
Abstract
Brief exposure to repeated episodes of low inspired oxygen, or acute intermittent hypoxia (AIH), is a promising therapeutic modality to improve motor function after chronic, incomplete spinal cord injury (SCI). Although therapeutic AIH is under extensive investigation in persons with SCI, limited data are available concerning cardiorespiratory responses during and after AIH exposure despite implications for AIH safety and tolerability. Thus, we recorded immediate (during treatment) and enduring (up to 30 min post-treatment) cardiorespiratory responses to AIH in 19 participants with chronic SCI (>1 year post-injury; injury levels C1 to T6; American Spinal Injury Association Impairment Scale A to D; mean age = 33.8 ± 14.1 years; 18 males). Participants completed a single AIH (15, 60-sec episodes, inspired O2 ≈ 10%; 90-sec intervals breathing room air) and Sham (inspired O2 ≈ 21%) treatment, in random order. During hypoxic episodes: (1) arterial oxyhemoglobin saturation decreased to 82.1 ± 2.9% (p < 0.001); (2) minute ventilation increased 3.83 ± 2.29 L/min (p = 0.008); and (3) heart rate increased 4.77 ± 6.82 bpm (p = 0.010). Considerable variability in cardiorespiratory responses was found among subjects; some individuals exhibited large hypoxic ventilatory responses (≥0.20 L/min/%, n = 11), whereas others responded minimally (<0.20 L/min/%, n = 8). Apneas occurred frequently during AIH and/or Sham protocols in multiple participants. All participants completed AIH treatment without difficulty. No significant changes in ventilation, heart rate, or arterial blood pressure were found 30 min post-AIH p > 0.05). In conclusion, therapeutic AIH is well tolerated, elicits variable chemoreflex activation, and does not cause persistent changes in cardiorespiratory control/function 30 min post-treatment in persons with chronic SCI.
Introduction
The respiratory and cardiovascular control systems are integrated to ensure the metabolic needs of tissues are met under varying conditions and demands. 1 After spinal cord injury (SCI), cardiorespiratory control is impaired, threatening the regulation of arterial O2 and CO2 partial pressures and the transport of gases to and from the tissues. Respiratory insufficiency and autonomic dysfunction are major concerns after SCI that can impact health-related quality of life and survival. 2
After decades of extensive research in rodents, interest has grown in the potential therapeutic application of repeated short-duration exposures to low inspired O2, or acute intermittent hypoxia (AIH). 3 In 2012, Trumbower and associates 4 reported an 82% increase in plantar flexion torque and 43% increase in gastrocnemius electromyographic activity 30 min post-AIH in 13 individuals with chronic, incomplete SCI. Positive outcomes have since been observed in many somatic motor functions, including: maximal inspiratory mouth pressure 5 ; resting ventilation 6,7 ; walking speed and endurance 8,9 ; hand-grip strength 10 ; and dynamic balance. 11 Early investigations have focused primarily on changes in motor output with less emphasis on the effects of AIH on cardiorespiratory control/function. 12
The mild-to-moderate AIH dose stimulates carotid body chemoreceptors and activates pontomedullary cardiorespiratory control centers that reflexively increase ventilation and heart rate (HR) in able-bodied individuals and those with SCI. 4 –6,13 –15 Although some differences in experimental protocols exist between studies (e.g. duration of hypoxic episodes, presence of concurrent hypercapnia), blood pressure appears well regulated without measurable change from baseline. 5,8,13,14 Few studies, however, have examined both the immediate (within-treatment exposure) and enduring (post-treatment exposure) cardiorespiratory responses to AIH and most lack sufficient detail (e.g. measurement of end-tidal gases, beat-by-beat blood pressure) to make conclusions regarding AIH safety and tolerability in persons with SCI.
Given the therapeutic potential of AIH and known deleterious effects of SCI on respiratory and autonomic function, 16,17 assessment of immediate and enduring cardiorespiratory responses to AIH is warranted. To that end, we sought to characterize cardiorespiratory responses to a single AIH treatment in persons with chronic SCI. We tested the hypotheses that AIH: (a) increases HR and ventilation without significantly altering arterial blood pressure during treatment exposure; and (b) does not elicit persistent short-term effects on any measure of cardiorespiratory control/function.
