
Abstract
Cervical spinal cord injury (SCI) results in significant sensorimotor impairments below the injury level, notably in the upper extremities (UEs), impacting daily activities and quality of life. Regaining UE function remains the top priority for individuals post-cervical SCI. Recent advances in understanding adaptive plasticity within the sensorimotor system have led to the development of novel non-invasive neurostimulation strategies, such as spinal cord transcutaneous stimulation (scTS), to facilitate UE motor recovery after SCI. This comprehensive review investigates the neuromotor control of UE, the typical recovery trajectories following SCI, and the therapeutic potential of scTS to enhance UE motor function in individuals with cervical SCI. Although limited in number with smaller sample sizes, the included research articles consistently suggest that scTS, when combined with task-specific training, improves voluntary control of arm and hand function and sensation. Further, the reported improvements translate to the recovery of various UE functional tasks and positively impact the quality of life in individuals with cervical SCI. Several methodological limitations, including stimulation site selection and parameters, training strategies, and sensitive outcome measures, require further advancements to allow successful translation of scTS from research to clinical settings. This review also summarizes the current literature and proposes future directions to support establishing approaches for scTS as a viable neuro-rehabilitative tool.
Introduction
Spinal cord injury (SCI) disrupts neural transmission, resulting in sensorimotor deficits at and below the injury level, including upper extremity (UE), lower extremity, and trunk. Approximately 60% of total SCI cases in the United States are cervical SCI, 1 which significantly impacts an individual’s ability to perform daily activities and impacts independence and quality of life. Recovery and prognosis of UE function post-cervical SCI are limited, and evidence is scarce. 2 Recent discoveries of adaptive plasticity within the sensorimotor system challenge the notion that the spinal cord is non-modifiable after SCI. 3,4 This in turn has led to the rapid development of promising, novel activity-based recovery training (ABRT) strategies aimed toward augmenting natural motor recovery after SCI. 5 –10 Further, recent evidence from pre-clinical and clinical research provides compelling evidence that the neurorehabilitation potential of ABRT strategies can be further potentiated using spinal cord stimulation via invasive epidural spinal cord stimulation using continuous (scES) 8,11 –13 or spatial-temporal approaches. 14,15 Although extremely promising, the invasive nature of epidural stimulation and the associated risks could potentially limit accessibility to patients with SCI for clinical translation and long-term rehabilitation. 16,17 Moreover, given that, similar to epidural stimulation, spinal cord transcutaneous stimulation (scTS) can target the spinal cord circuitry activating motor neuronal pools 18 and putatively exert its effect mostly via activation of posterior root structures 19,20 has opened a novel therapeutic window for the treatment.
Delivering scTS involves electrical stimulation using a unique waveform that accesses neuronal structures in the spinal cord without causing discomfort. 21 scTS to the thoraco-lumbar region has shown effectiveness in facilitating stepping-like activity, weight-bearing abilities during over-ground walking, reducing spasticity, and improving trunk control. 22 –26 scTS to the cervical region, in conjunction with task-specific training, has demonstrated efficacy in modulating UE motor and sensory outputs. 27 –32
Although initial reports provide evidence that applying scTS to the cervical region can facilitate motor and sensory recovery in individuals with SCI by enhancing spinal network excitability, optimizing training-specific parameters is crucial for effectively translating the utility of scTS from research into clinical practice. In particular, these studies lack clarification on critical aspects, including selection criteria for the optimal cervical site(s), optimal scTS parameters, training progression, and the therapeutic effectiveness of scTS in individuals with varied degrees of cervical SCI. Therefore, we present a comprehensive review to critically appraise existing literature, identifying existing gaps, and propose future directions for effective translation of scTS for UE recovery after cervical SCI from research to clinical facilities. This review focuses on the neural control of UE function, functional deficits post-SCI, natural recovery, stimulation parameters (intensity, frequency, and stimulation location/sites), single versus multi-site stimulation, and potential mechanisms of recovery with a multi-modal approach combining scTS + task-specific training post-cervical SCI. Further, the review addresses factors requiring attention in future clinical trials to understand scTS effectiveness in restoring UE function post-cervical SCI.
Neural Control of UE Function
