
Abstract
Neurofilament light (NF-L) is an axonal protein that has shown promise as a traumatic brain injury (TBI) biomarker. Serum NF-L shows a rather slow rise after injury, peaking after 1-2 weeks, although some studies suggest that it may remain elevated for months after TBI. The aim of this study was to examine if plasma NF-L levels several months after the injury correlate with functional outcome in patients who have sustained TBIs of variable initial severity. In this prospective study of 178 patients with TBI and 40 orthopedic injury controls, we measured plasma NF-L levels in blood samples taken at the follow-up appointment on average 9 months after injury. Patients with TBI were divided into two groups (mild [mTBI] vs. moderate-to-severe [mo/sTBI]) according to the severity of injury assessed with the Glasgow Coma Scale upon admission. Recovery and functional outcome were assessed using the Extended Glasgow Outcome Scale (GOSE). Higher levels of NF-L at the follow-up correlated with worse outcome in patients with moderate-to-severe TBI (Spearman's rho = -0.18; p < 0.001). In addition, in computed tomography–positive mTBI group, the levels of NF-L were significantly lower in patients with GOSE 7-8 (median 18.14; interquartile range [IQR] 9.82, 32.15) when compared with patients with GOSE <7 (median 73.87; IQR 32.17, 110.54; p = 0.002). In patients with mTBI, late NF-L levels do not seem to provide clinical benefit for late-stage assessment, but in patients with initially mo/sTBI, persistently elevated NF-L levels are associated with worse outcome after TBI and may reflect ongoing brain injury.
Introduction
Traumatic brain injury (TBI) is a major public health problem worldwide. An estimated 69 million TBIs occur each year, most of which are classified as mild. 1 Young drivers, athletes, and older adults are among the most susceptible risk groups. 2
Currently, the diagnostic process of TBI relies on clinical examination and brain imaging. Computed tomography (CT) and magnetic resonance imaging (MRI) are the standard techniques for TBI imaging, but both have their limitations in detecting TBI. 3
Blood levels of brain-enriched biomarkers have been increasingly studied as diagnostic aids for TBI. Several potential biomarkers such as S100B, glial fibrillary acidic protein (GFAP), neuron-specific enolase (NSE), ubiquitin carboxy-terminal hydrolase L1 (UCH-L1), neurofilament light (NF-L), and tau protein have been examined in various settings. 4 –9 Most studies on diagnostic and prognostic TBI-associated biomarkers have focused on measuring the early levels of these biomarkers, whereas late biomarker levels have been less studied. One study showed that late (measured 30, 90, and 180 days after the injury) NF-L levels have a better prognostic value for functional outcome after TBI than GFAP, tau, or UCH-L1. 9 A recent study reported that integration of UCH-L1 into established clinical outcome prediction models yielded the highest incremental prognostic value for functional outcome after TBI. 10
NF-L is a protein that is most abundantly expressed in myelinated axons of the white matter (WM). 11 –15 In the healthy population, serum levels of NF-L remain fairly stable in people under 60 years of age and increase thereafter. 16 Earlier studies have shown that serum levels of NF-L increase after a severe TBI and this increase persists for 10-12 days after injury, 17 -19 but the levels can remain elevated for up to 5 years after injury. 9,20 Persistently elevated NF-L levels also have been related to late WM volume loss for years after a TBI. 21
The aim of this study was to investigate whether plasma NF-L levels associate with functional outcome assessed on the same day on the average 9 months after the injury. Late elevated NF-L levels may have diagnostic value in patients with initially mild TBI (mTBI) with clinical confounding factors present at the time of diagnosis, or if they have had post-acute secondary problems that complicate the clinical assessment. In patients with more severe TBIs, these later NF-L levels may be useful in identifying patients at higher risk for developing progressive neurological damage.
