
Abstract
Outcomes from traumatic brain injury (TBI) including death differ significantly between high-, middle-, and low-income countries. Little is known, however, about differences in TBI research across the globe. The objective of this article was to examine randomized controlled trials (RCTs) of moderate-to-severe TBI in high-income countries (HICs) compared with low- and middle-income countries (LMICs), as defined by the World Bank income per capita cutoff of $13,205 US dollars. A systematic review was conducted for articles published in the English language to December 2022 inclusive using MEDLINE, PubMed, Scopus, CINAHL, EMBASE, and PsycINFO in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Inclusion criteria: (1) human participants with a mean age of ≥18 years; (2) ≥50% of the sample had moderate to severe TBI; and (3) the study design was a RCT. Data extracted included author, year, country, sample size, primary focus (medical/surgical management or rehabilitation), injury etiology, time post-injury, and indicator(s) used to define TBI severity. There were 662 RCTs (published 1978–2022) that met inclusion criteria comprising 91,946 participants. There were 48 countries represented: 30 HICs accounting for 451 RCTs (68.1%) and 18 LMICs accounting for 211 RCTs (31.9%). The 62.6% of RCTs from LMICs were conducted in the acute phase post-injury (≤1 month) compared with 42.1% of RCTs from HICs. Of RCTs from LMICs, 92.4% focused on medical/surgical management compared with 52.5% from HICs. Since 2016, more RCTs have been conducted in LMICs than in HICs, indicating the importance of better understanding this pattern of research output.
Introduction
Traumatic brain injury (TBI) is a challenging global health issue with high rates of morbidity and mortality across the world, particularly in low- and middle-income countries. 1 The medical, surgical, and rehabilitation management of TBI varies across the globe, and research into the diversity of practices being conducted in high-, middle-, and low-income countries may offer insights valuable to optimizing patient outcomes. 2 Yet little is known about the differences in research being conducted in persons with TBI worldwide. 3
It is estimated that 64 to 74 million people worldwide sustain a TBI each year. 4 A TBI can be mild, moderate, or severe and can result from a variety of mechanisms such as falls and vehicle collisions. 5 There are significant regional variations in TBI etiology, with Africa and Southeast Asia having the highest proportion of TBI attributable to road traffic accidents, 4 Japan and Europe having higher rates of TBI reported from falls as their populations age, 6,7 and countries experiencing violence or armed conflict having higher rates of TBI from blasts and firearms. 8,9
Like etiology of injury, patient outcomes, particularly for moderate to severe TBI, vary significantly across the world. De Silva and colleagues 10 found in a post hoc analysis of an RCT of 10,008 participants with TBI that mortality rate was higher 21% in middle- and low-income countries than in high-income countries. Given the worldwide prevalence of TBI, understanding factors that contribute to the differences in outcomes between high-, middle- and low-income countries is imperative to improving care for individuals with TBI.
Given the differences in both etiology and outcomes of individuals with TBI in high-income countries (HICs) and low- to medium-income countries (LMICs), it warrants a further look into how the research in these countries compares. This type of comparison has not been examined closely to date in the literature; however, a narrative analysis by Allen coworkers 2 found LMICs were conducting mostly non-randomized and single-center studies and noted that these might not offer the standard of care expected in HICs. 2 Evaluating the research landscape across high-, middle-, and low-income countries may therefore offer insights into differences in outcomes.
The objective of this article is to examine randomized controlled trials (RCTs) of moderate to severe TBI worldwide to compare the studies conducted in HICs with those conducted in LMICs.
Methods
Literature search
A systematic review was conducted for articles published in the English language, up to and including December 2022, using MEDLINE, PubMed, Scopus, CINAHL, EMBASE, and PsycINFO, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Literature searches were restricted to RCTs and English language articles. Select key terms such as “brain injury,” “head injury,” “head trauma,” “randomized,” “placebo controlled,” and “randomized controlled trial” were used in combination, and Medical Subject Headings (MeSH) were used as available in each database. Variations of these terms were used, as appropriate, for each separate database search. See Supplemental File 2 for search strategy.
Full search results from each database were imported to Endnote version 8 (Camelot UK Bidco Limited [Clarivate]), and duplicate references were removed. The titles and abstracts of unique articles were screened against inclusion criteria. Those meeting inclusion were reviewed in their entirety and assessed for eligibility for inclusion by two independent reviewers; any conflicts were resolved by an independent third reviewer. If the full-text version of an article could not be located, an email was sent to the corresponding author requesting a copy. Authors were given one month to respond before the article was excluded. For the full list of included RCTs, see Supplemental File 1.
Inclusion and exclusion criteria
Studies were included if they met the following a priori inclusion criteria: (1) human participants with a mean age of ≥18 years; (2) ≥50% of the sample had moderate to severe TBI; and, (3) the study design was a RCT. The RCTs that reported mixed etiologies (e.g., stroke, brain tumors) were only included if ≥50% of participants had traumatic etiology. Protocols and secondary analyses of RCTs were excluded, as were studies when the reporting of the injury severity and/or etiology was unclear.
Data extraction
Data extracted from studies meeting inclusion criteria included journal name, author, year, country, total sample size, injury etiology, time post-injury (TPI), indicator(s) used to define TBI severity, and primary focus (i.e., medical/surgical management or rehabilitation).
Defining high-income versus low- and middle-income countries
The World Bank classifies national economies as high-, upper-middle, lower-middle, and low-income based on gross national income per capita in U.S. dollars (USD), with HICs having a gross national income per capita above or equal to $13,205 USD in 2021 (World Bank). For the purposes of our analyses, and in alignment with the World Bank 2021 classification, HICs were defined as having an income per capita at or above $13,205 USD, and LMICs were defined as those countries having an income per capita below $13,205 USD. For this analysis, we did not further subdivide middle-income countries as upper- and lower-middle.
The country of each study was determined by reviewing the methods for the location in which the RCT occurred, or, if unavailable, using the country listed in the primary authors' affiliation. For international studies conducted in multiple countries by a team of international researchers (e.g., CRASH trials), the country was determined using the funding source, or, if unavailable, the country listed in the original registration of the trial. Funding sources can be found in Supplemental File 4.
