
Abstract
Outcomes after severe traumatic brain injury (TBI) can be represented by a sliding score that compares actual functional recovery to that predicted by illness severity models. This approach has been applied in clinical trials because of its statistical efficiency and interpretability but has not been used to describe change in functional recovery over time. The objective of this study was to use a sliding scoring system to describe the magnitude of change in Glasgow Outcome Scale Extended (GOSE) score at 6, 12, and 24 months after severe TBI and to compare patients who improved after 6 months to those who did not. This study included consecutive severe TBI patients (Glasgow Coma Scale ≤8; n = 482) from a single center. We grouped patients into four strata based on probability of unfavorable outcome (GOSE = 1–4) using the International Mission on Prognosis and Analysis of Clinical Trials (IMPACT) model, selected a dichotomous GOSE threshold within each stratum, and compared each patient's GOSE to this threshold to calculate a score (GOSE-Sliding Scale [SS]) from -5 to +4 at 6, 12, and 24 months. We compared GOSE-SS at 6 months with GOSE-SS at 12 and 24 months and also compared characteristics of participants who improved after 6 months with characteristics of those who did not using χ2 and t tests. Compared with at 6 months, 40% of patients (n = 74) had improved GOSE-SS at 12 months, and 53% had improved GOSE-SS by 24 months (n = 72). Among those who improved at 12 months, the average magnitude of improvement was 1.7 ± 0.9 and among those who improved at 24 months, the average magnitude of improvement was 1.9 ± 1.0. Those who improved their GOSE-SS score from 6 to 24 months had longer hospital stays (mean-difference = 8.6 days; p = 0.03), longer intensive care unit (ICU) stays (mean-difference = 5.5 days; p = 0.02), and longer ventilator time (mean-difference = 5 days; p = 0.02) than those who worsened. These results support an optimistic long-term outlook for severe TBI patients and emphasize the importance of long-term follow-up in severe TBI survivors.
Introduction
Traumatic brain injury (TBI) is a public health burden that costs the global economy $400 billion per year. 1 Predicting long-term outcomes has been a major focus of TBI research, as an accurate prognosis could inform early treatment decisions. 2 –4 Prognostic models, such as the International Mission on Prognosis and Analysis of Clinical Trials (IMPACT), were developed >25 years ago using clinical characteristics measured on admission. 5 IMPACT was validated to predict unfavorable functional outcomes at 6 months post-injury, a binary outcome defined as a Glasgow Outcome Scale (GOS) score of 1–3 or 1–4 on the GOS-Extended (GOSE) scale. 5
Dichotomizing outcomes substantially reduces the information contained in more granular ordinal scales such as the GOSE, reducing statistical power and clinical interpretability. 6 Considering GOSE as a fully ordinal model preserves information, but conventional statistical approaches rely on a proportional odds assumption (i.e., that the association of a particular predictor with outcome is constant across any one-point change in the outcome scale) that is frequently violated after TBI. 7 –9
An alternative approach, called the “sliding dichotomy,” was introduced in the late 1990s, and categorized patients based on baseline prognosis using models such as IMPACT. 7,10 Using this approach, the threshold to dichotomize GOSE is allowed to vary based on an individual patient's illness severity. Although it incorporated baseline prognosis, this technique still collapsed GOSE into a binary outcome. To overcome this limitation, the “sliding scoring” method was developed, which stratifies patients based on their predicted outcomes (like the sliding dichotomy approach) and then calculates the difference between patient's observed GOSE and their stratum's cut-point for favorable prognosis. 2,11 A key advantage of the sliding scoring approach is that it quantifies the magnitude of change in functional outcome while controlling for baseline prognosis. 2 This method has been applied to the interpretation of treatment effect in clinical trials and significantly improved study power at a 6-month cutoff, 2,11 although few clinical trials in TBI have used this approach. 11
The function of patients with severe TBI can improve over a longer recovery period than has been historically appreciated. 12 –14 By 2 years post-injury, most patients have either died or achieved favorable functional outcomes (when assessed in a binary fashion). 12 –16 Further, the sliding scale approach has only been applied to 6-month outcomes in clinical trials, limiting understanding of improvement over time. We applied this methodology to a cohort of severe TBI patients to characterize change in function over time, accounting for baseline prognosis. This approach can help improve power assessments in clinical trials for time points past 6 months. A secondary purpose of this study was to compare patients who survived and improved after 6 months with those who survived and regressed after 6 months, based on baseline clinical characteristics.
