
Abstract
Effective team science requires procedural harmonization for rigor and reproducibility. Multicenter studies across experimental modalities (domains) can help accelerate translation. The Translational Outcomes Project in NeuroTrauma (TOP-NT) is a pre-clinical traumatic brain injury (TBI) consortium charged with establishing and validating noninvasive TBI assessment tools through team science. Here, we present practical approaches for harmonization of TBI research across five centers providing needed vocabulary and structure to achieve centralized data organization and use. This includes data sharing as an essential step that enables validating data between domains, evaluating reproducibility between sites, and performing multimodal analyses. As part of this process, TOP-NT (1) produced a library of TBI-relevant standard operating procedures to coordinate workflow, (2) aligned 481 pre-clinical and clinical common data elements (CDEs), and (3) generated 272 new pre-clinical TBI CDEs. This consortium then (4) connected diverse data types to validate assessments across domains and to allow multivariable TBI phenotyping. Lastly, TOP-NT (5) specified technical quality controls for pre-clinical studies. These harmonization tools can facilitate reproducibility in team science, help distinguish a wide injury spectrum from technical variability, apply quality-controls, and ease higher level data analyses. TOP-NT uses three rat TBI models across four sites. Each site collects primary outcome measures, including magnetic resonance imaging (MRI) protocols and blood biomarkers of neuronal and glial injury, validated by histopathology and behavioral outcomes. Collected data are organized using the 481 TOP-NT pre-clinical CDEs, covering surgical, behavioral, biomarker, MRI, and quantitative histopathological methods. We report data curation steps suited for data storage using the Open Data Commons for TBI as a centralized data repository, allowing unbiased cross-site analysis. This approach leads to introducing a higher level, syndromic understanding of TBI signatures. TOP-NT authors outline a semantic and structural framework suggesting strategies for robust pre-clinical research in multicenter trials to improve translatability for TBI assessments.
Introduction
Traumatic brain injury (TBI) is a major cause of death and disability, with over 69,000 TBI-related deaths and 230,000 hospitalized TBI patients in the United States in 2021. 1 TBIs are complex and heterogeneous, with a spectrum of evolving neuropathologies, and require well-defined assessment tools for diagnosis and monitoring. Pre-clinical trauma models aim to improve care for TBI by facilitating clinical translation of new therapies. 2 A National Institute of Neurological Disorders and Stroke (NINDS) focus for translational animal TBI research is to improve both the noninvasive assessment in animal models and the understanding of their pathophysiological underpinnings (https://www.ninds.nih.gov/current-research/focus-disorders/focus-traumatic-brain-injury-research). The NINDS has therefore decided to mandate initiatives addressing this need by announcing in 2017 funding for a multicenter program called Translational Outcomes Project in NeuroTrauma (TOP-NT, see RFA-NS-17-023, companion paper by Radabaugh et al, and Supplementary Table S1 for TOP-NT terminology terms). 4
Translation is hampered by common generalization barriers that hinder pre-clinical-to-clinical relevancy including animal-to-human species mismatch in TBI mechanisms and disease progression and incongruent assessment approaches between pre-clinical and clinical research studies and practices, referred to jointly as problems of construct validity. 5 –8 Species differences in anatomy, metabolism, behavior, and chronicity in animal TBI models limit translatability, along with practical constraints. 9 –13 Yet, assessment tools can, in principal, be aligned between the realms by domain, that is, alignment by data types within modalities such as magnetic resonance imaging (MRI) and biomarkers. Funding agencies are impelling pre-clinical neurotrauma researchers to systematically implement noninvasive assessment tools and to improve reproducibility in common TBI models. Other consortia in neurotrauma include Operation Brain Trauma Therapy, which focused on treatments, and the recent Preclinical Interagency Research Resource-TBI (PRECISE-TBI), which focuses on further standardizing common data elements (CDEs) without conducting new experimental work (see companion paper by Radabaugh et al., J. Neurotrauma). TOP-NT directly addresses this mandate by experimental testing and by harmonizing noninvasive assessments in three rat TBI models. TOP-NT also developed and presents here a practical toolkit for data collection and curation, intended for centralized storage and public access in the Open Data Commons for TBI (ODC-TBI) repository (https://odc-tbi.org/). 3 The presented steps are necessary to enable centralized computation and multimodal analytics, which can improve phenotyping of TBI pathologies.
