
Abstract
Blast-related mild traumatic brain injury (blast-mTBI) can result in a spectrum of persistent symptoms leading to substantial functional impairment and reduced quality of life. Clinical evaluation and discernment from other conditions common to military service can be challenging and subject to patient recall bias and the limitations of available assessment measures. The need for objective biomarkers to facilitate accurate diagnosis, not just for symptom management and rehabilitation but for prognostication and disability compensation purposes is clear. Toward this end, we compared regional brain [18F]fluorodeoxyglucose–positron emission tomography ([18F]FDG-PET) intensity-scaled uptake measurements and motor, neuropsychological, and behavioral assessments in 79 combat Veterans with retrospectively recalled blast-mTBI with 41 control participants having no lifetime history of TBI. Using an agnostic and unbiased approach, we found significantly increased left pallidum [18F]FDG-uptake in Veterans with blast-mTBI versus control participants, p < 0.0001; q = 3.29 × 10−9 [Cohen’s d, 1.38, 95% confidence interval (0.96, 1.79)]. The degree of left pallidum [18F]FDG-uptake correlated with the number of self-reported blast-mTBIs, r 2 = 0.22; p < 0.0001. Greater [18F]FDG-uptake in the left pallidum provided excellent discrimination between Veterans with blast-mTBI and controls, with a receiver operator characteristic area under the curve of 0.859 (p < 0.0001) and likelihood ratio of 21.19 (threshold:SUVR ≥ 0.895). Deficits in executive function assessed using the Behavior Rating Inventory of Executive Function–Adult Global Executive Composite T-score were identified in Veterans with blast-mTBI compared with controls, p < 0.0001. Regression-based mediation analyses determined that in Veterans with blast-mTBI, increased [18F]FDG-uptake in the left pallidum-mediated executive function impairments, adjusted causal mediation estimate p = 0.021; total effect estimate, p = 0.039. Measures of working and prospective memory (Auditory Consonant Trigrams test and Memory for Intentions Test, respectively) were negatively correlated with left pallidum [18F]FDG-uptake, p < 0.0001, with mTBI as a covariate. Increased left pallidum [18F]FDG-uptake in Veterans with blast-mTBI compared with controls did not covary with dominant handedness or with motor activity assessed using the Unified Parkinson’s Disease Rating Scale. Localized increased [18F]FDG-uptake in the left pallidum may reflect a compensatory response to functional deficits following blast-mTBI. Limited imaging resolution does not allow us to distinguish subregions of the pallidum; however, the significant correlation of our data with behavioral but not motor outcomes suggests involvement of the ventral pallidum, which is known to regulate motivation, behavior, and emotions through basal ganglia–thalamo–cortical circuits. Increased [18F]FDG-uptake in the left pallidum in blast-mTBI versus control participants was consistently identified using two different PET scanners, supporting the generalizability of this finding. Although confirmation of our results by single-subject-to-cohort analyses will be required before clinical deployment, this study provides proof of concept that [18F]FDG-PET bears promise as a readily available noninvasive biomarker for blast-mTBI. Further, our findings support a causative relationship between executive dysfunction and increased [18F]FDG-uptake in the left pallidum.
Introduction
Persistent post-concussive symptoms (PPCS) are an insidious consequence of blast-related mild traumatic brain injury (blast-mTBI), the “signature injury” of the wars in Iraq and Afghanistan. 1,2 Even years after sustaining blast-mTBI(s), many active duty service members and Veterans report somatic, cognitive, and behavioral symptoms that impair aspirational, occupational, social, and interpersonal function, with associated distress, reduced quality of life, and in some cases, substantial longstanding disability. Currently, clinical evaluations for military service-related mTBIs rely on retrospective recall of often remote events, usually with limited if any substantiating evidence. The need for objective biomarkers to improve diagnostic and prognostic accuracy, better stratify exposure severity, appropriately tailor treatment and rehabilitation measures, monitor response to therapy, and inform medical disability claims is clear. Biomarkers also offer clues to the neuropathological links between the effects of blast-mTBI and resultant PPCS, which could help target and optimize treatments that would interrupt or reverse neuropathological alterations caused by these injuries or at least provide symptomatic relief.
A search for reproducible biomarkers of blast-mTBI has been underway as the key objective of the longitudinal Veterans Affairs (VA) Rehabilitation Research & Development Service-funded “Mild TBI and Biomarkers of Neurodegeneration” study at the VA Northwest Mental Illness Research, Education, and Clinical Center, which began recruiting participants in 2008. The study sample includes Iraq and Afghanistan-deployed Veterans with usually repetitive blast-mTBI (with or without history of impact mTBI) as well as deployed veteran and nonmilitary controls having no lifetime history of TBI of any cause or severity. Exploratory analyses of potential biomarkers in our study have included plasma and cerebrospinal fluid markers, 3 –6 pituitary hormones, 7,8 neurocognitive measures, 9 –13 and behavioral symptoms and structural and functional brain magnetic resonance imaging. 14 –16 Earlier in the enrollment of this cohort study, we reported reduced regional glucose uptake in cerebellum, vermis, pons, and medial temporal lobe in 12 blast-mTBI Veterans compared with 12 community civilian controls. 17 We later reported reduced regional glucose uptake in parietal, somatosensory, and visual cortices in 34 blast-mTBI veterans and 18 deployed control veterans. 14 Translational studies to confirm and further investigate observations from this population using a model of blast-mTBI in mice are ongoing. 18,19
Several plasma biomarkers, including glial fibrillary acidic protein (GFAP) and S100β (reflecting astroglial injury), ubiquitin C-terminal hydrolase-L1 and neuron-specific enolase (reflecting neuronal cell body injury), myelin basic protein (reflecting white matter injury), and neurofibrillary proteins (reflecting axonal injury) have been shown to be elevated in acute mTBI and in more severe head trauma. 20 –23
Plasma GFAP has shown clinical prognostic utility in mTBI in emergency department settings. 3 Although several biofluid markers have been demonstrated to differ between mTBI and control groups, substantial overlap between groups makes these potential biofluid markers unsuitable as diagnostic biomarkers. 3
Neuroimaging has the potential to provide an objective noninvasive biomarker for blast-mTBI. Although, by definition, mTBI does not exhibit abnormalities on standard clinical brain computed tomography (CT) or magnetic resonance imaging (MRI; VA/Department of Defense [DoD] Practice Guideline for the Management of Concussion–Mild Traumatic Brain Injury), more sophisticated structural and functional neuroimaging modalities in the research setting, such as MRI volumetrics, diffusion tensor imaging, resting state and task-based functional MRI, 24 and perivascular space burden 16 have all demonstrated differences between mTBI and control groups. As with biofluid parameters, substantial overlap between groups makes these neuroimaging parameters unsuitable as diagnostic biomarkers for remote head trauma. 25
[18F]Fluorodeoxyglucose–positron emission tomography ([18F]FDG-PET) as a functional imaging modality offers potential as a sensitive noninvasive modality to detect chronic effects of remote mTBI. 26 [18F]FDG is a glucose analog that can enter the brain and subsequently neurons and glia through glucose transporter proteins. Thereupon, [18F]FDG is trapped, with its amount of uptake proportional to metabolic activity, which in the brain is primarily driven by neuronal activity. Cohort neuroimaging studies have validated the use of [18F]FDG-PET for facilitating diagnosis in several common neurological conditions. 27 –29 [18F]FDG-PET is widely available and has been in clinical use for well over 20 years and is thus an appealing candidate for biomarker identification with a realistic path for clinical deployment.