Methods
Study population
This study was part of the European Union–funded TBIcare (Evidence-based diagnostic and Treatment Planning Solution for Traumatic Brain Injuries) project. The project was approved by the ethical board of the hospital. Consecutive eligible patients were recruited at Turku University hospital between November 2011 and October 2013 and the biomarker levels were measured and outcome was assessed between February 2012 and January 2014. For this study, the levels of NF-L were measured in 178 patients with TBI on average 9 months after the injury, and from 40 controls after a similar interval from an orthopedic injury. The inclusion criteria for patients with TBI were age over 18 years, clinical diagnosis of TBI, and indications for acute head CT according to National Institute for Health and Care Excellence criteria (
Biomarker analysis
Blood samples for plasma NF-L were drawn at the follow-up appointment, put on ice bath, centrifuged for 10 min at 10,000 rpm at 4°C within 30 min from sampling, and stored at -80°C until analysis. Freeze–thaw cycles were performed once prior to analysis. All samples were analyzed at the same time in a single batch. For measuring plasma NF-L levels, the Neurology 4-Plex A assay on an HD-1 Single molecule array (Simoa) device with instructions from the manufacturer (Quanterix, Billerica, MA) in the Clinical Neurochemistry Laboratory, Sahlgrenska University Hospital, Mölndal, Sweden, was used. For quality control (QC), two QC levels were run in duplicates at the beginning and at the end of each run. The repeatability was 10.5% and intermediate precision was 12.2% with a concentration of 10.8 pg/mL. With a concentration of 155 pg/mL, the same parameters were 7.7% for repeatability and 8.4% for intermediate precision. The lower limit of detection was 0.104 pg/mL, the lower limit of quantification 0.174 pg/mL and the calibration ranging from 0.533 to 453 pg/mL.
TBI severity and CT scan grading
The initial severity of TBI was assessed using the lowest recorded Glasgow Coma Scale (GCS) 22 before possible intubation. GCS values 13-15 were considered as mild, 9-12 as moderate, and 3-8 as severe. Due to the nature of the clinical questions of the study, we studied the moderate and severe TBI groups (mo/sTBI) together and analyzed them alongside the mTBI and control groups. CT images were graded according to the descriptive system proposed by Marshall and colleagues. 23 In the statistical analyses, patients were divided into two groups: CT-positive (Marshall score 2-6) and CT-negative (Marshall score 1).
Outcome and recovery grading
Patient recovery and outcome were assessed on the average 9 months from the injury (range 5.3-18.5 months) using the Extended Glasgow Outcome Scale (GOSE). 24 Outcomes were classified as favorable or unfavorable using a sliding dichotomy based on the initial severity of injury. In patients with mTBI, incomplete recovery (GOSE <8) was classified as unfavorable, while in mo/sTBI a GOSE of <4 was classified as unfavorable. During the same follow-up visit, the length of post-traumatic amnesia (PTA) was assessed and a blood sample for NF-L level analysis was taken. The length of PTA was assessed using the Rivermead method. 25 The outcome and PTA assessment were done by a single experienced neurologist (OT), who was blinded to the NF-L levels.
Statistical analysis
Demographics are presented either as mean ± standard deviation or frequencies and percentages depending on the type of variable. The normality of distributions was analyzed with the Kolmogorov-Smirnov test and visually. Because the levels of the NF-L were not normally distributed, the levels are presented as medians and interquartile range (IQR) and nonparametric tests were used in the statistical analyses. The longitudinal percentage change in NF-L levels were calculated subtracting the acute NF-L level from the late NF-L level and dividing the result by the acute NF-L level. Spearman's rank correlation coefficient was used to assess correlations between the biomarker levels and the clinical variables (CT-positivity, worst GCS, GOSE, and PTA). In correlation coefficient analyses, the effect of age and sex were accounted for. Mann-Whitney U test was used for comparing NF-L levels between the groups. IBM SPSS statistics (Version 28, IBM Corp, Armonk, NY), was used to perform all statistical analyses and a p value <0.05 was used to assess the statistical significance of the results.