In an intact nervous system, the spinal cord sensorimotor network continuously interacts with various neural entities located in the central and peripheral nervous system to ensure the successful execution of a motor task. More precisely, cortical neurons relay movement-related information via physiologically relevant descending spinal tracts, primarily the corticospinal (CST) and rubrospinal tract (RuST), to motor neurons located in the gray matter of the spinal cord via monosynaptic connections. These spinal motor neurons then project as spinal nerves or motor axons to innervate appropriate muscle groups involved in a motor task execution. 33 Further, in addition to the descending pathways, sensory and proprioceptive feedback from peripheral structures, such as muscle spindle fibers and Golgi tendon organ, significantly contributes to the refinement of the UE motor control. Sensory information from the peripheral structures ascends to the spinal cord level through sensory neurons in the dorsal root ganglion. These neurons establish mono or di-synaptic connections with the motor neurons in the ventral horns, as well as with interneurons projecting to the other interneurons in the same or adjacent spinal levels. In addition, ascending sensory information travels to the sensory nuclei in the thalamus via ascending tracts such as the spinothalamic and lemniscal pathways. The thalamic nuclei, in turn, establish connections with the primary sensory cortex. 34 This multi-level and bi-directional motor and sensory connection, along with feedback from the cerebellar connections, continuously evaluates the surrounding environment and enables necessary adaptations to the employed motor strategies 35,36 (Fig. 1). Indeed, SCI research involving rodents, non-human primates, and humans indicates the fine integration of the ascending and descending pathways along the spinal cord sensorimotor network for the successful execution of goal-directed voluntary motor tasks. 37 –40
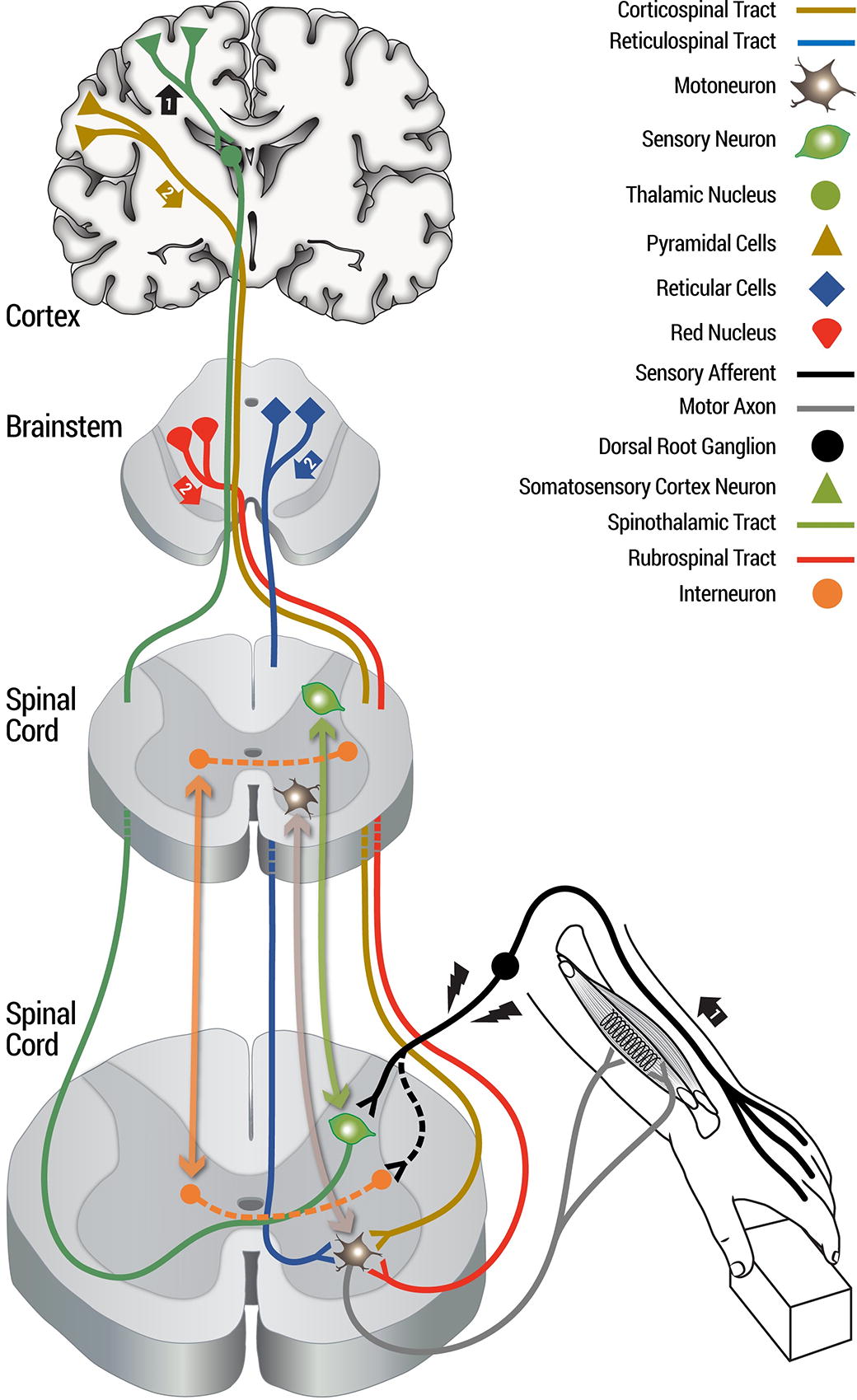
Schematic of neural control of UE function. (1) Action potential generated due to sensory stimulation travels via axon of the peripheral sensory organs to the spinal cord and establishes contacts with sensory neurons located in the dorsal gray matter. The action potential further travels up via the spinothalamic tract (green) to reach the thalamus. The sensory information is finally relayed to the cerebral cortex. (2) After integration of the sensory information at the cortex, a motor command is sent from the frontal cortex and brainstem via the corticospinal tract (brown trace), reticulospinal tract (blue trace), rubrospinal tract (red trace) to the motor neurons located in the gray matter of the spinal cord. The motor axon (gray) emerges from the motor neuron and connects to a muscle through a neuromuscular junction to cause contraction of the target muscle. Motor neurons, sensory neurons, and interneurons located at the same and different spinal cord segments establish multi-level and bidirectional motor and sensory connection to enable required sensorimotor network control required for neural control of UE function (bidirectional light brown, light green, and orange arrows). UE: upper extremity.
In addition to the neural structures mentioned above, the successful execution of complex motor tasks, such as reaching and grasping, heavily relies on the fine integration between motor neurons, propriospinal neurons (PSNs), and the interneuronal spinal circuitry. Seminal experiments conducted on cats and monkeys involving selective ablation of the CST and RuST at the C5 spinal level, while preserving the C3-C4 PSNs, provide compelling evidence regarding the relative contribution of PSNs to these motor tasks. Following an initial period of severe UE impairments, these species demonstrate viable intracellular recording from the motor neurons, indicating action potential transmission to the motor neurons, potentially via PSNs, along with a subsequent recovery in reaching function. 41 –43 As spontaneous long-distance regeneration of spinal cord pathways is absent in humans, spared descending neurons sprout to establish collateral connection with the PSNs and innervate denervated spinal targets. 44,45
UE Motor Deficits and Limited Recovery After Cervical SCI
Extensive longitudinal studies examining motor deficits and natural recovery of UE function in cats, rats, non-human primates, and humans post-cervical SCI consistently report severe debilitating effects on functional capacities and limited motor recovery (Fig. 2). Following the initial weeks of severe impairments in motor abilities after cervical SCI, cats and monkeys demonstrate variable rates of motor function recovery, depending on the site and severity of the injury. More importantly, in both species, reaching movements can still be achieved with impaired precision and coordination. 41 –43 Rats display comparable motor deficits and recovery patterns after experiencing SCIs of different severities at the C5 spinal level 46,47 (Fig. 2). Similarly, humans following C5-C6 SCI exhibit modest recovery of certain UE functions, such as reaching activities, attributed to the preservation of shoulder and elbow flexion innervated by the C5-C6 spinal segment. However, fine motor tasks, such as grasping and manipulating objects, remain more significantly affected. 48 Neuroimaging techniques further support a poor prognosis for sensorimotor recovery in individuals with extensive cervical spinal cord damage. 2,49,50 The severity of the injury, as evident from the loss of spinal cord cross-sectional area and the level of injury, significantly influences sensorimotor recovery after SCI, with cervical SCIs associated with particularly poor prognosis, especially when complete loss of sensory and motor function occurs below the injury level. 2
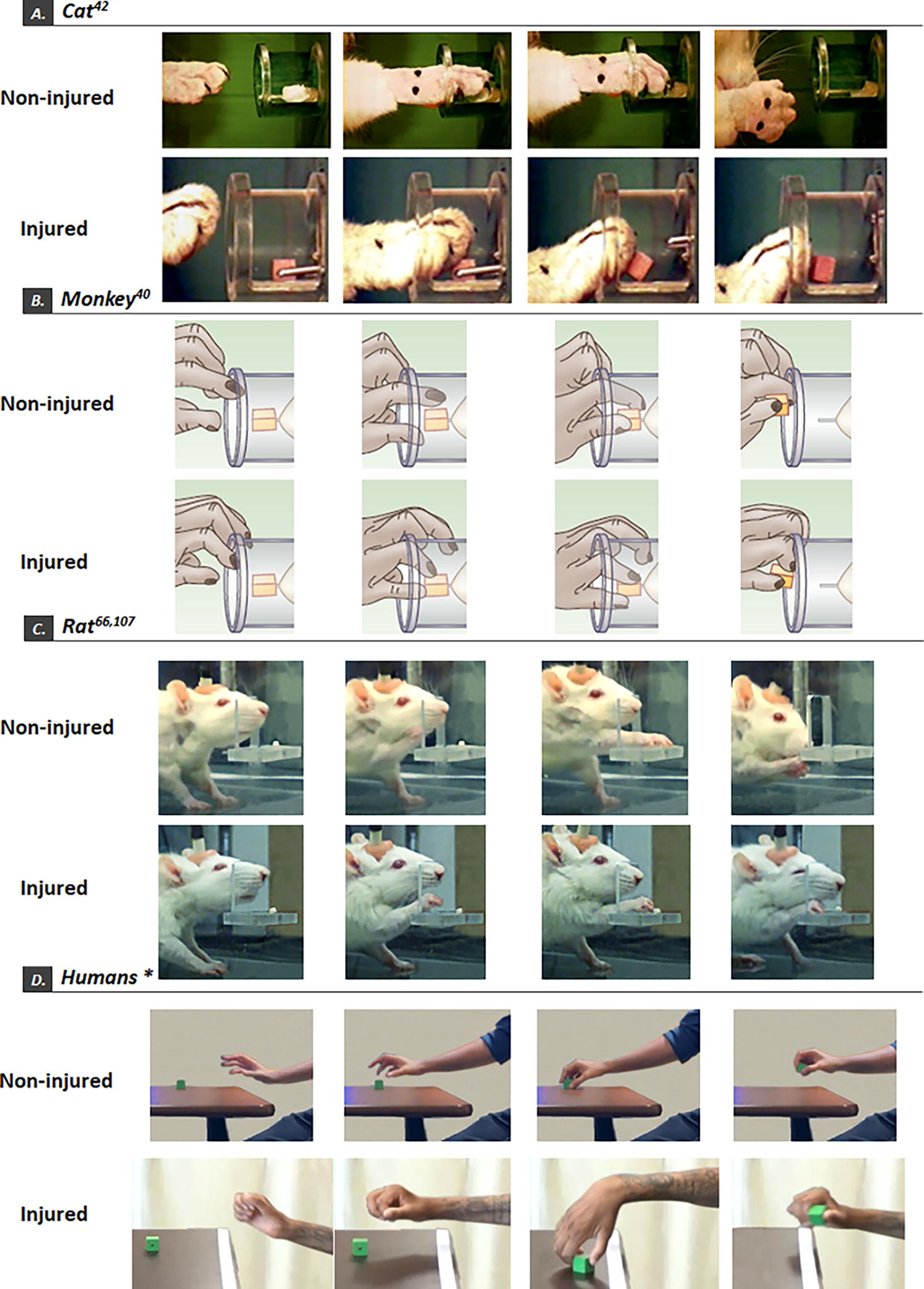
UE motor deficits across different species following cervical SCI. Shown are the reaching and grasping movement sequences in non-injured and C5 SCI (
Conventional Motor Rehabilitation Strategies After Cervical SCI