The value of multicenter studies that facilitate team science is increasingly recognized. 4,14 –20 Teams have an intrinsic need to develop strategies for adherence to transparent and well-defined, unbiased measures, similar to clinical studies, as has been shown, for example, by The Canadian Critical Care Translational Biology Group. 18 This approach may lead to lower effect sizes compared to reports from single laboratories, and provide a more realistic estimate of diagnostic tests and potential treatments. 18 Similar to other pre-clinical initiatives, pre-clinical TBI research can benefit from prospective harmonization by formalizing protocols and organizational steps that include an architecture for data sharing between centers and across domains. 15 Multisite studies can then boost statistical power by pooling sample sizes from the same TBI models and outcomes across centers. This allows research teams to achieve the power for controlling a number of covariate effects simultaneously, including sex, time, age, region of interest (ROI), and center, which is necessary to improve pre-clinical neurotrauma studies. 8,21,22
When pre-clinical research teams jointly embrace prospective harmonization, share standard operating procedures (SOPs), and use a common vocabulary, a procedural infrastructure exists as a foundation for accelerating clinical translation. Toward this goal, TOP-NT presents the following SOP compendium and a catalog of 481 CDEs, along with practical, structural data curation steps. These are essential tools for research to enhance reproducibility and narrow translational gaps. 15 –17 These structured methods can help researchers achieve external validity as they facilitate multisite sample pooling, data aggregation, and centralized analyses. 18 –20 In addition, this path supports TBI phenotyping toward new TBI signatures (see below).
Noninvasive Tracking of Pathophysiological Signatures in TBI
As recognized by clinicians and funding agencies, the complexity and heterogeneity of TBI requires an improved classification beyond the Glasgow Coma Scale score categories of mild, moderate, and severe TBI. 23 Discussed is a new classification system designed to incorporate the use of MRI and biofluid biomarkers, along with broader diagnostic criteria. 24,25 While familiar in use, underlying causes for changing biomarker profiles and MRI patterns need to be further investigated. Here is an opportunity, especially for pre-clinical TBI research, to align noninvasive assessments with pathophysiology. A TBI signature can be defined as a pattern or profile that reflects an underlying TBI pathophysiology (see Supplementary Data S1, Glossary for relation with similar terminology). Thus, it is a translational goal to identify noninvasive TBI signatures that associate with pathological states of the injured brain, where MRI and biomarkers are internally validated by correlations with histopathology or behavioral outcomes, and assays and sequences are standardized and replicated for external validation across laboratories. 14 Validated biomarkers that detect specific TBI pathologies with sensitivity and specificity can enable researchers to make informed inferences for diagnostic use or for monitoring of TBI trajectories; supporting clinical use.
Pre-clinical TBI studies commonly generate diverse raw data types that differ in structure and format, making it challenging to arrive at meaningful multimodal signatures. For example, different time points are used for repeated blood draws, imaging, and behavioral tests. Likewise, different brain ROIs are captured in macroscopic versus microscopic imaging. Hence, this article outlines practical steps that include grouping of features and data alignment to achieve standardized data organization for multimodal cross-site analytics. The presented semantic and structural framework can serve as a resource for pre-clinical research when engaging in multicenter studies using assessments from multiple domains. Toward this goal, the following important methodological deliverables are offered: a 481 CDE data dictionary, linked pre-clinical and clinical CDE bundles, and a practical guide on how to assemble data types for MRI, biofluid biomarkers, quantitative histopathology, and behavior outcomes. Thus, the presented framework provides tools to facilitate new findings for TBI phenotyping in addition to benefits from reproducibility (see above).
