
Abstract
Concussion often results in psychological symptoms, including anxiety. Post-concussion anxiety has been well documented, although much of this research has focused on collegiate athletes. The purpose of this study was to compare (1) anxiety symptoms in concussed and healthy controls over time and (2) to explore sex differences in post-concussion anxiety within the context of pubertal development. Participants (N = 126, mean age = 15.1 years old), including concussed (n = 86) and healthy adolescents (n = 40), completed the Pubertal Development Scale (PDS) and the Screen for Child Anxiety and Related Disorders (SCARED-C). The concussed groups completed SCARED-C at three visits (
Introduction
Concussion is a major public health concern that affects approximately 33 million children and adolescents each year worldwide. 1 These injuries are heterogenous and may involve a myriad of symptoms and impairments that reflect different subtypes, including anxiety/mood, cognitive, headache/migraine, ocular, and vestibular. 2,3 Adolescents may be at particular risk for protracted concussion recovery because of ongoing brain development, including incomplete myelination, as well as increased acceleration-deceleration forces from reduced neck strength. 4 –6 Consequently, they may take on average 30 days to recover compared with young adults who often recover in 7–10 days. 7 –9
Researchers have demonstrated that concussion often results in psychological symptoms including depression, anxiety, and irritability. 10,11 Researchers have reported higher rates of post-concussion anxiety compared with post-concussion depression. 12 A variety of explanations have been posited for how concussion has been associated with anxiety, including overaction of the behavioral inhibition system, the physiological mechanism responsible for individuals' responses to situations that may result in consequence or punishment. 13,14
Hypervigilance and rumination of symptoms 10,15,16 and a potential for a neurological predisposition to fear-conditioning after concussion may result in increased anxiety. In addition, post-concussion vestibular symptoms often overlap with symptoms of anxiety. Interestingly, past research has shown no differences in anxiety within one week after injury between patients with concussion and those with orthopedic injuries. 13 After a couple of weeks to months, the literature is inconsistent, with some studies showing elevated anxiety and others showing no differences in anxiety from controls. 17,18 For example, a study of collegiate football players found that in comparison with healthy controls, concussed individuals reported higher anxiety scores at three days and one week post-injury, but not at one month. 19
Sex may play a role in anxiety after concussion. Higher rates of anxiety disorders are diagnosed in females; they demonstrate higher levels of anxiety symptoms after a concussion compared with males. 16,20 –22 Females are also at greater risk for prolonged recovery after concussion, and this pattern is more pronounced in adolescents. 23,24 There are potential physiological and neuroanatomical explanations for these findings, including differences in neck strength, 24 as well as sex differences in brain structure and functioning. 25,26 Overall, females report more severe concussion symptoms in general than males, 27,28 which may also account for the higher anxiety symptoms.
Adolescence is a sensitive developmental period often associated with anxiety, especially for females. Females report higher levels of generalized anxiety, social anxiety, and panic disorder than males. 29,30 Overall, females are more likely than males to report elevated levels of anxiety from early childhood through adolescence. 31 Research has identified that pubertal development predicts mood and anxiety symptoms, for females, over and above chronological age. 32 –34
A study identified neural correlates of post-concussion anxiety in adolescents, with adolescents with more advanced pubertal maturation displaying white matter abnormalities, as measured by lower neurite density index (NDI), in key white matter tracts for emotional regulation. 34 Although it is well established that puberty is associated with anxiety in some adolescents, researchers have yet to examine the interaction between sex and puberty on anxiety in the early stages of concussion, or later.
There have also been many weaknesses in previous studies examining post-concussion anxiety, including the lack of a control group. In a systematic review of mental health outcomes after concussion, predominantly examining depression and anxiety, researchers reported that only two of seven studies included a control group. 35 Further, studies have often relied on measures such as the Beck Anxiety Inventory, which provides a total score, but lacks nuance regarding specific anxiety subtypes. 19,36,37
Many studies have focused on collegiate athletes and adults, 12 rather than adolescents, and studies have often been conducted across various post-injury time intervals, making synthesis of the data challenging. 35,38 In the studies comparing demographics, higher symptoms of anxiety are reported among females and those of pre-adolescent age. 20,39
The primary purpose of this study was to compare anxiety symptoms between concussed and healthy adolescents. A secondary purpose was to examine the longitudinal nature of post-concussion anxiety in adolescents to determine if post-concussion anxiety symptoms are transient in nature or if they persist for months after injury. Within this secondary purpose, we also sought to examine sex differences in post-concussion anxiety symptoms in the context of pubertal development.
