
Abstract
Of the four million children who experience a concussion each year, 30–50% of children will experience delayed recovery, where they will continue to experience symptoms more than two weeks after their injury. Delayed recovery from concussion encompasses emotional, behavioral, physical, and cognitive symptoms, and as such, there is an increased focus on developing an objective tool to determine risk of delayed recovery. This study aimed to identify a blood protein signature predictive of delayed recovery from concussion in children. Plasma samples were collected from children who presented to the Emergency Department at the Royal Children's Hospital, Melbourne, within 48h post-concussion. This study involved a discovery and validation phase. For the discovery phase, untargeted proteomics analysis was performed using single window acquisition of all theoretical mass spectra to identify blood proteins differentially abundant in samples from children with and without delayed recovery from concussion. A subset of these proteins was then validated in a separate participant cohort using multiple reaction monitoring and enzyme linked immunosorbent assay. A blood protein signature predictive of delayed recovery from concussion was modeled using a Support Vector Machine, a machine learning approach. In the discovery phase, 22 blood proteins were differentially abundant in age- and sex-matched samples from children with (n = 9) and without (n = 9) delayed recovery from concussion, six of whom were chosen for validation. In the validation phase, alpha-1-ACT was shown to be significantly lower in children with delayed recovery (n = 12) compared with those without delayed recovery (n = 28), those with orthopedic injuries (n = 7) and healthy controls (n = 33). A model consisting of alpha-1-ACT concentration stratified children based on recovery from concussion with an 0.88 area under the curve. We have identified that alpha-1-ACT differentiates between children at risk of delayed recovery from those without delayed recovery from concussion. To our knowledge, this is the first study to identify alpha-1-ACT as a potential marker of delayed recovery from concussion in children. Multi-site studies are required to further validate this finding before use in a clinical setting.
Introduction
Concussion is defined as a biomechanical injury to the head associated with transient post-concussive symptoms, and represents a growing public health concern affecting approximately four million children globally each year. 1 –4 Persistent post-concussion symptoms (pPCS), or delayed recovery, are experienced by 30% to 50% of children sustaining a concussion. 5 Delayed recovery from concussion is characterised by emotional, behavioral, cognitive, and physical attributes, which can affect the wellbeing of the child, delay return to school and sport, and have significant developmental and emotional effects. 6 –11
Early detection of children at risk of delayed recovery is crucial to optimize outcomes and to ensure targeted follow-up of those at risk; however, there are multiple limitations to accurate detection. Namely (i) available sideline diagnostic assessment tools are poor predictors of risk of delayed recovery 12 ; (ii) clinical diagnostic tools, administered in the emergency department (ED), are unreliable predictors 13 ; and (iii) up to 50% of children with concussion never present for medical care. 14 Without an appropriate, point of care predictive tool, children at risk of delayed recovery are likely to receive delayed care, which may compromise recovery.
Given its complex and heterogeneous nature, there is an increased focus on developing an objective tool to determine risk of delayed recovery from concussion in children. Through the study of many hundreds of proteins at once, blood proteomics has the capacity to optimize the capabilities of clinically viable proteins in predicting delayed recovery from concussion. 15 Proteomic blood markers to diagnose concussion and prognose outcome post-injury have been of increased focus, with the Food and Drug Administration approving glial fibrillary acidic protein (GFAP) and ubiquitin carboxy-hydrolase L1 (UCH-L1) as markers of intracranial abnormality after mild traumatic brain injury (TBI). 16 Studies have demonstrated, however, that neither of these markers is effective in predicting delayed recovery from concussion in children. 17 –19
In addition, our recent systemic review investigated blood markers of secondary outcomes after concussion and demonstrated significantly less focus on blood markers of concussion in children. Specifically, 10 studies included in our review focussed on pediatric participants only, compared with 38 studies that included adult participants only. 20
The Take Concussion Assessment and Recovery Research (Take CARe) Biomarkers study is a prospective, longitudinal cohort study which aimed to develop markers of delayed recovery from concussion in children by investigating outcomes of children who presented to the Royal Children's Hospital (RCH) in Melbourne, Australia, with a concussion or upper body orthopedic injury. 5
The blood marker aspect of this study involved two key components. The first aspect, outlined in Parkin et al., involved targeted testing of markers which were either previously shown to be implicated in concussion, or known markers of inflammation. 19 Briefly, these authors identified an increase in the concentration of tumor necrosis factor alpha (TNF-alpha) in children with delayed recovery compared with those without delayed recovery from concussion.
However, given the differences in concussion symptomology and recovery in children versus adults, there likely exists candidate markers of delayed recovery from concussion in children that have not previously been shown to be important in concussion.
21
As such, this article represents an additional innovative component of the blood marker aspect of the Take CARe Biomarkers study, which aimed to: Identify proteins that are differentially abundant between children who progress to delayed recovery post-concussion and those who do not. Develop and validate a novel blood protein signature that is clinically useful in predicting delayed recovery post-concussion in children.
Methods
This project represents a cross-sectional component of the Take CARe Biomarkers study that was undertaken at RCH and the Murdoch Children's Research Institute (MCRI). 5
Concussion participant recruitment and data collection
The Take CARe Biomarkers study is a single-center, prospective cohort study evaluating children with concussion and upper body orthopedic injuries (HREC, Study ID 33122). 5 Blood samples were collected from 5- to 18-year-old participants presenting to the ED less than 48h post-injury with a concussion or upper body orthopedic injury. A complete description of the participant recruitment process and study protocol is outlined in Takagi et al. 5
Participant assessment
For the purpose of this study, a concussion was defined as a direct or indirect force to the head resulting in one or more somatic, cognitive, or emotional symptoms, physical signs or behavioral changes, a definition based on the Berlin/Zurich Concussion in Sport Group Consensus Statements. 1,22
Initial clinical assessment was conducted in the ED by treating doctors, with follow-up assessments undertaken by a researcher including the Sport Concussion Assessment Tool 3 (SCAT3) and ChildSCAT3. 23,24 A Clinical Report Form was completed by the treating clinician after recruitment.
