
Abstract
Studies have demonstrated associations between cumulative concussion and repetitive head impact exposure (RHI) through contact sports with white matter (WM) alterations later in life. The course of WM changes associated with exposure earlier in the lifespan is unclear. This study investigated alterations in white matter (WM hyperintensity [WMH] volume and microstructural changes) associated with concussion and RHI exposure from adolescence to early midlife, as well as the interaction between exposure and age cohort (i.e., adolescent/young adult compared with early midlife athlete cohorts) on WM outcomes. Participating football players included an adolescent/young adulthood cohort (n = 82; Mage = 18.4 ± 1.7) and an early midlife cohort (37 former collegiate players approximately 15 years removed from sport; Mage = 37.7 ± 1.4). Years of football participation and number of prior concussions were exposures of interest. White matter outcomes included log-transformed manually segmented total WMH volume and neurite orientation dispersion and density imaging metrics of microstructure/organization (isotropic volume fraction [Viso], intracellular volume fraction [Vic], and orientation dispersion [OD]). Regression models were fit to test the effects of concussion history, years of football participation, and age cohort by years of football participation with WM outcomes. Spearman’s correlations assessed associations between significant WM metrics and measures of cognitive and psychological function. A significant age cohort by years of participation effect was observed for whole brain white matter OD, B = −0.002, SE = 0.001, p = 0.001. The interaction was driven by a negative association between years of participation and OD within the younger cohort, B = −0.001, SE = 0.0004, p = 0.008, whereas a positive association between participation and OD in the early midlife cohort, B = 0.001, SE = 0.0003, p = 0.039, was observed. Follow-up ROI analyses showed significant interaction effects for OD in the body of the corpus callosum, genu of the corpus callosum, cingulum, inferior fronto-occipital fasciculus, superior longitudinal fasciculus, and posterior thalamic radiation (p values <0.05). Greater concussion history was significantly associated with greater Viso in the early midlife cohort, B = 0.001, SE = 0.0002, p = 0.010. Years of participation and concussion history were not associated with WMH volume, p values >0.05. Performance on a measure of executive function was significantly associated with years of participation, ρ = 0.34, p = 0.04, and a trend was observed for OD, ρ = 0.28, p = 0.09 in the early midlife cohort only. The global characterization of white matter changes associated with years of football participation were broadly similar and stable from adolescence through early midlife (i.e., microstructural alterations, but not macroscopic lesions). An inverse association between years of participation and orientation dispersion across age cohorts may represent a process of initial recovery/reorganization proximal to sport, followed by later reduction of white matter coherence.
Introduction
Adverse neurobehavioral and neurological outcomes have been reported among older former contact sport athletes with a history of exposure to concussion and repetitive head impacts (RHI). 1 –5 The mechanisms underlying why individuals exposed to cumulative RHI or concussion early in life may be vulnerable to a range of adverse outcomes later in life, such as Alzheimer’s disease and related dementias (ADRDs), is not well understood. Among generally healthy younger (high school and collegiate level) contact sports athletes, subtle neurobiological alterations can be observed on advanced neuroimaging among those with higher levels of prior concussion and/or years of contact sport participation. 6 –8 For example, prior studies have reported increased functional network connectivity and white matter microstructural abnormalities in active high school and collegiate athletes with a greater history of concussions and years of participation, respectively. 9,10 These and other subtle neurobiological changes in advanced neuroimaging in younger athletes with greater RHI and concussion exposure in the absence of clinical disruption in function may represent a potential increased vulnerability to adverse outcomes later in life.
White matter hyperintensities (WMHs) are pathological lesions on magnetic resonance imaging (MRI) within the white matter of the brain, commonly observed on T2 fluid attenuation inversion recovery (FLAIR) sequences. The underlying pathology of WMH can be ambiguous, although most commonly are of vascular origin in older adults. 11 –13 WMH have also been associated with neuropathological deposition (e.g., beta-amyloid and studies regarding the spatial and overall association with tau are mixed) and axonal degeneration. 14 –16 In addition to being a consequence of pathological processes, WMHs are also a robust predictor of the rate of decline and disease progression in ADRD. 16 –19 For example, greater WMH burden has been observed predicting faster rates of future cognitive decline, cerebral atrophy, and progression of neurodegenerative disease. 20,21
Select studies have reported associations between white matter signal abnormalities on imaging and postmortem with higher levels of RHI exposure in older former contact sport athletes. 22 –24 For example, greater WMH burden on neuroimaging (i.e., total volume on FLAIR sequence) was recorded among former football players with contact sport exposure earlier in life. 25 Higher in vivo WMH burden significantly correlates with higher chronic traumatic encephalopathy (CTE) disease burden at autopsy, and both were positively associated with greater years of football participation in a study of former players. 24 Furthermore, higher levels of postmortem white matter degradation, which has been shown to be positively correlated with FLAIR WMH volume in nonathlete populations, have been observed in older former football players with greater levels of football participation. 23 These preliminary studies in older former contact sport athletes provide support that WMH burden potentially represents a primary risk factor and/or mechanism by which contact sport exposure decades prior may be associated with a range of adverse longer-term outcomes in older adults.
While representing a potential bridge between subtle neurobiological alterations at younger ages and adverse outcomes/ADRD later in life, studies of WMH in active, younger athletes have been limited. One large investigation involving two independent cohorts of adolescent/young adult athletes did not observe a greater prevalence of WMH (binary yes/no) among contact sport athletes compared with the noncontact control group; however, the analyses were limited in the characterization of WMH (binary yes/no present) and contact sport exposure (group comparison to noncontact athletes). 26 Independent of macrostructural changes (i.e., WMH volume), greater white matter microstructural abnormalities as measured by diffusion MRI (dMRI) have been recorded among active, younger athletes with more years of contact sport participation. 10 Studies of white matter alterations of any kind are extremely limited in former contact sport athletes during early midlife. This is critical, as longitudinal development of WMH in specific regions corresponds with the location of preceding white matter microstructural abnormalities in normal-appearing white matter (NAWM) in clinical, nonathlete cohorts (e.g., multiple sclerosis). 27 As such, it is possible that the white matter microstructural abnormalities observed among adolescent/young adult athletes may evolve toward greater burden of WMH during early midlife, preceding later life adverse outcomes.
