
Abstract
Central cord syndrome (CCS) is the most prevalent and debated incomplete spinal cord injury (SCI) syndrome, with its hallmark feature being more pronounced weakness of the upper extremities than of the lower extremities. Varying definitions encapsulate multiple clinical features under the single umbrella term of CCS, complicating evaluation of its frequency, prognosis discussions, and outcomes research. Often, people with CCS are excluded from research protocols, as it is thought to have a favorable prognosis, but the vague nature of CCS raises doubts about the validity of this practice. The objective of this study was to categorize CCS into specific subsets with clear quantifiable differences, to assess whether this would enhance the ability to determine if individuals with CCS or its subsets exhibit distinct neurological and functional outcomes relative to others with incomplete tetraplegia. This study retrospectively reviewed individuals with new motor incomplete tetraplegia from traumatic SCI who enrolled in the Spinal Cord Injury Model Systems (SCIMS) database from 2010 to 2020. Through an assessment of the prevailing criteria for CCS, coupled with data analysis, we used two key criteria, including the severity of distal upper extremity weakness (i.e., hands and fingers) and extent of symmetry, to delineate three CCS subsets: full CCS, unilateral CCS, and borderline CCS. Of the 1490 participants in our sample, 17.5% had full, 25.6% had unilateral, and 9% had borderline CCS, together encompassing >50% of motor incomplete tetraplegia cases. Despite the increased sensitivity and specificity of these subsets compared with existing quantifiable criteria, substantial variability in clinical presentation was still observed. Overall, individuals meeting CCS subset criteria showed a higher likelihood of American Spinal Injury Association (ASIA) Impairment Scale (AIS) D grade than those with motor incomplete tetraplegia without CCS. Upper Extremity Motor Score (UEMS) for those with CCS was lower on admission, a difference that diminished by discharge, whereas their Lower Extremity Motor Score (LEMS) consistently remained higher than for those without CCS. However, these neurological distinctions did not result in significant functional differences, as lower and upper extremity functional outcomes at discharge were mostly similar, with some differences observed within those with AIS D grade. The AIS grade, rather than the diagnosis of CCS, remains the foremost determinant influencing neurological and functional outcomes. We recommend that future studies consider incorporating motor incomplete tetraplegia into their inclusion/exclusion criteria, instead of relying on criteria specific to CCS. Although there remains clinical value in characterizing an injury pattern as CCS and perhaps using the different subsets to better characterize the impairments, it does not appear to be a useful research criterion.
Introduction
The profile of people with acute traumatic spinal cord injury (SCI) in the last few decades has changed, with a significant increase in age at the time of injury, a higher percentage of injuries caused by falls, and incomplete tetraplegia becoming the most common type of neurological impairment. 1 –4 Central cord syndrome (CCS), the most common incomplete SCI syndrome, is widely estimated to account for 18–70% of incomplete tetraplegia cases 5 –7 and 6–32% of traumatic SCI cases overall. 8,9 CCS has been a topic for debate in terms of its definition 7,10 –13 and prognosis, 14,15 as well as in terms of the necessity of and/or optimal timing of surgery. 16 –18
The definition most commonly used today for CCS is based on the description by Schneider and coworkers in 1954 that portrayed “disproportionately more motor impairment of the upper than of the lower extremities, bladder dysfunction, usually urinary retention, and varying degrees of sensory loss below the level of the lesion.’’ 19 The criteria for what constitutes “disproportionally more motor impairment” remains a topic of discussion. 10,20,21 Consequently, the current definition is widely inclusive and results in the classification of a broad range of impairments and injury types, ranging from patients experiencing slight tingling or weakness in their hands and fingers to those with complete tetraplegia. 11,22 –24
Because of the lack of consistent quantifiable criteria, various definitions have been used in the literature to describe CCS, and its classification has often been subjective and based on clinical impression. 16,23,25 Over a decade ago, the European Multicenter Study about Spinal Cord Injury (EM-SCI) group recommended using ≥10 motor points in favor of the lower extremities (LEs) 10 to quantify disproportionate weakness (referred to in this paper as the EM-SCI criteria). This criterion was frequently referenced in recent years 15,26 –29 but has not achieved universal acceptance.
In a recent review of CCS, 30 we demonstrated that the quantifiable criteria used today encompass a diverse array of clinical features, collectively referred to as CCS. For example, the EM-SCI criteria, 10 as well as other classification systems, 24,31,32 often classify cases of unilateral weakness (of the upper extremities [UEs] compared with LEs), isolated proximal weakness (i.e., only at C5–6 myotomes), or very mild weakness (e.g., all manual muscle testing grades of 4 in the UEs and normal grades in the LEs) as CCS, while at times excluding cases with significant distal UE (C8–T1) weakness in comparison to the LEs. 7,30
As a result of the wide range of possible classifications, there are also inconclusive data on the neurological and functional outcomes of people presenting with CCS. 14,15 Previously, the general consensus was that patients with CCS typically had a favorable prognosis. 32 –34 However, it is now recognized that the distinction of CCS in incomplete tetraplegia does not guide prognosis or management. 13,14 In fact, the authors of the EM-SCI criteria concluded that the American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade was more useful in the prognostication of outcomes than the classification of an injury as CCS using the EM-SCI criteria. 14 Others also suggested that in clinical practice, the term CCS should be accompanied by the neurological level of injury (NLI) and AIS grade information. 12,14 The presumed favorable prognosis, along with diverse patient characteristics, often leads to the exclusion of individuals with traumatic CCS from retrospective and prospective SCI studies. 35 –37
The understanding of the pathophysiology and clinical presentation of CCS has also changed since its initial description. Although originally characterized as a lesion to the central gray matter of the cord, affecting the surrounding white matter and medially located fibers of the corticospinal tract (CST) that were thought to control hand and arm function, 19,38 –40 subsequent studies have demonstrated a diffuse white matter injury to the lateral columns and CST, rather than to the central cord. 24 It is also now apparent that the CST is not somatotopically organized, and is critical for hand function, but less so for ambulation. 24,41,42 Over the years it has become increasingly evident that the distal UEs; that is, the hands and fingers (innervated by C8–T1 myotomes), are most affected in CCS. This notion evolved from both clinical 43 –45 and pathophysiological 24,46,47 perspectives.
