
Abstract
This systematic review provides a comprehensive overview on the effectiveness of rehabilitation on physical symptoms in patients of all ages with persistent concussion symptoms. PubMed, MEDLINE®, Cochrane library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Embase were searched from January 1, 2012 to September 1, 2023 using terms related to physical post-concussion symptoms. Eligible articles were critically appraised using the Scottish Intercollegiate Guidelines Network (SIGN) and the Quality Assessment Tool. The Grading of Recommendations Assessment, Development, and Evaluation system was applied to rate the quality of evidence. Thirty-two articles were included. Preliminary evidence suggests that transcranial magnetic stimulation improves symptoms in adults, specifically headaches. Young adults reported a significant decrease in physical symptoms following sub-symptom aerobic training as well as cervical spine manual therapy. Tentatively, adults demonstrated improvements in headache symptoms following neurofeedback sessions, and progressive muscle relaxation resulted in a decrease in monthly headaches. Multimodal therapy in adults produced significant change in physical symptoms when compared with usual care. However, no further reduction in physical symptoms was observed when adult patients received a program of care that afforded cervicovestibular rehabilitation with symptom-limited exercise compared with a symptom-limited exercise program alone. Cognitive behavioral therapy demonstrated inconsistent findings for its effects on physical symptoms, specifically headaches. Veterans had a significant change in post-concussive symptoms, specifically headaches, following 3-month use of an interactive smartphone application as compared with standard care. Finally, in a pediatric population, the use of melatonin did not produce any changes in physical persistent concussion symptoms as compared with placebo. Preliminary evidence suggests that various forms of rehabilitative therapies can improve persistent physical concussive symptoms. However, given the methodological limitations in the majority of trials, the results need to be interpreted with caution.
Introduction
Disabilities secondary to traumatic brain injury (TBI) are a major social and economic burden. Patients in Ontario seeking tertiary care for persisting symptoms following mild traumatic brain injury (mTBI) incur health costs of > $110,000,000 annually. 1 The majority of patients who sustain an mTBI recover; however, timelines are highly variable. 2 Additionally, recent findings suggest that up to 82% of patients report at least one symptom 6–12 months following an mTBI. 3 The implications for this are significant for the person, the healthcare system, and society.
Two recent systematic reviews have examined the state of the literature on treatment of persistent concussion symptoms. Rytter and coworkers examined non-pharmacological treatments for persistent (> 4 weeks) symptoms in mTBI and concussion samples. 4 They reported that there is weak evidence for the effectiveness of non-pharmacological interventions. 4 The second review by Makdissi and coworkers examined various treatment modalities in patients with sport-related concussion with persistent symptoms (> 10 days). 5 However, only two trials examined the efficacy of physical therapy on persistent symptoms.
Ultimately, there exists a gap regarding the state of literature on the effectiveness of rehabilitative interventions for physical dominant persistent concussion symptoms, such as headaches, dizziness, phonophobia, nausea, and visual problems. Prior well-designed reviews 4,5 have reported on rehabilitative treatments for persistent concussion symptoms; however, apart from exercise therapy, the reviews' discussion focuses on cognitive-based interventions. This is likely the result of the lack of well-designed clinical trials investigating interventions directed to patient's physical symptoms. Given that headaches are the most common symptom reported by patients following an mTBI, there is a major need to specifically examine the efficacy of interdisciplinary treatments specifically targeting physical symptoms. 6
The present review was developed to better understand the effects of rehabilitation in concussion patients experiencing persistent symptoms. Specifically, the objective was to determine the effectiveness, as measured by clinical outcomes, of non-pharmacological rehabilitation in the management of patients of all ages experiencing persistent physically dominant concussion symptoms, as compared with other interventions such as placebo/sham interventions, or no interventions.
Methods
Registration
This review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on June 12, 2022 (CRD42022341100).