Results
Demographics
In total, 178 patients with TBI and 40 orthopedic non-CNS trauma controls were included in the analyses, and their demographics are shown in Table 1. Most patients (62%) had an mTBI and approximately one-third (38%) had a mo/sTBI. Of all patients, 47% were CT-negative, and 53% CT-positive. The most common cause of injury was incidental fall (52.3% of patients with mTBI and 56.7% of patients with mo/sTBI). Half (51%) of the patients diagnosed with an mTBI had incomplete recovery. In more than half (58%) of the patients diagnosed with a mo/sTBI, the outcome was favorable.
Demographics and Clinical Characteristics of Subjects
Student's t-test; bchi-squared test; *comparison between TBI patient groups.
SD, standard deviation; min., minimum; max., maximum; TBI, traumatic brain injury; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia; IQR, interquartile range; GOSE, Glasgow Outcome Scale Extended,
The levels of NF-L in TBIs of different severities
The late levels of NF-L were significantly higher in patients with mo/sTBI (median 46.16; IQR 26.35, 66.22) when compared with patients with mTBI (median 16.16; IQR 9.99, 24.27; p < 0.001) and orthopedic controls (median 14.36; IQR 8.07, 18.56; p < 0.001). The distribution of NF-L levels in patients with TBIs of different severities are shown in Figure 1. The difference between the patients with mTBI and controls was not statistically significant (p = 0.233).

Neurofilament light (NF-L) levels in patients with moderate or severe traumatic brain injury (Mo/sTBI), patients with mild traumatic brain injury (mTBI), and orthopedic controls.
Levels of NF-L and outcome
Levels of NF-L in all patients with mTBI and complete recovery (median 17.80; IQR 9.85, 27.75) did not differ from those with incomplete recovery (median 13.30; IQR 9.91, 21.59; p = 0.579). The levels of NF-L by outcome and CT-positivity in patients with mTBI are shown in (Fig. 2). However, when NF-L levels of patients with GOSE 7-8 were compared with patients with GOSE <7, there was a significant difference (median 13.14; IQR 9.77, 23.78 and median 21.28; IQR 13.37, 47.13; respectively; p = 0.036). In case of mo/sTBI, those with favorable outcome had lower levels than those with unfavorable outcome (median 34.31; IQR 25.20, 48.13, and median 64.96; IQR 55.44, 71.52; respectively; p < 0.001).
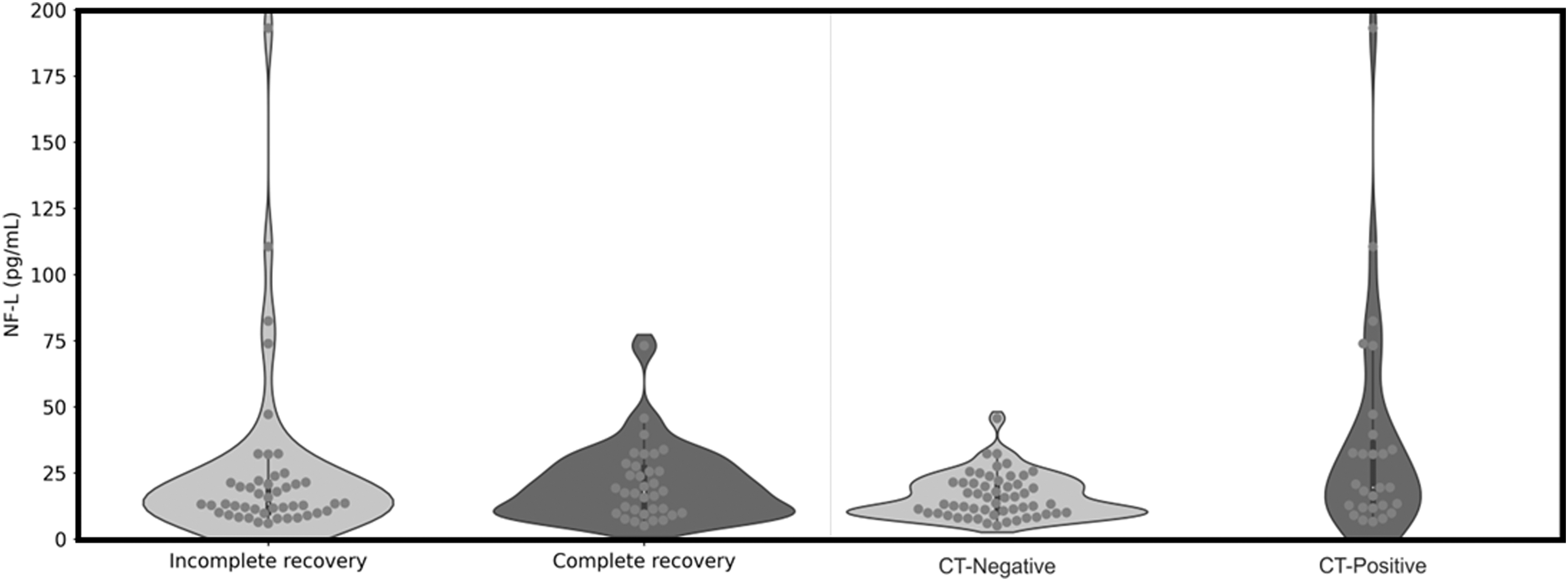