In this report, using an agnostic discovery approach to identify potential diagnostic biomarkers, we describe the results of an exploratory analysis of [18F]FDG-PET brain imaging in the complete cohort of 79 Veterans with blast-mTBI as compared with 41 control participants with no lifetime history of TBI and the association of imaging findings with motor, neuropsychological, and behavioral outcomes. Our analysis reveals consistently increased [18F]FDG-uptake in the left pallidum in the blast-mTBI group compared with controls with very good performance of receiver operator curve analysis, an unexpected but intriguing finding supporting the potential of [18F]FDG-PET brain imaging as a promising biomarker candidate for blast-mTBI.
Materials and Methods
Participants
The VA Puget Sound Health Care System and University of Washington Institutional Review Boards approved the study protocol. All participants provided written informed consent before any study procedures. Blast-mTBI Veterans and deployed control Veterans were recruited from Veterans receiving care at VA Puget Sound through presentations to providers who referred potential participants, through flyers posted at VA Puget Sound, and by word of mouth. Non-Veteran civilians as well as Veterans were recruited by posting flyers in the community in venues such as fitness centers and coffee shops.
Lifetime history of both blast and impact TBI were obtained from all Veterans and civilians through a semi-structured interview performed simultaneously by two expert TBI clinicians that queried lifetime head injuries by any mechanism. For Veterans with mTBI, detailed histories of the most severe blast-mTBIs, with respect to acute loss or alteration of consciousness symptoms, were obtained. In the non-TBI groups, neither Veterans nor civilians had history of head injury meeting American Congress of Rehabilitation Medicine (ACRM)/VA/DoD criteria for TBI of any severity. Inclusion criteria for the blast-mTBI Veteran group included history of deployment to Iraq and/or Afghanistan in Operations Enduring Freedom/Iraqi Freedom/New Dawn (OEF/OIF/OND) and at least one war zone blast or combined blast/impact exposure resulting in two or more symptoms meeting ACRM criteria for mTBI. Any lifetime history of moderate or severe TBI was exclusionary.
Control participants had no lifetime history of TBI of any severity and included Veterans who had been deployed to any of the OEF/OIF/OND combat theaters (DC) as well as community civilians with no history of military service (CC). These groups were combined, as there were no significant differences between them with regard to our primary measure of study (i.e., left pallidum [18F]FDG-uptake) and age. DC participants were matched to mTBI Veterans by age, birth sex, and years of military service. CC participants were matched by age and birth sex. The study was open to any gender, but only male participants enrolled. Exclusion criteria for all groups was history of seizure disorder, insulin-dependent diabetes, current or past diagnosis of schizophrenia or other psychotic disorder, bipolar disorder, dementia, or alcohol or other substance use disorder diagnosis within the 3 months before study enrollment.
mTBI assessments
TBI histories were obtained from blast-mTBI Veterans through a semi-structured interview performed simultaneously by two TBI expert clinicians that queried total number and severity of lifetime head injuries of any mechanism and associated acute PCS, with detailed characterizations for the most severe five blast exposures. 14
Motor, neuropsychological, and behavioral evaluations
All study participants underwent the same neurological, neuropsychological, and behavioral evaluations. The Unified Parkinson’s Disease Rating Scale (UPDRS) motor subscale 30 was performed by a study clinician as part of the neurological exam, as parkinsonian motor signs have been observed in patients with repetitive mTBI and chronic traumatic encephalopathy (CTE) 31 and mTBI has been associated with a 56% increased risk for Parkinson’s disease. 32
As part of the neuropsychological evaluation, all participants completed the Behavior Rating Inventory of Executive Function-Adult Version (BRIEF-A) 33 and the Frontal Systems Behavior Scale (FrSBe). 34 The BRIEF-A includes two indices of global executive function, the Behavioral Regulation Index (BRI) and the Metacognition Index (MI). The BRI provides a measure of the ability to appropriately regulate one’s behavior and emotional responses. Specific BRI subscales include Inhibit, Shift (cognitive flexibility), Emotional Control, and Self-Monitor. The MI is a measure of one’s ability to generate ideas and initiate action, organize and plan approaches, monitor outcomes, and appropriately adjust problem-solving strategies. MI subscales include Initiate, Working Memory, Plan/Organize, Task-Monitor, and Organization of Materials. The BRIEF-A Global Executive Composite (GEC) score is a summary measure that incorporates all of the BRIEF-A BRI and MI subscales. Results for any of the elements of the BRIEF-A are reported as age-adjusted T-scores using transformations of the raw data to evaluate an individual’s scores relative to a standardization sample. Previous research has shown that there is an association between number of prior mTBIs and level of symptom endorsement on the BRIEF-A. 35
The FrSBe is a self-report measure used to quantify behavioral problems associated with frontal lobe damage. 34 The FrSBe includes Apathy, Disinhibition, and Executive Dysfunction subscales and a Total Score, which is then corrected into age, education, and gender-adjusted T-scores. The FrSBe has been shown to have ecological validity, including being predictive of level of performance of activities of daily living among individuals with a range of neurological disorders. 36 Among individuals with TBI, elevated FrSBE scores have been associated with aspects of neuropsychological test performance 37 as well as EEG abnormalities. 38 The FrSBe Total T-score was used in this study as a second assessment of self-reported executive function.
Working memory was assessed using the 18-second subscale of the Auditory Consonant Trigrams (ACT) 39 test and prospective memory was assessed using the 15-min delay and Time Cue subscale scores from the Memory for Intentions Test (MIST). 40 Age-adjusted T-scores for the ACT and age and education-adjusted percentile scores for the MIST are used in the analyses. These specific subscales were chosen for analyses based on their sensitivity to the effects of blast-related mTBI. 15,41 In addition, all participants were administered the Test of Memory Malingering (TOMM) to assess performance validity. 42 All participants included in this sample performed above published cutoffs for valid performance on the TOMM, suggesting that their neuropsychological test performance is an accurate representation of current cognitive abilities.
Post-traumatic stress disorder (PTSD) symptoms in control and mTBI participants were evaluated with the PTSD Checklist-Military version (PCL-M); 43 although the PCL-5 was released after our study began, we maintained use of the PCL-M for consistency. Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI), 44 alcohol use with the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), 45 and symptoms of depression with the Patient Health Questionnaire-9 Item (PHQ-9). 46 All of these are self-report instruments.