Methods
Participants
Individuals with chronic (>1-year post-injury) SCI were recruited through an Institutional Review Board approved research recruitment registry, the clinicaltrials.gov website (NCT03833674), flyers, and local healthcare providers and researchers. The University of Florida Institutional Review Board approved the study, and all participants provided informed consent to participate. Data reported here constitute part of a larger phase 2 clinical trial.
Injuries were classified by a licensed physical therapist with expertise in SCI rehabilitation according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). Enrollment criteria included adults with >20% impairment in maximal inspiratory or expiratory pressure, and either: (a) incomplete SCI (C1 to T12) based on residual sensory and motor function below the level of injury or injury classification of American Spinal Injury Association (ASIA) Impairment Scale (AIS) B, C, or D; or (b) chronic complete SCI (C4 to T12; AIS A). Participants required clearance from a physician to ensure medical stability.
Exclusion criteria consisted of: diagnosis of an additional neurological condition such as multiple sclerosis, Parkinson disease, stroke or brain injury; presence of unstable or uncontrolled medical conditions such as cardiovascular or pulmonary disease, hypertension, heterotopic ossification; infections; severe neuropathic pain; known pregnancy; severe recurrent autonomic dysreflexia; and/or history of seizure disorder. To ensure eligibility, all participants were screened before initiating the study. Screening included an in-person participant interview, physical examination, and review of medical records.
Design
After enrollment, participants attended the laboratory on two separate occasions separated by a minimum of three weeks. The two testing sessions were conducted at the same time of day (in most cases) and the order of visits was randomized. Testing on both visits involved the same breathing apparatus and experimental protocol except for the inspired gas fraction during AIH (FIO2 ≈ 0.10) and Sham (FIO2 ≈ 0.21). Fifteen cycles of 60-sec hypoxia or normoxia exposures were interspersed with 90-sec intervals breathing ambient air. 5 Ventilation, HR, arterial blood pressure, and oxyhemoglobin saturation were measured before (baseline), during, and 20–30 min after AIH and Sham. Participants and assessors administering inspired gases were blinded to the intervention. All experiments were performed at Brooks Rehabilitation in Jacksonville, FL.
Spirometry
On the first visit, participants were seated comfortably and instrumented with a nose clip and a mouthpiece attached to a filter and calibrated pneumotachograph (MLT1000L; ADInstruments, Colorado Springs, CO). After a few normal resting breaths, participants were instructed to inspire fully, and then rapidly and forcefully expire until no more air could be exhaled. A minimum of three forced vital capacity maneuvers were performed, and the test was terminated when the three largest values varied by <150 mL according to testing guidelines. 18 Forced vital capacity is reported as the largest of three consistent trials. Participants were encouraged throughout all tests to ensure maximal effort.
Breathing circuit and apparatus
An illustration of the breathing circuit during AIH and Sham is shown in Figure 1. Participants were reclined in a power wheelchair or placed in a long sitting position on a mat with the trunk reclined 45 degrees. Participants were instrumented with a face mask (7450 V2; Hans Rudolph Inc., Shawnee, KS, USA) connected to a two-way non-rebreathing valve (2700; Hans Rudolph Inc.). A heated, calibrated pneumotachograph (3818; Hans Rudolph Inc.) was connected to the expired limb of the circuit. The inspired limb of the circuit was attached to a three-way stopcock (2100; Hans Rudolph Inc.) and hypoxia generator (HYP-123; Hypoxico, New York, NY) with a 5 L reservoir bag. Another two-way non-rebreathe valve was connected between the hypoxia generator and face mask for positive pressure from the generator to escape the circuit and prevent bias flow. Filters were placed on the inspired and expired limbs of the circuit.

Breathing circuit. See text for description. Pm, mouth pressure; PO2, partial pressure of O2; PCO2, partial pressure of CO2, NRBV, non-rebreathe valve; PNT, pneumotachograph.
Mouth pressure was continuously recorded via a side port in the face mask connected to a calibrated pressure transducer (113253; Hans Rudolph Inc.). Breath-by-breath inspired/expired O2 and CO2 concentrations were recorded at the mouth via a side port in the face mask connected to a calibrated O2/CO2 gas analyzer (GEMINI; CWE Inc., Ardmore, PA).