Methods
Design and participants
This is a retrospective analysis of prospectively collected database of patients who presented to a single level 1 trauma center with severe TBI (post-resuscitation Glasgow Coma Scale [GCS] ≤ 8) from 2002 to 2018 (n = 598). 17,18 Patients with complete clinical and outcomes data at 6 months post-injury were included for analyses (n = 482; 80.6%). Exclusion criteria for this study were being <18 years of age, pregnancy, penetrating trauma, or GCS = 3 with bilaterally non-reactive dilated pupils. Subjects' representative provided consent. This study was approved by the University of Pittsburgh 11 Human Research Protection Office.
IMPACT prognostic model
The full IMPACT prognostic model for unfavorable outcomes and mortality at 6 months were calculated based on age, GCS motor score, pupil reactivity, hypoxia, hypotension, computed tomography (CT) classification, traumatic subarachnoid hemorrhage on CT scan, epidural mass on CT scan, glucose (mmol/L), and hemoglobin (g/dL). This risk score ranges from 0 to 100%, with higher scores indicating greater risk of unfavorable outcome at 6 months. 5
Glasgow Outcome Scale Extended Sliding Scale (GOSE-SS)
GOSE is a functional outcome scale which in this cohort was prospectively completed at 6, 12, and 24 months post-injury by a trained researcher. GOSE scores range from 1 to 8, where 1 corresponds to death and 8 corresponds to upper good recovery. 19 In general, a higher GOSE score is viewed as more “favorable” to the patient, because of its association with higher level of independent function, than a lower score. The IMPACT model was used to generate predicted probabilities for an “unfavorable” outcome, which was defined for validation of the IMPACT model as a GOSE score of 1–4. Predicted probabilities were separated into four categories: 0–0.20, 0.21–0.40, 0.41–0.55, and ≥0.56, as proposed by Yeatts and coworkers. 2 For each category, the median GOSE score was determined and used as the reference score for that category. 2 The reference score for each prognostic category was based on 6-month outcomes to be consistent with the original IMPACT model. This reference score was used for all time points. Participants were then assigned a sliding score from -5 to +4 at each time point, calculated by comparing their GOSE score to their category's cutoff. An illustrative table of how the GOSE-SS is applied based upon the IMPACT model's predicted probabilities can be viewed in Table S1. Negative GOSE-SS corresponds to poorer recoveries than empirically predicted from the IMPACT model, whereas positive GOSE-SS corresponds to superior recoveries more than empirically predicted from the IMPACT model.
Statistical analysis
Descriptive statistics for the overall sample were calculated at 6, 12, and 24 months post-injury. To calculate differences in functional outcome over time, GOSE-SS scores were subtracted from the prior time point (i.e., GOSE-SS difference at 12 months = GOSE-SS at 12 months – GOSE-SS at 6 months). For comparison, we also described differences in GOSE scores classified as a binary outcome where 1–3 = unfavorable and 4–8 = favorable outcome for each time frame. GOSE scores of 1 (death) were included in summary statistics for sliding scale outcomes, but people with a GOSE = 1 at 6 months were not included in the difference over time analyses, because 95.8% of patients who died during the follow-up period (2 years) had died by 6 months. To compare characteristics of participants who improved over time (i.e., had a positive GOSE-SS difference from the previous time point) with those who deteriorated over time (i.e., had a negative GOSE-SS difference from the previous time point), χ 2 tests for categorical variables and independent samples t tests for continuous variables were conducted. Patients with no change in GOSE over time were excluded from that comparison. Little's test was statistically significant for GOSE at 6, 12, and 24 months to assess if missing data were completely at random. A sensitivity analysis was subsequently conducted to describe differences in baseline characteristics, IMPACT risk scores for mortality and unfavorable outcomes, and surgical/post-surgical variables. Chi-square tests for categorical variables and independent samples t tests for continuous variables were conducted. Statistical significance was set to p < 0.05. Analyses were conducted in SPSS v28.0.1.1.
Results
GOSE-SS long-term outcomes
Descriptive statistics for the overall sample can be viewed in Table 1. Sliding scale outcomes at 6, 12, and 24 months post-injury can be viewed in Figure 1. At 6 months post-injury, 81.3% of patients had negative GOSE-SS scores, 8.7% had GOSE-SS = 0, and 10.0% had a positive GOSE-SS score. At 12 months post-injury, 77.0% of patients had negative GOSE-SS scores, 7.6% had a GOSE-SS = 0, and 15.4% had a positive GOSE-SS score. At 24 months post-injury, 75.9% of patients had negative GOSE-SS scores, 8.0% had a GOSE-SS = 0, and 15.3% had positive GOSE-SS scores.

