
Abstract
Mild traumatic brain injury (mTBI) is a common condition seen in emergency departments worldwide. Blood-based biomarkers glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) are recently U.S. Food and Drug Administration–approved for the prediction of intracranial lesions on head computed tomography (CT) scans in mTBI. We evaluated the diagnostic performance of GFAP and UCH-L1 in a Dutch cohort using the i-STAT TBI assay. In a multi-center observational study, we enrolled 253 mTBI patients. Head CT scans were scored using the Marshall classification system. Logistic regression models were used to assess the contribution of biomarkers and clinical parameters to diagnostic performance. Detection of UCH-L1 and GFAP resulted in a sensitivity of 97% and specificity of 19% for CT positivity in mTBI patients, along with a negative predictive value of 95% (88-100%) and a positive predictive value of 27% (21-33%). Combining biomarker testing with loss of consciousness and time to sample increased specificity to 46%. Combined testing of UCH-L1 and GFAP testing resulted in possibly more unnecessary CT scans compared with GFAP testing alone, with only limited increase in sensitivity. This study confirmed high sensitivity of GFAP and UCH-L1 for CT abnormalities in mTBI patients using the i-STAT TBI test. The results support the potential use of GFAP and UCH-L1 as tools for determining the indication for CT scanning in mTBI patients, possibly offering a cost- and time-effective approach to management of patients with mTBI. Prospective studies in larger cohorts are warranted to validate our findings.
Introduction
Traumatic brain injury (TBI) is one of the most common neurological diseases seen in emergency departments (EDs) worldwide. 1 The incidence of TBI is estimated to be 200-790 per 100,000 population. 1 In addition, the rates of TBI-related ED visits have been increasing over the past years. 2 Most TBIs (90%) are mild (mTBI), defined by a Glasgow Coma Scale (GCS) score between 13 and 15 at the initial presentation. Between 6% and 38% of patients with mTBI have an identifiable intracranial abnormality on acute head-computed tomography (CT) scan. 3 –11 Moreover, only a small percentage 0.7%-8.7% of CT-positive mTBI cases required neurosurgical intervention. 3 –14 In the Netherlands, the CT in Head Injury Patients (CHIP) decision rule for the detection of (intra)cranial findings in adult patients following minor head injury is used. The CHIP decision rule is highly sensitive (97%) for the detection of intracranial abnormalities. However, an external validation of the CHIP decision rule in the Netherlands found a potential reduction of CT scans of only 21% compared with the scanning of all patients that could still be further improved. 15 Therefore, research has focused on blood-based biomarkers to improve the specificity of current decision rules to further reduce unnecessary head CT scans aiming to minimize radiation exposure, reducing length of stay in the ED, and a possibly reducing in healthcare costs.
Glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) are among the most frequently studied biomarkers for TBI. Recently, Bazarian and colleagues demonstrated a high negative predictive value (NPV) of 99.3% for the prediction of intracranial lesions with combined measurement of GFAP and UCH-L1 using the i-STAT Point-Of-Care (POC) device. 16 These data resulted in U.S. Food and Drug Administration (FDA) clearance of GFAP and UCH-L1 to aid in the decision making whether head CT should be performed after a mTBI. In Europe, serum S100 calcium-binding protein (S100B) was included as a screening tool for the assessment of mTBI in Scandinavian guidelines. 17 Recently, the French guidelines for the management of patients suffering from mTBI also suggest the use of UCH-L1 and GFAP as biomarkers to limit the number of head CT scans. 18 In the Netherlands, blood-based biomarkers have not yet established their utility in routine clinical applications and are not adopted in national guidelines.
Point-of-care testing (POCT) of GFAP and UCH-L1 is available since 2021, paving the way for rapid rule-out of intracranial lesions—enabling early treatment and discharge decisions. Current iterations of the i-STAT POC TBI test enable the quantification of GFAP and UCH-L1 within 15 min from plasma, with ongoing development for whole–blood POC testing. 19 Given the accessibility of GFAP and UCH-L1 POC testing, the length of stay in the ED of individuals suffering from mTBI could potentially be reduced.
Our goal is to evaluate whether the reported sensitivity and specificity of the i-STAT POC TBI test by Bazarian and colleagues are comparable in a Dutch multi-center ED population of patients with mTBI. 16 In addition, we aimed to improve prediction of intracranial abnormalities after mTBI using demographic, clinical characteristics together with GFAP and UCH-L1 results.
