
Abstract
The potential influence of pituitary-related hormones (including both pituitary gland and target gland hormones) on functional recovery after traumatic brain injury has been observed. However, the relationship between these hormones and the recovery of consciousness in patients with disorders of consciousness (DOC) remains unclear. In this retrospective and observational study, 208 patients with DOC were recruited. According to the Glasgow Outcome Scale (GOS) scores after 6 months, patients with DOC were categorized into two subgroups: a favorable prognosis subgroup (n = 38) comprising those who regained consciousness (GOS score ≥3), and a poor prognosis subgroup (n = 156) comprising those who remained in DOC (GOS score <3). Comparative analyses of pituitary-related hormone levels between the two subgroups were conducted. Further, a binary logistic regression analysis was conducted to assess the predictive value of pituitary-related hormones for the patients' prognosis. The favorable prognosis subgroup showed a significant increase in adrenocorticotropic hormone (ACTH) levels (p = 0.036). Moreover, higher ACTH levels and shorter days since injury were significantly associated with a better prognosis, with odds ratios (ORs) of 0.928 (95% confidence interval [CI] = 0.873-0.985, p = 0.014) and 1.015 (95% CI = 1.005-1.026, p = 0.005), respectively. A subsequent receiver operating characteristic (ROC) analysis demonstrated the potential to predict patients' prognosis with an area under the curve value of 0.78, an overall accuracy of 75.5%, a sensitivity of 77.5%, and a specificity of 66.7%. Our findings indicate that ACTH levels could serve as a clinically valuable and convenient predictor for patients' prognosis.
Introduction
Disorders of consciousness (DOC) refer to a specific subset of clinical populations that experiences significant impairment of consciousness resulting from severe brain injury, 1,2 such as vegetative state/unresponsive wakefulness syndrome (VS/UWS) 3 and minimally conscious state (MCS). 4 UWS was characterized by a lack of awareness of self or environment, 3 whereas MCS was marked by unstable yet reproducible signs of awareness. 4 With advancements in emergency techniques in recent years, an increasing number of patients with brain injuries are entering a state of DOC, making the diagnosis, prognosis, and treatment of these patients crucial yet challenging tasks. 5 –7 An essential concern for patients' relatives and clinicians revolves around the possibility of individuals with DOC regaining consciousness, 8 warranting collaborative efforts from researchers across various disciplines. 9 Although numerous studies have employed neuroimaging techniques such as electroencephalogram (EEG) or functional magnetic resonance imaging (fMRI) to predict the prognosis of patients with DOC, 10 –12 the quest for a more accessible and efficient biomarker remains unresolved.
Previous research has demonstrated that patients with brain injuries often experience post-trauma pituitary dysfunction, 13 –15 leading to abnormal levels of pituitary hormones, for example, adrenocorticotropic hormone (ACTH), 16 thyroid-stimulating hormone (TSH), 17 and prolactin (PRL). 18 These hormones, produced by the anterior and posterior lobes of the pituitary gland, 19 play a crucial role in stimulating target glands such as the gonads, thyroid, and adrenal gland, thereby regulating body metabolism and influencing neurological functions. 20 –22 Given their significance, changes in pituitary-related hormones (including both pituitary gland and target gland hormones) hold particular importance for individuals after brain injuries. 13,23,24
Previous studies have underscored the potential of pituitary-related hormones as key contributors to rehabilitation following brain injuries, influencing essential processes such as neurogenesis and neural plasticity. 25 –27 However, existing studies have primarily focused on patients with brain injury who have already regained consciousness, leaving a gap in evidence regarding the relationship between pituitary-related hormone levels and recovery of consciousness in patients with DOC. As a result, a comprehensive investigation into the impact of pituitary-related hormone changes on the prognosis of DOC could yield valuable insights for clinical decision-making. Nevertheless, this area remains relatively unexplored and warrants further investigation.