We expected that concussed adolescents would report higher anxiety symptoms than healthy controls and, specifically, that concussed adolescents would report higher levels of panic and school avoidance, as concussion symptom triggers (e.g., demanding environments such as school) often produce anxiety symptoms that overlap with and are qualitatively similar to certain concussion impairments (e.g., panic associated with vestibular symptomology). We also expected that females would report higher anxiety symptoms after concussion than males and anticipated that females with advanced pubertal maturation would report higher anxiety after concussion compared with their male counterparts.
Methods
Design
This study was approved by the University of Pittsburgh Institutional Review Board. An initial sample of 86 concussed adolescents and 40 healthy controls was recruited through a pre-existing longitudinal study, the Investigating Concussion in Adolescents at Risk for Emotional Dysregulation (iCare) study (R01MH11488101; PIs: Versace, Kontos).
Participants
There were 126 eligible participants enrolled in the study. Ten concussed participants had incomplete data at the first time point. Seven healthy controls were excluded because of missing data. The concussed group consisted of adolescents aged 12.8–17.4 years with a formally diagnosed concussion, as per current consensus guidelines, 40 within six days of injury. Concussed adolescents were age-and-gender matched to controls, with no history of concussion. Exclusion criteria for all participants included neurodevelopmental, neurological, or systematic disease, significant orthopedic injury within the past month, medical history of major psychiatric disorder (e.g., schizophrenia, major depressive disorder, delusional disorder), and ongoing illicit substance abuse or dependence (within the past three months).
Measures
SCARED
Participants completed the Screen for Child Anxiety and Related Disorders, Child Version (SCARED-C) to quantify anxiety symptoms. Concussed participants completed SCARED-C at three post-injury time points: visit 1 (≤10 days [≤10D]), visit 2 (Four ±1 weeks [4W]), and at visit 3 (Three ±1 months [3M]). Controls only completed SCARED-C at visit 1. The SCARED-C consists of 41 items assessing anxiety symptoms on a 3-point Likert scale (0 = Not True or Hardly Ever True, 1 = Somewhat True or Sometimes True, 2 = Very True or Often True). Item responses are summed to generate a total anxiety score, as well as five subscales: generalized anxiety disorder, separation anxiety disorder, social anxiety disorder, significant school avoidance, and panic disorder symptoms. The SCARED has demonstrated adequate psychometric properties, including strong internal consistency (α = 0.90), as well as good convergent validity with other well-validated self-report measures of anxiety. 41 –43
PDS
The Pubertal Development Scale was completed by controls and concussed participants at visit 1 (
Procedures
Participants with a suspected concussion were evaluated by trained medical professionals (e.g., neuropsychologists, physicians) at the University of Pittsburgh Concussion Clinic. All participants with a confirmed diagnosis of concussion were offered to participate in the study. Age- and sex-matched controls were recruited from the community through a local recruitment website (https://pittplusme.org). All participants, including parents and guardians when indicated, provided informed assent and consent to participate in this study.
Statistical analyses
A post hoc power analysis was conducted for the analyses comparing concussions and controls, using G*Power software, version 3.1. 47 To achieve 80% power in a one-way analysis of covariance (ANCOVA) model at 0.05 significance, with an estimated large effect size of 0.40, 48 a total of 80 participants is needed. The large effect size used in the power analysis was based on existing evidence of differences in anxiety between concussions and controls. 49
Descriptive statistics (means/standard deviations or count/frequencies) were calculated for the concussed (n = 86) and non-concussed cohorts (n = 40). Age, sex, pre-injury anxiety history, and PDSS were compared between groups with independent samples t tests or chi-square tests.
