
Abstract
Cardiac injury is a common complication following traumatic brain injury (TBI) that can lead to poor clinical outcomes. Angiotensin II type 2 receptor (AT2R) activation exerts protective roles in the brain and heart, yet its potential impact on TBI or TBI-induced cardiac deficits remains elusive. The goal of this study was to investigate the influence of AT2R activation on recovery after TBI-induced cognitive and cardiac injury using the selective nonpeptide AT2R agonist compound 21 (C21). TBI was induced by cortical impact injury in male adult C57BL/6J mice, and the mice received C21 (0.03 mg/kg, intraperitoneally) starting from 24 h after TBI and continuing once daily. C21 facilitated cognitive function recovery until 1 month after TBI. C21 alleviated blood-brain barrier leakage and brain edema and inhibited the expression of proinflammatory cytokines in the brain after 3 consecutive days of treatment. C21 improved cerebral blood flow after 1 month, although the lesion volume was not affected. C21 also reduced the expression of proinflammatory cytokines in the heart after a 3-day consecutive treatment. Meanwhile, C21 benefited cardiac function, as identified by increased left ventricular ejection fraction 1 month after TBI. In addition, C21 alleviated TBI-induced cardiac hypertrophy and fibrosis; however, blood pressure was not affected. Our results demonstrate that AT2R activation ameliorates TBI-induced neurological and cardiac deficits.
Introduction
Traumatic brain injury (TBI) is a major cause of trauma-related morbidity and mortality worldwide. For years, there have been no established therapies to reverse the effects related to TBI, and there is a substantial need for new treatments that provide improved symptomatic benefits. 1 -3 Primary brain injury triggers parenchymal damage, while the secondary cascade of injury, including systemic inflammation, has a significant impact on patient deterioration. 4 The heart is very susceptible to injury, and cardiac dysfunction has been extensively reported after TBI. 5 –8 Additionally, TBI of any severity causes a higher risk of developing long-term neurological and cardiovascular complications in patients without primary diagnoses. 8, 9
The renin–angiotensin system (RAS) plays a critical role in the cardiovascular system under physiological and pathophysiological conditions. 10 Increasing evidence indicates that the RAS is involved in neurological diseases via two major receptors: angiotensin-II type 1 (AT1R) and type 2 receptor (AT2R). 11 The local RAS identified in the brain has been associated with several neuropathologies, including TBI. Brain angiotensin II activity increases after TBI, and AT1R is at a much higher abundance than AT2R; its functions have been widely recognized. 12 AT1R-mediated modulation by sartans has been shown to have positive effects on blood-brain barrier (BBB) restoration and neuroprotection. 13 Increased AT2R stimulation is often considered to counteract the effects of AT1R, 12 whereas AT1R blockade and AT2R stimulation portray distinct roles, such as endothelial function. 14 Several studies have reported that activation of AT2R in stroke confers neuroprotection with a decrease in infarct volume 15 -17 ; thus, we hypothesized that AT2R may have an impact on both the brain and heart under TBI. The actions mediated by AT2R have rarely been studied in TBI and its associated heart injury; therefore, we planned to examine whether AT2R modulation affects TBI and its related cardiac injury.
In a previous study, we have shown that the immune system is a proposed mechanism of initiation of cardiac injury after TBI. 18 Recently, we also demonstrated that the immune modulator fingolimod promotes the ejection fraction and inhibits cardiac inflammation. 19 However, the immune modulator fingolimod may be associated with potentially negative consequences to the heart, such as atrioventricular block, heart rhythm and heart rate variability. 20
These unfavorable consequences may in turn cause unfavorable outcomes in the brain. 21 Fortunately, the clinical importance summarized by Ranjit et al. showed that compound 21 (C21), a selective nonpeptide AT2R agonist, successfully completed phase I clinical trials without significant side effects. 22 AT2R is involved in the development of pathological processes in the cardiovascular system, and AT2R stimulation prevents processes including inflammation, apoptotic cell death, cardiac fibrosis, and compensatory hypertrophy of cardiac myocytes. 14
Although AT2R stimulation plays a protective role in multiple disease models, such an approach in TBI has yet to be fully characterized. In the present study, we sought to investigate the potential efficacy and mechanism that C21 could regulate in TBI via the controlled cortical impact (CCI) model.
Methods
Animals
Male C57BL/6 mice (10 weeks old, weighing 21-25 g, purchased from the Vital River Laboratory Animal Technology, Beijing, China) were housed in specific pathogen-free (SPF) facilities (20 ± 2°C, standardized light/dark cycle) with ad libitum access to food and water. All procedures were carried out in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals and approved by the Animal Care and Use Committee of Tianjin Medical University General Hospital.
Induction of TBI
The TBI mouse model was induced by using a CCI device (eCCI model 6.3, American Instruments, Richmond, VA, USA) as previously described. 23 Briefly, mice received 5 mg/kg carprofen (Cayman Chemical, Ann Harbor, MI, USA) subcutaneously and were fixed to a stereotactic frame after anesthesia by 4% isoflurane inhalation and maintained by 1.5-2.0% isoflurane. Then, a midline incision was made, followed by drilling a 4-mm-diameter craniotomy between bregma and lambda and 1 mm lateral (right) to the midline to expose the dura mater. Then, mice were subjected to CCI, which was delivered with an electromagnetic piston (4-mm tip in diameter, 5 m/sec velocity, 1.5 mm depth and dwell time of 100 msec).