The primary objective of this study is to examine the potential association between pituitary-related hormones and the prognosis of patients with DOC. The measured hormones include ACTH, cortisol, TSH, free thyroxine (FT4), free triiodothyronine (FT3), PRL, luteinizing hormone (LH), follicle-stimulating hormone (FSH), and growth hormone (GH). These hormones are either directly released by the pituitary gland (including ACTH, TSH, PRL, LH, FSH, and GH) or are produced by corresponding target glands (e.g., cortisol by the adrenal glands and FT3 and FT4 by the thyroid glands) that are regulated by pituitary hormones.
A retrospective cohort of 208 patients with DOC was recruited from three independent medical centers (n = 33, 7, 168, respectively) spanning the period from November 2017 to November 2022. The patients were categorized into two subgroups based on their Glasgow Outcome Scale (GOS) scores after 6 months: a favorable prognosis subgroup comprising patients who regained consciousness (GOS score = 3–5, n = 38), and a poor prognosis subgroup including those who remained in DOC (GOS score = 1–2, n = 156). Using analysis of covariance (ANCOVA), comparative analyses of pituitary-related hormone levels were conducted between the two subgroups, adjusting for data sources, etiology, days since injury, age, and sex as covariates. Further, a binary logistic regression analysis was conducted to assess the predictive value of pituitary-related hormones in predicting the prognosis of patients with DOC.
Methods
Study design and participants
In this retrospective and observational study, we examined the correlation between pituitary-related hormones and prognosis in patients with DOC. A total of 208 patients with DOC resulting from brain injury were recruited from Guangzhou General Hospital of Guangzhou Military Command (n = 33), Guangdong Provincial Work Injury Rehabilitation Center (n = 7), and Zhujiang Hospital (n = 168) from November 2017 to November 2022.
The study design adhered to the ethical guidelines of the Declaration of Helsinki. Informed written consent was obtained from the legal representatives of all patients, and the study was approved by the Ethics Committee of Guangzhou General Hospital of Guangzhou Military Command, Guangdong Provincial Work Injury Rehabilitation Center, and Zhujiang Hospital (registration number: ChiCTR1800014458).
In the current study, the eligibility criteria included: (1) being diagnosed with acquired brain injury based on medical history and confirmed through head computed tomography (CT) or MRI examination; (2) being clinically diagnosed as being in a VS or MCS upon admission according to the Coma Recovery Scale–Revised (CRS–R) 28 ; and (3) having hormone tests performed at least 48 h after hospitalization. Exclusion criteria included: (1) patients with unstable vital signs; (2) medical history of neurological disorders; (3) history of past endocrine disorders or recent use of hormone therapy within the last 2 months; (4) use of medications affecting hormone secretion during the basic hormone level assessment; (5) patients with severe infection; and (6) DOC caused by poisoning, tumors, and inflammatory and metabolic disorders.
Within 48 h of admission, all patients were assessed using the CRS–R by trained clinical professionals (two evaluations per patient; the patient's best state was determined by longer periods of eye opening and sustained arousal). The assessments were repeated three times during the week of enrollment, following established criteria. 29 The CRS–R has a total score of 23, with six subscales used to evaluate auditory, visual, motor, oromotor/verbal, communication, and arousal responses in patients with DOC. The maximum scores for these subscales are as follows: auditory (4 points), visual (5 points), motor (6 points), oromotor/verbal (3 points), communication (2 points), and arousal (3 points). According to the criteria for VS and MCS, 28 when the CRS–R simultaneously meets auditory ≤2, visual ≤1, motor ≤2, oromotor/verbal ≤2, communication = 0, and arousal ≤2, the patient is classified as VS. When the auditory score is 3–4, or visual score is 2–5, or motor score is 3–5, or oromotor/verbal score is 3, or communication score is 1, the patient is classified as MCS.
The prognosis of patients with DOC was determined at least 6 months after the hormone assessment using the GOS. 30 The GOS enables the objective assessment of a patient's recovery in five categories: Death, Persistent vegetative state, Severe disability, Moderate disability, and Low disability. Following previous studies, 12,31 patients with a GOS score ≥3 (i.e., Severe disability, Moderate disability, and Low disability) were assigned to the favorable prognosis subgroup, whereas those with a GOS score <3 (i.e., Death and Persistent vegetative state) were assigned to the poor prognosis subgroup. Fourteen patients were excluded from the analysis due to unavailable GOS scores, resulting in 194 participants included in the final analysis.