Acquisition and preprocessing of [18F]FDG-PET imaging data
Imaging was performed at two sites using the same tracer administration and data reconstruction protocols. A standard resting 15-min brain PET acquisition was performed following a 60-min tracer uptake period after intravenous injection of 8–10 mCi of [18F]FDG, with participants resting awake in a dimly lit room. Images were acquired using a GE Advance PET scanner (GE Medical Systems, Milwaukee, Wisconsin), which has in-plane and axial resolutions of 5 mm and 3 mm (full-width-half-maximum [FWHM]), respectively, with a 25-min germanium-68 transmission scan for attenuation correction, or a Philips Gemini PET/CT, which has in-plane and axial resolutions of 2 mm and 2 mm FWHM, respectively, with a low-intensity CT for attenuation correction. Ordered subset expectation maximization (OSEM) was used for data reconstruction.
Three 5-minute frames were averaged following motion correction, smoothed with a 3D Gaussian filter at 8x8x8 mm resolution, and transformed directly into Montreal Neurological Institute standardized space using the Della Rosa PET phantom 47 with pixel interpolation in SPM12. Individual images were scaled for intensity using a volume of interest (VOI) applied to parenchyma (equivalent to standardized uptake value ratio, SUVR, to whole brain) or intensity-scaled uptake (unitless) as the outcome value. 48
Image analysis
Images meeting quality control standards were evaluated together. To control for potential differences in spatial resolution and attenuation correction inherent in images acquired on the two different scanners, images were conservatively smoothed two to three times the axial resolution FWHM (6 mm), using statistical parametric mapping 12 (SPM12). Images were analyzed in the nonparametric toolbox (SnPM; http://warwick.ac.uk/tenichols/snpm), which implements a single-tailed test, using age as a covariate, and adjusted significance value (paired Family Wise Error, pFWE-corrected <0.025, equivalent to t-score >5). To eliminate potential confound of camera differences in image-based outcomes, voxelwise analyses are reported only using images obtained from the same camera. An exploratory voxelwise assessment of combined image sets covaried by camera was performed.
Coregistered, spatially smoothed, and intensity-scaled whole brain [18F]FDG-PET images were regionally segmented using the automatic anatomical labeling (AAL2; 120 regions) atlas library of PMOD (PMOD Technologies, Switzerland). To identify brain regions affected by blast-mTBI, VOIs were extracted from individual images using a standard atlas, segmenting images into discrete neuroanatomical regions yielding averaged intensity-scaled radioactivity within the volume. To assess for potential bias from different PET cameras, VOI-based outcome measures were assessed between groups by camera.
Statistical analyses
Statistical analyses were conducted in SPSS (version 26; SPSS Inc., Chicago, IL) or the statistical software R [version 4.1.2 (2021-11-01)]. Values are expressed as mean ± SEM unless otherwise stated. A two-tailed p-value <0.05 was considered to be statistically significant, and p-values between multiple comparisons were false discovery rate adjusted. 49 Two-tailed analysis of variances are used where noted.
Validation analyses were performed for each scanner using statistical parametric mapping 12 (SPM12). These images were analyzed on a voxelwise basis using SPM12 with 6 mm smoothing in the nonparametric toolbox (SnPM; http://warwick.ac.uk/tenichols/snpm), which implements a single-tailed test, using age as a covariate, and adjusted significance value (pFWE-corrected <0.025, equivalent to t-score >5).
Statistically significant differences in [18F]FDG-uptake among whole anatomically defined functional brain regions were identified between the Veteran blast-mTBI and control groups using an agnostic 1% false discovery rate-adjusted approach. To evaluate the diagnostic performance of greater [18F]FDG measures for discriminating participants with blast-mTBI from controls, we used receiver operating characteristic curves (ROCC) to establish the derived accuracy index (i.e., area under the curve; AUC) and likelihood ratio (LR). ROC analyses are widely used to determine diagnostic performance of blood biomarker candidates and imaging measures in the classification of dichotomous outcomes such as diseased versus healthy persons. 50 –52 The LR is a combined index of sensitivity and specificity and represents the ratio of the true positive rate to the false-positive rate.
Mediation of [18F]FDG-uptake measures associated with deficits in measures of executive function for blast-mTBI versus control participants were evaluated using a nonparametric method with validation by bootstrapping with the Mediation package in R. Mediation assesses the statistical probability that an intermediate variable drives the primary statistical relationship. For validation, indirect effects (with 95% confidence interval) were computed for 10,000 bootstrapped samples.
Results
TBI and clinical measures
Participant characteristics, including demographics, TBI history, and results of motor, neuropsychological, and behavioral assessments are provided in Table 1. A total of 79 Veterans with blast-mTBI and 41 controls, comprising 29 DC Veterans and 12 CC civilians, were included in this study. Demographic information was obtained by self-report. There was no significant difference in age between the blast-mTBI and the pooled control group (mean ± standard deviation [SD] years; age range), 34.7 ± 9.5 (22–60) and 33.0 ± 8.9 (20–59), respectively. The 79 blast-mTBI Veteran participants reported 28.6 ± 3.4; 1–100+ (mean ± SEM; range) blast exposures resulting in acute symptoms of mTBI with 2.3 ± 0.3; 0–12 (mean ± SEM; range) episodes of loss of consciousness. The most recent blast exposure was 5.4 ± 0.3 years; 0.5–12.1 (mean ± SEM; range) before [18F]FDG-PET imaging. Control groups significantly differed with respect to PTSD symptom severity (DC: 27.0 ± 2.3, CC: 18.7 ± 0.5; p = 0.019).
Participant Characteristics
A, Asian; AUDIT-C, Alcohol Use Disorders Identification Test–Consumption; B/AA, Black/African American; BRIEF-A GEC, Behavior Rating Inventory of Executive Function (Adult Version) Global Executive Composite; LOC, loss of consciousness; MOS, Military Occupational Specialty; mTBI, mild traumatic brain injury; O, Other; PCL-M, PTSD Checklist–Military Version; PET, positron emission tomography; PHQ-9, Patient Health Questionnaire-9; PSQI, Pittsburgh Sleep Quality Index; W, White.
Regional differences in brain [18F]FDG-uptake in the Veteran blast-mTBI group compared with the control group
Of 120 brain regions evaluated, seven met our criteria for significant groupwise differences. Five of the seven areas showed significantly greater [18F]FDG-uptake in the blast-mTBI versus control participants, with high-confidence differences observed in the left pallidum (blast-mTBI: 0.9042 ± 0.0058; control: 0.8397 ± 0.0068, p < 0.0001; q = 3.29 × 10

Discovery analysis comparing [18F]FDG regional brain uptake in the Veteran blast-mTBI group (n = 79) to the non-TBI control group (n = 41 [29 DC, 12 CC]). CC, community control; DC, deployed control.
