
Abstract
Impaired attention is one of the most common, debilitating, and persistent consequences of traumatic brain injury (TBI), which impacts overall cognitive and executive functions in these patients. Previous neuroimaging studies, trying to understand the neural mechanism underlying attention impairment post TBI, have highlighted the role of prefrontal white matter tracts in attentional functioning in mild TBI (mTBI). Goal-Oriented Attentional Self-Regulation (GOALS) is a cognitive rehabilitation training program that targets executive control functions in participants by applying mindfulness-based attention regulation and goal management strategies. GOALS training has been demonstrated to improve attention and executive functioning in patients with chronic TBI. However, its impact on microstructural integrity of attention-associated prefrontal white matter tracts is still unclear. Here, using diffusion magnetic resonance imaging in a pilot randomized controlled trial, we investigated the effect of GOALS training on prefrontal white matter microstructure in 19 U.S. military veterans with chronic mTBI, compared with a matched control group of 14 veterans with chronic mTBI who received standard of care brain health education. We also tested for an association between microstructural white matter changes and sustained attention ability in these patients pre- and post-GOALS training. Our results show significantly better white matter microstructural integrity in left and right anterior corona radiata (ACR) in the GOALS group compared with the control group post-training. Moreover, we found a significant correlation between sustained attention ability of GOALS training participants and white matter integrity of their right ACR pre- and post-training. Finally, our findings indicated that the improved white matter integrity of the ACR in GOALS training participants was the result of increased neurite density and decreased fiber orientation dispersion within this tract.
Introduction
Mild traumatic brain injury (mTBI) is the most common type of TBI, accounting for about 80% of all head trauma. 1,2 Impaired attention is one of the most frequent, debilitating, and persistent consequence of TBI, which impacts overall cognitive and executive functions in these patients. 3 –6 Inability to sustain attention is the main contributor to poor memory and executive control, so that it can impede rehabilitation of dysfunction in other cognitive domains as well. 3 Cognitive rehabilitation in TBI has, therefore, been suggested to be largely focused on attention and executive functions training. 7 –9
Brain structural changes in prefrontal cortex have been frequently reported as the neural mechanism underlying the cognitive impairments post TBI. 10 –12 Moreover, using diffusion tensor imaging (DTI), we previously found the white matter fractional anisotropy (FA), a commonly used metric of microstructural integrity, of anterior corona radiata (ACR) to be positively correlated with attentional functioning in chronic symptomatic mTBI and in controls. 13 ACR has also been shown to be the tract with most frequently low FA values in patients with chronic symptomatic mTBI, defined in the study as persistent symptoms still present more than 4 months post-injury, indicating impaired white matter microstructural integrity. 14
Goal-Oriented Attentional Self-Regulation (GOALS) is a cognitive rehabilitation training program that targets executive control functions in participants by applying mindfulness-based attention regulation and goal management strategies. 15 In contrast to training via practice on isolated tasks, this training protocol involves application of attention regulation skills and strategies to participant-defined goals in their own lives and community, in ecologically valid settings. One of the main training aims is to improve self-regulatory control mechanisms as they contribute to goal attainment. An overarching hypothesis is that improving attention regulation while engaging in goal-directed behavior will help establish more efficient and better integrated functional networks for the performance of goal-relevant tasks and, ultimately, goal attainment in real-life contexts. GOALS training has been demonstrated to improve attention and executive functioning in patients with chronic TBI. 15 –18 However, it is still unclear if GOALS training could indeed lead to microstructural changes in attention-associated prefrontal tracts (e.g., ACR) and whether these brain changes are correlated with attention improvements in the participants.