Defining primary study focus
For this analysis, studies were classified as focused on either rehabilitation or medical/surgical management. Studies were categorized as rehabilitation if they addressed the improvement of functional outcomes, including (but not limited to): speech, physical movement, cognition, emotional, behavior and social participation; early rehabilitation that occurs in critical care was also considered to belong to this group. 11 Studies in the medical/surgical management category addressed critical care and interventions to prevent death and further neurological damage, often in intensive care unit (ICU) settings, including (but not limited to): tracheostomy, red blood cell transfusion, hypothermia therapy, surgery, and intracranial pressure (ICP) management and monitoring. 12
The majority of pharmacological interventions were included in the medical/surgical management group (e.g., mannitol, tranexamic acid). Pharmacological interventions to improve motor function, sleep quality, cognition, among other domains, were included in the rehabilitation group (e.g., betahistine, methylphenidate). Some of these interventions were combined with non-pharmacological interventions (e.g., botulinum toxin + motor training). Decisions on classification of pharmacological RCTs related to the aim of the study, TPI, outcome measures used, and the setting. For instance, electrolytic solutions used in an ICU setting were considered part of medical/surgical, while cognitive enhancers for rehabilitation of chronic attention or memory difficulties in the chronic phase were classified as rehabilitation.
TPI
The TPI was defined as: acute (≤1 month), subacute (>1 to <6 months), chronic (≥6 months), or not reported and was measured as the time from initial injury to time of enrollment in the study. The mean TPI of the study participants within each RCT was used to categorize studies.
Determining journal impact factor
Impact factor is frequently used as an indicator of the importance and relevance of articles published by a specific journal. In this analysis, impact factor was used as a measure of study quality. Studies have demonstrated empirically that journals with higher impact factors publish studies of higher quality. 13 –16 To determine journal impact factor, the journal name for the year of the RCTs' publication was searched in Clarivate Journal Citation Reports 2023. If the journal did not have an impact factor in the year of the RCT's publication, “not available” (N/A) was entered, regardless of future impact factor ratings. Impact factors are not available for RCTs published before 1997.
Statistical analysis
Standard descriptive statistics were used to summarize the study characteristics and extracted variables. Data management and the generation of geographic heatmaps and tables were conducted using Microsoft Excel for Mac Version 16.74 (Microsoft, 2023). Given the distinct total numbers of RCTs in HICs and LMICs, percentages were incorporated into the tables to show the differences while controlling for the total RCT counts. Chi square tests were used to compare the proportions of RCTs across different time post-injury categories (SPSS, version 29.0.0).
Results
Description of studies
There were 12,400 articles identified. After removing duplicates, 9053 unique articles were screened for title and abstract; of these, 846 underwent full text review. Finally, 662 RCTs published from 1978 to 2022, representing 91,946 participants, met inclusion criteria and underwent data extraction (Fig. 1).
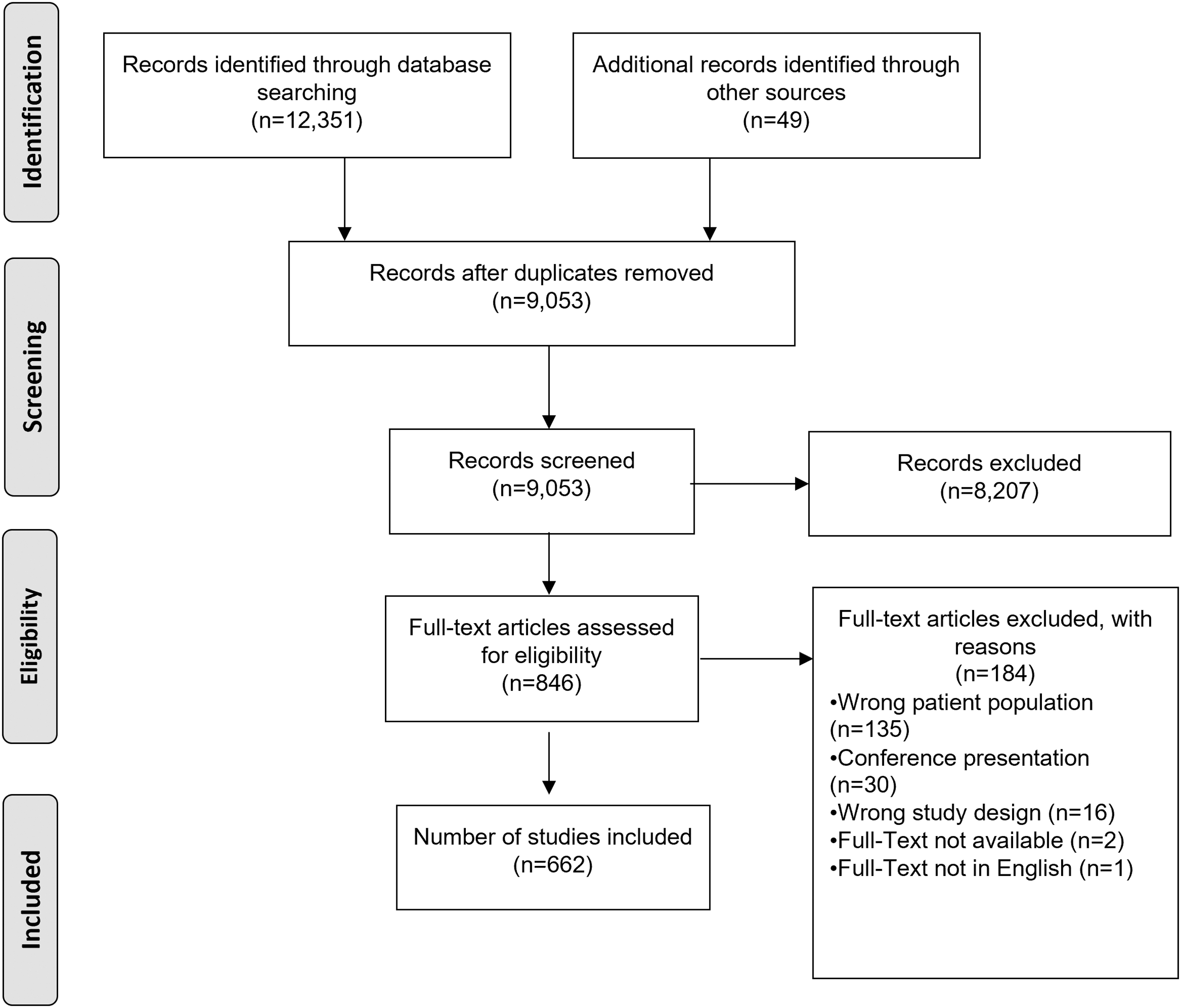
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Sample sizes
The mean sample size was 147.4. Sample sizes in the individual RCT ranged from 3 to 12,737 participants. The majority of RCTs (507, 76.6%) had sample sizes of <100 individuals; 141 RCTs (21.3%) had sample sizes of 101–500 individuals, and only 14 RCTs (2.1%) had sample sizes of >500 individuals (Supplementary File 3), all with a research focus on medical/surgical management.