TOP-NT consists of four sites (teams) conducting experiments at the University of California Los Angeles (UCLA), the University of Florida and Morehouse School of Medicine (UF/MSM), Georgetown University and Uniformed Services University (GU/USU), and John Hopkins University (JHU). An additional center based at the University of California San Francisco (UCSF) is responsible for independent centralized data management and analysis. Noninvasive assessments include MRI modalities and blood-based biomarkers that are used in clinical research, but are not yet common in clinical practice. Some biomarkers are being tested in model systems as developmental markers for novel diagnostics. Biomarker validation will use unbiased quantitative histopathology and behavioral testing. The common biomarkers that are collected across sites include diffusion-weighted imaging (DWI) with fractional anisotropy and mean diffusivity, and the blood biomarkers glial fibrillary acidic protein (GFAP), neurofilament light chain (NFL), and total tau/phospho-tau protein (T-tau/P-tau). 26 –31 Newer markers include amide proton transfer (APT)-weighted imaging, a local regional heterogeneity measure of functional connectivity (HCorr) derived from resting-state functional MRI (fMRI), and the brain-enriched astrocyte biomarker aldolase-C (ALDOC). 32 –36 The controlled cortical impact (CCI) injury model is used by all centers. In addition, the lateral fluid percussion injury (FPI) and closed head impact model of engineered rotational acceleration (CHIMERA) injury models are each used at two of the four sites. The design is balanced with equal numbers of male and female rats at all sites.
Paper Overview/Navigation
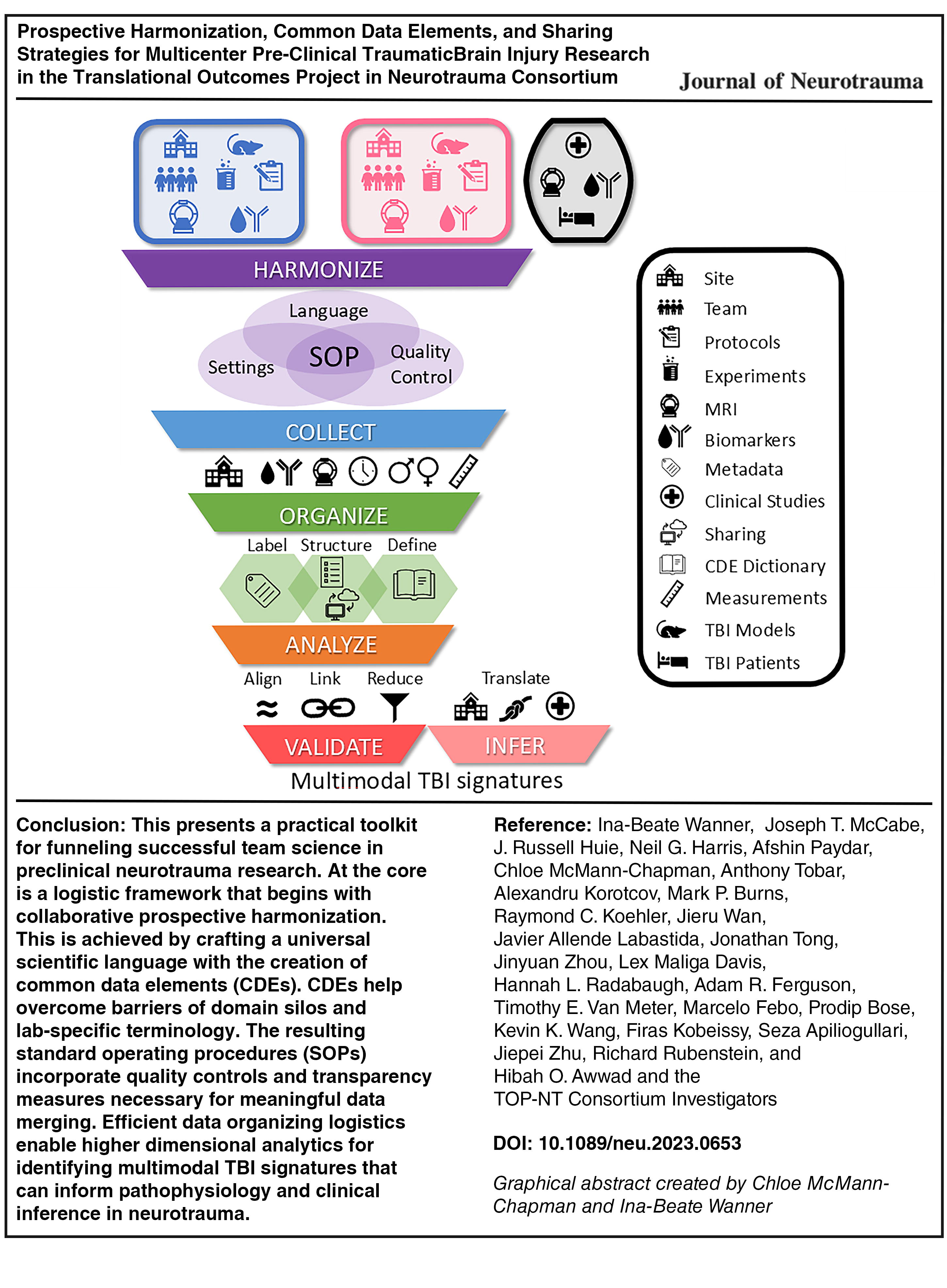
Figure 1 provides a step-by-step overview for different laboratories to harmonize experiments by sharing language, settings, and quality controls to arrive at jointly used SOPs. It then outlines data organizing using CDEs and curation to funnel into centralized analyses ultimately producing multimodal TBI signatures to inform clinical assessments via inference. Figure 2 outlines data types and the key information reported from each site, allowing groups to study sources of data variation within and between centers. Figure 3 identifies