
Abstract
Neuroinflammation is a significant and modifiable cause of secondary injury after traumatic brain injury (TBI), driven by both central and peripheral immune responses. A substantial proportion of outcome after TBI is genetically mediated, with an estimated heritability effect of around 26%, but because of the comparatively small datasets currently available, the individual drivers of this genetic effect have not been well delineated. A hypothesis-driven approach to analyzing genome-wide association study (GWAS) datasets reduces the burden of multiplicity testing and allows variants with a high prior biological probability of effect to be identified where sample size is insufficient to withstand data-driven approaches. Adaptive immune responses show substantial genetically mediated heterogeneity and are well established as a genetic source of risk for numerous disease states; importantly, HLA class II has been specifically identified as a locus of interest in the largest TBI GWAS study to date, highlighting the importance of genetic variance in adaptive immune responses after TBI. In this review article we identify and discuss adaptive immune system genes that are known to confer strong risk effects for human disease, with the dual intentions of drawing attention to this area of immunobiology, which, despite its importance to the field, remains under-investigated in TBI and presenting high-yield testable hypotheses for application to TBI GWAS datasets.
Introduction
Traumatic brain injury (TBI) is a major cause of morbidity and death worldwide, with an estimated 70 million cases annually. 1 Secondary injury (additional brain injury caused by downstream processes triggered by the initial mechanical trauma) is thought to be a substantial and potentially preventable determinant of outcome after TBI, with only approximately one third of outcome variability being currently explained by initial injury and patient factors. 2,3 Neuroinflammation is a key component of secondary injury in the acute phase, occurring via both direct glial responses to injury and indirect responses to systemic inflammation, and is also thought to contribute to chronic neurodegeneration post-TBI. 4 While most neurotrauma research has focused on the innate arm of the immune system, it is increasingly recognized that adaptive immune responses, including trauma-induced autoimmunity, play an important role through either the beneficial clearance of cell debris or destructive autoimmune damage. 5,6
The immune system displays great heterogeneity between individuals, with genetic factors representing significant determinants in the host response to infection, cancer, and the development of immunological diseases. 7 –9
While autoimmune diseases are often individually rare, it is estimated that up to 8% of the population are affected by autoimmune disease, 10 and therefore the genetic predisposition toward autoimmunity is even more common. Given the high frequency of genetic variants affecting the immune response, it is likely that these contribute to the heterogeneity in immune response seen after TBI and may in turn represent determinants of outcome.
The largest genome-wide association study (GWAS) in TBI (n = 5268) has recently been reported and estimates that 26% of outcome variation is genetically mediated, but was not able to demonstrate any specific variants that met the genome-wide threshold of significance (p < 5
An alternative approach, which substantially reduces the burden of multiple comparisons, is to apply a hypothesis-driven candidate gene approach to the dataset, based on pre-determined biological hypotheses. We hypothesise that genetic variants that are known risk factors for autoimmunity are likely to also predispose to the loss of immunological self-tolerance after TBI and would therefore predict worse outcome; indeed one of the few loci of interest reported by the recent TBI GWAS was Human Leukocye Antigen HLA-DQB1, 11 which is implicated in a number of autoimmune diseases including those of the central nervous system (CNS). 12
In this review, we identify genes that are most frequently recognized as risk factors for autoimmunity from GWAS of several immune-mediated disorders and discuss how variants affecting these genes may be biologically relevant in post-TBI autoimmunity and should therefore be investigated independently within GWAS datasets.
Methods
Lists of GWAS for eight common autoimmune conditions and the relevant associated single nucleotide polymorphisms (SNP)/genes were extracted from the NHGRI-EBI GWAS Catalog. 13 These conditions were Crohn disease, ulcerative colitis, systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), multiple sclerosis (MS), type 1 diabetes mellitus (T1DM), autoimmune thyroid disease, and celiac disease. The top 20 genes that were implicated most frequently across these eight conditions were identified (Table 1).
Genes Commonly Implicated in Association Studies Across Multiple Autoimmune Disorders
A Python script was written to distill relevant information regarding each gene from PubMed MEDLINE for inclusion in this review (Fig. 1). This script used three parameters: [GENE NAME], phrase [IMMUNE], and list of each [DISEASE(s)] used earlier. It then performed individual searches for all listed [DISEASE(s)] and after comparison, produced a list of publications that were repeated between the searches.
