
Abstract
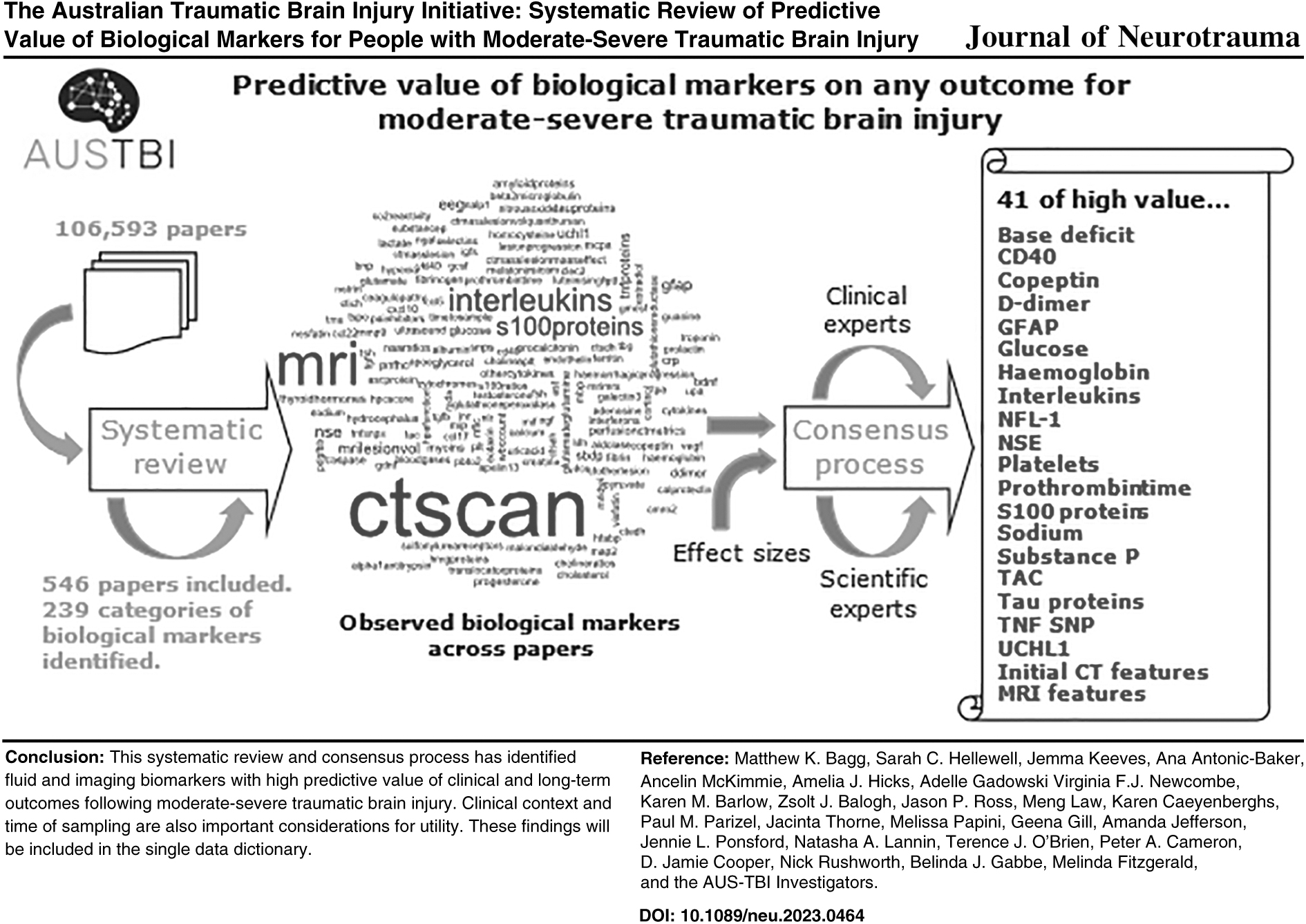
The Australian Traumatic Brain Injury Initiative (AUS-TBI) aims to co-design a data resource to predict outcomes for people with moderate-severe traumatic brain injury (TBI) across Australia. Fundamental to this resource is the data dictionary, which is an ontology of data items. Here, we report the systematic review and consensus process for inclusion of biological markers in the data dictionary. Standardized database searches were implemented from inception through April 2022. English-language studies evaluating association between a fluid, tissue, or imaging marker and any clinical outcome in at least 10 patients with moderate-severe TBI were included. Records were screened using a prioritization algorithm and saturation threshold in Research Screener. Full-length records were then screened in Covidence. A pre-defined algorithm was used to assign a judgement of predictive value to each observed association, and high-value predictors were discussed in a consensus process. Searches retrieved 106,593 records; 1,417 full-length records were screened, resulting in 546 included records. Two hundred thirty-nine individual markers were extracted, evaluated against 101 outcomes. Forty-one markers were judged to be high-value predictors of 15 outcomes. Fluid markers retained following the consensus process included ubiquitin C-terminal hydrolase L1 (UCH-L1), S100, and glial fibrillary acidic protein (GFAP). Imaging markers included computed tomography (CT) scores (e.g., Marshall scores), pathological observations (e.g., hemorrhage, midline shift), and magnetic resonance imaging (MRI) classification (e.g., diffuse axonal injury). Clinical context and time of sampling of potential predictive indicators are important considerations for utility. This systematic review and consensus process has identified fluid and imaging biomarkers with high predictive value of clinical and long-term outcomes following moderate-severe TBI.
Keywords
Introduction
Traumatic brain injury (TBI) is a prevalent and burdensome injury, experienced by 69 million people per year worldwide. The experience of injury is complex, and severe life-changing consequences may extend for many years. Although recently debated, 1 the conventional classifications are mild, moderate, and severe TBI, with moderate-severe TBI (msTBI) often grouped. Whereas prediction of outcome at the level of the individual is currently imprecise, outcomes are known to be related to pre-morbid and injury-related factors. Biological markers (biomarkers) of acute-phase pathology and injury responses have been intensively investigated as potential predictors of outcome in msTBI, with potential biomarkers predominantly identified through neuroimaging or analysis of blood or cerebrospinal fluid (CSF) samples.
Neuroimaging biomarkers of TBI have been observed to relate to outcomes when metrics are derived from computed tomography (CT) and magnetic resonance imaging (MRI). Early literature focussed on a range of CT scores, with many comparisons of these indices as descriptors of the degree of damage. 2 More recently, MRI features and investigations have incorporated newly evolving analytical methods. Fluid or tissue markers have also been observed to relate to outcome. The most commonly investigated indicators are in blood (either serum or plasma) and studies have recently concentrated on glial fibrillary acidic protein (GFAP), ubiquitin C-terminal hydrolase L1 (UCH-L1), neurofilament light (NFL), and S100 beta.3,4
Although the research literature is extensive, and syntheses of specific biological markers are available, information on both imaging and fluid biomarker domains has not yet been integrated. 5 This may be a barrier to interpretation; for example, the pathological nature and relevance of imaging findings (e.g., increased radio-intensity on T2 fluid-attenuated inversion recovery [FLAIR]) may be elucidated through joint consideration of fluid markers for inflammation (e.g., interleukin[IL]-6), or axonal degeneration (e.g., NFL), among others. 6 Moreover, integration in a single synthesis facilitates shared methods of describing predictive power in diverse sets of information. A collated approach may therefore ease interpretation, allow evaluation of established biomarkers, and aid in identification of leading candidates warranting further research for predictive capacity.
A systematic review of biomarkers potentially predictive of clinical outcomes was undertaken to inform the design of a common data dictionary for the Australian Traumatic Brain Injury Initiative (AUS-TBI). AUS-TBI is a collaborative network seeking to improve outcome prediction and care for people with msTBI. 7 The purpose of this data dictionary is to compile a list of common data elements that could feasibly be collected at national scale. This article is focused on biomarkers, defined as any metric or output derived from a sample taken from the patient, or from an imaging technique, that reflects changes in homeostasis of the central nervous system. An additional five related study areas inform the data dictionary: demographic, injury event, and social characteristics, 8 pre-existing health conditions, 9 the clinical experience, 10 acute interventions, 11 and long-term outcomes. 12
The identified data elements from each study area will be collected and integrated to generate predictive algorithms using novel analyses. 7 Prior work by AUS-TBI researchers 13 has identified features of consensus processes that had been used to define data dictionaries for people with neurological afflictions, including TBI. In approximately half of cases, extant literature was used alongside stakeholder input in the consensus processes. Although a minority used systematic reviews, these are the best-practice means of evidence synthesis. Thus, a single joint integration of the evidence for biological markers using both systematic reviews and consensus processes stands to make an important contribution to the field, and to the aims of AUS-TBI.
The objective of this study was to conduct a systematic review of all biological markers that have been evaluated for relation to clinical outcomes in people with msTBI and describe a consensus assessment of the identified predictors. This work is intended as part of a series of analyses similarly addressing study areas of social, 8 health, 9 clinical, 10 intervention, 11 and long-term outcomes 12 following msTBI.
Methods
This systematic review was prospectively registered on PROSPERO (CRD42022297902). The study is reported herein with respect to the 2020 Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement. 14
Objectives
The objectives of this study are four-fold:
Identify published records of studies evaluating biological markers for predicting clinical outcomes in people with msTBI. Identify unique biological markers evaluated by studies in the record set. Assign judgements of predictive value to each observed association between biological marker (predictor) and clinical outcome. Identify biological markers that are feasible to collect.
Outcomes
The primary outcome of this study is the set of unique feasible predictors. Secondary outcomes are the sets of unique predictors, clinical outcomes, and studies.
Sampling
Standardized, piloted, search strategies were used to search CINAHL, Embase, Medline, SportDiscus, and PsycINFO from inception to April 28, 2022. Records were sequentially de-duplicated using automatic functions in Endnote (20.6), Zotero (6.0.26), Covidence, 15 and Research Screener. 16 A panel of review team members (MKB, SAH, VFJN, JT, MP, CB, ZB, MF)—leveraging clinical area expertise and prior experience conducting systematic reviews—were trained to apply the eligibility criteria. Record titles and abstracts were screened in subsets of 50 by a single team member (MF) using Research Screener. Research Screener implements a prioritization algorithm to calculate likelihoods of inclusion for records yet to be screened, using (1) an initial subset of seed records (known to be included), and (2) the scores assigned by human screeners.