Hormone assessment
Fasting venous blood samples were collected from patients within 48 h of hospital admission, during the time frame of 6:00 to 8:00 a.m. All patients rested 30 min prior to testing after insertion of an indwelling catheter in a large forearm vein. Blood was centrifuged at 3000 rpm for 10 min and the serum was stored at −80℃ until further processing. Using radioimmunoassay (DXI-800 chemistry analyzer with reagents from Beckman Coulter, USA), various pituitary-related hormones, including ACTH, cortisol, TSH, FT4, FT3, PRL, LH, FSH, and GH, were measured. Note that we did not use the GH stimulation test to assess GH levels, a common method for diagnosing pediatric GH deficiency. 32 In our present study, all included patients with DOC had a history of brain injury, leading to cognitive impairments and unstable medical conditions. This circumstance renders the GH stimulation test, encompassing both physiological and pharmacological aspects, 33 challenging and risky for these patients.
Although a previous study reported an association between testosterone and estradiol hormone levels and prognosis after severe traumatic brain injury, 34 our study did not examine these two hormones for several reasons: (1) previous studies have generally considered the diagnosis of hypopituitarism to be primarily related to LH/FSH, 35 –37 as LH and FSH are secreted by the pituitary gland, offering better sensitivity in assessing pituitary function; (2) testosterone and estradiol levels are influenced by factors such as age, gender, and menstrual cycle, 38,39 exhibiting considerable variability, and were therefore excluded from testing; and (3) considering the unique characteristics of female patients with DOC, obtaining detailed menstrual histories was challenging, leading us to exclude indicators such as estradiol.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA). Firstly, the ANCOVA was employed to explore the variations in hormone levels between the two prognosis subgroups, that is, the favorable and poor prognosis subgroups. Specifically, a multivariate general linear model was conducted using SPSS, with the grouping variable representing either a favorable or poor prognosis subgroup as the fixed factor. The dependent variables were all types of pituitary-related hormones, and covariates included data sources, days since injury, etiology, sex, and age. It should be noted that data sources and etiology were controlled by setting them as dummy variables. The resulting p-values were corrected using the false discovery rate (FDR) method.
Secondly, the predictive value of pituitary-related hormones for prognosis in patients with DOC was examined using logistic regression. Specifically, a binary logistic regression analysis was performed with the hormones that showed significant group-level differences and all covariates as independent variables, and the grouping categories (i.e., poor and favorable prognosis subgroups) as the dependent variable. Additionally, the logistic regression model provided the predicted probability for each participant, and based on these probabilities, a receiver operating characteristic (ROC) curve was plotted. Following previous studies, 11,40 an optimal cutoff point of the predicted probability was calculated by maximizing the Youden Index, 41 and the sensitivity and specificity of this cutoff point were assessed.
Finally, to further investigate the relationship between patients' behavioral functions (measured by the CRS–R) and pituitary-related hormone levels, a partial Spearman correlation analysis was conducted. Specifically, correlation coefficients and p-values between patients' CRS–R subscale scores and hormone levels were calculated using a partial Spearman correlation analysis, while adjusting for data sources, days since injury, etiology, sex, and age as covariates. The resulting p-values of the correlation coefficients were corrected using the FDR method.
Results
Demographic and clinical characteristics
Among the 194 patients (139 males, mean age 45.3 ± 13.59 years), 38 were classified with a favorable prognosis (27 males, mean age 42.16 ± 12.98 years), whereas 156 were categorized with a poor prognosis (112 males, mean age 46.07 ± 13.66 years) based on the GOS scores. There were no significant differences between patients with favorable and poor prognosis regarding age (p = 0.112, independent samples t-test) or sex (p = 0.927, chi-squared test). Further, we conducted a 2 (favorable and poor prognosis) * 2 (male and female) ANCOVA, with data sources, days since injury, etiology, and age as covariates. Our results revealed no significant interaction between sex and prognosis for any pituitary-related hormone. For detailed demographic and clinical characteristics of each participant, please see Supplementary Table S1.