Participant recovery was assessed using the Post-Concussion Symptom Inventory (PCSI) questionnaire, which is a set of symptom scales to assess physical, cognitive, emotional, and sleep domains. 22
A qualified clinician collected 1.4 mL of venous blood in S-Monovette tubes (Sarstedt, Australia), containing 1:9 volumes citrate to blood. Samples were centrifuged at 3800g for 10 min at room temperature within 1h of collection. Supernatant plasma was aliquoted off and stored at -80°C until testing.
Determination of recovery status post-concussion
Parents of all participants with concussion, and participants over the age of 13 were required to complete the PCSI at two weeks post-injury, where participants were determined to have delayed or non-delayed recovery from concussion based on scores from the parent PCSI. For this project, delayed recovery, or pPCS, was defined as two or more post-concussion symptoms experienced for at least two weeks post-injury, with at least two symptoms above pre-injury baseline, by one point or more. 25 As outlined in Tagaki et al., 5 defining delayed recovery at two weeks post-injury was selected because a large portion of children recover within two weeks, and those who do not will seek intervention at this time.
Age and sex matched healthy participant recruitment and data collection
Blood samples were collected as part of the Harmonising Age Pathology Parameters in Kids (HAPPI Kids, HREC, Study ID 34183) study from children undergoing minor day surgical procedures at the RCH. Samples were collected from participants before surgery, with participants with presence of systematic abnormalities being excluded from study collection. 26 Samples were collected in S-Monovette citrate 3.2% tubes (Sarsdedt, Australia). Samples were centrifuged at 3800 rpm at room temperature for 5 min, and plasma was stored in 500 μL aliquots at -80°C until testing. For the study outlined herein, these samples acted as age- and sex-matched healthy controls. An outline of the study protocol is published elsewhere. 27
Blood protein analysis
The process taken to identify clinically relevant blood markers of delayed recovery from concussion in this study is shown in Figure 1.

The blood marker development pipeline. SWATH-MS, Single Window Acquisition of All Theoretical Mass Spectra. MRM: multiple reaction monitoring. ELISA, enzyme-linked immunosorbent assay. Created with BioRender.com
Blood marker discovery phase
Untargeted testing of all proteins detectable in age- and sex-matched plasma samples from children with (n = 9) and without (n = 9) delayed recovery from concussion was conducted at the Australian Proteome Analysis Facility (APAF) using Single Window Acquisition of All Theoretical Mass Spectra (SWATH-MS), an approach used previously in the pediatric setting. 28
Sample preparation
This followed the method previously outlined in Bjelosevic et al. 28 Briefly, 25μL of each plasma sample was diluted with ammonium bicarbonate (ABC) (Sigma, St. Louis, MO) solution. Samples underwent digestion and alkylation at 65°C for 30 min and at room temperature for 30 min in the dark, respectively. One-fifth of the sample underwent tryptic digestion overnight at 37°C, and was then diluted with 0.1% formic acid.
Data acquisition
Samples were analyzed using the Triple Time of Flight (Triple TOF) 6600 (Sciex) mass spectrometer coupled with an Eksigent Ultra nano liquid chromatography (nanoLC) system and data acquired in information dependent acquisition (IDA) experiments to generate an ion library for SWATH analysis according to Supplementary Methods S1. Protein identification from IDA search was performed with ProteinPilot (v5.0) (Sciex) using the ParagonTM algorithm in thorough mode by searching against Homo sapiens species from SwissProt (SwissProt_2018_08.fasta) containing 20,386 proteins. Carbamidomethylation of Cys residues was selected as a fixed modification. An ion library was constructed by merging the 1D-IDA library with an external plasma library using the SwathXtend script. 29,30
Samples were subsequently acquired by SWATH analysis and peptide quantification was performed using PeakView (v2.2) in accordance with Supplementary Methods S2.
Blood marker validation phase
A subset of proteins identified as being differentially abundant between groups with and without delayed recovery was selected for validation using the Clinically Useful Selection of Proteins (CUSP) protocol, which is outlined in Swaney et al. 41 The CUSP protocol is a systematic approach to identify proteins that are most likely to be clinically useful markers and is comprised of a statistical and non-statistical component. Briefly, the statistical component ranked each differentially abundant protein by p value obtained using a linear mixed effects adjusted analysis of variance and log fold change. The non-statistical component assessed availability of commercially and clinically used assays for each protein, as well as previously established biological relevance.
Multiple reaction monitoring (MRM)
The absolute abundance of proteins in plasma was further validated using high resolution (MRM-HR) technology. Stable isotope labeled (SIL) peptides were used as internal standards (Supplementary Table S3).
Sample preparation
A pooled sample to assess technical variability of sample processing and data analysis was prepared by mixing 5 μL of each unprepared sample. Twenty-five μL from each plasma sample was diluted with 475 μL 50 mM ABC solution, reduced with dithiothreitol (5 mM final concentration DTT) and alkylated with iodoacetamide (10 mM final concentration IAA). The sample was then further diluted with 50 mM ABC solution (1 mg/mL concentration of plasma). The 50 μg of sample was digested by addition of 2 μg trypsin and incubation at 37°C overnight (16h), and digestion was stopped by formic acid acidification.