TOP-NT CDEs that are shared by all domains, comprised of joint metadata and identifiers. These canonical CDEs allow for data linking between domains toward multimodal modeling as is outlined in Figure 4. Table 1 informs on CDE provenance listing newly written and adopted elements with respective sources. Figures 5 –9 provide an overview of 481 TOP-NT CDEs grouped by domain and listed in organized fashion, guiding users toward relevant CDE structures, groups, and subgroups/bundles. The taxonomy in Figure 10 aligns pre-clinical and clinical CDE structures to facilitate translational inference among assessments.

Steps for prospective harmonization and multimodal multisite data management. The TOP-NT teams at UCLA, UF/MSM, GU/USU, JHU are the four experimental centers that conducted separate TBI models with site-specific protocols generating MRI patterns and biomarker profiles (top symbolized by two separate boxes, UG-3 phase). Provided common SOPs share language, instrument settings, and quality controls for harmonized cross-site studies (Supplementary Data S1, Study Design and Methods). Standardized key experimental definitions and simplified terminology are documented in the TOP-NT common data elements (TOP-NT-CDEs). TOP-NT CDEs are assembled in the consensus CDE data dictionary that uses consistent labels and an interoperable data format (Supplementary Table S2, CDE Data Dictionary). Biomarkers, stains, and scan modalities are recorded along with critical metadata (Figs. 5–9). Datasets are being curated and deposited in the Open Data Commons for TBI; they are code-accessible and will be made public (ODC-TBI, https://odc-tbi.org). Thus, semantic and structural alignment enables multivariable associations for emerging pathophysiological multimodal TBI signatures. These jointly can support inferential equivalence, to reveal parallels between animal and clinical TBI assessments. GU/USU, Georgetown University and Uniformed Services University; JHU, John Hopkins University; SOPs, standard operating procedures; TBI, traumatic brain injury; TOP-NT, Translational Outcomes Project in NeuroTrauma; CDE, common data element; UCLA, University of California Los Angeles; UF/MSM, University of Florida and Morehouse School of Medicine; MRI, magnetic resonance imaging.