These likelihoods are used to select each subsequent prioritized subset of 50 records. 16 We pre-specified the stopping rule that screening would cease when the team member included zero records from two consecutive subsets. The full length of potentially eligible records were retrieved using institutional subscriptions, loan requests, or open sources. These records were screened by a single team member [from the panel] to confirm inclusion in Covidence. Record authors were not contacted to clarify eligibility criteria for this iteration of the review. Records excluded from the full-length stage are listed in Supplementary Appendix S1.
Eligible records were published, English-language reports of any study evaluating relationships between biomarkers and clinical outcomes in at least 10 people with msTBI. Case series, abstracts, review articles, errata, and other journal material were excluded. The biomarkers of interest to this study were any fluid, tissue, or imaging-based marker measured at the time of injury or during the TBI experience. Clinical outcomes were considered broadly as any dependent variable (in that particular study report) reflective of the clinical features or lived experience of TBI. msTBI was defined as the reported, medically confirmed presence of at least one of the following: (1) initial or lowest Glasgow Coma Scale (GCS) score less than 13, (2) post-traumatic amnesia duration greater than 24 h, or (3) abnormal findings on CT imaging of the head. This operational definition includes the complicated-mild injury type. 17
As outlined by Gabbe and colleagues, 8 studies sampling participants without TBI, or with mild, non-complicated TBI were only included if the data on participants with msTBI were reported separately from other participants or, greater than 80% of the baseline sample comprised people with msTBI. Studies without clearly reported medical confirmation of msTBI were included on the expert clinical area judgement of the review team that medical confirmation would have necessarily occurred in the study context. There were no restrictions on demographic characteristics of individuals or injury circumstances.
Data extraction
The coordinating team members and AUS-TBI Steering Committee co-designed the data items (variables) for extraction from included study reports. Standardized data sheets were built in Google Sheets (GSuite, Monash University), piloted, then adapted to the requirements of this review. Detailed data extraction methods are described elsewhere. 8 Briefly, the data items captured information on study identifiers, measured outcomes, measured predictor variables (in this review: fluid, tissue, or imaging biomarkers), baseline sample size, subgroups, covariate adjustment, and reported measures of effects. Study authors were not contacted to request missing data or to clarify uncertain data for this iteration of the review.
Data were extracted from each record by a single team member from a trained panel (MKB, SCH, JK, JT, MP, VFJN, GG, AJ, KB, ZB, JR, ML, KC, PP, MF). First, inclusion criteria were checked and confirmed. Next, expert judgement was used to identify only predictor:outcome associations meeting the above criteria. In this review, this was all associations between a biomarker and clinical outcome evaluated in each study. Relevant associations not reported in full (e.g., missing effects) were extracted. Associations identified as relevant to other study area reviews were extracted and coded relevant to the respective review. The sheets included additional data items that summarized or structured the information in the extracted data items. These were filled during the extraction process. Upon completion, the team member used a pre-defined decision algorithm (see the sidebar, Decision Algorithm for Judgements of Predictive Value) to assign a judgement of predictive value to each observed predictor:outcome association. A strong predictive relationship was considered one that was statistically significant (p < 0.05) and when in conjunction with the other elements of sample size >100 and adjustment for covariates, a high predictive value was allocated. The judgements of predictive value were randomly cross-checked by an independent team member.
HIGH: large sample size (n > 100) AND association tested in whole study sample AND adjusting for covariates AND a strong predictive relationship was observed.
MEDIUM: smaller sample size (n < 100) AND association tested in whole study sample AND adjusting for covariates AND a strong predictive relationship was observed.
MEDIUM: large sample size (n > 100) AND association tested in whole sample AND limited adjustment for covariates OR moderate predictive relationship.
LOW: small study size (n < 100) OR association tested in subset of sample OR limited predictive relationship observed.
NB: ignore study size if the predictor is an imaging marker.
Data management
Completed data sheets were locked to editing, mirrored to static versions on OneDrive (Microsoft 365, version ccc), and read to R (version 4.3.1) using readxl. 18 Data were inspected for implausible and missing values, cleaned, then summarized using tidyverse 19 and labelled. 20 Implausible values were replaced in the R object (i.e., operating data set), with recourse to the study report as required. The extent of missing values was calculated for each variable. Observations coded relevant to other study area reviews were parsed to the appropriate data set object. Categorical variables were summarized using the frequency of observations on each level. Variables that captured semi-structured text were coerced to factors (the categorical structure in R) and unique levels were identified through homogenization by the review team. Original free text was preserved. The subsequently “cleaned” data set was written out to .csv, with values locked to editing. Word clouds 21 were used to display the observed frequency of unique predictor variables and outcomes in the included studies (Figs. 2 and 3).
AUS-TBI consensus process
AUS-TBI integrates multiple stakeholders. The contributions of (1) clinicians and researchers, (2) people with lived experience, and (3) people identifying as Aboriginal or Torres Strait Islander were sought at distinct stages of development of the data dictionary. In this “Biologicals” study area, clinicians and researchers were consulted at an interim stage, to enable the independently facilitated consensus meetings to be conducted in close temporal proximity to each other, thereby aiding in consistency of process. The consensus process was organized by a member of the Initiative Steering Committee (MF). Consultation occurred in a real-time virtual meeting, facilitated by an external consultant. Participants were sent the interim results of the systematic review prior to attending the meeting. The interim data set contained 526 predictive factors and 129 outcomes, arising from full-text review of 217 publications. Participant input was collected using structured questioning focused on the high-value predictors, open discussion, and voting. Specific details of the consensus process and scoring system used are described elsewhere. 8
Due to the experimental nature of the majority of the high-value fluid and imaging biomarkers identified at the interim stage, the scoring was confined to a rating of 1, 2, or 3, with 3 indicating strong support from the group. The consensus discussion also separately considered the predictive value of the measures for adults and children. The complete set of high-value predictive biomarkers was recirculated to the consensus group at completion of the data extraction process, for further feedback via circular email, and that feedback was integrated into the final choice of biomarkers to generate a feasible list of prospective items for the data dictionary. Clinician and researcher participants were members of AUS-TBI Investigator group who self-nominated for this “Biologicals” study area consensus process. Some of the identified markers were also relevant for the “Clinical” study area and further input was invited from the AUS-TBI Investigator group at manuscript review stage.
Differences between protocol and this iteration of the review
First, in the protocol we stated that in addition to searching original published articles we would also include a search of “gray” literature. This search of government, institutional, and consumer sources was not completed for reasons of feasibility and yield. Second, we did not use the JBI extraction tool but rather built our own. Third, we did not assess the risk of bias of the included studies due to the time frames required to be met for the consensus meetings and project completion. Additionally, as the purpose of this review was not to identify a “correct” predictive relationship, but to describe the existing literature in sufficient detail in preparation for people to make an informed decision about predictors in the consensus meeting, a full risk of bias assessment was not indicated.
Results
The searches identified 106,593 records, including 31,774 duplicates. The title and abstract of 74,696 records were screened: 7186 by the team members and 66,093 through the prioritization algorithm. The full lengths of 1417 records were successfully obtained and screened, and 871 records were excluded, yielding 546 records for this iteration of the review (Fig. 1). Full texts of 106 records were not obtainable for this iteration of the review (see Supplementary Appendix S1).
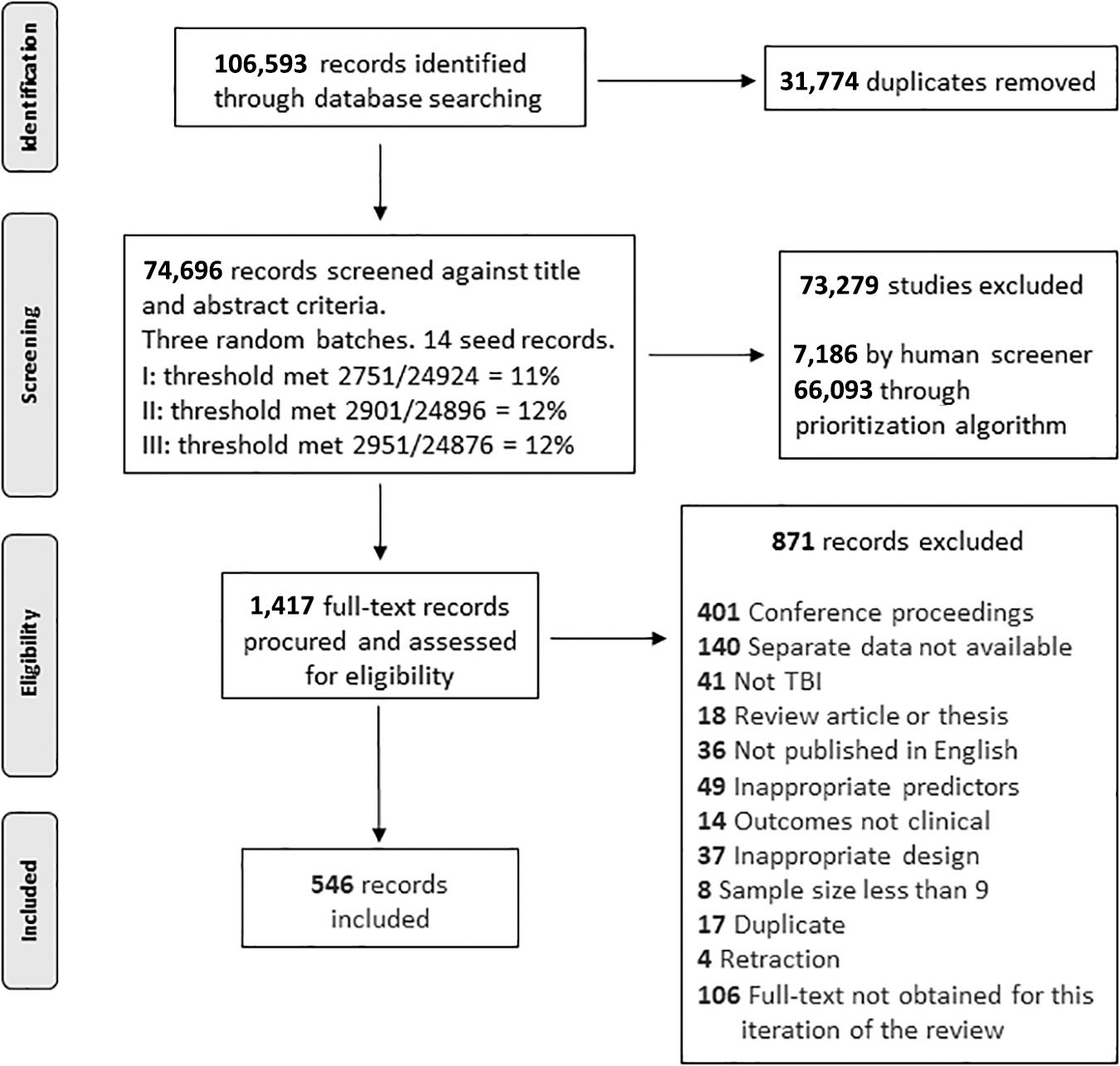
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram.