Population
This review examined the best available evidence regarding the effectiveness of non-pharmacological conservative treatments on physical symptoms in patients of all ages experiencing persistent concussion symptoms. The definition used for persistent concussion symptoms was taken from Tator and coworkers, which indicates that persistent symptoms reflect a failure to recover within 1 month. 7
Evaluation of assessment
We restricted our review to articles assessing the effectiveness of non-pharmacological rehabilitation on patients with persistent concussion symptoms. “Rehabilitation” was defined as per the World Health Organization (WHO) as a “set of interventions designed to optimize function and reduce disability in individuals with health conditions in interaction with their environment.” 8
Outcomes
This review focused on either self-rated recovery outcomes (global perceived recovery) or changes in clinical outcomes (e.g., pain and symptom severity scores). Outcomes related to psychological variables (e.g., depression, anxiety, stress scores), administrative outcomes, or outcomes related to costs were excluded from this review.
Inclusion and exclusion criteria
To be included in our review, articles had to fulfill the following inclusion criteria: (1) be written in English, (2) be published from January 1, 2012 to September 1, 2023, (3) be published in a peer-reviewed journal, (4) describe clinical trials examining the effectiveness of treatment in patients of all ages experiencing persistent concussion symptoms, and (5) discuss a patient population who had symptoms beyond 4 weeks as per the definition of post-concussion syndrome by Tator and coworkers. Articles examining mild, moderate, and severe TBI were included only if it was possible to separate data on the populations.
Articles fulfilling any of the following criteria were excluded: (2) publication types including guidelines, letters, editorials, commentaries, unpublished manuscripts, dissertations, government reports, books and book chapters, conference proceedings, meeting abstracts, lectures and addresses, consensus development statements, and guideline statements; (2) study designs including systematic and non-systematic reviews, and case studies; (3) cadaveric or animal trials; and (4) articles solely targeting individuals with cognitive or emotional symptoms. Articles that examined pharmacological treatments or any trial solely examining the effectiveness of any treatments directed to mood/affect or cognitive post-concussion symptoms were excluded.
Data sources
We systematically searched the following electronic databases: MEDLINE®, PubMed, Cochrane Central Register of Controlled Trials, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). Search terms consisted of subject headings specific to each database (e.g., MeSH in MEDLINE and PubMed) and free text words relevant to concussion, post-concussion, headache, therapy, treatment, and rehabilitation (Supplementary Appendix I). In addition, the reference lists of included articles and related systematic reviews were screened to identify any article that we may have missed using our search strategy.
Study selection
Articles were screened for relevance in different phases. The first phase involved screening titles and abstracts for relevance and possibly relevant citations based on the aforementioned inclusion and exclusion criteria. The full text of potentially relevant articles was then independently screened by two reviewers (N.M. and S.G.) to determine final article selection. Discrepancies were resolved by consensus between the two reviewers. Disagreements were resolved by a third reviewer.
Risk of bias
Two independent reviewers assessed risk of bias with the Scottish Intercollegiate Guidelines Network (SIGN) criteria for randomized controlled trials (RCTs), cohort studies, and case-control studies (Table 1). 9 The tool includes seven items divided into six domains of bias: selection, performance, detection, attrition, reporting, and any other bias. A summary assessment of risk of bias within a study was then made by grading a study as being of high, acceptable, or low quality using the SIGN criteria. For case series, single-armed observational studies, and retrospective observational studies the Effective Public Health Practice Project Quality Assessment Tool was utilized (Table 2). The tool evaluates studies under the headings of selection, design, confounders, blinding, data collection, and withdrawals/dropouts, generating a final global rating for quality assessment of weak, moderate, or strong. 10 Consensus between reviewers was reached through discussion. An independent third reviewer (S.K.) was included to resolve disagreements when consensus could not be reached.
Risk of Bias Rating for Controlled Trials Based on the Scottish Intercollegiate Guidelines Network (SIGN) Criteria
Y, yes; N, no; U, unclear; N/A: not applicable.
Risk of Bias of Non-Controlled Trials Based on Either Scottish Intercollegiate Guidelines Network (SIGN) Criteria or the Quality Assessment Tool for Quantitative Studies (QAT)
Y, yes; N, no; U, unclear; N/A, not applicable.