Acute intermittent hypoxia and Sham
Approximately 10 min of resting breathing data were collected before AIH and Sham (i.e. baseline). Once ventilatory and cardiovascular variables were stable, AIH or Sham commenced. The AIH and Sham protocols were identical except for the FIO2 level during episodes. Fifteen, 1-min episodes of hypoxia (AIH; FIO2 ≈ 0.10) or normoxia (Sham, FIO2 ≈ 0.21) interspersed with 90-sec intervals breathing ambient air were delivered. Cardiorespiratory responses were recorded at baseline, during AIH/Sham episodes, and 20–30 min post-AIH/Sham (i.e. recovery). Immediately following AIH and Sham, participants were relieved of the face mask for comfort purposes. During that time, participants were permitted to use the restroom and drink water only.
Cardiovascular variables
The HR, blood pressure, and arterial oxyhemoglobin saturation (SpO2) were recorded continuously at baseline, during AIH/Sham and during recovery. Heart rate was obtained using 3-lead ECG (ML-132; ADInstruments). Beat-by-beat blood pressure was recorded using finger photoplethysmography (Finapres; Finapres Medical Systems BV, Arnhem, Netherlands). Finger arterial pressure was calibrated to brachial pressure using an automated sphygmomanometer. The SpO2 was measured using a finger pulse oximeter (ML320/F; ADInstruments).
Data analysis
Expired tidal volume (VT) was calculated by integrating the expired flow (
Cardiorespiratory variables were averaged over the final 2–3 min of baseline conditions. During AIH and Sham exposures, cardiorespiratory variables were averaged over the final 20–30 sec of each hypoxic/normoxic episode and the normoxic intervals. Cardiorespiratory variables were averaged over the final 2–3 min of the post-AIH/Sham recovery period. The hypoxic ventilatory response during AIH was calculated as Δ

Example of cardiorespiratory responses to acute intermittent hypoxia (AIH). Example breath-by-breath and beat-by-beat traces from one participant (SCI_15). Note the increases in heart rate (HR) and minute ventilation (
Statistics
Changes in cardiorespiratory variables were tested at baseline and during AIH/Sham using a linear mixed model. Fixed effects were condition, time, and the interaction between condition and time. Participant was a random effect. Condition consisted of two levels (AIH and Sham), and time consisted of 30 levels (baseline, episodes 1 to 15, and intervals 1 to 14). Mean changes from baseline in cardiorespiratory variables during AIH versus Sham exposure and during recovery after AIH versus Sham were compared by paired t tests.
Associations between the magnitude of change in ventilatory parameters (VT, fb, and
All data were inspected for normal distribution of residuals via Q-Q plots and histograms. Bonferroni corrections were applied when necessary to account for multiple comparisons. Because of equipment failure and/or difficulties instrumenting participants, the following data were omitted from analyses: five individuals for end-tidal gases during AIH; two individuals for end-tidal gases during Sham; five individuals for beat-by-beat blood pressure during AIH; and 10 individuals for beat-by-beat blood pressure during Sham. Statistical tests were performed using jamovi (V2.2.5; the jamovi project). Data are reported as means ± one standard deviation. Statistical significance was set at p ≤ 0.05.
Results
Participant characteristics
Twenty individuals met the inclusion criteria and were enrolled. One participant withdrew because of a health condition unrelated to the study. Thus, 19 participants (18 males; age = 33.8 ± 14.1 years) were studied with varied injury characteristics: neurological level of injury C1 to T6; injury severity AIS A (n = 8), B (n = 4), C (n = 4), and D (n = 3); and average time since injury of 5.4 ± 7.5 years (range = 1–28 years). Forced vital capacity was 3.8 ± 1.1 L (range = 1.70–5.75 L, 36–109%-predicted). Full participant information and injury details are provided in Table 1.
Participant Informatio
NLI, neurological level of injury; AIS, American Spinal Injury Association (ASIA) Impairment Scale; FVC, forced vital capacity; SCI, spinal cord injury; SD, standard deviation.