The 546 records were published across the period of 1978 to 2022. These were 350 prospective (including 5 randomized controlled trials) and 155 retrospective cohort designs, 30 prospective and 10 retrospective case-control designs, and a single cross-sectional case-control design. At least 3450 observations of associations between biomarkers and clinical outcomes were identified in the included records. The 1217 observed predictors (biomarkers) were homologized to 239 unique predictors, and the 383 observed outcomes to 101 unique outcomes (Supplementary Appendix S2).
The most frequently observed predictors were the “interleukins” (8.9%, n = 287/3210 total observations), followed by “S100 proteins” (6.2%, n = 199/3210), “CT, mass lesion, mass effect” (4.8%, n = 155/3210), “CT, Marshall CT score” (3.8%, n = 123/3210), “CT, Rotterdam CT score” (2.8%, n = 90/3210), and neuron-specific enolase (NSE); 2.6%, n = 85/3210) (Fig. 2). The most common outcomes were Glasgow Outcome Scale-Extended (GOSE; n = 1481), mortality (n = 582), GCS (n = 115), neuropsychological function (n = 90), cognitive function (n = 82), and hemorrhagic progression on CT (n = 71) (Fig. 3).
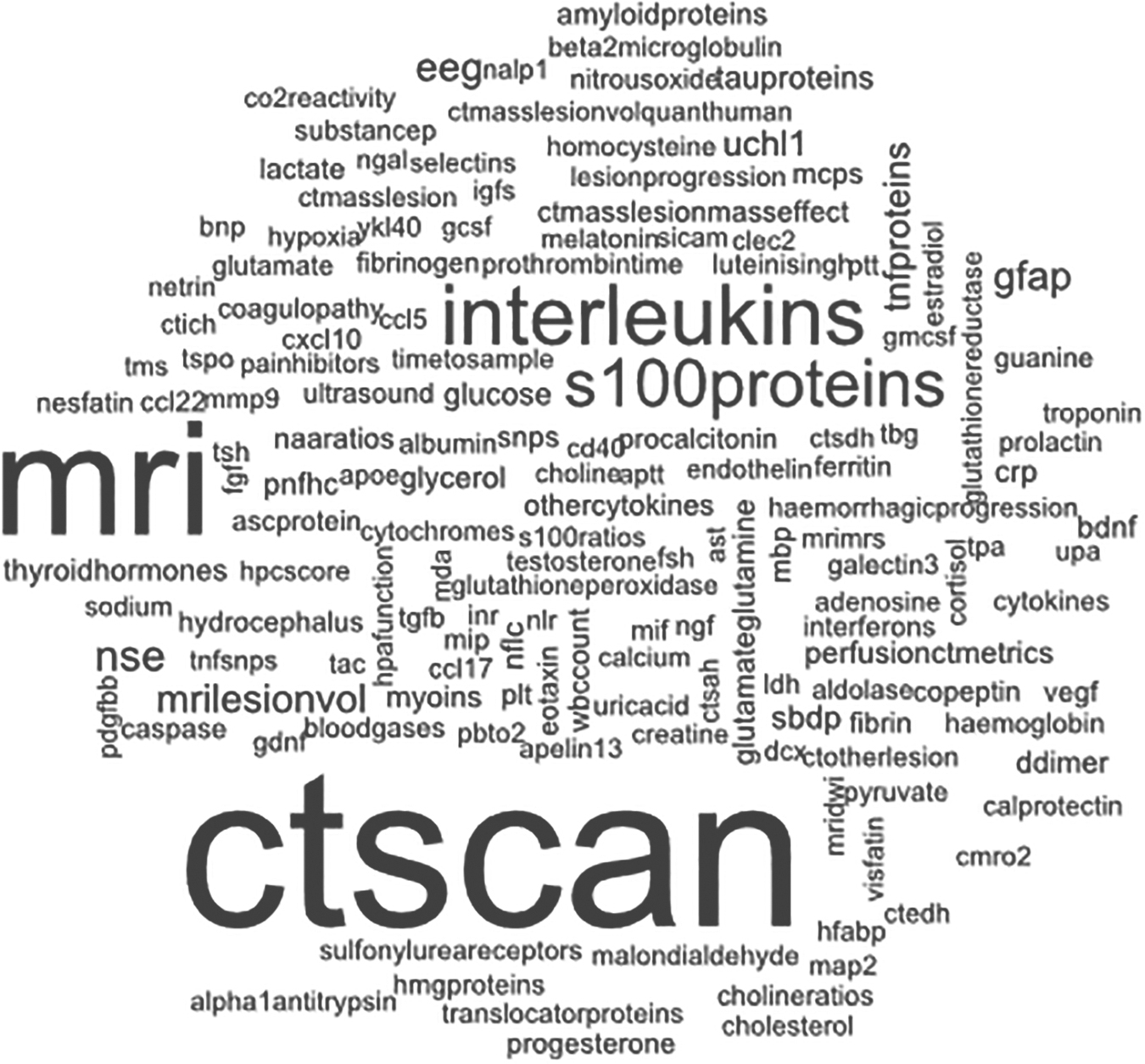
Word cloud of predictors of outcome (size of word denotes frequency in included records): apelin13, Apelin-13; apoe, Apolipoprotein E; aptt, Amide-Proton-Transfer; ascprotein, ASC protein; ast, aspartate aminotransferase; bdnf, brain-derived neurotrophic factor; bnp, brain natriuretic peptide; caspase, cysteine-dependent aspartate-specific protease; cd40, cluster of differentiation 40 (CD40); clec2, CLEC-2; cmro2, cerebral metabolic rate of oxygen; co2reactivity, carbon dioxide reactivity; ctscan, computed tomography (CT) scan; crp, C-reactive protein; ctedh, CT, extradural hemorrhage; ctich, CT, intracranial hemorrhage; ctmasslesion, CT, mass lesion; ctlesionvol, CT, mass lesion, lesion volume; ctmasslessionmasseffect, CT, mass lesion, mass effect; ctotherlesion, CT, other lesion; ctsah, CT, subarachnoid hemorrhage; ctsdh, CT, subdural haematoma; dcx, doublecortin; ddimer, D-dimer; eeg, electroencephalography; fgf, fibroblast growth factors; fsh, follicle-stimulating hormone; gcsf, granulocyte-colony stimulating factor; gdnf, glial cell line-derived neurotrophic factor; gfap, glial fibrillary acidic protein; gmcsf, granulocyte macrophage colony-stimulating factor (GM-CSF); hfabp, heart fatty-acid binding protein (H-FABP); hmgproteins, high mobility group (HMG) proteins; hpafunction, hypothalamic-pituitary-adrenal (HPA) function; hpcscore, hemorrhagic progression of contusion (HPC) score; igfs, insulin-like growth factors; inr, international normalized ratio; ldh, lactate dehydrogenase; luteinisingh, luteinising hormone; map2, MAP-2; mbp, myelin basic protein; mcps, monocyte chemoattractant proteins (MCPs); mda; malondialdehyde; mdc, macrophage-derived chemokine; mif, macrophage migration inhibitory factor; mip, macrophage inflammatory protein; mmp9, matrix metallopeptidase 9; mri, magnetic resonance imaging (MRI); mridwi, MRI, diffusion weighted imaging (DWI); mrimrs, MRI magnetic resonance spectroscopy; myoins, myoinositol; naaratios, N-acetylaspartate (NAA) ratios; nalp1, NOD-like receptor protein (NALP-1); nflc, neurofilament light chain; ngal, neutrophil gelatinase-associated lipocalin; ngf, nerve growth factor; nlr, neutrophil to lymphocyte ratio; no, nitric oxide; nse, neuron-specific enolase; pbto2, partial brain tissue oxygen pressure (PbtO2); pdgfbb, platelet-derived growth factor BB (PDGF-BB); plt, platelets; pnfhc, phosphorylated neurofilament heavy chain (pNF-H); ptt, partial thromboplastin time; sbdp, spectrin breakdown products; sicam, soluble intercellular adhesion molecule; snps, single nucleotide polymorphisms (SNPs); tac, total antioxidant capacity; tbg, thyroxin-binding globulin; tgfbeta, transforming growth factor-beta (TGF-β); tms, transcranial magnetic stimulation; tnfproteins, tumor necrosis factor proteins; tnfsnps, TNF SNPs, tumor necrosis factor single nucleotide polymorphisms; tpa, tissue plasminogen activator; tspo, translocator protein; uchl1, ubiquitin C-terminal hydrolase L1; upa, urokinase plasminogen activator; vegf, vascular endothelial growth factor; wbccount, white blood cell count; ykl40, chitinase-3-like protein 1 (YKL-40).
