
Abstract

To the Editor:
We read with interest the results of the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC) survey addressing prognosis and withdrawal of life sustaining treatment (WLST) after traumatic brain injury (TBI). 1 We were encouraged that respondents recognized the prevalence of therapeutic nihilism, refrained from using prognostic calculators to predict individual patient outcome, and valued establishing a person-centered definition of “favorable” outcome. These findings suggest growing recognition of the potential for meaningful recovery after severe TBI. 2 However, we were concerned that >60% of respondents reported WLST is justifiable for persons who would ultimately recover to the lower severe disability (LSD) category on the Glasgow Outcome Scale-Extended (GOSE = 3). 3 An additional 15% indicated WLST is justifiable in persons who recover to the upper severe disability (USD) category.
The lower limit of the LSD category is a minimally conscious state and the upper limit is a level of function that permits safe independence in the home environment for up to 8 h. 3 The distinguishing feature separating the upper limit of LSD from the lower limit of USD is one additional hour of in-home independence. Empirically, the LSD category spans the full range of Functional Independence Measure 4 total scores (Fig. 1). Thus, although LSD is often considered an “unfavorable” outcome, along with death and vegetative state, partial in-home independence can be achieved within this category.
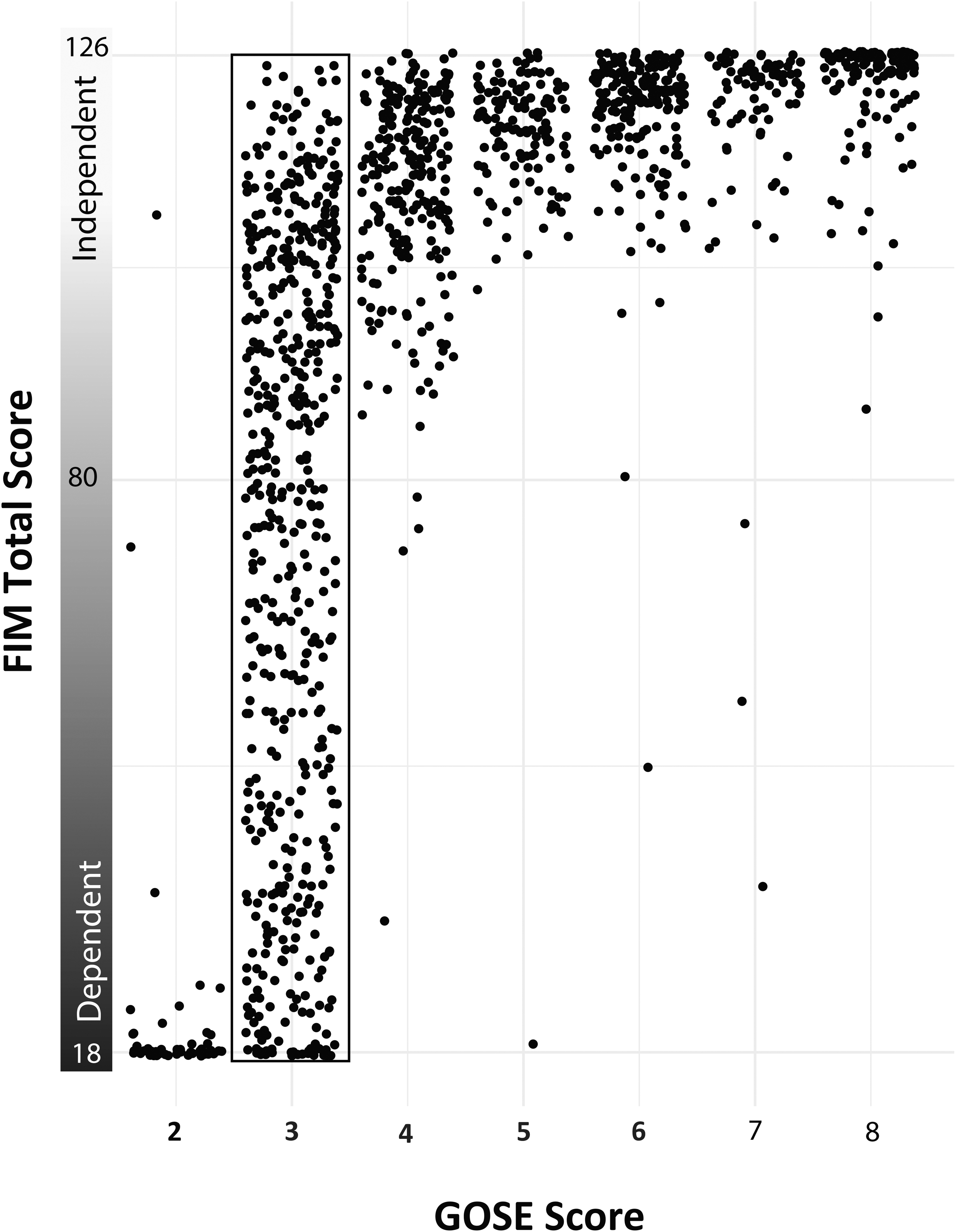
Dots represent outcomes at 1 year for participants with moderate to severe traumatic brain injury (TBI) who were enrolled in the TBI Model System program and were not following commands on admission to inpatient rehabilitation. The x-axis is the Glasgow Outcome Scale-Extended (GOSE) score at 1 year post-injury and the y-axis is the Functional Independence Measure (FIM) score for each participant. The FIM ranges from 18 to 126 with scores <80 representing some level of dependence. Participants scoring in the lower severe disability (LDS) category (GOSE = 3, black rectangle) concurrently obtained FIM scores as high as 125, indicating recovery of independence. Adapted from Snider and colleagues. 4
Acute care neurotrauma physicians may not have the opportunity to follow patients long-term and to observe the process by which one's values could change over time. The well-documented “disability paradox,” which reflects the bias held by able-bodied persons that those with disability have worse quality of life, was demonstrated in Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI), where more than one-third of persons with TBI-related severe disability reported a quality of life within the normative range. 5 Assuming individuals with disability lead a less fulfilling or significant life emanates from ableism and though likely unintentional, may result in premature WLST in patients who may have achieved a personally meaningful recovery.
Nearly all TBI studies dichotomize outcome into “favorable” and “unfavorable” categories, a distinction easily influenced by individual clinician and investigator biases, cultural norms, and societal value systems. Across recent high-impact TBI studies, the cut-point for “unfavorable” outcome ranged from GOSE ≤3 to GOSE ≤7. 6 This finding and the SIBICC survey results highlight the lack of a consensus around the definition of “favorable” outcome and points to the need for patient and caregiver perspectives to inform this fundamental aspect of recovery.
In summary, premature WLST may result from poor understanding of the broad range of function represented by the GOSE LSD category, lack of opportunities to follow patient's recovery long-term, and biases that influence cut-points for “favorable” outcome. These factors contribute to variability in physician judgement as to whether to pursue aggressive care. Indeed, variability in WLST decision-making was reported as being “troubling” for 95% of SIBICC survey respondents. More precise outcome measures that expand the lower end of the GOSE and incorporate patient and caregiver perspectives on outcome are needed.
Footnotes
Authors' Contributions
All authors contributed to writing, editing, and reviewing this Letter.
Funding Information
National Institutes of Health National Institute of Neurological Disorders and Stroke (U01 NS1365885, U01-NS086090), National Institute on Disability, Independent Living and Rehabilitation Research (NIDILRR), Administration for Community Living (90DPTB0011-01-00, 90DP0039).