Neurofilament light (NF-L) levels by patient outcome assessed with Glasgow Outcome Scale Extended (GOSE; on left) and computed tomography (CT)-positivity assessed with Marshall score (on right) in patients with mild traumatic brain injury (mTBI). For patient outcome, GOSE 8 was used for full and GOSE <8 for incomplete recovery. For CT-positivity, Marshall score 1 was used for CT-negative and Marshall score 2-6 for CT-positive.
NF-L levels were compared between the outcome groups in CT-positive and CT-negative patients separately. In patients with mTBI, there was no significant difference in CT-negative patients (median 17.37; IQR 10.19, 25.12 for complete recovery and median 12.53; IQR 8.99, 20.20 for incomplete recovery; p = 0.174) nor CT-positive patients (median 25.14; IQR 8.54, 35.24 for complete recovery and median 20.12; IQR 12.74, 67.18 for incomplete recovery; p = 0.551). However, when mTBI patients with GOSE 7-8 were compared with patients with GOSE <7, there was a significant difference in CT-positive patients (median 18.14; IQR 9.82, 32.15 for GOSE 7-8 and median 73.87; IQR 32.17, 110.54 for GOSE <7; p = 0.002) but not in CT-negative (median 12.47; IQR 9.56, 22.39 for GOSE 7-8 and median 16.43; IQR 10.43, 21.41 for GOSE <7; p = 0.702). For patients with mo/sTBI, there was significant difference in NF-L levels between favorable and unfavorable outcome in CT-positive patients (median 32.78; IQR 25.39, 48.93 for favorable outcome and median 63.11; IQR 53.73, 70.88 for unfavorable outcome; p = 0.006). For CT-negative patients, the analyses were not performed since there were only 10 CT-negative patients in mo/sTBI group.
Longitudinal percentage change of NF-L level correlated with GOSE (Spearman's rho = 0.228, p = 0.016) when all patients with TBI were included. However, when the severity groups were analyzed separately, the significance was lost (Spearman's rho = 0.029; p = 0.814 for patients with mTBI and Spearman's rho = -0.0.276; p = 0.070 for patients with mo/sTBI).
The levels of NF-L by GOSE are shown in Figure 3. There was no correlation between the levels of NF-L and GOSE in patients with mTBI (Spearman's rho = 0.101; p = 0.373), but there was a negative correlation in patients with mo/sTBI (Spearman's rho = -0.18; p < 0.001). When the correlation was assessed for CT-positive and CT-negative patients separately, there were no correlation between the NF-L levels and GOSE in CT-negative (Spearman's rho = 0.113; p = 0.430) nor CT-positive (Spearman's rho = - 0.125; p = 0.560) patients with mTBI. However, there was a negative correlation in CT-positive (Spearman's rho = - 0.431; p = 0.009) but not CT-negative (Spearman's rho = - 0.569, p = 0.404) patients with mo/sTBI.