Post-digest sample pools were prepared by combining 5 μL of each digested sample. Each sample was spiked with SIL peptides prior to MRM-HR analysis, with post-digest samples being acquired after every five samples. Further detail on the SIL products used, and spiked amounts of each SIL peptide for each injection are outlined in Supplementary Tables S2 and S3, respectively.
Assay method development
Six healthy control samples and 48 concussion samples were combined to create a healthy plasma and concussion plasma pool, respectively. Pooled samples were digested using a previously established protocol. 28 The SIL peptides were pooled and spiked into the plasma pools before MRM-HR analysis. Digestion efficiency, sample loading, and precursor ion selection was optimized for peptide measurement.
Data acquisition
Individual samples (10 uL injections) were analyzed using the Triple TOF 6600 (Sciex) mass spectrometer coupled with an Eksigent Ultra nanoLC system in MRM experiments with transition settings in Supplementary Table S4 and acquisition details outlined in Supplementary Methods S3.
Data processing
The MRM-HR data were processed in MultiQuant (Version 2.1.1, Sciex) and peptide peak areas calculated by the sum of individual fragment areas. Individual peptide and absolute protein abundances were calculated for each of the quantified proteins by comparison of the area of the known amount of SIL heavy labeled spike relative to the area of the unlabeled peptide in the samples. Protein amount was extrapolated from calculated peptide quantities based on relative mass of peptide to protein. Error tolerant searches were conducted on the healthy control plasma pool to identify evidence of post-translational and chemical modifications, as well as amino acid substitutions listed on the UniMod database (unimod.org).
Enzyme-linked immunosorbent assay (ELISA)
Protein concentration in plasma was measured using ELISA. Testing was conducted according to their specifications detailed in the test kit inserts (Supplementary Table S1). ELISA testing was performed in a blinded fashion to limit investigator bias.
Statistical methods
For the discovery study, statistical methods followed an analysis workflow outlined in Wu et al. 31 Briefly, protein peak areas were normalized to the total peak area of each run and difference between groups assessed by analysis of variance in R Studio. Protein abundance was normalized using row median normalization. Proteins were considered differentially abundant with a p < 0.05 adjusted for mixed effects, with proteins indicated to be differentially abundant included as candidates for validation. Statistical methods are outlined in further detail in Supplementary Methods S2.
For the validation study, statistical analysis was undertaken using R-software in R Studio (version 2023.09.1 + 494). All data were analyzed using non-parametric analysis to accommodate the sample size, as well as non-normal distributions. Difference in protein concentration and abundance between clinical outcome groups was compared using a Mann-Whitney U test between two groups and a Kruskal-Wallis test when comparing between multiple groups. Statistical significance was determined to be p < 0.05, which was adjusted using a false discovery rate approach.
Spearman correlation analysis was conducted to compare protein abundance and concentration of validated proteins, obtained using MRM and ELISA, respectively. Protein concentration was also correlated with peptide abundance of the two SIL peptides used to quantify each protein for MRM analysis. A statistically significant correlation was determined to be p < 0.05.
An additional step in the validation study was creating a support vector machine (SVM), a type of machine learning model that was designed to emulate the blood marker signature's power in predicting delayed recovery. Data from participants with and without delayed recovery from concussion were split into training and testing data, on which the model was run. Variables fed into the model included protein abundance or concentration of all validated proteins and clinical variables including age, sex, post-injury loss of consciousness, vomiting, amnesia, and seizures.
To select the combination of variables that could predict delayed recovery with the highest sensitivity and specificity, partial least squares (PLS) analysis was run on all variables, and three variables that best predicted delayed recovery outcome were selected for inclusion in the model. This technique was adapted from Kuhn and Johnson. 32 A maximum of three variables was selected for inclusion in the final model to reduce the risk of overfitting. 33
As the protein concentration and abundance data were non-parametric, a radial basis function kernel SVM was selected, set in classification mode using the kernlab engine. To account for the small sample size, the SVM was fitted with resampling, where a 10-fold crossvalidation was applied to the training data. Model performance was measured based on sensitivity and specificity, which were demonstrated using receiver operating characteristic (ROC) curves.
Results
Patient demographics
Eighty patients were recruited for this study: concussed (n = 40), healthy controls (n = 33) and orthopedic controls (n = 7) (Table 1). No difference was observed between groups in age or sex.
Baseline Participant Characteristics
Mechanism of injury and post-injury outcomes including Glasgow Coma Scale score, loss of consciousness, vomiting, amnesia, and seizure are shown in Table 2. There was no difference seen between mechanism of injury and post-injury outcomes between participants with and without delayed recovery from concussion, except for post-traumatic amnesia, where 6 (50%) children with delayed recovery experienced post-traumatic amnesia, compared with 9 (32.1%) of children without delayed recovery from concussion.
Mechanism of Injury and Post-Injury Outcomes in Children with Concussion
Discovery study
Twenty-two proteins were identified as being differentially abundant in plasma samples from children with and without delayed recovery from concussion, which is shown in Supplementary Figure S1.
There were six proteins selected for validation: angiotensin converting enzyme (ACE), alpha-1-antichymotrypsin (alpha-1-ACT), hepatocyte growth factor like protein (HGFL), immunoglobulin heavy constant gamma 3 (IgG3), matrix metallo-proteinase 9 (MMP-9) and selenoprotein P (SEPP1) (Table 3).
Proteins Identified as Being Differentially Abundant in Children With and Without Delayed Recovery from Concussion That Were Selected for Validation
NR, normal recovery; IQR, interquartile range; DR, delayed recovery; ANOVA, analysis of variance; MRM, multiple reaction monitoring; LME, linear mixed effects; OC, orthopedic control; HC, healthy control; FDR, false discovery rate;
Blood marker validation
Some unlabeled target peptides associated with target proteins were not detected on MRM, and suitable ELISAs were not available for certain proteins of interest. As such, not all proteins were investigated using both validation methodologies.