Because the diagnosis of CCS is not indicative of injury severity, prognosis, or pathophysiology, recent reports have recommended that the terminology and definition of CCS be revisited. 11 –13,48 Further, it has been questioned if CCS should even be regarded as a distinct entity in incomplete tetraplegia. 13,14 To address these concerns, the primary objectives of this study were to: (1) identify different variations of CCS, as existing criteria represent a board spectrum of cases of incomplete tetraplegia; (2) assess the prevalence of these subsets and their overlap with the EM-SCI criteria for CCS; and (3) compare neurological and functional outcomes of different forms of motor incomplete tetraplegia. To achieve these aims, we conducted a retrospective analysis of a large cohort of adults with traumatic SCI in the United States.
Methods
This investigation involved a secondary analysis of existing data from the national Spinal Cord Injury Model Systems (SCIMS) database. 49 Initiated in 1970, the SCIMS database is a prospective study of the continuum of care of people with traumatic SCI who receive rehabilitation from a network of centers throughout the United States. The database includes information on participants' demographics, injury characteristics, and long-term health, functioning, and community living outcomes. All participants provided informed consent according to protocols approved by the institutional review boards of the designated centers. Further information on the SCIMS database is described in detail elsewhere. 50 –52 This study involved data collected between 2010 and 2020 (n = 6997), when data elements characterizing individual dermatome light touch and pinprick scores were added to the SCIMS database.
Study population
The analytic sample was based on the following inclusion criteria: (1) being ≥16 years of age at the time of injury, (2) having a complete neurological examination between 3 and 30 days post-injury, and (3) having motor incomplete tetraplegia; that is, NLI between C1 and C8, and AIS grades of C or D. This resulted in a final sample size of 1490. Further analysis was performed for the subsample of individuals with complete discharge and 1-year follow-up neurological examinations (n = 368), and the subsample of individuals with Functional Independence Measure (FIM) 53 assessments on admission and discharge (n = 1284).
Outcomes
The neurological outcomes in this study, namely NLI, AIS, upper extremity motor score (UEMS), and lower extremity motor score (LEMS), were derived from examinations conducted according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 54 These measures were obtained at three distinct time points: the first complete neurological examination (usually upon admission to rehabilitation), discharge from rehabilitation, and the 1-year follow-up examination.
The FIM 53 was used for the assessment of the following functional outcomes on admission and discharge from acute rehabilitation: eating, upper body dressing, transfers, and ambulation. Independence was defined by a score of 6 (modified independence) or 7 (complete independence) on the FIM scale. To assess independent ambulation, similar to previous studies, 55,56 the locomotion component of FIM was used. Independent walking was defined by FIM locomotor score of 6 or 7 and locomotion mode of either “walk” or “both walk and wheelchair.” Independent transfers were defined by the “bed/chair/wheelchair” transfers component. FIM scores were only available for a portion of the sample, specifically, those enrolled through 2019, when the FIM was discontinued and replaced with the Continuity Assessment Record and Evaluation (CARE) Item Set at inpatient rehabilitation facilities across the United States. Further, FIM scores are only available at admission and discharge, as patient self-report measures are used in the SCIMS database at the 1-year follow-up and subsequent interviews to assess functioning of people living in the community.
CCS definitions
After a review of previous CCS descriptions and their limitations, 30 we developed several clinical subcategories of CCS using SCIMS data, prioritizing the following clinical features: (1) degree of distal UE weakness (in C8–T1 myotomes) to account for the importance of hand and finger weakness, and (2) degree of symmetry. By categorizing CCS into distinct clinical subsets, our goal was to highlight differences in the clinical presentation, with the expectation that these differences might be reflected in neurological and functional outcomes. These subsets were formulated using a combination of existing literature and data-driven methodologies. 19,24,30,34 The thresholds employed for these subsets were essential for describing and quantifying the variations, all while recognizing that there is no single definitive threshold. This led us to the following three categories of CCS: full (bilateral), unilateral, and borderline (see Fig. 1 for descriptions and Figs. 2 –4 for examples).

CCS Definitions. CCS, central cord syndrome; LE, Lower Extremity; UE, Upper Extremity; avg, average.