Motor training is crucial for promoting functional recovery in individuals with SCI by enhancing mobility, strength, and coordination. 51,52 Restoring arm and hand function is essential for performing daily activities and achieving independence. Traditional physical therapy interventions for individuals with SCI encompass a variety of strategies, including targeted exercises to strengthen the remaining muscle groups, stretching to preserve joint integrity, and compensatory strategies to facilitate activity of daily living. 52 Collectively, research findings suggest that control groups receiving education only or no motor training report no significant changes in motor functions compared with groups receiving motor training targeting lost UE motor functions. 52 However, despite the effectiveness of these approaches in enhancing motor function, recovery remains slow and limited. 30,53 Recent advancements in neuro-rehabilitation have shifted the focus toward promoting neuroplasticity and recovery of neuromuscular activity both below and above the level of injury. 54,55 Task-specific or activity-based motor training approaches have emerged as effective methods, activating the injured nervous system through repetitive sensory input to the spinal network. 54,55 This approach aims to facilitate the retention and recovery of specific motor tasks, harnessing the potential of the nervous system to reestablish connections and regain function. These findings underscore the potential for the nervous system to reestablish lost neuronal connections and regain function through targeted rehabilitation interventions. A large proportion of individuals with cervical SCI face considerable challenges when it comes to performing activities of daily living, with gaining UE function often ranking as their top rehabilitation priority. 56,57 Therefore, task-specific training, which centers on enhancing gross and fine motor skills through repetitive training, holds the potential to significantly improve functional independence for individuals with SCI. By targeting specific tasks and engaging in repetitive practice, individuals can regain or improve their ability to perform essential activities, fostering a greater sense of autonomy and independence.
Methodology
Search strategy
For this review, a comprehensive search was conducted in the PubMed database to identify relevant articles. The eligibility criteria for inclusion in this review were as follows: (1) studies involving adults with cervical SCI and (2) studies examining the application of scTS to the cervical region and task-specific training to improve UE deficits or facilitate recovery. The search was focused on the following keywords: transcutaneous spinal cord stimulation, non-invasive spinal cord stimulation, neuromodulation, cervical SCI, UE deficits, and task-specific training. The search encompassed articles from the inception up until July 30, 2023. After evaluating the abstracts, the articles that met the required inclusion criteria were retrieved in their full-text version. The identified articles underwent a thorough data extraction process. To ensure accurate citation and eliminate duplicates, the search results were imported into EndNote, a reference management software.
Participants Clinical Characteristics
A total of 55 participants (40 males) with cervical SCI participated in studies investigating the therapeutic effects of scTS to the cervical region to improve motor function post-cervical SCI. Six participants had motor complete SCI, with each participant injured at or above the C8 spinal cord level. The participants’ demographics and clinical characteristics from the identified studies are presented in Table 1.
Demographic and Clinical Characteristics of Participants in the Selected Studies
Only 15 participants received spinal cord transcutaneous stimulation (scTS) combined with robot-aided upper extremity training. The total sample size for the study was 22.
AIS, ASIA Impairment Scale.
scTS Site Selection and Parameters to Improve Motor Outcomes
All 10 studies examined the combined use of scTS and task-specific training to UE motor functions. 27 –32,58 –61 In 8/10 studies, the active electrode (cathode) placement for stimulating the cervical spinal cord varied across studies, ranging from C3-C4 to C7-T1 vertebral levels with the passive electrode (anode) placed over the iliac crest, bilaterally. In the remaining two studies, only one stimulating electrode was placed at the C5 vertebral space with the passive electrode over the iliac crest. 29,61 The selection of stimulation sites was based on two major factors: (1) overlaying the region above, at, or below the level of injury and (2) stimulation sites resulting in greater activation of the paralyzed or hypoactive UE muscles as evident from the obtained electromyography (EMG)-evoked potentials. In one study, in addition to the cervical electrodes, T11-T12 placement was also used to stimulate the thoracolumbar spinal cord region, aiming to promote a upright sitting posture and increase cervical spinal cord network excitability 60 (Fig. 3 and Table 2).

Commonly employed scTS parameters and therapeutic effectiveness of scTS to facilitate UE recovery post-cervical SCI. (
Study Design, Electrode Location, Stimulation Parameters, Motor Rehabilitation Intervention, Used Outcomes, Major Findings, and Follow-up Period Employed in the Selected Studies
GRASSP, Graded and Redefined Assessment of Strength, Sensibility, and Prehension; WHO-QOL, World Health-Organization-Quality of Life; SCIM, Spinal Cord Independence Measure; ARAT, Action Research Arm Test; UEMS, upper extremity motor score, EMG; electromyography; SCI-QOL, Spinal Cord Injury—Quality of Life; CUE-Q, Capabilities of Upper Extremity-Questionnaire; CUE-T, Capabilities of Upper Extremity Test; SCIM, Spinal Cord Independence Measure; VAS, Visual Analogue Scale; ASIA, American Spinal Injury Association; MAS, Modified Ashworth Scale; BBT, Box and Block Test; FNPA, Functional Neurophysiological Assessment; NRS, Neurorecovery Scale.