Left pallidum [18F]FDG-uptake is highly correlated with the number of blast-mTBIs
To investigate the potential dose dependency between the degree of pallidum [18F]FDG-uptake and the number of blast-mTBIs, we performed linear regression analyses to evaluate for any correlation between the number of self-reported symptomatic blast-mTBIs and pallidum [18F]FDG-uptake in the Veteran blast-mTBI group. Given the wide range in the number and frequency distribution of blast exposures, we used a log scale (log10[number of blast-mTBIs + 1]), which enabled us to include all participants in the statistical linear regression analyses. A general linear relationship was observed between the number of blast-mTBIs and left, right, or averaged bilateral pallidum [18F]FDG-uptake (Fig. 2a, b, c). We focused further analyses on the left pallidum because of the strength of these findings. The number of blast-mTBIs experienced with the most recent mTBI occurring a mean of ∼5.4 years before the [18F]FDG-PET brain imaging for this study accounted for 21% of left pallidum [18F]FDG-uptake variability (Fig. 2a; r2 = 0.21, p < 0.0001). The relationship between left pallidum [18F]FDG-uptake and the number of blast-mTBIs remained statistically significant after controlling for common covariates using multivariate linear regression (log scale number of blast exposures, p = 0.038; motor signs [UPDRS total score], p = 0.40; PTSD symptom severity [PCL-M total score], p = 0.031; age, p = 0.040; sleep quality [PSQI total score], p = 0.75; overall model F[5, 96] = 10.11, p < 0.0001; adj. r2=0.31). These results support a dose dependency in left pallidum [18F]FDG-uptake related to the number of blast-mTBIs, a finding that is robust to the effects of age, sleep quality, motor signs, and comorbid PTSD symptoms.
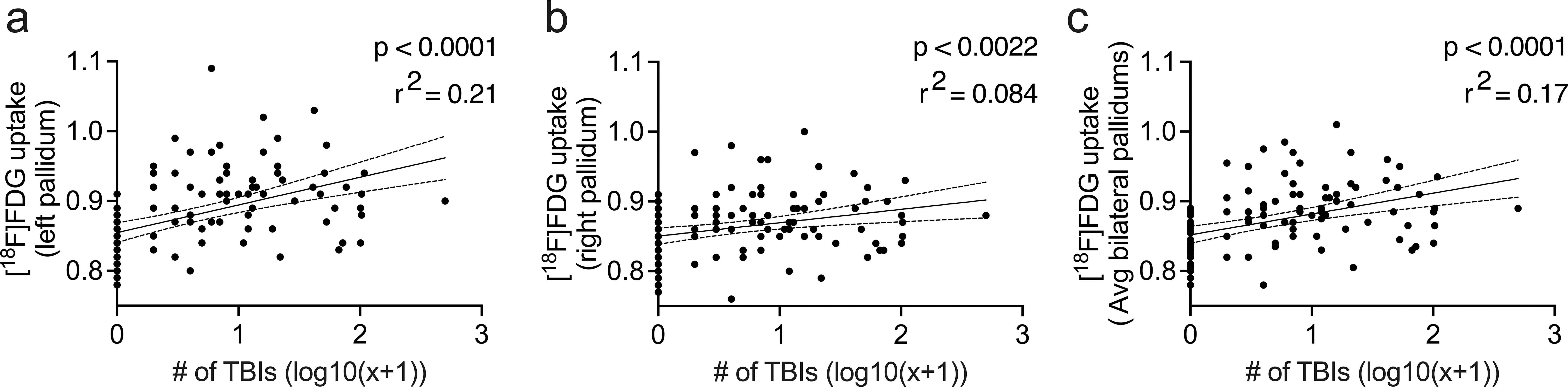
Average pallidal [18F]FDG uptake versus log10[number of blast-mTBIs +1] in the blast-mTBI Veteran group. Linear regression models demonstrate a positive correlation between [18F]FDG uptake and number of symptomatic blast-mTBI exposures in the
Greater left pallidum [18F]FDG-uptake discriminates blast-mTBI from control participants
Region-specific patterns of brain [18F]FDG-uptake can be of diagnostic utility in differentiating Alzheimer’s disease, dementia with Lewy bodies, frontotemporal dementia, and cerebrovascular impairment, and have been reported in Parkinson’s disease, 53 stroke, TBI, 26 and other conditions. 54 –56
Greater [18F]FDG-uptake in the left pallidum provided good-to-excellent discrimination between Veterans with blast-mTBI and control participants, with an ROCC-AUC of 0.859 (p < 0.0001; Fig. 3a). ROCC-AUCs for right pallidum and averaged bilateral pallidum uptake were 0.700 (p = 0.0002) and 0.809 (p < 0.0001), respectively (Figs. 3b, c).

ROCs and AUCs for
Diagnostic biomarkers can guide “rule in” medical conditions when positive LRs are >10-fold. 57 An analysis of specificity and sensitivity was conducted to determine whether pallidum [18F]FDG-uptake thresholds yielded LRs >10. The LR for Veterans with blast-mTBI was well above 10; Veterans having left pallidum [18F]FDG-PET intensity scaled values ≥0.895 uptake were ∼21 times more likely to be correctly categorized (Fig. 3d). LRs for right and averaged bilateral pallidum [18F]FDG-uptakes did not reach the >10 threshold difference (Figs. 3e, f).
Greater left pallidum [18F]FDG-uptake in Veterans with blast-mTBI is not related to motor function or handedness
Neuroimaging studies with functional magnetic resonance imaging (fMRI) and magnetoencephalography demonstrate that cortical and subcortical outcome measures may lateralize depending on a person’s dominant handedness. 58,59 Therefore, we examined whether lateralized [18F]FDG-uptake in the pallidum covaried with dominant handedness to ascertain whether the observed changes may reflect potential neural adaptations related to handedness or alterations in conserved circuits unrelated to handedness. Dominant handedness information was available for 39 of 41 control and 77 of 79 blast-mTBI participants. In left-handed control participants, no difference between left or right pallidum for [18F]FDG-uptake was found (t[5] = 1.348, p = 0.2354; Supplementary Fig. S1a, left panel). This contrasted with left-handed blast-mTBI Veterans in whom significantly greater left pallidum [18F]FDG-uptake was observed (t[10] = 4.777, p = 0.0007; Supplementary Fig. S1a, right panel). Similar observations were made in right-handed participants, with no lateralization in controls (t[31] = 0.463, p = 0.6468) and greater [18F]FDG-uptake in the left versus right pallidum in blast-mTBI Veterans (t[58] = 6.971, p < 0.0001; Supplementary Fig. S1b). Therefore, greater left pallidum [18F]FDG-uptake in Veterans with blast-mTBI does not covary with dominant handedness. In ambidextrous individuals, lateralization was not observed (control n = 1; blast-mTBI t[6] = 1.737, p = 0.1331; Supplementary Fig. S1c]. Lastly, a multivariate adjusted linear regression analysis using UPDRS total score with left pallidum [18F]FDG-uptake was not statistically significant.