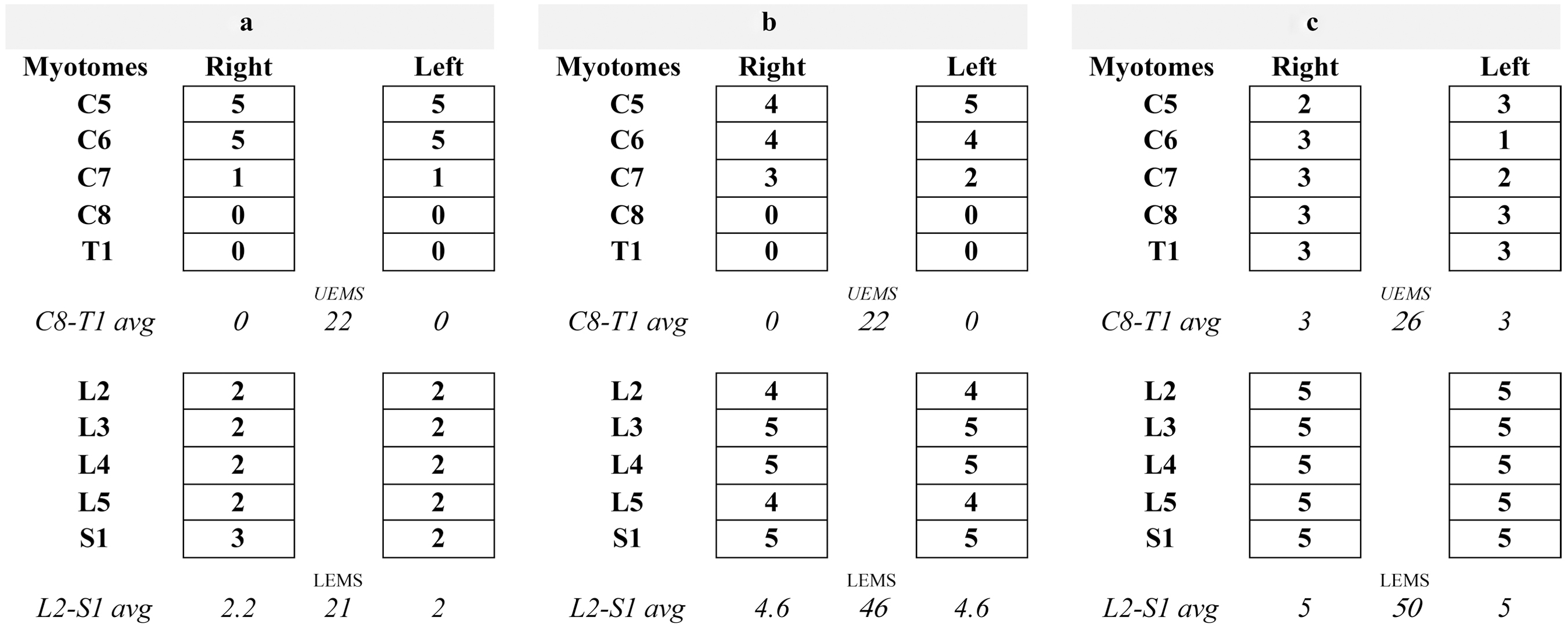
Sample cases from the SCIMS database that fulfill the criteria for full (bilateral) CCS (n = 260). SCIMS, Spinal Cord Injury Model Systems; CCS, central cord syndrome; UEMS, upper extremity motor score; LEMS, lower extremity motor score; UE, upper extremity; LE, lower extremity; avg, average.

Sample cases from the SCIMS database that fulfill the criteria for unilateral CCS (n = 381). SCIMS, Spinal Cord Injury Model Systems; CCS, central cord syndrome; UEMS, upper extremity motor score; LEMS, lower extremity motor score; UE, upper extremity; LE, lower extremity; avg, average.
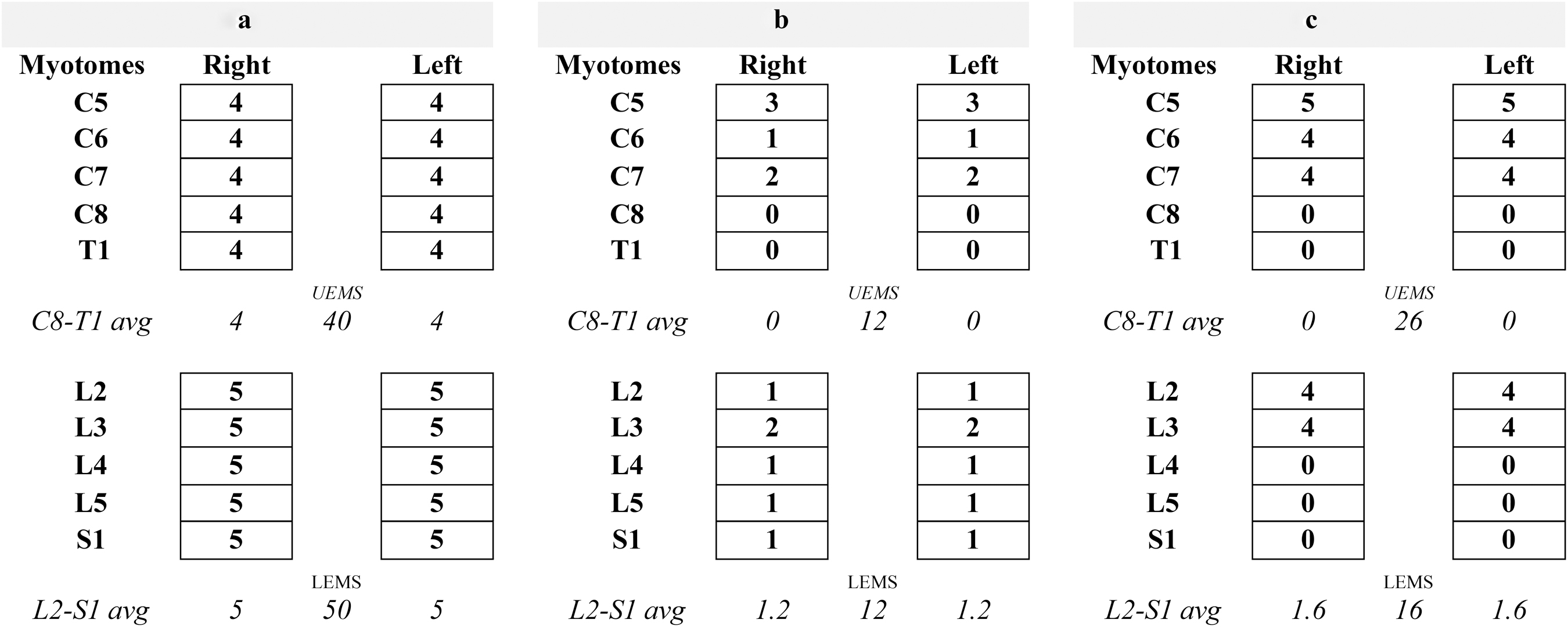
Sample cases from the SCIMS database that fulfill the criteria for borderline CCS (n = 134). SCIMS, Spinal Cord Injury Model Systems; CCS, central cord syndrome; UEMS, upper extremity motor score; LEMS, lower extremity motor score; UE, upper extremity; LE, lower extremity; avg, average.