Administration dose and animal groups
Mice were randomly divided into experimental groups, receiving intraperitoneal injection of C21 (0.03 mg/kg, Cay33758, Cayman Chemical, Ann Harbor, MI, USA) or phosphate-buffered saline (PBS). The administration dose chosen was based on previous publications that suggested it as the most effective dose in stroke and myocardial infarction. 24,25
The mice that underwent sham surgery without TBI or C21 treatment were used as a TBI control (sham group). The initial intraperitoneal injection was performed from 24 h after injury until the end of the experiments.
Behavioral tests
A battery of cognitive-related behavioral tests was performed by an investigator who was blinded to the experimental groups. The Morris water maze (MWM) test, novel object recognition (NOR) test and nest-building experiment were performed following previously described methods 21–29 days after TBI. 26,27
Magnetic resonance imaging analysis
A 9.4-T high-field magnetic resonance imaging (MRI) scanner (BioSpec 94/30 USR, Bruker) was used in the measurement as previously detailed. 28, 29 Briefly, animals were anesthetized by 4% isoflurane inhalation and maintained by 2% isoflurane and then positioned in the magnet, and respiration and heart rate were monitored during scanning. T2-weighted image sequence (echo time, 33 msec; repetition time, 2,500 msec; slice thickness, 0.5 mm; field of view, 20 × 20 mm; image matrix, 256 × 256; spatial resolution 0.078 × 0.078 mm) was performed to assess lesion volume, including the area of edema and necrosis, at 4 days after CCI. Lesion volumes were manually outlined and calculated by multiplying the sum of the volume by the distance between sections (0.5 mm) using a Digital Imaging and Communications in Medicine (DICOM) Viewer. Volumes were calculated as total lesion volume minus necrosis volume. Two investigators blinded to the experimental groups performed the MRI data analysis.
Evans blue permeability assay
Four days after CCI, Evans blue (EB) solution (2% in saline; 4 mL/kg, Sigma) was injected into the tail vein after anesthetization with 2% isoflurane gas. Brains were extracted followed by a 2-h circulation, and then the EB in the brains was extracted by incubation with formamide for 24 h in a 60°C water bath. The supernatant was harvested and put onto a 96-well plate for EB quantification after centrifugal precipitation. The absorbance was measured at a wavelength of 610 nm with a spectrophotometer.
Cerebral blood flow measurement
Regional cerebral blood flow (CBF) was measured 32 days following CCI injury using laser Doppler flowmetry (Perimed AB, Sweden). Briefly, mice were anesthetized as described above, the skull was exposed after a midline scalp incision, and regional CBF in both brain hemispheres was continuously recorded by using a laser speckle imager for 30 sec.
Blood pressure measurement
To test the influence of C21 on blood pressure (BP), systolic BP (SBP), diastolic BP (DBP) and mean arterial pressure (MAP) were measured 30 days after TBI by using a tail-cuff method (CODA noninvasive BP system, KENT scientific). The mice were put into plastic restrainers for 5 min for a 3-consecutive day habituation before the test. Then, body temperature was maintained at 37.0 ± 1.0°C on a thermostatically controlled mat during testing, and BP was recorded and averaged after 15 consecutive readings.
Histological staining and assessment
After all functional tests, the mice were perfused transcardially with ice-cold PBS solution after anesthesia with 5% isoflurane. The mouse brains were removed and fixed in 4% paraformaldehyde for 2 days at 4°C. The mouse forebrain was cut into a 2-mm-thick coronal block for seven equal blocks per mouse by a mouse brain matrix. Brain tissues were dehydrated and transparent in gradient alcohol and xylene. Then, tissues were embedded in paraffin and cut into a series of 8-μm-thick slides of each block and stained with hematoxylin-eosin staining kits (G1120, Solarbio). The lesion volumes were calculated by multiplying the sum of the volume by the distance between sections and analyzed by using ImageJ (U.S. National Institutes of Health) software. Heart coronal sections were cut into a series of 8-μm-thick slides from paraffin-embedded blocks. Picrosirius Red (PSR, a fibrosis marker, 1:1,000; Sigma) staining was performed to assess the interstitial collagen fraction of the heart.
Echocardiography
Cardiac function was assessed in mice 31 days after TBI, as previously described. 18 Transthoracic echocardiography measurements were performed using a Vevo 3100 Imaging System. The cardiac cycle was recorded by M-mode ultrasound from the long-axis parasternal view as well as the short-axis view. The left ventricular ejection fraction (EF) and fractional shortening (FS) were measured and analyzed.
Luminex liquid suspension chip detection
Brain and heart tissues were harvested and homogenized at 4 days after TBI. Then, a Luminex liquid suspension chip detection immunoassay of 33 chemokines and cytokines was employed according to the manufacturer's instructions (Bio-Plex Pro™ Mouse Chemokine Panel 33-Plex #12002231, Bio-Rad Inc.). The values were read using a Luminex 200 system.
Statistical analysis
All animals were randomly assigned to treatment groups. Statistical analyses were performed using GraphPad Prism 9 Software (GraphPad Inc.), and data are shown as the mean± standard deviation. Two-tailed unpaired t tests were used to compare two groups. One-way analysis of variance (ANOVA) followed by the Tukey post hoc test was used to compare data from multiple groups. The p values <0.05 were considered statistically significant.