Further elucidation of the relationship between concussion/RHI exposure, WMH, and white matter microstructural alterations, as well as the patterns of changes, in nonolder adults is critical for better understanding the way in which subtle biological alterations on neuroimaging in younger athletes may represent a risk factor for future decline later in life. As such, the aims of the current study were to investigate (1) the association between history of cumulative concussion and exposure to football with total WMH volume and whole brain and regional microstructural changes (neurite orientation dispersion and density index [NODDI] metrics) in white matter in two age cohorts of active or former football players, ranging from adolescence to early midlife. We also investigated (2) the interaction between years of football participation with age cohort (i.e., adolescent/young adulthood compared with early midlife athlete cohorts) on WMH volume and white matter microstructure. For those metrics in which a significant interaction was observed, (3) we examined the association between years of participation and WM metrics with neurobehavioral function across each age cohort. We hypothesized that white matter microstructural alterations would be associated with greater years of sports participation, this association will be stronger in the cohort of former athletes in early midlife compared with younger, active athletes, and that WMH burden would be associated with greater years of contact sport participation only in the midlife cohort. In addition, we hypothesized that years of participation and significant WM metrics of interest would be associated with clinical outcome measures in the early midlife cohort only.
Materials and Methods
Participants
Adolescent and young adulthood cohort
High school and collegiate football players were enrolled at preseason as part of a prospective study on the acute effects of concussion (Project Head-to-Head II is described in greater detail elsewhere). 26,28 Exclusion criteria for this study included: contraindication to study procedures (e.g., unable to complete MRI), history or suspicion of conditions known to influence study outcomes (e.g., epilepsy, moderate-to-severe TBI, or neurological disease), current psychotic disorder, or narcotic use. For the purposes of this study investigating the chronic effects of cumulative concussion and contact sport exposure, uninjured contact sport control athletes were the group of interest. As such, not sustaining a concussion within the last 6 months was an additional exclusion criterion of the current study.
Demographic data, health history, and self-reported concussion (diagnosed and undiagnosed) and football participation history were collected at a preseason assessment visit. Athletes were provided a standard definition of concussion when inquiring about previous injury history. The definition was based on that of the U.S. Department of Defense, which included “a blow to the head followed by a variety of symptoms that may include any of the following: headache, dizziness, loss of balance, blurred vision, seeing stars, feeling in a fog or slowed down, memory problems, poor concentration, nausea, or throwing up. Getting knocked out or being unconscious does not always occur with a concussion.” Due to the distribution of concussion history within the sample, concussion history was characterized as a categorical variable, including groups of 0, 1, and 2 or more (2+) prior concussions. This study was approved by the Medical College of Wisconsin Institutional Review Board (IRB). Adult participants and parents of minor participants provided written informed consent. Written assent was provided by minor participants.
Early midlife cohort
Former National Collegiate Athletic Association (NCAA) football players of 15 years, removed from participation who had previously participated in an online health survey were recruited. 29 Participants were required to be involved in at least one year of collegiate football to be eligible for the study. Exclusion criteria involved a history of psychotic disorder with active symptoms, as well as contraindication to neuroimaging and travel for in-person visit. 30 Participants completed comprehensive assessments, including collection of demographic information, health history, administration of a clinical assessment battery, and concussion and football participation history. Participants were provided the same definition of concussion listed above when reporting injury history to aid in accurate characterization (diagnosed and undiagnosed). Concussion history was characterized as a continuous variable in this cohort. The number of years of football participation was also provided by participants during in-person assessment. During the study visit, participants completed neuroimaging based on a protocol that generally paralleled the Head-to-Head II study (see below and Supplemental Table S1). This study was approved by the Medical College of Wisconsin and University of North Carolina at Chapel Hill IRBs and all participants provided written informed consent.
Imaging protocol and processing
Adolescent and young adulthood cohort
High-resolution T1-weighted images (1 mm x 1 mm x 1 mm) were acquired on 3 Tesla General Electric MR750 whole-body MR scanners using a 32-channel receiver coil array through a magnetization-prepared rapid gradient-echo (MPRAGE) sequence with the (Supplementary Table S2) following parameters: FOV = 256 mm, acquisition matrix = 256, 160 slices, slice thickness = 1 mm, TR/TE/TI = 7.592/3.008/900 ms, flip angle = 8°. A 3D T2-weighted FLAIR sequence was acquired in the sagittal plane based on the following parameters: FOV = 256 mm; acquisition matrix = 256 × 256; 160 slices; slice thickness = 1 mm; TR/TE/TI = 6500/69.82/1889 ms, flip angle = 90°.
Diffusion-weighted images were obtained using a single-shot spin-echo EPI sequence with 3-mm isotropic voxels and b-values of 1000 sec/mm2 and 2000 sec/mm2. Thirty diffusion directions were collected for each b-value. A nondiffusion-weighted spin-echo EPI scan with the phase encoding polarity reversed was acquired to enable correction for magnetic susceptibility variation-related distortions.
Early midlife cohort
High-resolution T1-weighted images (1 mm × 1 mm × 1 mm) were acquired on 3 Tesla Siemens Magnetom Prisma MR scanner using a 32-channel receiver coil array through a three-dimensional (3D) MPRAGE sequence with the following parameters: TR/TE/TI = 2540/2.03/900 ms, flip angle = 8°, FOV = 256 mm, Matrix = 256 × 208, 176 slices. T2-weighted FLAIR images were acquired with the following parameters: TR/TE/TI = 6500/253/1890 ms, FOV = 256 mm, and 160 slices.
Diffusion-weighted images were obtained using a multiband accelerated spin-echo (factor = 3) EPI sequence with 1.5-mm isotropic voxels and b-values of 1000 sec/mm2 and 2000 sec/mm, 2 with 167 diffusion directions collected. Similar to the adolescent/young adulthood cohort, a nondiffusion-weighted spin-echo EPI scan with the phase encoding polarity reversed was acquired to enable correction for magnetic susceptibility variation.
NODDI dMRI processing
As per the software developer’s request (QSIPrep and QSIRecon), specific standardized descriptions of the preprocessing and processing protocol were generated as part of the output and can be found in the supplementary methods. 31 The protocol will be highlighted briefly below. For more details of the pipeline, see the corresponding supplemental methods.