In this context, DTI, a quantitative magnetic resonance imaging (MRI) technique, has provided important insights into white matter microstructure by providing information on the direction and degree of water diffusivity in white matter tracts. 19 The degree of anisotropy (FA) of water in the white matter tracts reflects their level of integrity. 20,21 Evidence from human brain imaging studies suggests that white matter integrity could change with experience. For example, damage or degeneration to a tract is shown to be associated with a decrease in its white matter integrity (FA). 22 –27 Likewise, training-induced or experience-dependent increases in white matter integrity have also been reported in humans. 28 –30 Moreover, recently developed neurite orientation dispersion and density imaging (NODDI) methodology, based on biophysically inspired modeling of diffusion MRI data, provides further information about tissue microstructure, for example, neurite density and fiber orientation dispersion. 31 –34 The neurite density index (NDI) is a measure of intracellular volume fraction and corresponds to axonal density in white matter; therefore, higher NDI typically corresponds to better microstructural integrity. The fiber orientation dispersion index (ODI) is lowest in tracts with highly collimated white matter fibers; therefore, lower ODI typically corresponds to better microstructural integrity. NODDI has shown promise in the study of a range of disorders, such as neurodegenerative diseases, 35 –38 stroke, 39 epilepsy, 40 first-episode psychosis, 41 amyotrophic lateral sclerosis, 42 and mTBI. 43,44
Recent longitudinal DTI studies in TBI patients have revealed a complex trajectory of microstructural metrics following injury in both civilian mTBI 45 and combat-related TBI. 46,47 DTI has also been used to attempt to disentangle the white matter microstructural changes of mTBI versus post-traumatic stress disorder (PTSD) in combat veterans, 48 with recent data suggesting a role for impaired uncinate fasciculus FA in veteran PTSD. 49 Identifying specific areas of white matter disruption in veterans with TBI is crucial for developing targeted treatment strategies. By tracking changes in white matter microstructure over time or in specific trainings, DTI can help reveal patterns of progression or recovery following TBI in veterans, which is potentially helpful in developing more effective treatment for these individuals.
To this end, we used diffusion MRI to examine the training-induced microstructural changes of prefrontal white matter tracts due to GOALS training in a group of US military veterans with chronic mTBI compared with a matched control group of veterans with chronic mTBI receiving standard of care brain health education (BHE). To our knowledge, this is the first randomized controlled trial to examine rehabilitation-related brain microstructural changes in a sample consisting exclusively of mTBI patients in the chronic phase. We tested our results via both region of interest (ROI) analysis, as well as voxel-wise tract-based spatial statistics (TBSS) analysis. Subsequently, the link between the microstructural integrity of prefrontal white matter tracts in individuals with GOALS training and their sustained attention scores pre- and post-training was tested using DTI. Finally, we used NODDI analysis to investigate whether better white matter integrity in the GOALS group compared with BHE group is the result of changes in tracts’ neurite density and orientation dispersion post-training.
Materials and Methods
Participants
This study was approved by institutional review boards (IRBs) at the University of California San Francisco and San Francisco VA Medical Center. Participants were recruited from the San Francisco VA TBI Clinic, local VA community clinics, and veteran groups using IRB-approved information sheets and flyers. All participants provided informed consent before any study procedures. Inclusion criteria included age of 18 or older, history of chronic mTBI (>6 months post-injury, sustained either in combat or as a civilian), stable psychoactive medication regimen, report of one or more moderate or severe residual cognitive symptoms (on Neurobehavioral Symptom Inventory) that interfere with daily function, and interest and availability to participate in cognitive training. History of mTBI was confirmed through DOD/VA medical records and/or in-person Ohio State University TBI Instrument. Exclusion criteria included history of moderate or severe TBI; unstable medical, neurological, or psychiatric conditions including psychosis, severe PTSD, severe anxiety, or depression precluding participation in research activities such as assessment and/or training; contraindications to MRI; illicit drug or alcohol use problems; and poor English comprehension. Depressive symptoms were assessed using the Beck Depression Inventory-II (BDI-II) 50 . Symptoms of PTSD were evaluated with the PTSD Checklist, Military Version (PCL-M) 51 . Participants also completed self-report measures of daily and emotional functioning, including the Mayo–Portland Adaptability Inventory, 52 a measure of common sequelae of TBI including impact on activities of daily living, emotional adjustment, and community integration. Alcohol use was assessed using the Alcohol Use Disorders Identification Test. Following baseline evaluation, participants were placed in small groups, consisting of two to three participants of similar age for training and the entire group was then randomized to receive either GOALS or BHE training.
Neurocognitive assessment of sustained attention
Participants were evaluated with a multi-level battery that included neuropsychological measures administered before and after GOALS or BHE trainings. Like our previous studies, 15,16 the current study used a neuropsychological battery that included measures of executive function (Delis–Kaplan Executive Function System and Trail Making Test-Part B) and memory (Hopkins Verbal Learning Test–Revised and Brief Visual Memory Test–Revised). The specific focus was to assess sustained attention that is commonly affected by TBI and targeted by GOALS training. Assessments were administered by the same evaluator at both time points, and every attempt was made to administer them at the same time of the day. Evaluators were blinded to participants’ treatment conditions, and evaluators and therapists were separate individuals.