Respiratory responses to AIH and Sham
Immediate (within-treatment exposure) respiratory responses to AIH and Sham are shown in Figure 3 and Table 2A. A main effect of time was found for VT, fb,

Respiratory responses to acute intermittent hypoxia (AIH) and Sham. Figure shows respiratory responses to AIH and Sham in absolute values. B, baseline; fb, breathing frequency; PETCO2, end-tidal partial pressure of CO2; PETO2, end-tidal partial pressure of O2;
Cardiorespiratory Responses at Baseline and During Exposures to Acute Intermittent Hypoxia and Sham
Mean changes in VT, fb, and
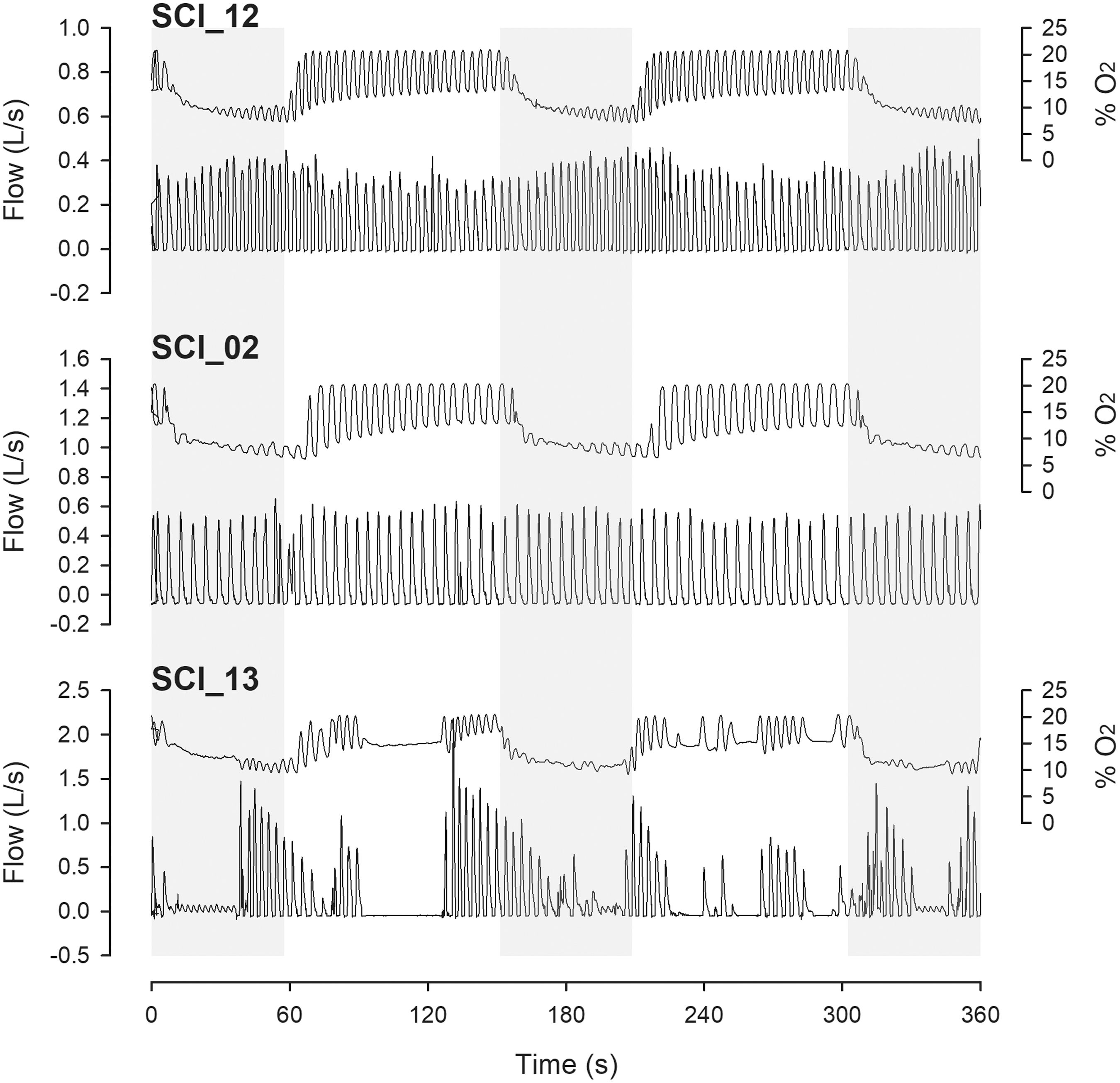
Variability in respiratory responses to acute intermittent hypoxia (AIH). Figure demonstrates vast differences in respiratory responses to AIH between participants. SCI_12 is an example of an individual with normal chemoreflex modulation of breathing. SCI_02 is an example of an individual without evidence of chemoreflex modulation of breathing. SCI_13 is an example of an individual with multiple episodes of apnea followed by hyperventilation.