Data extraction
The reported data were extracted in a two-step process. Firstly, the lead author (N.M.) extracted the data from accepted articles to build the evidence tables. Author name, year of publication, number of participants, description of intervention, (where applicable) description of control/comparison interventions, subjects under investigation, primary outcomes, and key findings including: (1) summary statistics for each group, and (2) effect estimate and precision (when reported). Second, the two reviewers (N.M. and S.G.) independently reviewed the accuracy of the extracted data by referring to the original articles.
Quality of evidence assessment
In order to rate the quality of evidence, the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system was applied to the articles' primary outcome measure. 11 The assessment was based on the five downgrading factors (risk of bias, inconsistency, indirectness, imprecision, and publication bias) and three upgrading factors (large effect, dose response, and all plausible confounding). In brief, the two reviewers independently assessed the quality of evidence level. Assessments were then compared during a formal meeting during which consensus with regard to the strength of evidence was reached (high, moderate, low, or very low). The quality of evidence level, coupled with the risk of bias score, was taken into consideration in the Results/Discussion section. 12
Study homogeneity was assessed via visually examining the data extraction tables. Secondary to the considerable variability in subjects, therapeutic interventions, and definitions of post-concussion syndrome or persistent symptoms, meta-analysis was not possible. A narrative synthesis was conducted with articles grouped according to therapeutic intervention utilized.
Statistical analysis
The agreements among the two reviewers for the screening of articles were computed and the kappa coefficient (ĸ) reported. 13,14 The percentage agreement was calculated for classifying controlled trials as high quality, acceptable, or low quality and for classifying non-controlled trials as strong, moderate, or weak following independent critical appraisal. We considered conducting a random effect analysis if the trials were homogeneous. However, because of the clinical heterogeneity of the articles (population, treatment rendered, use of control groups or comparison, outcome measures used), no meta-analysis was performed. 15
Reporting
This review complies with the Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Supplementary Appendix II). 16
Results
Study selection