The intensity at selected stimulation sites varied across different studies, ranging from 10 to 160mA in eight studies, 27 –32,60 whereas two remaining studies did not report the intensity used. 58,59 The selection of stimulation intensity was based on various factors across the studies. Four studies utilized a range of intensity that facilitated hand contraction during maximal handgrip task with no discomfort to participant. 27 –29,31 In contrast, others adjusted intensity based on patient feedback during type of tasks such as strength versus motor skill training. 30,32 Regarding the type of current selection, eight studies reported using rectangular waves, with waveform selection either biphasic 31,58,60 or monophasic 28,32,59 or both. 27,30 However, one study used sinusoidal biphasic pulses, 61 and one study did not report the waveform used for stimulation. 29 Only one study provided the rationale for using monophasic and biphasic stimulation with monophasic to facilitate strength and biphasic to train fine motor tasks. 30 Although biphasic current has been shown to reduce the risk of tissue damage and evoke the required motor response, pulses with carrier frequency, also called Russian currents, were employed to further reduce the risk of tissue damage. 62,63 In eight of the studies, a carrier frequency of 5 or 10 kHz was used in combination with a burst frequency ranging from 5 to 30 Hz. 27,28,30 –32,58 –60 However, one study used 50 Hz stimulation 61 and one of the studies did not provide any information on modulation, despite using the same burst frequency range 5–30 Hz. 29 In nine studies, the stimulation was delivered at the cathode electrode using a 1-ms pulse width, 27 –32,58 –60 whereas in the remaining study, 0.5-ms pulses were used. 61
Task-Specific Training Combined with scTS
The training program in some of these studies involved task-specific training to improve voluntary hand contraction during grip strength, grasping objects with a variety of shapes and weights, fine motor tasks such as pinch grip, and practicing the release of small objects of different sizes. 27 –30,32 To ensure that participants continued to challenge themselves and make progress, the training intensity was progressively increased by either increasing the task difficulty level or by increasing the number of repetitions. 30,32,60 In the rest of the studies, standard physical therapy, including stretching, assisted range of motion, overhead press, and motor manipulative exercises, was included as part of the training component with and without stimulation. 31,59 However, in one study, participants performed isometric elbow extension against a custom-designed board, 61 while in another study, participants underwent training with a robotic exoskeleton and scTS focused on reaching and grasping, and hand opening and closing tasks. 58
Functional, Clinical, Neurophysiological, and Quality-of-Life Outcomes
Improved hand function on GRASSP, grip-strength, and CUE-T functional outcomes
Seven studies utilized the Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) as the primary functional outcome measure to evaluate the effectiveness of scTS combined with task-specific training on UE motor recovery. 28,30 –32,58,60,61 All seven GRASSP-based studies reported a significant increase in scores following the intervention, indicating improved functional performance. Three out of these seven studies and two additional studies employed grip strength, as an additional functional outcome measure. 27 –29,32,58 Moreover, the two studies measuring grip strength demonstrated post-intervention improvements when scTS was combined with task-specific training. Notably, one study exclusively assessed and reported positive enhancements in the Capabilities of Upper Extremity Test (CUE-T). 59 Further, four studies evaluated lateral pinch strength 30 –32,58 and consistently demonstrated significant improvements in both left and right lateral pinch force following training with scTS. In addition, one of these studies reported notable enhancements in tip-to-tip, lateral key, and total prehension ability bilaterally, further highlighting the positive impact of scTS on fine motor control and overall prehensile capabilities following cervical SCI. 58
Improvements in other functional outcomes
In addition to GRASSP, Freyvert et al. reported significant improvement in hand function, as evaluated by the Action Research Arm Test, post-intervention. 29 Tefertiller et al. utilized the Nine-Hole Peg Test to quantify finger dexterity and reported improvements in scores for every participant who completed the test. 59 Further, García-Alén et al. reported a significant enhancement in the Box and Block Test scores for both the control (scTS) and experimental (robotic + scTS) groups. 58
Reduction in spasticity
Two studies investigated the effects of training with scTS on spasticity using the Modified Ashworth Scale (MAS). Inanici et al. reported a notable average decrease in MAS scores of 3.5 for the group, indicating reduced spasticity levels. 30 Similarly, Huang et al. found that the combination of stimulation and buspirone tended to decrease the overall spasticity as measured by the MAS and the visual analog scale, and also reduced the occurrence of spasms, which was assessed by the Penn Spasm Severity/Frequency Scale. 28
Improved motor and sensory function on ASIA assessment
The severity of SCI was evaluated and quantified using the American Spinal Injury Association (ASIA) assessment in all ten conducted studies. Three studies utilized the UE motor score (UEMS). 27,29,59 Freyvert et al. reported a substantial 7-point improvement (group) in UEMS post-intervention for the group assessed. 29 Gad et al. found that four out of six participants displayed UEMS improvements of 1 or 2 points (either right or left), with only one participant experiencing a notable 4-point increase bilaterally. 27 In the study by Tefertiller et al., four out of seven participants demonstrated significant UEMS enhancements of 5, 7, and 11 points. Interestingly, the remaining three participants, two experienced a decrease in motor score, one reported no change, and two reported a decrease in sensory score after the intervention. 59 Four studies utilized the ASIA Impairment Scale to assess both motor and sensory functions. 28,30,31,59 Inanici et al. reported an improved neurological level of injury from C3 to C4 in one patient following the application of scTS combined with training. 31 Further, in their subsequent study, all six participants demonstrated improvements in their overall neurological level of injury and sensation bilaterally after undergoing 4 weeks of UE training with stimulation. 30 Huang et al. found that individuals with limited residual hand motor function who received a combination of buspirone and scTS experienced improved sensory scores for light touch and pinprick, although motor scores did not exhibit significant changes. 28 In a separate study, four out of seven participants who received functional task-specific training for UE in combination with scTS reported improved motor scores. 59 These findings highlight the potential for improved motor and sensory outcomes on ISNCSCI-recommended ASIA evaluation when training is combined with spinal cord stimulation. It could be suggested that training alone may be responsible for improvements in motor and sensory outcomes. However, previous studies have not reported significant improvements in hand motor function without stimulation. In addition, patients with chronic SCI typically show minimal to no recovery of motor function. 64,65 Interestingly, Inanici et al. found that training alone did not improve hand motor function, but after four subsequent weeks of training with stimulation, participants showed improved hand motor function and performance. 30,31 Similarly, Freyvert et al. demonstrated that a combined approach facilitated the recovery of hand function in patients with chronic SCI, as training alone did not lead to significant improvement in function. 29 Therefore, a combinatorial approach of stimulation with task-specific training can promote substantial recovery of hand function in patients with chronic SCI.