Percent of participants with each sliding scale score at 6 (n = 448), 12 (n = 435), and 24 months (n = 386) following severe TBI.
Descriptive Statistics for the Overall Sample With Complete Data at 6 Months Post-Injury (n = 482; Mean ± SD or Number [%])
SD, standard deviation; GCS, Glasgow Coma Scale; CT, computed tomography; IMPACT, International Mission on Prognosis and Analysis of Clinical Trials
Difference in GOSE-SS outcomes between 6 and 12 months, between 12 and 24 months, and between 6 and 24 months can be viewed in Figure 2. Comparisons between the binary classification method outcomes and GOSE-SS outcomes over time can be viewed in Table 2. Group comparisons between participants missing GOSE and those not missing GOSE can be viewed in Table S2. On average, patients who survived at least 6 months improved their GOSE score by a magnitude of 0.5 ± 1.2 from 6 to 12 months and by a magnitude of 0.3 ± 1.1 from 12 to 24 months. Patients who survived 6 months improved their GOSE score by 0.8 ± 1.4 from 6 to 24 months.
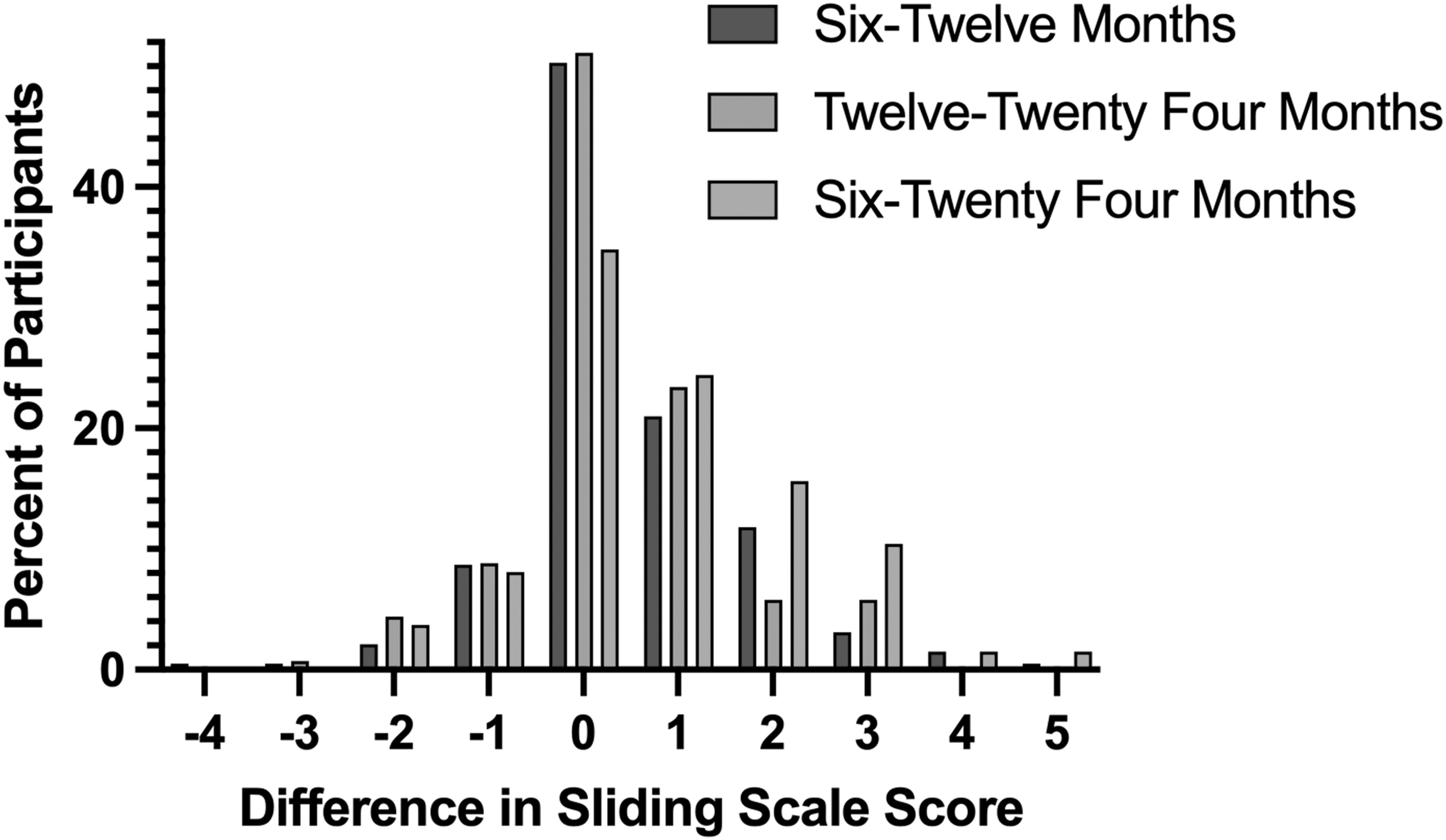
Difference in sliding scale scores from 6 to 12 months, 12 to 24 months, and 6 to 24 months post-injury in patients who survived at least 6 months. Zero indicates no change from 6 months. Positive integers indicate improvement from 6 months. Negative integers indicate worse functioning from 6 months.