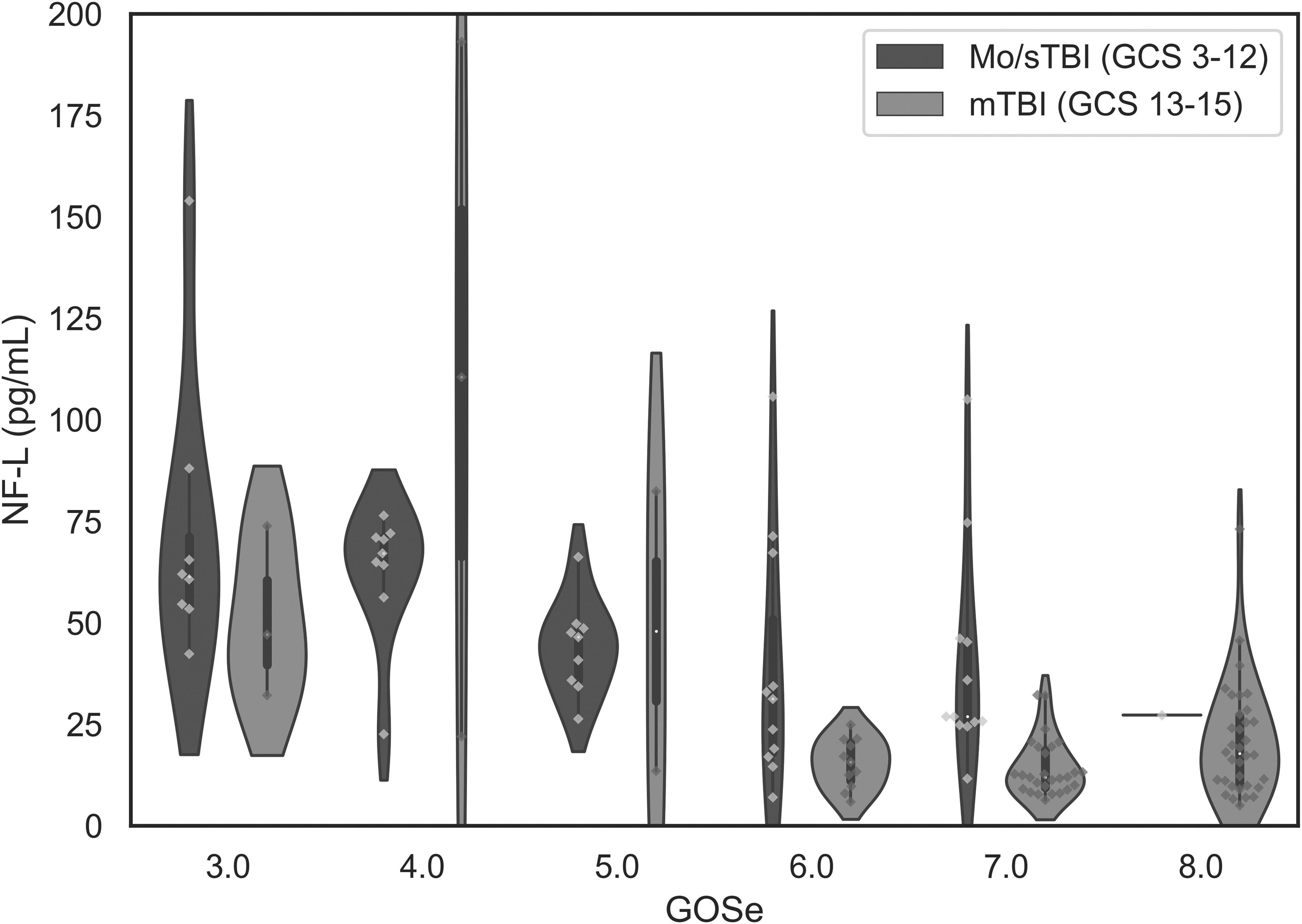
Neurofilament light (NF-L) level by patient outcome assessed with Glasgow Outcome Scale Extended (GOSE) in patients with moderate or severe brain injury (mo/sTBI) and patients with mild traumatic brain injury (mTBI).