A one-way ANCOVA was conducted to assess between-group differences in SCARED-C total score for non-concussed controls (n = 33) and concussed adolescents (n = 76) at visit 1, controlling for age, sex, and PDSS. The interactions of all variables included in the models were assessed, and when the assumption of homogeneity of regressions slopes was met (p > 0.05), the interactions were removed from the model. All other assumptions of ANCOVA were evaluated and met. Post hoc analysis of adjusted means was performed with a Bonferroni confidence interval adjustment.
A one-way multi-variate analysis of covariance (MANCOVA) was also conducted to examine between-group differences in the SCARED-C subscales (SCARED-C panic, SCARED-C generalized anxiety, SCARED-C separation anxiety, SCARED-C social anxiety, SCARED-C school avoidance) at visit 1, controlling for age, sex, and PDSS. The interactions of all variables included in the models were assessed, and when the assumption of homogeneity of regressions slopes was met (p > 0.05), the interactions were removed from the model. All other assumptions of MANCOVA were evaluated and met.
Follow-up univariate one-way ANCOVAs were performed to determine between-group differences for each SCARED-C subscale. A Bonferroni adjustment was made such that statistical significance was accepted when p < 0.01 (i.e., 0.05/5 = 0.01; 5 SCARED-C subscale dependent variables). Statistically significant one-way ANCOVAs were followed up with pairwise comparisons with a Bonferroni adjustment.
For concussed adolescents with data at all three time points (n = 56), a three-way mixed ANCOVA was performed to understand the effects of sex, PDSS, time, and the interaction between these independent variables on the SCARED-C total score while controlling for age. Between-subjects factors were sex (male, female) and PDSS. For the PDSS factor, participants were grouped into those who scored
For a significant three-way interaction, univariate general linear models were performed to calculate simple two-way interactions of sex and PDSS at each time point. A Bonferroni adjustment was made such that statistical significance was accepted when p < 0.0167 (i.e., 0.05/3 = 0.0167; two-way interaction at each time point). For main effects, follow-up pairwise comparisons were performed with the Bonferroni procedure to control family-wise type I errors. For all analyses, statistical significance was set at p < 0.05. Estimations of effect size for mean differences were reported as partial eta-squared (partial η 2 ) values and interpreted as small (0.01–0.08), medium (0.09–0.24), and large (>0.25). 50 All statistical analyses were performed using SPSS software (version 28.0; SPSS, Inc, Chicago, IL).
Results
Descriptive data
Descriptive statistics for the concussed sample are provided in Table 1. Descriptive statistics for concussed males and females are provided in Table 2. There were no statistically significant differences between adolescents with a concussion and healthy controls in age (15.1 ± 2.3 years vs. 15.2 ± 1.5 years, p = 0.64), sex (55.8% male vs. 57.5% male, p = 0.96), pre-injury anxiety history (11.8% vs. 7.5%, p = 0.4) or PDSS score (3.9 ± 1.1 vs. 3.9 ± 1.2, p = 0.94).
Descriptive Statistics for Continuous and Categorical Variables for Concussed Adolescents
SD, standard deviation; PDSS, Pubertal Development Scale Score; ADHD, attention-deficit hyperactivity disorder; LD, learning disorder.
2 levels: yes/no
Descriptive Statistics for Concussed Male and Female Adolescents
SD, standard deviation; PDSS, Pubertal Development Scale Score.
Significant at p < 0.05.
The concussed sample had predominantly sport-related concussions (77.5%) and was 43% female. The overall sample's PDSS had a negatively skewed distribution, indicating the sample had a higher number of adolescents with advanced pubertal development. At visit 1, full data were available for 88.4% of concussed (n = 76) and 82.5% of non-concussed controls (n = 33). Control data were only collected at visit 1, and those values were used for comparison against concussed. Seven non-concussed controls were lost to missing data, because this study was conducted during the COVID pandemic. At visit 2, full data were available for 79.1% of concussed (n = 68). At visit 3, full data were available for 66.3% of concussed (n = 57).