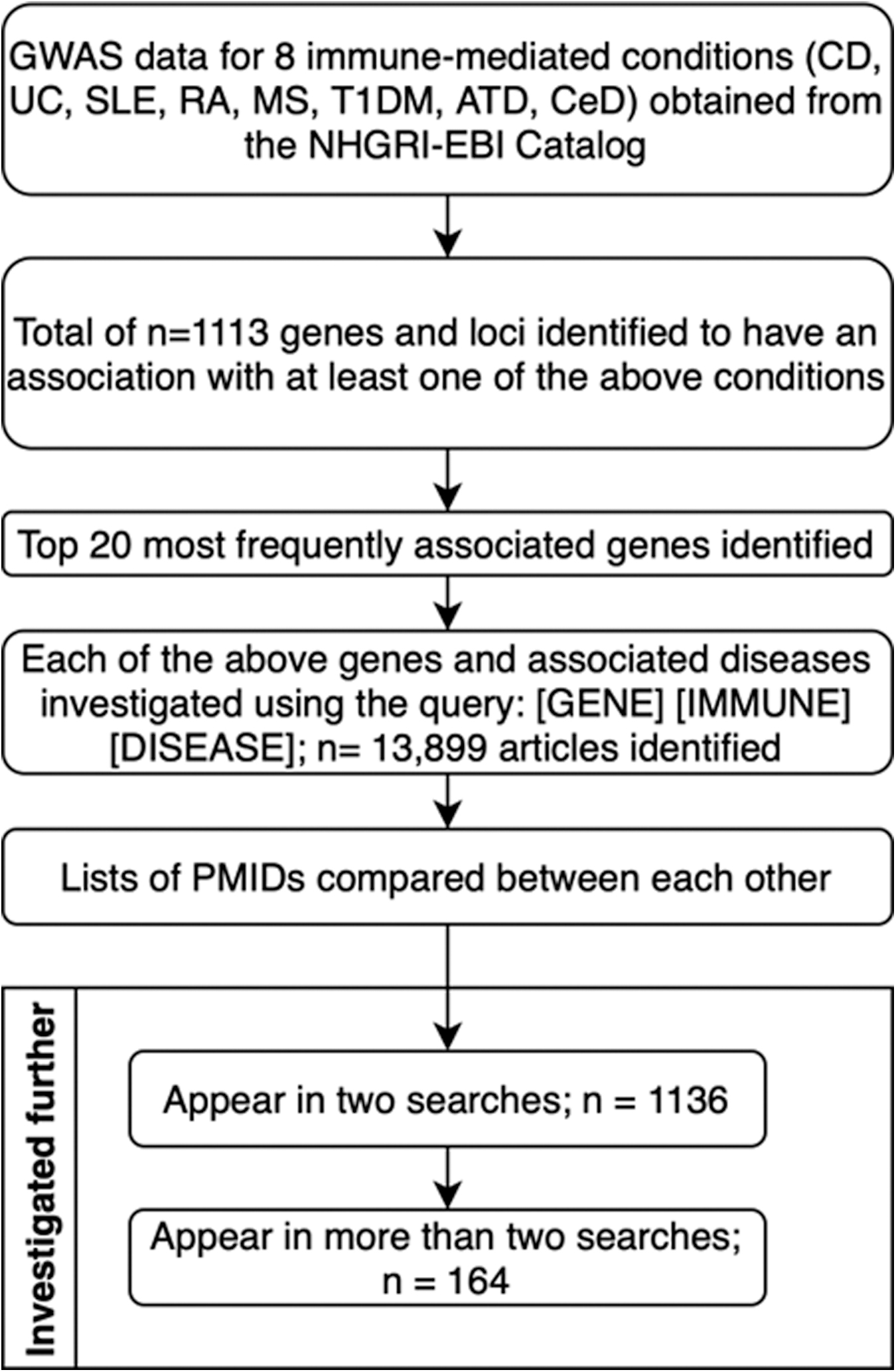
Illustration of the search strategy. The NHGRI-EBI Catalogue was searched, and data extracted manually for genes associated with eight autoimmune conditions (CD Crohn Disease, UC–Ulcerative Colitis, SLE–Systemic Lupus Erythematosus, RA–Rheumatoid Arthritis, MS–Multiple Sclerosis, T1DM–Type 1 Diabetes Mellitus, ATD–Autoimmune Thyroid Disease, CeD–Celiac Disease). Literature relevant to the top 20 most frequently associated genes were then reviewed using a Python script sifting through Pubmed database and comparing lists of PMIDs produced by the [GENE] [IMMUNE] [DISEASE] query. [GENE]–currently investigated gene, [IMMUNE]–fixed element of the query, [DISEASE]–investigated disease. This initial query produced 13,899 articles. For each gene, an additional search with the query [GENE] [IMMUNE] [BRAIN] was performed. Lists of PMIDs for each gene and each disease were created, and inside one gene group compared between themselves (including the [BRAIN] query). If a PMID repeated once, it was added onto the “Appear in two searches” list. If it appeared more than twice it was added onto the “Appear in more than two searches” list. Both lists were reviewed manually for the final selection of articles to be discussed in the review.