Comparison of hypoxic ventilatory response between healthy controls and people with chronic spinal cord injury (SCI). Panel A shows the change in arterial O2 saturation (SpO2) and minute ventilation (
Enduring (post-treatment exposure) respiratory responses to AIH and Sham are provided in Table 2B. No differences were found in ΔVT (p = 0.684, d = 0.10 vs. Sham), Δfb p = 0.111, d = 0.40 vs. Sham), Δ
Cardiorespiratory Responses at Baseline and 30 Minutes after Acute Intermittent Hypoxia and Sham (Recovery)
AIH, acute intermittent hypoxia; VT, tidal volume; fb, breathing frequency;
Statistics: Paired t test.
Cardiovascular responses to AIH and Sham
Immediate (within-treatment exposure) cardiovascular responses to AIH and Sham are shown in Figure 6 and Table 2A. A main effect of time was found for SpO2, SBP, and MAP. A main effect of condition was found for SpO2, HR, and DBP. An interaction effect was found for SpO2 (F = 90.3, p < 0.001). Full statistical comparisons and results are presented in Supplementary Table 1.

Cardiovascular responses to acute intermittent hypoxia (AIH) and Sham. Figure shows cardiovascular responses to AIH and Sham in absolute values. B, baseline; DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial blood pressure; SBP, systolic blood pressure; SpO2, arterial O2 saturation. Statistics: Linear mixed model (condition
Mean changes in SpO2, HR, SBP, DBP, and MAP during hypoxic episodes from baseline were -13.06 ± 2.58% (p < 0.001, d = 5.92 vs. Sham), +4.77 ± 6.82 bpm (7 ± 10%; p = 0.010, d = 0.76 vs. Sham), +4.45 ± 6.72 mm Hg (3.8 ± 6%; p = 0.930, d = 0.03 vs. Sham), +4.19 ± 6.28 mm Hg (5 ± 9%; p = 0.803, d = 0.09 vs. Sham), and +4.28 ± 6.26 mm Hg (4 ± 8%; p = 0.891, d = 0.05 vs. Sham), respectively. On average, SpO2 decreased to 82.1 ± 2.9% and HR increased to 73.3 ± 10.5 bpm during hypoxic episodes from baseline.
Enduring (post-treatment exposure) cardiovascular responses to AIH and Sham are provided in Table 2B. No differences were found in ΔSpO2 (p = 0.622, d = 0.12 vs. Sham), ΔHR (p = 0.847, d = 0.05 vs. Sham), ΔSBP (p = 0.591, d = 0.20 vs. Sham), ΔDBP (p = 0.683, d = 0.15 vs. Sham) or ΔMAP (p = 0.638, d = 0.17 vs. Sham) expressed as %-change from baseline.