Further, as shown in Supplementary Table S2, there are some missing values for each type of pituitary-related hormone, with the following counts: ACTH (39), cortisol (5), TSH (2), FT3 (4), FT4 (2), LH (19), FSH (19), GH (25), and PRL (23). For the formal analysis, listwise missing value deletion was implemented as the default option in SPSS 26, which resulted in the exclusion of all observations that contained one or more missing values across all variables.
Pituitary-related hormone dysfunction
Table 1 shows the detailed information on pituitary-related hormone dysfunction for each type of hormone. These hormones are either directly released by the pituitary gland (including ACTH, TSH, PRL, LH, FSH, and GH) or are produced by corresponding target glands (e.g., cortisol by the adrenal glands and FT3 and FT4 by the thyroid glands) that are regulated by pituitary hormones. The normal range of hormone levels in healthy adults at the research center was as follows: ACTH 1.6–13.9 pmol/L; cortisol 171–536 nmol/L; TSH 0.27–4.2 uIU/mL; FT3 3.1–6.8 pmol/L; FT4 12–22 pmol/L; LH 1.24–8.62 IU/L (male) and 2.12–58.64 IU/L (female); FSH 1.27–19.26 IU/L (male) and 3.85–113.5 IU/L (female); GH 0.03–2.47 ug/L (male) and 0.13–9.88 ug/L (female); PRL 3.46–19.4 ug/L (male) and 5.18–26.53 ug/L (female).
Prevalence of Pituitary-Related Hormone Dysfunction
ACTH, adrenocorticotropic hormone; FSH, follicle stimulating hormone; FT3, free triiodothyronine; FT4, free thyroxine; GH, growth hormone; LH, luteinizing hormone; PRL, prolactin; TSH, thyroid stimulating hormone.
Pituitary-related hormone dysfunction is determined when PRL is higher than normal or other hormones are lower than normal. 42 According to the available data in Table 1, the results showed that of 208 patients, at least 132 (63.5%) had hormone dysfunction, including 83 cases of single hormone dysfunction (39.9%), and 49 cases of two or more hormone dysfunctions (23.6%). The prevalence of hormone dysfunction in descending order was: PRL (36.22%) > FT4 (19.9%) > FT3 (19.61%) > LH (11.11%) > cortisol (8.37%) > ACTH (5.33%) > TSH (3.4%) > FSH (2.65%) > GH (2.19%). Our findings revealed that over half of the patients with DOC exhibited pituitary-related hormone dysfunction following brain injury, which aligns with previous research findings. 15,24
Comparison of hormones between favorable and poor prognosis subgroups
Forty-eight patients were excluded from the ANCOVA analysis due to one or more missing hormone data, resulting in a final sample size of 146 participants, including 30 with a favorable prognosis. In specific, a multivariate general linear model was conducted in SPSS, with the grouping variable (favorable or poor prognosis subgroups) as the fixed factor. The study examined all types of pituitary-related hormones as dependent variables, with data sources, days since injury, etiology, sex, and age serving as covariates. Data sources and etiology were controlled by setting them as dummy variables. Table 2 presents the statistical results of ANCOVA between the favorable and poor prognosis subgroups, indicating a significant between-subject difference in ACTH levels after FDR correction (p = 0.036). Figure 1 displays the bar plot for ACTH, demonstrating a statistically significant increase in ACTH levels among patients with a favorable prognosis.