After this, publications produced by [GENE NAME][DISEASE(s)][BRAIN] or [BRAIN INJURY] were added to each list. The search resulted in two lists of publications: those appearing in two searches, and those that appear in more than two. This helped identify key publications as well as bring attention to ones for further exploration.
Results and Discussion
Risk loci for autoimmunity can be broadly categorised into five main areas: HLA type, regulators of lymphocyte activation, cytokines and their receptors, transcription factors and related modulators of gene expression, and intracellular signaling pathways. These are presented in Figure 2, and discussed below in turn.

(
HLA–Major Histocmopatibility Complex (MHC) Class 1 and 2
The MHC class II molecule is responsible for recognizing and presenting extracellular antigens to immune cells of the adaptive immune system (namely T-cells) and represents the largest source of genetic predisposition to autoimmune disease. 14 Further, the effect size of risk conferred by MHC II variants can be substantial (e.g., an odds ratio of more than 7 for HLA-DQA1 in celiac disease). 15
The MHC II is expressed by glia within the CNS and is required for the trafficking of self-reactive T-cells into the CNS and subsequent generation of autoimmune neurological diseases such as MS. 16 The MHC II is significantly upregulated in the brain after TBI in mice, with a notable variation between genetically different strains, and leads to significant T-cell influx in this context. 17
The MHC II polymorphisms are also implicated in autoimmune neurological disease that arises from outside the CNS; LGI1 and CASPR2 encephalitides are conditions with strong MHC II allelic associations that are characterized by the production of autoantibodies within the peripheral compartment that then enter the CNS to cause neuroinflammation. 16
Given its function, MHC II is likely to be involved in the initiation of both the cellular and humoral adaptive immune responses against released neural antigens seen in the peripheral compartment after TBI. 18 –20 Particular mutations increasing promiscuity of the receptor—i.e., in the DQ 21 or in DR molecule 22,23 —may increase the likelihood for self-recognition, and indeed HLA-DQB1 was identified in the TBI GWAS study as a locus of interest at the subgenome-wide level of significance. 11
The MHC type I is expressed by all nucleated cells of the body and is responsible for the presentation of both self and non-self intracellular antigens. 24 Response to presented self-antigens is usually inhibited by both central and peripheral tolerance mechanisms. 25 Even though less frequently associated with autoimmune disease, several haplotypes that strongly predispose to certain autoimmune disease have been identified, with perhaps the most well-established of these being HLA-B27 and ankylosing spondylitis. 26 Introduction of human HLA-B27 and β2 microglobulin genes into rats precipitates an inflammatory disease strikingly similar to HLA-B27-associated disease in humans, highlighting the magnitude of effect that HLA-type can infer. 27
While there is less evidence of the role of MHC I in neuroinflammatory disease, sustained exposure to interferon gamma (as is seen in TBI) leads to upregulation of MHC I on neurons, with subsequent antigen-specific cytotoxic T-lymphocyte mediated neuronal destruction. 28 Further, upregulation of MHC I antigen processing and presentation pathways is seen in glial cells after TBI, raising the possibility that a similar process might lead to glial injury. 29
T-cell activation–CD28 and cytotoxic T-lymphocyte-associated protein 4 (CTLA4)
A CD28 is a receptor for CD80/86 and a major costimulatory molecule for the activation of T-cells, lying in close genetic approximation with CTLA4 on chromosome 2, 30 meaning that many SNPs in the CD28 and CTLA4 genes show linkage disequilibrium. 31 Combined CD28 and CD3 stimulation in the presence of self-antigen presentation may be used to experimentally induce autoimmune conditions; CD28 knockout mice are relatively protected against autoimmune disease, 32 and T-cells from CD28 knockout mice fail to migrate and infiltrate tissues in experimental autoimmune encephalomyelitis. 33
The CD28 super-agonist induced T-reg expansion, however, limits brain damage in an experimental model of stroke in mice, 34 pointing to a dual role of CD28-CD80/86 signaling by both promoting tolerance by T-reg expansion and aggravating autoimmunity by T-effector stimulation.