Methods
Participants
Inclusion of patients in AIM-TBI study (Dutch trial register no. NL8484) took place between January 2020 and December 2022 at the ED of two level 1 trauma centers in the Netherlands: University Medical Centre Groningen (UMCG) and the Medisch Spectrum Twente (MST). The study enrolled participants aged 18 or above with mTBI according to the (former) guidelines established by the American Congress of Rehabilitation Medicine. 20 This definition entails a GCS score ranging from 13 to 15, along with a maximum duration of loss of consciousness (LOC) of 30 min and/or post-traumatic amnesia (PTA) lasting no more than 24 h. Selection of patients eligible for a head CT scan was based on the CHIP-decision rule. 15 Exclusion criteria encompassed significant neurologic or psychiatric comorbidity, prior hospital admission for TBI, drug abuse, mental disability, language barriers, or illiteracy that would hinder the comprehension and completion of questionnaires. All patients were seen by a Neurology Resident at the ED who carried out eligibility checking using the above-mentioned criteria. Blood samples were collected with deferred consent during trauma evaluation. Prior to discharge at the ED, or ward, patients were fully informed and written consent was obtained. Secondary exclusions (e.g., based on new information on drug use or comorbidity) are depicted in Figure 1. The AIM-TBI study was approved by the Medical Ethical Committee of the UMCG (METc 2018/681), and all participants provided written informed consent. All study procedures were performed in accordance with the declaration of Helsinki.
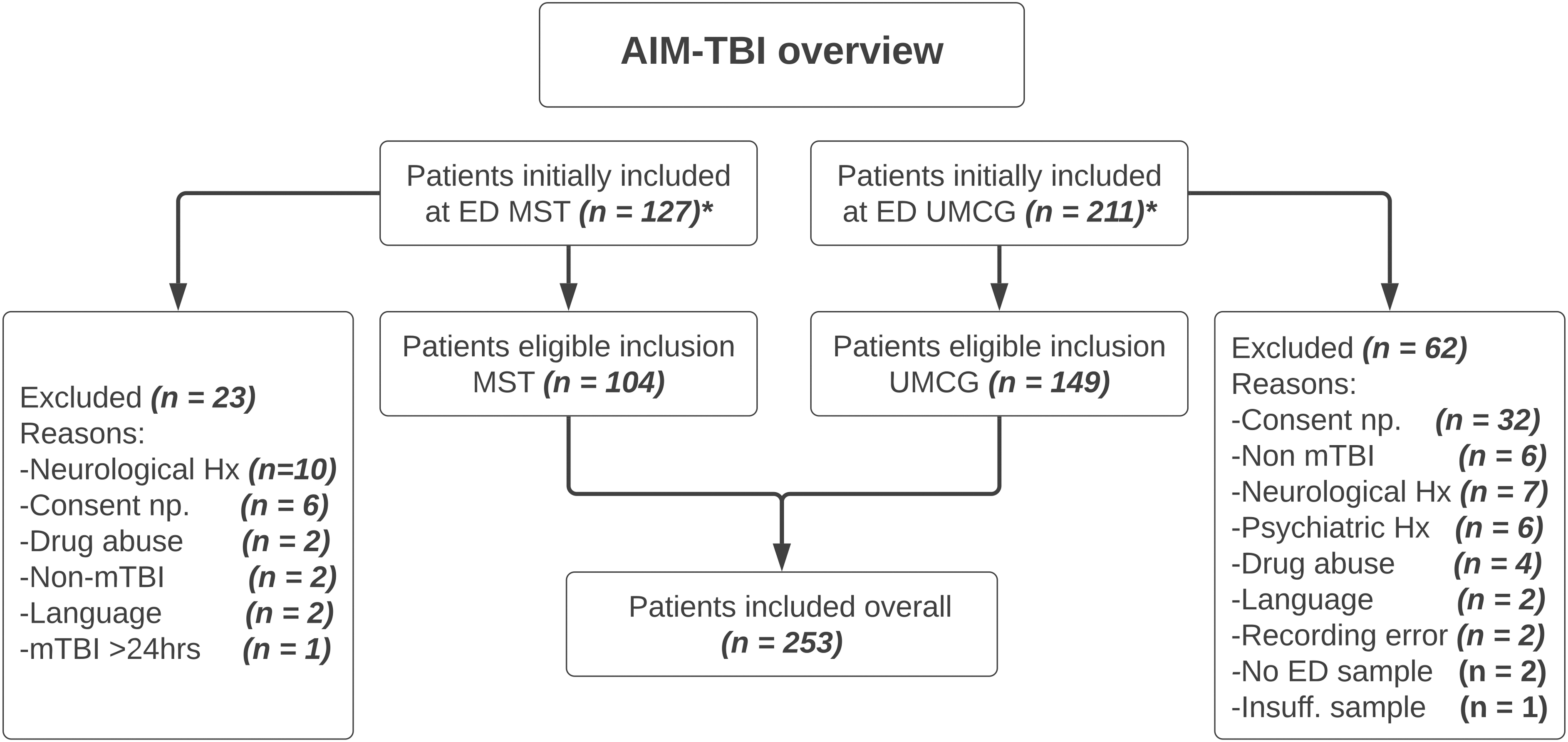
Flowchart of inclusion of participants for this study stratified by participating center. *Initial inclusion was based on deferred consent.