Altered spinal cord network excitability evident from spinal cord-evoked potentials
Four studies examined changes in spinal cord-evoked potentials following training. 27,31,32,60 Inanici et al. observed a progressive increase in the amplitude of short latency and reemergence of long latency responses, specifically in the right opponens pollicis muscle after the training compared with the baseline. 31 Gad et al. reported an increase in spinal-evoked responses in distal arm muscles, while demonstrating a decrease in evoked response amplitude in proximal muscles, such as the biceps brachii, after the intervention. 27 Another case study demonstrated increased spinal-evoked potentials in both proximal and distal muscles, particularly in early and late latency responses following intervention. 32 These neurophysiological findings suggest that scTS combined with training modulates spinal network excitability and allows remodeling of the intersegmental neural pathways responsible for the reemergence of the polysynaptic late responses, potentially leading to functional improvements post-SCI. 37,66
Improved quality-of-life measures
Regarding the assessment of quality of life, four studies employed the Spinal Cord Independence Measure III questionnaire. These studies reported increases in self-care score by 1 point, 31 4 points for the group, 30 and an overall score improvement of 20 points for the group, 28 and a 3-point increase for the group. 58 Further, three studies utilized the World Health Organization-Quality of Life-Brief questionnaire, 30,31,58 with findings indicating a 1-point increase in social relationships, 58 a significant improvement of 19 points in psychological well-being and physical health domain for the group, 30 and a 3-point enhancement in the physical health domain. 58 In addition to the aforementioned findings, Inanici et al. also observed improvements in bladder function, assessed as part of the quality-of-life measurement using SF-Quavean. 31 Huang et al. also reported enhancements in the Capabilities of Upper Extremity Questionnaire score, providing insights into participants’ functional levels post-intervention. 28 These results underscore the positive impact of the intervention on various aspects of quality of life, including self-care, social relationships, psychological well-being, and bladder function.
Durability of motor outcomes
Four studies assessed the durability of improved motor outcomes after the cessation of intervention to explore the long-term carryover effects of scTS on UE functional recovery. 28,29,31,32 Among these studies, two included a 3-month post-follow-up period. Inanici et al. reported that the improvements in GRASSP scores and lateral pinch strength were maintained during the follow-up period. 31 Freyvert et al. observed sustained improvement in hand grip force for three participants. These improvements in grip strength were accompanied by a significant increase in EMG amplitude in the biceps brachii, wrist flexors, and extensor muscles. 29 Zhang et al. conducted follow-up assessments at three time-points (1, 2, and 3 months post-intervention) for one participant. 32 The functional gains in strength and prehension ability on the right side were maintained compared with the left side. In addition, the gains in hand grip strength were sustained for both the left (11–73% above baseline) and the right hand (233–250% above baseline). The functional task improvements measured using the Neuromuscular Recovery Scale were maintained throughout the 3-month follow-up period. Huang et al. reported that three out of five participants with residual hand force at baseline, maintained improvements in hand function for up to 5 months post-intervention. 28 However, the remaining seven participants did not demonstrate changes in the hand grip force during the follow-up period. These findings highlight the potential for sustained improvements in motor function following scTS combined with task-specific training, but also suggest individual variability in long-term outcomes.
Safety and adverse effects
Studies investigating the neuro-rehabilitative effects of spinal cord stimulation strategies have recognized the significance of documenting and reporting on safety measures. In the studies highlighted in this review, researchers monitored and documented adverse events linked to scTS to the cervical region. Among the nine studies examined, six studies explicitly documented and reported on the safety and adverse effects associated with stimulation. 30 –32,58 –60 Notably, in the studies conducted by Inanici et al. in 2018 and 2021, participants tolerated the stimulation well, with anticipated hyperemia occurring under the stimulation site of the neck, which resolved within 5–10 min. Hyperemia or skin redness was the most reported adverse event and was anticipated due to scTS-induced local chemical changes at the skin level during stimulation. No other significant adverse effects related to scTS were observed throughout the training and experiment sessions. 30,31 Similarly, Zhang et al. and Tefertiller et al. reported no serious unexpected adverse events that impeded participants from continuing with their training. 32,59 In the study conducted by Garcia-Alen et al., two out of 15 participants reported a worsening of UE spasticity. In addition, one participant experienced a feeling of nausea, while two others reported coughing during stimulation. Notably, two participants also experienced episodes of autonomic dysreflexia during stimulation. To address and mitigate these adverse events, the stimulation intensity was promptly reduced, and continuous follow-up was conducted to monitor emerging symptoms. 58 Although the available data on participants who experienced autonomic dysreflexia with stimulation are not comprehensive, it is clear that further details are needed to draw firm conclusions on the association between stimulation and incidences of autonomic dysreflexia. It is also important to identify any history of autonomic dysreflexia, typical signs and symptoms, medication, and how to monitor these symptoms from patients’ medical records to ensure proper care. Therefore, it is important to take appropriate measures when optimizing or intervening by increasing the stimulation intensity. Specifically, caution is warranted while utilizing scTS to ensure that the benefits of the intervention are not outweighed by any potential risks.
Mechanisms of Action
SCIs are rarely complete and the residual neural circuitry establishing supralesional control over the sublesional neural circuitry can be reinforced using scTS resulting in sensorimotor recovery post-SCI. 27,29,67 Below, we discuss the potential mechanisms contributing to the UE sensorimotor recovery following scTS application (Fig. 4).

Schematic of the potential mechanisms of scTS for UE functional recovery. Primary sensory afferent (black) arising from the muscle controlling a motor action is recruited by scTS (lightning symbols) and generated action potential is relayed to the motor neuron directly or via interneurons (orange dots). Due to synaptic connections of motor neurons with various spinal network structures, such as corticospinal tract (blue), reticulospinal tract (blue), and serotonin system (green dot), scTS potentially alters the spinal cord network and supraspinal structure (cortex and brainstem) excitability. Corticospinal tract shares synaptic connections with inhibitory GABAergic neurons (red dots) responsible for pre-synaptic inhibition. Due to scTS interaction with interneurons (orange dots) via sensory afferent, scTS effects are exerted on the adjacent spinal segments. Improved spinal network and supraspinal structure excitability allow better integration (plus sign) of the ascending and descending neural inputs for volitional movement execution. Note that the schematic only illustrates mechanistic changes in one half of the spinal cord for ease of understanding. scTS: spinal cord transcutaneous stimulation; UE: upper extremity; GABA: gamma-aminobutyric acid.