Overall, 2015 articles were screened for eligibility and 241 duplicates were excluded. Titles and abstracts of 1773 articles were screened for eligibility and 52 articles were recovered for full text evaluation (Fig. 1). Following full-text review, a total of 20 articles were excluded for ineligible study design or publication type (7 citations), intervention other than rehabilitation (4 citations), inclusion of participants outside the scope of the review (5 citations), and primary outcome outside the scope of the review (3 citations). One RCT that was deemed to be at high risk of bias in accordance with the SIGN checklist (1 citation) was also excluded. Therefore, 32 articles were considered acceptable and were included in the analysis.
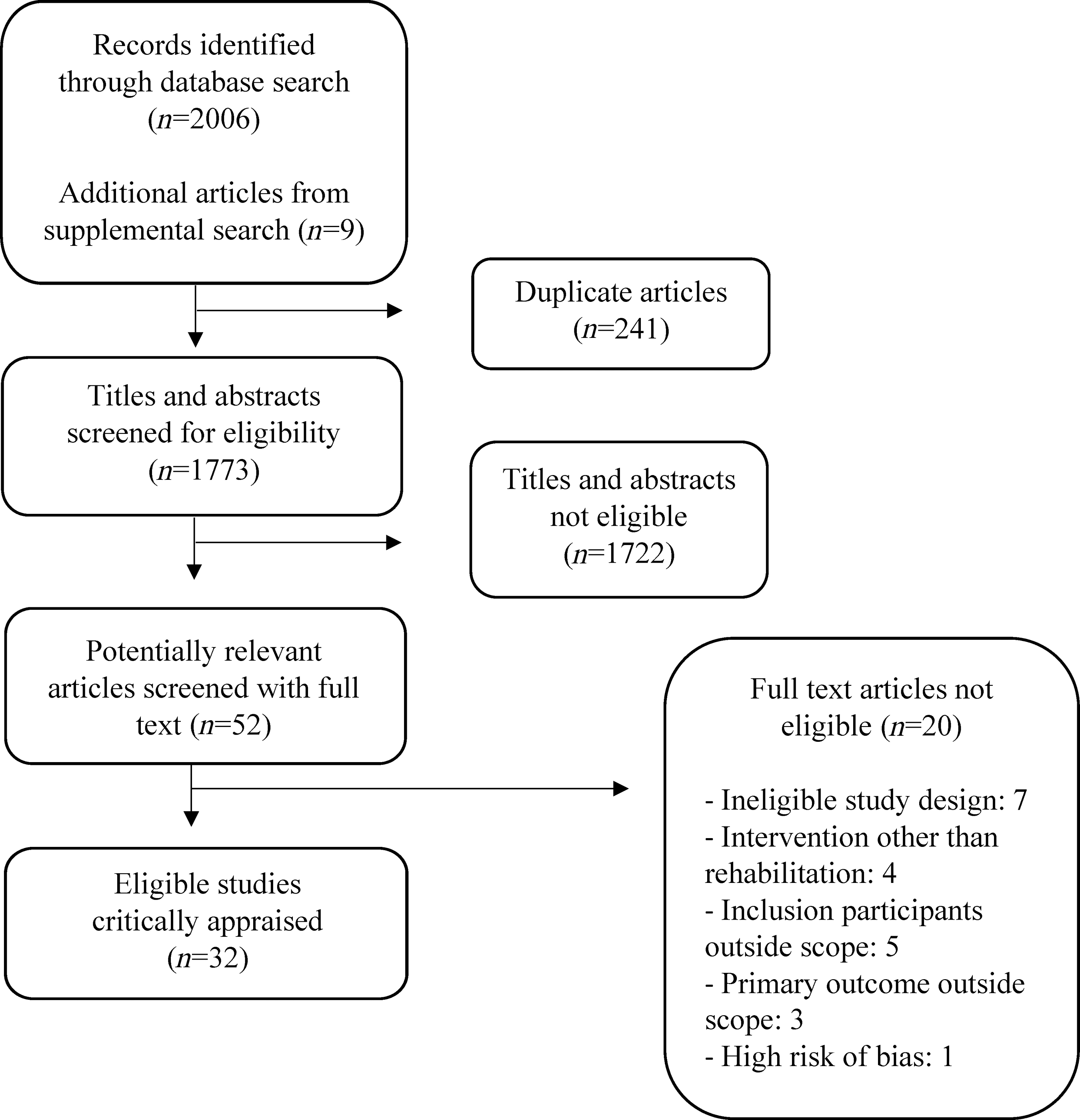
Identification and selection of articles on the effectiveness of non-pharmacological conservative treatments on somatic symptoms in patients with post-concussion syndrome.
The inter-rater agreement for screening of articles was k = 0.74. The agreement for classifying articles as high quality, acceptable, or low quality was 89%. Consensus was achieved without the need for a third reviewer.
Study characteristics
Various forms of rehabilitation were identified, including repeated transcranial magnetic stimulation (rTMS), 17 –25 aerobic exercise, 26 –28 cognitive behavioral therapy (CBT), 29 –31 physical therapy directed to the cervical spine, 32 –38 multimodal rehabilitative interventions, 39 –43 neurofeedback training, 44,45 progressive muscle relaxation (PMR), 46 interactive smartphone application, 47 and the effects of melatonin supplementation. 48
Risk of bias assessment
All acceptable RCTs used clear research questions, and apart from one study, 26 achieved similarities at baseline between groups. The majority of articles reported on adequate concealment, methodology of randomization, and intention-to-treat analysis. The follow-up rate for all RCT articles, apart from two articles, 21,31 was <25%. All acceptable non-controlled trials used a clear research question. A minority of trials utilized blinding of outcome assessors and participants; however, the vast majority of trials did not report on intention-to-treat analysis, nor did the majority of trials report on consistency of intervention or on unintended interventions. The majority of trials did not report sample size calculations, although their studies were properly powered. Additionally, of the 32 included trials, only 18 utilized validated and reliable outcome measures for this population, such as the Rivermead Postconcussion Questionnaire.