Anxiety differences between concussed adolescents and non-concussed controls
SCARED-C total scores for male and female participants in the healthy control group at visit 1 and male and female participants in the concussed adolescent group at each visit (
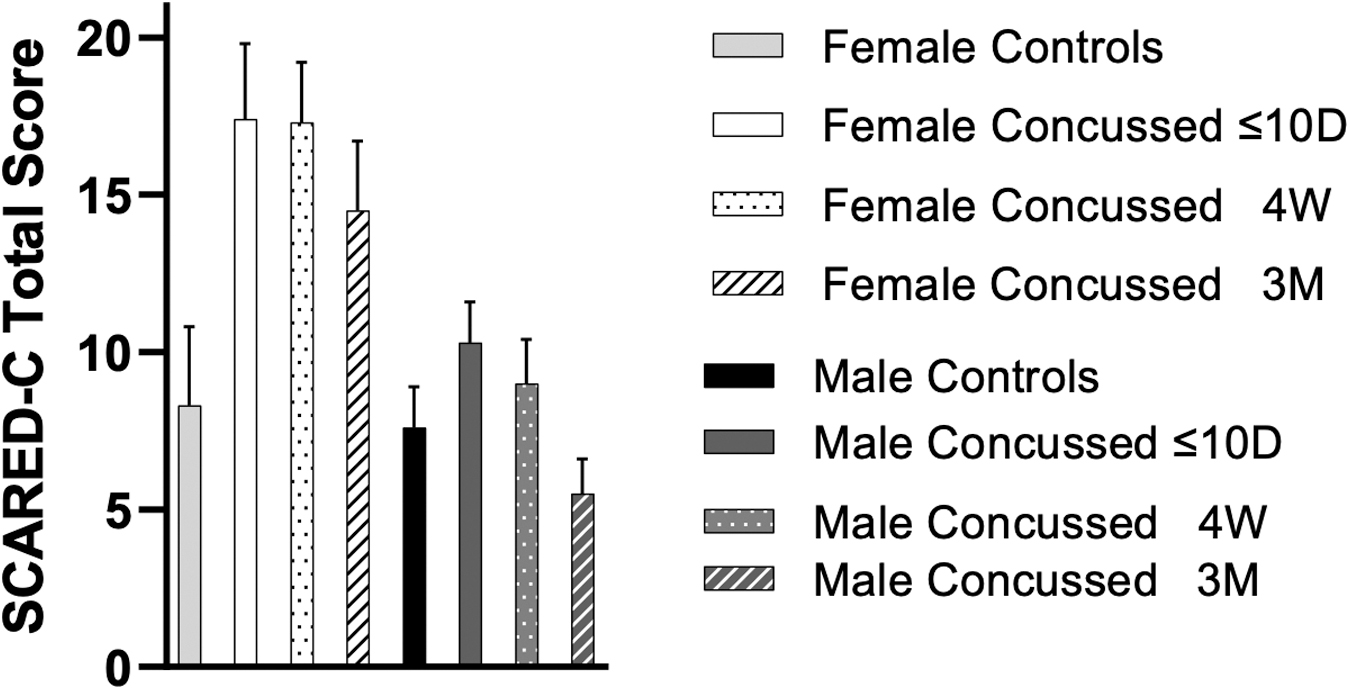
SCARED-C total score for male/female healthy controls at visit 1 and male/female concussed adolescents at each visit (≤10D, 4W, and 3M). SCARED-C, Screen for Child Anxiety Related Emotional Disorders.
Results for Between-Subjects Comparisons of Concussed Adolescents and Healthy Controls at Visit 1 for Screen for Child Anxiety Related Emotional Disorders-C Outcomes When Adjusting for Age, Sex, and Pubertal Development Scale Score
ANCOVA, analysis of covariance; M, mean; Madj, adjusted mean for age; SE, standard error; SD, standard deviation; MANCOVA, multi-variate analysis of covariance; SCARED-C, Screen for Child Anxiety Related Emotional Disorders.
Significant at p < 0.05.
Significant difference between adjusted means based on Bonferroni adjustment (p < 0.01).