Sustained attention was assessed using the Digit Vigilance Test (DVT) time and error scores. 53 The DVT requires sustained visual attention and accurate identification of target stimuli. Briefly, the participant was given a pencil and two pieces of paper, each containing rows of 35 single-digit numbers. The individual was instructed to cross out every “6” (or “9” post-training, using alternate forms) as rapidly as possible. The examiner recorded the time in seconds that the individual took to complete both pages, as well as the number of errors of omission and commission.
Sustained attention time and error raw test data were converted into T scores obtained from the corresponding normative manual which corrected for demographic factors (including age, education, and gender). 54 These T scores were then transformed into z scores for consistency. The composite sustained attention score is the average of the time and error DVT z scores.
Interventions
GOALS and BHE were matched closely for time with therapists and training intensity. Both were administered across ten 2-h group sessions, three 1-h individual sessions, and 20 h of home practice across 5 weeks. The interventions were conducted in a small group format with two to three participants and two therapists per group. Intervention manuals were written for instructors and participants. 55
GOALS training
GOALS training consisted of two key components. First component included regulation of distractibility which is addressed via applied mindfulness-based attention regulation to redirect cognitive processes toward task-relevant activities. Participants learned to use a metacognitive strategy (‘‘stop-relax-refocus’’) to stop activity when distracted, anxious, and/or overwhelmed; relax; and then refocus attention on the current primary goal. Second component included active application of these GOALS skills to a range of situations and complex goals, from simple information processing tasks to challenging low-structure situations occurring in their own lives (e.g., finding an apartment, looking for a job, writing a school term paper, planning a vacation). Homework included practice in maintaining goal direction during challenging real-life situations identified by participants. Treatment compliance was assessed with a homework log; the beginning of each training session involved a discussion of homework.
BHE training
BHE training was an active comparison matched with GOALS for time with therapists, homework load, and group and individual session participation hours. It was also conducted in a small group format with two to five participants and two therapists per group. The BHE training was designed to be engaging and provide information about brain functioning and brain health. Although session materials included information about effects of stress, sleep, and diet, they were educational in nature, emphasizing knowledge and not skills. Group leaders did not assist participants with making connections between the material presented and possible positive effects on their own daily functioning or how to integrate into their daily lives. Further, the presumed active ingredients of GOALS training, which include applied problem solving and attention regulation, were not part of the BHE intervention.
Scanning parameters
Participants underwent MRI acquisition at baseline and again post-intervention (approximately 6 weeks later) on a 3T Siemens Skyra scanner at the SF VA Medical Center with a 32-channel head coil. Anatomical MPRAGE scans were acquired using T1-weighting with the following parameters: repetition time (TR) = 2400 ms; echo time (TE) = 2.24 ms; flip angle = 8 degrees; in-plane resolution = 0.8 mm; slice thickness = 0.8 mm; number of slices = 208. Multishell multiband diffusion MRI was collected using the Human Connectome Project protocol consisting of spin-echo echo-planar imaging with the following parameters: multiband factor = 3, in-plane resolution = 1.8 mm, TR = 4550 ms, TE = 110 ms, flip angle = 90 degrees; matrix size = 118 × 118, Field Of View (FOV) = 212 × 212 mm, slice thickness = 1.8 mm, and number of slices = 78. Three diffusion MRI scans were collected with 71, 72, and 73 diffusion volumes in sequential order, each with intermixed b values of 0 s/mm2, 1500 s/mm2, and 3000 s/mm2. The scans contained 32 b = 1500 volumes, 32 b = 3000 volumes, and 7, 8, or 9 b = 0 volumes.