That neither motor function nor handedness was significant in accounting for increased pallidum [18F]FDG-uptake in Veterans with a history of blast-mTBI suggests possible involvement of nonmotor domains, such as behavior or cognitive function.
Behavioral dysregulation is mediated by increased left pallidum activity in blast-mTBI
The BRIEF-A was administered in control and mTBI groups to comprehensively assess normative deficits across broad domains of executive function. To do this, the BRIEF-A assesses separate indices of behavioral regulation (BRI) and metacognition (MI) to comprise a GEC, with higher scores reflecting greater impairment. BRIEF-A results and their component subscales are provided in Supplementary Figure S2. The GEC T-score was significantly higher in the mTBI group: control versus blast-mTBI 51.8 ± 3.0 versus 68.1 ± 2.3, t(64) = 5.18, p < 0.0001. Veterans with blast-mTBI had similarly significantly elevated T-scores on both BRI and MI. These results support that participants with a history of blast-mTBI endorse broad executive dysfunction.
We next identified which self-reported executive difficulties were correlated with left pallidum [18F]FDG-uptake using linear regression analyses. After adjusting for multiple comparisons, the BRIEF-A GEC T-score, as well as the BRI T-score and each of its component subscales were significantly associated with increased [18F]FDG-uptake in the left pallidum. These results are summarized in Table 2. Within the MI domain, only the Planning/Organization subscale remained statistically significant after adjusting for multiple comparisons. Therefore, greater uptake of [18F]FDG in the left pallidum is linearly related to global self-reported executive difficulties associated with blast-mTBI and apparently driven by changes in the behavioral regulation domain. This contrasts with the metacognitive executive functions related to blast-mTBI, which generally lacked significant associations with left pallidum [18F]FDG-uptake.
Normalized BRIEF-A Scales Versus [18F]FDG-Uptake in the Left Pallidum
Statistically significant q-values (<0.05) appear in bold.
[18F]FDG, [18F]fluorodeoxyglucose; BRIEF-A, Behavior Rating Inventory of Executive Function (Adult Version); FDR, False Discovery Rate Adjustment (reported with adjusted p-values [q-Value]); LRM, linear regression model.
Altogether, these data support a model where blast-mTBI leads to greater left pallidum [18F]FDG-uptake, which in turn associates with chronic self-reported difficulties in executive function. To test this hypothesis, we performed a statistical mediation analysis with bootstrap validation to evaluate the relationship between blast-mTBI, left pallidum [18F]FDG-uptake, and self-reported executive function, assessed using the BRIEF-A GEC T-score. Following bootstrap validation, the adjusted causal mediation estimate (ACME) of left pallidum [18F]FDG-uptake to mediate the effects of blast-mTBI (log scale) on impaired self-reported executive function was significant (ACME: β = 4.5 [range 0.6–10.5], p = 0.021; Fig. 4a). However, the direct effect of blast-mTBI on the BRIEF-A GEC score lost significance upon adjustment (direct effect estimate [DE]: initial β = 6.0, p = 0.044; adjusted DE [ADE]: β = 1.5 [range −6.4to 9.7], p = 0.67). Thus, in this statistical model, chronic self-reported difficulties in global executive function are predominately mediated by changes in left pallidum [18F]FDG-uptake in individuals with a history of blast-mTBI exposure (total effect estimate of model [TE]: β = 6.0 [range 0.3–13.6], p = 0.039).

Multiple executive dysfunctions linked by causational analysis to blast-mTBI are mediated by increased left pallidum [18F]FDG uptake. Path analysis diagrams for causal mediation analyses with dependent variables
We performed an identical analysis evaluating the potential mediation between left pallidum [18F]FDG-uptake and elevated behavioral regulation index (BRIEF-A BRI; Fig. 4b). We did not evaluate the BRIEF-A metacognition index (MI) since our regression analyses of left pallidum [18F]FDG-uptake predicted broad changes in BRI and not metacognitive domains, which only showed association with planning/organization scores (summarized in Table 2). Following bootstrap validation, differences in behavioral regulation were similarly mediated by differences in left pallidum [18F]FDG-uptake in blast-mTBI participants (ACME: β = 3.4 [range 0.2–8.4], p = 0.032), with initial direct effects of blast-mTBI losing significance after adjustment (initial DE: β = 7.1, p = 0.013; ADE: β = 2.8 [−5.2to 9.4], p = 0.4). Therefore, differences in left pallidum [18F]FDG-uptake in blast-mTBI participants statistically underlay impaired behavioral regulation, as measured by the BRIEF-A BRI (TE: β = 6.2 [range 0.6–13.2], p = 0.032).
The FrSBe composite T-score was considered as a validation measure of self-reported executive function. The validated ACME and TE estimates were statistically significant (ACME: β = 4.5 [range 6.0–10.5], p = 0.021; TE: β = 11.0 [range 4.0–20.4], p = 0.0014; Fig. 4c), supporting the conclusion that frontal systems impairment, including self-reported difficulties in executive function, is mediated by changes in left pallidum [18F]FDG-uptake resulting from blast-mTBI.
To determine whether left pallidum [18F]FDG-uptake mediates cognitive/behavioral dysregulation through specific modalities, we performed mediation analyses across BRI subscales. These results are illustrated in Supplemental Figure S3 and summarize mediation analyses across BRI subscales and the Plan/Organize component of the MI domain. Mediation estimates for the BRI shift and emotional control subscales were statistically significant and summarized in Table 3. These results support the hypothesis that left pallidum [18F]FDG-uptake mediates self-reported difficulties in cognitive set-shifting and emotional control following cumulative blast-mTBI.
Validation Summaries for Mediation Relationships Between Left Pallidum [18F]FDG-Uptake and BRIEF-A Outcome Measures
Only subscores meeting FDR-adjusted significance thresholds in Table 2 were evaluated.
ACME, adjusted causal mediation estimate; ADE, adjusted direct effect estimate; BRIEF-A, Behavioral Rating Inventory of Executive Function (Adult Version); CI, confidence interval; FDR: false discovery rate; LRM, linear regression model; TE, total effect estimate.