Assessment of evidence
After reviewing all relevant trials, only a single RCT was rated “high” in regards to the primary outcome measure addressed (self-reported Post-concussion Symptom Inventory Score). Half of the reviewed RCT trials were rated as “moderate” (8/16) regarding primary outcome measures (Postconcussion Symptom Inventory [PCSI], Rivermead Postconcussion Questionnaire [RPQ], medical clearance, Numerical Rating Scale [NRS]), with downgrading resulting from issues with risk of bias and imprecision (Table 3). A minority of RCT trials were rated “low” (6/16) regarding primary outcomes (RPQ, change in headache scores, NRS) with downgrading resulting from issues with risk of bias and imprecision. One RCT trial was rated very low regarding primary outcome (fMRI activation and number of symptoms) with downgrading resulting from risk of bias and imprecision. The majority of non-controlled trials were rated “very low” (14/16) regarding primary outcomes (Global Improvement Scale [GIS], Numerical Pain Rating Scale [NPRS]/NRS, Postconcussion Symptoms Scale [PCSS], exercise tolerance test), with downgrading as a result of issues with risk of bias, imprecision, and inconsistency. Two non-controlled trials were rated as “low” regarding primary outcome measures (patient reported self-dizziness and headache frequency) with downgrading as a result of risk of bias and imprecision (Table 3).
Summary of Findings of Primary Outcomes and Quality Assessment
p < 0.05; ^p < 0.0004.
rTMS, repetitive transcranial magnetic stimulation; RPQ, Rivermead Postconcussion Questionnaire; PCS, Post-concussion syndrome; FU1, follow-up 1 month; FU2, follow-up 2 months; post-tx, post-treatment; CBT, cognitive behavioral therapy; SD, standard deviation; NDI, Neck Disability Index; DHI, Dizziness Handicap Inventory.
Summary of evidence
rTMS
All trials investigated the effectiveness of rTMS on an adult population. Evidence suggests that this form of rehabilitation, as measured by the RPQ, NRS, or self-reported headache intensity/frequency, shows statistically significant improvements (Table 3). Across all RCTs, the use of rTMS was consistently compared with a sham TMS treatment. Evidence from the five non-controlled trials also suggests that rTMS reduces persistent post-concussion symptoms, specifically headache intensity and frequency as measured by the NPRS, PCSS, RPQ, and participant-reported headache intensity/frequency (Table 3). The quality of the evidence for rTMS, as rated by the GRADE criteria, ranged from very low to moderate. The reasons for downgrading were risk of bias, imprecision, and publication bias secondary to specific issues with sample sizes, study design, and a lack of reporting on confidence intervals.
Aerobic exercise
Leddy and coworkers identified that after 12 weeks of sub-symptom aerobic training, adult participants reported a significant decrease in self-reported symptoms. 26 Sub-symptom aerobic training required participants to exercise aerobically for 20 minutes six times per week, at an intensity of 80% of the heart rate attained when their symptoms were aggravated on a baseline treadmill exertion test. The comparison group were advised to perform a 12-week low-impact breathing and stretching program. Kurowski and coworkers also reported 6 weeks of sub-symptom aerobic exercise training lead to significant reductions in post-concussion symptom inventory when compared with a full-body stretching program; however, they studied an adolescent population. 27 Again, participants were instructed to perform sub-symptom exercise aerobically 5–6 days per week. The comparison group was instructed to perform upper and lower body stretching for 6 weeks. Lastly, Leddy and coworkers showed via a non-controlled trial that adult participants who engaged in 5–6 days of sub-symptom aerobic exercise had significant change in post-concussion symptoms via a graded symptom check list (Table 3). 28 The quality of the evidence, as rated by the GRADE criteria, for aerobic exercise ranged from very low to moderate. The reasons for downgrading were risk of bias and imprecision secondary to issues with study design and lack of reporting on confidence intervals.