The mean sample size for all 662 RCTs was 147.2 (median 52.5). Among medical/surgical RCTs, the mean sample size was 195.8 (median 62.0) compared with a mean of 56.4 (median 36) in rehabilitation RCTs. The RCTs from HICs had a mean sample size of 89.64, while the mean sample size in LMICs was 73.15. When comparing the individual countries in each group, United Kingdom had the highest mean sample size (M = 778.93) in the HICs group, and China had the highest mean sample size (M = 122.57) in the LMICs group.
Countries and RCTs
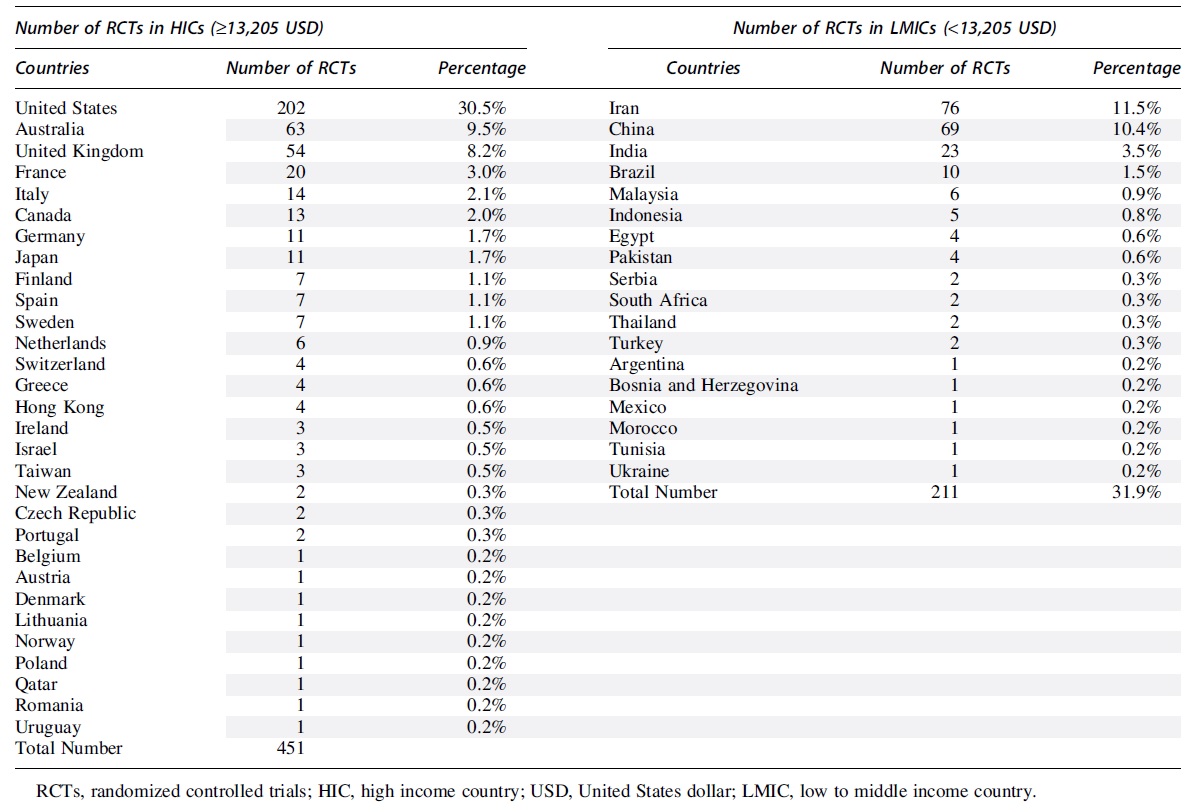
The 662 included studies were conducted in 48 countries (Fig. 2). Of 662 RCTs (68.1%), 451 were conducted by authors in HICs, and 211 (31.9%) were conducted by authors in LMICs (Table 1). The largest proportion of studies was conducted in the United States (30.5%), followed by Iran (11.5%), China (10.4%), Australia (9.5%), and the United Kingdom (8.2%) (Table 2).
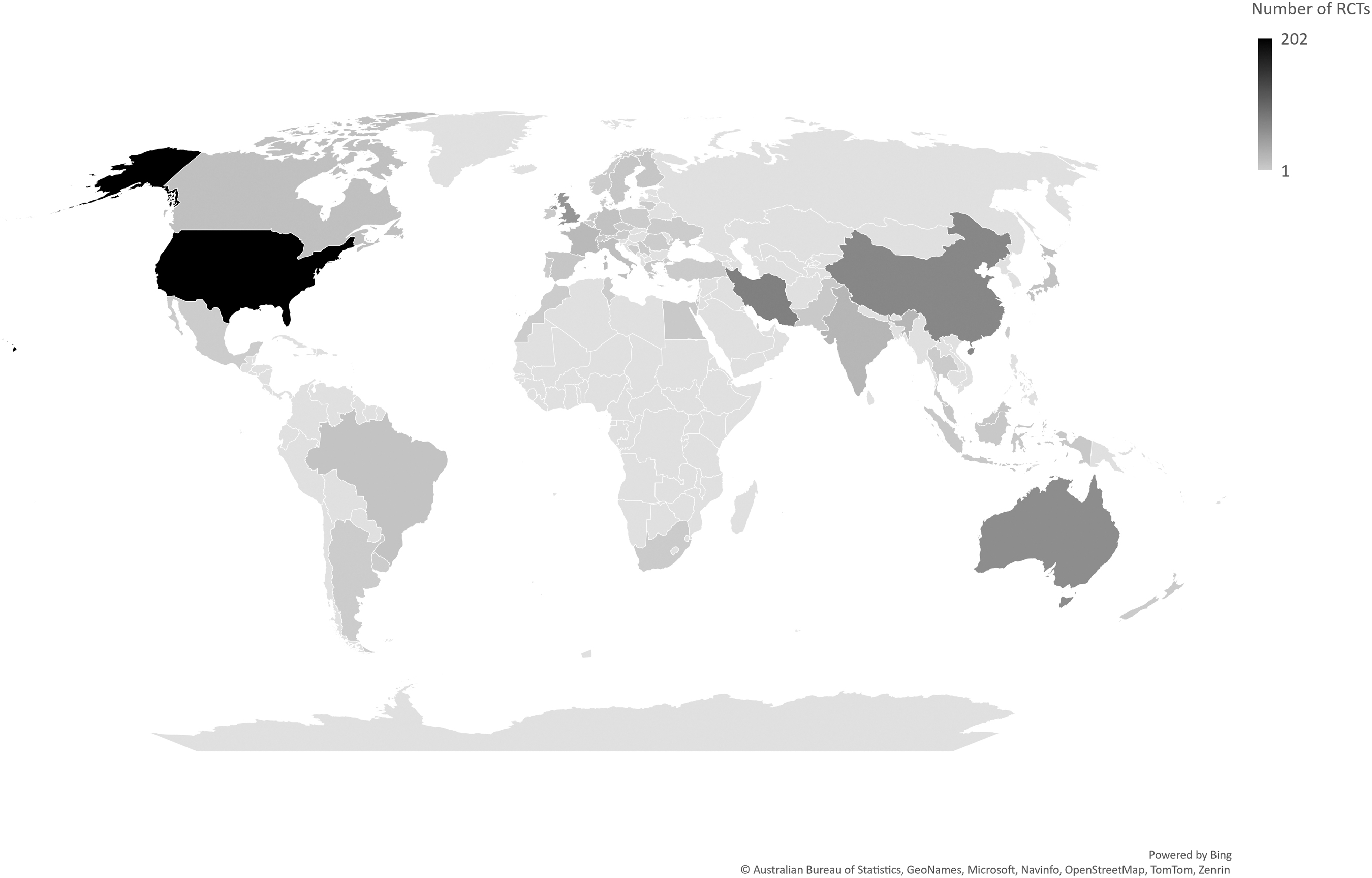
Global distribution of number of randomized controlled trials (RCTs) of moderate to severe traumatic brain injury by country.
