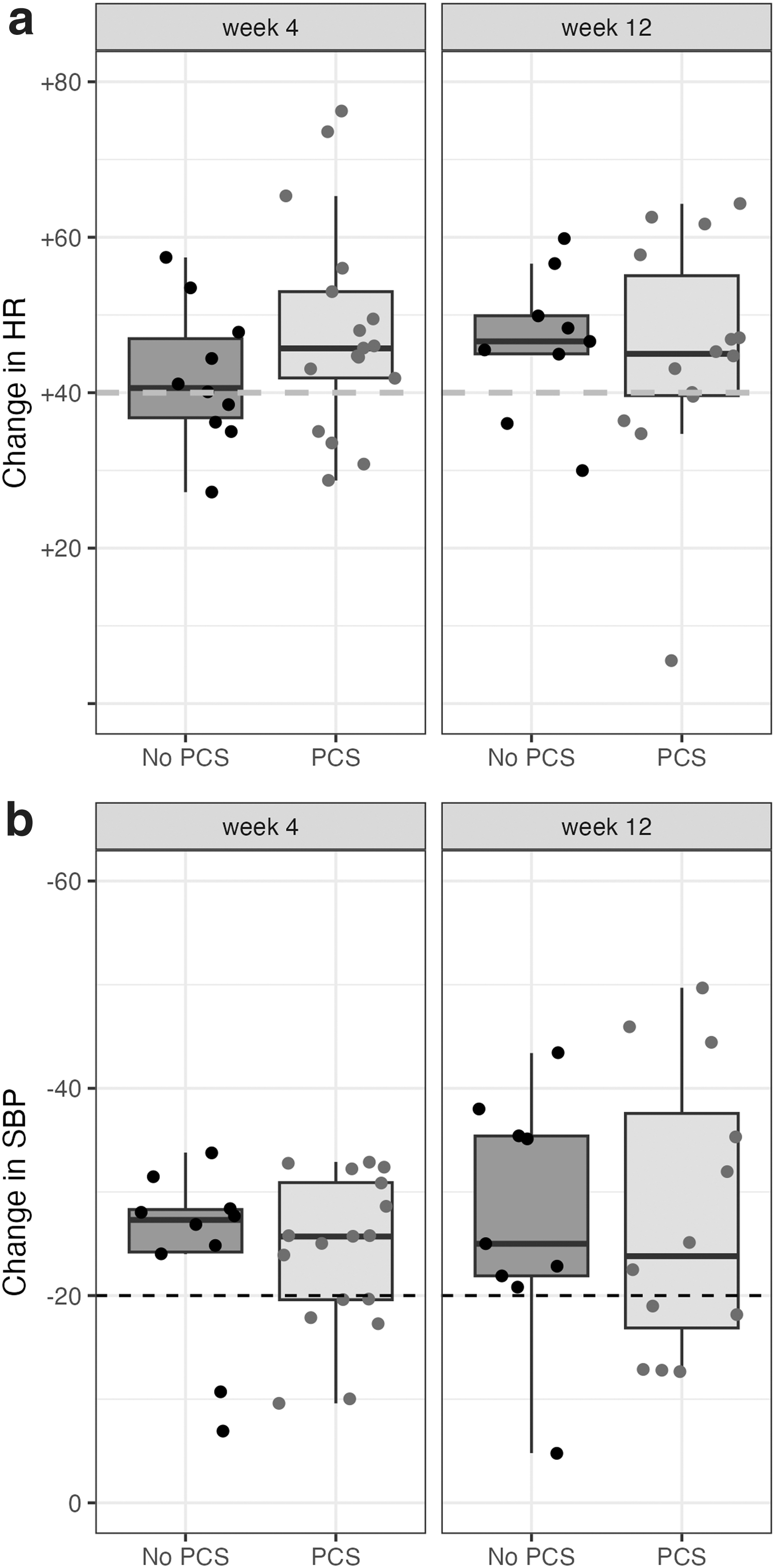
At week 12, data for change in HR with head-up tilt was available for 23 participants. The difference in means between groups was not significantly greater than 0 in the unadjusted analysis using the non-parametric Wilcoxon rank sum test because of non-normal distribution (W = 67, p = 0.8). The log of HR change was also not significantly different between groups when controlling for age and female sex in the adjusted analysis (p = 0.3). However, the overall median change in HR with head-up tilt was 45.5 (interquartile range [IQR] 39.8, 53.2) and was statistically significantly greater than 40 bpm (V = 200, p = 0.01)
Table 2 summarizes additional derived and secondary measures, including orthostatic intolerance grading scale, presence of orthostatic tachycardia >40 bpm, presence of orthostatic hypotension <20 mm Hg, HR change with deep breathing, and ratio between the lowest and highest HR with Valsalva held at 40 mm Hg. In summary, there were no significant differences in any of the measures when comparing those with and without PPCS. However, 70% (n = 19/27) overall met physiological criteria for postural orthostatic tachycardia with an increase in HR >40 bpm at week 4, and 74% (n = 17/23) met the criteria at 12 weeks.