Physical therapy directed to the cervical spine
One RCT 32 demonstrated that physical therapy produced a statistically significant improvement in physically dominant persistent concussion symptoms. Both the intervention and control groups received weekly session with a physiotherapist for 8 weeks. The intervention group received additional cervical spine and vestibular rehabilitation.
Of the six non-controlled trials, four of them were descriptive case series. All trials investigated changes in post-concussion symptoms as measured by various patient-generated outcome measures after manual therapy directed to the cervical spine. The articles tentatively suggest that manual therapy directed to the cervical spine is effective at reducing physical persistent concussion symptoms in adults (Table 3). The quality of the evidence for physical therapy directed to the cervical spine, as rated by the GRADE criteria, ranged from very low to moderate. The reasons for downgrading were risk of bias, imprecision, and publication bias secondary to specific issues with sample sizes, study design, and a lack of reporting on confidence intervals.
Neurofeedback
Two non-controlled clinical trials evaluated the effectiveness of neurofeedback on physical post-concussion symptoms in adults. Walker and coworkers afforded neurofeedback therapy for 26 adult patients with persistent symptoms. 44 Participants were given five training sessions designed to instruct them on how to normalize abnormal quantitative electroencephalography (qEEG). Overall, 88% of participants, after a mean of 19 sessions, had a change in global improvement score of ≥50%. 44 Elbogen and coworkers examined the effectiveness of neurofeedback on physical post-concussion symptoms with a portable EEG in 41 veterans with chronic pain following an mTBI. 45 They reported that after a mean of 33 neurofeedback sessions over a course of 3 months, participants had a statically significant change in self-reported pain intensity. The quality of the evidence for neurofeedback, as rated by the GRADE criteria, ranged from very low to moderate. The reasons for downgrading were risk of bias, imprecision, inconsistency, and publication bias secondary to issues with either sample sizes, study design, study procedures, or a lack of reporting on confidence intervals.
Progressive muscle relaxation (PMR)
One non-controlled clinical trial examined the feasibility and impact of PMR on persistent headaches following a concussion in adults. Usmani and coworkers reported that despite the lack of compliance, participants on average reported a decrease in monthly headaches from 15 at baseline to 9.7 by the 3rd month follow-up. 46 The quality of the evidence for PMR was very low, as rated by the GRADE criteria. The reasons for downgrading were risk of bias and imprecision secondary to issues with study design and a lack of reporting on confidence intervals.
CBT
Two of the three RCTs 29,30 examined the impact of CBT on persistent concussion symptoms as compared with waitlist controls in adults. Both articles failed to show any significant change post-treatment for physical dominant symptoms as measured by the RPQ or a headache diary. McGeary and coworkers compared CBT to usual care in veterans with post-traumatic headaches attributed to mTBI. They found a significant improvement in participants' headaches as compared with usual care and cognitive processing therapy. 31 The quality of the evidence for CBT ranged from moderate to low, as rated by the GRADE criteria. The reasons for downgrading were risk of bias, and imprecision secondary to issues with study design (lack of concealment in blinding), and a lack of reporting on confidence intervals.
Multimodal rehabilitation
The majority of trials utilizing multimodal rehabilitative care were randomized (3/5). Thastum and coworkers investigated the effects of an 8-week program inclusive of CBT in adults, as applied by a neuropsychologist, occupational therapist, and physiotherapist, with gradual return to activities. 40 The authors found a significant change in RPQ score when compared with enhanced usual care (EUC). Rytter and coworkers compared a 22-week program that included neuropsychological treatments, group therapy, and individualized exercise training (S-REHAB), with usual care in adults. 39 They showed that the S-REHAB significantly reduced symptoms as measured by the RPQ when compared with usual care. 39 Finally, Langevin and coworkers examined the effects of a symptom-limited aerobic exercise program combined with cervicovestibular rehabilitation as compared with symptom- limited aerobic exercise training alone. 43 They found that in adults with persistent symptoms, there was no additional benefit noted for the group randomized to receive the additional cervicovestibular rehabilitation. However, they reported that both groups demonstrated significant improvements from baseline on the Postconcussion Symptom Scale following the 6-week programs, which remained significant at the 26-week follow-up assessment. 43 The quality of the evidence for multimodal rehabilitation ranged from very low to moderate, as rated by the GRADE criteria. The reasons for downgrading were risk of bias, imprecision, and publication bias secondary to specific issues with sample sizes, study design (observational trials), and a lack of reporting on confidence intervals.