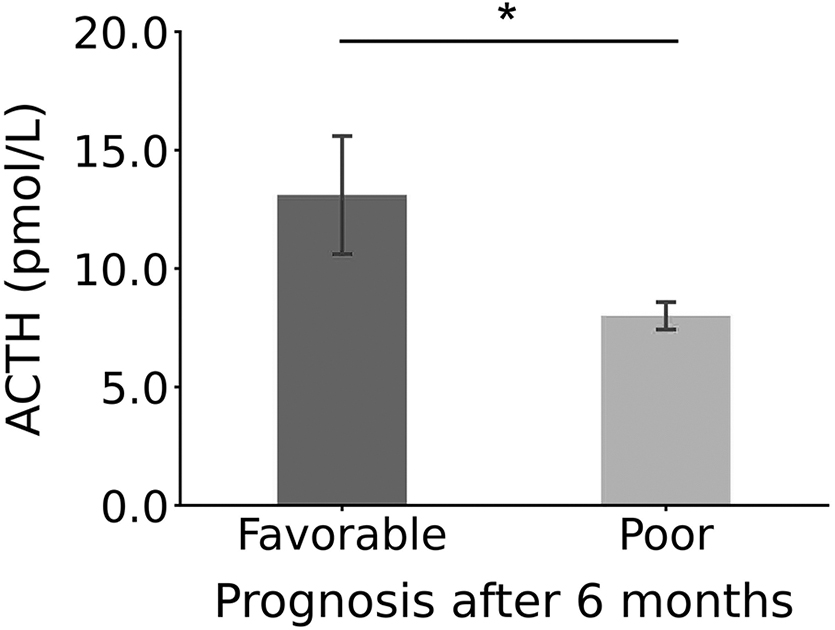
Comparison of ACTH levels between the favorable and poor prognosis subgroups in patients with DOC. Using ANCOVA, the ACTH levels exhibited a significant between-subject effect between the two subgroups, with ACTH significantly higher in the favorable subgroup. The “Favorable” subgroup denotes patients who regained consciousness after 6 months (GOS score ≥3 6 months after the hormone assessment), whereas the “Poor” subgroup represents patients who remained in DOC after 6 months (GOS score <3 6 months after the hormone assessment); *p < 0.05 after FDR correction. ACTH, adrenocorticotropic hormone; ANCOVA, analysis of covariance; DOC, disorders of consciousness; FDR, false discovery rate; GOS, Glasgow Outcome Scale.
Comparison of Pituitary-Related Hormones Levels Between Favorable and Poor Prognosis Subgroups
Bold values mean that the value is statistically significant.
ACTH, adrenocorticotropic hormone; FDR, false discovery rate; FSH, follicle stimulating hormone; FT3, free triiodothyronine; FT4, free thyroxine; GH, growth hormone; LH, luteinizing hormone; PRL, prolactin; TSH, thyroid stimulating hormone.
Predictive value of hormone levels for prognosis of patients with DOC using logistic regression analysis
In the binary logistic regression analysis, patients' prognosis (i.e., favorable or poor prognosis subgroup) was used as the dependent variable, whereas statistically significant hormone (i.e., ACTH) and all covariates (including data sources, days since injury, etiology, sex, and age) were utilized as independent variables. As shown in Table 3, the results revealed that a higher level of ACTH (odds ratio [OR] = 0.928, 95% CI = 0.873-0.985, p = 0.014) and a shorter day since injury (OR = 1.015, 95% CI = 1.005-1.026, p = 0.005) were significant independent predictors of prognosis of patients with DOC. The Hosmer-Lemeshow test for the model was not significant (χ 2 = 1.748; p = 0.988), indicating a well-fitted model.
Logistic Regression Analysis of Prognostic Factors in Patients With DOC
The bold values mean that the value is statistically significant.
ACTH, adrenocorticotropic hormone; GS, Guangdong Provincial Work Injury Rehabilitation Center; GZ, Guangzhou General Hospital of Guangzhou Military Command; SIH, spontaneous intracerebral hemorrhage; TBI, traumatic brain injury; ZJ, Zhujiang Hospital. The Exp (B) represents the odds ratio, indicating the predicted change in odds for a unit increase in the predictor. The notation ‘3E+08’ denotes 3 times 10 to the power of 8.