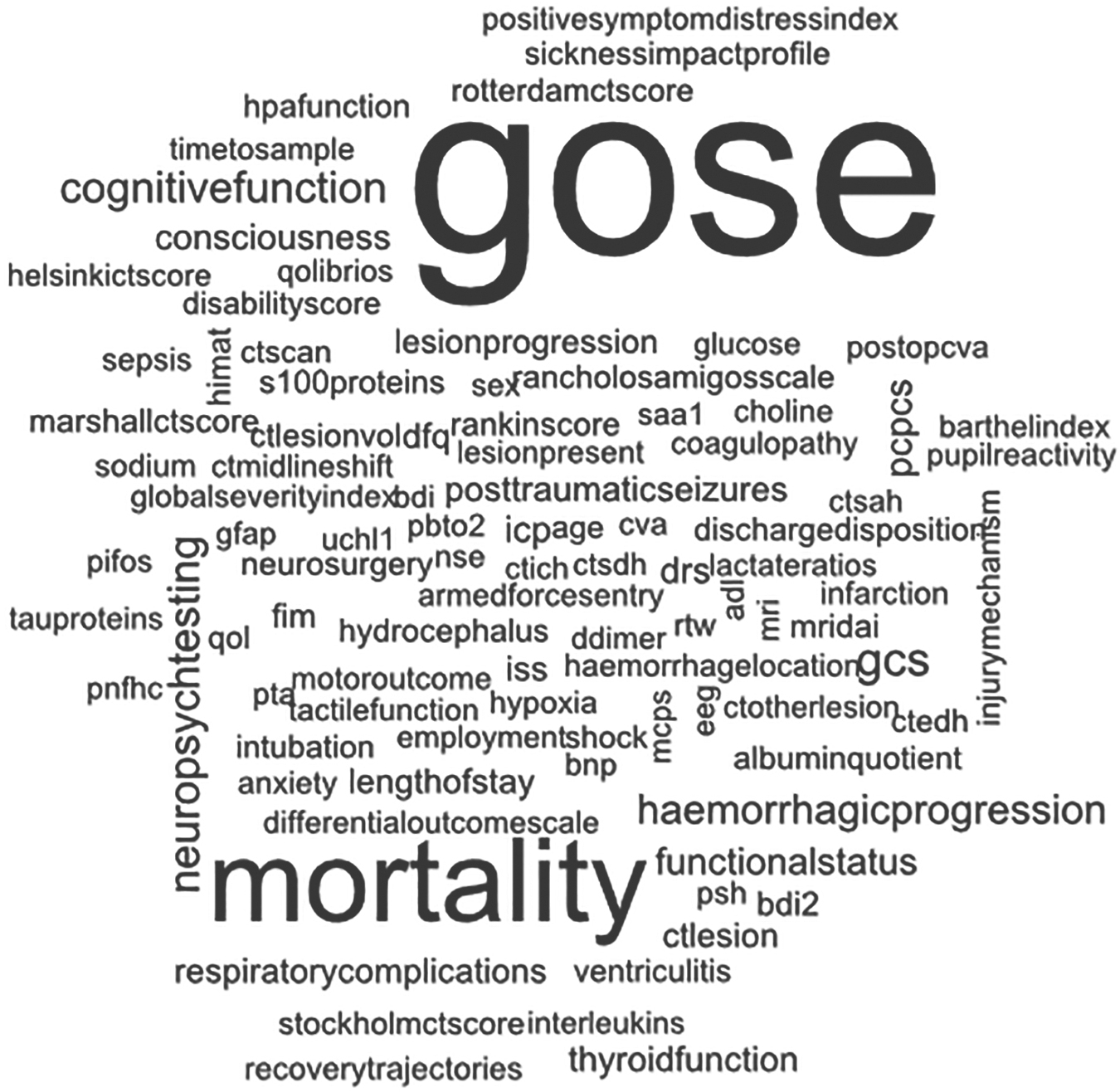
Word cloud of outcomes assessed against the predictors (size of word denotes frequency in included records): adl, activities of daily living; bdi, Beck Depression Inventory; bdi2, Beck Depression Inventory-II; bnp, brain natriuretic peptide; ctscan, computed tomography (CT) scan; ctedh, CT, extradural hemorrhage; ctich, CT, intracerebral hemorrhage; ctlesion, CT lesion; ctmidlineshift, CT, midline shift; ctlesionvol, CT, lesion volume; ctotherlesion, CT, other lesion; ctsah, CT, subarachnoid hemorrhage; ctsdh, CT, subdural hematoma; cva, cerebrovascular accident (CVA); ddimer, d-dimer; dfq, developmental functional quotient; drs, Disability Rating Scale; eeg, electroencephalography; fim, Functional Independence Measure; gcs, Glasgow Coma Scale; gfap, glial fibrillary acidic protein; gose, Glasgow Coma Scale-Extended (GOSE); helsinkictscore, Helsinki CT score; himat, High Level Mobility Assessment Tool; hpafunction, hypothalamic-pituitary-adrenal (HPA) function; icp, intracranial pressure; iss, Injury Severity Score; marshallctscore, Marshall CT score; mcps; monocyte chemoattractant proteins (MCPs); mri, magnetic resonance imaging (MRI); mridai, MRI, diffuse axonal injury; nse, neuron-specific enolase; pcpcs, Pediatric Cerebral Performance Category Scale; pifos, Pediatric Injury Functional Outcome Scale; pnfhc, phosphorylated neurofilament heavy chain (pNF-H); postopcva, post-operative CVA; psh, paroxysmal sympathetic hyperactivity; pta, post-traumatic amnesia; pbto2, partial brain tissue oxygen pressure (PbtO2); qol, quality of life; qolibrios, Quality of Life After Brain Injury–Overall Scale (QOLIBRI-OS); rlas, Rancho Los Amigos Scale; rotterdamctscore, Rotterdam CT score; rtw, return to work; saa1, serum amyloid A1; stockholmctscore, Stockholm CT score; uchl1, ubiquitin C-terminal hydrolase L1.
There were 39 predictors arising from the screened and extracted literature with at least a single observation of high predictive value (Table 1). These predictors were evaluated for associations with 15 clinical and long-term outcomes: hemorrhagic progression, progressive hemorrhagic injury, lesion progression, development of circulatory shock and raised intracranial pressure, post-operative pain, length of stay in intensive care, recovery of consciousness, mortality/death, GOS/GOSE, Functional Independence Measure (FIM), recovery trajectories, disability rating scale, motor function, and cognitive function. The outcomes identifying the predictive measures as high-value were assessed at times after injury ranging from the first 72 h (n = 6 studies), in hospital or at discharge (n = 16 studies), 1–3 months (n = 4 studies), 6 months or longer (n = 28 studies) or of an unclear sampling time (n = 4 studies), noting some studies assessed at multiple time-points. Full details are available in the complete data set (Supplementary Appendix S2). The high-value predictors included fluid biomarkers from both CSF and blood, and imaging characteristics from both CT and MRI.
Associations Between Biomarkers and Clinical Outcomes Judged as High Predictive Value

Total number of studies reporting high, medium, low, or null predictive value. Total does not include studies where the predictive value was unclear or study design didn't allow determination.
ABCB1, ATP-binding cassette B1; ADC, apparent diffusion coefficient; CD40, cluster of differentiation 40; CSF, cerebrospinal fluid; CT, computed tomography; DAI, diffuse axonal injury; DFQ, developmental functional quotient; DRS, disability rating scale; DWI, diffusion-weighted imaging; EDH, extradural hemorrhage; FIM, functional independence measure; GFAP, glial fibrillary acidic protein; GOSE, Glasgow Outcome Scale-Extended; ICH, intracerebral haemorrhage; ICP, intracranial pressure; IVH, intraventricular hemorrhage; LOS, length of stay; MRI, magnetic resonance imaging; PC1, principal components-1; SAH, subarachnoid hemorrhage; SDH, subdural hematoma; SBDP, spectrin breakdown products; TCDB, Traumatic Coma Data Bank; TNF SNPs, tumor necrosis factor single nucleotide polymorphisms; UCHL1, ubiquitin C-terminal hydrolase L1.
Integrating input from the consensus group
The meeting of the panel of clinicians and researchers was convened in June 2022. The panel considered the interim evidence from the systematic review, focusing on the high-value predictors identified at that time. The expected coverage, feasibility, and fidelity of collection in the Australian context was considered and an overall rating score agreed for each predictor identified to date (Table 2). Additional potential predictors raised by the panel were also identified, some of which were subsequently identified in the completed review; details are in Table 2. The consensus group agreed that although individual scores and characteristics from CT and MRI scans could be predictive, a better approach to ensure complete capture of known and future predictive indicators would be to directly analyze CT and MRI scans, for example using machine learning approaches. Further iterative review of the final list of high predictive value biomarkers was provided by the consensus group using circular e-mail once the systematic review was completed. The additional measures were not scored; feedback was noted in comment form as a footnote (Table 2).