Full (bilateral) CCS
This category represents the classic presentation of CCS, in which each side has a difference of ≥2 between the average lower extremity (L2–S1) motor scores and distal upper extremity (C8–T1) motor scores. The threshold of
Unilateral CCS
This category represents cases in which only one side fulfills the criteria of the difference between the averages of LE and distal UE motor scores of ≥2 (example depicted in Fig. 3). It is debatable whether such cases should be included in the CCS criteria; however, current criteria (e.g., EM-SCI) often include such cases. 30 It is therefore important to identify this form of clinical presentation, although it does not meet the criteria for the classic presentation of CCS.
Borderline CCS
Included in this category are cases exhibiting bilateral distal UE weakness compared with the LEs, but to a lesser extent than in full CCS. The difference of the average LE and distal UE motor scores is between 1 and <2 bilaterally (example depicted in Fig. 4).
Statistical analysis
Participant characteristics were summarized using means and standard deviations (SD) for continuous variables such as age (in years), and frequency counts and percentages for categorical variables. Associations between categorical variables were tested by χ 2 and Fisher's exact tests. A one-way analysis of variance (ANOVA) test was performed for a comparison of continuous variables and adjusted for multiple comparisons using the Bonferroni correction. In the comparison of neurological and functional outcomes, the data were stratified based on AIS grades C and D. A p value of <.05 was considered a statistically significant difference.
Results
A total of 1490 individuals with motor incomplete tetraplegia were included in this analysis. Of these, 368 (24.7%) had complete neurological data at discharge and the 1-year follow-up. Table 1 displays the admission characteristics of both the full sample and the follow-up sample. The distributions of the sample characteristics of those with and those without follow-up data were similar. The only notable exception was related to NLI, where those with follow-up were more likely to have a C1–C3 level injury (40.8% vs. 32.5%) and less likely to have a C4 NLI injury (27.4% vs. 33.4%) compared with the sample without follow-up data (χ 2 = 17.6, df = 7, p = 0.014).
Sample Characteristics Obtained Upon Admission to Acute Rehabilitation for Adults With Motor Incomplete Tetraplegia
Full analytical sample of adults with motor incomplete tetraplegia.
Subsample of adults with motor incomplete tetraplegia and complete neurological data at both discharge and the 1-year follow-up.
SD, standard deviation; AIS, American Spinal Injury Association (ASIA) Impairment Scale; NLI, neurological level of injury.
Frequency and variability of CCS subtypes
The categorization of the total sample (n = 1490) of individuals with motor incomplete tetraplegia into the different subtypes of CCS included 17.5% (n = 260) with full CCS, 25.6% (n = 381) with unilateral CCS, and 9.0% (n = 134) with borderline CCS. Together these comprise 52.0% (n = 775) of the total cases of motor incomplete tetraplegia included in this analysis.
Full CCS represents the classic form of CCS, with a significant difference in strength between the distal UE and LE on each side. Variability exists among the cases, with some predominantly demonstrating distal UE weakness (Fig. 2a), whereas the majority exhibit both distal and proximal UE weakness (Fig. 2c).
In unilateral CCS, one side displays significant distal UE weakness compared with the LE (difference ≥2); however, there is substantial variability on the other side, ranging from extreme weakness to intact motor scores. Of the 381 cases with unilateral CCS, 194 (50.9%) also exhibited some distal UE weakness on the other side, but to a lesser extent (difference between 1 and <2, see Fig. 3a). Twenty-three (6.0%) subjects were intact on the other side (i.e., combined UE and LE motor scores = 50, see Fig. 3b). The opposite scenario, of a very weak other side, was less frequent, as only two (0.5%) people with unilateral CCS had a score of zero in all myotomes on the other side (see Fig. 3c for a similar scenario, with a sum of left UE and LE motor scores = 1).