Image preprocessing
Processing of T1-weighted (T1w) images for diffusion workflow involved intensity nonuniformity, skull stripping, nonlinear spatial normalization and registration, and tissue segmentation of cerebral spinal fluid, white matter, and gray matter. 32 –35 Diffusion-weighted images were denoised using the Marchenko–Pastur principal component analysis approach. 36 Corrections for head motion, Eddy current, and susceptibility distortion were applied using FSL. 37 DWI images were resampled to ACPC, generating a preprocessed DWI run in ACPC space with 2 mm isotropic voxels following resampling of DWI time series to ACPC.
Conventional diffusion tensor imaging (DTI) metrics including fractional anisotropy (FA), axial diffusivity, radial diffusivity, and mean diffusivity have been previously reported in a subset of the HTH2 cohort. 10 Fractional anisotropy was derived in this study to enable processing through tract-based spatial statistics (see below). The current study focused on metrics derived from the NODDI model fit using the AMICO implementation, 38,39 as the complex multicompartmental diffusion model allows for estimation of more detailed features of white matter microstructure. Specifically, this includes estimates of neurite density or compactness (intracellular volume fraction; Vic), neurite dispersion or fanning (orientation dispersion; OD), and free water surrounding neurites within voxels (isotropic volume fraction; Viso). 38
ENIGMA DTI tract-based spatial statistics
Participant FA maps were aligned to the ENIGMA-DTI FA template using tract-based spatial statistics (TBSS) in FSL. 40 Details regarding the properties and development of the ENIGMA-DTI FA template and protocol are detailed elsewhere. 41 Briefly, FA data for all participants were projected onto a mean FA tract skeleton in standard space. 42 Skeletonization was performed separately for each study age cohort. The three primary NODDI images (Vic, Viso, OD) were projected onto participants’ FA skeleton, and values for each metric were derived for 25 bilateral white matter regions of interest (ROIs) using the John’s Hopkins University atlas. Consistent with the ENGIMA-DTI protocol, 24 ROIs (19 bilateral structures, 3 subregions of the corpus callosum, and the fornix) and full white matter skeleton (global WM) were extracted from the ENIGMA template in Montreal Neurological Institute space and total Vic, Viso, and OD were averaged across left and right hemisphere tracts. QA of preprocessing and reconstruction of DWI data was performed at multiple steps of the above described QSIprep, QSIrecon, and ENGIMA-DTI protocols and participants in which processing failed due to any reason were excluded from the analyses.
WMH tracing and segmentation
Manual tracing of WMH for all subjects was performed by a single rater (PV or SO) who was trained by a board-certified neuroradiologist (AK). Identification and classification of WMH were completed in accord with the Standards for Reporting Vascular Changes on Neuroimaging (STRIVE) guidelines. 43 A second rater with expertise (BLB) reviewed all manually traced volumes as a quality assurance measure. For instances in which there was conflict between raters, the team neuroradiologist made the final determination regarding the lesion presence/absence and boundaries. Tracing was performed in ITK-SNAP software based on FLAIR images, although T1 and T2 scans were available for additional review. 44 Binary masks generated using AFNI 3dROIstats and WMHs volumes, expressed in mL, were calculated for each subject. Due to the positive skew of WMH volume within the sample, data were log-transformed to better approximate a normal distribution. Manual tracing of WMH was completed for the current study, as prior work from our group and others have demonstrated poor accuracy of automated software/methods for segmenting WMH among younger, relatively healthy individuals (Supplementary Methods).
Clinical measures of neurobehavioral function
Two domains of cognitive function, including processing speed and a select executive function (ability to maintain a complex set), were assessed in both age cohorts through Trail Making Test A and B (TMT-A) and TMT-B, respectively. 45 Higher scores (i.e., slower completion times) represent worse performance on both TMT-A and TMT-B. General distress and psychiatric symptoms were assessed through the Brief Symptom Inventory-18 (BSI-18). 46 Three subscales representing different dimensions of psychiatric symptomatology, including depression, somatization, depression, and anxiety were calculated from the 18 items and converted to standardized T-scores (mean = 50; SD = 10).
Statistical analyses
General linear regression models were fit to determine the interaction effect of years of football participation and age cohort on primary white matter metrics of WMH volume and mean OD, Vic, and Viso in the global WM ROI, with main effects of age cohort and years of participation. To further interrogate global WM interaction effects in which a significant age cohort by years of participation effect was observed, follow-up analyses involving similar regression models with age cohort by years of participation interactions were fit for individual white matter ROIs that contribute to the global white matter metric (listed in Table 3). Associations between concussion history and the four primary white matter metrics of interest (WMH volume, OD, Vic, Viso) were examined separately across age cohort due to sample differences in distribution of concussion history. Specifically, as noted above, concussion history was characterized as a categorical variable, including groups of 0, 1, and 2 or more (2+) prior concussions in the adolescent/young adulthood cohort and a continuous variable in the early midlife cohort. Linear regression models examining the association between concussion history and white matter metrics of interest were fit and post-hoc ROI models were fit for white matter ROIs in which a significant global average white matter diffusion effect was observed. Additionally, for white matter metrics in which a year of participation by age cohort interaction is observed, Spearman’s correlation coefficients were calculated for the WM metric identified and years of participation with the five neurobehavioral measures for each age cohort independently. Statistical significance was evaluated at the 0.05 uncorrected alpha level and correction for multiple comparisons was not employed based on the expected effect size, nature of the population (younger, nonclinical /healthy), and complementary nature of the analyses (see Supplementary Data S1 for further justification). For all models in which the assumption of homoscedasticity was violated, robust standard errors were calculated and included for interpretation of parameter estimates. This approach adjusts standard errors of the model for instances in which model residuals, or the size of the error term, varies across the continuum of independent variable. 47 Statistical analyses were conducted using IBM SPSS Statistics version 27 (Armonk, NY). All data used for the above analyses are available in the Supplementary Data S1 and Supplementary Data S2.