Integration of Systematic Review and Clinical and Research Expert Consensus Group Input for High-Value Fluid (Blood and CSF) and Imaging Predictors
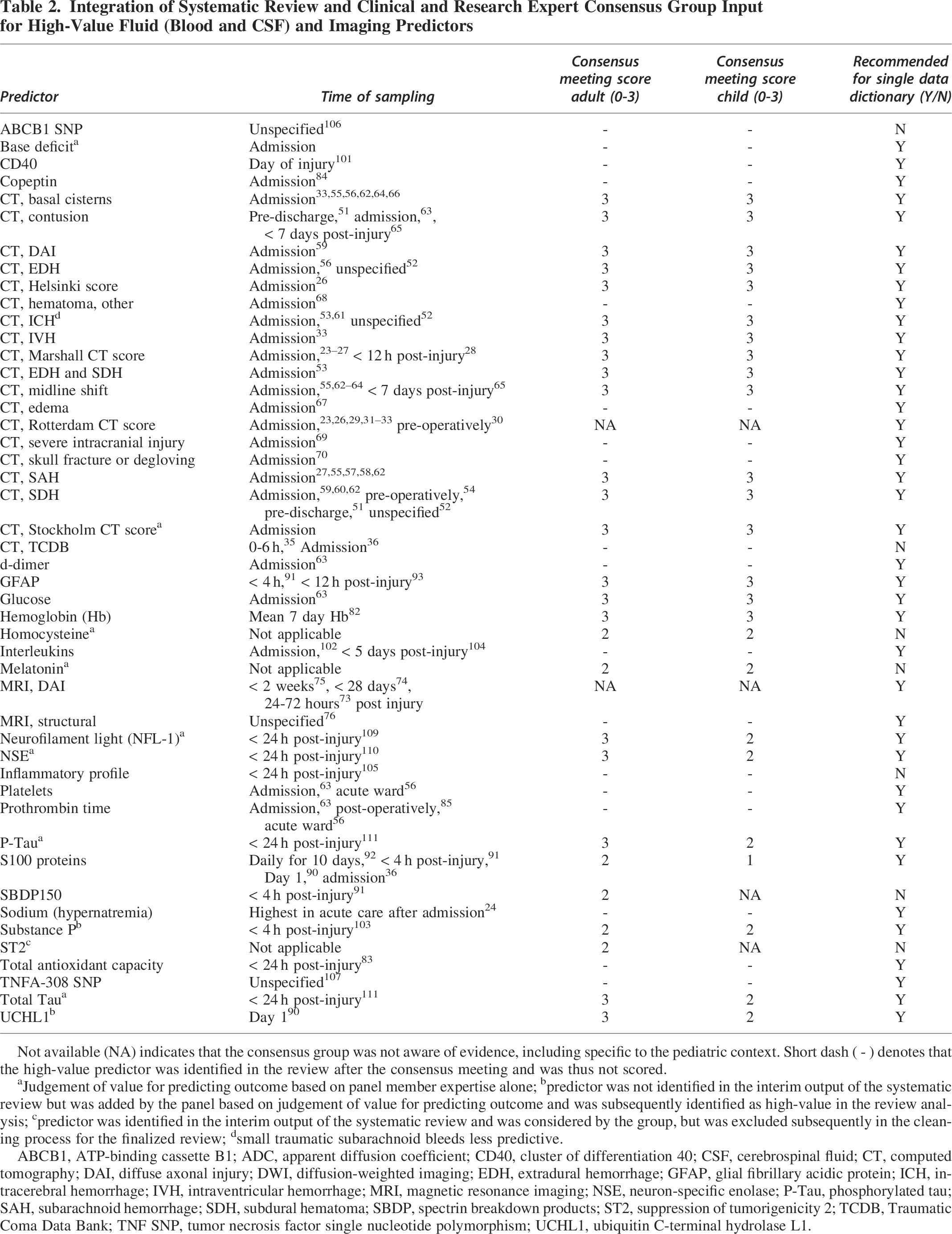
Not available (NA) indicates that the consensus group was not aware of evidence, including specific to the pediatric context. Short dash ( - ) denotes that the high-value predictor was identified in the review after the consensus meeting and was thus not scored.
Judgement of value for predicting outcome based on panel member expertise alone; bpredictor was not identified in the interim output of the systematic review but was added by the panel based on judgement of value for predicting outcome and was subsequently identified as high-value in the review analysis; cpredictor was identified in the interim output of the systematic review and was considered by the group, but was excluded subsequently in the cleaning process for the finalized review; dsmall traumatic subarachnoid bleeds less predictive.
ABCB1, ATP-binding cassette B1; ADC, apparent diffusion coefficient; CD40, cluster of differentiation 40; CSF, cerebrospinal fluid; CT, computed tomography; DAI, diffuse axonal injury; DWI, diffusion-weighted imaging; EDH, extradural hemorrhage; GFAP, glial fibrillary acidic protein; ICH, intracerebral hemorrhage; IVH, intraventricular hemorrhage; MRI, magnetic resonance imaging; NSE, neuron-specific enolase; P-Tau, phosphorylated tau; SAH, subarachnoid hemorrhage; SDH, subdural hematoma; SBDP, spectrin breakdown products; ST2, suppression of tumorigenicity 2; TCDB, Traumatic Coma Data Bank; TNF SNP, tumor necrosis factor single nucleotide polymorphism; UCHL1, ubiquitin C-terminal hydrolase L1.
Imaging markers from CT identified in the review were predominantly measures that form part of the standard CT scoring measures of the Marshall, Helsinki, Rotterdam, and Stockholm indices. Nevertheless, specific imaging features were identified in the review that may have particular predictive value, including abnormal basal cisterns, presence/location of lesion or hemorrhage, and diffuse axonal injury (Table 2).
Discussion
Review findings
The purpose of this review was to identify biological predictors of clinical outcome after msTBI that are established in the literature, and to determine which of these had the capability to be used with high predictive value in a large-scale effort to predict injury outcomes across Australia. The 546 published studies assessed could be broadly grouped as those employing neuroimaging or biofluid predictors, with 239 unique predictors assessed relative to 101 outcome measures. Despite the large body of literature, reported biological markers were most often found to be of null or low predictive value due to small sample sizes and/or lack of predictive capacity for reported outcomes. Despite this, 39 biological markers were determined to be of high predictive value.
These high-value predictors predicted outcomes related to 15 clinical measures, including progression of hemorrhage or lesion, development of circulatory shock or raised intracranial pressure, recovery of consciousness, length of stay in the intensive care unit (ICU), mortality, post-operative pain, FIM, recovery trajectory, or measures of outcome including GOS/GOSE, score on disability rating scale, or motor or cognitive function. These markers were reviewed and considered by the consensus group for their fidelity and feasibility for collection and measurement, and additional potential predictors were added where the panel deemed appropriate. This yielded a final set of 41 potentially predictive markers, which will be used to inform the design of the AUS-TBI common data dictionary.
High-value outcome predictors derived from CT classification systems
Due to the frequency of abnormal imaging findings in patients with msTBI, CT scans are often among the first diagnostic tests employed to guide emergent treatment. 22 CT has high sensitivity and specificity for location and severity of intracranial pathology. Both the Marshall and Rotterdam CT classification systems are used frequently in clinical practice to grade injury severity and guide clinical management. Some of the most compelling evidence of predictive capacity for msTBI to date has been derived from these classifications. The Marshall score is a superior predictor of in-hospital mortality23,24 and length of ICU stay, 25 whereas both the Marshall and Rotterdam scores on admission are high-value predictors of mortality at 6 months post-injury. 26 Similarly, both the Marshall and Rotterdam systems have been used to generate high-value predictors of long-term outcome, successfully predicting GOS and/or GOSE scores at 6 months,27,28 12 months, 29 and 42 months. 30 The Rotterdam score also has evidence of predictive capacity for mortality,23,31 recovery of consciousness, 32 and motor function at the time of hospital discharge. 33
Two studies were found employing the Traumatic Coma Data Bank (TCDB) CT classification 34 as a high-value predictor of early mortality and brain death at the more severe levels, whereas types IV (diffuse injury with shift), V (surgically evacuated mass lesion), and VI (non-evacuated mass lesion) on admission successfully predicted mortality within the first 48 h 35 and types V and VI detected on admission were predictive of brain death. 36 This scoring system has received comparatively less attention, and was decided by the consensus panel not to be progressed at this stage. Newer CT scoring systems have been more recently developed that extend on the Marshall and Rotterdam scores, including the Stockholm and Helsinki CT scoring systems.37,38 We found only one instance meeting our criteria in which the Helsinki score was determined as a high-value predictor, with capacity to successfully predict mortality at 6 months. 26 No studies using the Stockholm CT scoring system were found to yield a high-value predictor; however, use of both the Stockholm and Helsinki scores was strongly supported by the consensus group due to emerging evidence for use in adult and pediatric populations, 39 and they were subsequently integrated into the data dictionary.
High-value outcome predictors derived from CT biomarkers of pathology
Up to 56% of patients with msTBI will present with intracranial hemorrhage. 40 These bleeds have been shown to significantly worsen in-hospital mortality and may signal poor prognosis. 41 Depending on anatomical location, hemorrhage may be classed as epidural, subdural, intracerebral, or contained within the subarachnoid space, 42 although differing types of intracranial hemorrhage may occur concurrently.43,44 Early detection of hemorrhage is vital as it may progress and grow within hours and days after injury.45,46
Management of intracranial hemorrhage is dependent on the size and location of the bleed. Surgical evacuation or decompression may be required depending on intracranial pressure 47 and size and location of the hemorrhage,48,49 particularly for those that are extradural or subdural. Smaller hematomas may resolve with time; however, the choice for early surgical intervention or more conservative management may depend on the site and clinical impression in the absence of intracranial pressure monitoring. 50 Surgical intervention modifies outcomes following msTBI, and it is covered in detail in a further article. 11
From the body of literature assessed in this study, we determined that early detection of hemorrhage could also be used as a significant predictor of hemorrhagic progression, mortality, and functional outcome when located in the subdural, epidural, or intracerebral spaces.51–54 Likewise, hemorrhage in the epidural or subarachnoid space was a high-value predictor of in-hospital mortality 55 and poor outcome at 6 months,27,56–58 subdural hemorrhage predicted both 12-month mortality 59 and poor GOSE, 60 and intracerebral hemorrhage was a high-value predictor of poor outcome at 24 months post-injury. 61 Presence of subarachnoid or subdural hemorrhage was a good predictor of poorer recovery trajectory overall, 62 whereas intraventricular hemorrhage was a highly significant predictor for poor cognitive and motor function. 33 The secondary consequences of this progression can be particularly dangerous, causing mass effect, edema formation, and midline shift.