Neuropsychological measures of working and prospective memory is negatively correlated with left pallidum [18F]FDG-uptake
Reduced working and prospective memory are often cited as distressing and disabling symptoms in Veterans with blast-mTBI and PPCS, and our research has demonstrated that these aspects of cognitive functioning may be particularly sensitive to the effects of blast-related mTBI. 15,41 Although the function of the pallidum in memory formation and retrieval is not as well understood as for other neuroanatomical regions, the pallidum has been shown to be integral for short-term memory formation within the corticobasal ganglia–thalamo–cortical loop. 60 In particular, suppression of, or lesions in, the pallidum can result in impaired short-term memory and reversal learning. 61 –64 Our [18F]FDG-PET analysis revealed that working memory, assessed using the 18-second subtest of the ACT test, 39 was negatively correlated with T-score-corrected outcomes in all participants (F[2, 68] = 4.762, p = 0.0116) and more strongly when blast-mTBI was included as a covariate (F[3, 67] = 12.75, p < 0.0001). Prospective memory, assessed using the MIST, 40 revealed that [18F]FDG-uptake in the left pallidum negatively correlated with the 15-min delay score in all participants (F[2, 67] = 4.242, p = 0.0184) and was more strongly correlated when blast-mTBI was included as a covariate (F[3, 66] = 13.54, p < 0.0001). [18F]FDG-uptake was also negatively correlated with time-cued scores in blast-mTBI Veterans (F[3, 66] = 13.29, p < 0.0001), a task that has higher executive functioning demands that other aspects of the MIST because of the need for self-monitoring 65 but not controls. These findings suggest that greater [18F]FDG-PET uptake in the left pallidum may reflect changes in memory and recall in persons with a history of blast-mTBI.
Discussion
We have identified the left pallidum as a brain region having significantly increased [18F]FDG-uptake in Veterans with a history of blast-mTBI and have found that the degree of [18F]FDG-uptake is proportional to the number of blast-mTBIs. We also found that these Veterans endorse a high level of executive dysfunction as reflected across a variety of BRIEF-A subscale T-scores, conferring face and construct validity, as these impairments represent substantial and often debilitating PPCS following blast-mTBI. The association of our primary finding has high sensitivity and specificity, as supported by a ROCC-AUC of 0.859 and demonstrates diagnostic potential, with a LR >10 for values of [18F]FDG-uptake ≥ 0.895. The association is robust to handedness, motor function, age, sleep quality, symptoms of depression, alcohol use, or PTSD symptom severity. Our findings are consistent and robust within our study group and our statistical modeling suggests that the relationship between blast-mTBI and increased [18F]FDG-uptake in the left pallidum mediates behavioral aspects of executive dysfunction. Further, our analysis supports that executive dysfunction following blast-mTBI is driven by processes that result in increased [18F]FDG-uptake in the left pallidum. Altogether, our findings support further study of pallidum dysfunction in blast-mTBI and consideration of increased [18F]FDG-PET in the left pallidum as a potential biomarker of blast-mTBI and PPCS.
This study was not intended to elucidate a molecular or neurobiological mechanism for the observed increased [18F]FDG-uptake in the left pallidum associated with blast-mTBI. Therefore, we cannot comment with certainty as to the cause of this finding and the reported associations. Increased regional uptake of [18F]FDG is understood to reflect increased local metabolic demand, which could be driven by neurons, glia, or both, and could reflect upregulation of glucose transporters, glycolysis, or both. Robust regional increases of [18F]FDG would presumably be driven primarily by neurons, as their metabolic demand is typically high and drives much of [18F]FDG retention in the brain. In conceptualizing mTBI in the spectrum of neurodegenerative disorders, a focal region of increased neuronal activity may seem counterintuitive. Prior analyses by our group17,18 and others 66,67 have typically focused on identification of regional deficits of metabolic or functional demand given that neuronal loss is a known consequence of mTBI, and that TBI is possibly the greatest environmental risk factor for dementia. However, the pallidum within the corticobasal ganglia–thalamo–cortical loop is rich with GABAergic interneurons and afferents, which, when disrupted due to neuronal injury or death, could result in a loss of inhibitory activity and result in an imbalance of excitatory activity. Excess excitatory activity mediated by glutamate or dopamine would, in turn, contribute to increased synthesis of those neurotransmitters with associated metabolic demand and a reduction of organized function of efferent projections—such as to the prefrontal cortex. In support of the possibility that blast-mTBI results in greater neuronal activity, we have previously reported that in a mouse model of blast-mTBI, blast exposure potentiates evoked phasic dopamine release in the nucleus accumbens, 19 a section of the basal ganglia’s ventral striatum that synapse in the pallidum. Conversely, greater pallidum neuronal activity could be a consequence of upstream loss of inhibitory regulation, such as in the prefrontal cortex due to injury resulting from blast-mTBI or thalamic afferents, which have been hypothesized as a confluent concentration of anterograde and retrograde Wallerian degeneration. 68
A relatively large positive difference in metabolic demand could arguably be driven by glia, as baseline metabolic demand of neurons is high and glia outnumber neurons in the pallidum at roughly 2:1. 69 As with neurons, glia contribute to the synthesis, release, and reuptake of glutamate, which could drive metabolic demand. As well, astrocytes and microglia are integral to neuroinflammation, which has been reported by our group and others following blast-mTBI. 18,70 –72 However, acute blast exposure likely exposes the entire brain to abrupt pressure-induced fluid density changes and increased hydrostatic pressure in the vascular column into the brain, which might be expected to yield a more diffuse injury pattern throughout brain. Perl et al. have suggested that density interfaces within brain, such as gray–white junctions, 73 might be more susceptible to axonal stretching and shearing during pressure wave dispersion and refraction, making those areas more prone to subsequent neuroinflammation. The pallidum is richly intermixed with gray and white matter, likely making it highly susceptible to neuroinflammation from this potential cause. Whether such inflammation reflects a persistent degenerative process versus ongoing, insufficient, or aberrant repair remains unclear and warrants investigation. Furthermore, robust glial activity could potentially contribute to the observed [18F]FDG-uptake increases more than deficits accounted for by neuronal loss, thereby masking the interpretation of neuronal loss as assessed by [18F]FDG-PET in the face of mixed pathology.
Localized increase of [18F]FDG in the pallidum may reflect a functional or compensatory response to neurophysiological deficits following blast-mTBI. Executive dysfunction, characterized by behavioral dysregulation and impaired metacognition, is common following TBI. 74 Executive function requires the refinement of multiple cortical and subcortical inputs to produce optimal, contextually appropriate output behaviors. As part of the basal ganglia, the pallidum is the final prethalamic output to the cortex influencing final behavioral output. Among executive functions, deficits in emotional control, cognitive flexibility, behavioral inhibition, planning/organization, and memory are well-recognized outcomes of neurodegenerative disease and trauma affecting corticobasal ganglia–thalamic circuits. 75 –77
The ventral pallidum receives projections from limbic striatum and sends projections to limbic and frontal regions and therefore is likely involved in cognitive, emotional, and memory functions, while the dorsal pallidum receives projections from nonlimbic striatum and sends projections to the motor cortex and therefore is likely integrated within motor function. While the resolution from our imaging study and the preprocessing filters utilized limit our ability to reliably distinguish ventral from dorsal pallidum, the significant correlations of our data with behavioral but not motor outcomes suggest our finding is driven by activity (indicated as increased [18F]FDG-uptake) in the ventral pallidum. Within basal ganglia–thalamo–cortical circuits, the ventral pallidum provides feedback about downstream signaling outcomes. 78 Nonmotor domains of the pallidum include executive function, verbal memory, and self-efficacy. 79 Lesions to the ventral pallidum lead to deficits in these domains as well as abulia, loss of emotional expression, reduction of spontaneous thought content, and disinhibition. 62,80 Individuals who have sustained mTBI, including the blast-mTBI Veterans in our study, often report that performing routine cognitive activities requires increased effort, which can be fatiguing, frustrating, and debilitating. 81,82 Given the role of the ventral pallidum in learning, information processing, and self-efficacy, our finding may reflect its neuroplastic potential as a compensatory measure for widespread neuronal injury. Taken together, we propose that blast-mTBI exposure leads to general neuronal injury, requiring increased metabolic resources and demands upon the ventral striatum to achieve desired functional and cognitive outcomes by affected individuals.