Smartphone application
One RCT examined the effectiveness of an interactive smartphone application, Concussion Coach, on veterans' persistent concussion symptoms. 47 Belanger and coworkers compared the Concussion Coach application to treatment as usual over a 3-month period. They reported a significantly greater probability (odds ratio of 1.29) of reduced persistent concussion symptoms for those randomized to the smartphone application as compared with treatment as usual. 47 The quality of the evidence for smartphone application was moderate, as rated by the GRADE criteria. The reasons for downgrading were risk of bias and inconsistency
Melatonin supplementation
One RCT examined the effectiveness of melatonin supplementation on post-concussive symptoms in a pediatric population. The trial compared 3 mg or 10 mg supplementations with a placebo. The changes observed were not statistically significant between the placebo and either treatment group. 48 Additionally, there were no group differences on actigraphy sleep parameters after treatment, as measured by a wrist-worn accelerometer. The quality of the evidence for melatonin supplementation was high, as rated by the GRADE criteria.
Weight of evidence
The quality of the evidence ranged from “very low” to “high.” Excluding the single trial investigating the effects of melatonin supplementation, multimodal rehabilitation consistently demonstrated the highest level of evidence. Three of the five trials were found to be among the strongest methodological trials in this literature search, illustrating preliminary evidence for improved physical persistent concussion symptoms. 39,40,43 The quality of the evidence of the three trials was “moderate,” and downgrading for these trials was the result of risk of bias or imprecision.
Adverse events
Eleven of the 32 acceptable articles reported on adverse events (Table 3). 22 –24,27,28,30,31,37,40,45,48 No serious adverse events were reported.
Discussion
There have been well-executed reviews on the topic of rehabilitation in those with persistent concussion symptoms; however, the focus of discussion in prior reviews has been on the effects of cognitive therapies for alleviating cognitive, mood, or overall symptoms.
It is well documented that the potential source for the cluster of concussion symptoms includes the brain, neck, vestibular system, oculo-motor system, and affective disorders. 49,50 To date, clinical trials have directed management of persistent concussion symptoms toward addressing cognitive impairments. By broadening the potential origin of symptoms, clinicians can be better directed to determine most probable sources of symptoms and therefore can more accurately direct treatment.
Other systematic reviews
The results of this review agree with those of previous reviews. 4,5,51,52 In their review, Rytter and coworkers reported that there is weak evidence for the benefits of graded physical exercise, vestibular rehabilitation, manual therapy to the neck, psychological treatment, and interdisciplinary rehabilitation. 4 Makdissi and coworkers reported that there is preliminary evidence for the benefits of symptom-limited exercise, targeted physical therapy, and CBT. 5 Bergersen and coworkers noted several methodological limitations resulting in avoidance to make strong treatment recommendations after reviewing the literature for effective psychotherapies for persistent concussion symptoms. 51 Finally, most recently, Möller and coworkers reported that problem-solving therapy and CBT have been shown to improve depressive symptoms and psychological function, and that interdisciplinary rehabilitation reduces residual symptoms. 52 Considerable methodological limitations prevented strong recommendations from the reviews for any therapy studied.
Clinical implications
This review has shown that there is preliminary evidence for the effective treatment of physically dominant symptoms in those with persistent concussion symptoms. It is unfortunate that currently, the majority of trials investigating the efficacy and effectiveness of non-pharmacological treatments for persistent physical concussion symptoms have been non-controlled clinical trials with systematic errors in methodology, or case studies leading to caution when interpreting the results.