Results
Delayed C21 treatment alleviates cognitive function recovery
To assess the impact of AT2R modulation on TBI recovery, we measured the effects of C21 on cognitive and cardiac function recovery in CCI mice. CCI mice received PBS or C21 from 24 h after CCI until the experiments were ended (Fig. 1A). To determine whether C21 treatment could ameliorate cognitive decline in TBI mice, a battery of cognitive-related behavioral tests was performed to test spatial learning and memory 21-29 days after TBI, including the MWM, NOR and nest-building tests. C21 significantly improved spatial learning and cognitive deficits, as shown by significantly reducing escape latency to the platform and increasing the percentage of time spent in the target platform quadrant in the MWM test (Fig. 1B-E). The NOR test results revealed that animals in the C21-treated group showed an increased interest in exploring novel objects compared to those in the PBS-treated TBI group as determined by the discrimination index for novel objects (Fig. 1F). Furthermore, experimental nesting data showed that the C21-treated animals achieved better scores than the PBS-treated TBI animals (Fig. 1G-H).
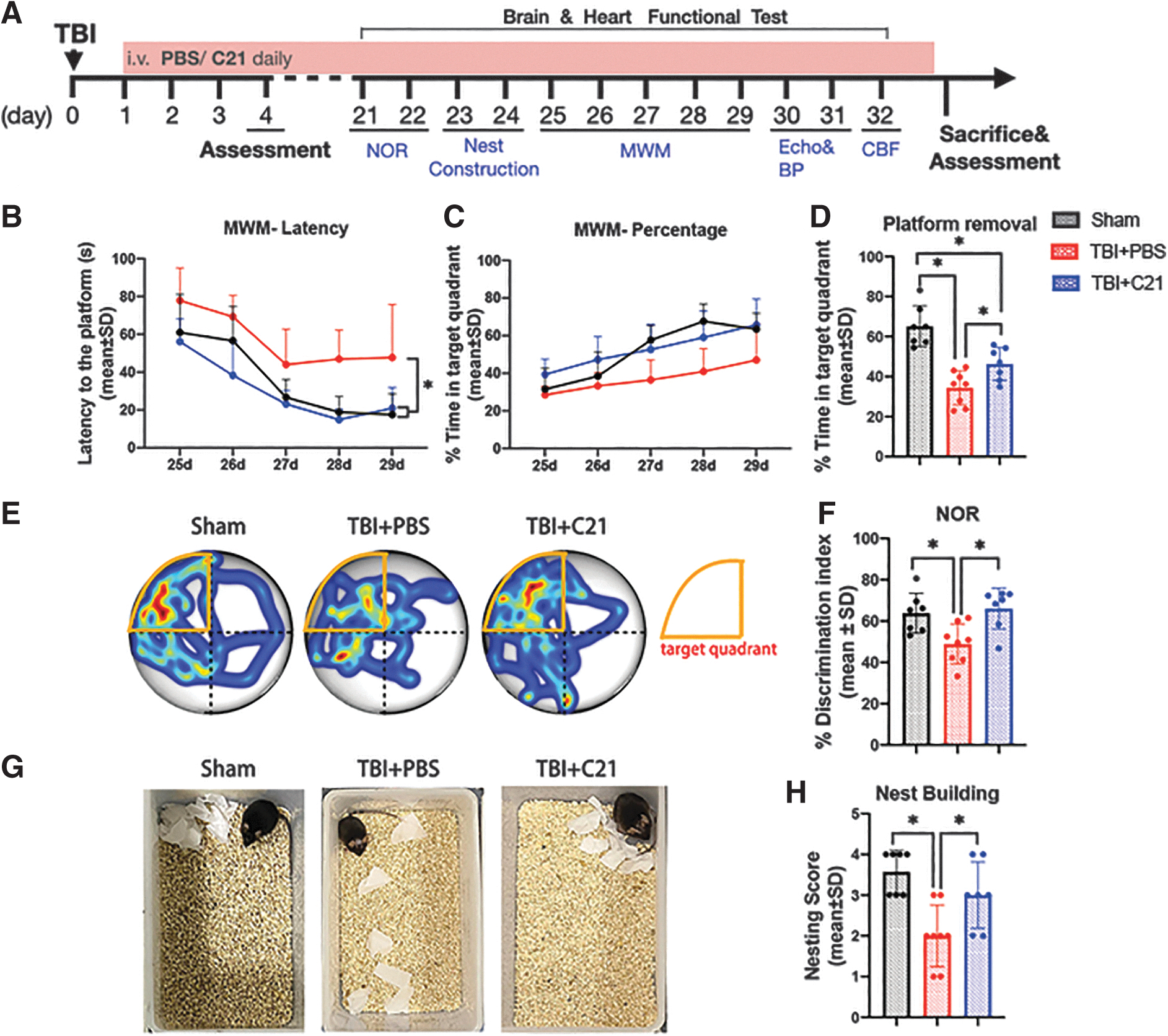
Delayed angiotensin II type 2 receptor (AT2R) activation by compound 21 (C21) improved cognitive function recovery in traumatic brain injury (TBI) mice.
Delayed C21 treatment attenuates cerebral edema, BBB leakage, and CBF
As brain inflammation can induce secondary brain damage by intensifying cerebral edema, to determine the effect of C21 on the BBB, we measured the edema volume and BBB leakage by MRI and EB permeability at 4 days after TBI. C21 treatment significantly decreased the edema volume compared with the PBS treatment group. (Fig. 2A, 2B). Meanwhile, compared with the PBS-treated group, animals in the C21 treatment group exhibited lower concentrations of EB after injection, suggesting that TBI-induced BBB damage was attenuated by C21 administration (Fig. 2C, 2D). With daily treatment for over 30 days after TBI, animals in the C21-treated group showed an increase in CBF compared to those in the PBS-treated group (Fig. 2E, 2F). However, C21 treatment had no impact on the lower lesion volume compared to the PBS-treated group (Fig. 2G, 2H).