Unilateral CCS often demonstrated patterns of asymmetrical weakness (see Fig. 3), similar to Brown Sequard syndrome (BSS). However, in contrast to CCS definitions that almost always refer to the motor element alone, the definition for BSS also incorporates impairment in pinprick sensation (contralateral to the motor-impaired side) and light touch sensation (ipsilateral). 57,58 The distinctive clinical pattern of unilateral CCS lies in its description of UE weakness on a single side relative to the LE on the same side. Conversely, in BSS, one side is compared with the other. A total of 64 cases (16.8%) of unilateral CCS had BSS-like motor impairments (using recently proposed quantifiable criteria for BSS 7 ).
As demonstrated in Figure 4, there is also notable variability in borderline CCS. Of the 134 cases of borderline CCS, 30 (22.4%) had full LE strength (LEMS = 50, see Fig. 4a), whereas three (2.2%) had significant LE weakness (LEMS = 10) (see Fig. 4b for a similar scenario, with LEMS = 12).
Overlap with the EM-SCI criteria
Of the total sample of persons with motor incomplete tetraplegia, 39% (n = 582) fulfilled the EM-SCI criteria (LEMS - UEMS ≥10). 10 The breakdown of these 582 cases, using our subcategories for CCS, includes 235 (40.4%) cases with full CCS (example in Figs. 2b and c), 245 (42.1%) with unilateral CCS (Figs. 3b and c), and 64 (11.2%) with borderline CCS (Fig. 4a). The 38 (6.5%) remaining cases that fulfilled the EM-SCI criteria did not fulfill any of the CCS subcategories (see Fig. 5 for examples).

Sample cases from the SCIMS database that fulfilled the EM-SCI criteria, but none of the new CCS subcategories (n = 38). SCIMS, Spinal Cord Injury Model Systems; CCS, central cord syndrome; UEMS, upper extremity motor score; LEMS, lower extremity motor score; UE, upper extremity; LE, lower extremity; avg, average.
The EM-SCI criteria for CCS encompassed these new CCS subsets, but only in part, capturing 90% (235/260) of full CCS (see Fig. 2a for an example of a case missed by EM-SCI), 64% (245/381) of unilateral cases (see Fig. 3a for a case missed by EM-SCI), and 48% (64/134) of borderline cases (see Figs. 4b and c for cases missed by EM-SCI).
Demographics and injury characteristics
Although the three categories of CCS (i.e., full, unilateral, and borderline) may have benefits in describing the clinical presentation of individual cases, the classifications of unilateral and borderline CCS are composed of a large range of residual motor sparing, from significant weakness to almost intact strength. Our initial analysis using these classifications did not prove significant in delineating neurological and functional outcomes. Therefore, unilateral and borderline classifications were grouped and referred to as intermediate CCS variants for subsequent analyses.
As depicted in Table 2, persons classified with full CCS were, on average, older than those classified with intermediate and non-CCS (F[2,1487] = [4.238], p = 0.015). They were also more likely to have sustained their SCI as the result of a fall (χ 2 = 29.5, df = 8, p < 0.001). There were no differences in the acute rehabilitation length of stay (LOS) between the motor-incomplete tetraplegia subsets, with an average of ∼42 days for all (including those with non-CCS).
Participant Characteristics (Age and Injury Etiology) Within the Different Motor Incomplete Tetraplegia Subsets (n = 1490)
Intermediate CCS variants include the unilateral and borderline subsets.
Age differed significantly between the subsets: F(2,1487) = (4.238), p = 0.015, specifically between individuals with full CCS and those with non-CCS (p = 0.011).
Etiology differed significantly between the subsets: χ 2 = 29.5, df = 8, p < 0.001.
SD, standard deviation; CCS, central cord syndrome.
The most common NLI on admission for all motor incomplete tetraplegia subsets was C4, accounting for 36.2% of full CCS, 35.1% of intermediate CCS, and 28.1% of non-CCS cases. NLI at C6 or below was less common for persons with CCS, with ∼5% of full and intermediate CCS compared with 15.5% of non-CCS cases (see Table 3).
Number and Percentage of Participants in Each Motor Incomplete Tetraplegia Subset by Admission NLI (n = 1490)
A statistically significant difference in NLI was observed between the subsets (χ 2 = 68.8, df = 14, p < 0.001).
Intermediate CCS variants include the unilateral and borderline subsets.
CCS, central cord syndrome; NLI, neurological level of injury
Neurological outcomes
Of the subsample of 368 people with complete neurological data at all three time points (rehabilitation admission, discharge and 1-year follow up), 41.8% (n = 154) had an initial AIS C classification on admission. As reported in Table 4, the majority of these persons had converted to AIS D, with only 15.5% (n = 57) and 7.9% (n = 29) remaining an AIS C at rehabilitation discharge and at the 1-year follow up, respectively. There was a noted difference in initial AIS grade and improvement from AIS C to D at follow up at 1 year between those with CCS and non-CCS classifications. Specifically, nearly half (48.2%) of persons classified with non-CCS had an AIS C grade on admission, compared with only 20.3% of those with full CCS (χ 2 = 15.3, df = 2, p < 0.001). Individuals with non-CCS were also less likely to improve to AIS D grade at the 1-year follow-up, with 15.5% compared with 1.6% of those with full CCS remaining AIS C (χ 2 = 24.6, df = 2, p < 0.001).
Percentage of İndividuals With AIS C Grade on Admission and Discharge, and at the 1-Year Follow-Up (n = 368) Within the Different Motor İncomplete Tetraplegia Subsets
Statistical significant differences in AIS grades (C vs. D) across subsets were observed at each time point.
Intermediate CCS variants include unilateral and borderline subsets.
On admission, χ 2 = 15.3, df = 2, p < 0.001.