Discussion
Main findings
The purpose of the present study was to characterize cardiorespiratory responses to AIH in persons with chronic SCI. Four major findings were: (1) AIH activates chemoreflexes that increase
We interpret these findings to mean that AIH is safe and tolerable in persons with chronic SCI. Because of large variability in AIH responses, capture of beat-by-beat and breath-by-breath data may provide a useful index to tailor AIH treatment to individual responses, thus mitigating possible occurrences of confounding factors that disrupt the neurotherapeutic potential of AIH, such as recurrent apneas. 3,20 –24
Immediate AIH effects on respiratory control
On average, hypoxia increased
During hypoxia, PETO2 and PETCO2 (respectively) decreased to 55 and 35 mm Hg. To our knowledge, this is the first study to record PETO2 and PETCO2 during poikilocapnic AIH in persons with SCI. Although previous comparisons are not available, values found here are within ranges reported for healthy young adults. 13,15
Unexpectedly, increases in
Large variability in AIH responses was observed (Fig. 4). Such variable responses are important for three reasons. First, limited chemoreflex activation during AIH may diminish potential therapeutic benefits because weaker chemoafferent stimulation predicts lesser activation of the serotonergic raphe neurons that drive respiratory motor plasticity. 3 When released in the spinal cord, serotonin binds to 5-HT2 receptors on phrenic motor neurons, initiating intracellular signaling cascades leading to new protein synthesis that increases phrenic motor output (i.e., phrenic motor plasticity). 22 –24
Second, irregular breathing or apnea may alter the magnitude of fall in arterial and spinal tissue PO2 during hypoxic episodes. With longer apneas, arterial and spinal tissue PO2 could fall to levels sufficient to trigger glial adenosine triphosphate release and spinal adenosine accumulation, undermining AIH-induced phrenic motor plasticity. 26 –28
Third, apnea combined with hypoxia may induce asphyxia (hypercapnia plus hypoxia). While the effects of asphyxia on respiratory motor plasticity in persons with chronic SCI are unknown, acute intermittent hypercapnic-hypoxia is a more potent stimulus to ventilatory long-term facilitation 12,29 and enhanced corticodiaphragmatic neurotransmission versus AIH alone in healthy able-bodied individuals 14,30 ; however, asphyxia is also a hallmark feature of sleep apnea.
Sleep disordered breathing has been implicated in adverse responses to SCI rehabilitation, 31 and chronic intermittent hypoxia increases ventilatory loop gain, leading to increased frequency of apneic events during sleep in persons with obstructive sleep apnea. 32 Thus, additional work is needed to determine whether our mild-to-moderate AIH protocol elicits changes in apneic events during subsequent sleep. Alternatively, pairing AIH with hypercapnia may prevent apnea during treatment by increasing ventilatory drive and conscious awareness of breathing, while also enhancing respiratory motor plasticity.
Immediate AIH effects on cardiovascular control
On average, SpO2 decreased to 82% during hypoxic episodes, similar to that of previous studies of mild-to-moderate AIH in persons with SCI 4,5 (Fig. 6). During hypoxic episodes, HR increased by 5 bpm on average, reflecting modest chemoreflex activation. Our results are in accord with previous work reporting increases in HR during hypoxic episodes in persons with SCI. 5,8 While HR increased during hypoxic episodes, it is unknown whether stroke volume, cardiac output, or peripheral vascular resistance was altered.
No changes in SBP, DBP, or MAP were observed during hypoxic episodes, although responses were highly variable. Persons with SCI often exhibit diminished sympathetic control of BP, 33,34 leading to hypotension at rest and increased risk of syncope during exercise 35,36 or changes in posture. 37 A recent study found impaired BP responses during the cold-pressor test in individuals with cervical SCI versus healthy able-bodied controls, supporting the notion that SCI alters the ability to regulate BP in response to environmental stress. 38
Nevertheless, similar to results reported here, BP does not appear to change during acute poikilocapnic hypoxemia in healthy humans, 39 perhaps indicating that our therapeutic AIH dose does not present a major challenge to BP regulation. In support of this postulate, more severe intermittent hypoxia protocols do report increases in arterial BP. 40,41 In persons with obstructive sleep apnea and hypertension, daily intermittent hypoxia increases SBP during treatment, but lowers resting SBP between treatments. 42,43 A lack of data investigating mechanisms of altered cardiovascular control during and after AIH limits interpretation of our data.
Persistent AIH effects on cardiorespiratory control
Table 2 provides an overview of group mean averages for various indices of cardiorespiratory control at baseline and 30 min post-AIH. No persistent short-term changes in respiratory or cardiovascular responses were found, suggesting that AIH per se has limited sustained impact on cardiorespiratory control/function post-SCI.