Compound 21 (C21) attenuated blood–brain barrier (BBB) leakage and brain edema and improved cerebral blood flow (CBF).
Delayed C21 treatment reduces TBI-induced neuroinflammation
The inflammatory response peaked 72 h after TBI, and we sought to understand the influence of C21 on neuroinflammation. After 3 days of consecutive treatment, a Luminex assay was used to measure various inflammatory cytokines and chemokines in the brain and heart. Multiple proinflammatory cytokines and chemokines in the brain significantly decreased with C21 treatment, including C-C motif chemokine ligand 2 (CCL2), CCL4, CCL7, CCL12, CCL19, C-X-C motif chemokine ligand 1 (CXCL1), CXCL5 and CXCL11 (Fig. 3A-H).
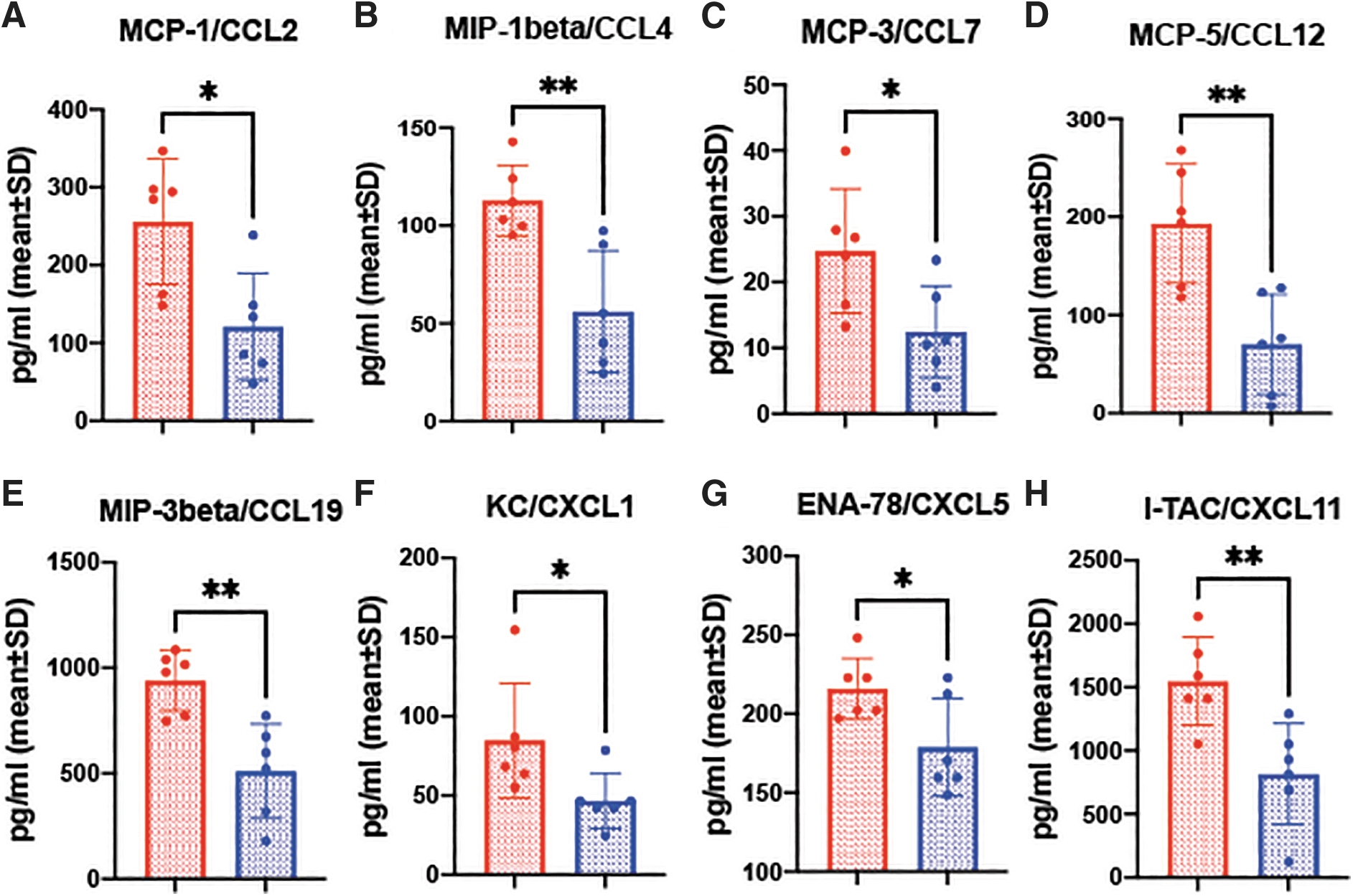
Compound 21 (C21) decreased the traumatic brain injury (TBI)-induced inflammatory response in the brain. Inflammatory cytokines and chemokines were quantified by using a Luminex assay 4 days after TBI;
Delayed C21 treatment reduces TBI-induced cardiac inflammation
Our previous investigation found that TBI-induced cardiac inflammation was more intense in the acute phase at 3 days after TBI. To determine whether C21 treatment has anti-inflammatory effects in this condition, a Luminex assay was also used to measure various inflammatory cytokines and chemokines in the heart after 3 consecutive days of treatment. Multiple proinflammatory cytokines and chemokines in the heart were also significantly decreased, including interleukin-1beta (IL-1beta), CCL5, CCL20, CCL27, CXCL5, CXCL10 and interferon gamma (IFN-gamma), which were significantly decreased in the heart (Fig. 4A-G).