Further, the logistic regression model provided predicted probabilities for each participant, which were used to perform a ROC curve analysis. As depicted in Figure 2A, the area under the curve (AUC) was 0.78, with a 95% CI of 0.69-0.86, and the sensitivity and specificity were 77.5% and 66.7%, respectively. Based on the results from the ROC analysis, a cutoff point for predicting prognosis was defined as a value of 0.77 according to the Youden Index. Moreover, the logistic regression model demonstrated the potential to predict patients' prognosis with an overall accuracy of 75.5% (Fig. 2B). The chi-square test indicated significant results regarding classification accuracy (χ 2 = 22.29, p < 0.01).

The ROC curve for the binary logistic regression model predicting prognosis of patients with DOC. Using the ACTH that showed a significant between-subject difference and all covariates (data sources, days since injury, etiology, sex, and age), we generated the ROC curve
Partial Spearman correlation between hormones and CRS–R score
To further investigate the relationship between patients' behavioral functions, as measured by CRS–R scores, and pituitary-related hormones, a Spearman partial correlation analysis was conducted, with data sources, etiology, days since injury, age, and sex as covariates. As depicted in Figure 3, significant correlation coefficients were observed between FT4 and arousal (rho = 0.34, p < 0.01), FT4 and CRS–R total scores (rho = 0.27, p = 0.016), FT3 and auditory (rho = 0.25, p = 0.038), FT3 and CRS–R total scores (rho = 0.27, p = 0.016), and PRL and oromotor/verbal (rho = 0.26, p = 0.016). All p-values were FDR corrected.

Partial Spearman correlation between pituitary-related hormones and behavioral functions of patients with DOC measured by the CRS–R. The matrix displays all correlation coefficients (i.e., Rho values), where data sources, etiology, days since injury, age, and sex were treated as covariates; **p < 0.01, *p < 0.05, FDR corrected. ACTH, adrenocorticotropic hormone; CRS–R, Coma Recovery Scale–Revised; FDR, false discovery rate; FSH, follicle stimulating hormone; FT3, free triiodothyronine; FT4, free thyroxine; GH, growth hormone; LH, luteinizing hormone; PRL, prolactin; TSH, thyroid stimulating hormone.
Discussion
The present study investigated the relationship between changes in pituitary-related hormone levels and the prognosis of patients with DOC. Our findings revealed a statistically significant increase in ACTH levels among patients with a favorable prognosis, as indicated by GOS scores ≥3 after 6 months. With binary logistic regression analysis, we found that the OR for predicting prognosis was significant for ACTH (OR = 0.928, 95% CI = 0.873-0.985, p = 0.014). Our results revealed ACTH is an independent predictor of prognosis in patients with DOC, which is consistent with previous reports from animal experiments. 43 Considering the role of ACTH in regulating metabolism, maintaining blood pressure, controlling blood glucose levels, and reducing inflammation, 27,44 these findings suggest that ACTH may play a crucial role in the long-term recovery of consciousness in patients with DOC.
The current study made a contribution by firstly establishing the association between the level of ACTH and the recovery of consciousness in patients with DOC. ACTH, produced by the anterior pituitary under the regulation of the hypothalamic-pituitary-adrenal axis, serves a crucial role in regulating cortisol and androgen levels, 45 while also influencing glucose metabolism and immune system function. 44,46 In experimental animal models of traumatic brain injury promising findings have been observed, 43 where fragments and analogs of ACTH have demonstrated potential in lowering blood–brain barrier permeability, alleviating cerebral hypoperfusion, and preventing pathological elevation of intracranial pressure. 47 For instance, administering ACTH analogs after injury may help mitigate cerebrovascular brain injury and effectively reduce elevated brain water levels to a non-significant extent. 48 These studies suggest that the administration of ACTH compounds after injury may assist in facilitating the recovery of neural and behavioral function subsequent to brain injury. 43,49
Moreover, the effects of ACTH extend to safeguarding against retrograde degeneration after axon terminal damage, 50 while also promoting intracellular mechanisms that enhance neuritogenesis. 27,51 Consistent evidence has shown that adrenalectomy, which results in increased ACTH levels, can have a positive impact by reducing the development of cortical edema and promoting neurological recovery. 52
In summary, previous evidence from animal experiments supports the notion that ACTH plays a vital role in influencing the rehabilitation process following brain injury. Therefore, we may postulate that an elevated ACTH level following brain injury may serve as a crucial prerequisite for the subsequent recovery of consciousness in patients with DOC. This highlights the need for further investigation in this area to deepen our understanding.