On discharge, χ 2 = 22.7, df = 2, p < 0.001.
At the 1-year follow-up, χ 2 = 24.6, df = 2, p < 0.001.
AIS, American Spinal Injury Association (ASIA) Impairment Scale; CCS, central cord syndrome.
In the full sample of motor incomplete tetraplegia, the average UEMS and LEMS on admission were 26.1 (± 13.7) and 30.6 (± 16.7), respectively, and 66% (n = 999) of individuals had higher LEMS score (LEMS - UEMS ≥1). Within the sample with complete follow-up data (n = 368), as expected, UEMS on admission was significantly lower for full CCS and intermediate CCS variants than for non-CCS; however, these differences were no longer present by discharge and at the 1-year follow-up. On the other hand, LEMS on admission was lowest for non-CCS and highest for full CCS, and remained lower for non-CCS through discharge and at the 1-year follow-up (see Table 5).
Average UEMS and LEMS on Admission, Discharge, and 1-Year Follow-Up, for Motor Incomplete Tetraplegia Subsets, Stratified by AIS (n = 368)
Analyses were performed separately for AIS C, AIS D, and the combined group. Additionally, separate individual analyses were conducted for each row. Comparisons that are
Full CCS versus non-CCS
Intermediate CCS variants versus non-CCS
Full CCS versus intermediate CCS variants.
Intermediate CCS variants include unilateral and borderline subsets.
UEMS, upper extremity motor score; LEMS, lower extremity motor score; CCS, central cord syndrome; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Functional outcomes
A total of 1284 individuals had FIM data at both admission and discharge from acute rehabilitation, as reported in Table 6. Upon discharge, individuals with full CCS were less likely to achieve independence in UE functions; namely, feeding and upper body dressing. For the former, 37.7% achieved independent feeding, compared with 49.7% of those with intermediate CCS variants and 52.9% of those with non-CCS (p < 0.001). The differences observed in upper body dressing were not statistically significant. By contrast, those with full CCS were more likely to be independent in transfers and ambulation, especially compared with persons with non-CCS, although there was no statistical significance.
Independence (FIM 6-7) on Discharge from Rehabilitation for Motor Incomplete Tetraplegia Subsets Stratified by AIS (n = 1284)
Analyses were performed separately for AIS C, AIS D, and the combined group. Additionally, separate individual analyses were conducted for each row. Comparisons that are
Intermediate CCS variants include unilateral and borderline subsets.
Independent walking is defined by a FIM locomotor score of 6 or 7 and mode locomotion of either “walk” or “both walk and wheelchair”.
FIM, Functional Independence Measure; CCS, central cord syndrome; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Within each subset, individuals with AIS C grade were substantially more dependent than those with AIS D in both upper and lower body functions (p < 0.001). Nevertheless, those with full CCS and AIS D grade were significantly less independent at discharge than others with AIS D (intermediate and non-CCS) in feeding, upper body dressing, and transfers.
Discussion
The current definitions of CCS have noted limitations, including heterogeneous injury patterns, severities, patient characteristics, and prognoses. In response to the need to re-evaluate and more specifically define the criteria, 11 –13,30,48 the objective of this study was to determine if greater delineation of the clinical variations of CCS would enhance its use in research inclusion/exclusion criteria and result in distinct neurological and functional outcomes.
Based on data analysis and insights from previous literature, three subsets of CCS (full, unilateral, and borderline) were established to better distinguish CCS from other types of incomplete tetraplegia. Despite the heightened sensitivity and specificity of these subsets compared with existing quantifiable criteria, considerable variability in clinical presentation still persisted within them. Although we observed differences in neurological outcomes between CCS subsets and other cases of motor incomplete tetraplegia, there were very few significant differences in functional outcomes at discharge (mainly feeding), as most differences were only significant within individuals with AIS D. Our analysis underscores that the initial AIS grade continues to be the primary determinant influencing outcomes, superseding the diagnosis of CCS, and that future studies should consider using criteria for motor incomplete tetraplegia as opposed to relying on CCS-specific criteria.
In our proposed clinical variations, we emphasize important characteristics that have not been addressed in previous definitions, specifically focusing on distal UE (i.e., hands and fingers) weakness and the extent of symmetry. Although Schneider and coworkers 19 and subsequent clinical and pathophysiological investigations have highlighted the prominent motor impairment of the distal UEs in CCS, this observation has not been translated into previously published definitions. 24,30,43 –47 Our new criteria addressed this gap by comparing the distal UEs to the LEs. In addition, it is worth noting that although the work of Schneider and others implies bilateral involvement in CCS, this aspect has not been consistently included in existing criteria. This is a noteworthy consideration, as weakness in CCS can exhibit different degrees of symmetry, ranging from complete symmetry to substantial asymmetry resembling Brown–Sequard syndrome. 24,34,59,60 The results from the subsample analysis also support the importance of this factor.
Based on our analysis, 52% of motor incomplete tetraplegia cases can be classified into three subtypes of CCS: full (17.5%), unilateral (25.6%), and borderline CCS (9.0%). The overall prevalence of the inclusive definition (all CCS subsets combined) of >50% is comparable to previous, albeit limited, data. 14 However, when using only the full CCS criteria, the prevalence of 17.5% in this study is lower than in other CCS studies, 7,14,61 which is unsurprising, given our utilization of a more specific definition for full CCS.