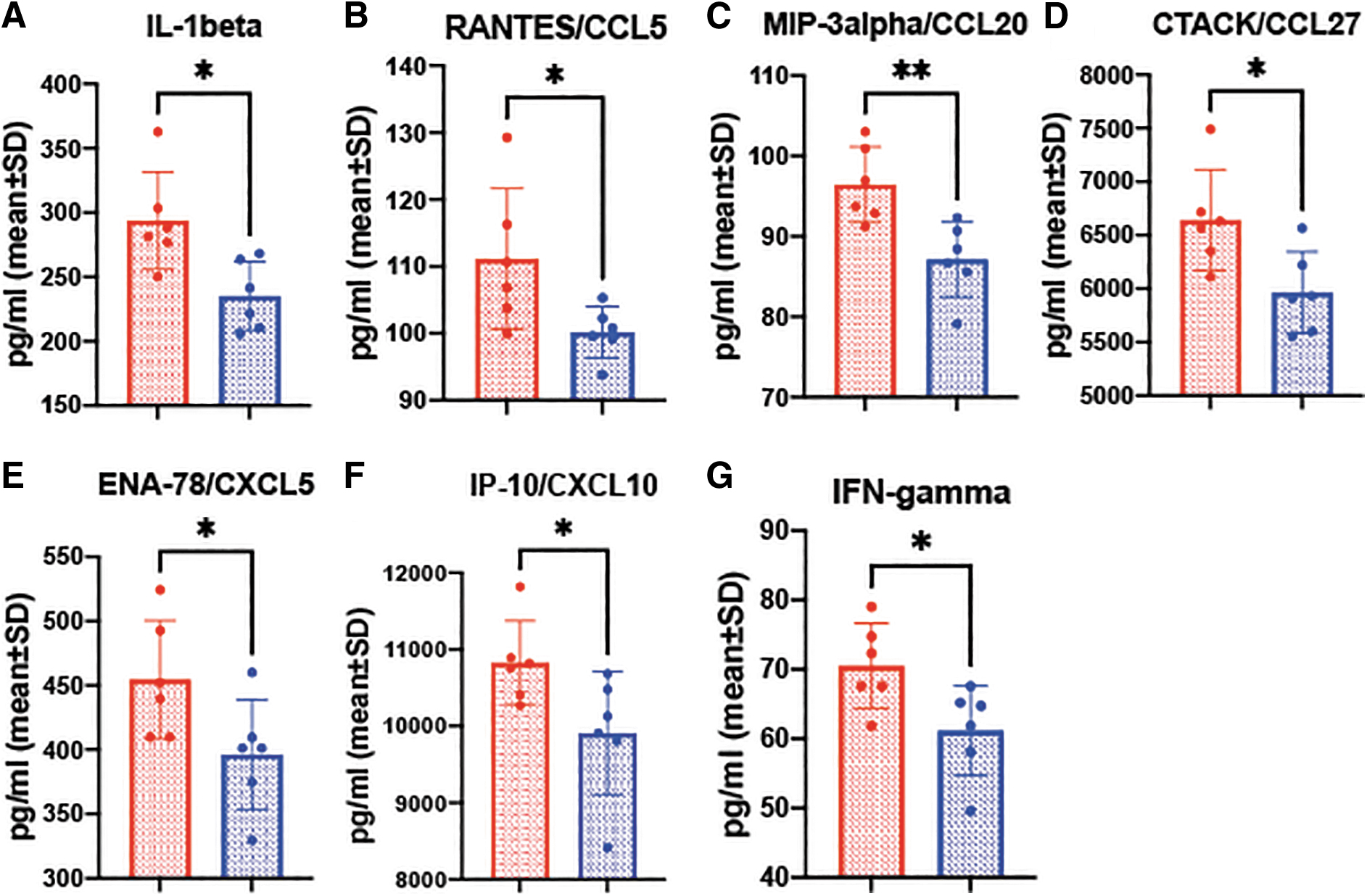
Compound 21 (C21) decreased the traumatic brain injury (TBI)-induced inflammatory response in the heart. Inflammatory cytokines and chemokines were quantified by using a Luminex assay 4 days after TBI.
Cardioprotective effects with delayed administration of C21
To determine whether C21 treatment contributes to TBI-induced cardiac dysfunction, echocardiography was performed 32 days after TBI. (Fig. 5A-C) shows that C21 treatment significantly alleviated cardiac contractile function, as identified by increased left ventricular EF and FS. To test whether C21 treatment influences blood pressure, the tail-cuff method was performed. We found that continued C21 treatment had no impact on systolic, diastolic, or mean arterial pressure. (Fig. 5G-I). Moreover, PSR staining was performed to investigate whether improved cardiac function and cardiac remodeling were associated with cardiac fibrosis reduction and to determine the influence of C21 on the heart. C21 significantly decreased TBI-induced cardiac hypertrophy (Fig. 5D-F). C21 also significantly decreased TBI-induced interstitial fibrosis compared to PBS-treated mice after TBI (Fig. 5J, 5K).