Strength and limitations
This review has several strengths. We defined explicit inclusion and exclusion criteria to identify relevant articles from the searched literature. In addition, we had two reviewers independently screen and critically appraise the trials to minimize error and bias. Lastly, the two reviewers used well-accepted and valid sets of criteria for critically appraising controlled trials and multi-arm cohort trials with the SIGN criteria 9 and used the Quality Assessment Tool for all other non-controlled trials. 10
This review also has a number of limitations. First, scientific judgment varies among reviewers, which may affect the process of study appraisal. Training on the use of standardized critical appraisal tools and the use of a consensus process to reach decisions were done to help avoid bias. Second, the fact that a considerable number of the primary and secondary outcome measures utilized by the various trials, although standardized, were derived from the participants' own self-report, is an additional limitation. This subjective nature of the data may have influenced the results. However, given that the therapeutic strategies were chosen on the basis of the subjective complaints of the participants, this was considered a strength to the internal validity of the study. Third, for feasibility reasons, this review did not attempt to search grey literature.
Recommendation
The majority of trials suffer from significant methodological flaws limiting the generalizability and interpretation of the results. More specifically, the majority of articles reported here consistently failed to include a treatment control group, did not recruit sufficient participants to properly power the trial, or failed to use reliable and validated clinical outcome measures.
Future research should be focused on conducting RCTs comparing multimodal forms of care with current standards of care utilizing validated and reliable clinical outcome measures. Choice of outcome measures is important, especially with regard to interventional trials. They should ideally be responsive to the intervention and have enough resolution to answer the research question posed. It is also essential to apply validated and reliable clinical outcome measures, such as the Rivermead Post-Concussion Questionnaire or the Post-Concussion Symptom Scale, when assessing for change post-care. Unfortunately, a significant minority of trials are electing to use self-reported pain (numerical pain rating scale) or functional neuroimaging in isolation, which both come with drawbacks. Further, to assist with patient demographic diversity and generalizability, the study population should be recruited from large concussion assessment centers, similar to several found in this review. 18,20,22 –24,26 –33,39 –41,43,44,46 –48 We strongly encourage future trials to adopt the most recent presented definition of post-concussion syndrome by Tator and coworkers, which requires a participant to report any three or more symptoms lasting at least 1 month following the diagnosis of a concussion. 7 This can assist with creating homogeneity across study groups with respect to biological, psychological, and social factors. Lastly, for interventional trials, authors are encouraged to “isolate” the intended effects of the studied intervention(s). This can improve the specificity of the study and consequently improve the visibility.
Conclusion
The best available evidence on rehabilitative treatments of persistent concussion symptoms suggests that various forms of non-pharmacological therapy may provide a reduction in physical symptoms. However, significant methodological limitations of the current trials preclude us from making strong recommendations. Instead, given the encouraging preliminary findings from the multimodal therapy trials, we suggest further research in this area.
Transparency, Rigor, and Reproducibility Summary
The study was registered with PROSPERO on June 12, 2022 (CRD42022341100). A search of the literature was conducted in PubMed, MEDLINE, the Cochrane library, CINAHL, and Embase using terms related to physical post-concussion symptoms. After careful review of relevant full-text articles, 32 studies were included for analysis. Because of study methodology heterogeneity, we could not perform a meta-analysis.
Footnotes
Authors' Contributions
N.M. was responsible for conceptualization, methodology, formal analysis, investigation, writing – original draft, writing – review and editing, and visualization. S.G. was responsible for investigation, and writing – review and editing. M.R.P. was responsible for conceptualization, writing – review and editing, and supervision. S.K. was responsible for conceptualization, writing – review and editing, and supervision. All authors read and approved the final manuscript.
Funding Information
No funding was received for the support of the research, authorship, and/or publication of this article.
Author Disclosure Statement
Milos R. Popovic is co-founder, director, and shareholder in the companies MyndTec Inc. and ERNE Inc. He is also a consultant for the company Fourier Intelligence. The other authors have no competing interests to disclose.
Supplementary Material
Supplementary Appendix I
Supplementary Appendix II
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.