Number of Randomized Controllled Trials from High Income and Low to Middle Income Countries
RCT, randomized controlled trial; HIC, high income country; LMIC, low to middle income country.
Number of Moderate to Severe Traumatic Brain Injury Randomized Controlled Trials Published by Country and Gross National Income Per Capita
Temporal Trends in RCTs in HICs and LMICs
The number of RCTs being conducted in LMICs has been accelerating in the last 12 years. In LMICs, 84.4% of the RCTs were published after 2011, compared with only 15.6% of RCTs conducted before 2011 (Fig. 3). In 2016, the annual number of RCTs from LMICs exceeded the annual number of RCTs from HICs for the first time. Since 2016, the annual number of RCTs from LMICs has consistently surpassed that from HICs in six of the last seven years.
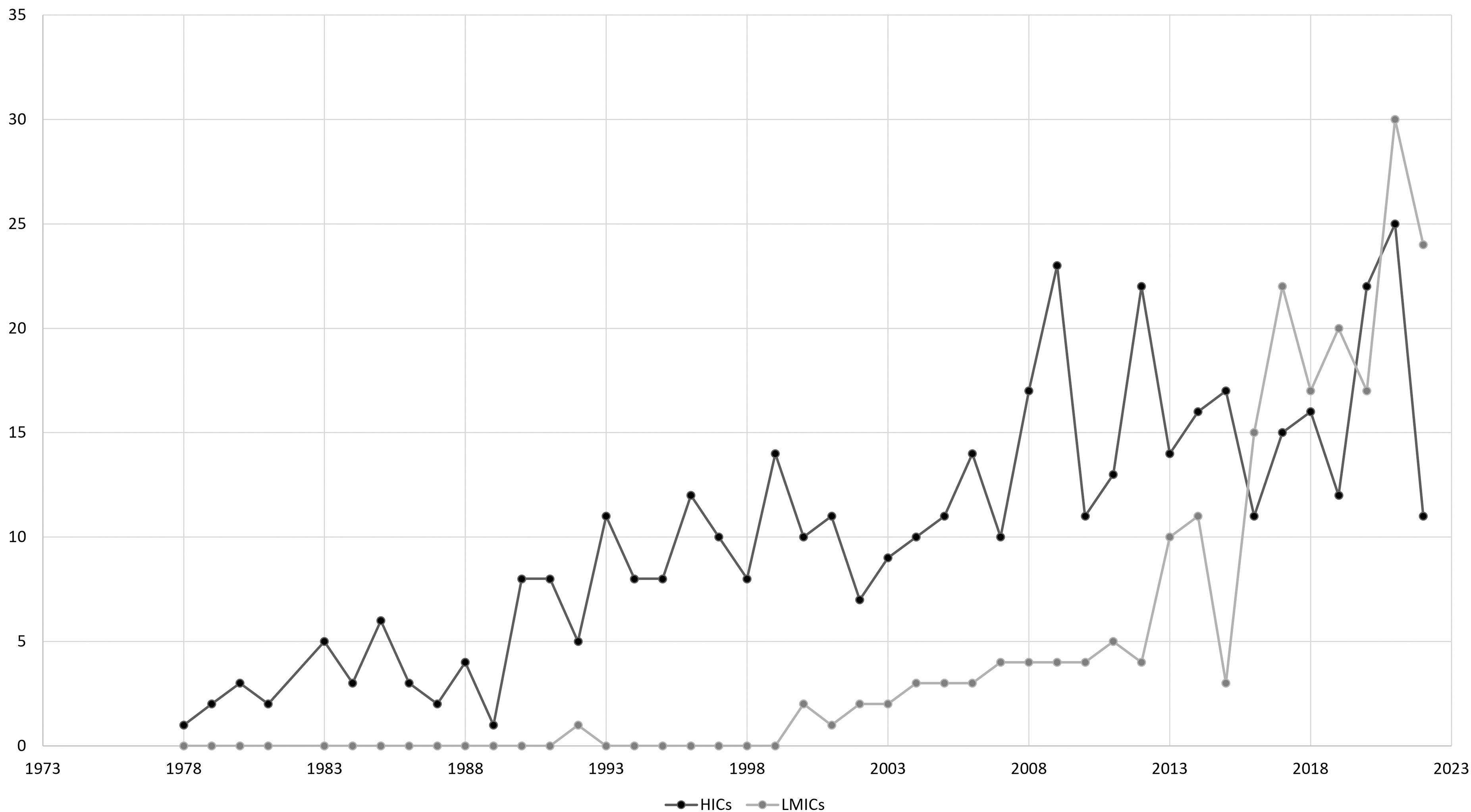
Annual number of randomized controlled trials (RCTs) from high income countries (HICs) and low to middle income countries (LMICs).
As shown in Figure 4, this shift in TBI RCT output is driven primarily by marked increases in the number of medical/surgical management RCTs being conducted in LMICs. Whereas the number of annual medical/surgical management RCTs from HICs has remained relatively stable since 1990, the number of medical/surgical management RCTs from LMICs has dramatically increased since 2010 (Fig. 4). This increase has been driven largely by Iran, China, and to a lesser extent India. These account for 168 (79.6%) of 211 RCTs in LMICs.