Data acquisition time-points
Blood samples were collected within 24 h of trauma at the ED. During ED visit, a range of injury characteristics were recorded: the presence of LOC and PTA, initial GCS score, alcohol intoxication, injury mechanism, and the presence of peripheral trauma (any fracture below the head).
CT scanning
Patients meeting the criteria for CT scanning as outlined in Dutch guidelines underwent head CT scans. CT scans were scored according to the Marshall score. 21 Scores were dichotomized as negative (Marshall score 1, no abnormalities) or positive (Marshall score >1, indicating lesions, compressed cisterns, or midline shifts).
Blood sample handling
Venous blood samples were obtained in a 10 mL vacutainer K2E (EDTA) (BD-Plymouth, UK). Blood samples were centrifuged at 1300 g and plasma was stored at -80°C. Plasma samples were subjected to a single freeze-thaw cycle.
POCT analysis
The i-STAT mTBI plasma test cartridge consists of immunoassays for GFAP and UCH-L1 which are simultaneously measured. 16 Samples were measured retrospectively within 2 days on 12 different i-STAT Alinity systems, minimizing inter-day variation and inter-operator variation. Plasma samples were thawed and centrifuged at 10,000 RCF for 10 min before measurement. Measurement of GFAP and UCH-L1 was performed according to manufacturer's instructions. In short, we applied 20 μL plasma into the i-STAT TBI plasma test cartridge, closed the lid and inserted the cartridges into the i-STAT Alinity analyzer. Two levels of i-STAT TBI control material, L1 (i-STAT TBI Control Level 1) and L2 (i-STAT TBI Control Level 2), were measured to ensure cartridge quality. Further, we conducted measurements of both control samples (L1 and L2) during each day of analysis to ensure stability of cartridges and analyzers. The reportable range of GFAP and UCH-L1 is 30-10,000 pg/mL and 200-3200 pg/mL, respectively. Manufacturer's recommended cut-off values were used for UCH-L1 and GFAP, 360 pg/mL and 30 pg/mL respectively. Values below the reportable range were replaced by the lower limit of quantification. Values above the reportable range were replaced by the upper limit of quantification.
Statistical analysis
Baseline demographic and clinical characteristics were presented as means ± standard deviation (SD) or proportions n with corresponding percentages (%). Non-normally distributed data were presented as medians [min – max]. Assessment of normality of continuous variables was assessed visually with histograms and normal probability plots (Q-Q plots) and quantitatively using the Shapiro-Wilk test. Biomarker data was non-normally distributed. Therefore, group differences were assessed with the Mann-Whitney U test.
Diagnostic performance of UCH-L1, GFAP and both markers combined was assessed by calculating the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and likelihood ratio (LR). Logistic regression modeling was used to assess the potential contribution of clinical and demographic parameters to the performance of the biomarker panel. The aim of the model was to identify a combination of predictors that would optimize specificity at a sensitivity ≥95%. To ease interpretation of the model, participants were grouped into tertiles for both GFAP and UCH-L1, based on their concentration. The base model included grouped biomarker data, which was forced into all subsequent models. Next, the base model was extended iteratively with all possible combinations of clinical parameters available (age, sex, LOC, PTA, alcohol intoxication, high energy trauma mechanism, time to sample, GCS score and the presence of peripheral injury). Specificity of the baseline model and best model at the optimal threshold was compared using McNemar's chi-squared test. Finally, we investigated the influence of time to sample on the concentrations of GFAP and UCH-L1. Given that the upper quartile of time to sample was 3 h, we compared biomarker group differences between CT- and CT+ patients for patients presenting before 3 h and after 3 h post injury. Two-tailed p values ɑ = 0.05 were considered statistically significant. Data were analyzed and visualized using Python (version 3.8.13) and associated libraries.
Results
A total of 253 mTBI patients were enrolled in this study (Fig. 1), demographic and clinical characteristics of participants are described in Table 1. Traumatic head CT abnormalities (CT+) were identified in 59 patients (23%, Marshall score >1). Most participants were enrolled in the UMCG (59%) but the proportion of CT+ patients enrolled at both centers did not significantly differ (X 2 = 0.46, p = 0.50). The median age at enrollment was 48 years (range 18-92) and most participants (58%) were male (Table 1). The majority of patients had an admission GCS score of 15 (60%), and most patients provided an initial blood sample within the first 3 h after injury (median [IQR], 1.8 [1.0-3.0] h).
Demographic and Clinical Characteristics of the Study Population
mTBI, mild traumatic brain injury; CT, computed tomography; GCS, Glasgow Coma Scale; PTA post-traumatic amnesia; LOC, loss of consciousness; UMCG, University Medical Centre Groningen; MST, Medisch Spectrum Twente; MVA, AUTH.