Cardiac Autonomic Reflex Responses to Valsalva, Deep Breathing, and Head-Up Tilt
n (%); median (interquartile range [IQR])
Fisher's exact test; Wilcoxon rank sum test
Fisher's exact test; Wilcoxon rank sum exact test; Wilcoxon rank sum test
PPCS, persisting post-concussive symptoms; HR, heart rate; BP, blood pressure.
Change in SBP and orthostatic hypotension with head-up tilt
The change in systolic BP with head-up tilt is presented in Figure 3b and illustrates no significant differences between those with and those without PPCS. At the 4-week follow-up, the median decrease in systolic BP with head-up tilt was -26.9 mm Hg (IQR -32.6, -22.3) in the non-PPCS group and -25.1 mm Hg (IQR -32.2, -18.2) in the PPCS group. The unadjusted (W = 80, p = 0.8) and adjusted analysis for age (years) and female sex (p = 0.8) were not significant. Overall, 19 of 26 participants (73%) demonstrated orthostatic hypotension at 4 weeks on head-up tilt defined as a decrease in systolic BP >20 mm Hg. At 4 weeks, the overall median decrease in systolic BP was -25.8 mm Hg (95% CI -29.8, -19.7) with was significantly less than -20 mm Hg (V = 90, p = 0.01). Similarly, at 12 weeks, the overall median decrease in systolic BP was -25.0 mm Hg (IQR, -35.4, -19.00) and was significantly less than -20 mm Hg (V = 49, p = 0.01).
HR variability
Measures of short-term (5 min) heart rate variability calculated from the HR signal at rest are presented in Table S1. All measures in the time domain were consistently lower in the PPCS group compared with the non-PPCS group, but group differences were not statistically significant. Similarly, the low frequency (LF) and high frequency (HF) bands in the frequency domain were lower in the PPCS group, but the differences were not statistically significant. The LF/HF ratio was higher in the PPCS group at rest. Group differences were not statistically significant when adjusting for multiple comparisons using the Bonferroni method (p < 0.003).
Measures of HR variability were compared between head-up tilt and rest by subtracting short-term measures at rest from tilt. Group comparisons at 4 and 12 weeks are presented in Table S2. No statistically significant group differences were observed. The direction of change was consistent for differences, in the time being lower in the PPCS group than in the non-PPCS group.
QSART
Data for the QSART are presented in Table S3. There were significant missing data for QSART at the arm and foot for technical reasons (i.e., the iontophoresis device was inconsistently functioning producing unreliable results). The quality of data at the proximal and distal leg was better. No statistically significant differences were observed between groups for the 4- and 12-week follow-ups.
Discussion
Our observations failed to support our original hypothesis that symptom recovery after concussion or PPCS correlates with cardiac autonomic dysregulation. However, we surprisingly observed that most concussed participants, with or without PPCS, demonstrated significantly abnormal cardiac reflex control of HR and BP in response to head-up tilt. Almost 90% of the entire cohort met physiological criteria for postural orthostatic tachycardia with a sustained increase in HR >40 bpm with head-up tilt and we did not observe a significant difference between those with and those without PPCS. Most of these observations persisted at 12 weeks following the original concussion injury, whether PPCS symptoms were reported or not.
The presence and persistence of abnormalities in cardiac autonomic control supports the hypothesis that autonomic dysregulation underpins some aspects of the physiological response to concussion. However, we did not observe a significant association with PPCS, suggesting that autonomic dysregulation is not the prevailing predictive factor. Other factors, such as a prior history of migraine, recurrent brain injury, or sex, have a much stronger association with prolonged symptoms after a concussion, 1 and may have unique pathophysiological pathways.
Compared with in previous studies, all our study participants had sustained a concussion, and we compared those with and those without PPCS. Several studies have reported autonomic dysregulation following concussion, and suggest that the dysregulation may underlie many of the classic symptoms of concussion. 5,14 Most studies have used HR variability to measure autonomic function, while a smaller number report on cardiac autonomic reflexes or cerebral blood flow velocity. 15 Our observations for HR variability were not significantly different between those with and those without PPCS. Also, our short-term measures at rest (Table S1) would generally fall within a normal expected range based on reported normative data. 16,17 Overall previous studies of HR variability in concussion report variable levels and types of autonomic dysregulation, with little consistency among studies. Moreover, HR variability as a quantitative measure of autonomic function presents many potential pitfalls, are difficult to interpret in isolation, and are influenced by numerous factors such as time of day, sleep, mood, and diet. 18
Orthostatic intolerance is a defining symptom in many disorders of autonomic regulation such as postural orthostatic tachycardia syndrome (POTS). Orthostatic intolerance is defined as the development of symptoms such as dizziness or lightheadedness on standing that are relieved by recumbence. In a recent study, concussed adolescents reported orthostatic intolerance at a much higher rate than non-concussed controls (37% vs. 4%), but they did not observe a differential rate in orthostatic hypotension. 19 We observed a relatively high rate of orthostatic intolerance of 39% for the whole group at 4 weeks. More than 50% of the PPCS group reported at least mild orthostatic intolerance, but <20% in the non-PPCS group did. Group differences were not statistically significant at 4 weeks, likely because of the small sample size, but at 12 weeks were at the 5% level of significance. Using continuous non-invasive BP in a specialized autonomic laboratory, we also observed early orthostatic hypotension in almost 40% of participants at 4 weeks after their concussion, with no significant difference between groups. However, orthostatic hypotension decreased to ∼22% at 12 weeks, suggesting some recovery.