scTS alters spinal cord network excitability
Experimental 18,20 studies and computational models 68,69 suggest that unmodulated low-frequency (0.2–2 Hz) scTS putatively exerts its effect mostly via activation of posterior root structures. More recent findings, such as (1) reduction in spinal cord-evoked responses during paired-pulse stimulation indicating toward post-activation depression (PAD) (classical hallmark for sensory fiber activation) 70 and (2) similar latency and morphology of the spinal cord-evoked responses with unmodulated and modulated scTS indicate that both forms of scTS potentially interact with large-to-medium-diameter sensory fibers located in the dorsal root afferent scTS. 71 Through sensory afferent connections with segmental motor neurons and interneurons via mono (type Ia), di (type Ib) polysynaptic (type II) pathways, sensory afferent’s repeated stimulation potentially modulates the membrane excitability of these structures. 72 Consequently, this altered membrane excitability results in excitation or inhibition of these neural structures. The increased neuronal excitability elevates the spinal cord into an optimal state, allowing weak or residual descending inputs to exert greater and more effective supraspinal control over the sensorimotor spinal network. 27,31,73,74 Recent findings, such as greater amplitudes of UE spinal-evoked responses and reemergence of long latency polysynaptic responses, support increase in the excitability of the spinal cord network following scTS combined with task-specific training. 27,31,75
In addition to the facilitatory effects, the inhibitory effect of repeated scTS on the membrane potential, particularly the PAD caused by a transient decrease in neurotransmitter release from Ia sensory terminals, 18,20 needs further exploration. Decreased neuronal excitability potentially results in improved motor activation by attenuating the deleterious effects of reflex hyperexcitability seen in individuals with SCI. 76 It is likely that scTS exerts both excitatory and inhibitory effects in a synchronized manner to allow motor function execution. However, the specific contributions and interactions of these mechanisms in augmenting functional recovery post-SCI remain largely unknown and require further investigation.
scTS alters pre-synaptic inhibition
Motor task execution also relies on the local inhibitory interneurons that shape the response to the diverse excitatory inputs from the supraspinal structures. 77 These interneurons have been found to form axo-axonic connections with the sensory afferents, and can regulate the sensory-motor drive via pre-synaptic inhibition through GABAergic action. 78 In addition to the sensory afferents, these interneurons are also known to share connections and regulate other neural entities, such as primary major descending pathways and local spinal neural circuitry, likely interacting with the scTS. More importantly, these interneurons hold prime importance in regulating the coordination between the agonist and antagonist muscles. Therefore, reemergence of the coordinated contraction of agonist–antagonist muscles can potentially be due to the altered pre-synaptic inhibition during natural or augmented motor recovery post-SCI. 79 Pre-synaptic inhibition of the monosynaptic responses is heavily dysregulated in individuals with SCI due to decreased supraspinal control. 80 Therefore, improved activation of inhibitory intraneuronal circuitry potentially plays a crucial role in reducing spinal hyper-reflexibility and improved motor function execution. 76 Moreover, improved pre-synaptic inhibition likely restricts the primary afferent transmission to spinal motor neurons and reduces motor neuron inadvertent activation. 81
scTS alters supraspinal structure excitability
Recent studies involving functional magnetic resonance imaging and electroencephalography recording from the cortical and subcortical regions of neurologically intact individuals during motor performance in the presence of scTS suggest immediate changes in the cortical sensorimotor areas involved in UE motor control. These changes suggest that scTS can likely neuromodulate supraspinal sensorimotor networks and facilitate effective integration of the ascending sensorimotor information at the cortical level. 82,83 Similarly, following scTS to the cervical region, increased amplitudes of motor-evoked potentials (MEPs) recorded from UE muscles have been reported, indicating improved activation of CST pathways innervating UE. 84,85 Apart from increasing the cortical activation, scTS is also known to improve the intracortical inhibition required to perform a coordinated motor task. 85 The biaxial neuromodulatory changes occurring at the supraspinal and spinal levels allow effective integration of ascending and descending neural information necessary for successful motor task execution. In addition, sensory improvements following scTS application likely indicate that the sensory pathways can be modulated with scTS leading to improved ascending sensory and proprioceptive inputs to the spinal cord, resulting in improved motor task execution. 28,30,31,86
Remodeling of the spared neural circuitry at the spinal cord level
Remodeling or establishing new neural detours between the supraspinal pathways and the spared neural circuitry below the injury level plays a crucial role in neural recovery following SCI. 87,88 Such anatomical adaptations enable uninterrupted flow of neural information between the cortex and distal end-organs. 44,89 In rats and non-human primates with complete or incomplete mid-thoracic SCI, CST axons sprout onto the long PSN, which in turn arborizes over the lumbosacral motor neurons resulting in improved locomotion and CST conduction across the injury site. 87,90 In addition, recent findings suggest the facilitatory effects of scTS to the cervical region combined with lumbosacral scES on voluntary control of stepping movements in individuals with SCI. 91 These findings highlight the pivotal role of spared neural structures, especially the PSN, in facilitating the effective reorganization of neural circuitry to bypass the injury site following an SCI. Recent findings from neurologically intact individuals suggest that a long PSN can be a potential target to accelerate the establishment of viable neural pathways to bypass the injury site and can facilitate the neural transmission from the supralesional to sublesional neural circuitry. 84,92 Moreover, as most cervical SCIs occur around C5 spinal level, the short PSN can be potentially neuromodulated to establish detours between the upper (C3-C4) and lower cervical (C7-T1) spinal cord to bypass the injury site and enable uninterrupted flow of neural information between the cortex and UE muscles.
Increased benefits combining scTS with task-specific training
Pre-clinical and clinical studies suggest that the combination of spinal cord stimulation and task-specific training results in greater activity-dependent neuroplastic changes for motor recovery post-SCI. 93 Indeed, in individuals with cervical SCI, greater changes in the UE motor function are observed when scTS is added to the task-specific training plan. 29 –31 Most likely, scTS combined with task-specific training potentially strengthens or accelerates the rate of establishment of the abovementioned neurophysiological or neuromodulatory changes resulting in UE functional recovery post-cervical SCI. 94,95
Future Directions
Stimulation site selection, optimization, and progression with training
Identifying the optimal number of stimulation sites and their locations is crucial in achieving effective targeting of the sensorimotor neuronal pool and resulting motor outcomes. 21,96,97 Future studies should provide a comprehensive rationale for the selection of stimulation site(s). The selection of the number of stimulation sites should consider factors such as target neural pathways, desired motor response, and individual patient characteristics. A thorough understanding of the underlying neural circuitry and its functional relevance to the motor outcome is crucial in guiding the decision-making process. In addition, future studies should employ rigorous methodologies and comparative analyses to evaluate the effectiveness of different stimulation site configurations, including frequency and pulse-width. By addressing these criteria and providing a rationale for selecting the appropriate number of stimulation sites, future research can further enhance our understanding of the optimal strategies for achieving positive motor outcomes. The studies highlighted in this review elucidate the application of rectangular currents, either in biphasic or monophasic configurations. The preference for these distinct waveforms stems from the understanding that biphasic waveform exhibits heightened tolerance to stimulation intensity due to its limited electrochemical polarization effect. Consequently, this characteristic permits the administration of higher current intensities with reduced discomfort, a benefit over monophasic waveform. 98 Nonetheless, there are limited studies investigating and comparing the effects of various waveforms on motor responses, and long-term safety and efficacy profiles are needed. Future studies should explore these parameters to improve waveform selection criteria for interventions targeted to improve UE motor function. Moreover, Sharma et al. demonstrated greater activation of UE muscles with anode over the clavicles compared with the iliac crest. 66 Future studies targeting UE motor recovery can potentially utilize similar cathode–anode electrode configurations.