Utilizing a comprehensive approach involving ANCOVA analysis, binary logistic regression, and ROC curve analysis, the current results demonstrate in the prognosis of patients with DOC the predictive value of ACTH. Previous studies have revealed that patients with traumatic brain injury may experience secondary ACTH insufficiency as a result of pituitary dysfunction. 16,53,54 As previously mentioned, ACTH is under the regulation of the hypothalamic-pituitary-adrenal axis, which serves as a crucial protective mechanism in response to stress, 45 eliciting an acute fight-or-flight response that is crucial for ensuring survival. 55 Therefore, a deficiency of ACTH and the subsequent absence of the stress response may contribute to inflammation and hemodynamic instability, 16 potentially leading to a poor prognosis after brain injury. Our results provide support for this hypothesis and further clarify the relationship between elevated levels of ACTH and the recovery of consciousness in patients with DOC.
Further, evidence has shown that ACTH could mediate the cortisol awakening response (CAR). 56 According to a recent study, a normal CAR may contribute to an optimal state of brain functioning by proactively enhancing functional coordination between the hippocampus and prefrontal cortex, which is involved in executive functioning and plays a crucial role in preparing for forthcoming cognitive and environmental challenges. 57 These findings may help to explain the mechanism linking increased ACTH levels and the recovery of consciousness in patients with DOC.
More importantly, in our study, employing logistic regression analysis, we discovered that higher levels of ACTH were predictive of patients' prognosis (OR = 0.928, 95% CI = 0.873-0.985, p = 0.014). Further, based on the predicted probabilities from the binary logistic regression model, a subsequent ROC analysis demonstrated good accuracy in predicting prognosis in patients with DOC, with an AUC value of 0.78, an overall accuracy of 75.5%, a sensitivity of 77.5%, and a specificity of 66.7%. Our findings indicate that ACTH could serve as a valuable predictor for the recovery of consciousness in patients with DOC in clinical settings. In addition, our findings are comparable to previous studies that used EEG 10,11 or fMRI 31 indexes. For instance, a previous study utilizing EEG-based graph-theoretic metrics demonstrated an accuracy of 82%, sensitivity of 92%, and specificity of 64% in predicting prognosis in patients with DOC. 11 Additionally, another study using between-region functional connectivity based on resting-state fMRI showed an accuracy of 74%, sensitivity of 81%, and specificity of 69% in predicting prognosis in patients with UWS. 31 In conclusion, our findings suggest that ACTH could be a more convenient biomarker for predicting the prognosis of patients with DOC compared to other potential EEG- or fMRI-based indexes, due to its simplicity in clinical obtainment.
Through a partial Spearman correlation analysis, we discovered significant relationships between various pituitary-related hormones and patients' behavioral functions as assessed by the CRS–R. For instance, we found a positive association between FT3 levels and both the CRS–R total score (rho = 0.27, p < 0.05) and Audio subscale scores (rho = 0.25, p < 0.05). Additionally, FT4 levels were positively correlated with the CRS–R total score (rho = 0.27, p < 0.05) and Arousal subscale scores (rho = 0.34, p < 0.01). These findings were consistent with a recent study that demonstrated an association between cognitive impairment in patients with subarachnoid hemorrhage and reduced levels of FT3 and FT4. 58 In addition, we observed a positive correlation between levels of PRL and patients' Speak subscale scores (rho = 0.26, p < 0.05). This finding is supported by a previous study that established negative associations between levels of PRL and cognitive functions. 59 In summary, our preliminary findings indicate that FT3, FT4, and PRL are associated with patients' behavioral functions rather than serving as predictors of prognosis. These results call for further investigations in the future to gain a more comprehensive understanding of their roles.