Alpha-1-ACT and IgG3 were validated using both MRM and ELISA to investigate absolute protein abundance and protein concentration, respectively. Median absolute abundance of alpha-1-ACT was significantly lower in delayed compared with non-delayed recovery groups (18300.18 ± 3148.0 vs. 22839.21 ± 6044.58, p = 0.02) as was median concentration (42970.00 ± 18257.50 vs. 80977.50 ± 40396.25, p = 1.81e-04) (Fig. 2, B,C). This confirms our discovery study findings, where the median relative expression of alpha-1-ACT was lower in participants with delayed recovery compared with those without (22.55 ± 0.13 vs. 22.74 ± 0.10, p = 0.004) (Fig. 2A).

Comparison of outcomes from discovery and validation studies for proteins validated using multiple reaction monitoring and anzyme-linked immunosorbent assay. (
Median absolute abundance of IgG3 was significantly lower in delayed compared with non-delayed recovery groups (4244.75 ± 727.64 vs. 8344.90 ± 6302.82, p = 3.17e-03), which confirms our discovery study findings (22.22 ± 0.57 vs. 22.96 ± 0.28, p = 0.011) (Fig. 2 D,E). Median concentration of IgG3 was significantly higher in delayed recovery participants compared with non-delayed recovery participants, which did not reflect our discovery findings (496835 ± 339512 vs. 119607.50 ± 392255, p = 0.02) (Fig. 2F).
The correlation between protein abundance obtained using MRM and protein concentration obtained using ELISA is demonstrated in Fig. 3A. Specifically, there was a statistically significant correlation seen between alpha-1-ACT abundance and concentration (p = 2.6e-04, R = 0.43). There was also a statistically significant correlation seen between ITLLSALVETR (p = 3.1e-04, R = 0.43) and EQLSLLDR (p = 9.2e-04, R = 0.4) abundance, the two SIL peptides that were used to determine alpha-1-ACT abundance, and alpha-1-ACT concentration (Fig. 3B,C).
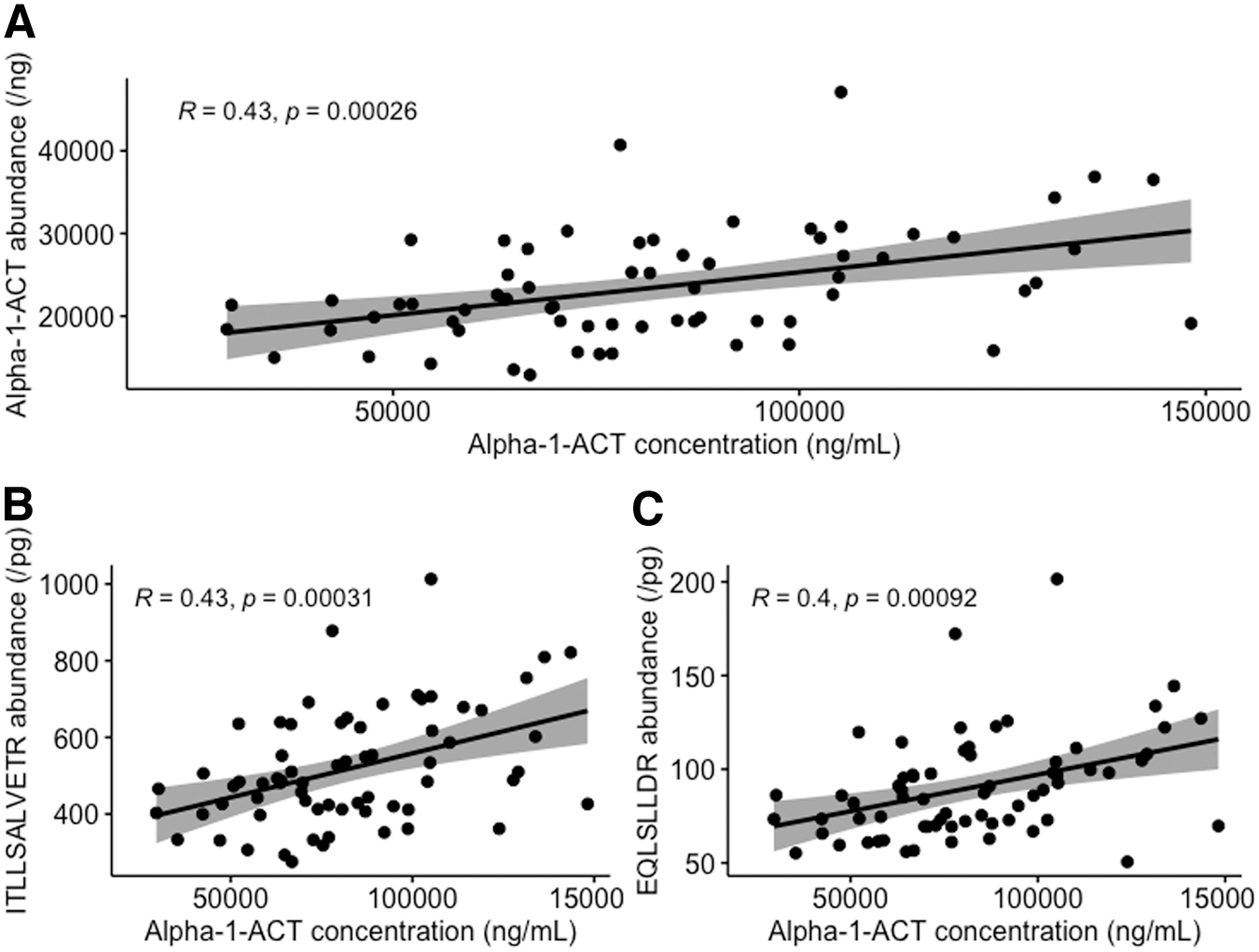
Correlation of alpha-1-ACT concentration and abundance as measured by enzyme-linked immunosorbent assay and multiple reaction monitoring. (
HGFL was validated using MRM only (Fig. 4). There was no difference in median absolute abundance of HGFL seen in delayed versus non-delayed recovery groups (Fig. 4A,B).