The presence of midline shift was determined as a significant predictor of outcome in five studies conducted in both adult and pediatric populations. Midline shift was a high-value predictor of mortality at discharge 55 and of progressive hemorrhagic injury, 63 and it was an early signifier of poor functional outcomes,62,64,65 particularly where the shift was 5 mm or greater. Likewise, early effacement of the basal cisterns was a high-value predictor of mortality at discharge 55 and of motor and general functional outcomes at 6 months33,56,62,64 post-injury. In contrast, patency of the basal cisterns has been documented as a high-value predictor of both survival and good outcome at 6 months. 66 CT has also been the modality of choice for other high-value predictors for a variety of outcomes, including edema, which was a significant predictor of 24-h mortality in children when assessed at admission. 67
Over the longer term, mortality at 12 months has been predicted by the presence of six or more white matter lesions indicative of diffuse axonal injury (DAI) 59 and by early presence of any hematoma. 68 The presence of mass lesion on admission was also determined as a high-value predictor of length of stay in the ICU. 25 Other assessments of documented CT signs also indicate that parenchymal contusions could act as high-value predictors of hemorrhagic progression in children and adults,51,63 and may also predict poor long-term functional outcomes. 65 Similarly, the presence of any severe intracranial injury could significantly predict 90-day mortality, 69 whereas an a priori classifier of significant head trauma (including signs of basal or depressed skull fracture or degloving) significantly predicted raised intracranial pressure. 70
High-value outcome predictors derived from MRI biomarkers of pathology
CT scans are among the most rapid and readily interpretable methods to detect hemorrhage after msTBI; however, MRI has a distinct advantage in detecting non-hemorrhagic lesions and DAI. 71 The histopathological grading system for DAI first proposed by Adams and colleagues 72 in 1989 is still prominently used for MRI today, and was found to be a high-value predictor of outcome in three studies within this body of literature. The presence of multiple lesions in the corpus callosum (DAI grade 2) was a significant predictor of length of time to recovery of consciousness, 73 whereas DAI lesions of grades 2 and 3 were determined to be a high-value predictor of poor GOS score at 6 months post-injury in the same study. 73 Likewise, DAI of any grade on MRI within the first 2 weeks of msTBI was highly predictive of both functional independence score at discharge and 12-month GOSE, with the presence of DAI predictive of poorer functional status.74,75 MRI has also been used for anatomical and/or structural assessment, whereby atrophy within the bilateral thalami and basal ganglia was determined a high-value predictor of poor GOSE scores at 6 months. 76
Geographic considerations of CT and MRI biomarker implementation
In the latest estimates from 2022, there were 69.57 CT scanners per million people in Australia, 77 ranking only behind Japan in accessibility. There were also 15 MRI scanners per million people in Australia, 78 ranking eighth worldwide. Australia is thus well-positioned to collect CT and MRI biomarkers, with relatively equal distribution of CT and MRI scanners across Australian states and territories. However, geographic disparity exists with regard to imaging facilities and technical expertise to acquire and interpret scans in more geographically remote areas. 79 This disparity must be considered when choosing predictive indicators applicable to the Australian population as a whole.
High-value outcome predictors derived from routine clinical blood tests
Fluid biomarkers present an attractive and minimally invasive option to monitor brain pathology after msTBI. Markers may be derived from different cellular sources and capture a range of aspects of primary and secondary pathology, 80 or may be more general physiological indicators of systemic health. Importantly, fluid biomarkers are well suited to serial sampling, allowing for monitoring of temporal trajectories 81 and real-time theragnostic assessment in clinical trials. Four high-value predictors of mortality identified in this study were derived from routine laboratory diagnostic tests, suggesting high feasibility and capacity for uptake. These were hemoglobin, for which a mean 7-day concentration below 90 g/L predicted in-hospital mortality 82 ; hypernatremia, for which greater sodium concentrations predicted significantly lower inpatient survival rates 24 ; total antioxidant capacity, which was a significant predictor of 30-day mortality when serum concentrations rose above 2.59 nmol/mL in the first 24 h following injury 83 ; and plasma copeptin concentration on admission, which was a high-value predictor of 6-month mortality in a pediatric population. 84
Four routine diagnostic tests were found to be of high utility in predicting hemorrhagic progression, including prothrombin time in adult and pediatric patients,63,85 and platelet count, d-dimer, and glucose in pediatric patients, 63 for which admission concentrations at or above 5 mg/L or 10 mmol/L (respectively) on admission were significant predictors of progressive hemorrhagic injury. Three standardized diagnostic tests were high-value predictors of poor outcome as measured by GOSE scores at 6 months post-injury, including acute platelet concentration and prothrombin time in adult and pediatric patients, 56 and copeptin concentration in pediatric patients. 84 Given the widespread and standardized use of these markers in clinical practice and relative ease of laboratory processing, these markers hold considerable promise for incorporation into prognostic guidelines. An important caveat, however, is patient context, as the individual relevance and performance of these markers may differ depending on age, interventions, and the underlying clinical presentation.
High-value outcome predictors derived from fluid biomarkers of astrocytes and neurons
Injury-specific fluid biomarkers are most typically assessed in the very acute stages after msTBI, although optimal sampling time depends on the biomarker of interest and the time at which it is sampled, with some biomarkers most useful weeks and even months post-injury. 86 Markers reflecting astrocyte responses and neuronal injury typically peak within the first 48 h after injury. 81 Indeed, acute measurement of the astrocyte (and to a lesser degree, oligodendrocyte 87 and adipose 88 ) marker S100B has now been implemented in the Scandinavian guidelines for management of mild-to-moderate TBI, 89 where its high sensitivity could reduce the need for up to 32% of CT scans. 89 We found S100B to be a high-value predictor in four studies of msTBI. S100B concentrations at admission or 24 h were significant predictors of brain death, particularly for patients with photomotor reflex in at least one pupil, for whom brain death could be predicted with 85.7% sensitivity and 79.3% specificity. 36 Twenty-four-hour S100B concentration was a significant predictor of circulatory shock within the first 72 h post-admission. 90 S100B also had high predictive value for 6-month outcomes assessed by GOS or GOSE when measured acutely or over a 7-day time-course,91,92 highlighting the dynamic nature of the astrocytic response.
Although less frequently researched as a fluid biomarker compared with S100B, the more specific astrocyte marker GFAP was a high-value predictor of 6-month outcome in two studies when assessed acutely after injury.91,93 A drawback of S100 measurement is the influence of extracranial injuries, which was considered by the consensus group in overall evaluation of this marker. Despite this, S100B was progressed to the single data dictionary, as both S100 and GFAP have increasingly been found to be attractive candidates for clinical prognostic integration94–97 across all TBI severities.94,97 As with routine lab tests, there exists limited evidence for the predictive capacity of S100B and GFAP in pediatric and geriatric populations, and thus their clinical utility may not be relevant for all patient populations.
Markers of direct neuronal and axonal pathology have been more recently investigated; however, predictive capacity has been limited by smaller cohort studies that potentially lack predictive power. This was particularly the case for the markers NFL-1, NSE, and total and phosphorylated tau, for which high-value evidence was found to be lacking. In the case of these markers, progression to the single data dictionary was highly recommended by the consensus group due to the evolving state of evidence for these markers.
Most frequently localized to the soma and dendrites, the neuron-specific marker UCH-L1 was a significant predictor of development of circulatory shock when assessed in serum within 24 h. 90 The consensus panel deemed UCH-L1 to be of particular use in adults, especially given the recent evidence94,97 from the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) and Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) studies that were published after the formal literature search conducted in this study but considered valuable evidence for consensus review.
The axonal cytoskeleton may be damaged in msTBI both directly (as primary shear injury) and indirectly (as secondary injury). A particular target of calpain and other cysteine proteases, 98 αII-spectrin degradation results in breakdown products reflective of successive brain injury processes. We identified spectrin breakdown product 150 (SBDP150) as a high-value predictor of 6-month unfavorable outcome on GOSE in one study. 91 Although promising, the consensus panel rated this a marker of moderate predictive capacity. More evidence will be needed for inclusion of SBDP150 in the AUS-TBI data dictionary, as well as more evidence of feasibility, given the present lack of a robust clinical assay. Although less researched compared with astrocyte markers, these studies nonetheless suggest that biomarkers derived from white matter proteins can be detected and sampled peripherally, with evidence of high predictive value for deleterious outcomes.
Although more difficult to detect due to rapidly changing temporal dynamics, five biomarkers of inflammation 99 and edema 100 were determined to be of high predictive value in our analysis. The platelet-derived CD40 ligand (a member of the tumor necrosis factor family), was highly predictive for 30-day mortality when assessed in serum on the day of msTBI. 101 Likewise, the IL-33 receptor serum soluble ST2 was an independent predictor of mortality when elevated on admission. 102 An early increase in the edemogenic and pro-inflammatory neuropeptide substance P was also a high-value predictor of 30-day mortality, 103 whereas sustained, high IL-6 concentration in the CSF provided highly accurate prediction of poor outcome at 6 months. 104 Using a biomarker discovery approach with dimension reduction via principal component analysis, a panel of 21 inflammatory markers including IL-6, IL-8, and C-reactive protein was highly predictive of GOSE at both 3 and 6 months, with lower 24-h biomarker panel scores indicative of greater recovery. 105 Although this panel was promising, the consensus group was of the opinion that more research was required into the utility and feasibility of collecting and analyzing this predictor panel.
We found two studies to date that demonstrated a genetic influence on outcome from msTBI: presence of the CT+CC genotype of the ATP-binding cassette B1 (ABCB1) C345T was predictive of good outcome at 6 months, 106 whereas the TNFA-308 single nucleotide polymorphism was highly predictive of poor outcome at this time. 107 Although we have identified several promising fluid biomarker candidates for inclusion into the single data dictionary, practical considerations may preclude use of the entire set of predictive biomarkers in future studies.
Since the literature searches were conducted, a number of articles have been published that provide further high-quality evidence of predictive utility of biological markers. For example, utilizing a subset of CENTER-TBI data, Zeiler and colleagues 108 demonstrated that a reduction in cardiovascular (as derived using heart rate in the first 72 h of the injury) and cerebrovascular system (as indexed using intracranial pressure) entropy was associated with death and unfavorable outcome at 6 months, in patients with msTBI. Further, serum biomarkers (including GFAP, NFL, S100B, and UCH-L1) improved outcome prediction after msTBI across the range of imaging severities and especially in patients with TBI with negative findings on CT scans. 109 These results are in alignment with a recent review 5 suggesting it is helpful to use advanced multi-modal biomarkers (neuroimaging or serum in particular), given the heterogeneity of TBI and the complexity of multiple secondary injury mechanisms in msTBI. These findings provide further evidence in favor of including these measures in the AUS-TBI single data dictionary.