Plasma GFAP concentrations were below the LOD for 58 patients (23%) and plasma UCH-L1 concentrations for 40 patients (16%). Plasma UCH-L1 were significantly higher in CT+ patients (median [IQR], 671 [324-1037] pg/mL) compared with CT- patients (386 [263-640] pg/mL; U = 7070.5, p < 0.01). A similar result was found for the GFAP measurements (399 [150-779] pg/mL vs. 55 [30-151] pg/mL, U = 9306, p < 0.001). Patients with a GCS score of 13 or 14 and CT+ showed higher plasma GFAP and UCH-L1 concentrations than CT- patients with GCS score of 13 or 14 (Fig. 1). Patients with a GCS score of 15 and CT+ showed higher GFAP concentrations than CT- patients with GCS of 15 (Fig. 2). However, UCH-L1 concentrations did not differ between patients with CT+ and CT- within patients with a GCS score of 15 (Fig. 2).

Glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) concentrations in patients with Glasgow Coma Scale (GCS) score 13-14 and GCS 15. The black dotted line indicates the cut-off value of a positive result. The cut-off value for GFAP and UCH-L1 was set at 30 pg/mL and 360 pg/mL, respectively.
Diagnostic performance of GFAP and UCH-L1
Diagnostic performance of GFAP, UCH-L1, and combined (GFAP and/or UCH-L1) for CT outcome in patients with mTBI was assessed. The NPV of GFAP was 95% (95% confidence interval [95% CI], 89-100%) and for UCH-L1 84% (95% CI, 77-91%; Table 2). Positivity for GFAP and/or UCH-L1 resulted in similar NPV compared with GFAP alone 95% (95% CI, 88-100%; Table 2). Combined measurement of the biomarkers reduced unnecessary CT scans to 62% in patients with mTBI eligible for a head CT (Table 2). ROC curves of GFAP and combined detection of GFAP and UCH-L1 resulted in similar AUC, 0.81 and 0.82 respectively (Fig. 3). However, AUC of UCH-L1 for the detection of CT lesions in mTBI patients was lower compared with GFAP (Fig. 3).
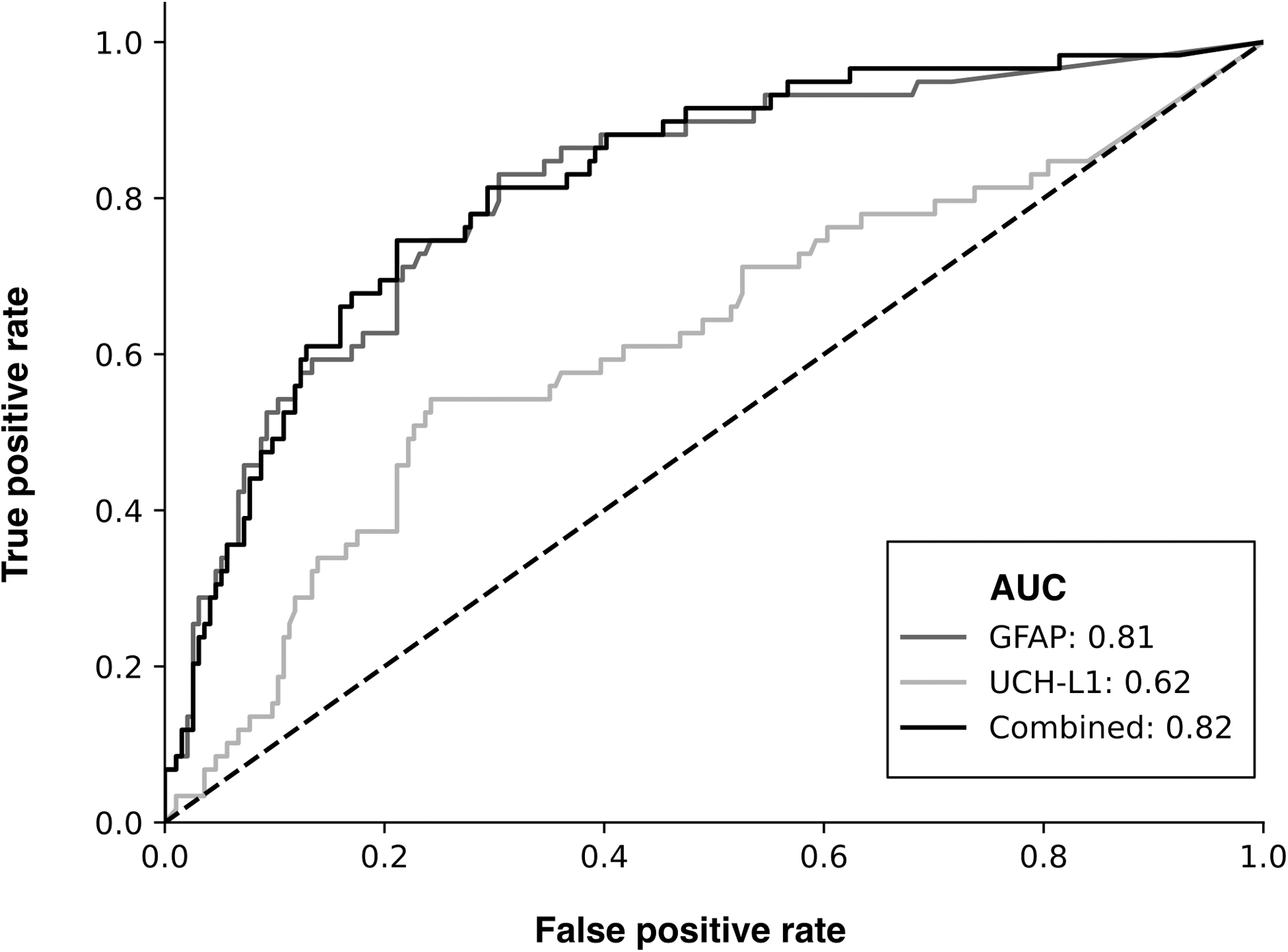
Receiver operating characteristics (ROC)-curve of glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) for predicting head computed tomagraphy lesions after mild traumatic brain injury.
Diagnostic Performance of GFAP and/or UCH-L1 for Head CT Outcome in mTBI Patients
GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase; IQR, interquartile range; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; CT, computed tomography.