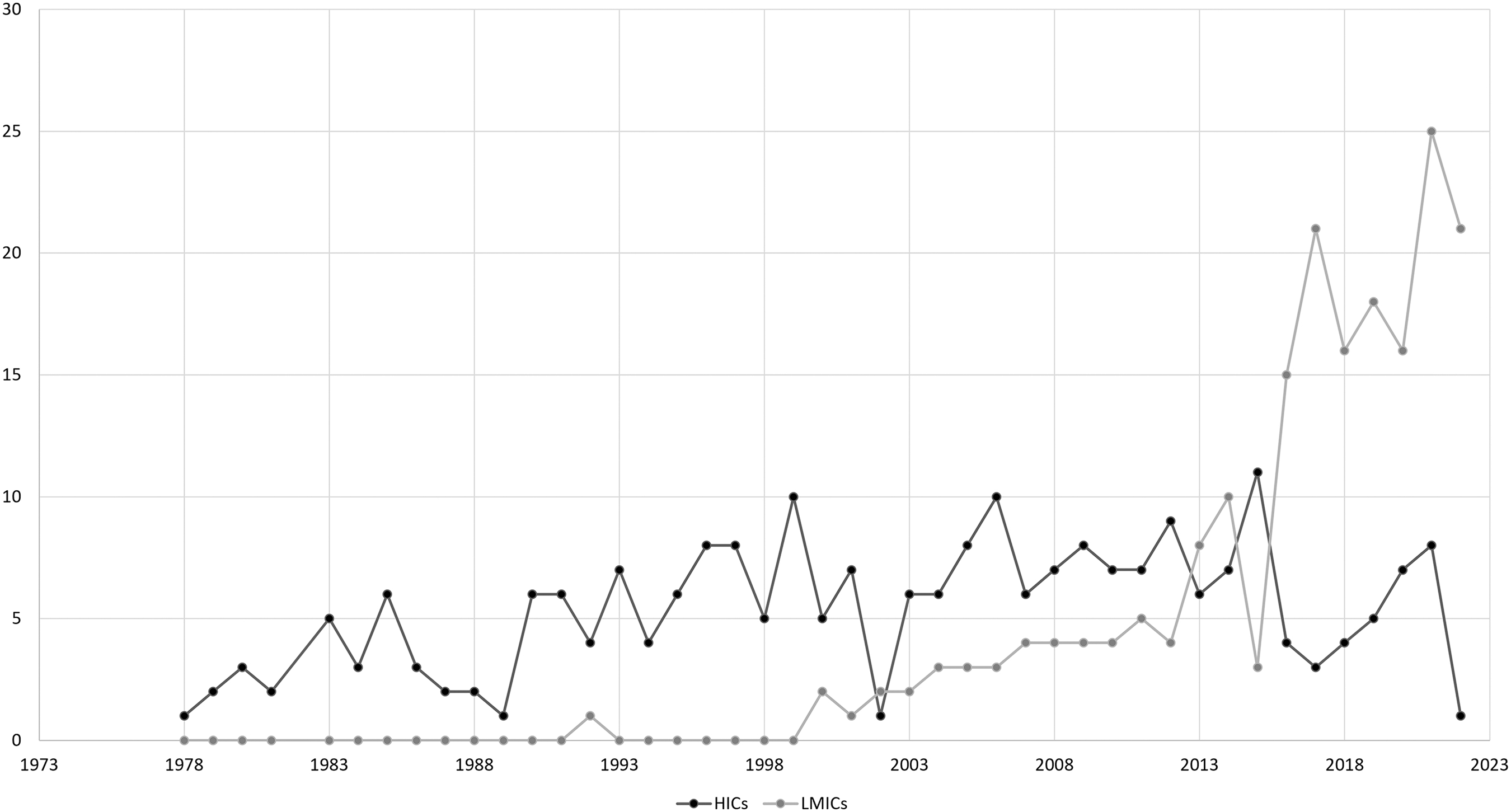
Number of medical/surgical management randomized controlled trials (RCTs) over time from high income countries (HICs) and low to middle income countries (LMICs).
Figure 5 shows the change over time for the annual number of rehabilitation RCTs from HICs and LMICs. Rehabilitation RCTs from LMICs have shown a modest increase since 2017; before 2017, there were only three LMIC rehabilitation RCTs.
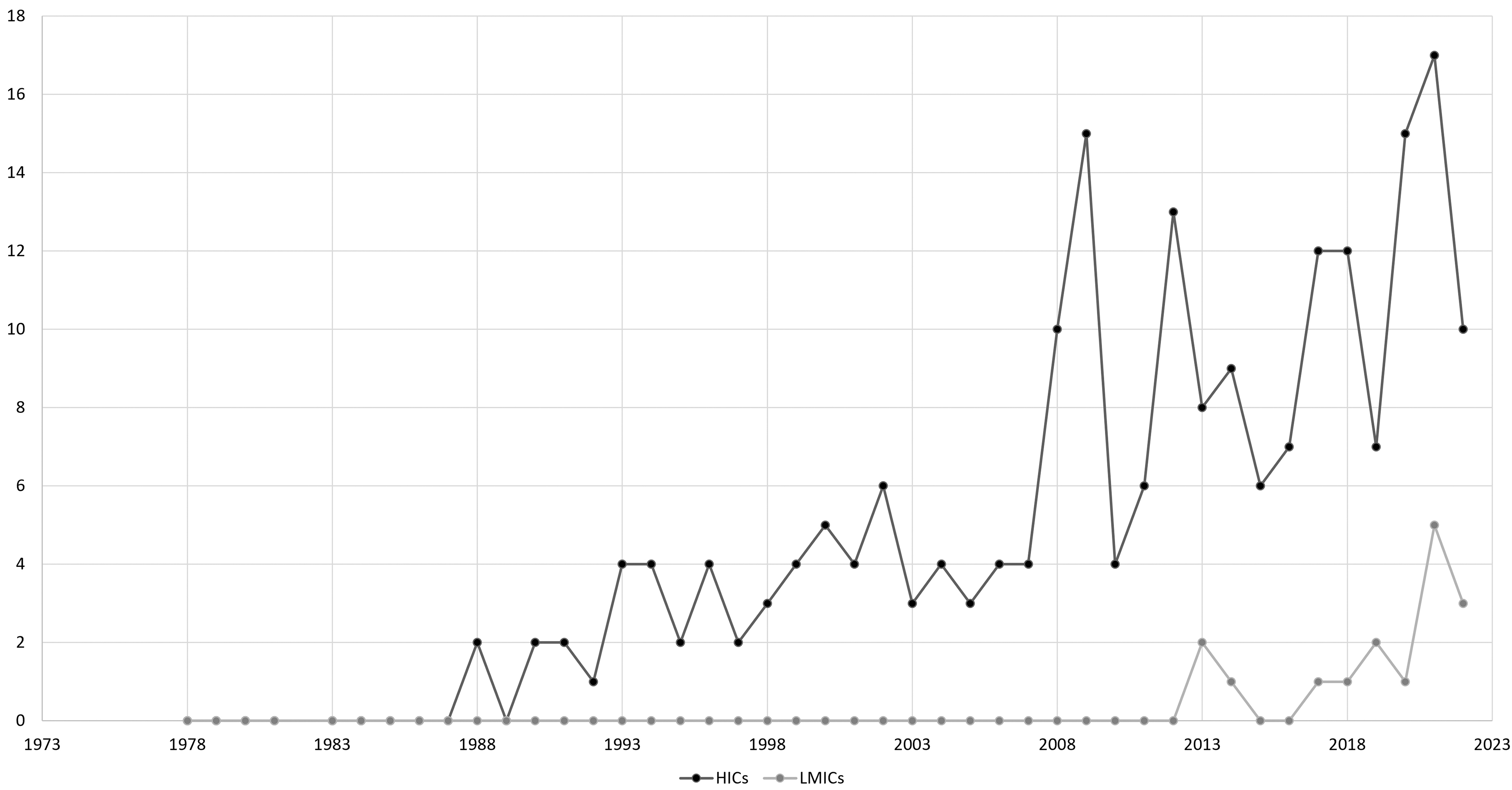
Number of rehabilitation randomized controlled trials (RCTs) over time from high income countries (HICs) and low to middle income countries (LMICs).