The CTLA4 is an immunosuppressive molecule with high-affinity for its ligands CD80 and CD86. It is constitutively expressed by regulatory T-cells and upregulated on activation of T-cells in a homeostatic manner, acting to prevent unbridled T-cell activation. 35 In a dramatic genetic example of its function, multifaceted autoimmune disease with large CNS lesions develops in haploinsufficient patients, demonstrating how loss-of-function mutations can predispose to autoimmunity. 36
Association studies have implicated variants in the CD28/CTLA4 locus with a wide array of autoimmune disease including T1DM, autoimmune thyroid disease, SLE, and MS. 37,35 Although the effect size of risk alleles is small, they have a high frequency within the population. 38,39
Therapeutically harnessing the effects of CTLA4 can significantly ameliorate neuroinflammation 40,41 and therefore might represent a tractable target in TBI. Further, it has been shown to promote neuronal stem cell survival and differentiation and therefore genetic variants might have downstream effects on repair mechanisms post-TBI. 42 –44
Cytokines–interleukin (IL)-2, IL-2RA, IL-10, IL-12B, and IL-21
Cytokine-related genes are recognized risk loci for a number of autoimmune diseases, and indeed there is support in the literature for SNPs in IL-1β and tumor necrosis factor (TNF)α associating with unfavorable outcomes post-TBI. 45,46
Regulatory T-cells constitutively express the IL-2 receptor and are dependent on IL-2 for their development and function. 47 The IL-2 is therefore considered a potent anti-inflammatory cytokine, and polymorphisms relating to IL-2 and its receptor have been implicated in autoimmune disease including T1DM, RA, and MS. 48 IL-2 gene knockout in mice leads to systemic autoimmune disease, but also to increased migration of T-cells into the brain. 49
After TBI, IL-2 concentrations within the CNS drop to a level where regulatory T-cells cannot survive, and rectifying this deficit significantly reduces lesion size in a mouse model. 50 Despite being broadly regarded as an anti-inflammatory cytokine, in high concentrations IL-2 can drive effector cell activation and therefore inflammation, 51 as well as promoting blood-brain barrier disruption, thus allowing immune cells and autoantibodies to enter the brain parenchyma, 52 highlighting the importance of tight regulation.
The IL-10 is the main immunosuppressive cytokine produced by T-regs, B-regs, and monocytes. In B-cell deficient mice, IL-10 introduction significantly limits post-stroke CNS inflammation and increased T-reg populations. 53,54 Circulating IL-10 levels surge after TBI, in turn suppressing astrocytic production of pro-inflammatory IL-6 in response to IL-1β released from injured brain tissue. 55 In addition, IL-10 improves neuronal survival after axotomy and limits microglial inflammatory responses. 56
It may thus be speculated that post-TBI IL-10-mediated immune suppression is a natural mechanism protecting the CNS from inflammation. The IL-10 secreting B-reg populations decrease after TBI, however, and pneumonia developed in patients with high levels of these cells on day 1 after TBI. 57 The IL-10 may be both protective against post-TBI autoimmunity but also be the cause for poor patient outcomes from infection, highlighting the competing interests between compartments.