In a cohort of 253 patients, we identified two patients with a false negative test result (Table 3). Both patients were male with a GCS of 15 and diagnosed with an acute subdural hematoma (SDH) based on CT scan without any neurosurgical intervention required (Table 3). One patient had injuries from a motorized scooter collision at 60 km/h and was transferred to a regional hospital. The other patient was admitted to the hospital for 3 days for reconstruction of facial fractures after a heavy object (∼200 kg) fell on his face. The latter patient had a UCH-L1 concentration above LOD >200 pg/mL but not above the cut-off of 360 pg/mL. Blood sampling of these two patients took place within 3 h after injury.
Demographic and Injury Characteristics of Patients With Head CT Lesion, but Negative GFAP and UCH-L1 (False Negatives)
Data on admission duration was unavailable as the patient was transferred to another hospital.
CT, computed tomography; GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase; GCS, Glasgow Coma Scale score.
Addition of patient characteristics and demographics to POCT biomarkers
For ease of interpretation of the model, patients were split into tertiles for GFAP (cut-offs <44 pg/mL and <160 pg/mL) and UCH-L1 (cut-offs <309 pg/mL and <602 pg/mL). The distribution of the tertiles across CT outcome is visualized in Supplementary Figure S1. The best specificity at a sensitivity >95% was achieved by a model including LOC and the time to sample. The addition of these clinical variables to the model resulted in increased specificity from 36%, without clinical variables, to 46%, with a sensitivity of 97% (Table 4). This increase was statistically significant (McNemar's chi square: 17.05, p < 0.001). Consequently, the use of clinical variables together with UCH-L1 and GFAP resulted in a lower rate of unnecessary head CT scans 41%, compared with the biomarkers alone (49%) (Table 4).
Diagnostic Performance of Biomarker Only Model and Biomarker+Clinical Model
Clinical variables include Time to sample and presence or absence of loss of consciousness.
CI, confidence interval; CT, computed tomography.
Diagnostic performance of UCH-L1 is dependent on the time to sample
Patients with a positive CT scan post-mTBI had higher UCH-L1 concentrations than patients with a negative CT scan if the sample time was within 3 h (Fig. 4). When time of sampling exceeded 3 h, no significant difference in UCH-L1 concentrations was found between patients with a positive CT scan and a negative CT scan post-TBI (Fig. 4).