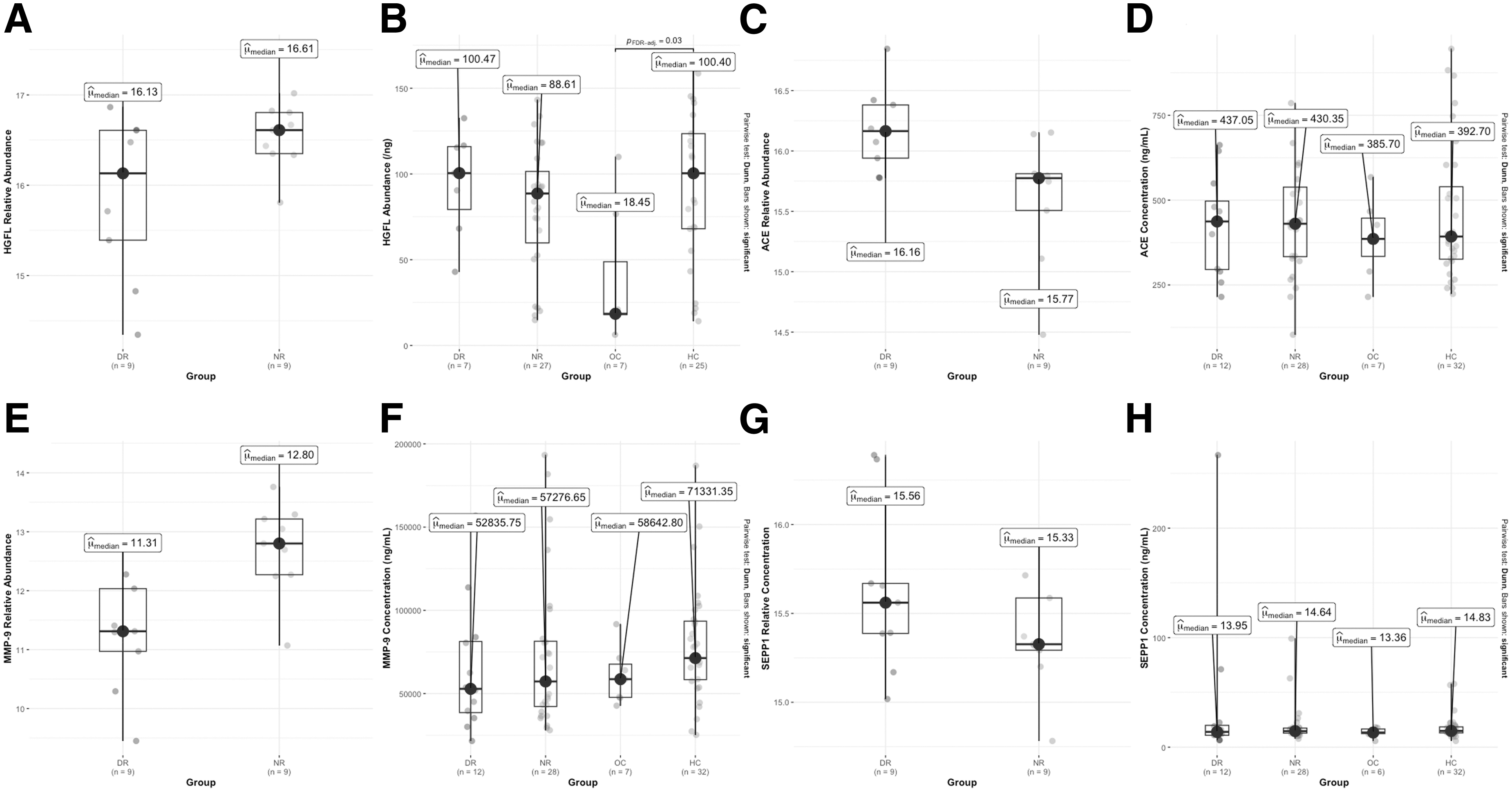
Comparison of outcomes from discovery and validation studies for proteins validated using either multiple reaction monitoring or enzyme-linked immunosorbent assay. ACE, angiotensin converting enzyme; HGFL, hepatocyte growth factor-like protein; MMP-9, matrix metalloproteinase 9; SEPP1, selenoprotein P; PFDR-adj, false discovery rate adjusted p value; μmedian: median.
The ACE, MMP-9, and SEPP1 were validated using ELISA only. There was no difference in the average concentration of ACE, MMP-9. and SEPP1 seen in delayed versus non-delayed recovery groups (Fig. 4 C–G).
A model to predict delayed recovery
The PLS analysis demonstrated that the variables that best differentiate between participants' recovery outcomes were alpha-1-ACT concentration, IgG3 concentration, sex, and post-injury characteristics of amnesia and seizure (Fig. 5). This was shown by the inclusion of these variables in PLS1 and PLS2 (Fig, 5B), which when combined created the most clustering of participants based on recovery outcomes (Fig. 5A). Because IgG3 concentration obtained using ELISA was not reflective of IgG3 relative or absolute abundance, it was not included in the final model.