Results
Participant characteristics
Among the adolescent/young adulthood cohort, a total of 86 participants met the criteria for study inclusion. Image reconstruction or processing failed in four cases, resulting in a final sample of n = 82. The sample mean age was 18.4 ± 1.7 years with a mean of 8.6 years ± 2.7 of prior football participation. Of the adolescent/young adulthood cohort, 16 (19.5%) were enrolled in high school and 66 (8.05%) participants were enrolled in collegiate football. Concussion history in this cohort included those with 0 (n = 49; 59.8%), 1 (n = 18; 22.0%), and 2+(n = 15; 18.2%). Of the 39 eligible early midlife cohort of former collegiate football players, two were not included in the analyses due to discontinuation of the neuroimaging session (n = 1) and failed processing (n = 1). The remaining participants (n = 37) reported a mean age of 37.7 ± 1.4 years and 12.0 ± 3.2 years of prior football participation. Concussion history within this cohort of former players approximately 15 years removed from sport included a median of 4 (IQR = 1–7; range = 0–14). Further demographic and medical/psychiatric history for both cohorts are provided in Table 1.
Demographic and Participant Characteristics
White matter hyperintensities
A significant age cohort by years of participation interaction on WMH volume, B = 0.02, robustSE = 0.11, p = 0.841 was not recorded for the full sample (Table 2). When the nonsignificant interaction was removed from the model, a main effect of years of participation, B = −0.05, robustSE = 0.06, p = 0.396, was not observed (Supplementary Table S2). As expected, a greater degree of WMH burden was observed among the early midlife cohort as compared with the adolescent/young adulthood athlete cohort, B = −2.02, robustSE = 0.372, p < 0.001. Significant associations of greater history of concussion were not observed for the adolescent/young adult, (0 compared with 1, B = −0.37, robustSE = 0.59, p = 0.533 and 0 compared with 2+, B = 0.73, robustSE = 0.38, p = 0.058), or the early midlife cohort B = 0.05, SE = 0.04, p = 0.246.
White Matter Alterations and Years of Participation across Age Cohorts
Part., participation; WM, white matter; CI, 95% confidence interval; WMH, white matter hyperintensities; Beta, unstandardized beta coefficient; SE, standard error; partial η2, partial eta-squared.
Robust standard error parameterized within model
White matter microstructure
Within the full sample, a significant age cohort by years of participation interaction was observed for OD, B = −0.002, robustSE = 0.001, p = 0.001 (Table 2; Fig. 1). This interaction effect was driven by disparate associations of years of participation and OD across the two age cohorts. Specifically, among the adolescent/young adulthood athlete cohort, there was a significant inverse association between years of participation and OD, B = −0.001, SE = 0.0003, p = 0.010. Conversely, among early midlife former football players, greater years of participation were associated with greater global white matter OD, B = 0.001, SE = 0.0003, p = 0.018. Associations between years of participation and whole brain white matter OD remained statistically significant when controlling for history of concussion across the adolescent/young adulthood athlete cohort, B = −0.001, SE = 0.0004, p = 0.009, and early midlife cohort, B = 0.0009, SE = 0.0003, p = 0.017.
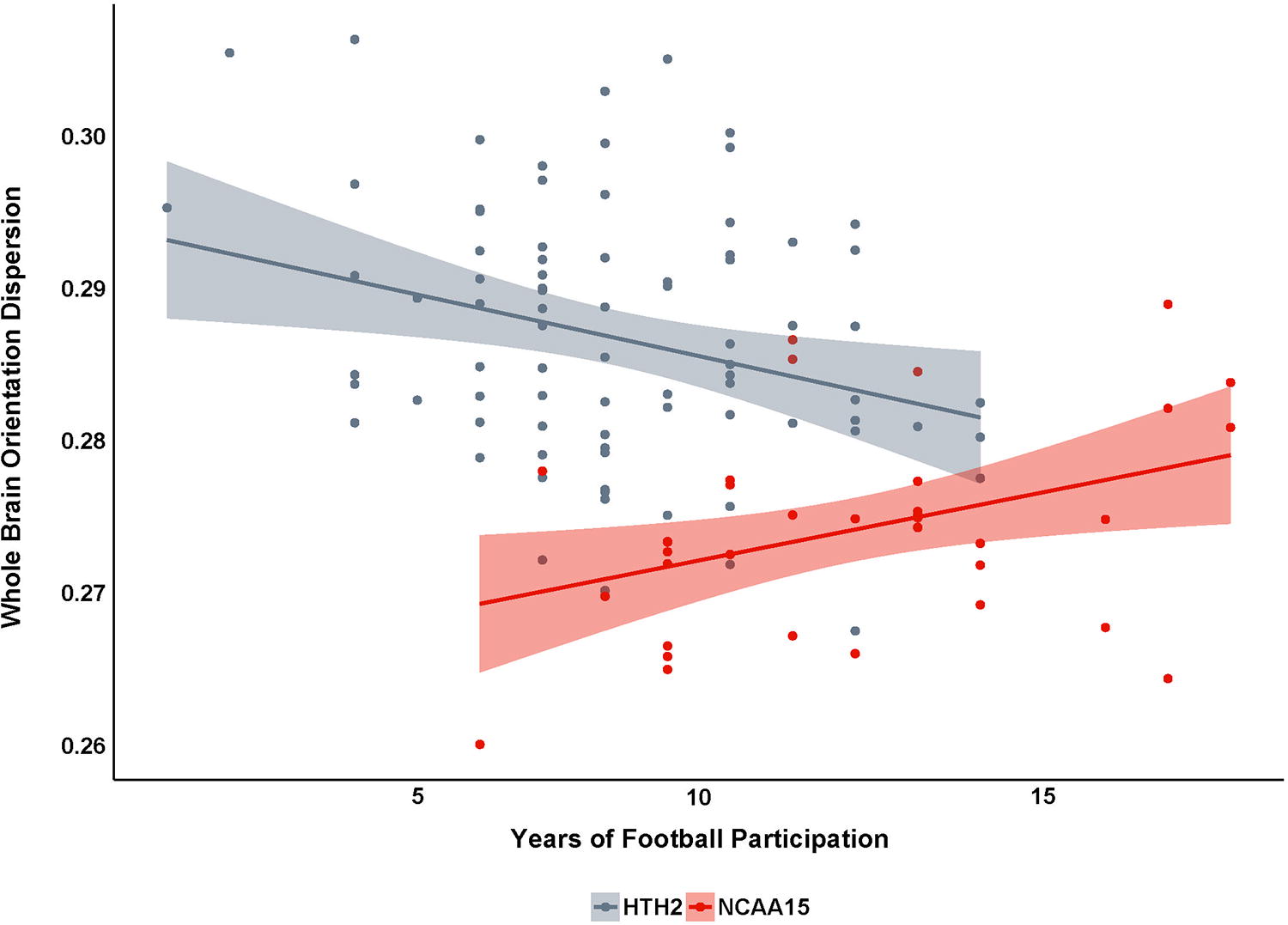
Scatterplot of NODDI orientation dispersion with years of participation across both age cohorts. NODDI, neurite orientation dispersion and density index.