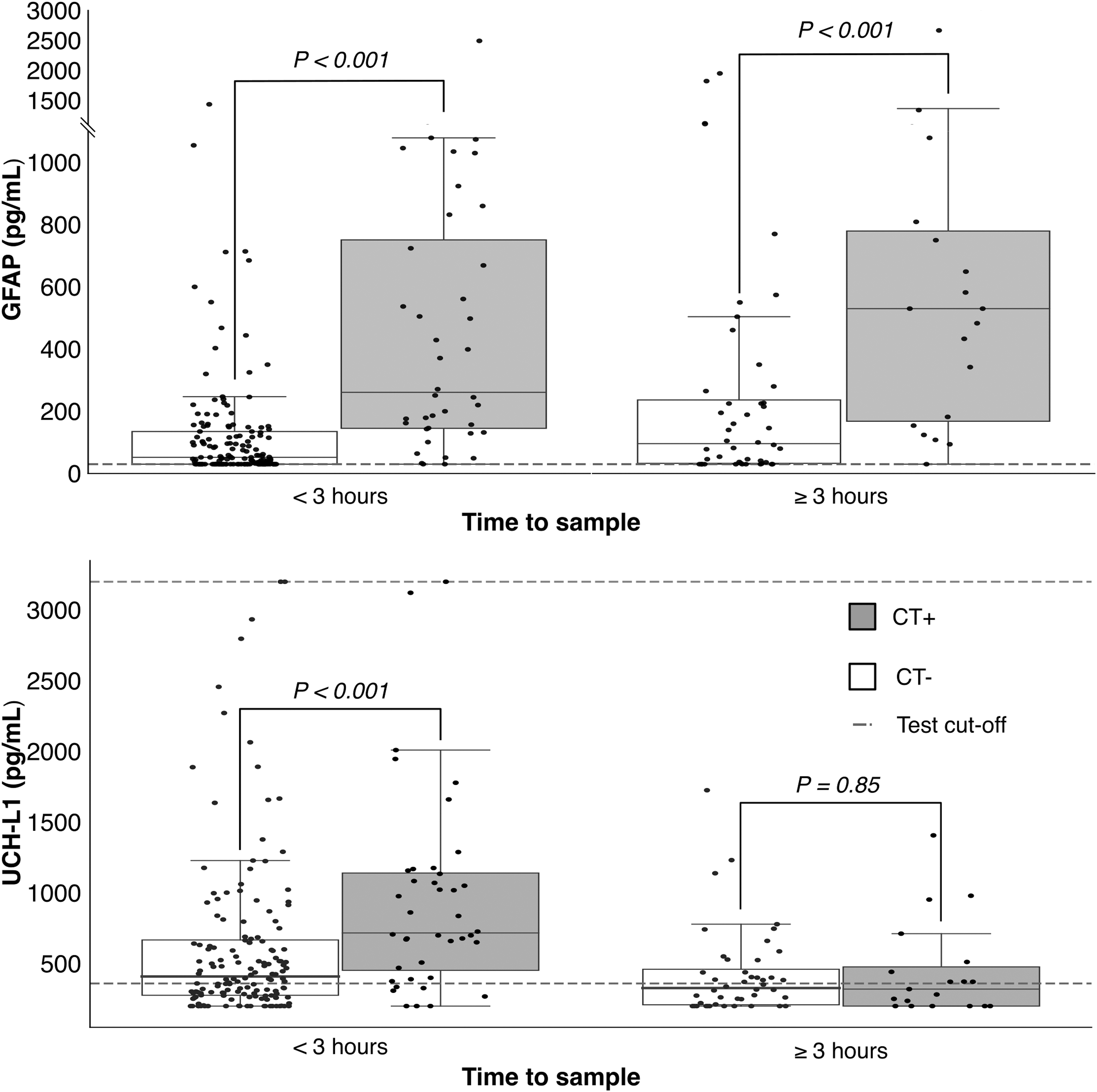
Glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) concentrations stratified by time to sample. The black dotted line indicates the cut-off value of a positive result. The cut-off value for GFAP and UCH-L1 was set at 30 pg/mL and 360 pg/mL, respectively.
Discussion
In this multi-center observational study of patients with mTBI we evaluated FDA-approved plasma biomarkers GFAP and UCH-L1 using the i-STAT POC device for the prediction of intracranial lesions on CT scans in a Dutch population. Our results confirm the high sensitivity (97%) of combined measurement of GFAP and UCH-L1 as reported previously by Bazarian and colleagues. 16 Further, we showed increased specificity of the biomarker panel with the addition of clinical data.