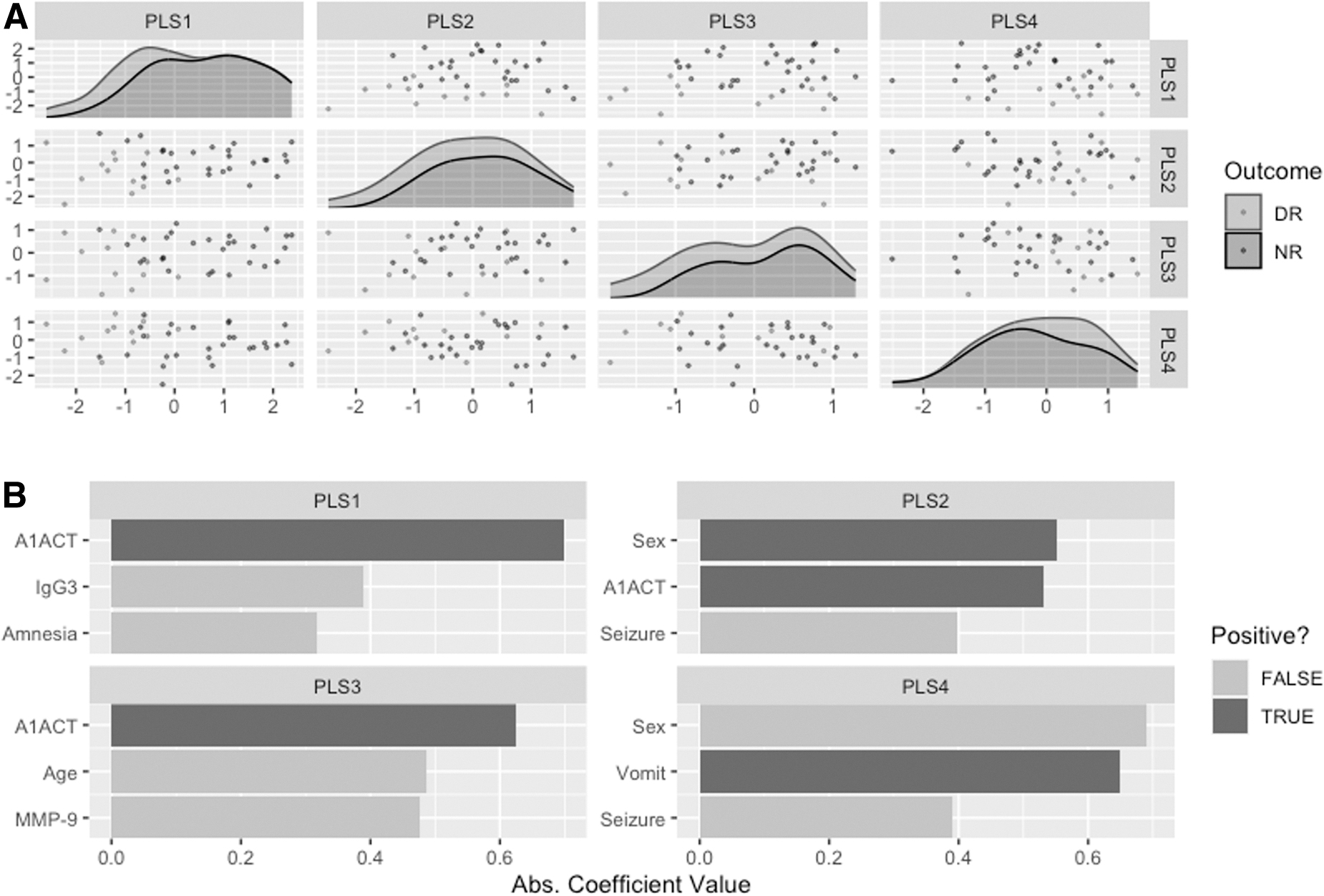
Partial least squares (PLS) analysis demonstrating best predictive variables of delayed recovery from concussion. (
To demonstrate the impact of clinical variables on model accuracy, two SVMs that included the following variables were created:
Alpha-1-ACT concentration, sex, amnesia, and seizure. Seizure was ultimately removed by the model because it was an unbalanced variable, in that only one participant across the entire participant cohort (n = 40) experienced a seizure.
Alpha-1-ACT as a standalone predictor
Both models demonstrated an area under the curve (AUC) on ROC curves of 0.952 (Fig. 6). Following 10-fold cross-validation, however, model two demonstrated a higher mean AUC (0.88 ± 0.13) compared with model one (0.75 ± 0.25).