The IL-12B encodes the IL-12p40 subunit, which is a component of both IL-12 and IL-23, the latter of which is a potent driver of the Th17 responses that are so characteristic of many autoimmune conditions. 58 Variants such as V298F mutation impair IL-12 and IL-23 assembly and in turn decrease immune activation and risk of autoimmunity. 59
Although not essential for autoimmunity development, IL-21 promotes CD8+ T-cell response toward low-affinity (i.e., self) ligands and is a key driver of germinal center development and maintenance. 60 –62 It enhances Th17 proliferation and inhibits that of T-regs. 63,64 BITRAP, a fusion protein targeted at both TNF-α and IL-21, successfully decreased Th17 numbers and increased IL-10 levels in vitro. 65 In MS lesions, IL-21 is expressed by CD4+ infiltrating T-cells and from neurons that expressed IL-21R as well, suggesting an additional mechanism of inflammation maintenance. 66 The IL-21 producing T-cells have also been implicated as key players in several different non-neurological autoimmune conditions. 67 –69
Transcription factors and other regulators of gene expression
Mutations in a number of transcription factors have been implicated in autoimmunity, with certain loss-of-function mutations causing frank syndromic autoimmune disease such as FOXP3 leading to the Immunodysregulation Polyendocrinopathy Enteropathy X-linked syndrome (IPEX), and AIRE causing Autoimmune Polyglandular Syndrome type 1. 70 Four transcription factors have been strongly implicated across a number of autoimmune diseases including SLE, RA, inflammatory bowel disease, and MS: ETS1, IKZF3, IRF5 and BACH2. 71 –76 The IRF5 raises particular interest, given that a relatively high risk for SLE (odds ratio 1.45) is conferred by the rs4728142 SNP, which is found commonly in the population with a high allelic frequency. 77
Broadly speaking, these transcription factors either promote proinflammatory functions of immune cells, or mediate regulatory countermeasures. The ETS1 is widely expressed on both T and B lymphocytes and promotes IL-2 expression with subsequent effects on regulatory T-cells, suppression of Th17 cell expansion, and autoimmunity development; 78,79 a SLE-like syndrome develops in knockout models. 80
The IKZF3 encodes the protein Aiolos, which is a key transcription factor for B-cell proliferation and differentiation, 81 a mediator of innate NK and ILC1 responses, 82 and a promoter of Th-17 differentiation via suppression of IL-2 synthesis. 83
Interferon regulatory factor 5, encoded by the IRF5 gene drives macrophages toward a proinflammatory phenotype, modulates B-cell maturation and antibody production, and pushes T-lymphocytes toward Th1 and Th17 differentiation. 84,85,75 Of note, upregulation of the expression of type 1 interferon signaling pathway genes including regulatory factors such as IFR5 have been demonstrated in microglia after TBI 86 and particularly in aged mice, 87,88 suggesting an additional important inflammaging effect.
Further, inhibiting these pathways seems to be beneficial, with Interferon-β knockout mice displaying reduced neuroinflammation and better pathological and functional outcomes after TBI, and treatment with anti-type 1 interferon antibodies transiently improving functional outcome. 89
BACH2 is a transcription factor acting on the JAK/STAT pathway that restricts terminal T-helper cell differentiation and is essential for efficient T-reg formation. 90,91 Mice deficient for Bach2 on T-lymphocytes showed abnormal Tfh proliferation and development of humoral autoimmunity. 92
In addition to mutations in transcription factors themselves, both upstream and downstream modulators of gene expression have similarly been recognized to infer risk of autoimmunity. The TNFAIP3 product A20 is rapidly induced by TNF 93 and acts as a potent inhibitor of the NFκB pathway, 94 protecting against unbridled inflammation and autoimmune responses. A20 deficiency in mice results in increased number of B-cell germinal centres and raised autoantibody titres. 95
Three SNPs (rs13192841, rs2230926 and rs6922466) have been associated with increased susceptibility to RA and SLE (some with large effect sizes), suggesting a wider overall role of TNFAIP3 in autoimmune disease. 96 Injection of A20 into RA mice showed significant NFκB signaling reduction and amelioration of the disease phenotype. 97 In MS, A20 is reduced at disease onset. 98 Further, A20 has been shown to inhibit necroptosis and therefore may serve a broader role as a neuroprotective agent in post-TBI damage; 99 silencing of A20 leads to significantly increased necroptosis after TBI via its inhibitory effect on the TNF-mediated downstream RIP1/RIP3-MLKL signaling pathway, as well exacerbating neuroinflammation (both as a result of the increased necroptosis and its more classic effects on the NFκB pathway). 100
The PUS10 is a ubiquitous enzyme, which acts predominantly by promoting microribonucleic acid (mRNA) biogenesis and post-transcriptional regulation of gene expression. 101 It is essential for TRAIL-induced apoptosis progression, and mutations are associated with cell immortality and better proliferation, 102,103 contributing to “immortalization” of autoimmune effector cells.