The i-STAT Alinity and TBI plasma cartridge measures UCH-L1 and GFAP simultaneously and produces both qualitative (elevated or not elevated) and quantitative (concentration) results. In accordance with existing evidence, patients with a positive CT scan displayed notably higher concentrations of GFAP and UCH-L1 compared with those without evident intracranial abnormalities on CT. 16,22 -24 In addition, we found higher GFAP and UCH-L1 concentrations in patients with a GCS score of 13 or 14 with a positive CT scan compared with patients with a negative CT scan. Also, GFAP concentrations were statistically different between the two groups (CT positive versus CT negative) in patients with a GCS score of 15. However, no significant difference was found for UCH-L1 levels. The association between GFAP and UCH-L1 concentrations and severity of trauma was confirmed in multiple studies. 22,25,26
UCH-L1 is a neuron-specific cytoplasmic enzyme. 27 Increased UCH-L1 concentrations can be measured within 1 h after TBI and levels peak at 8 h post-injury. 24 GFAP is a monomeric intermediate filament protein which is the main component of the astroglial cystoskeleton. 24,28,29 Increased GFAP concentrations can also be found within 1 h after TBI, but GFAP levels peak 20 h post injury. 24,29 These biomarkers have proven to complement each other for the detection of intracranial lesions as GFAP is released upon astrogliosis/astroglia injury while UCH-L1 is released after neuronal cell body injury. In addition, the kinetics of the biomarkers provide a reliable 12-h testing window for the detection of cellular damage post TBI. 24 In our cohort, combined testing of GFAP and UCH-L1 did not increase the NPV compared with GFAP testing alone (95%, CI; 88%-100% vs. 95%, CI; 89%-100%, respectively). In addition, the AUC of the ROC curve of GFAP and UCH-L1 was similar to GFAP testing alone. These results are similar to those reported previously, where UCH-L1 testing did not improve the AUC compared with GFAP testing alone in CT positive versus CT negative patients post TBI. 23,24 Our results suggest that combination of UCH-L1 and GFAP testing result in possibly more unnecessary CT scans compared with GFAP testing alone, with only limited increase in sensitivity. However, another study suggests that combined testing of UCH-L1 and GFAP might be of added value for the prediction of unfavorable outcome on the long term. 23
We found that the association between UCH-L1 and head CT findings was dependent on the time to sample. When time of sampling exceeded 3 h, UCH-L1 concentrations were not significantly different between patients with positive and negative head CT scans while this was the case if sampling occurred within 3 h of injury. This contradicts a previous study that reported significantly higher UCH-L1 concentrations in patients with a positive CT scan compared with patients with a negative CT scan up to 48 h after injury. 24 The observed variation may be attributed, in part, to the limited sample size in this group. Another explanation, might be the use of other platforms to detect UCH-L1. In a recent study comparing the i-STAT mTBI test with the ARCHITECT assay, it was observed that UCH-L1 values measured by the ARCHITECT were notably higher than those recorded by the i-STAT. 19 Also, adoption of a lower cut-off threshold may influence the clinical efficacy of UCH-L1 for identifying positive head CT findings during screening. Further investigations involving a more extensive cohort are warranted. Nevertheless, GFAP concentrations were higher in patients with a positive CT scan compared with a negative CT scan when samples were collected after 3 h. In agreement, another study reported significantly higher GFAP concentrations in patients with a positive CT scan compared with patients with a negative CT scan after TBI up to 7 days (except at 168 h after injury). 24
Despite the observed high sensitivity of the biomarkers, the specificity (19%) of the biomarkers for a positive CT scan was lower than previously described (40%), consequently leading to more unnecessary CT scans. 16 One reason for this might be that in our study, eligibility for head CT in patients with mTBI that presented at the ED was based on the CHIP decision rule, 30 while the study that led to the FDA-approval of the POC test of UCH-L1 and GFAP used broader inclusion criteria with 47% subjects having neither LOC or amnesia. 16 Application of different decision rules can lead to a variation in CT scanning rates among patients with mTBI. 15 In addition, diagnostic performance of the biomarkers UCH-L1 and GFAP has shown to vary, depending on the decision rule used. 31 Further, the limited specificity of the biomarker panel in our cohort might be due the ability of the panel to predict subtle lesions, such as microhemorrhage, which is only visible on magnetic resonance imaging scan and not CT scan. 16,32 Nevertheless, we were able to increase the specificity from 36% to 46% for predicting a positive CT scan in mTBI patients by including LOC and time to sample, with similar sensitivity. The use of patient characteristics (LOC and time to sample) and blood-based biomarkers (GFAP and UCH-L1) should be further investigated in a larger patient cohort as increased specificity of the test may result in less unnecessary CT scans and consequently lower healthcare costs, reduced radiation exposure and reduced length of stay at the ED.
Within the total study population (n = 253), two (0.8%) patients with a positive CT scan post-TBI were classified negative for GFAP and UCH-L1 using POCT. Interestingly, one patient did not have increased GFAP or UCH-L1 concentration, despite the high energy trauma and maxillofacial fractures. Although a CT scan would not be indicated upon screening using the biomarkers UCH-L1 and GFAP, a CT scan was indicated according to current guidelines. Also, a SDH may occur without extensive parenchymal injury, possibly explaining negative biomarkers results.