Percent of Overall Cohort Who Had Improved, Unchanged, or Worsened Functional Status Over Time per a Binary (Glasgow Outcome Scale Extended = 1–3 vs. 4–8) or Sliding Scale Classification
Improvement in binary classification terms denotes changing from a Glasgow Outcome Scale Extended (GOSE) score of ≤3 to ≥4, whereas worsening denotes the opposite. Improvement in sliding scale (i.e., GOSE-SS) terms denotes any position change in functional status, whereas worsening denotes any negative change in functional status.
Five (2.5%) patients who were alive at 6 months died by 12 months. The proportion of patients with negative sliding scale scores who died by 6 months (3.1%) was not different from the proportion of patients with positive sliding scale scores who died by 12 months (1.4%; p = 0.66). Nine (6.3%) patients who were alive at 6 months died by 24 months. The proportion of patients with negative sliding scale scores who died by 24 months (7.4%) was not different from the proportion of patients with positive sliding scale scores who died by 24 months (4.0%; p = 0.50).
Among severe TBI survivors with negative GOSE-SS at 6-months, 21.0% transitioned to neutral or positive outcomes by 12 months, and 37.9% had transitioned to neutral or positive GOSE-SS at 24 months.
Characteristics of patients who improved GOSE scores at 12 and 24 months
Patients who improved GOSE-SS from 6 to 12 months averaged a 1.7 ± 0.9 magnitude improvement. No difference was observed between those who improved their GOSE-SS score from 6 to 12 months and those who worsened from 6 to 12 months in their age (p = 0.91), GCS score at admission (p = 0.76), IMPACT mortality risk score (p = 0.26), IMPACT unfavorable outcomes risk score (p = 0.23), number of males (p = 0.23), having surgery (p = 0.27), length of hospital stay (p = 0.10), length of intensive care unit (ICU) stay (0.23), or number of days on a ventilator (0.37).
Patients who improved their GOSE-SS from 6 to 24 months averaged a 1.9 ± 1.0 magnitude improvement. Those who improved their GOSE-SS score between 6 and 24 months (n = 72) had longer hospital stays (mean difference = 8.6 days; p = 0.03; d = 0.63), longer ICU stays (mean difference = 5.5 days; p = 0.02; d = 0.68), and longer time on a ventilator (mean difference = 5 days; p = 0.02; d = 0.64) than those whose GOSE-SS score worsened from 6 to 24 months following injury (n = 16). There was no difference between groups in age (p = 0.22), GCS score at admission (p = 0.46), IMPACT mortality risk score (p = 0.16), IMPACT unfavorable outcomes risk score (p = 0.054), number of males (p = 0.55), or having surgery (p = 0.10).
Discussion
In this cohort study of severe TBI survivors at 6 months post-injury, adjusting the definition of favorable outcome to incorporate baseline prognostic risk revealed that approximately one in three improved their GOSE from 6 to 12 months post-injury, and that half improved their GOSE from 6 to 24 months post-injury. This method revealed improvements in functional status that would have been missed with binary classification of favorable (GOSE = 4–8) and unfavorable (GOSE = 1–3) outcomes, as only 6.8–9.0% of patients improved from unfavorable to favorable classification over those time frames. Only 1 in 10 patients who survived to 6 months worsened from 6 to 24 months post-injury. Approximately 40% of severe TBI patients who survived 6 months with functional outcomes worse than predicted (i.e., had negative GOSE-SS scores) improved to meet or exceed prognostic expectations by 24 months (i.e., had GOSE-SS ≥0). Patients whose GOSE improved from 6 to 24 months had longer stays in the ICU (+5.5 days), longer time on a ventilator (+5 days), and longer general hospital stays (+8 days). These results contribute to this growing body of literature by demonstrating the added value of the sliding scoring method for monitoring long-term changes in functional outcome, the significance of interpreting functional outcomes within the context of acute clinical presentation, and the importance of optimistic and aggressive acute clinical care for better outcomes in severe TBI survivors.