Strengths and limitations
This study has notable strengths. Methods were pre-specified in the registration, departures having been transparently reported herein. Searches were exhaustive of the published literature, and records were identified using clear criteria. The consensus processes followed shared methods across the AUS-TBI Initiative, 8 leveraging insights from our initial work. 13
A limitation is the single-person screening of records at title and abstract, and at full-length stage. That noted, the team members screening at title and abstract stage were highly experienced, and all inclusion decisions were confirmed by another team member during data extraction. The likelihood of missed records is judged to be minimal and will be redressed as needed in the planned conversion and updating of this review in the living evidence context. The machine learning approach to title and abstract screening may have resulted in the inadvertent exclusion of relevant records. These can be included in later iterations of this review as living evidence.
Another limitation is the possibility for associations between biological predictors and outcomes to have been missed from included study reports. Although team members were trained and are experienced, reporting standards varied across the included records. It is possible that judgements of predictive value, as they stand, may misrepresent the truth in some cases. Reasons for this include missing information precluding accurate judgements, selective reporting, or team member error. In view of this, we checked all judgements of predictive value for sensibility at the data-cleaning stage. Moreover, the public facing data set (Supplementary Appendix S2) and future iterations of this review (as living evidence) will facilitate amendment as needed.
By nature of a literature search, this study was also limited to the use and inclusion of specific search terms. Our primary focus was to collate information on potentially predictive fluid and imaging biomarkers, and it is likely that there are some markers that were not captured by our search terms. The consensus process was therefore integral as a mechanism to take forward markers that did not arise in the literature search. As an example, the consensus group suggested inclusion of base deficit, for which there is predictive evidence 110 that was not otherwise captured.
A further consideration is that the first iteration of the consensus process was conducted on an incomplete data set. Once data extraction was complete, the complete list of high-value predictive measures from the systematic review was circulated to the consensus group and e-mail feedback was used to prioritize and generate a feasible list for inclusion in the common data elements.
Lastly, the systematic review and consensus process used the definition of msTBI from the Mayo guidelines, 17 in which complicated mild TBI is necessarily included. This may have influenced the results. We evaluated the effect of excluding all studies containing people with complicated mild TBI (5.13%, 28/546) on the sets of high-value predictors and overall predictors identified in the systematic review. These sensitivity analyses indicated a nil effect on the list of high-value predictors and a minimal effect on the overall list. Only brain natriuretic peptide, “time to sample,” “CT angio, lesion,” “CT angio, lesion otherwise labelled,” and “MRI Adams DAI classification” were contributed exclusively by studies including participants with complicated mild TBI, and these were not classified as high-value predictors.
Conclusions
This systematic review and consensus process has identified a substantial number of high-value biomarkers of a range of clinically and socially relevant outcomes following msTBI. These data will be collected as part of the ongoing AUS-TBI workflow wherever feasible. In concert with information from other areas, these data will be integrated in the development of predictive algorithms to personalize care following msTBI. The high predictive value of a number of data elements derived from routine imaging and readily collected biofluids indicates the translation potential of the research. Together, these might facilitate improvements in outcomes for people who experience msTBI.
Transparency, Rigor, and Reproducibility Summary
This study was conducted following a planned protocol. Deviations from protocol have been clearly reported herein. The data set (excluding categorical summary variables) and search strategies are available in Supplementary Appendixes S2 and S3, respectively. Annotated R scripts are available on request, subject to written agreement. Further information is available at the discretion of the corresponding author.
The AUS-TBI Investigators
Tara Alexander, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Vicki Anderson, Psychology Service, The Royal Children's Hospital, Melbourne, Victoria, Australia; Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Ana Antonic-Baker, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Elizabeth Armstrong, School of Medical and Health Sciences, Edith Cowan University, Perth, Western Australia, Australia; Franz E. Babl, Department of Emergency Medicine, The Royal Children's Hospital, Melbourne, Victoria, Australia; Departments of Paediatrics and Critical Care, University of Melbourne, Melbourne, Victoria, Australia; Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Matthew K. Bagg, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; School of Health Sciences, University of Notre Dame Australia, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Centre for Pain IMPACT, Neuroscience Research Australia, Sydney, New South Wales, Australia; Zsolt J. Balogh, Department of Traumatology, John Hunter Hospital and University of Newcastle, Newcastle, New South Wales Australia; Karen M Barlow, Acquired Brain Injury in Children Research Program, Queensland Children's Hospital, Brisbane, Queensland, Australia; Centre for Children's Health Research, University of Queensland, Brisbane, Queensland, Australia; Judith Bellapart, Department of Intensive Care Services, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Faculty of Medicine, University of Queensland, Brisbane, Queensland, Australia; Niranjan Bidargaddi, Flinders Digital Health Centre, College of Medicine & Public Health, Flinders University, Adelaide, South Australia, Australia; Erika Bosio, Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; School of Biomedical Science & School of Medicine, University of Western Australia, Perth, Western Australia, Australia; Peter Bragge, BehaviourWorks Australia, Monash Sustainable Development Institute, Monash University, Melbourne, Victoria, Australia; Michael Bynevelt, School of Surgery, The University of Western Australia, Perth, Western Australia, Australia; Neurological Intervention and Imaging Service of Western Australia, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Karen Caeyenberghs, Cognitive Neuroscience Unit, School of Psychology, Deakin University, Geelong, Victoria, Australia; Peter A. Cameron, National Trauma Research Institute, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; Jacquelin Capell, Australasian Rehabilitation Outcomes Centre & Australian Health Services Research Institute, Faculty of Business and Law, University of Wollongong, Wollongong, New South Wales, Australia; Kevin E.K. Chai, School of Population Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Curtin Institute for Computation, Curtin University, Perth, Western Australia, Australia; Lyndsey E. Collins-Praino, School of Biomedicine, University of Adelaide, Adelaide, South Australia, Australia; D.J. Jamie Cooper, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred, Melbourne, Victoria, Australia; Gill Cowen, School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Louise M. Crowe, Clinical Sciences Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Tim Cudmore, AUS-TBI Lived Experience Advisory Group; Jennifer Cullen, Synapse, Brisbane, Queensland, Australia; James Cook University, Townsville, Queensland, Australia; Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; Kate Curtis, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, New South Wales, Australia; Illawarra Shoalhaven Local Health District, Wollongong, New South Wales, Australia; Illawarra Health and Medical Research Institute, Wollongong, New South Wales, Australia; George Institute for Global Health, Sydney, New South Wales, Australia; Anthony Delaney, Division of Critical Care, The George Institute for Global Health, Sydney, New South Wales, Australia; Malcolm Fisher Department of Intensive Care Medicine, Royal North Shore Hospital, Sydney, New South Wales, Australia; Northern Clinical School, Sydney Medical School, University of Sydney, Sydney, New South Wales, Australia; Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria Australia; Graeme Dibdin, AUS-TBI Lived Experience Advisory Group; Sandra Eades, Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, University of Melbourne, Melbourne, Victoria, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Gary F. Egan, Monash Biomedical Imaging & School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Daniel Y. Ellis, Department of Trauma, Royal Adelaide Hospital, Adelaide, South Australia, Australia; Statewide South Australian Trauma Service, South Australia, Australia; School of Public Health and Tropical Medicine, James Cook University, Queensland, Australia; Ari Ercole, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Cambridge Centre for AI in Medicine, University of Cambridge, United Kingdom; Daniel M. Fatovich, Emergency Medicine, Royal Perth Hospital, University of Western Australia, Perth, Western Australia, Australia; Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research, Perth, Western Australia, Australia; Murray J. Fisher, Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, University of Sydney, New South Wales, Australia; Royal Rehab, Ryde, Sydney, New South Wales, Australia; Mark Fitzgerald, National Trauma Research Institute, Melbourne, Victoria, Australia; Melinda Fitzgerald, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Jennifer Fleming, School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia; Roslyn Francis, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; Belinda J. Gabbe, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Health Data Research UK, Swansea University Medical School, Swansea University, Singleton Park, United Kingdom; Adelle Gadowski, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; John Gilroy, Aboriginal and Torres Strait Islander Research, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Mitchell A. Hansen, Department of Neurosurgery, John Hunter Hospitals and University of Newcastle, Newcastle, New South Wales, Australia; James E. Harrison, College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia; Luke J. Haseler, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Leanne Hassett, Institute for Musculoskeletal Health & Sydney School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Sydney Local Health District, Sydney, New South Wales, Australia; Sarah C. Hellewell, Curtin Health Innovation Research Institute & School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Nedlands, Western Australia, Australia; Amelia J. Hicks, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Brain Injury Research Center, Icahn School of Medicine at Mount Sinai, New York City, New York, United States of America; Andrew F. Hill, College of Science, Health and Engineering, La Trobe University, Melbourne, Victoria, Australia; Andrew J.A. Holland, The Children's Hospital at Westmead Clinical School, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Stephen Honeybul, Department of Neurosurgery, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; Department of Neurosurgery, Royal Perth Hospital, Perth, Western Australia, Australia; Rosalind L. Jeffree, Kenneth G. Jamieson Department of Neurosurgery, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical School, School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Chris Joyce, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Elizabeth