The widely used EM-SCI definition for CCS (LEMS−UEMS ≥10), serving as a basis for comparison with our findings, has acknowledged limitations 7,10 that arise from the definition's relative sensitivity in identifying individuals with prominent UE weakness, while lacking the specificity to differentiate between various subtypes of this syndrome. Our analysis demonstrated that the EM-SCI criteria partially overlaps with all subsets of CCS (full, unilateral, and borderline). However, numerous cases within these subsets did not meet the EM-SCI criteria. For example, certain cases of full CCS with significant weakness in the distal UEs were not classified as CCS according to the EM-SCI criteria. On the other hand, some cases with unilateral neurological deficits or only mild UE weakness were classified as CCS by the EM-SCI criteria without differentiation (see Figs. 2–4).
Although the suggested subsets of CCS may provide insights into the clinical patterns, it is worth noting that the categories of unilateral and borderline CCS still encompass a wide range of cases, posing challenges in accurately describing the clinical presentation and predicting neurological or functional prognosis. In unilateral CCS, there is significant variability in the strength observed on the contralateral side, whereas in borderline CCS, some individuals exhibit generalized weakness whereas others demonstrate nearly intact motor scores. Further, many clinicians may not even consider unilateral and borderline CCS to be genuine CCS, yet it remains important to define and quantify these subtypes, as they are often included within existing definitions of CCS. In the main analysis, we grouped unilateral and borderline CCS classifications into an intermediate CCS subtype. The subsequent comparison therefore involves full CCS, intermediate CCS variants, and non-CCS subsets of motor incomplete tetraplegia.
In line with previous literature for CCS, 7,14 full CCS was associated with older age and a higher incidence of falls. C4 was found to be the most common level of injury among all subsets of motor-incomplete tetraplegia (CCS or not). NLI at C6 or below was present in only ∼5% of individuals with any CCS, which is within the previously reported range of 2–20% of individuals with CCS having NLI at C6 or below. 7,14,15,62 These findings indicate that although our definitions primarily emphasize the distal UEs, there is typically some degree of involvement in the proximal UEs as well. However, the impairment observed in the proximal UE region is often less pronounced than that in the distal UEs.
Also in alignment with previous research, 7,14,15 individuals with CCS (full or intermediate) were more inclined to have AIS grade D than those with non-CCS. This disparity is evident from admission data through discharge and up to the 1-year follow-up. Notably, nearly all individuals with full CCS achieved recovery to AIS D, whereas 15% of those without CCS remained AIS C at 1 year. These distinctions, alongside our aim to maintain consistency with the EM-SCI group study, 14 led us to stratify neurological and functional outcomes based on AIS grades.
As expected, individuals with full CCS had lower UE motor scores on admission than the other subsets; however, by discharge there were no notable differences in UE muscle strength between the subsets. Despite this, people with full CCS demonstrated greater dependence in feeding tasks on discharge from rehabilitation. This may be explained by AIS grade stratification, which showed that those with full CCS AIS D had lower UE scores on discharge and were more dependent in various UE functional outcomes, including feeding, upper body dressing, and transfers, when compared with non-CCS AIS D individuals. It is possible that these functional differences may diminish by the 1-year follow up, particularly considering the nearly intact UE scores observed across all subsets at 1 year. However, because of limited availability of 1-year follow-up functional outcomes in the SCIMS database, our analysis was restricted to discharge outcomes.
With regard to LEMS, those with non-CCS, who initially had lower scores than other CCS subsets, maintained relatively low scores even after 1 year. However, they also demonstrated the most significant improvement in LEMS compared with the other subgroups, which may have been limited by a ceiling effect. In terms of functional mobility outcomes, at the time of discharge, individuals classified as non-CCS were less likely to transfer or walk independently, but this difference was not statistically significant.
Given the notable variability within existing criteria for CCS and even among these subsets, it is understandable that there are diverse outcomes in terms of neurological and functional recovery. Historically, a prevailing belief suggested a more favorable prognosis for CCS, as noted by Schneider and coworkers and subsequent studies. 19,27,32,63,64 However, recent research, including our findings, challenge this perspective, revealing that CCS functional outcomes are largely comparable to other forms of incomplete tetraplegia, 14 despite differences noticed in neurological outcomes. Consistent with past research, we find that the primary determinant of neurological or functional outcomes remains the AIS grade, rather than the diagnosis of CCS. 14
The EM-SCI criteria, outlined in a three-article series, previously established three categories of traumatic CCS (TCCS) 14 : Non-TCCS for individuals with LEMS < UEMS, intermediate (Int)-TCCS for those with LEMS - UEMS difference of 1 to 9 points, and TCCS for cases in which LEMS - UEMS ≥10. The latter is denoted as the EM-SCI criteria in this article. The EM-SCI criteria were formulated through a review of the existing literature and a survey involving spine surgeons. 10,65 In contrast, our criteria were derived from observations made within the SCIMS database. Although the EM-SCI categories differ from our subsets of non-CCS, CCS intermediate variants and full CCS, similar trends were observed. Individuals with TCCS tended to be older, were more likely to have had AIS D grade on the initial examination, and exhibited comparable trends (to full CCS) in UEMS and LEMS scores on admission and 1-year follow-up. A comparison of functional outcomes between the studies was not performed, because of differences in the timing of outcome assessments (our study assessed discharge functional outcomes whereas the EM-SCI article used 1-year outcomes).