The results of the current study support the notion of a more optimistic long-term outlook following severe TBI than had been previously appreciated. 17,18,20 Many studies have reported that the predominant reason for death after severe TBI was the withdrawal of life-sustaining care, commonly occurring within 72 h post-injury. 21 –23 As a result, the American College of Surgeons Trauma Quality Improvement Program guidelines for management of TBI currently recommend at least 72 h of care before withdrawal of life-sustaining care determinations could be made. 24 However, several large multi-center studies (e.g., Transforming Research and Clinical Knowledge in Traumatic Brain Injury [TRACK-TBI], TBI Model Systems Program) have reported that a majority of severe TBI patients in a vegetative state or with disorders of consciousness can improve neurological and functional status over the course of weeks to years post-injury. 14,15,25 This evidence has not translated into clinical practice. 26 In 2022, a survey of 308 practicing neurosurgeons listed impaired neurological function and likelihood of being in a vegetative state as significant factors associated with their recommendation to withdraw life-sustaining care. 27 In 2023, the Seattle International Severe Traumatic Brain Injury Consensus Conference Working Group reported that 15% of panelists would justify withdrawal of care if the ultimate outcome was “upper severe disability.” 28 On the GOSE, upper severe disability corresponds to a GOSE = 4, which is now widely considered to be a favorable outcome from severe TBI because of its association with up to 8 h of independent living per day. Communicating this robust body of evidence to neurotrauma practitioners is critical to limit unnecessary loss of life in this population.
In the present study, longer time in the hospital and ICU and on a ventilator were associated with improving GOSE score from 6 to 24 months. Patients who improved over this time frame stayed on a ventilator for an average of 14 days and in the ICU for 20 days, and had a total hospital stay of 28 days. This is substantially longer than previously reported in studies of severe TBI patients. Williamson and coworkers 23 retrospectively analyzed the American College of Surgeons-Trauma Quality Improvement Program database from 2013 to 2015, which incorporates >700 trauma centers in the United States. In an analysis of nearly 38,000 patients with severe TBI, patients who were withdrawn from life-sustaining therapy (n = 7869) stayed on a ventilator for an average of 4.8 days, in the ICU for 5.2 days, and in the hospital an average of 5.3 days. 23 The length of care in the present study was approximately double the length of care reported for those who did not experience withdrawal of life-sustaining therapy in the study study by Williamson and coworkers 23 (n = 30,080; ventilator days = 7.5, ICU days = 9.7, total hospital days = 15.4). Unfortunately, long-term follow-up was not available for the study by Williamson and coworkers. 23
The present study emphasizes the importance of long-term follow-up for patients with severe TBI. Follow-up past the acute phase of recovery from TBI can be challenging. 25 Obtaining GOSE at 6 months post-TBI is the research gold standard for primary outcome, but many prospective or interventional studies report missingness of this variable >10%. 29 –31 TBI research dogma is that patients with missing outcome data are either doing well or doing poorly, but there are currently no standards within TBI research to address missingness. 29 Richter and coworkers 31 conducted a systematic review of how missing outcome data is handled in TBI research, and found that 36% of studies provide insufficient information about missingness and that only half of the studies that acknowledge missing data attempt to explain why. Comparing patients with missing GOSE to those without at 6, 12, and 24 months in the present study revealed meaningful differences between groups. The general trend observed was that patients who were lost to follow-up at 6, 12, and 24 months following severe TBI exhibited baseline clinical characteristics suggestive of less severe injuries and better prognosis, such as younger age, less severe CT classification, lower risk scores, and increased time receiving level 1 trauma hospital care (Table S1). This result may suggest that if complete data were obtained for GOSE at all time points, higher percentages of positive changes (or neutral changes) would have been observed. Restated, the results of the present study may underestimate the number of patients who improved from 6 to 12 or from 6 to 24 months.