Results of the one-way MANCOVA revealed a statistically significant difference between concussed adolescents and controls on the combined SCARED-C subscales after controlling for age, sex, and PDSS, F(5, 100) = 2.54, p = 0.033, Wilks' Λ = 0.887, partial η 2 = 0.113. There were statistically significant differences in adjusted means between groups for SCARED-C panic (F(1, 104) = 7.57, p < 0.007, partial η 2 = 0.1) and SCARED-C generalized anxiety (F(1, 104) = 7.59, p < 0.007, partial η 2 = 0.1), but not for the SCARED-C separation anxiety, SCARED-C social anxiety, or SCARED-C school avoidance subscales. Concussed adolescents had significantly greater panic symptoms (Adj. mean = 2.21 ± 0.24) than healthy controls (Adj. mean = 1.002 ± 0.37; p = 0.007) and significantly greater generalized anxiety symptoms (Adj. mean = 4.42 ± 0.403) than healthy controls (Adj. mean = 2.39 ± 0.61; p = 0.007) after adjusting for age, sex, and PDSS (Table 3).
Anxiety in concussed adolescents over time
Results for the three-way mixed effects ANCOVA revealed a statistically significant interaction between time, sex, and PDSS on SCARED-C total score while controlling for age, F(2, 102) = 4.29, p = 0.016, partial η 2 = 0.1 (Fig. 2). There was no statistically significant within-subjects main effect of time, F(2, 102) = 0.332, p = 0.718, partial η 2 = 0.01. There was a statistically significant between-subjects main effect of sex, F(1, 51) = 10.194, p = 0.002, partial η 2 = 0.17, but there was no significant between-subjects main effect of PDSS, F(1, 51) = 0.01, p = 0.93, or age, F(1, 51) = 0.01, p = 0.95. There were no statistically significant simple two-way interactions between sex and PDSS on SCARED-C total score at visit 1, F(1, 71) = 0.31, p = 0.579, visit 2, F(1, 63) = 3.815, p = 0.055, or visit 3, F(1, 52) = 0.525, p = 0.472, while controlling for age.

Mean ± standard error SCARED-C total scores across visit 1 (
Pairwise comparisons for SCARED-C total score based on sex, PDSS, and time, while controlling for age, are reported in Table 4. Females had higher SCARED-C total scores across all three time points compared with males (≤10D: p = 0.02, 4W: p = 0.005, 3M: p = 0.002), while PDSS groups had similar scores at all three time points (≤10D: p = 0.901, 4W: p = 0.710, 3M: p = 0.988).
Screen for Child Anxiety Related Emotional Disorders Total Scores of Concussed Adolescents (n = 56) Over Time Based on Sex and Pubertal Development Scale Score Group While Controlling for Age
PDSS, Pubertal Development Scale Score; SCARED-C, Screen for Child Anxiety Related Emotional Disorders.
Data are presented as adjusted mean (standard error).
Females had higher scores at all three visits compared with males (≤10D: p = 0.02, 4W: p = 0.01, 3M: p < 0.01).
Females in the >4 PDSS group had higher SCARED-C total scores compared with males in the >4 group at visit 1 (p = 0.02) and at visit 3 (p < 0.01).
Females in the
Females in both PDSS groups had higher SCARED-C total scores compared with males in those groups (
Discussion
The current study is the first to identify sex differences in post-concussion anxiety symptoms across multiple post-concussion time points, within the context of pubertal development. Overall, the findings indicated differences in anxiety symptoms between concussed and controls, supporting our primary hypothesis. Total anxiety, generalized anxiety, and panic anxiety were all higher in adolescents after concussion than in healthy controls. Within the concussed sample, the findings also supported our hypothesis for sex differences in anxiety symptoms, with females reporting higher anxiety symptoms compared with males. When considering pubertal development, females who had completed development (PDSS >4) and females who were still developing (PDSS
As expected, higher levels of overall anxiety were endorsed among our concussed sample compared with controls. This is consistent with the empirical literature demonstrating transient self-reported post-concussion emotional changes. 51 –53 There may be underlying physiological mechanisms to explain the onset of emotional symptoms post-concussion. Specifically, the neurometabolic dysfunction evidenced with concussion often mimics the neurometabolic changes displayed on neuroimaging in individuals with psychopathology, including anxiety. 4 This pattern of overlap in the pathophysiology between concussion and psychopathology was also demonstrated in reference to neurological alterations in limbic-frontal circuitry, in addition to fluctuations in neurotransmitter level, specifically in serotonin and dopamine. 53 -56
Interestingly, only the generalized and panic anxiety subdomains of the SCARED-C were higher in the concussed sample compared with controls. There were no group differences for separation, social anxiety, or school avoidance, compared with the non-concussed sample. Considering that vestibular symptoms of concussion often overlap with panic symptoms and social anxiety, and occur in school settings, these findings were partially surprising. 53,57 Provocation of overall concussion symptoms in the environments associated with these subdomains of anxiety is common.