Evidence has emerged demonstrating that poikilocapnic or isocapnic AIH does not elicit ventilatory long-term facilitation in healthy humans. 44 –46 Human ventilatory long-term facilitation has been observed most often when AIH is paired with hypercapnia, either sustained 47,48 or intermittent. 49 Mechanisms differentiating poikilocapnic versus hypercapnic AIH have not been comprehensively studied. Acute intermittent hypercapnic-hypoxia, but not AIH alone, however, enhances corticodiaphragmatic conduction by a central neural mechanism of respiratory motor plasticity. 13
Thirty minutes after AIH, HR had returned to baseline and BP remained unaltered. These findings are in line with previous studies in humans with chronic SCI, which report minimal (or no) persistent AIH effects on HR or BP regulation. 6,8,10 Although prolonged effects were not observed, intermittent hypercapnic-hypoxia (or asphyxia) experienced during sleep apnea elicits long-lasting pathology. 50
Numerous studies report sustained increases in muscle sympathetic nerve activity after various intermittent hypoxia protocols 51,52 ; however, increased muscle sympathetic nerve activity is not always associated with changes in BP. 53 Indeed, reductions in BP have been observed after AIH in healthy individuals 54 and persons with chronic SCI given the non-steroidal anti-inflammatory drug, ibuprofen. 55
A recent study in healthy humans found that intermittent asphyxia elicited long-lasting increases in muscle sympathetic nerve activity, MAP, and the translation of increased sympathetic outflow to changes in DBP; yet, forearm vascular conductance was unchanged, suggesting regional differences in sympathetic neurovascular transduction after intermittent asphyxia. 56 In rats with cervical spinal hemisection, moderate AIH elicits renal but not splanchnic sympathetic long-term facilitation. 57
Thus, it remains to be determined whether AIH can be harnessed to improve autonomic function and orthostatic tolerance post-SCI. Future studies are needed to test whether AIH alters sympathetic outflow, cardiac contractility, endothelial function, sympathovagal balance, and hemodynamics, in addition to establishing whether concomitant hypercapnia enhances these responses, as is known with breathing.
Limitations
We studied a heterogeneous sample of 19 individuals with chronic SCI, with injury levels ranging from C1–T6 and injury severities from AIS A–D. In addition, the age range of subjects was large (19–67 years) and included only one female participant. Although these broad inclusion criteria generated a large dataset, they limit our ability to isolate specific subgroup effects. While our predominantly male cohort aligns with the demographic distribution of individuals living with chronic SCI, 58 we acknowledge that the limited female representation prohibits generalizability of our findings. Future studies are needed to determine whether AIH responses differ on the basis of injury level/severity, age, sex, and/or genetic biomarkers of plasticity. 59
Some data were omitted (described in Methods) because of unreliable beat-by-beat and/or breath-by-breath recordings caused by equipment malfunction or difficulties instrumenting participants because of (in part) injury characteristics and symptoms, such as hyperreflexia/spasticity. Our data are limited to some degree by the narrow time window studied post-AIH despite being consistent with previous literature describing enhanced motor functions in persons with SCI. 4,5,7,55,60
Conclusions
We investigated immediate and enduring cardiorespiratory responses to AIH in persons with chronic SCI. Although AIH elicited robust chemoreflex activation, increasing
Transparency, Rigor and Reproducibility Summary
The current study is a substudy of a larger clinical trial that was pre-registered with clinicaltrials.gov (NCT03833674). As such, the pre-specified analysis plan, statistical power, and sample size calculations were made based on primary outcomes from the parent clinical trial. The current study is a secondary analysis with a planned sample size of 20 participants. Observed effect sizes (Cohen's d) for mean changes in
Footnotes
Acknowledgments
We thank our research participants for their time and dedication.
Authors' Contributions
JFW: conceptualization, methodology, software, validation, investigation, formal analysis, data curation, writing – original draft, writing – review and editing, visualization, supervision; AKV: conceptualization, methodology, software, validation, investigation, formal analysis, writing – review and editing, supervision; KC: investigation, methodology, validation GB: investigation, methodology, validation; LAD: investigation, supervision; HS: investigation, supervision; CNW: investigation, methodology, supervision; GJ: investigation, supervision; JN: investigation, methodology; GSM: conceptualization, methodology, validation, resources, writing – review and editing, project administration, supervision, projecting administration, funding acquisition; EJF: conceptualization, methodology, validation, resources, data curation, writing – review and editing, project administration, supervision, projecting administration, funding acquisition.
Funding Information
University of Florida (UF) McKnight Brain Institute, Craig H. Neilsen Foundation (SCIRTS), United States Department of Defense (SCIRP W81XWH-17), National Institutes of Health (R01 HL147554), Brooks Rehabilitation/UF College of Public Health and Health Professions Research Collaboration.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.