DTI data preprocessing
Each participant’s diffusion MRI data underwent quality control inspections and the same preprocessing pipeline to compute DTI and NODDI metrics. The FMRIB Software Library version 6.0.2 (FSL: Oxford Centre for Functional MRI of the Brain, UK; http://www.fmrib.ox.ac.uk/fsl/) 56,57 was used for image preprocessing and DTI parameter computation. The three sequences with interleaved b = 0 s/mm2, b = 1500 s/mm2, and b = 3000 s/mm2 shells were concatenated. A brain mask was created from the first volume of the multi-shell data using Freesurfer’s SynthStrip. 58 FSL’s eddy was applied to the raw multishell diffusion data to correct for motion and eddy current distortions, outlier replacement, susceptibility-by-movement, and slice-to-volume correction. 59 –62 A second brain mask was created from the first volume of the eddy corrected data and applied for skull stripping. The b = 1500 s/mm2 shell volumes were extracted from the processed multishell data and used to calculate DTI parameters. To increase signal-to-noise ratio, the b = 0 s/mm2 were averaged together and used as the first volume followed by the 64 b = 1500 and b = 3000 volumes; this input was used in FSL’s dtifit to calculate FA, mean diffusivity, axial diffusivity, and radial diffusivity maps. The full processed, multishell data including the b = 3000 s/mm2 volumes was analyzed in the accelerated microstructure imaging via convex optimization Toolbox 63 to calculate the NODDI metric maps including NDI, ODI and free water fraction.
ROI analysis
The Johns Hopkins University (JHU) white matter atlas was used for identifying the ROI masks. We used the left and right ACR as ROI for this study, as prior work demonstrated that this was the most frequently injured tract with abnormally low FA in chronic symptomatic mTBI 14 and the one for which FA is correlated with attentional function. 13 We also used left and right superior corona radiata and genu of corpus callosum as the secondary ROI for further FA comparison analysis. The FA value within each ROI for each participant was calculated by taking the average voxel intensity of the skeletonized FA map within the binary mask of the ROI. Between-group comparisons for each ROI were then carried out by entering the individual subject FA value within the ROI into two-sample t-test analyses.
TBSS analysis
Voxel-wise statistical analysis of the DTI FA images was carried out using TBSS 64 in FSL. First, all subjects’ FA images were aligned to the standard 1 × 1 × 1 mm MNI152 template in FSL, using the nonlinear registration tool. Next, the mean FA image was created and thinned to create a mean FA skeleton representing the centers of all tracts, using a threshold of 0.25. Each subject’s aligned FA map was then projected onto this skeleton resulting in each subject’s skeletonized FA image. The analysis was then limited to prefrontal white matter, using the Harvard–Oxford atlas including frontal pole, superior, middle and inferior frontal gyri, frontal orbital cortex, frontal medial cortex, cingulate gyrus, and frontal operculum cortex.
Group differences in voxel-wise FA were examined by entering each subject’s prefrontal white matter skeletonized FA into a general linear model (two-sample t-test) design matrix with nonparametric permutation testing, using the randomize tool in FSL (5000 permutations). The results were thresholded at p = 0.05 (corrected), using the threshold-free cluster enhancement (TFCE) option to find clusters without setting an initial cluster level. 65
To further test whether sustained attention improvement in GOALS group participants was associated with their white matter integrity, we ran a within-group voxel-wise correlation analysis between GOALS participants’ prefrontal white matter skeletonized FA and their sustained attention scores pre- and post-training. Results were multiple comparisons corrected at p = 0.05 using the TFCE option to find the clusters with significant positive or negative correlation with sustained attention in GOALS group participants.
NODDI analysis
For NODDI ROI analysis, the NDI and ODI values within left and right ACR for each participant were calculated by taking the average voxel intensity of the skeletonized NDI/ODI map within the binary mask of the left and right ACR. Also, for investigating the neurite density and orientation dispersion differences between groups within the cluster in which GOALS group had a higher FA than BHE post-training, the cluster that resulted from TBSS analysis was used as the region of analysis. Between-group comparisons for these ROIs were then carried out by entering the individual subject NDI and ODI values within the ROI into two-sample t-test analyses.
Results
Demographics
A total of 426 individuals were assessed for eligibility and 57 consented to this study. Of those who consented, 24 participants were later excluded from the study; 14 withdrew post-consent but before randomization due to loss of contact, moved out of area, or too much time/distance. Eight participants withdrew from the study because of scheduling/travel difficulties and/or family circumstances after being randomized. Two participants completed group training but were unable to complete post-training evaluations because of the COVID-19 shelter-in-place order and are therefore not included in analyses. Therefore, a total of 33 patients with mTBI (19 in GOALS group and 14 in BHE group) completed the study procedures and were included in the present analyses (24% female; mean age = 44.6 years [standard deviation or SD = 14.2]; mean years education = 15.2 [SD = 2.35]). Head injuries were sustained from mixed causes including blunt force injuries, motor vehicle accidents, as well as blast-related. History of more than one mTBI (e.g., military combat training, martial arts training, high school football) was reported by 36% of participants. All participants were independent in basic activities of daily living but reported mild to moderate difficulties on tasks involving organization, problem solving, multitasking, and distractibility. Most participants were not working or going to school, 5 participants were gainfully employed, and 10 were students. Demographics of the two groups are presented in Table 1. There were no significant differences between the groups in demographic or clinical characteristics at baseline.