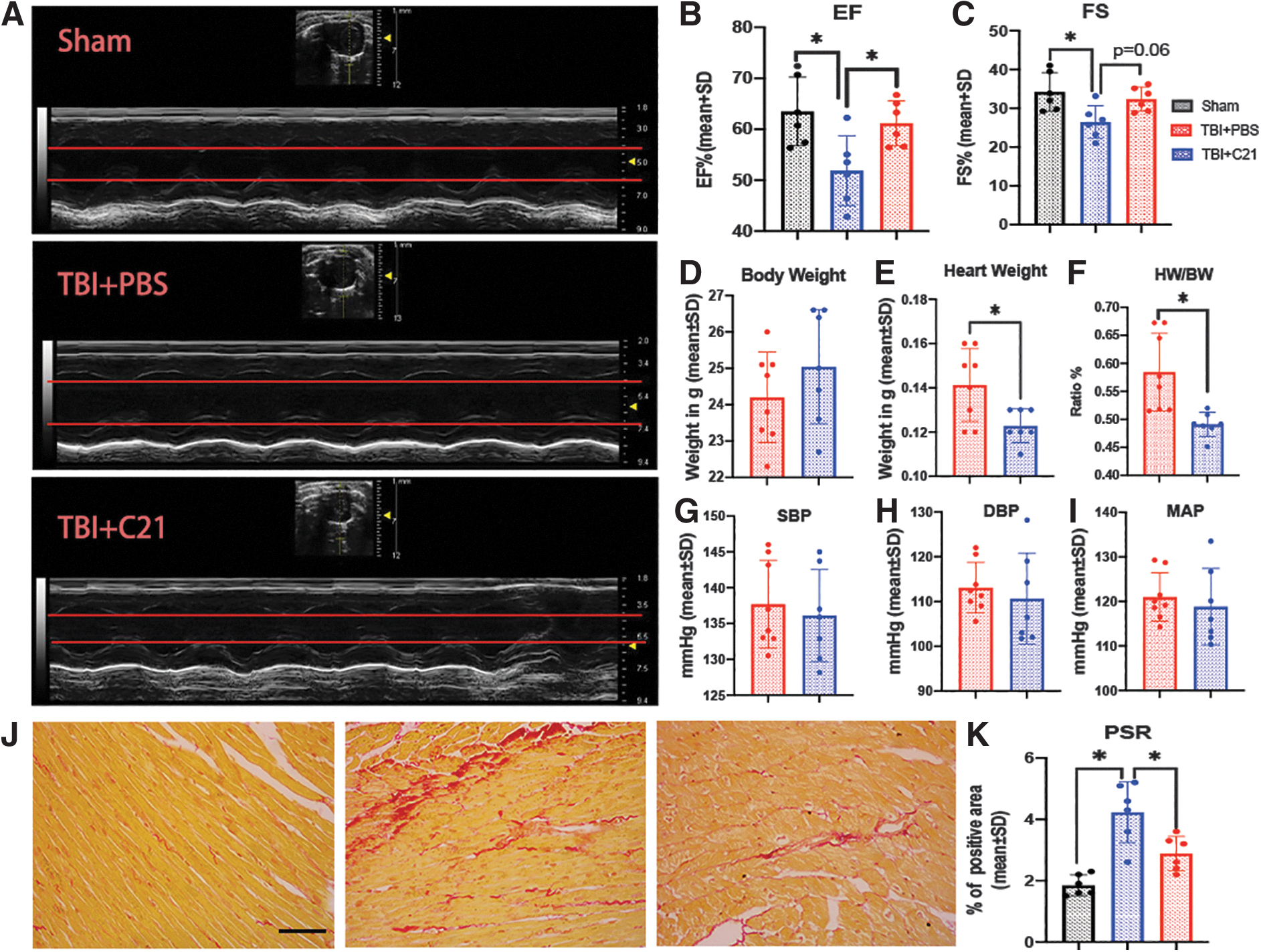
Compound 21 (C21) exerted cardioprotective effects after traumatic brain injury (TBI). Representative images of echocardiography
Alleviation of cognitive dysfunction significantly correlates with improved cardiac function
Pearson's correlation test was performed to investigate the correlations between cognitive function and cardiac function. We found that spatial memory retention, NOR discrimination index, nest-building score and CBF were significantly correlated with left ventricular EF, as shown in Figure 6A-D, which indicates that improved cardiac function has a correlation with cognitive dysfunction.