The majority of studies highlighted in this review utilized subjective criteria to identify the optimal stimulation intensity during training. Researchers reported adjusting stimulation intensities based on subjective feedback from participants while performing selected motor tasks. Although easy to implement and user-friendly in nature, the absence of objective criteria for intensity selection poses a challenge for replicating the study in other research setup and clinical facilities, hence affecting clinical translation. Objective criteria are necessary to ensure standardization and could include factors such as muscle activation thresholds, sensory perception, tolerance, and/or motor performance measures. By incorporating objective measures, researchers and clinicians can establish clear guidelines for adjusting stimulation intensity based on the specific training tasks and observed motor improvements. As participants make progress in their training, it is essential to regularly re-assess and fine-tune the stimulation intensity and dosage. This adjustment should be based on both the training task requirements and the individual’s demonstrated motor improvements. This dynamic approach to intensity modulation allows for ongoing optimization and personalized treatment plans. To bridge this gap, future studies should focus on addressing these concerns by highlighting and providing objective criteria for the optimization and progression of stimulation intensity during training. Addressing these important factors will contribute to the refinement of neurotherapeutic interventions and ultimately improve the efficacy and precision of motor rehabilitation approaches.
Modulated versus unmodulated scTS
Unlike epidural stimulation, which is positioned closer to the target neural structure and involves lower stimulation intensities (2.5–20 mA), 8,13 scTS involves the delivery of relatively high-intensity stimulation (30–200 mA) via self-adhesive electrodes placed directly over the skin. 99 scTS readily activates cutaneous sensory fibers due to their lower activation thresholds and can result in unwanted sensations, such as tingling, burning, pain, and intense discomfort. More importantly, given that the average duration of scTS session can range between 30 and 120 min, 31,32 such discomfort can adversely affect the motor training execution and progression. To suppress sensory hyperactivation and to achieve greater stimulation intensities, modulated scTS is often utilized, involving stimulation pulses wrapped within 5–10 kHz carrier frequency, also known as Russian currents. 100 In neurologically intact individuals, modulated scTS at 5 kHz modulation allows stimulation delivery at 103 mA with no pain, while unmodulated scTS has a maximal tolerable amplitude of 39 mA. 71 Recent evidence suggests that at motor threshold levels, 10 kHz-modulated monophasic scTS requires more charge to evoke similar amplitude spinal cord responses compared with an unmodulated monophasic pulse. 70 The available scientific evidence is drawn from studies involving neurologically intact individuals. As pain and altered sensations are commonly reported by individuals with SCI, 101 the findings may not be directly generalized to this population.
Cervical–lumbar coupled stimulation for UE recovery
Delivering scTS to the lumbar spinal cord is likely to neuromodulate the cervical spinal cord due to long PSNs between the cervical and lumbar spinal cord, and likely holds potential in facilitating UE recovery post-cervical SCI. 45,75,96 Moreover, the neuromodulatory effects on the cervical cord might be more pronounced when scTS is delivered to the cervical and lumbar spinal cord simultaneously. Indeed, in healthy adults, simultaneous application of scTS to the cervical and lumbar region is known to facilitate the amplitude of the H-reflex in flexor carpi radials by 19.6% compared with scTS to the lumbar region alone that results in an 11.1% increase. In addition, simultaneous delivery of scTS to the cervical and lumbar region facilitates the amplitude of flexor carpi radials MEP compared with cervical or lumbar stimulation alone resulting in no change. 73,84 More importantly, the neuro-rehabilitative effects of this reciprocal organization between the cervical and lumbar spinal cord might be more pronounced post-SCI as pre-clinical studies suggest that PSN are known to establish more viable and effective connections resulting in motor recovery following an SCI. 45,87 Along the line, recent findings from our group demonstrated immediate improvements in the hand grip and wrist extension strength in the presence of scTS to the thoracolumbar and cervical region in the pediatric population with SCI. 102 Similar immediate improvements in the activation of the extensor carpi radialis muscle during wrist extension while delivering scTS to the lumbar spinal cord have been demonstrated in adults with complete cervical SCI. 60
In addition to the neurofacilitatory effects of scTS to the lumbar region on the cervical spinal cord, the neuromotor control exerted by scTS to the lumbar region on the trunk stability and upright sitting cannot be underweighted as optimal trunk control and upright posture are an essential substrate for the successful execution of the UE motor tasks. 103 –105 Recent findings suggest that scTS targeting the lumbar spinal cord along with repeated motor training is effective in enabling trunk stability by improving trunk muscle activation and limits of stability. 25,26,106 Therefore, therapeutic interventions incorporating cervical and lumbar cord-coupled stimulation could further potentiate the neurofacilitatory effects of scTS targeting cervical cord alone. Moreover, additional multi-modal or paired stimulation strategies, such as lateral electrode placement compared with the midline placement for greater UE muscle activation, 18 using closed-loop stimulation, 107,108 paired cortex and spinal cord stimulation, 109,110 and employing robot-guided motor rehabilitation strategies along with scTS to the cervical region, 58 are other emerging avenues that can be further explored to expand the therapeutic effectiveness of scTS in facilitating UE recovery post-cervical SCI.
Selection of intervention
Studies investigating motor function recovery in individuals with SCI have emphasized the importance of high-intensity rehabilitation protocols. 13,55 ABRT, particularly locomotor training, in combination with stimulation, has demonstrated its effectiveness in improving and restoring ambulation in individuals with SCI. 111 As the majority of research focused on recovering locomotion following an SCI, principles governing activity-based locomotor training have been well developed. In contrast, similar training principles for UE recovery have attracted limited attention. Moreover, the complexity of UE neural control, multiple joints with varying degrees of freedom, a wide range of motor tasks performed by UE, and the need to address the diverse motor skills learned before the injury, makes it even more challenging. Studies examined in this review employed diverse training protocols, including stretching, assisted range of motion exercises, overhead press, hand grip strength tasks, fine motor skills practice, and bimanual task performance. 27 –32,58,59 However, unlike lower limb training protocols, these interventions lack standardized principles based on neuroplasticity and recovery. 112 Therefore, future studies should prioritize the standardization of training protocols, incorporating the use of standardized objects to facilitate grip and fine motor task training. These standardized protocols will serve as valuable guidance for research trials investigating the efficacy of activity-based training, with or without stimulation, in individuals with SCI.
Patient selection and role of lower motor neuron injury in UE motor recovery
In addition to the major descending tract damage, such as the CST, commonly referred as upper motor neurons, SCI may also damage the lower motor neuron structures, such as motor neurons and spinal nerve. 101 A few longitudinal studies also demonstrate progressive death or degeneration of motor neurons around the lesion epicenter in chronic SCI. 113,114 In addition, cross-sectional studies have reported signs and symptoms related to lower motor neuron (LMN) dysfunction, such as muscle weakness and atrophy, in humans with SCI at and below the injury site. 115,116 Theoretically, without structurally intact LMNs at or below the injury site, spared long-axons motor tracts face significant challenges in establishing a functional neural pathway or detour to exert volitional motor control. 44,89,117 Indeed, newer evidence suggests limited motor recovery in individuals with associated LMN lesions following an SCI. 118 Provided that the scTS exerts its therapeutic effectiveness by increasing spinal network excitability via medium- to large-diameter sensory afferents, 19 damage of the spinal nerves and motor neurons might pose a greater challenge in facilitating motor and sensory recovery post-SCI. Overall, it becomes crucially important to investigate the intrinsic factors, such as LMN injury or extensiveness of the injury, and their potential role in dictating functional recovery to comprehensively understand the neurofacilitatory capacity of scTS to the cervical region in facilitating UE recovery post-cervical SCI.