Several issues should be noted. Firstly, the retrospective design and limited sample size of this study call for caution when generalizing the findings. The absence of a power analysis further emphasizes the need for more prospective studies to validate the results. Therefore, these findings should be considered preliminary, and further research is required to establish more robust conclusions using larger sample sizes. Secondly, it is crucial to note that the primary focus of the current retrospective study was to identify associations rather than delve into underlying mechanisms. Therefore, future investigations are necessary to provide insights into the mechanisms involved and enhance our understanding of the phenomenon. Thirdly, although all patients received consistent medication and rehabilitation measures during hospitalization in accord with Chinese experts' consensus on diagnoses, treatments, and rehabilitation of DOC, 60,61 variations in treatment and rehabilitation post-discharge could potentially influence patients' prognosis. Future investigations into predicting prognosis in DOC should consider addressing the impact of post-discharge rehabilitation.
Lastly, a subset of patients with DOC had post-injury times exceeding 180 days in our study, potentially impacting the reliability of our findings. To mitigate this, we excluded data samples beyond 180 days post-injury, yielding a cohort of 35 patients with a GOS score ≥3 and 122 patients with a GOS score <3. Using binary logistic regression analysis, we observed a consistent result, where a higher level of ACTH (OR = 0.933, 95% CI = 0.879-0.991, p = 0.024) and a shorter day since injury (OR = 1.016, 95% CI = 1.002-1.030, p = 0.028) were significant independent predictors of prognosis of patients with DOC (see Supplementary Table S3 for detailed results). Further, considering the limited number of subacute patients (within 28 days after injury), we acknowledge the necessity for caution in drawing definitive conclusions about the association between ACTH levels and prognosis of patients with DOC. Further studies are warranted to validate these findings.
In conclusion, our preliminary findings suggest that ACTH levels could serve as a clinically useful predictor for prognosis in patients with DOC. Most importantly, the ease of obtaining ACTH clinically makes it a convenient biomarker, offering potential advantages over other methods such as neuroimaging techniques in terms of simplicity and practicality.
Transparency, Rigor, and Reproducibility Summary
The analysis plan was not formally pre-registered. In this observational and retrospective study, a total of 208 patients with DOC resulting from brain injury were recruited between November 2017 and November 2022. The sample size was determined based on the availability of participants with DOC. The inclusion and exclusion criteria are clearly outlined in the Methods section. The primary outcome and key inclusion criteria adhere to established standards in the field of DOC. Statistical analysis was carried out using IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA). All test and model assumptions were thoroughly assessed, and appropriate statistical methods were employed, as detailed in the final paragraph of the Methods section. Missing data were managed through listwise deletion, following the default option in SPSS 26. Correction for multiple comparisons was performed using FDR correction. All the data needed to evaluate the conclusions in the article are present in the article. Any anonymized data not published within this article will be accessible upon request from qualified investigators. Analytical codes used in this study are not publicly available as they employ commonly known methods. The authors are willing to provide the full manuscript upon request by contacting the corresponding author.
Footnotes
Acknowledgments
We would like to express our gratitude to the patients and their families for participating in the study, as well as to the support staff from the respective clinical centers for their valuable assistance. Please note that the manuscript has not been uploaded to any preprint server.
Authors' Contributions
PQ and QX designed and conceptualized the study. HW, WL, and LJ analyzed the data and drafted the manuscript for intellectual content. WL, ZC, QL, XH, and HZ contributed to the data acquisition. All authors contributed to the critical revision and final approval of the manuscript version for publication.
Funding Information
This work was supported by the National Natural Science Foundation of China (31971032, 81974154, 82171174, and 82002374), the Key Realm R&D Program of Guangzhou (202007030005), the Major Program of the National Social Science Fund of China (18ZDA293), the Guangdong-Hong Kong-Macao Greater Bay Area Center for Brain Science, and the BrainInspired Intelligence Fund (2019023).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.