Very few studies have used traditional clinical assessments of cardiac autonomic reflex control on HR and BP. These studies typically require specialized equipment such as continuous non-invasive blood pressure monitors. The study by Heyer and coworkers 7 examined a cohort with PPCS and used testing procedures similar to ours comparing those with a history of syncope and those diagnosed with POTS with those without syncope or POTS. Participants with PPCS and symptoms of lightheadedness had high rates of comorbid diagnoses of syncope and POTS. Not surprisingly, patients diagnosed with POTS also demonstrated significant postural changes in HR. Their cohort did not include participants without PPCS. Unlike in our study, they observed a correlation between the recovery from PPCS and resolution of POTS.
Numerous pathophysiological models have been suggested that link autonomic dysregulation to concussion symptoms and PPCS. 5 Some of these include exaggerated sympathetic activation leading to inflammation and oxidative stress as well as perturbations in cerebral blood flow. The possible link between cerebral flow and orthostatic intolerance following concussion has been suggested by others, 20 but interestingly, measures of cerebral blood flow velocity using transcranial Doppler are not consistently abnormal in patients with POTS. 21 A satisfactory unifying mechanism that explains symptoms of reduced cerebral perfusion on standing (i.e., orthostatic intolerance) especially in the context of normal SBP, has not been offered. Alterations in cerebrovascular reactivity, brain perfusion, or energetic requirements of the brain following concussion – all much more difficult to measure – may need to be explored in future studies.
Measures of cardiac autonomic control may provide a biomarker of recovery from concussion and help to inform return to activity advice. In our study, reported symptoms did not correlate with normalized autonomic regulation. Participants without PPCS continued to demonstrate significant aberrations in autonomic control 4 and 12 weeks after injury. The concussed participants had not yet returned to their presumably normal, pre-injury, homeostatic state, despite the absence of PPCS, raising concern that symptom reporting alone may not correlate with physiological recovery from concussion.
Limitations
Limitations of our study are the relatively small sample size of 26 participants with primary outcome data, with some additional loss to follow-up at 12 weeks, and reduced power to detect a clinically meaningful difference between groups. No pre-injury testing was available given our study design. We also recruited from a single tertiary center. which may limit the generalizability of our findings. While the use of standardized measures of autonomic reflex control is a strength of our study, the need for specialized equipment and laboratory testing conditions may have influenced some of our observations based on anxiety or other participant factors. The testing procedures were however identical to our standard clinical autonomic testing.
Conclusion
Significant autonomic cardioregulatory abnormalities of postural tachycardia were observed in most participants with a concussion, and did not correlate with the presence or absence of PPCS. Autonomic control of cardiac reflexes on HR and BP may serve as a more sensitive biomarker of ongoing physiological dysregulation after concussion independent of reported symptoms. The clinical utility of these observations requires further assessment.
Footnotes
Transparency,Rigor,and Reproducibility Summary
This study protocol for the primary study entitled Predicting and Preventing Postconcussive Problems in Paediatrics (5P) study was published in an open access journal. 1 The study presented here was a single site sub study. The analysis plan was not formally pre-registered. A total sample size of 30 participants was estimated to provide a 90% power to detect a clinically meaningful difference between groups (defined as a difference in HR of 20 bpm or SBP of 15 mm Hg with head-up tilt). Enrolment continued until the target sample size was completed. Statistical analysis and/or review was performed by Ken Tang, who has the appropriate qualifications including a PhD in clinical epidemiology and bisotatistics.
Both the original measures of statistical error rates and corrected measures of statistical error rates have been reported in the text. To our knowledge, no replication or external validation studies have been performed or are planned/ongoing at this time. De-identified individual participant data (including data dictionaries) will be made available in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to
Data Sharing Statement
De-identified individual participant data (including data dictionaries) will be made available in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to lricher@ualberta.ca
Authors' Contributions
Lawrence Richer conceptualized and designed the study, applied for funding, performed data coordination and analysis, drafted the original manuscript, and approved the final manuscript as submitted. William Craig enrolled participants, reviewed data analysis, drafted the manuscript, and approved the final manuscript as submitted. Meghan Lindsell enrolled participants, performed autonomic studies and data analysis, and approved the final manuscript as submitted. Ken Tang performed data analysis and interpreted results, drafted the original manuscript, and approved the final manuscript as submitted. Roger Zemek led the parent study and conceptualized, and designed this study, applied for funding, performed data coordination and analysis, drafted the original manuscript, and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding Information
This study was partially funded by the Canadian Institute of Health Research (CIHR) Operating Grant (MOP: #126197) as well as by a CIHR mild traumatic brain injury team grant (TM1: #127047) and research support funding from the Women and Children's Health Research Institute. The funder/sponsor played no role in the conduct, analysis, and write-up of this study.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix A
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.