Post-hoc ROI analyses revealed that differences in whole brain white matter OD associated with years of participation across age cohorts were primarily driven by significant age cohort and years of participation interaction effects in the following structures (bilateral): body of the corpus callosum, genu of the corpus callosum, cingulum, inferior fronto-occipital fasciculus, superior longitudinal fasciculus, and posterior thalamic radiation (p values <0.05; Table 3; Fig. 2; Fig. 3).
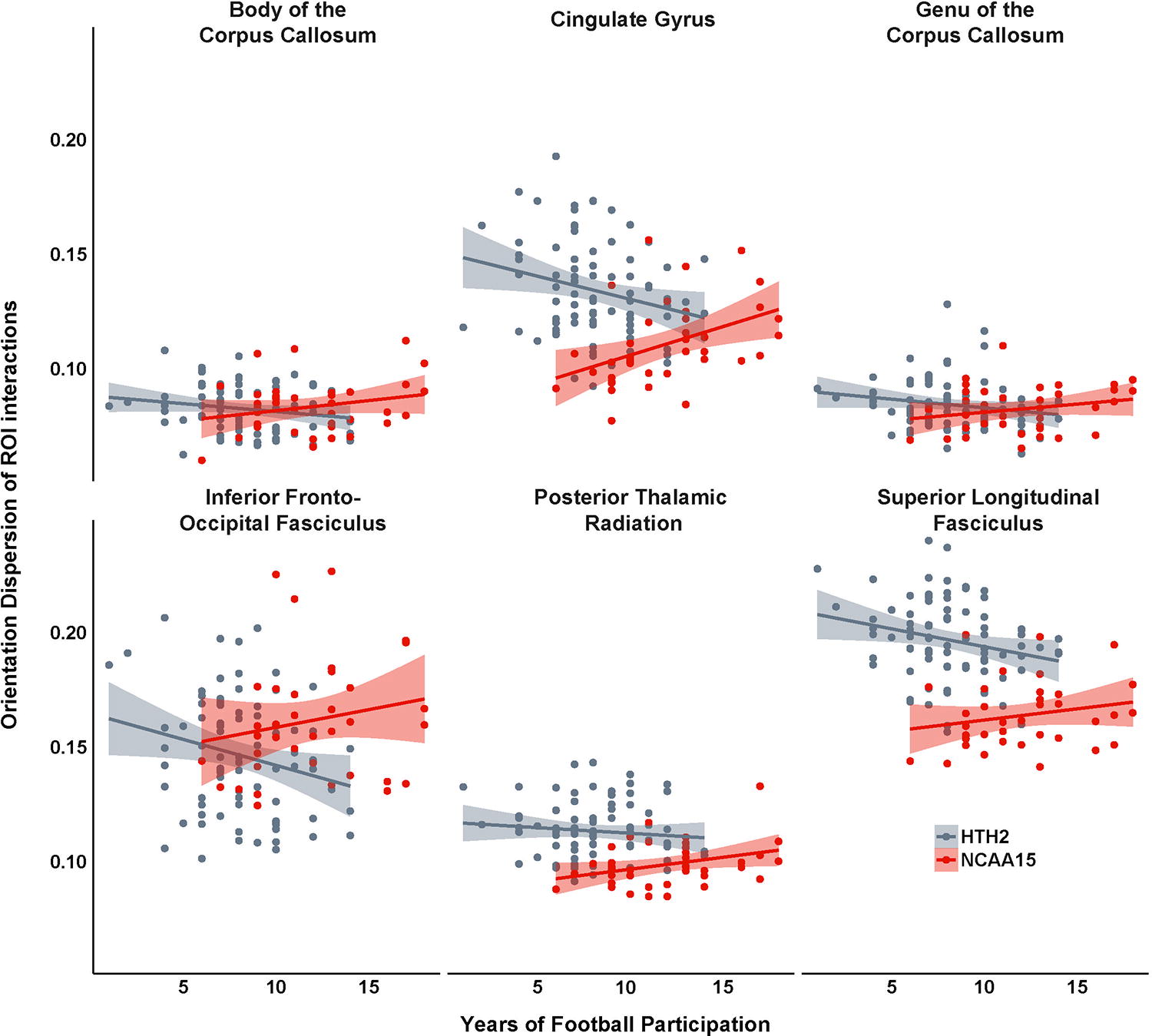
Scatterplot of NODDI orientation dispersion for ROIs in which age cohort and years of participation was observed. NODDI, neurite orientation dispersion and density index; ROI, region of interest.

Strength of interaction effect (-Log10 p value) of age cohort and years of participation on orientation dispersion for bilateral ROIs; coordinates provided in MNI space. MNI, Montreal Neurological Institute; ROI, region of interest.
Age cohort by Years of Participation Interaction Effects on Orientation Dispersion Regions of Interest
ROI, region of interest; CI, 95% confidence interval; Beta, unstandardized beta coefficient; SE, standard error; partial η2, partial eta-squared; CR, corona radiata; IC, internal capsule; CC, corpus callosum; HPC, hippocampus; FO, fronto-occipital; PTR, posterior thalamic radiation; LF, longitudinal fasciculus.
Robust standard error parameterized within model.