Correlations between the levels of NF-L and clinical variables
In patients with mo/sTBI—but not in patients with mTBI—the duration of PTA correlated with the levels of NF-L (Spearman's rho = 0.491; p = 0.003). All correlations between the levels of NF-L and clinical variables are shown in Table 2. In CT-positive patients with mTBI, NF-L levels were not correlated with patient outcome measured with GOSE (Spearman's rho -0.125; p = 0.560). In addition, levels of NF-L did not differ in patients with mTBI when patients with PTA <24 h were compared with patients with PTA >24 h (median 12.99, IQR 9.85, 21.47 and median 19.51; IQR 11.10, 32.10; respectively; p = 0.246). For patients with mo/sTBI, similar analyses were not done since only one patient had PTA <24 h and three patients PTA 1 to 7 days.
Correlation Between the Levels of Neurofilament Light (NF-L) and Clinical Variables
Significant p values in bold.
mTBI, mild traumatic brain injury; mo/sTBI, moderate to severe traumatic brain injury; GOSE, Glasgow Outcome Scale Extended; NF-L, neurofilament light; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia.
Discussion
In this study, we sought to investigate whether NF-L levels measured on the average 9 months after the injury are associated with the contemporaneous outcome in patients with TBIs of different initial severities. The main finding of this study is that in patients with initially mo/sTBI the late levels of NF-L associate significantly with outcome. In addition, CT-positivity in the acute stage was correlated with the later levels of NF-L in patients with initially mTBI. The levels of NF-L were significantly higher in patients with mo/sTBI compared with patients with mTBI and orthopedic controls. However, the significance was found only in CT-positive patients but not in CT-negative patients. These results suggest that in patients with more severe injuries or worse outcome, the levels of NF-L may remain elevated for several months after the injury and these elevated NF-L levels, when combined with the other variables, associate with worse outcome. The diagnostic value of late NF-L in patients with mTBI remains negligible. These findings are in line with the previous studies. 9,20,26,27 When the longitudinal change was compared, the patients with more severe TBI had greater change in the NF-L levels between the two time-points than patients with mTBI. There was correlation between the NF-L percentage change and GOSE when all patients with TBI were included. However, there were no significant correlations at the subgroup level. This may be because of too low sample size for statistical significance.
The duration of PTA has been a strong predictor for long-term outcome in many studies, outperforming the predictions based on GCS. 28 -30 Similarly, in our study, the duration of PTA was strongly associated with the outcome in patients with mTBI, as well as in patients with mo/sTBI. The levels of NF-L correlated with the duration of PTA in patients with mo/sTBI, but not in patients with mTBI. Patients with mo/sTBI had both higher levels of NF-L and longer PTA durations. It has been reported that patients with sports-related concussion and PTA have higher elevations in NF-L levels than those without and that the levels remain increased days after TBI. 31 The pathophysiological mechanism of PTA is not well understood, but it has been suggested to reflect the degree of diffuse axonal injury, 20 although there may also be other underlying mechanisms. Thus, one could expect that the levels of NF-L as an axonal biomarker correlate with the duration of PTA, but this was the case only in patients with mo/sTBI in this study. The lack of association between the levels of NF-L and PTA in milder cases may reflect the small number of cases with a longer PTA or uncertainties in assessing the true duration, which is reflected also in the large number of missing data (PTA was impossible to assess reliably).
Our findings agree with earlier studies that have shown that the levels of NF-L may remain elevated for months to even years after injury. 9,20 This may reflect progressive damage in brain tissue, correlating with a slowly progressively worsening outcome, which may occur in some patients after a TBI. 21,32 In patients with mTBI, the late levels of NF-L did not correlate significantly with outcome. However, when outcome in this group was dichotomized to GOSE 7-8 versus <7, the latter group showed significantly higher levels. Individual cases with mTBI showed fairly high levels of NF-L as shown in Figure 1, but all these with clearly elevated levels were CT-positive.