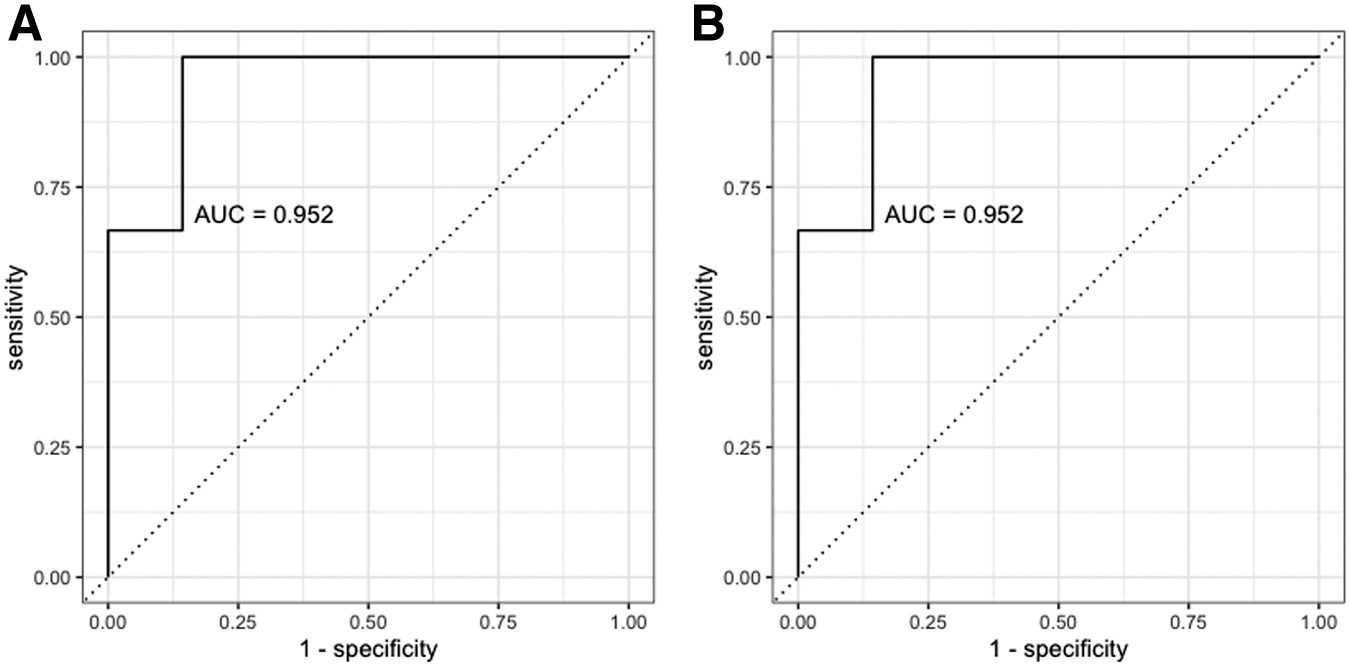
Support vector machine receiver operating characteristic curves showing sensitivity and specificity of (
As such, alpha-1-ACT as a standalone marker was ultimately the best predictor of delayed recovery from concussion in this study's participant cohort.
Discussion
This study aimed to identify blood proteins which were differentially abundant between children with and without delayed recovery from concussion, and therefore develop a blood protein signature to predict delayed recovery post-concussion in children. In the limited number of previous studies that investigated blood markers of delayed recovery from concussion in children, blood markers of concussion in adults have been applied to a pediatric setting, which has not yet resulted in a robust and reproducible marker. 20
As such, in this study we employed an untargeted proteomics approach to investigate plasma proteins in a manner that was sensitive and specific, but not focused on previously identified blood markers of concussion in adults. We found that alpha-1-ACT is a protein that can predict the risk of delayed recovery in children with concussion with a mean AUC of 0.88.
Alpha-1-ACT has been investigated previously as a serum biomarker to grade the severity of TBI (n = 10 per group; mild, moderate, and severe TBI), and found to be increased across all strata of TBI compared with healthy controls. 34 However, no study has investigated its plasma concentration or abundance in children with delayed recovery from concussion. The physiological function of alpha-1-ACT in the setting of concussion is largely unknown; however, this protein has been shown to play a role in upregulating the brain renin-angiotensin system (RAS). 35
Of note, brain RAS is generally seen to be upregulated after a concussion, where the activity of ACE, ACE-2, and specific aminopeptidases increases levels of angiotensin II. 35 A reduction in alpha-1-ACT may impede the typical RAS response, which is generally upregulated after a concussion. Further investigation of the physiological function of alpha-1-ACT is required to better understand its role in recovery after concussion.
Our discovery study demonstrated that IgG3 relative protein abundance was significantly lower in participants with delayed recovery compared with those without delayed recovery. This was reflected in the validation study investigated IgG3 absolute abundance; however; IgG3 concentration was shown to be significantly higher in participants with delayed recovery compared with those without. At this stage, previous literature surrounding the concentration of IgG3 in children with delayed and normal recovery is not sufficient to exclude our findings from further analysis.
There are a number of possible explanations as to why the relative abundance of IgG3 investigated during the discovery study were not reflected in our investigation of its plasma concentration during our validation study. Most pertinently, key issues have been identified with the sensitivity and specificity of antibody products, which can influence the reproducibility of research findings. 36
Our prospective study design ensured minimal sample bias, and our choice of analysis tools ensured that the blood marker developed was accurate and findings were robust. Age- and sex-matched healthy controls were utilized to account for age dependent changes in protein concentration. In addition, the study cohort is generalizable to a broader cohort of children sustaining a concussion between 5 and 18 years of age, where 25% of participants with concussion in our study were female. 37 Children with upper body orthopedic injuries were included in our validation study as an additional control. As such, we were able to ascertain the specificity of changes in protein concentration to concussion compared with other injuries with similar mechanism of injury and clinical presentation. 5
As a form of mass spectrometry (MS), MRM is highly sensitive and specific. Most notably, MRM does not encounter the issue of crossreactivity, which is present in antibody technologies like ELISA, where the antigen binds with an antibody that was raised to a different antigen. ELISAs utilize antibody technology, are cheaper than MS technology, commercially available, and more often utilized as a clinically useful tool. As such, it is a critical part of the blood marker development pipeline that proteins are analyzed using ELISAs or related antibody technology, to assess their feasibility as a blood marker of delayed recovery post-concussion.