Currently, individuals with concussion are often being treated with a more active, exposure-based approach, including completing social exposures and their normal-day-to-day activities. 58 This contemporary concussion treatment strategy may promote an adaptive cognitive framework, interpreting symptom exacerbation as non-threatening, and may ultimately explain why adolescents endorsed lower levels of separation, social anxiety, and school avoidance.
The breakdown of survey items may provide some insight into why panic and generalized anxiety scores were elevated within the concussed group. The SCARED items encompassing the generalized anxiety subdomain often examine adolescents' feelings of worry related to ability and interpersonal acceptance (e.g., “I worry about being as good as other kids”). These sources of positive reinforcement are often disrupted by concussion and consequent removal from sports, where adolescents may find themselves worrying about their athletic performance and place within their peer groups. During adolescence, a developmental time where peer relationships begin taking precedence over parent-child relationships, 59 adolescents' inability to be connected to peers through athletics and other extracurricular activities may result in increased feelings of closeness to ones' immediate family.
The SCARED items encompassing the panic subdomain often assess feelings of anxiety related to somatic symptoms (“When I get frightened, I feel dizzy”), providing a potential explanation for why panic was elevated in the concussed group. Dizziness is present in approximately 50–84% after concussion 39,60 and may persist over weeks to months. 61 These findings help to identify the potential types of anxiety that might be implicated during concussion recovery, which can then be targeted in throughout the course of recovery.
Our findings also support the hypothesis that females would endorse higher anxiety symptoms than males post-concussion, and this relationship persisted across all time points. Specifically, when taking sex and pubertal development into consideration together, female adolescents, compared with males, reported higher total symptoms across all three visits. These findings are reflective of previous research identifying that post-concussion vestibular dysfunction is more common in females, and this vestibular dysfunction is often associated with anxiety symptoms. 24,53,62
These findings also align with research on healthy adolescents, 63 which found that adolescent females endorsed higher mean levels of generalized anxiety, social anxiety, and panic disorder compared with adolescent males. Taken together, this pattern may suggest one reason why females present with a higher post-concussion symptom burden, both acutely and in the chronic stage of recovery, compared with males. 14
Although females had higher anxiety than males in both pubertal groups, one potential explanation for the sex differences pertains to sex-specific hormonal changes with pubertal development, including fluctuations in adrenal hormones, growth hormone, and luteinizing hormone (LH). These hormonal differences set the stage for elevated levels of anxiety, especially in concert with increased psychosocial stressors, for example, elevated academic demands and increased social pressure for inclusion and high social functioning. 64,65
Clinical implications
This study highlights the potential clinical utility of administering a well-validated anxiety inventory with subdomains of anxiety. Understanding which subdomain of anxiety is elevated can help the clinician refine the treatment plan for those with post-concussion anxiety. For example, panic symptoms may be best addressed through exposures, 66 while generalized anxiety symptoms may respond to cognitive restructuring techniques. 67,68
This study also reinforces the notion that adolescent females are at risk for acute and chronic anxiety post-concussion. Clinicians should be aware of these sex discrepancies in outcomes and should inform their individualized treatment plan accordingly. For example, more proactive treatment for anxiety post-concussion may be indicated for adolescent females. The study also highlights the importance of clinicians administering validated measures of anxiety through all stages of recovery, because this will allow clinicians to quantify the magnitude of patients' post-concussion anxiety and appropriately respond. Treatment for post-concussion anxiety may include psychoeducation concerning the typical course of recovery from concussion, guided exercise, and referral to a mental health specialist.