This was a secondary analysis of a prospective study examining a well-characterized cohort. The main limitation in our study is the nature of our mTBI population, which is more severe than an average mTBI population, based on the recruitment issues in our study. In the recruitment process, only the worst GCS score between the scene of accident and emergency department was used to assess the severity of the TBI. In this cohort, there is a high percentage of CT-positive patients with an mTBI because they were more easily recruited due to hospital admission. 16 Another limitation is that the severity of TBI was graded solely based on the worst GCS. Thus, there are patients that were graded as mild even though some of them had significant intracranial trauma findings and some also a PTA of >24 h. On the other hand, this point underlines our main finding that the late diagnostic value of NF-L in milder TBIs is not clinically applicable even when using ultrasensitive assay. The whole concept of classifying TBIs from mild to severe has been increasingly questioned, due to the uncertainties behind this classification and the often-misleading labels created. 33,34
Moreover, the appropriate time to assess initial severity remains nebulous. Due to the dynamic nature of TBI, up to 40% of patients develop neuroworsening in the intensive care during the first two days. 35,36 The classification of this study has been used also in previous TBIcare-project related papers. 37,38 A larger and more representative population especially in case of mTBI would be needed, and there is a possibility that some of the results are driven by a minority of mTBI patients with neuroworsening. A retrospective assessment of the PTA duration can also be considered as a limitation, although the same experienced neurologist did all assessments using the Rivermead technique. Moreover, information of the PTA duration was missing from a significant percentage of patients in all severity groups because the assessment was not considered reliable due to confounders, such as inebriation or sedatives given. In addition, this was a single center study, which is also a limitation. Last, in accordance with the constraints of clinical reality, there was wide variation in the time of patients' follow-up visits. In some patients, this may have led to better recovery and a decrease in their biomarker levels. However, as far as we can see, this does not change the main result of our study.
Conclusions
Our study supports the concept that NF-L levels may remain elevated for months after the injury and indicate a worse outcome. This was apparent in patients with more severe TBI, but not seen in milder cases in this study. Whether an elevated NF-L > 6 months from the injury simply reflects the severity of the initial injury or is a sign of ongoing damage, remains to be confirmed in future studies. Our results do not support the use of NF-L in the late diagnostics after an initially mild TBI. Further research is needed to study the relationships between acute and late NF-L levels, clinical variables, and patient outcomes.
Transparency, Rigor, and Reproducibility Summary
This study was not formally registered because at the time the study was conducted, observational studies were not routinely registered outside research institutions. The analysis plan was not formally pre-registered, but JPP and OT with primary responsibility for the study and analysis certify that the analysis plan was pre-specified. A sample size of 178 patients and 40 controls with available late phase biomarker levels was included based on the availability of 203 patients and 40 controls from 620 potential participants were screened. Human participants were blinded to results of the fluid biomarker measurements. Handling of biofluid samples was performed by team members who were aware of relevant characteristics of the participants. Fluid biomarker measurements were performed by investigators blinded to relevant characteristics of the participants. Fluid biomarker quality control decisions and analyses were performed by investigators blinded to relevant characteristics of the participants. Fluid biomarkers were labeled using codes that were not linked to participant identifying information. Samples were acquired on average 9 months after the injury (range 5.3-18.5 months) at the Turku University Hospital, Turku, Finland. The samples were centrifuged for 10 min at 10,000 rpm at 4°C, and the plasma was immediately frozen at -80°C for further analysis. Freeze-thaw cycles were performed one time prior to analysis. All samples were analyzed at the same time in a single batch. All equipment and analytical reagents used to perform measurements on the fluid biomarkers are widely available from commercial sources. Additional characteristics of the primary fluid biomarker analyses are presented in the “Methods” section. The key inclusion criteria are established standards in the field. The statistical tests used were based on the assumptions of variable distributions and outliers were defined as described in the “Methods” section. Data are available for qualified investigators upon request from the corresponding author.
Footnotes
Acknowledgments
The results of the study have not been presented or published before.