Within the adolescent/young adulthood cohort, history of concussion was not significantly associated with whole brain white matter OD, Viso, or Vic, p values >0.05 (Table 4). In the early midlife cohort, a greater history of concussion was associated with greater whole brain white matter Viso, B = 0.0007, SE = 0.0002, p = 0.010, but not OD, B = −0.00003, SE = 0.0003, p = 0.918, or Vic, B = −0.0004, SE = 0.0007, p = 0.586. Significantly higher whole brain white matter Viso among those with greater history of concussion in the early midlife cohort remained statistically significant when accounting for years of participation within the model, B = 0.0008, robustSE = 0.0004, p = 0.031. Interestingly, within these analyses in the early midlife cohort accounting for number of prior concussions, years of participation was also positively associated with Viso, B = 0.0008, robustSE = 0.0003, p = 0.016. Post-hoc ROI analyses showed that number of prior concussions was significantly associated with greater Viso in the body of the corpus callosum only, B = 0.001, SE = 0.0003, p = 0.001 (Table 5). This potentially indicates that the association between the number of prior concussions and greater whole brain white matter Viso may represent more global, diffuse increases in free water.
Concussion History and White Matter Metrics in Adolescent/early Adulthood Athletes
Part., participation; WM, white matter; CI, 95% confidence interval; WMH, white matter hyperintensities; Beta, unstandardized beta coefficient; SE, standard error; partial η2, partial eta-squared.
Robust standard error parameterized within model.
Number of Prior Concussion and Isotropic Volume Fraction across Regions of Interest
ROI, region of interest; CI, 95% confidence interval; Beta, unstandardized beta coefficient; SE, standard error; partial η2, partial eta-squared; CR, corona radiata; IC, internal capsule; CC, corpus callosum; HPC, hippocampus; FO, fronto-occipital; PTR, posterior thalamic radiation; LF, longitudinal fasciculus.
aRobust standard error parameterized within model.
Given the scanner/protocol differences across age cohorts, sensitivity analyses were performed in an attempt to reduce the potential inherent differences in NODDI metrics and WMH volume associated with these factors. Linear-mixed effect models in which age cohort/site were modeled as a random effect (i.e., independent intercepts) were fit to test the interaction effect of age and years of participation on white matter outcomes. The sensitivity analyses revealed results that were generally comparable to those reported above, showing significant age (years) by years of participation interaction for OD, B = 0.00009, SE = 0.00003, p < 0.001, but not for other white matter metrics of interest p values >0.05. Additionally, due to the fact that there were notable differences in years of football participation across the two cohorts, sensitivity analyses were performed to replicate the age cohort by years of participation interaction effect for OD in a “matched exposure” sample. Specifically, the lower end of exposure in the adolescent/young adult cohort was restricted to best match the early midlife cohort by only including those with 9+ years of prior football exposure. This achieved broadly comparable group size and exposure across the two cohorts (adolescent/young adult cohort n = 32, mean football exposure = 10.8 ± 1.5; early midlife cohort n = 34, mean football exposure = 12.4 ± 2.9). Results from these sensitivity analyses revealed a similar age cohort by years of participation interaction effect on OD, B = −0.002, robustSE = 0.001, p = 0.015. In addition, when split by age cohort, similar inverse associations were observed, such that more years of participation was associated with less OD in the adolescent/young adult cohort (to a lesser degree), B = −0.002, SE = 0.001, p = 0.103, whereas more years of participation was associated with greater OD in the early midlife cohort, B = 0.001, SE = 0.003, p = 0.055.
Clinical measures of neurobehavioral function
Given that a significant interaction effect for age cohort by years of participation was observed for global OD, Spearman’s correlations were calculated for years of participation and global OD with clinical outcome measures for each age cohort independently. Results revealed a significant correlation between years of participation and Trail Making Test B, ρ = 0.34, p = 0.04, for the early midlife cohort, but not the adolescent/young adulthood cohort (p values >0.05). A trend association was also observed for global OD and Trail Making Test B, ρ = 0.28, p = 0.09 for the early midlife cohort, but not the adolescent/young adulthood cohort (p values >0.05). Significant associations between years of participation and global OD with other clinical measures of neurobehavioral function were not observed for either cohort (p values >0.05; Table 6). Associations between significant OD ROIs (based on age cohort and years of participation interaction effects) and neurobehavioral measures are provided in Supplemental Table S3.
Spearman’s Correlation Coefficients for Years of Participation and Global White Matter Orientation Dispersion with Clinical Outcomes
Yrs., years; WM, white matter; OD, orientation dispersion; R, Spearman’s rho; BSI, Brief Symptom Inventory-18 item.
Discussion
Microstructural white matter integrity, but not macroscopic WMH volume, was significantly associated with years of football participation in this study of active and former football players between the ages of 14 and 41. The pattern of white matter changes associated with years of participation during adolescence/young adulthood through early midlife was broadly similar (i.e., alterations in neurite orientation dispersion with minimal association with macroscopic white matter lesions), although the association between years of participation and microstructural white matter abnormalities was inverted later in the lifespan at early midlife. Future longitudinal studies are required to track the evolution of these abnormalities and the way in which they may or may not progress toward macroscopic lesions and/or rarefaction later in the lifespan.
Exposure and white matter in adolescents/young adults and early midlife
The observed changes in white matter microstructure in the current study align with the limited prospective studies examining changes pre- to postseason and cumulative exposure over multiple seasons of contact sport exposure. Specifically, prior studies have observed significantly decreased OD 48 and increased FA 49 (which correlates with OD in nonconcussed individuals) 50 among collegiate and high school football players, respectively, over the course of multiple seasons of exposure. Importantly, many of the regions of interest (body of the corpus callosum, superior longitudinal fasciculus, thalamic radiation, and cingulum) associated with years of participation in the current study showed a high degree of overlap with pre- to postseason and cumulative changes over the course of multiple seasons in the aforementioned studies. Altogether, these studies demonstrate that white matter microstructural alterations in particularly vulnerable regions are observed following one season and increase with cumulative exposure over multiple years in high school and collegiate contact sport athletes.
Many previous investigations of white matter microstructure abnormalities among former contact sport athletes have involved professional athletes and group-level comparisons (athletes vs. controls), which limit generalizability and the ability to differentiate concussion history from cumulative contact sport exposure. 51 –53 Within a study of older (mean age = 55), symptomatic former football players with a range of playing-level histories, a targeted analysis of corpus callosum revealed white matter microstructural abnormalities in a select subregion of the corpus callosum with greater estimated head impact exposure based on an advanced exposure metric (CHII); 54 although concussion history could not be differentiated and exposure effects outside of the corpus callosum were not reported. Among the former football players in the current study, greater years of football participation was associated with lower global and region-specific white matter alterations (i.e., OD), which remained stable when controlling for history of concussion. Ultimately, this suggests that diffuse exposure-specific effects in white matter microstructure can be observed at early midlife among former athletes at levels of play below the professional level, as well as in current, adolescent, and young adult athletes.