Medical/surgical management versus rehabilitation
The majority of RCTs in moderate to severe TBI studied interventions in medical/surgical management (432; 65.3%) and the minority studied interventions in rehabilitation (230; 34.7%) (Table 3 and Fig. 3, 4). The RCTs in HICs were nearly evenly divided between medical/surgical management and rehabilitation. Of the 451 RCTs conducted in HICs, 237 RCTs (52.5%) studied medical/surgical management and 214 RCTs (47.5%) studied rehabilitation interventions. In contrast, RCTs in LMICs focused overwhelmingly on medical/surgical management. Of the 211 RCTs conducted in LMICs, 195 (92.4%) evaluated medical/surgical management, and 16 RCTs (7.6%) studied rehabilitation interventions.
Area of Research Focus in Randomized Controlled Trials from High Income Countries Compared With Low to Middle Income Countries
HIC, high income countries; LMIC, low to middle income countries.
When examining RCTs focused on rehabilitation interventions, there has been steady growth over time primarily originating from authors in HICs (Fig. 4). In comparison, there were three rehabilitation RCTs from LMICs before 2017 with only a modest increase seen after that (Fig. 4). Figure 5 demonstrates the steady increase in the overall number of RCTs published, the dramatic rise in medical/surgical management RCTs from LMICs, and the more gradual rise in rehabilitation RCTs from HICs over time.
Almost half of RCTs examined pharmacological interventions (313; 47.3%), alone or in combination with other pharmacological and non-pharmacological interventions. Of these, a total of 98 (31.3%) RCTs were conducted in the United States, followed by Iran (56; 17.9%) and United Kingdom (29; 9.3%). Together, Iran, China, and India accounted for 28.4% (n = 89) of pharmacology RCTs.
TPI
The TPI was reported in 519 RCTs (78.4%) (Table 4). The TPI was not reported in 71 (15.7%) RCTs from HCIs and 72 (34.1%) RCTs from LMICs, a statistically significant difference (p < 0.001). Of all studies (322/662), 48.6% recruited participants in the acute phase (≤1 month post-injury); this accounted for the majority (62.0%) of RCTs for which TPI was reported (322/519). The majority of RCTs conducted in LMICs recruited participants in the acute phase post-injury, with few studies conducted in the subacute and chronic phases post-injury (Table 4). This was statistically significant (p < 0.001).
Summary of Randomized Controlled Trials in High Income Countries versus Low to Middle Income Countries by Time Post-Injury
TPI, time post-injury; RCT, randomized controlled trials; HICs, high income countries; LMIC, low to middle income countries.
Within the HICs, the proportion of RCTs conducted in the acute phase was comparable to RCTs in the chronic phase, with the smallest percentage of RCTs in the subacute phase (p < 0.001). Overall, the least studied TPI was subacute, (>1 to <6 months post-injury), accounting for 5.6% of all RCTs (p < 0.001). The RCTs conducted in the subacute and chronic phases post-injury were statistically significantly more likely to be conducted in HICs than LMICs (p < 0.001). Of the 168 RCTs from Iran, China, and India, 107 (63.7%) were conducted in the acute phase post-injury, one study was conducted in the subacute phase, three studies in the chronic phase post-injury, and 57 (33.9%) did not report time post-injury.
Indicators of injury severity
The majority of RCTs (545/662; 82.3%) used the Glasgow Coma Scale (GCS) to determine TBI severity (Table 5). The next two most reported severity indicators were duration of post-traumatic amnesia (PTA), reported in 120 (18.1%) RCTs and duration of loss of consciousness or presence of a disorder of consciousness (LOC/DOC), reported in 65 (9.8%) RCTs. The Abbreviated Injury Scale (AIS) and the Injury Severity Score (ISS) were often used in studies with polytrauma populations, alone or in combination with the indicators above
Injury Severity Indicators Used in High Income Countries and Low to Middle Income Countries Randomized Controlled Trials
GCS, Glasgow Coma Scale; PT, post-traumatic amnesia; LOC/DOCV, loss of consciousness/disorder of consciousness; AIS, Abbreviated Injury Scale; Injury Severity Score.
Percentages are calculated based on the total number of RCTs across the database, and on total of RCTs per income category (high income = 451, and low to middle income = 211)
In RCTs from LMICs, 196 (92.9%) RCTs used the GCS to determine TBI severity, while PTA and LOC/DOC were reported in very few RCTs (<5% for both). In RCTs from HICs, 349 (77.4%) RCTs used the GCS to determine TBI severity; PTA and/or LOC/DOC were reported in 175 studies. In RCTs from both LMICs and HICs, few studies determined TBI severity using AIS (2.0%) or ISS (3.5%) (Table 5).
Impact factor of RCTs in LMICs and HICs
The impact factor for the journal of publication could be determined in 490 studies, 350 from HICs and 140 from LMICs (Table 6); with 93 studies published before 1997 (92 from HICs, one from LMICs), and therefore impact factor could not be determined. Of all TBI RCTs, 60/662 (9.1%) were published in journals with impact factors >5.0, of which 91.7% were from HICs and 8.3% from LMICs. Of all RCTs, 246 (37.2%) were published in journals with impact factor of >2.5, of which, 81.3% were from HICs and 18.7% from LMICs (Fig. 6).