Although GOSE remains the gold-standard functional outcome in TBI trials, there is a growing consensus that modifications could improve its impact. For example, Hong and coworkers used the Rasch partial-credit model to investigate the psychometric properties of GOSE items and found a ceiling effect and poor reliability. 32 In an effort to promote inter-rater reliability within studies and across institutions, an updated manual for GOSE was published in 2021. 33 Magnus and coworkers 34 used item-response theory from the GOSE structured interview and reported higher sensitivity to detect changes in functional outcome. Alternatively, the Brain Injury Functional Outcome Measure (BI-FOM) was recently introduced by the TBI Model Systems investigators as a reliable and valid measure of functional outcome in moderate-to- severe TBI patients. 35 Efforts to improve assessment of functional status in this highly variable population will improve research study design and clinical impact.
Limitations
These results should be considered within the context of certain limitations. This study is a retrospective analysis, which introduces bias. This data set was obtained from patients who presented to a single level 1 trauma center, indicating the results (especially for treatment time) may not generalize to other medical centers. Only severe TBI patients were included in this analysis. It is unclear how (or if) the sliding scoring system applies well to moderate or mild TBI. Missingness of analyzed data ranged from 0 to 30.3%. However, all variables except GOSE had missingness <10%. Multiple imputation has been recommended for TBI research with missing data, 30,31 but was not conducted in this study. There is disagreement on whether or not missing ordinal data should be imputed, 36 which is the structure for our primary outcome (GOSE). As a result, no guidelines exist for imputing GOSE data for TBI research without recoding it as a continuous variable, which introduces significant bias. 6,36 IMPACT has been repeatedly validated to discriminate between favorable and unfavorable outcomes at 6 months, but only recently have researchers reported that IMPACT has similar discriminative validity at 12 and 24 months post-injury. 17 Future work should investigate the sliding scoring approach with longer follow-up times. The GOSE-SS approach identified that 81% of the surviving sample had negative GOSE-SS scores at 6 months, indicating that their functional outcome was worse than would have been predicted by the IMPACT model. Given that the IMPACT model was validated to predict unfavorable 6-month outcomes, exploring this result further could be an important area of future work beyond the scope of this article.
Conclusion
In this cohort study of patients with severe TBI who presented to a level 1 trauma emergency department, meaningful improvements in functional outcome were observed from 6 months to 2 years post-injury when evaluated with the sliding scoring method. If analyzed based on the traditional binary classification, only 4.5–9.0% of patients would have improved from having unfavorable to having favorable outcomes over time. For patients with functional outcome data at follow-up, 38–53% improved functional status by 12 and 24 months post-injury, while only 12% worsened functional status. Patients who improved had longer hospital stays and longer time on a ventilator, emphasizing the importance of acute commitment to recovery. Approximately 40% of survivors with suboptimal outcomes at 6 months improved to meet or exceed prognostic expectations by 2 years post-injury. Patients who were lost to follow-up appeared to have less severe injuries based upon baseline characteristics than patients who completed follow-up. The results of this study suggest that severe TBI patients treated acutely at a level 1 trauma center have the capacity to improve functional status after 6 months up to 2 years post-injury. The sliding scoring method appears to be a useful metric to describe magnitude of longitudinal improvement in functional outcome compared with the binary classification method. The results of this study support clinical optimism for long-term outlook following severe TBI.
Transparency, Rigor, and Reproducibility Summary
This study was not pre-registered online, as data collection for the data set has been ongoing for 4 years. The analysis plan was not pre-registered online but was conceived and executed by S.R.E. and reviewed by M.P. and J.E. with biostatistics backgrounds. S.R.E.certifies that the analysis was pre-specified. A sample size of 482 was utilized based on availability of data from patients with severe TBI. Given the novel application of a newer statistical technique, effect sizes were not calculated. Data collection and analyses were performed by investigators who were aware of relevant participant characteristics. Data were pulled from institutional electronic health records. All outcome measures used are publicly available. Data and analytic code can be made available based on reasonable request. SPSS v28 was used for all analyses. The key inclusion criteria are established standards in the field. Missing data were handled as reported in the text. No replication or external validation studies have been performed or are planned/ongoing at this time, to our knowledge.
Footnotes
Authors' Contributions
S.R.E. conceived of the study, conducted the statistical analyses, and drafted the initial manuscript, and reviewed, revised and approved the manuscript. J.E. and M.P. reviewed the statistical analyses and reviewed, revised, and approved the manuscript. E.N., H.D., and D.O.O. contributed to drafting the initial manuscript, and reviewed, revised, and approved the manuscript.
Funding Information
There was no funding for this research.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.