KB is supported by the Swedish Research Council (#2017-00915), the Alzheimer Drug Discovery Foundation (ADDF), USA (#RDAPB-201809-2016615), the Swedish Alzheimer Foundation (#AF-930351, #AF-939721 and #AF-968270), Hjärnfonden, Sweden (#FO2017-0243 and #ALZ2022-0006), the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG-715986 and #ALFGBG-965240), the European Union Joint Program for Neurodegenerative Disorders (JPND2019-466-236), the National Institute of Health (NIH), USA, (grant #1R01AG068398-01), and the Alzheimer's Association 2021 Zenith Award (ZEN-21-848495).
IH is supported by the Päivikki and Sakari Sohlberg Foundation, the Paulo Foundation, the Finnish Medical Foundation, and the Finnish Cultural Foundation.
HZ is a Wallenberg Scholar supported by grants from the Swedish Research Council (#2018-02532), the European Union's Horizon Europe research and innovation program under grant agreement No 101053962, Swedish State Support for Clinical Research (#ALFGBG-71320), the Alzheimer Drug Discovery Foundation (ADDF), USA (#201809-2016862), the AD Strategic Fund and the Alzheimer's Association (#ADSF-21-831376-C, #ADSF-21-831381-C, and #ADSF-21-831377-C), the Bluefield Project, the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden (#FO2022-0270), the European Union's Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No 860197 (MIRIADE), the European Union Joint Programme–Neurodegenerative Disease Research (JPND2021-00694), and the UK Dementia Research Institute at UCL (UKDRI-1003).
VFJN is supported by an Academy of Medical Sciences / The Health Foundation Clinician Scientist Fellowship.
JPP is supported by the Academy of Finland (Grant 17379) and the Maire Taponen Foundation.
Authors' Contributions
Tuure: Conceptualization; writing—original draft; formal analysis; interpretation of data.
Mohammadian: Conceptualization, formal analysis; writing—review and editing.
Tenovuo: Conceptualization; data curation; resources; writing—review and editing.
Blennow: Resources; writing—review and editing; interpretation of data.
Hossain: Writing—review and editing; interpretation of data.
Hutchinson: Resources; writing—review and editing; interpretation of data.
Maanpää: Writing—review and editing; interpretation of data.
Menon: Resources; writing—review and editing; interpretation of data.
Newcombe: Resources; writing—review and editing; interpretation of data.
Sanchez: Resources; writing—review and editing; interpretation of data.
Takala: Resources; data curation; writing—review and editing; interpretation of data.
Tallus: Resources; data curation; writing—review and editing; interpretation of data.
Zetterberg: Resources; Writing—review and editing; interpretation of data.
Posti: Conceptualization; data curation; resources; writing—review and editing; supervision.
Funding Information
This work was partially funded by the European Commission under the 7th Framework Programme (FP7-270259-TBIcare). Other funding: The Päivikki and Sakari Sohlberg Foundation (IH), The Paulo Foundation (IH), The Finnish Medical Foundation (IH), The Finnish Cultural Foundation (IH), UK NIHR and Royal College of Surgeons of England (PH). The academy of Finland (Grant 17379 to JPP), the Maire Taponen Foundation (JPP).
Author Disclosure Statement
KB has served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, BioArctic, Biogen, JOMDD/Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Ono Pharma, Pharmatrophix, Prothena, Roche Diagnostics, and Siemens Healthineers, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program, outside the work presented in this paper.
HZ has served at scientific advisory boards and/or as a consultant for Abbvie, Acumen, Alector, ALZPath, Annexon, Apellis, Artery Therapeutics, AZTherapies, CogRx, Denali, Eisai, Nervgen, Novo Nordisk, Passage Bio, Pinteon Therapeutics, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, Biogen, and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work).
DKM received personal fees from Lantmannen AB, GlaxoSmithKline plc, Calico Life Sciences LLC, PresSura Neuro, Integra Neurosciences, and NeuroTrauma Sciences, LLC; grants from GlaxoSmithKline plc; and a shared National Institutes of Health grant from Gryphon Collaborators on a grant application outside the presented work.
VFJN holds a grant with Roche Pharmaceuticals for biomarker work outside of the submitted work.
For the other authors, no competing financial interests exist.