Microstructure alterations associated with exposure and lifespan differences
The specific process(es) underlying the alterations in OD associated with years of football participation, as well as the opposite associations across age cohorts cannot be definitively determined based on the study data. In general, OD represents the coherence of neurite organization and the degree to which neurites are positioned in parallel as compared with being distributed in space. It has been suggested that alterations in OD reflect a range of contributing factors, depending on the clinical sample and direction. In other words, a similar increase in OD may reflect elevated neurite dispersion due to acute neuroinflammation, 55,56 axonal loss/degeneration, 57 demyelination, 58 or other potential processes. 59 Future preclinical and multimodal imaging human subject studies are required to further interrogate the underling pathology driving alterations in neurite orientation dispersion associated with years of football participation.
The developmental course of white matter microstructure organization (i.e., OD) based on the advanced multicompartmental diffusion modeling of NODDI follows a steady increase throughout the lifespan, with a more curvilinear increase around the seventh decade of life. 60,61 Although the precise process driving opposing OD effects within the current cohorts cannot definitely be determined, it is possible that lower levels of neurite dispersion (i.e., decreased OD) associated with more years of participation among the cohort of adolescent and young adult football players may reflect slowed or delayed maturation of white matter microstructure development. This pattern of decreased OD may also reflect a process of repair and/or regeneration, such as gliosis 62,63 and axonal white matter regeneration associated with neuroplasticity; 64 –66 although these findings have been primarily reported in TBI populations/animal models, particularly involving greater injury severity. Alternatively, it cannot be fully ruled out that the observed decrease in neurite dispersion represents a more favorable process, such as greater white matter microstructure integrity associated with the beneficial effects of physical activity. 67
Given that OD progressively increases with age, the higher levels of neurite dispersion (i.e., higher OD) associated with more years of football participation within the early midlife cohort may reflect an advanced or accelerated trajectory of aging. As noted above, these alterations in white matter microstructure associated with greater years of participation may represent a potential risk factor, among several other modifiable risk factors, 68 for adverse outcomes and ADRDs later in life. 69,70 Autopsy studies of former American football players (majority at the professional level) have observed greater levels of rarefaction and decreased levels of myelin proteins (proteolipid protein 1 and myelin-associated glycoprotein) within white matter, which would be consistent with the global and region-specific increases in neurite dispersion observed in the current study. Future longitudinal studies within these cohorts are required to assess the contribution of white matter microstructure alterations as a potential risk factor an accelerated course of aging and ADRD risk.
White matter hyperintensities/macroscopic lesions
Within the current study, WMH (macroscopic lesion) volume was not significantly associated with greater years of football participation or number of prior concussions across either cohort. WMH burden was not significantly greater among former professional football players <60 years of age compared with asymptomatic men without a history of football participation within the DETECT CTE cohort. 25 Conversely, greater WMH burden in the frontal, temporal, and parietal lobes, as well as total volume, was recorded in former professional football players ≥60 years of age compared with asymptomatic men without football history of the same age. Regardless of age, total years of football play were not associated with WMH burden in the aforementioned study. Within a subset of the DETECT CTE cohort, associations between RHI exposure and white matter microstructural abnormalities (i.e., axial diffusivity) were recorded within the full age range of enrolled former football players (aged 40–69 years). 54 Taken together, results from the current study indirectly align with those reported in an independent cohort of former football players described throughout above, in that both show associations with head impact exposure and microstructural alterations regardless of age, but limited evidence of greater WMH burden at younger ages among those with higher levels of football participation.
While diffusion was only examined for subregions of the corpus callosum in the aforementioned DETECT CTE study, differences in white matter microstructural abnormalities were significantly associated with neurocognitive measures of processing speed and executive function, depending on the particular subregion. 54 Within the current study a trend association between global WM OD and a select executive function was observed, both of which were significantly associated with years of participation. In a large sample of 328 older adults with a range of cognitive statuses (unimpaired to dementia), NODDI metrics significantly correlated with global cognitive function and performance in multiple domains, but were most robustly associated with TMT-B across various white matter tracts. 70 Investigations into the degree to which measures of white matter microstructure correlate with cognition during adolescence and young adulthood are limited, one study did not observe a significant association between DTI metrics and performance on computerized cognitive battery in hockey players during young adulthood. 71 The small, but notable associations of global white matter OD and executive function in only the early midlife cohort in the current study may reflect an intermediary period where the strength of the relationship intensifies with greater age, as reported in other studies of older adults. 70,72
The above-reported collection of results indicates that age may interact with microstructural abnormalities to evolve toward greater WMH burden over time. Although diffusion abnormalities within NAWM have been observed as preceding the development of WMH lesions longitudinally, the rate of progression and evolution can vary significantly based on several factors, such as cardiovascular burden and neuroinflammation, and WMH regression has been reported in a number of studies. 13,43,73,74 As such, the white matter microstructural abnormalities observed in the current study of adolescent/young adulthood through early midlife football players potentially represent a vulnerability whereby pathological aging and risk for later life cognitive decline associated with WMH burden may be instigated or exacerbated by other modifiable and nonmodifiable (e.g., genetic) risk factors. 75,76 Future studies are needed to better understand the evolution of white matter changes and moderating factors across the lifespan in younger contact sport athletes.