Kendall, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; Kate King, John Hunter Trauma Service, John Hunter Hospital, Newcastle, New South Wales, Australia; College of Health, Medicine and Wellbeing, University of Newcastle, Newcastle, New South Wales, Australia; Natasha A. Lannin, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Meng Law, Departments of Neuroscience and Radiology, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Alzheimer's Disease Research Center & Department of Neurological Surgery, Keck School of Medicine, University of Southern California, Los Angeles, California, United States of America; Andrew I.R. Maas, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Adam Mahoney, Trauma Service, Royal Hobart Hospital, Hobart, Tasmania, Australia; 2nd General Health Battalion, Australian Defence Force; Peter Makin, AUS-TBI Lived Experience Advisory Group; Peter Mayhew, AUS-TBI Lived Experience Advisory Group); Alison McDonald (AUS-TBI Lived Experience Advisory Group; Skye McDonald, School of Psychology, University of New South Wales, Sydney, New South Wales, Australia; Stuart J. McDonald, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Ancelin McKimmie, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Robert McNamara, Department of Intensive Care Medicine, Royal Perth Hospital, Perth, Western Australia, Australia; School of Medicine, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Shiv Meka, Department of Health, Government of Western Australia, Perth, Western Australia, Australia; David K. Menon, Division of Anaesthesia, University of Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; Wolfson Brain Imaging Centre, University of Cambridge, Cambridge, United Kingdom; Gary Mitchell, Emergency and Trauma Unit, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Royal Brisbane Clinical Unit, University of Queensland, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Queensland Rugby Union; Brisbane, Queensland, Australia; Rowena Mobbs, Brain & Mind Centre, University of Sydney, Sydney, New South Wales, Australia; Macquarie University, Sydney, New South Wales, Australia; Fatima A. Nasrallah, Queensland Brain Institute, University of Queensland, Brisbane, Queensland, Australia; Virginia F.J. Newcombe, PACE Section, Department of Medicine, Addenbrooke's Hospital, University of Cambridge, Cambridge, United Kingdom; Terence J. O'Brien, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; John H. Olver, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Medicine, Monash University, Melbourne, Victoria, Australia; Gerard M. O'Reilly, National Trauma Research Institute, Melbourne, Victoria, Australia; Emergency and Trauma Centre, The Alfred Hospital, Melbourne, Victoria, Australia; School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Tamara Ownsworth, The Hopkins Centre, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia; School of Applied Psychology, Griffith University, Brisbane, Queensland, Australia; Paul M. Parizel, University of Antwerp, Edegem, Belgium; Department of Radiology, Royal Perth Hospital & University of Western Australia, Perth, Western Australia, Australia; West Australian National Imaging Facility Node, Perth, Western Australia, Australia; Michael Parr, Intensive Care Unit, Liverpool Hospital, University of New South Wales, Sydney, New South Wales, Australia; Intensive Care Unit, Macquarie University Hospital, Macquarie University, Sydney, New South Wales, Australia; Jennie L. Ponsford, School of Psychological Sciences, Monash University, Melbourne, Victoria, Australia; Monash Epworth Rehabilitation Research Centre, Epworth Healthcare, Melbourne, Victoria, Australia; Bruce Powell, AUS-TBI Lived Experience Advisory Group; Patricia Ratajczak, AUS-TBI Lived Experience Advisory Group; Michael C. Reade, Faculty of Medicine, University of Queensland, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia; Joint Health Command, Australian Defence Force, Canberra, Australian Capital Territory, Australia; Sandy Reeder, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Christopher Reid, School of Public Health, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia; Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Julia Robertson, AUS-TBI Lived Experience Advisory Group; Suzanne Robinson, School of Population Health, Faculty of Health Sciences, Curtin University, Perth Western Australia, Australia; Stephen E. Rose, The Australian e-Health Research Centre, Commonwealth Scientific and Industrial Research Organisation, Brisbane, Queensland, Australia; Jeffrey V. Rosenfeld, Department of Neurosurgery, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; F. Edward Hébert School of Medicine, Uniformed Services University of The Health Sciences, Bethesda, Maryland, United States of America; Jason P. Ross, Molecular Diagnostic Solutions, Health and Biosecurity, Commonwealth Scientific and Industrial Research Organisation, Australia; Danette Rowse, AUS-TBI Lived Experience Advisory Group; Nick Rushworth, Brain Injury Australia, Sydney, New South Wales, Australia; Adam Scheinberg, Neurodevelopment and Rehabilitation Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Bridgette D. Semple, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Alfred Health, Melbourne, Victoria, Australia; Department of Medicine, Royal Melbourne Hospital, The University of Melbourne, Melbourne, Victoria, Australia; Sandy R. Shultz, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Grahame K. Simpson, Brain Injury Rehabilitation Research Group, Ingham Institute for Applied Medical Research, Sydney, New South Wales, Australia; John Walsh Centre for Rehabilitation Research, Sydney School of Medicine, University of Sydney, Sydney, New South Wales, Australia; Warwick J. Teague, Trauma Service & Department of Paediatric Surgery, The Royal Children's Hospital, Melbourne, Victoria, Australia; Surgical Research, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; Department of Paediatrics, University of Melbourne, Melbourne, Victoria, Australia; Leanne Togher, Speech Pathology, School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, New South Wales, Australia; Andrew A. Udy, Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia; Department of Intensive Care and Hyperbaric Medicine, The Alfred Hospital, Melbourne, Victoria, Australia; Kirsten Vallmuur, Centre for Healthcare Transformation, Australian Centre for Health Services Innovation, Queensland University of Technology, Brisbane, Queensland, Australia; Jamieson Trauma Institute, Brisbane, Queensland, Australia; Dinesh Varma, Department of Radiology, The Alfred Hospital, Melbourne, Victoria, Australia; Department of Surgery, Monash University, Melbourne, Victoria, Australia; National Trauma Research Institute, Melbourne, Victoria, Australia; James Vickers, Wicking Dementia Research and Education Centre, College of Health and Medicine, University of Tasmania, Hobart, Tasmania, Australia; Janet Wagland, Brightwater Group, Perth, Western Australia, Australia; James Walsham, Intensive Care Unit, Princess Alexandra Hospital, Brisbane, Queensland, Australia; School of Medicine, University of Queensland, Brisbane, Queensland, Australia; Adam J. Wells, Department of Neurosurgery, Adelaide Hospital, Adelaide, South Australia, Australia; Department of Surgery, University of Adelaide, Adelaide, South Australia, Australia; Neurosurgical Research Foundation, Adelaide, South Australia, Australia; Luke Whiley, Health Futures Institute, Murdoch University, Perth, Western Australia, Australia; Perron Institute for Neurological and Translational Science, Perth, Western Australia, Australia; Gavin Williams, Department of Physiotherapy, Epworth Healthcare, Melbourne, Victoria, Australia; Department of Physiotherapy, University of Melbourne, Melbourne, Victoria, Australia; Jodie K. Williams, National Critical Care and Trauma Response Centre, Royal Darwin Hospital, Darwin, Northern Territory, Australia; Roslind Witham, AUS-TBI Lived Experience Advisory Group; David K. Wright, Department of Neuroscience, Central Clinical School, Monash University, Melbourne, Victoria, Australia; Louise York, Australian Institute of Health and Welfare, Canberra, Australian Capital Territory, Australia; Jesse T. Young, Centre for Health Equity, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia; Centre for Adolescent Health, Murdoch Children's Research Institute, Melbourne, Victoria, Australia; School of Population and Global Health, University of Western Australia, Perth, Western Australia, Australia; National Drug Research Institute, Curtin University, Perth, Western Australia, Australia; Heidi Zeeman, The Hopkins Centre, Menzies Health Institute Queensland, Griffith University, Brisbane, Queensland, Australia.
Footnotes
Author Disclosure Statement
MKB has received personal fees for travel or consulting from the Chiropractor's Association of Australia, Memorial University of Newfoundland, Life Ready Health Group, and Active Linc Pty. Ltd. MKB has received research funding from the Australian National Health and Medical Research Council of Australia (NHMRC), MRFF, and Research Training Program (RTP) schemes, and University of New South Wales (UNSW) and Neuroscience Research Australia (NeuRA). DJC occasionally consults to Pressure P/L, with all funds to Monash University. DJC, JP and BJG were supported by NHMRC Investigator Grants (ID2016324, ID1174473, ID2009998). MF is the CEO of the charitable organization Connectivity—Traumatic Brain Injury Australia. VFJN holds a grant with Roche Pharmaceuticals.
Funding Information
This work was funded by the Australian Government's Medical Research Future Fund (MRFF), ID2008223. The funder had no role in study design, data collection and analysis, data interpretation and manuscript writing, or the decision to submit the article for publication.
Authors' Contributions
The authors contributed as follows. Matthew K. Bagg: methodology, project administration, resources, data curation, visualization, formal analysis, writing—original draft; Sarah C. Hellewell: methodology, data curation, writing—original draft, writing—review and editing; Jemma Keeves: data curation, visualization, writing—review and editing; Adelle Gadowski: methodology, project administration, resources, data curation, visualization, writing—review and editing; Ana Antonic-Baker: methodology, project administration, resources, data curation, visualization, writing—review and editing; Ancelin McKimmie: methodology, project administration, resources, data curation, visualization, writing—review and editing; Amelia J. Hicks: methodology, project administration, resources, data curation, visualization, writing—review and editing; Virginia F.J. Newcombe: data curation, writing—review and editing; Karen M. Barlow: data curation, writing—review and editing; Zsolt J. Balogh: data curation, writing—review and editing; Jason P. Ross: data curation, writing—review and editing; Meng Law: data curation, writing—review and editing; Karen Caeyenberghs: data curation, writing—review and editing; Paul M. Parizel: data curation, writing—review and editing; Jacinta Thorne: data curation, writing—review and editing; Melissa Papini: data curation, writing—review and editing; Geena Gill: data curation, writing—review and editing; Jennie L. Ponsford: conceptualization, funding acquisition, methodology, writing—review and editing; Natasha A. Lannin: conceptualization, funding acquisition, methodology, writing—review and editing; Terence J. O'Brien: conceptualization, funding acquisition, methodology, writing—review and editing; Peter A. Cameron: conceptualization, funding acquisition, methodology, writing—review and editing; D. Jamie Cooper: conceptualization, funding acquisition, methodology, writing—review and editing; Nick Rushworth: conceptualization, funding acquisition, methodology, writing—review and editing; Belinda J. Gabbe: conceptualization, funding acquisition, methodology, writing—review and editing; Melinda Fitgzerald: conceptualization, funding acquisition, methodology, project administration, supervision, writing—original draft, writing—review and editing; AUS-TBI Investigators: conceptualization, writing—review and editing.