Following stratification by AIS grade, the EM-SCI study revealed minimal significant differences in chronic phase UEMS and LEMS outcomes between participants with TCCS and those with non-TCCS. However, no significant differences were observed in functional UE and LE outcomes at 6 or 12 months post-injury between the two groups. Despite the authors' recommendation more than a decade ago that future outcomes studies in motor incomplete tetraplegia should not select or stratify patients based on the TCCS diagnosis, 14 but rather continue to use AIS grades for prognostication, it is noteworthy that many studies continue to use the EM-SCI criteria in their inclusion criteria. 15,25,27,66 –68 It is of note that in their three-article series, a survey involving 157 spine specialists demonstrated that the majority (61%) viewed a difference of 10 points as an acceptable cutoff. However, 40% of participants also felt that applying a single criterion to the diagnosis of CCS was insufficient for research purposes. 10
According to a recent report from the SCIMS database, 4 incomplete tetraplegia is the most common type of SCI in the United States, comprising 47% of all SCI cases since 2015. In particular, the majority of injuries within this group involve motor incomplete tetraplegia, with incomplete syndromes accounting for a significant portion. 7 This was also evident in our study, with CCS accounting for 17.5–52% (full CCS to any CCS, respectively). Given that CCS constitutes more than half of total cases of motor incomplete tetraplegia when considering all three CCS categories together, it raises the question of whether CCS can truly be classified as a distinct syndrome. Moreover, in 66% of motor incomplete tetraplegia cases, the motor scores in the LEs are higher than those in the UEs (i.e., LEMS > UEMS), resembling the pattern observed in CCS.
Considering the substantial variability in CCS, along with its significant overlap with motor incomplete tetraplegia, we endorse previous recommendations against treating CCS as a distinct entity in research. 12 –14 Instead, we believe it should be considered within the broader category of motor incomplete tetraplegia. Although this perspective was previously explored in terms of functional outcomes (revealing no significant differences between CCS and other forms of incomplete tetraplegia) and timing of surgery, this article introduces an additional viewpoint by scrutinizing the definitions and clinical presentations. Nonetheless, there remains clinical value in characterizing an injury pattern as CCS, as it represents notable UE weakness compared with the LEs.
This study has several limitations that should be considered. First, it is important to note that there is no gold standard definition for CCS, which makes it challenging to establish a definitive benchmark for comparison. It is possible that alternative approaches exist, offering improved precision in delineating different variations of CCS. Second, the criteria for unilateral and borderline CCS are still broad; however, there is only a limited number of subcategories that can be feasibly defined. Moreover, the SCIMS database assesses the overall presence of associated injuries that may occur with a traumatic SCI, but data collection does not involve details on specific diagnoses such as a plexus injury. As a result, in scenarios such as the one depicted in Figure 3b, which displays a prominent unilateral UE lesion, the possibility of a brachial plexus injury cannot be dismissed.
Another limitation is the small sample size of cases with 1-year functional follow-up data in the SCIMS database, which prevented direct comparison with the EM-SCI study. Instead, the analysis was based on discharge data, which may not capture long-term outcomes. Further, it should be noted that many of the observed results, particularly in relation to functional outcomes, were not statistically significant. We did not extensively delve into the outcomes of the intermediate CCS subtype (combining unilateral and borderline CCS) as the results were typically somewhere in between those of full CCS and non-CCS, and often lacking statistical significance. Future research may consider addressing these limitations to enhance our understanding of CCS.
Conclusion
Three variations of CCS have been described to elucidate the highly variable clinical presentation of CCS. Although there are some differences between these variations and non-CCS motor incomplete tetraplegia, these subsets may not offer a clear distinction that allows a comprehensive analysis of outcomes from a research perspective.
Our study further strengthens the notion that outcomes of CCS are not substantially different from those for other forms of incomplete tetraplegia. The considerable overlap between CCS and motor incomplete tetraplegia suggests that CCS should not be considered as a separate entity for research, and that inclusion/exclusion criteria in future studies should instead focus on aspects such as the AIS and NLI in those with motor incomplete tetraplegia. Nonetheless, we advise researchers focusing specifically on the clinical presentation of CCS (significant UE weakness compared with the LEs) to be mindful of the inherent limitations in existing quantifiable criteria (such as EM-SCI) or the specific variants (e.g., full CCS) emphasized in this study.
Transparency, Rigor, and Reproducibility Summary
In this retrospective study, 6997 individuals were screened and 1490 were retained for the analysis. Assumption of normality was not needed, because of the large sample size. Correction for multiple comparisons was performed using Bonferroni. Individuals with missing data were excluded from the study. Statistical analysis was performed by the corresponding author who has expertise in rehabilitation medicine and quantitative data analysis. The data are archived in https://www.nscisc.uab.edu/ and are available upon request for the current year. Requests must be submitted to the NSCISC in writing, using this protocol https://www.nscisc.uab.edu/Public_Pages/Database_files/Using_National_SCIMS_Database.pdf. Analytic codes used to conduct the analyses presented in this study are not available in a public repository. They may be available by e-mailing the corresponding author.
Footnotes
Authors' Contributions
E.E.H.: conceptualization, writing–original draft, writing–review and editing, formal analysis; B.S.: writing–original draft, reviewing and editing; A.B. reviewing and editing, formal analysis; F.E.: writing–original draft, reviewing and editing; S.K. conceptualization, writing–original draft, writing–review and editing, supervision.
Funding Information
The contents of this publication were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90SIMS0012). This work was supported by the Devivo Mentored Research Award. The National Spinal Cord Injury Statistical Center funds this award through a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90SIMS0016).
Author Disclosure Statement
No competing financial interests exist.