The GFAP and UCH-L1 biomarker panel has been FDA approved for determining the need for head CT scans since 2018. However, these biomarkers are still not implemented in most national guidelines for the management of patients with mTBI. Here, we showed the potential of GFAP and UCH-L1 as a screening tool to exclude CT scanning in mTBI patients within a well-designed observational Dutch multi-center study. Implementation of biomarkers might be even more interesting if results can be obtained shortly after admission to the ED using whole–blood. Although the i-STAT Alinity is an easy-to-use portable analyzer, to date, whole blood testing of UHC-L1 and GFAP is not available, hampering high throughput analysis. Further, whole–blood POC testing may also allow for triaging decisions to be made outside of the ED—being applied in sports or military settings. Nevertheless, screening with GFAP and UCH-L1 in mTBI patients using plasma samples could reduce unnecessary CT scans, consequently minimize radiation exposure, reducing length of stay in the ED and possibly result in a reduction of healthcare costs. A recent study, however, used a decision model indicating that screening with GFAP and UCH-L1 was associated with a decrease of CT scans, while maintaining similar costs and health outcomes. 33 Unfortunately, the model did not include any clinical decision rules or long-term effects. The i-STAT Alinity could result in less ED visits if GFAP and UCH-L1 are measured when visiting the general practitioner (GP). However, detailed analysis is warranted to assess the cost-effectiveness of UCH-L1 and GFAP screening in patients with mTBI for CT abnormalities in primary and secondary care. POC testing in whole blood could potentially reduce ED visits or length of stay in the ED and consequently possibly reduce healthcare costs.
Our study has several limitations. The relatively small sample size (n = 253) resulted in wide confidence intervals for the estimated sensitivity and specificity. Another possible limitation is that for this study, plasma samples underwent a single freeze-thaw cycle. However, no impact on the results of GFAP are expected as a previous study has shown that GFAP concentrations remain stable over multiple freeze-thaw cycles. 34 To our knowledge, the effect of freeze-thaw cycles on the stability of UCH-L1 has not yet been properly investigated. Also, a small number of samples (14) were sampled 12 h after injury. The study that resulted in FDA approval of the biomarkers was not validated for these time-points. However, a previous study showed that maximal GFAP concentrations were measured 20 h after injury, but UCH-L1 elevations may not be detected after 12 h post-TBI. 24 Although theoretically the diagnostic performance of UCH-L1 could be influenced by these time-points, this effect is likely limited as only 5% of the patients were included later than 12 h after injury.
Despite these limitations, this study confirmed the high sensitivity of GFAP and UCH-L1 for the detection of CT abnormalities (based on a Marshall score >1) using a i-STAT Alinity and TBI plasma cartridge in a Dutch multi-center study. In addition, we showed that specificity of the biomarkers could be increased by the addition of LOC and time to sample. Altogether, these results support the potential use of GFAP and UCH-L1 in reducing CT scanning in patients sustaining mTBI. POCT of GFAP and UCH-L1 paves the way for rapid rule-out of intracranial lesions, enabling early treatment and discharge decisions. This approach also offers opportunities to assess the necessity of CT scans in patients seeking care from General Practitioners (GPs) and those with sports-related concussions in the context of brain injury diagnosis. Large prospective European study cohorts are warranted to validate our findings.
Transparency, Rigor, and Reproducibility Summary
The study cohort was enrolled as part of the Acute Injury Markers in mTBI (AIM-TBI) study. The AIM-TBI study is a prospective observational cohort study which was pre-registered at the Dutch Trial Register (no. NL8484, https://onderzoekmetmensen.nl/en/trial/24795). This study and the corresponding analytic plan were developed after inclusion started for the AIM-TBI study, for all participants written informed consent for future studies is available. All mTBI patients, seen at the emergency department of participating centers, meeting the eligibility criteria of the AIM-TBI study during the enrolment period (January 2020–December 2022) were approached for inclusion. Although an informal power calculation was made the final sample size (n = 253) was capped due to time constraints partly because of the Covid-19 pandemic. Participants were not provided the results of the fluid biomarker measurements unless this was requested. Handling of biofluid samples and analysis was performed by trained team members blinded to relevant characteristics of the participants. Methodology and decisions for formal statistical analysis as well as multiple comparisons management are described in detail in the methods sections. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. Data from the study is not currently publicly available due to certain datapoints having not been published yet. The analytical code base can be made available on reasonable request to the corresponding author. The authors agree to provide the full content of the manuscript on request by contacting the corresponding author.
Footnotes
Authors' Contributions
WC: conceptualization, formal analysis, analyzing samples, writing original draft. KV: conceptualization, statistical analysis, writing original draft. MdK: conceptualization, inclusion of patients, project administration, writing – review and editing. JvdN: writing—review and editing. RI: writing—review and editing. AB: writing—review and editing. JK: conceptualization, supervising sample analyses, writing—review and editing. HvdH: conceptualization, inclusion of patients, project administration, writing – review and editing.
Acknowledgments
The authors thank Gera ter Braak, Mirjam Kleinsman, Ilona Lubben, Marlies Horst and Agnes Oude Luttikhuis for their technical assistance and Abbott Point of Care for providing mTBI plasma cartridges.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding Information
Cartridges for the detection of mTBI markers in plasma were provided by Abbott.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.