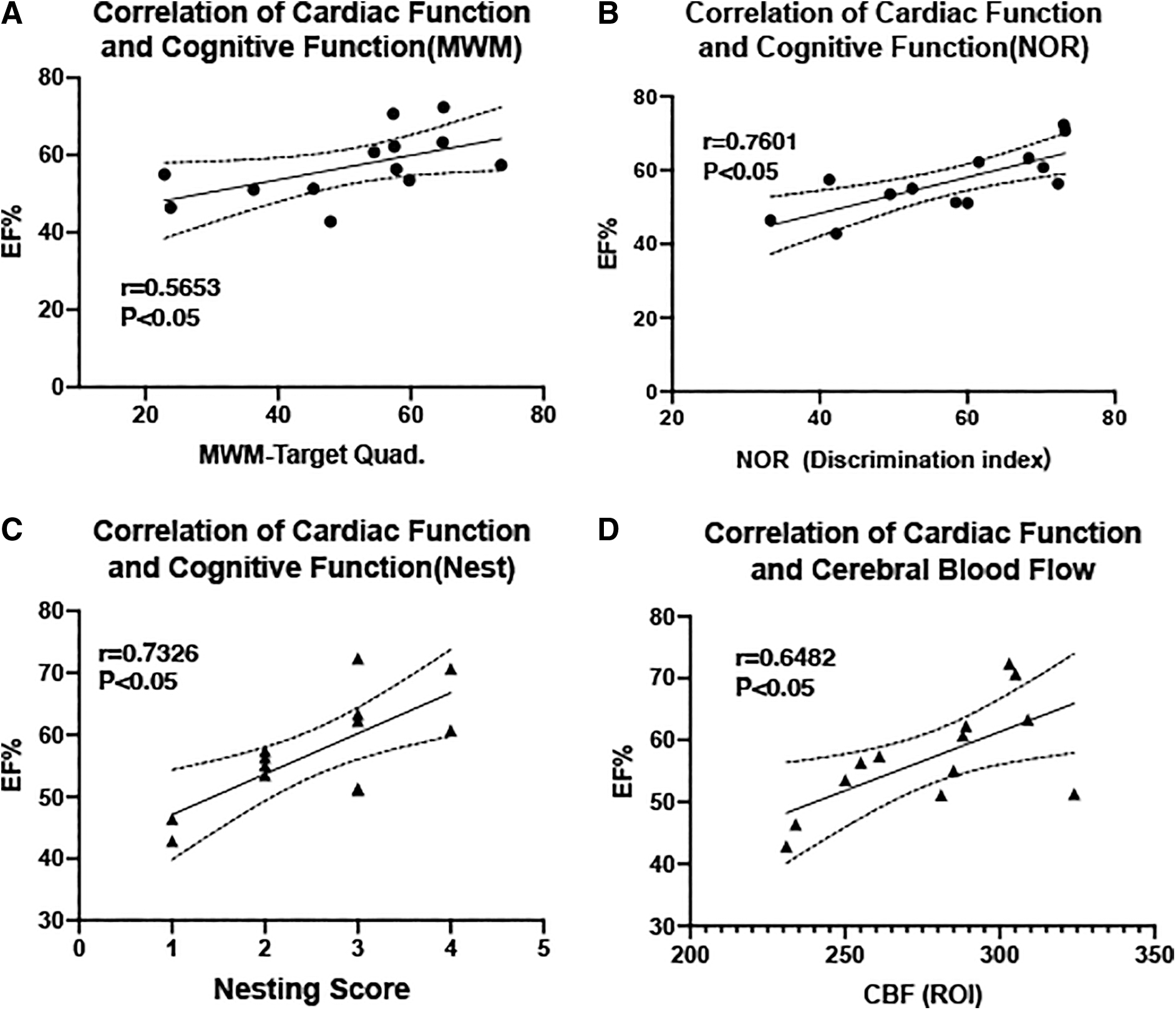
Correlation analysis between cognitive function and cardiac function. Correlation analysis of
Discussion
Our study has demonstrated that delayed administration using a selective nonpeptide AT2R agonist C21 improves neurological and cardiac recovery in mice after TBI. As documented here, C21 treatment led to decreased inflammatory chemokines and cytokines in the early phase of TBI, together with amelioration of cardiac fibrosis and increased left ventricular ejection fraction in the late phase of TBI, which revealed a previously unrecognized role of AT2R activation in both TBI and TBI-induced cardiac deficits.
Pre-clinical studies of potential TBI treatments have failed to translated in clinical trials, though the link between brain and heart after TBI has been recognized, few therapeutic strategies focused on brain-heart interaction. 3,30,31 An increasing number of studies have reported that activating AT2R exhibits a protective effect in both cerebrovascular and cardiovascular diseases, such as ischemic stroke, 14 hypertension, 32 and myocardial infarction. 33 As TBI patients receive treatment that is inadequate or even delayed after onset and pharmacological intervention studies using animal models are often evaluated preinjury or immediately after injury, which are not applicable in clinical scenarios, we elected delayed administration of C21 to increase the possibility of translatability in the study. Then, we chose to start C21 treatment 24 h after TBI, as delayed AT2R activation has shown protective roles in stroke. 17 It is therefore reasonable to postulate that delayed AT2R stimulation may exert benefits in TBI-induced neurological and associated cardiac deficits.
Recently, both Timaru-Kast and colleagues 34 and Ismael and colleagues 35 reported the effects of C21 in the acute phase of TBI and selectively tested a few inflammation-related markers at 1 and 5 days after TBI, respectively. As we reported previously, neuroinflammation is more intense, and extensive proinflammatory cytokines and chemokines are increased in the brain at 3 days following TBI; however, neuroinflammation is subtle at 14 days post injury. 23 After three consecutive C21 treatments, we found that multiple proinflammatory cytokines and chemokines, including CCL2, CCL4, CCL7, CCL12, CCL19, CXCL1, CXCL5 and CXCL11, were significantly decreased; therefore, C21 may serve as a potent anti-inflammatory agent in TBI.
As inflammatory processes can give rise to the disruption of the BBB, BBB breakdown after brain insult aggravates brain edema and causes increased intracranial pressure, which is associated with poor outcomes after TBI. 23 In naive rodents, only a trace mount of C21 was detected following intraperitoneal injection, and the concentration of C21 significantly increased in the cerebral cortex and striatum after BBB disruption. 36 We found that delayed C21 treatment decreased brain edema volume as well as BBB leakage. Importantly, the chemokines and cytokines we found to be increased above are associated with the process of brain edema; therefore, C21 alleviated brain edema, and BBB leakage may come as a result of its anti-inflammatory effects.