Demographic Characteristics
Sustained attention represents the average of the group scores at baseline.
p-Values provide the statistical GOALS versus BHE comparison (chi-square test for sex, race, and ethnicity, and two sample t-tests for all other variables).
Missing data: years of education, n = 1 (GOALS); Mayo–Portland total, BDI-II, and PCL-M, n = 7 (GOALS), n = 2 (BHE); sustained attention score, n = 1 (GOALS).
BDI-II, Beck Depression Inventory-II; BHE, brain health education; GOALS, Goal-Oriented Attentional Self-Regulation; PCL-M, Post-traumatic Stress Disorder Checklist—Military Version; SD, standard deviation.
Neurocognitive (sustained attention) test scores
There was no significant difference between the groups in sustained attention z scores at the baseline (p = 0.26). However, a significant group (GOALS vs. BHE) by time (pre- vs. post-training) effect was identified for the sustained attention score (p = 0.03, F = 5.08), such that individuals who received GOALS demonstrated more improvement after treatment compared with those individuals who participated in the BHE intervention. Sustained attention scores (mean and SD) of GOALS and BHE groups pre-training and post-training are presented in Table 2.
Sustained Attention Scores in GOALS and BHE Groups Pre-Training and Post-Trainings
BHE, brain health education; GOALS, Goal-Oriented Attentional Self-Regulation; SD, standard devitaion.
Group differences in white matter integrity based on ROI analysis
Our ROI analysis of white matter tracts in prefrontal lobe (left and right ACR, left and right superior corona radiata, and genu of corpus callosum) demonstrated no significant difference between GOALS and BHE groups before training. However, our ROI results revealed a significantly higher white matter FA in the GOALS group compared with BHE group post-training only in left ACR (t = 1.69, p = 0.034, GOALS: 0.52 ± 0.02; BHE: 0.50 ± 0.03) and right ACR (t = 1.69, p = 0.041, GOALS: 0.51 ± 0.02; BHE: 0.49 ± 0.03). The FA values of right ACR for both groups had a normal distribution. The FA of left ACR in GOALS group, however, had a slightly asymmetrical distribution (skewness = −1.06, p = 0.045). We, therefore, repeated this between-group comparison with nonparametric Mann–Whitney U test as well, and confirmed the FA of left ACR in GOALS group to be significantly higher than BHE group (z score = 1.76, p = 0.038).
We then tested for any association between these white matter differences in ACR and the sustained attention measurement. Our ROI results indicated a moderate correlation between the sustained attention scores of the GOALS group participants pre- and post-trainings with their white matter integrity of right ACR (p = 0.04, R = 0.32; Supplementary Fig. S1A, the datapoints presenting GOALS group data of both pre- and post-training). When we tested for any association between the improvements in sustained attention scores and the changes in white matter integrity in GOALS group, the results indicated a moderate (R = 0.38) but insignificant correlation (due to the small sample size) between the FA of left ACR and the changes in sustained attention score. However, we found that changes in white matter integrity of left ACR in both groups pre- to post-training had a moderate correlation (R = 0.33) with the changes in their sustained attention scores at a strong trend level (p = 0.057; Supplementary Fig. S1B; the datapoints presenting data of both groups post-training).
Group differences in white matter integrity based on voxel-wise analysis
Similar to our results from ROI analysis, voxel-wise (TBSS) analysis indicated no significant difference between GOALS and BHE groups in white matter integrity of prefrontal lobe before training. The results of voxel-wise analysis indicated a significantly higher white matter FA in the GOALS group compared with BHE group post-training in left ACR and left anterior thalamic radiation (Fig. 1A). In order to further explore the between-group differences which would emerge in this randomized controlled trial if the threshold was relaxed, we performed the between-groups voxel-wise comparison post-training with a less conservative corrected p value <0.1 as well. As shown in Figure 1B, GOALS group had a higher white matter FA post-training in a number of left prefrontal white matter tracts, including left ACR, left anterior thalamic radiation, and left side of the genu of corpus callosum. There were no white matter tracts with lower FA in GOALS group than BHE group post-training even with a less conservative p value threshold.