The sensitivity and specificity of a blood marker is reflected in its false positive and negative rate. A low false negative rate is extremely important when developing a screening test for disease or injury. 38 The low false negative rate of alpha-1-ACT, demonstrated in the SVM's AUC of 0.88, contributes to its effectiveness as a clinically useful tool. In the case of concussion, misclassifying a patient as being predicted to have normal recovery could result in the patient following a suboptimal or delayed treatment plan that may impact on the recovery trajectory.
The accuracy, sensitivity, and specificity of alpha-1- ACT in our study supports potential clinical utility for employing blood biomarker methods to identify children at risk of delayed from concussion, enabling early intervention and targeted treatment.
Clinical implications
The key to optimum patient outcomes in pediatric concussion is early and accurate diagnosis, effective treatment, and safe return to exercise, learning, and sports and leisure. 39,40 In children presenting to acute care services within 48h of injury, our results suggest that alpha-1-ACT can contribute to the identification of risk of delayed recovery, enabling clinicians to provide individualized patient treatment in a timely fashion and to effectively target scarce education and therapy resources. An accurate prognostic method of this nature has not yet been achieved through the methods of clinic-based assessment and imaging protocols.
Limitations
Our participant sample included a small number of orthopedic controls (n = 7). While we accounted for this issue by including samples from age- and sex-matched healthy controls (n = 33), this study is limited in its ability to determine the specificity of alpha-1-ACT in differentiating between participants with delayed recovery from concussion and orthopedic injury.
In addition, machine learning models such as SVMs are limited in their ability to effectively emulate a blood marker in predicting delayed recovery outcomes in a clinical setting when trained on a relatively small sample size (n = 40). On a small sample size of 40 patients, the model can overfit, where the model loses its learning capacity and is then only able to classify patients based on specific values in the data that it has been given. 33 Hence, further studies need to focus on applying this model to a larger sample size to reduce the chance of it overfitting.
Conclusion
Pediatric concussion is now widely understood to be different to adult concussion in its symptomology and recovery. In addition, the pediatric proteome is vastly different from that of adults. Acknowledging such crucial differences, our study shows that alpha-1-ACT concentration can differentiate between children experiencing delayed and normal recovery from concussion with an 0.88 AUC. Alpha-1-ACT has potential to transform acute clinical management by providing clinicians with a robust predictive marker with which to guide and target treatments to children most likely to experience delayed recovery.
Transparency, Rigor, and Reproducibility Summary
The study was pre-registered at the Australian Clinical Trials Registry (ACTRN12615000316505). The analysis plan was registered after beginning data collection but before data analysis in Takagi et al 5 . A sample size of 30 participants with concussion and 30 participants with orthopaedic upper body injuries was planned. A sample size of 30 participants with concussion and 7 participants with orthopaedic upper body injuries was achieved. However, an additional 30 samples from age- and sex- matched healthy controls were collected to account for the low number of orthopaedic controls. Participants were blinded to results of the fluid biomarker measurements. Biofluid samples were labelled using codes linked to participant identifying information, and handling was performed by team members blinded to injury and recovery status of the participants. Fluid biomarker measurements, analyses and quality control decisions were performed by investigators blinded to relevant characteristics of the participants. Samples were collected using venepuncture into a S-Monovette tube (Sarsdedt, Australia), containing 1:9 volumes citrate to blood. Samples were centrifuged at 3800g for 10 minutes at room temperature within one hour of collection. Supernatant was then aliquoted off and the samples were immediately stored at 70°C until testing, with one freeze thaw cycle performed prior to analysis. For each of the SWATH-MS and ELISA analyses samples were analysed at the same time in a single batch. For MRM analysis, samples were analysed in multiple batches, with pooled samples injected onto the mass spectrometer to assess technical variability. All equipment and analytical reagents used to perform blood marker validation using ELISA assays are widely available from commercial sources, which are outlined in the Supplementary Files. The key inclusion criteria are established standards in the field and are outlined in the published study protocol 5 . Statistical analysis was conducted by ES, and was reviewed by SJCH, who holds a Graduate Diploma in Biostatistics. No replication or external validation studies have been performed or are planned at this time. Due to ethics constraints, de-identified data from this study are not available in a public archive.
Footnotes
Acknowledgments
We thank participating families, emergency department staff, and study volunteers from the Royal Children's Hospital, Melbourne, Victoria.
Authors' Contributions
VA and FEB conceived the study, obtained grant funding, designed the study, provided supervision, and revised the manuscript critically. VI conceived the proteomics aspect of the study, provided supervision, supervised analysis of the data, interpreted the data and revised the manuscript critically. ES obtained the data, analyzed the data, interpreted the data, and wrote the initial draft of the paper. VR, NA and GP obtained the data and revised the manuscript critically. GHS, TZ and LC obtained the data, analysed the data, interpreted the data, and revised the manuscript critically. MT, MLS and GAD designed the study, provided overall supervision and revised the manuscript critically. All authors gave final approval to be published and agreed to be accountable for all aspects of the work.
Funding Information
This work was supported by the Royal Children's Hospital Foundation. ES is being supported by an Australian Government Research Training Program Scholarship throughout the duration of her Doctor of Philosophy candidature.
Author Disclosure Statement
Gavin Davis is a member of Concussion in Sport Group, an honorary member of the Austrlian Football League (AFL) Concussion Working Group Scientific Committee, and has attended meetings organised by sporting organisations including the National Football League (NFL), National Rugby League (NRL), International Ice Hockey Federation (IIHF) and Federation Internationale de Football Association (FIFA); however, has not received any payment, research funding, or other monies from these groups other than for travel cost. For the remaining authors, no competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Figure S1
Supplementary Methods S1
Supplementary Methods S2
Supplementary Methods S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.