Why are these results strongly lateralized? While greater [18F]FDG-uptake was seen in both the right and left pallidum, our findings were strongly lateralized to the left. Evidence suggests that functional outputs from the basal ganglia may be lateralized across behavioral domains. Whereas the left executive circuits drive motivation and volitional motor and behavioral responses, projections from the contralateral (right) hemisphere have inputs that may attenuate these functions. 83 However, even though right lateralized pallidum [18F]FDG-uptake was elevated in the blast-mTBI Veterans, it did not significantly correlate with metacognitive deficits. Greater left pallidum volume on MRI has been reported in people with obsessive–compulsive disorder compared with controls 84 and in adolescents 85 and adults with 86 or at risk for 87 psychosis. In individuals with schizophrenia, greater blood flow to the left pallidum was observed compared with controls using PET-based methods, 88 and low pallidal–cortical connectivity was associated with lower functioning after six months on resting-state fMRI. 89 Video gamers and gamblers have been shown to exhibit increased gray matter, dopamine transporter density, and activity-dependent blood flow in left ventral striatum and/or pallidum. 90,91 In a cohort of elderly Chinese participants, pallidum volume was greater in those who used the internet, and in particular left pallidum volume on MRI was positively correlated with change of Mini-Mental Status Exam scores after one year, 92 suggesting that future studies of blast-mTBI should monitor changes in pallidum size as well as measures related to its metabolic activity and or regional blood flow.
There are several strengths to this study. First, we used an unbiased approach to identify differences in regional brain [18F]FDG-uptake having diagnostic potential for blast-mTBI and prognostic for its cognitive and executive functional outcomes. Second, we utilized a standard, nonarterially sampled clinical brain PET scan protocol using [18F]FDG, a readily available tracer. Third, our use of neuroimaging supports left pallidum [18F]FDG-uptake as an objective measure of brain function for persons with a history of blast-mTBI, given its strong ROCC-AUC finding. Currently, biomarker-based assessments for mTBI measure blood proteins, with the presumption that any observed concentration changes reflect coincident neurovascular injury, although significant peripheral sources of common assay targets, such as GFAP and tau, exist. In cases of comorbid body trauma, which often occurs in blast-mTBI, these peripheral sources may confound the interpretation and monitoring of TBI. Presumably, an imaging biomarker for mTBI would be more independent of peripheral effects. Therefore, we propose that left pallidum [18F]FDG-uptake may facilitate diagnosis, prognosis, and monitoring the response to treatment in persons with mTBI. Fourth, given that greater left pallidum [18F]FDG-uptake was observed in participants an average of over 5 years since their most recent blast-mTBI, this finding appears to inform a past history of blast-mTBI, although longitudinal studies are clearly needed to establish the decay constant as a function of time after injury. Finally, the stability of our finding between two different PET scanners supports the generalizability of this finding.
There are several limitations to this study. First, our assessment of the frequency and timing of blast-mTBIs is largely dependent on participant report and recollection of sometimes remote events and is therefore subject to recall bias. In an effort to reduce recall bias while ensuring the most accurate as possible TBI history, a semi-structured clinician interview performed simultaneously by two expert TBI clinicians to obtain consensus was used, results of the interview were correlated with available information in the medical record. Only blast-mTBI exposures with self-reported co-occurring acute symptoms meeting ACRM criteria for mTBI were considered as qualifying mTBI events. Importantly, in this study cohort we have previously reported the strong, statistically significant relationship between the number of self-reported blast-mTBI events with both objective measures of brain function and behavioral deficits related to military blast exposure and experimentally confirmed brain pathology caused by repetitive blast-mTBI in the suspect regions in a mouse model of blast-mTBI. 18 Second, participants with blast-mTBI in this study may have endured one or more lifetime impact mTBI either independently (e.g., unrelated military combat, military training, contact sports, and civilian accidents) or as a secondary or tertiary injury associated with blast-mTBI. History of impact mTBI is highly comorbid in individuals with blast-mTBI, and therefore clinically may be more practical to consider as a mixed exposure than blast-mTBI in isolation. Our available data do not enable definitive dissection of the primary finding associated with blast-mTBI independent from impact mTBI; however, these data demonstrate a strong “dose–response” of the number of blast-mTBIs to our finding, and is found in comparison to a group with no lifetime history of any TBI. Third, while we have demonstrated our primary finding is independent of multiple comorbid conditions, and mediation analyses suggest attributability between blast-mTBI, behavioral symptoms, and the imaging finding, we cannot rule out the possible contribution of common comorbidities in the mTBI group on our primary outcome. Future studies utilizing a control group with such comorbidities without history of blast-mTBI could be considered, although common comorbidities with blast-mTBI and PPCS might have overlapping or dependent etiology 93 and might not be independently represented by physiological or psychiatric pathologies in a control group without blast-mTBI. Fourth, our assessment and results are cross-sectional and therefore draw upon correlations and associations for the primary findings. We have assumed that greater left pallidum [18F]FDG-uptake in Veterans with blast-mTBI and PPCS did not predate their blast-mTBI exposure and that under premorbid conditions, our blast-mTBI and control cohorts were similar on imaging and other assessment measures. Because [18F]FDG-PET brain studies preceding blast-mTBI exposure are unavailable, whenever possible we have attempted to control for potential confounding variables and adjusted for multiple comparisons and we have performed a bootstrap-validated mediation analysis, which demonstrates the strength of the connectedness of our findings. Fifth, our decision to use clinical [18F]FDG-PET scan protocols limits the full potential of our interpretations. By using static scans, we lack a full kinetic analysis to quantitatively characterize the cerebral metabolic rate of glucose (CMRglu) consumption and other parameters. We have assumed that correlations between intensity scaled regional uptake values approximate the interpretation provided by CMRglu, without the invasiveness of arterial modeling in our participants. Sixth, our neuropsychological assessments might be influenced by confounding factors difficult to control. For example, prior research suggests that scores on the ACT test can be confounded by years of education, impulsivity, and symptoms of depression. 39 However, we have attempted to control for these variables as much as possible by using available normative data and, consistent with the standards of clinical neuropsychology, incorporating a measure of performance validity in this assessment battery. Seventh, to reduce intersubject variability and systemic variability by using PET scanners of differing resolution while preserving primary group differences, we have applied a filter with a moderate spread function. The use of such a filter may contribute to spillover activity from adjacent regions of interest, for example the putamen or mixed subregions of the basal ganglia. Our approach to identifying a potential imaging biomarker is not dependent on accurately delineating a particular brain region but rather its consistent identification between groups. Lastly, the inclusion of civilians in the control group could be considered a limitation. Although we combined the deployed control Veterans and civilians to form the non-mTBI control group, there are important differences between deployed control Veterans and civilians with respect to selection biases for military service, military training experiences, and exposure to the stresses (including combat PTSD) and potential toxic exposures of the Iraq and Afghanistan war zones even without experiencing TBI. Approximately half the deployed control Veterans were in combat Military Occupational Specialties (MOSs) and half in administrative and support MOSs. In contrast to the deployed control Veterans, civilian controls did not have a lifetime history of PTSD or more than mild symptoms of depression. However, despite these participant differences, regional [18F]FDG-uptake in the left pallidum in civilian controls did not differ from that in the deployed Veteran controls.