Intracellular signaling
The PTPN2 and PTPN22 genes encode non-receptor protein tyrosine phosphatases, and have both been reproducibly identified as common risk loci for autoimmune disease, 104,105 with a comparatively high frequency of risk alleles in the population. 106,107
The PTPN2 expression induces regulatory T-cells, encourages differentiation away from Th1/17 phenotypes, reduces responsiveness to interferon-γ, and inhibits autophagy. Loss-of-function mutations show aggravated NOD-2 responses to bacterial recognition and subsequent Crohn disease development. 108 The PTPN2 deficient T-cells precipitate widespread autoimmunity that is transferrable by CD8+ T-cell transfer to wild-type mice, 109 and humoral autoimmunity develops in knockout mice. 110
The PTPN22 is one of the better established non-HLA risk factors for autoimmune disease. It effects a potent inhibitory influence, predominantly at the T-cell receptor, by dephosphorylating a number of key kinases at their activation loop tyrosines. 111 The R620W (C1858T) gain-of-function mutation infers a significantly increased risk for a range of autoimmune conditions such as T1DM and RA, 112 and importantly this gain-of-function polymorphism has a high frequency in the population (up to 15.5% in some countries), 113 identifying it as a high yield gene to study in TBI. Further, given its limited expression outside immune cells, it is a promising target for treatment—e.g., with short interfering RNA because off-target effects are likely to be minimal. 114,115
The SH2B3, known as the Lnk adaptor protein, is expressed mainly in lymphoid tissues. Loss-of-function mutations lead to increased susceptibility to autoimmunity and acute lymphoblastic leukemia, and the rs3184504 SNP predisposes to a number of autoimmune conditions. 116 An SH2B3 deficiency results in heightened number and responsiveness of DCs and inflammatory CD8+ T-cells in affected mice. 117,118 Of particular interest is the association of the rs3184504 SNP with reduced death in sepsis, 119 again raising the notion that a predisposition to autoimmunity in critical illness is not necessarily detrimental and may be protective.
The TAGAP is a small GTPase activating protein, key in the regulation of Th17 differentiation. In TAGAP-deficient mice, fungal infections develop but mice are partially protected from MS. 120 The STAT4 is phosphorylated by Janus kinases and transduces signals from IL-12, IL-23, and IFNγ. The Th2 cells show decreased levels of STAT4, and artificial induction of this protein leads to a Th1-like repolarization of these cells. 121,122 It suppresses T-reg differentiation, and when knocked out can lead to their increased proliferation and prevention of experimental colitis in mice. 123
The TYK2 belongs to the Janus kinase family; thus it can signal via STAT pathways. Its deactivation via IFN-β action leads to better outcomes in patients with MS. 124 Small biological TYK-2 inhibitors proved to be useful in IL-12 and IL-23 cytokine signaling pathway dampening and may be efficacious in managing selective autoimmune conditions. 125
Conclusion
Approximately 26% of variation in TBI outcome is thought to be genetically mediated, but studies using purely data-driven analysis approaches have yet to identify crucial predisposing variants. In a disease as complex as TBI, applying hypothesis-driven approaches to datasets offers a chance to identify risk variants by using an understanding of the biology of TBI to highlight candidate genes (Table 1), and therefore limit the volume of data analyzed.
Adaptive immune responses to TBI represent an important, therapeutically modifiable part of the disease process, and heterogeneity in adaptive immune responses has a well-documented genetic basis. By focusing on genes that are known to have significant effects on predisposition toward autoimmunity, either through the strong effect of an uncommon variant or the combined weak effects of common variants, it may be possible to identify important genetic drivers of TBI outcome, and in due course novel treatment targets; looking to the future, the advent of personalized medicine will rely heavily on rapid genotyping to inform an individual's treatment regimen, and tailoring immunomodulatory treatments by genotype will optimize efficacy and safety.
This review identifies candidate genes that may be likely to confer effects on post-traumatic autoimmunity as a framework on which to base hypothesis-driven analysis of current and future GWAS data in TBI.
Footnotes
Acknowledgments
Figure 1 was created using ![]() was created with BioRender.com.
was created with BioRender.com.
Author's Contributions
MD and JL performed the literature search and drafted the manuscript. EN devised the manuscript concept, and supervised the manuscript drafting. DM revised the manuscript.
Funding Information
EJN and DKM are supported by the Medical Research Council (UK) within the framework of ERA-NET NEURON, and by Brain Research UK.
DKM is supported by an NIHR Senior Investigator Award and European Union 7th Framework program (EC grant 602150).
Author Disclosure Statement
MD, JL, and EN have no disclosures.
DKM reports grants, personal fees, and nonfinancial support from GlaxoSmithKline Ltd.; grants, personal fees, and other from NeuroTrauma Sciences; grants and personal fees from Integra Life Sciences; personal fees from Pfizer Ltd.; grants and personal fees from Lantmannen AB; from Calico Ltd.; personal fees from Pressura Neuro Ltd.; and others from Cortirio Ltd., outside the submitted work.