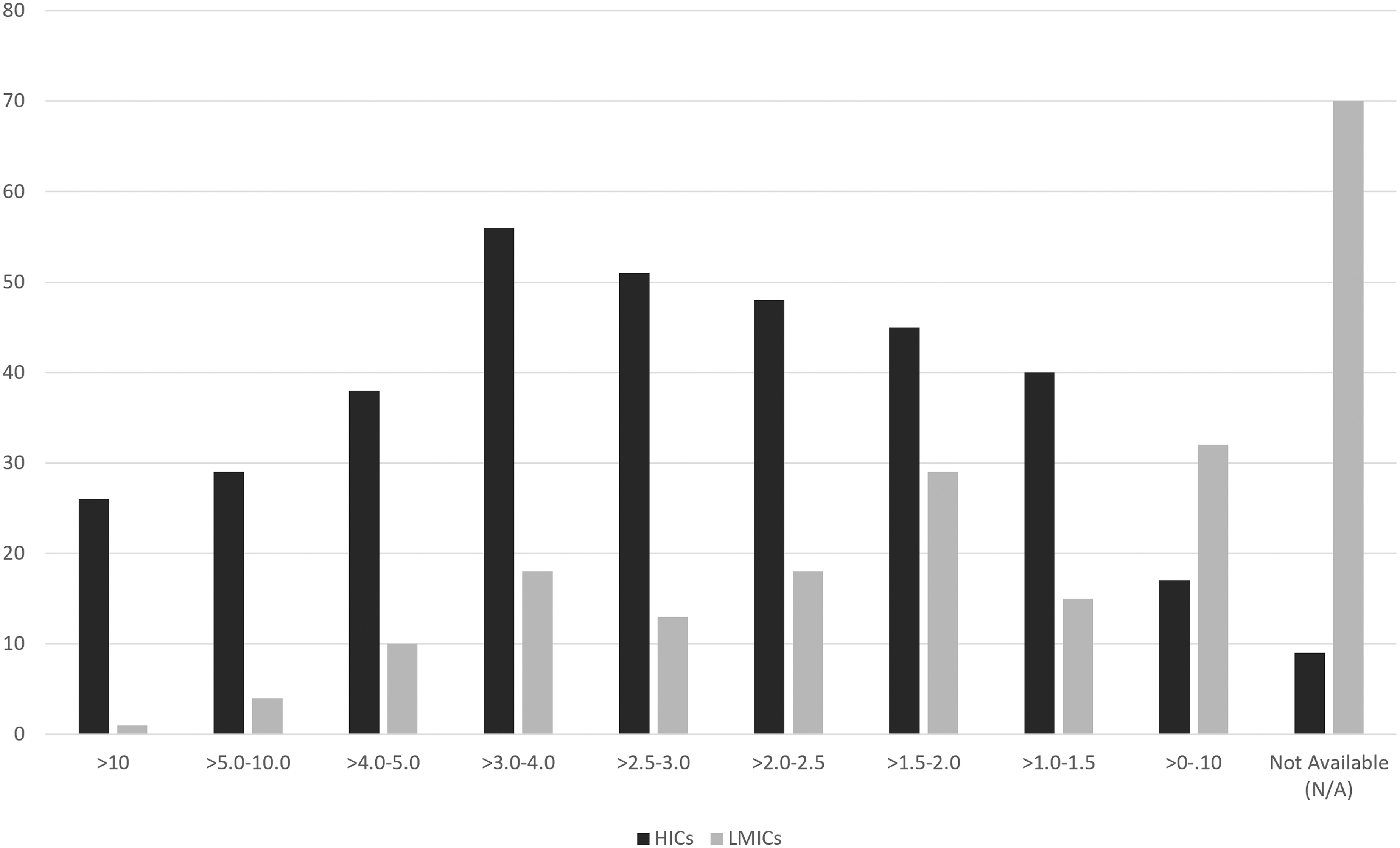
Distribution of impact factors for randomized controlled trials (RCTs) in high income countries (HICs) and low to middle income countries (LMICs).
Impact Factors for Randomized Controlled Trials of Moderate to Severe Traumatic Brain Injury in High Income Countries Versus Low to Middle Income Countries
HICs, high income countries; LMIC, low to middle income countries.
The most common impact factor for RCTs from HICs was >3.0–4.0 (56 RCTs, 12.5%) and for LMICs was N/A (69 RCTs, 32.4%) followed by >0–1.0 (32 RCTs, 15.0%). The least common impact factor for HICs was N/A (10 RCTs, 2.2%), followed by >0–1.0 (17 RCTs, 3.8%) and for LMICs was >10.0 (1 RCT, 0.5%).
Discussion
This systematic review of 662 RCTs of moderate to severe TBI illustrates significant diversity in TBI research across the globe and the significant, increasing role of LMICs in moderate to severe TBI research. While TBI RCTs have originated from a total of 48 countries, the three most productive countries are the United States, Iran, and China; the latter two are categorized as LMICs. The relative productivity of HICs and LMICs has shifted over time.
Although less than a third of all TBI RCTs were conducted in LMICs, in the last decade, the proportion of RCTs published worldwide shifted from the majority in HICs to the majority in LMICs. The recent substantial and growing RCT output from LMICs has shifted the landscape of TBI research as a whole in three ways: toward research in the acute phase post-injury; toward research focusing on medical/surgical interventions; and toward publication in non-indexed or low impact factor journals.
The reason for the first of these shifts is that the marked increase in TBI RCT output from LMICs is largely driven by a significant increase in studies being conducted in the acute phase post-TBI. Whereas 48.6% of all RCTs took place during the acute phase (≤1 month post-injury), RCTs from LMICs accounted for a markedly higher proportion herein than RCTs from HICs. The proportion of acute phase studies may be an underestimate, because 21.6% of RCTs did not report TPI; this was more common in RCTs from LMICs than HICs (34.1% and 15.7%, respectively).
This increasing research emphasis on acute phase studies in LMICs may also explain the differences in measures of injury severity used in RCTs in LMICs compared with HICs. Severity can be determined using radiographic or clinical tools, the most common of which is the GCS, with lower scores of 3–12 indicating moderate to severe injuries. 17 In RCTs from LMICs, GCS was almost universally reported as the metric for determining injury severity (92.5%), whereas RCTs from LMICs rarely reported duration of PTA (0.9%) or presence and/or duration of LOC/DOC (4.2%). In contrast, RCTs from HICs frequently used GCS (77.4%) as one or part of injury severity determination but were also more likely to report duration of PTA (26.4%) and/or LOC/DOC (12.6%).
Given that determining the duration of PTA and/or LOC/DOC requires longitudinal evaluation, these measures of injury severity are less useful for studies recruiting in the first month post-TBI, when many eligible patients with moderate to severe TBI may be in PTA and/or LOC/DOC and thus the duration cannot be established at the time of enrollment.
A second consequence of the shift to the recent majority of RCTs being from LMICs is a relative change in RCT focus away from rehabilitation and toward medical/surgical interventions. The HICs accounted for 451 (68.1%) RCTs of which 214 were in rehabilitation (47.5%) and 237 were medical management (52.5%). The LMICs accounted for 211 (31.9%) RCTs of which 16 were in rehabilitation (7.6%) and 195 were in medical/surgical management (92.4%).