Our results were generated from an observational cohort study using an unbiased approach and without an a priori hypothesis, and therefore additional research is warranted to strengthen, validate, and deepen the understanding of our findings. Our findings are compelling on a groupwise basis, but to assess if increased [18F]FDG-PET uptake in the left pallidum is a reliable clinical biomarker, a single-subject-to-control-cohort analysis will be required and would be strengthened by comparison to findings for common comorbid disorders. Complementing our metabolic imaging with advanced structural and functional imaging may be useful to assess possible underlying pathophysiological mechanisms. In addition, we have proposed that neuroplasticity may underlie our region-specific finding. Intraindividual imaging changes over time correlated with cognitive outcomes may support this assertion. Should our finding of elevated [18F]FDG-uptake in the left pallidum be confirmed as a reliable biomarker of blast-mTBI exposure, potential applications include gauging an individual patient’s blast-mTBI exposure burden for disability assessment purposes; evaluating long-term change in left pallidum or other regional [18F]FDG-uptake patterns with serial assessments to characterize the evolution of post-mTBI effects; determining whether changes in left pallidum [18F]FDG-uptake would be useful for monitoring response to treatment.
Conclusions
In this study, [18F]FDG-uptake in the left pallidum is significantly greater in Veterans with blast-mTBI compared with control participants and demonstrates high sensitivity and specificity in distinguishing those groups. The regionally restricted increased uptake correlates with the number of symptomatic blast-mTBIs and mediates the relationship between blast-mTBI number and broad domains of executive dysfunction. Our results provide proof of principal that [18F]FDG-PET neuroimaging, available across civilian, military, and Veterans Affairs health care settings, may facilitate diagnosis and dosimetry of blast-mTBI exposure. Validation studies are warranted to reliably identify Veterans with blast-mTBI and PPCS as distinguished from common co-occurring conditions and mechanistic studies are warranted to identify potential therapeutic targets to address the often-disabling consequences of blast-mTBI.
Transparency, Rigor, and Reproducibility Summary
The Veterans Affairs “mTBI and Biomarkers of Neurodegeneration” study (2008–2023) was not preregistered at clinicaltrials.gov because of its start date preceding such requirements. The analysis plan was conducted in accord with unbiased and declared multiple comparison-adjusted discovery-focused methods. The original power/sample size analysis for the study of 50 participants per group was based on detecting an effect size (difference in population means at baseline between the two groups divided by population standard deviation at baseline) of 0.57 with 80% power, and an effect size of 0.65 with 90% power, using a two-sided 5% Type I error. As noted in the Discussion section, we have already reported statistically significant differences at baseline between groups in neurological, behavioral, neurocognitive, neuroimaging, and cerebrospinal fluid biomarker outcomes. 15,41 A total of 153 potential participants were screened, PET imaging data were obtained from 119, and successfully analyzed in 119. Participants were not told the results of any study assessments. Imaging acquisition and analyses were performed nonblinded, by team members having prior knowledge to relevant characteristics of the study participants. Clinical outcomes were assessed by team members blinded to imaging results. All equipment and software used to perform imaging and preprocessing are widely available from commercial sources or as freeware as described in the Methods section. The key inclusion and exclusion criteria are as previously described in detail in the Methods section. Outcome measures are established as discussed in the study methods. The study group is seeking additional funding for replication and validation. Deidentified data from this study are available upon approved written request. Analytic code used to conduct the analyses is similarly available upon written request. This article will be published under a Creative Commons Open Access license, freely available at https://www.liebertpub.com/loi/neu upon publication.
Footnotes
Acknowledgments
The authors acknowledge the support of the VA Puget Sound Research & Development Service Seed grant program (J.S.M.), the University of Washington Friends of Alzheimer’s Research (E.R.P.), and the Northwest Network Mental Illness Research Education and Clinical Center (J.S.M., E.R.P., G.E.T., C.L.M.). This study was supported by the Assistant Secretary of Defense for Health Affairs and Department of Defense, through the FY22 Traumatic Brain Injury and Psychological Health Research Program Translational Research Award (W81XWH-22-TBIPHRPTRA), under Award Number HT94252310755 to J.S.M. issued by the U.S. Army Medical Research Acquisition Activity. The contents herein represent the authors’ views and are not strictly endorsed by the U.S. Government or the Department of Veterans Affairs (VA). The study abstract was previously summarized and published as a poster abstract for the American College of Neuropsychopharmacology’s 62nd Annual Meeting. 94
Authors’ Contributions
G.T.: Methodology, validation, formal analysis, investigation, data curation, writing—original and revised drafts, writing—reviewing and editing, and visualization. K.F.P.: Methodology, validation, formal analysis, and investigation. M.M.: Methodology and formal analysis. C.M.: Writing—original draft. D.R.M.: Project administration. A.G.S.: Conceptualization. T.L.R.: Methodology, software, and formal analysis. C.M.E.: Conceptualization. A.C.: Conceptualization. C.M.N.: Conceptualization. G.M.: Conceptualization. P.M.: Conceptualization. J.R.P.: Conceptualization. J.P.M.: Conceptualization. R.G.T.: Methodology, software, and formal analysis. M.A.R.: Conceptualization. E.R.P.: Funding acquisition, data acquisition, resources, supervision, methodology, validation, formal analysis, writing—reviewing and editing, and writing—revised draft. J.S.M.: Funding acquisition, supervision, visualization, methodology, validation, formal analysis, investigation, data curation, writing—original and revised drafts, and writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist for any of the authors.
Funding Information
J.S.M. and A.G.S. received funding from the VA Office of Biomedical Laboratory Research & Development (J.S.M.,
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.