Limitations
There are a number of limitations of the current study worth mentioning when interpreting the reported findings. First, the self-report nature of prior concussions and years of participation contains the potential for retrospective recall error; although years of participation would be expected to consist of less error due to less uncertainty with diagnosed versus undiagnosed concussions. Years of football participation is a proxy metric for RHI exposure and does not contain more granular details of exposure, such as games started and contact hours. Relatedly, years of contact sport exposure outside of football was not included as part of the RHI proxy, and omission of this information may introduce error (over- or underestimation) in the study estimates of exposure with white matter metrics. Within the current study, the site/scanner differed across age cohort and the effect size of the interaction between the two age cohorts in OD may be biased to some degree. Although OD values can be affected by the scanner and protocol, an age by years of participation interaction on OD was observed in sensitivity analyses involving mixed-effect models with site parameterized as a random factor (independent intercepts). Additionally, the inverse association between OD and years of participation across age cohorts was observed independently when analyzed separately. Only two b-values were used as part of the higher order NODDI diffusion model, while three b-values are more common. While this may potentially result in misclassification of tissue and free-water signal, prior studies have effectively applied this approach in identifying group differences in other clinical populations. 77
The comparability of the current sample to the reference population is an important consideration with regard to the generalizability of the current findings. Football players who did not identify as White are somewhat underrepresented in the early midlife cohort based on the available reported demographic data of collegiate football players for the 2000–2001 season (cohort comprising 78% compared with 63% of White-identifying players; 16% compared with 28% Black-identifying players, and 5.4% Multiracial identifying compared with 9% ‘other’ identifying). 78 The adolescent/young adult cohort generally reflected the racial identity distribution of the reference population (mainly division III collegiate football players; although notable differences between Division I and III demographics exist) when data were collected, with 77% compared with 69% White-identifying players, 22% compared with 18% Black identifying players, and 1% American Indian/Alaskan Native identifying compared with 12% “other.” 79 Although direct comparison is difficult due to discrepancies in age bands for published data, the frequency of vascular risk factors (hypertension, hyperlipidemia, coronary artery disease) was slightly lower in the early midlife cohort compared with national prevalence rates, and the current sample may under account for additional cardio/cerebrovascular contributions to WM changes. 80,81 These two above points in conjunction are notable given rates of vascular risk factor burden are greater among Black-identifying individuals, and as such, cerebrovascular changes may have a disproportionate effect in aging. 82,83 Taken together, while the current findings indicate that greater years of contact sport participation may influence white matter alterations from adolescence to early midlife, the magnitude of these estimates may slightly under-represent the true degree of this association in the overall population of contact sport collegiate athletes where potential for compounding risk exists.
Conclusions
The global characterization of white matter changes associated with years of football participation were broadly similar and stable from adolescence/young adulthood through early midlife (microstructural alterations, but not macroscopic lesions predictive of future cognitive declines). An inverse association between years of participation and orientation dispersion across age cohorts may represent a process of initial recovery/reorganization proximal to sport, followed by later reduction of white matter organization/integrity. Future longitudinal studies are required to track the evolution of these abnormalities and the way in which they may progress toward further white matter degradation, as well as factors that may attenuate or potentiate these changes.
Transparency, rigor, and reproducibility summary
Sample size was determined based on enrollment of the parent studies and not planned a priori power analyses; however, with 119 subjects, the study had 80% power to detect Spearman’s correlation of ± 0.26 for the years of participation and age cohort effect for white matter metrics (WMH, WMH, OD, Vic, Viso) at a significance criterion of .05 for a two-tailed test. Regarding concussion history, the study had 80% power to detect Spearman’s correlation of ± 0.45 for the concussion history and white matter metrics (WMH, WMH, OD, Vic, Viso) analyses within the early midlife cohort at a significance criterion of .05 for a two-tailed test. For the adolescence/young adulthood cohort, the study had 80% power to detect group differences (1 prior concussion or 2+ prior concussions compared with 0 prior concussions) of medium magnitude (Cohen’s f = 0.35) at the .05 level. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was used to guide processes of the study. Of the 125 eligible participants enrolled in the parent studies, six were excluded due to failed processing of neuroimaging data and/or poor data quality. 84 Neuroimaging (dMRI, T1w, and FLAIR) acquisition parameters and sequences are provided in the article. All neuroimaging preprocessing and processing were completed using standardized, open-access pipelines and methods (e.g., FSL, QSIprep, QSIrecon, TBSS, ENIGMA ROIs). These methods, along with links for online access, are provided in the article and in greater detail within the supplemental methods section. A deidentified dataset of all the variables used to complete the study analyses are provided as an attachment in the Supplemental Content.
Footnotes
Acknowledgments
The authors thank Alexa Wild, Amy Nader, Robyn Furger, and Candice Goerger for study coordination and operational management; Daniel Huber for assistance with data quality and management; and Nicholas Weyenberg and Lezlie España for assistance with data quality, management, and processing of neuroimaging data. The authors are grateful for the participation of the athletes without whom this research would not be possible.
Authors’ Contributions
B.L.B.: Designed and conceptualized the study, analyzed data, and drafted and revised the article for intellectual content. A.K.: analyzed data, and drafted and revised the article for intellectual content. P.V.: analyzed data, and revised the article for intellectual content. S.O.: analyzed data, and revised the article for intellectual content. K.G.: Designed and conceptualized study, revised the article for intellectual content, and major role in acquisition of the data. M.A.M.: Designed and conceptualized study, revised the article for intellectual content, and major role in acquisition of the data. T.B.M.: Designed and conceptualized study, analyzed data, and drafted and revised the article for intellectual content.
Author Disclosure Statement
Dr. Brett reports grants from the National Institute on Aging and National Institute of Neurological Disorders and Stroke, and honoraria for conference presentations. Dr Guskiewicz reports compensation from National Collegiate Athletic Association for other services and grants from Boston Children's Hospital (subaward from the National Football League). Dr. McCrea reports researching funding to Medical College of Wisconsin from the National Institutes of Health, Department of Defense, Department of Veterans Affairs, Centers for Disease Control and Prevention, National Football League, National Collegiate Athletic Association, and Abbott Laboratories. He previously served as a consultant to Neurotrauma Sciences, Inc. and is a clinical consultant to the Green Bay Packers professional football club. He also reports honoraria and travel support for professional speaking engagements. Dr Meier reports receiving compensation as a member of the Clinical and Scientific Advisory Board for Quadrant Biosciences Inc, and grants from the National Institute of Neurological Disorders and Stroke and the Department of Defense.
Funding Information
This study was supported by the Department of Defense Broad Agency Announcement for Extramural Medical Research through award number W81XWH-14-1-0561, National Institutes of Health National Institute on Aging under award number K23AG073528-01, and National Institute of Neurological Disorders and Stroke of the NIH under award numbers R01NS102225 and L30NS113158, and National Collegiate Athletic Association. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding bodies.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Data S1
Supplementary Data S2
Supplementary Methods