Although a recent murine TBI study with C21 treatment within 3 h postinjury exhibited unaffected lesion volume and neurological outcome, 34 the study mainly focused on the acute period of the injury; however, this is consistent with our finding that even using continuous C21 treatment over 1 month, the lesion volume was also unaffected compared with the untreated group. This evidence indicates that C21 treatment group assignment (early onset or delayed) did not affect the outcome of lesion size, but prolonged treatment did alleviate cognitive function in the later phase after TBI. We performed MRI to measure perilesional edema, which is different from the above study that applied histological methods to evaluate total hemispheric brain volumes. As brain insult can cause systemic inflammation and C21 is a potent anti-inflammatory agent after TBI, a previous study demonstrated that peripheral inflammatory stimuli aggravate BBB breakdown and cerebral edema but do not influence infarct size in ischemic brain injury, indicating that inflammatory modulation by C21 may not be the major effector of lesion size. 37
In addition, vascular endothelial growth factor (VEGF) serves as a potent activator of neurogenesis after TBI, 38 AT2R activation inhibits VEGF-induced angiogenesis in the microvascular endothelium, 39 however, inhibition of VEGF signaling benefits brain swelling without lesion size regulation 40 ; therefore, it is reasonable to postulate that the inherent property of C21 has no effect on TBI lesion volume. Moreover, continuous C21 treatment improved cognitive impairment as well as cerebral blood flow. Hypoperfusion is a major factor in the development of cognitive dysfunction; 41 thus, apart from neuroinflammatory suppression, improved cognitive function may be attributed to CBF modulation by C21.
Brain health interacts with the cardiovascular system in complex ways, and several neurological diseases have been reported to cause cardiac deficits that lead to lifelong cardiac problems or increased mortality. 19,41,42 Zhao and colleagues found that TBI-induced cardiac inflammation is more intense in the early phase (3 days post-injury), although it can last as long as 1 month. 18 In this study, we also found that C21 treatment reduced the expression of proinflammatory chemokines and cytokines, including IL-1beta, CCL5, CCL20, CCL27, CXCL5, CXCL10 and IFN-gamma, which indicates that C21 has broad anti-inflammatory properties in TBI with cardioprotective effects. Many of these proinflammatory factors have direct or indirect relationships to cardiac remodeling and fibrosis; for example, CCL5 facilitates collagen accumulation in the heart with chronic inflammatory induction, resulting in prohypertrophic events and interstitial fibrosis. 43 We found that C21 significantly decreased cardiac hypertrophy and fibrosis, which may be attributed to the immunomodulation of C21 in the heart.
Consistent with recent findings, Timaru-Kast and colleagues reported that lower or higher doses of C21 treatment did not affect BP, 34 which was monitored BP in the early phase of TBI. We found that even with continued administration, C21 did not significantly counteract BP in TBI, although lowering BP via renovascular regulation and possibly benefiting long-term BP regulation. However, early pharmacological studies indicate that C21 may have a limited impact, which may not sufficiently lower BP. 44 BP management is critical in TBI, whereas both early hypertension and hypotension are considered to potentially have negative impacts during TBI, 45 and the ineffectual role of C21 in BP reduces the potential side effects caused by BP modulation. The results indicate that C21 did not interfere with BP in either the acute phase or chronic phase of TBI, which may suggest that the protective effects of C21 in TBI are not involved in BP modulation.
In summary, delayed administration of C21 improves neurological and cardiac recovery after TBI. Few actual studies have identified drugs capable of exerting protection against brain injury and brain injury-induced cardiac deficits, and our findings suggest that activation of AT2R may serve as a feasible strategy to benefit the long-term prognosis of TBI patients.
Limitations
Investigation of therapeutic strategies to alleviate cardiac deficits in TBI patients is clinically relevant. 5 The present study is grounded in the fact that there is currently no medication clinically available for treating cardiac deficits induced by TBI. Although TBI affects more male patients than female patients, direct comparisons of the severity and therapeutic effects of C21 in TBI-induced cardiac dysfunction between male and female animals require further evaluation. More importantly, elderly people are more susceptible to cardiovascular disease, and the pathway by which TBI aggravates cardiac damage is not clear. Although we found that improved cognitive and cardiac function in TBI after C21 treatment is correlated, a recent study revealed a strong phenotypic and genetic connection between brain and heart health. 46 The mechanisms by which AT2R activation modulates brain-heart relationships have not yet been elucidated and warrant further investigation. Moreover, it is also worth exploring the interactions between the brain and other organs and systems, and multiorgan or multisystem pathophysiological mechanisms in TBI may provide potential insights to benefit TBI patients.
Transparency, Rigor, and Reproducibility Summary
Six to eight mice per group were employed to assess the overall significant effects by two-tailed unpaired t tests, and ANOVA followed by the Tukey's post hoc test was used to compare data from multiple groups. A p < 0.05 was considered significant after comparisons. Overall, 87 male mice were subjected to the experiment in this study. Different experimenters were assigned to give treatment or perform behavior tests, and they were blinded to condition until the study was complete. Six animals died after CCI before receiving treatment, two were excluded for technical reasons in the EB permeability test, and one was too weak to participate in the behavior tests. Complete data were obtained from 79 8- to 10-week-old mice at the time of injury. Mice were subjected to experimental CCI or sham procedures and were randomly assigned using an online random number generator to experimental groups.
Footnotes
Acknowledgments
We would like to thank Jianwei Liu from Tianjin University of Traditional Chinese Medicine and Shenghui Li from Tianjin Medical University General Hospital for their technical support in echocardiography and MRI respectively.
Authors' Contributions
Conception and design: PL, RJ; data acquisition: YQ, SD, MN, ML, YT; data analysis and interpretation: XL, WJ, JY; manuscript drafting: YQ; manuscript critical review: RJ, PL. All authors have read and approved the manuscript.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (via Grant No. 82201518 to Y Qian and Grant No. 82071390 to R Jiang).
Author Disclosure Statement
No competing financial interests exist.