Long-term safety implications
Adequate documentation and reporting the presence or absence of adverse effects are crucial in establishing the clinical safety and feasibility of the neurotherapeutic approach. In the case of scTS, it is imperative for future studies to address the long-term safety of applying scTS over skin and other physiological systems. Several studies have reported adverse effects such as skin irritation, hyperemia, increased spasticity, and in rare instances, autonomic dysreflexia. 30,31,58 To ensure the widespread therapeutic potential of scTS, it is essential that studies involving long-term stimulation at the same location thoroughly address and report the long-term safety implications of this technology. This includes assessing any potential risk or complication that may arise from prolonged exposure to stimulation at specific sites. Long-term safety assessments should encompass extended follow-up periods and rigorous monitoring of participants to identify any delayed or cumulative effects that may emerge over time. In addition, future studies should explore strategies to mitigate adverse events and optimize the safety profile of scTS. By addressing the long-term safety considerations associated with scTS, future studies can provide a comprehensive understanding of the technology’s safety profile and facilitate its effective and responsible implementation in clinical settings. This will enhance patient care and contribute to the advancements of scTS as an accessible and accepted neuro-rehabilitative intervention.
Extending therapeutic effectiveness beyond research
Most individuals following cervical SCI first resort to conventional motor rehabilitation strategies that include physical and occupational therapy targeting recovery of lost UE function. Conventional motor rehabilitation aims to facilitate the appropriate afferent inputs to the intact spinal cord to promote activity-dependent plasticity and facilitate motor recovery. 94,119 Although effective in enhancing hand function in people with tetraplegia, 120,121 the therapeutic effects are slow and functional regains remain limited. 30,53 Although limited in number, the discussed published work provides initial indications of scTS to the cervical region as a viable neuromodulatory tool that can be utilized by physicians, physical therapists, and occupational therapists targeting arm and hand function recovery post-cervical SCI. However, several aspects, such as optimal scTS parameters, motor rehabilitation strategies, outcome measures, and therapeutic potential, need to be explored in detail for effective clinical translation. Moreover, given the complexity of cervical SCIs, heterogeneity in the patient population, and recruitment challenges associated with SCI, a well-designed multi-central clinical trial is a demand of the time to gather scientifically grounded evidence to allow successful translation of this promising therapeutic tool from research setup to clinical settings. In addition, the non-invasive nature of scTS and easy-to-use feature make it a suitable neuromodulation device that can accelerate its translation to clinical practice for recovering UE function post-SCI.
Extending therapeutic benefits beyond SCI
Similar to SCI, other neurological diseases, such as stroke, cerebral palsy, multiple sclerosis, peripheral nerve injury, and spinal muscle atrophy, disrupt the normal functioning of major descending tracts (CST, Reticulospinal tract, RuST), and other neural structures along the brain–spinal cord axis. 35 This in turn severely affects the optimal integration of the ascending and descending information required for successful execution of motor functions. Given that sensory afferents in the posterior root structures activated via scTS establish direct or indirect connections with different neural entities along the brain–spinal cord axis, scTS can be used to induce optimal neuromodulatory changes to facilitate motor recovery following the abovementioned neurological diseases. Most likely, scTS improves the activation threshold of the neural structures interacting with scTS, such as motor neurons, interneurons, and motor axons, to a level that allows weak or residual descending pathways projecting to the spinal cord to activate them. 27,73 Indeed, newer studies provide compelling evidence of scTS therapeutic effectiveness in cerebral palsy, 122,123 spinal muscle atrophy, 124 stroke, 125 multiple sclerosis, 126,127 and peripheral nerve injury. 128 The more the populations in which scTS is demonstrated to be therapeutically effective, the more attention and funding it will draw resulting in evidence-based outcomes, ultimately leading to a better and wider acceptance of scTS in clinical settings.
Conclusions
Regaining UE function remains a top priority for individuals post-cervical SCI. Recent advances in understanding adaptive plasticity within the spinal cord sensorimotor network and its capabilities to interpret descending efferent and ascending afferent inputs to produce appropriate motor output post-injury have led to the development of novel non-invasive neurostimulation strategies, such as scTS to the cervical region, for motor recovery after SCI. A comprehensive understanding of UE motor control, sensorimotor deficits following cervical SCI, and critical appraisal of the available scientific evidence will allow the use of scTS as a viable neuro-rehabilitative tool. In this review, we comprehensively delineated the UE neuromotor control, motor deficits, and limited recovery following cervical SCI, and critically appraised research articles investigating the therapeutic potential of scTS to the cervical region in combination with task-specific training to facilitate functional recovery in individuals with cervical SCI. Although identified studies were limited in number and lacked an adequate sample size to draw scientifically grounded inferences, the reported findings unanimously support the utility and feasibility of scTS to the cervical region combined with task-specific training as an effective neuromodulatory approach to recover sensory and motor function in the UE post-SCI. The majority of studies indicated that scTS was well tolerated, with few addressable adverse effects such as skin redness under the stimulating electrodes. Further, our detailed review also identified several methodological limitations that warrant attention in future studies. These included standardization of stimulation and training strategies, optimal stimulation sites, use of standardized outcome measures, the necessity for randomized controlled clinical trials, and improved reporting of adverse effects. Addressing these challenges in future research will facilitate the effective translation of scTS from a promising therapeutic intervention in the research setting to a clinically viable approach in real-world clinical practice.
Transparency, Rigor, and Reproducibility Statement
A review protocol was developed but not registered for this study. The protocol is available by contacting the corresponding author. The review process followed Arksey and O’Malley’s methodological framework for systematic reviews and the PRISMA checklist extension for systematic reviews. The full list of search terms within the scope of review is mentioned in the Methods section. Title and abstract review, full-text review, and data extraction were conducted by G.S. and P.S. who achieved inter-rater agreement >90% before conducting the review. Any discrepancies in screening or data extraction were resolved through consensus between the reviewers.
Footnotes
Authors’ Contributions
Conceptualization: G.S. and P.S. Methodology: G.S. and P.S. Supervision: S.H., G.F., A.B., and Y.G. Writing—original draft: G.S. and P.S. Writing—review and editing: G.S., P.S., S.H., G.F., A.B., and Y.G. All authors read and approved the final version of the article.
Author Disclosure Statement
Y.G. holds a shared interest in Cosyma Inc. and Onward. The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
Dr. Y.G. is supported by the National Institute of Health and the Program of Pavlov Scientific World-Class Center, agreement No. 075-15-2022-303. Dr. A.B is supported by the Kosair for Kids, Craig H. Neilsen Foundation, and the Kentucky Spinal Cord and Head Injury Research Trust. Drs. S.H and G.F are supported by the Tim and Caroline Reynolds Center for Spinal Stimulation, New Jersey and Kessler Foundation, New Jersey.