Tracts with higher white matter fractional anisotropy (FA) in Goal-Oriented Attentional Self-Regulation (GOALS) group compared with brain health education (BHE) group post-training.
We then tested for any correlation between white matter integrity of prefrontal tracts in the GOALS group with their sustained attention scores pre- and post-training using the same voxel-wise TBSS analysis. As shown in Figure 2, there was a significant positive correlation between white matter integrity of right ACR and sustained attention scores in GOALS group pre- and post-training. There was no negative correlation between sustained attention scores and any prefrontal white matter tracts in the GOALS group.
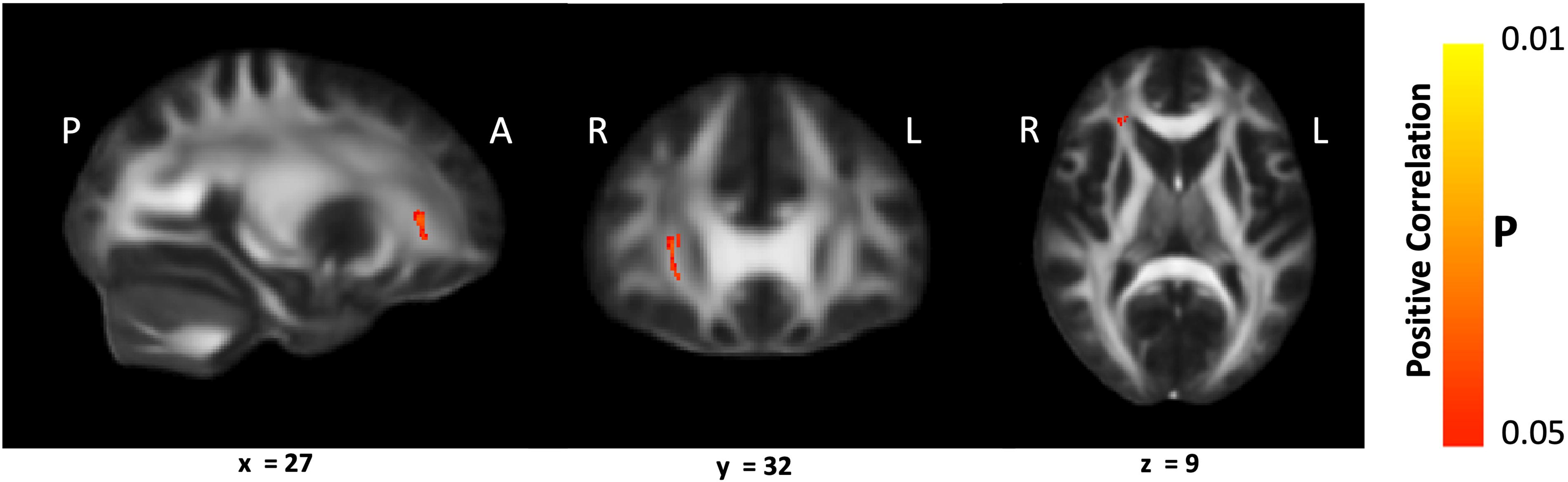
Tracts with significant correlation between white matter fractional anisotropy (FA) and sustained attention score in Goal-Oriented Attentional Self-Regulation (GOALS) group. Sustained attention score in the GOALS group was positively correlated with the white matter FA of right ACR pre- and post-training, after correction for multiple voxel-wise comparisons (p < 0.05). There was no significant negative correlation between sustained attention scores and any white matter tracts in the GOALS group.
There were no statistically significant within group differences pre- to post-training in either group, due to the small sample size of this randomized control trial.