Exercise is particularly salient given it is a treatment approach that can address multiple symptoms and impairments associated with concussion, in addition to anxiety. Subthreshold exercise results in increased cerebral blood flow, improved regulatory processes, including sleep, as well as autonomic nervous system regulation in patients with concussion. 10,69 Exercise may alleviate anxiety through multiple proposed mechanisms including acting as a form of exposure therapy, improved self-efficacy, and neurotransmitter and hormonal changes including release of endorphins. 70 –72
Limitations
There are several limitations to this study. The demographics of the sample, including both athletes and non-athletes, makes study results difficult to generalize, because athletes may present with different pre-injury levels of fitness and may engage in various post-injury exertion regimens that may impact their anxiety levels. Further, with this sample being collected at a specialty concussion clinic, results may not generalize to other healthcare settings (e.g., emergency department, pediatrician's office). In addition, patients with non-sport mechanisms of injury—for example, motor vehicle accidents—may have trauma-related symptomology or secondary gain, which was not measured in this study.
Approximately 12% of the concussed sample had a pre-existing history of anxiety, which may result in higher rates of post-concussion anxiety. The percentage of the concussed adolescents with pre-injury anxiety, however, was not significantly different than that of the controls. Nonetheless, future studies should examine the role of pre-injury anxiety and other clinical risk factors.
A higher proportion of physically developed adolescents were recruited, possibly resulting in a higher level of pre-injury baseline anxiety than would be expected in a more evenly distributed adolescent sample. Incorporating symptom severity, as measured by a post-concussion symptom scale, would add valuable clinical information to help quantify to what extent these finding may be mediated by symptom burden. Future studies should also examine treatment efficacy for post-concussion anxiety among adolescents. Last, a larger sample size should be recruited in future research, because our study was underpowered to meet our secondary analyses.
Conclusion
This study was the first to examine sex and pubertal development differences in anxiety among adolescents after concussion. The key findings suggested that adolescents reported higher levels of anxiety after concussion compared with controls, and females reported higher anxiety after concussion than males. Females who completed pubertal development and who were still developing reported higher levels of anxiety after concussion than males at the same respective pubertal developmental stages. These findings highlight the importance of assessing anxiety after concussion in adolescents. Healthcare professionals should include validated measures of anxiety in their multi-domain concussion assessment. Clinicians should also be prepared to provide both psychoeducation and referrals for psychological treatment for adolescents with anxiety, when indicated.
The results also emphasize the need to consider the role of both sex and pubertal development on anxiety after concussion in adolescents. Early identification of adolescents at risk for later development of post-concussion anxiety (e.g., females) should be used to inform earlier behavioral interventions and referrals to mitigate anxiety after concussion in this at-risk population.
Transparency, Rigor, and Reproducibility Summary
This study was a conducted through of a pre-existing longitudinal study, Investigating Concussion in Adolescents at Risk for Emotional Dysregulation (iCare) study (R01MH11488101; PIs: Versace, Kontos). The data analysis plan was formulated prior to beginning collection. The analysis plan was not pre-registered, but the lead statistician (Dr. Eagle) confirms that the proposed statistical analysis plan was pre-specified. A sample size of 80 participants was planned based upon 80% power required for the proposed statistical analyses. 126 participants (40 healthy controls, 86 concussed adolescents) were initially included in the study, with 97 participants remaining enrolled by the final visit. Seven healthy controls were lost to missing data, and 66.3% of the concussed sample was available by the third visit. Data analyses were performed by investigators aware of relevant characteristics of the study participants. Data was initially collected in concert with patients' presentation for concussion treatment. Data was collected using demographic questionnaires and standardized self-report measures. Inclusion/exclusion criteria and clinical outcomes were assessed by investigators with long-standing records of empirical research. Statistical tests were based on the assumptions that dependent variables and covariates were coded as continuous variables. Bonferroni corrections were applied as appropriate. No external validation studies are ongoing. The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. There is no analytic code associated with this study. The contributing authors all agree to provide the full content of the manuscript, on request, by contacting the corresponding author.
Footnotes
Funding Information
This study was funded through the pre-existing longitudinal study, Investigating Concussion in Adolescents at Risk for Emotional Dysregulation (iCare) study (R01MH11488101; PIs: Versace, Kontos).
Author Disclosure Statement
Drs. Kontos and Collins receive book royalties from APA Books, and funding for their research through the University of Pittsburgh from the Centers for Disease Control and Prevention, Chuck Noll Foundation for Brain Injury Research, Department of Defense (CDMRP, USAMRAA, USUHS), National Football League, National Institutes of Health (NICHD, NIMH, NINDS), and private donors.