Because TBI RCTs conducted in LMICs overwhelmingly focused on medical/surgical management instead of rehabilitation, the relative proportion of rehabilitation and chronic phase studies has diminished over time. The precise reasons for this predominance of acute phase RCTs focused on medical/surgical management from LMICs is not known and is likely multi-factorial.
Putative reasons for this research observation include differences in priorities for health systems resource allocation and/or RCT funding in LMICs compared with HICs. This LMICs productivity may reflect a greater emphasis on acute medical and surgical resource allocation in LMICs compared with HICs, where healthcare resources may be more equitably distributed between acute and chronic phases and rehabilitation post-TBI is more widely available. 2,18 In addition, there are significant unmet needs for rehabilitation services in LMICs, often exacerbated by lack of infrastructure, as well as unequal distribution of resources, unavailability of skilled health personnel, and barriers to transportation. 19 Therefore, the lack of rehabilitation RCTs in LMICs likely reflects the limited provision of rehabilitation services in these countries and the need to integrate rehabilitation in all levels of the healthcare system. 20
Another possibility is that RCT funding differences vary markedly between HICs and LMICs. In one systematic analysis of neurosurgical trials, RCTs in LMICs were more likely to receive institutional funding compared with industry funding, whereas the opposite was true in HICs. 21 An additional possibility is that there may be different research participation regulations in acute phase settings in LMICs and/or in chronic phase settings in HICs, which may explain the recent dominance by LMICs in acute TBI RCTs.
Having few RCTs from LMICs in the rehabilitation phase requires one to extrapolate from research performed in more wealthy countries. Likewise, the increasing dominance of LMICs in the production of medical/surgical, almost entirely acute RCTs, means that one must increasingly rely on these RCTs for best evidence. Thus, the applicability of conclusions drawn from rehabilitation RCTs in HICs and from acute medical/surgical RCTs in LMICs may not translate to LMICs and HICs, respectively.
The final shift is in where RCTs examining moderate to severe TBI are published. Compared with RCTs from HICs, RCTs from LMICs were much more likely to be published in journals without an impact factor (33.2% compared with 2.0%). Because journal impact factor is a measure of study rigor and quality, these findings align with those of Allen and coworkers, 2 who reported evidence that much of the TBI research performed in LMICs is of lesser quality.
Importantly, however, the present systematic review identified that this is not universal, and a sizeable proportion of RCTs (n = 46, 18.7%) from LMICs are published in journals with impact factors >2.5, indicating high quality research. Moreover, there may be many barriers to publication in high impact factor journals aside from study quality. One possibility is, as Eckmann and Bandrowski 22 reported, that developing countries experience challenges with publishing research.
Among the potential barriers heightened for research from LMICs is high costs of publication, lack of institutional support and/or external funding, language, and bias. A second possibility is that LMICs are using low or no impact factor journals to publish negative trials, as a way to overcome biases against negative trial publications, although this analysis was beyond the scope of this review. 23 –25 A third possibility is that high impact factor journals are wary of accepting RCTs in which ethical conduct of researchers is in question. Several analyses have identified concerns with research conducted in countries where illiteracy is high, yet written consent is frequently obtained for research participation, including but not limited to Iran, which was the second largest contributor to TBI RCTs in this review. 26 –28 Although beyond the scope of this review, this finding that LMICs tend to be published in lower quality journals needs to be assessed in greater detail, with a more in-depth assessment of the methodological quality of the RCTs in question.
Limitations
This systematic review has several limitations. One major limitation is that only articles published in the English language were eligible for inclusion; therefore, we may not have a comprehensive picture of all RCTs being conducted worldwide. This may affect RCTs from both HICs and LMICs whose primary language is not English. Second, we characterized the number of studies being conducted, but not the total numbers of participants represented in the studies.
Third, this systematic review relied on journal impact factor as a surrogate for study quality because of the enormous diversity in the interventions studied. Impact factor is frequently used as an indicator of the importance and relevance of articles published by a specific journal, and studies have empirically demonstrated that journals with higher impact factors publish studies of higher quality. 13 –16 This methodology for study quality, however, does not specifically analyze each individual RCT. Moreover, it is not known whether impact factor correlates well with RCT quality in LMICs, where barriers to publication other than study quality may also limit publishing in higher impact journals because– most researchers in LMICs do not use English as their primary language. 22 Other limitations relate to the narrow focus of the review, which did not consider studies of persons with mild TBI and only included RCTs.
Conclusion
This systematic review of 662 RCTs of moderate to severe TBI reveals nearly a third of all RCTs were conducted in LMICs and, since 2016, more than half of all RCTs published worldwide originated from LMICs. There has been a dramatic increase in the number of TBI RCTs published by authors in LMICs. The 65.3% of TBI RCTs focus on medical/surgical management, and almost two-thirds of TBI RCTs recruit patients in the acute phase post-injury. This is driven, in part, by the majority of RCTs published by authors in LMICs focusing on medical and surgical management in the acute phase post-TBI.
Universally, across LMICs and HICs, the GCS is the most reported metric for establishing TBI severity. Nearly all research on rehabilitation of moderate to severe TBI and nearly all research in the chronic phase post-injury comes from HICs. A better understanding of the roles of LMICs and HICs is critical to understanding the landscape of the moderate to severe TBI research literature.
Transparency, Rigor and Reproducibility Summary
A protocol was not registered on the International Prospective Register of Systematic Reviews previous to this submission. This manuscript presents data from a database of 662 RCTs on moderate to severe TBI. An initial search was conducted up to June 2021, with an updated search conducted up to and including December 2022. The impact factor reported in Journal of Citations Report was used as a metric of quality. We did not perform GRADE or Cochrane risk of bias. We acknowledge that countries can change their income status overtime; however, we only considered the income classification of the World Bank data reported for 2021 since our data is up to 2022.
Footnotes
World Bank Hyperlink
Acknowledgments
The authors would like to acknowledge the valuable contributions of Muskan Sait to the preparation of this article.
Authors' Contributions
R. Teasell conceptualized and designed the study, C. Flores-Sandoval, S. Janzen and S. Mehrabi contributed to data extraction, analysis and writing. All authors contributed to the drafting, writing and editing of the manuscript.
Funding Information
Funding was provided by the Ontario Ministry of Health and Long-Term Care through Neurotrauma Pathways and the St. Joseph's Health Care (London) Foundation.
Author Disclosure Statement
R. Teasell had received a grant from Allergan, now Abbvie (makers of Botox) for Stroke research within the last three years. For the remaining authors, no competing financial interests exist.
Supplementary Material
Supplementary File 1
Supplementary File 2
Supplementary File 3
Supplementary File 4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.