Group differences in white matter integrity based on NODDI analysis
We further investigated microstructural changes of the tracts in which the GOALS group had a higher white matter FA than BHE group post-training. On JHU ROI analysis, there was no significant between-group difference in NDI or fiber ODI of left or right ACR before training. However, the mean NDI of the right ACR was higher in the GOALS group compared with the BHE group after training (p = 0.048, GOALS: 0.64 ± 0.02; BHE: 0.61 ± 0.06) with a strong trend toward higher mean NDI in the left ACR as well (p = 0.057, GOALS: 0.66 ± 0.03; BHE: 0.63 ± 0.06). The NDI values of the right and left ACR for both GOALS and BHE group had normal distributions. When testing the between-group differences in NDI and ODI post-training within the voxel cluster which had a significantly higher white matter FA in the GOALS group vs. BHE group, there was significantly higher NDI (p = 0.029, GOALS: 0.63 ± 0.03; BHE: 0.59 ± 0.07) as well as significantly lower ODI (p = 0.005, GOALS: 0.16 ± 0.01; BHE: 0.18 ± 0.02) in the GOALS group than BHE group post-training.
Discussion
Impaired attention is one of the most debilitating and persistent consequence of TBI, and the main contributor to poor memory, comprehending language, and executive control, which can impede rehabilitation of dysfunction in other cognitive domains as well. 3 –6 Cognitive rehabilitation in TBI has, therefore, been suggested to be largely focused on attention and executive functioning training. 7 –9 Previous DTI studies, trying to understand the neural mechanism underlying attention impairment post TBI, have highlighted the role of prefrontal white matter tracts, especially decreased white matter integrity of ACR in patients with mTBI. 10 –14 Recent large-scale longitudinal DTI studies have revealed a complex trajectory of microstructural metrics following TBI, with declining FA and rising diffusivities indicating deteriorating white matter integrity especially in frontal lobes, as demonstrated in both civilian mTBI 45 and combat-related TBI. 46,47 DTI has also been used to attempt to disentangle the white matter microstructural changes of TBI versus PTSD in combat veterans, 48 with recent data suggesting a role for impaired uncinate fasciculus FA in veteran PTSD. 49 Identifying specific areas of white matter disruption in veterans with TBI is crucial for developing targeted treatment strategies. By tracking changes in white matter microstructure over time, DTI reveals patterns of progression or recovery following TBI in veterans, which is potentially useful for monitoring the effectiveness of treatment.
GOALS is a cognitive rehabilitation training program that targets executive control functions in participants by applying mindfulness-based attention regulation and goal management strategies. 15 GOALS training improves attention and executive functioning in patients with chronic TBI. 15 –18 However, it has been still unclear if GOALS training could lead to microstructural changes in attention-associated prefrontal tracts (e.g., ACR) and whether these brain changes are correlated with attention improvements in the participants.
In this study, we used DTI and NODDI in a proof-of-concept randomized controlled trial to investigate the effect of 5 weeks of GOALS training on the microstructural changes of prefrontal white matter in patients with chronic mTBI, compared with a matched control mTBI group receiving standard of care. Moreover, we tested for any association between these microstructural changes and sustained attention ability in these patients pre- and post-GOALS training.
Our neurocognitive measurements indicated a significant group (GOALS vs. BHE) by time (pre- vs. post-training) effect for the sustained attention score, such that individuals who received GOALS demonstrated more improvement after treatment compared with those individuals who participated in the BHE intervention. ROI analysis of white matter tracts from DTI in prefrontal lobe revealed significantly higher white matter integrity in GOALS group compared with BHE group post-training in left and right ACR tracts. Also, our voxel-wise TBSS analysis indicated a significant increased white matter integrity in GOALS group compared with BHE group post-training in left ACR and left anterior thalamic radiation tracts. Moreover, from both ROI and voxel-wise correlation analyses, GOALS group participants showed a significant positive correlation between their sustained attention scores and the white matter integrity of right ACR pre- and post-training.
While looking at the correlation between the improvements in sustained attention scores and the changes in white matter integrity, we found the FA of left ACR in both groups pre- to post- training to be correlated with the changes in their sustained attention. It is noteworthy to mention that one of the GOALS participants had a substantial gain from this training as demonstrated in their significant changes of both sustained attention scores and white matter integrity. Although they might appear as a potential outlier for the study and the observed correlation could be much less without them (Supplementary Fig. S1B), in a pilot study, it is important to document such results since larger follow-up studies may show an important subset of patients that may exhibit outsized gains from the treatment and even lead us to a further investigation of identifying the subset of patients who would have the maximum gain from the type of training.
Finally, NODDI analysis demonstrated a higher neurite density in the left and right ACR in the GOALS group as compared with the BHE group after training. When testing the between-group differences in NDI and ODI post-training within the voxel cluster which had a significantly higher white matter integrity in GOALS group vs. BHE group, we found that higher white matter FA in GOALS group, compared with BHE group, post-training was due to increased neurite density and decreased fiber orientation dispersion in this region of the ACR. Therefore, rising intracellular volume fraction contributes to the observed neuroplasticity of ACR on DTI, whereas improved fiber organization also plays a role in the core region of microstructural change within the ACR.
These findings represent, to our knowledge, the first evidence of neuroplasticity associated with cognitive training in chronic mTBI, although the precise neurobiological mechanism remains unclear. The attention training-related improvements of microstructural integrity in the ACR are consistent with prior work implicating this prefrontal white matter tract in microstructural damage long-term post-mTBI 14 and in attention deficits in chronic symptomatic mTBI patients. 13 Limitations of the study include that (1) longer-term treatment-related benefits of this intervention are unknown, (2) other treatments that the veterans may have been undergoing were not accounted for, and (3) missing data due to compliance issues, especially for tests such as the BDI-II and PCL-M, (4) although a correlation of ∼0.3 is considered moderate by some standards and is in line with other cognitive/behavioral treatment interventions, the effect size of the observed benefit of GOALS in this study can be considered modest. These shortcomings are mostly due to the smaller sample size that reflect the recruitment limitations during the COVID-19 pandemic. The next follow-up studies with larger sample size will help overcome this limitation.
These proof-of-concept observations need to be validated in larger studies designed to assess the potential of diffusion MRI metrics as biomarkers for mTBI patient selection and for treatment response in trials of cognitive/behavioral interventions. Continuing progress in MR scanner hardware, pulse sequences, and computational image processing, including deep learning and generative artificial intelligence, should yield further advances in the sensitivity and precision of diffusion MRI for brain microstructural plasticity as well as help translate this methodology into clinical practice.
Transparency, Rigor, and Reproducibility Statement
The study was pre-registered at clinicaltrials.gov (NCT02920788). The analysis plan was not formally preregistered. A sample size of 62 subjects was planned and the sample size for the present study is 33 subjects, 19 in the treatment group, and 14 in the active control group. Enrollment fell short of the target due to the COVID-19 pandemic: 426 potential participants were screened, imaging data were obtained from 43, and successfully analyzed in 33 who completed treatment, provided pre- and post-diffusion MRI data, and met data quality assurance criteria. Imaging acquisition, imaging quality control decisions, and analyses were performed by team members blinded to treatment allocation of participants. All equipment and software used to perform imaging and pre-processing are widely available from commercial sources. The key inclusion criteria and outcome evaluations are established standards. At this time, no replication or external validation studies have been performed or are planned/ongoing to our knowledge, but our team is currently in the early stages of planning a replication and validation study. De-identified data from this study are not available in a public archive. De-identified data from this study will be made available (as allowable according to IRB standards) by emailing the corresponding author. Analytic toolboxes used to conduct the analyses presented in this study are available as open-source software. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Footnotes
Acknowledgment
The authors would like to acknowledge Jerry Chen, Marissa Cassar, and Maria Kryza-Lacombe for their valuable contributions to this project.
Authors’ Contributions
H.K.: Formal analysis (co-lead); writing—original draft (lead); and writing—review and editing (supporting). J.W.-J.: Formal analysis (co-lead); software (lead); writing original draft (supporting); and writing—review and editing (supporting). A.H.: Methodology (supporting) and software (supporting). R.S.: Methodology (supporting) and writing—review and editing (supporting). S.R.: Methodology (supporting). L.T.C.: Methodology (supporting) and software (supporting). J.X.: Methodology (supporting) and software (supporting). B.A.M.: Formal analysis (supporting). G.A.: Conceptualization (equal); methodology (supporting); and writing—review and editing (supporting). T.N.A.: Conceptualization (equal); methodology (equal); formal analysis (supporting); and writing—review and editing (supporting). P.M.: Conceptualization (lead); methodology (lead); formal analysis (supporting); and writing—review and editing (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by grant 1 I01 RX002300 awarded to P.M. by VA Rehabilitation Research & Development and the Office of Academic Affiliations Department of Veterans Affairs. The data analysis and writing of the article were supported by Advanced Fellowship in Polytrauma by Office of Academic Affiliations of Veterans Affairs awarded to H.K. and by grant 23CDA1054207 from American Heart Association awarded to H.K.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.