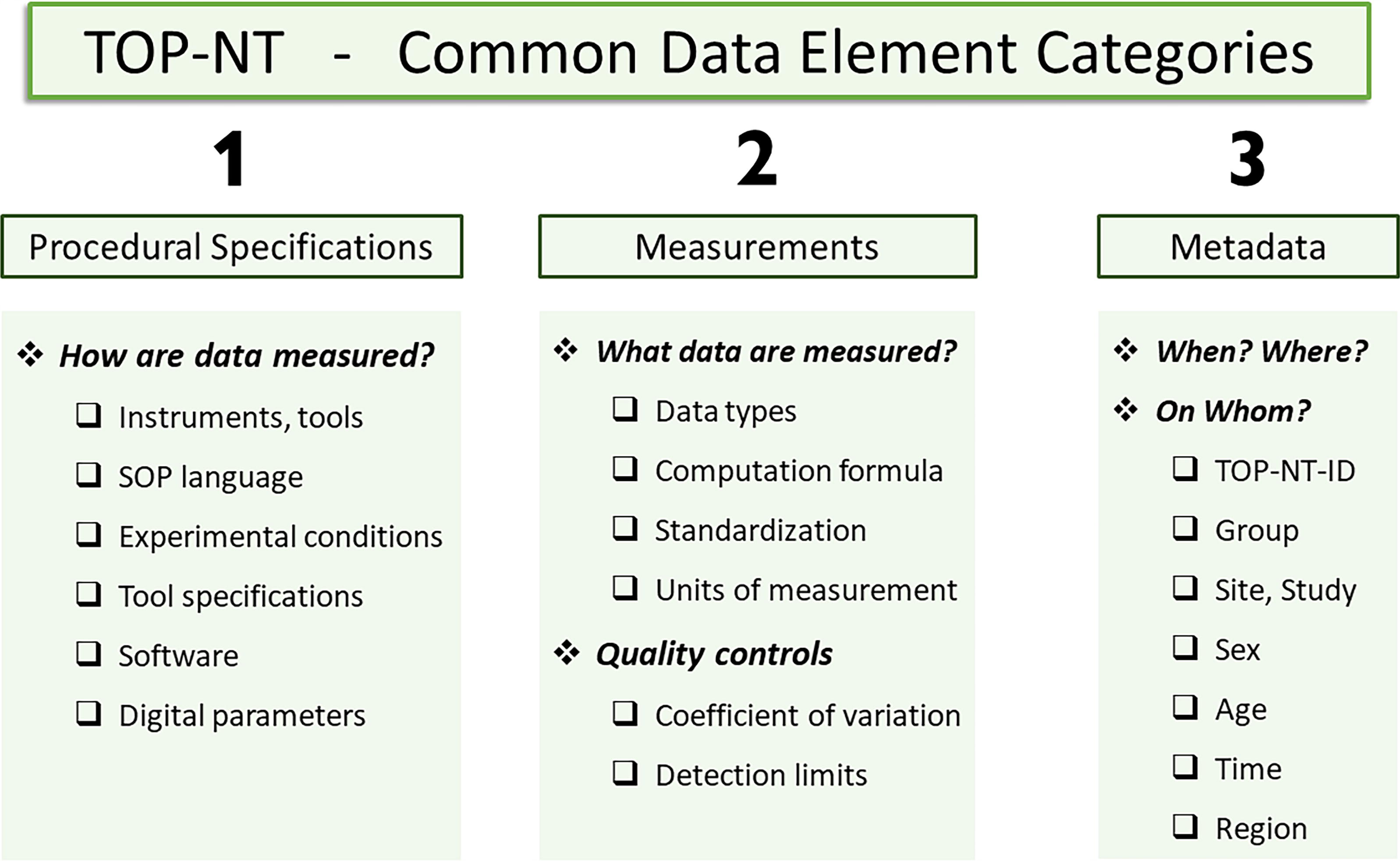
CDE categories in the data dictionary. Three different data element categories are in the TOP-NT CDE data dictionary (Supplementary Table S2): (1) Procedural Specifications include experiment and instrument settings with digital parameters from harmonized SOPs (Supplementary Data S2). (2) Measurement definitions are succinct, specific descriptions of what is measured with data types, formulas, and units. Quality controls include coefficient of variation (CV) and detection limits. (3) Metadata inform when and where and on whom experiments are done. These are critical reference data identifying the subject, attributes, measurement conditions, and covariates. CDEs, common data elements; SOPs, standard operating procedures; TOP-NT, Translational Outcomes Project in NeuroTrauma.

Canonical CDEs are essentially Metadata: These are critical covariates and controls for translation and cross-domain linkage. Canonical TOP-NT CDEs are identified as essential data elements that are shared between domains, pre-clinical and clinical CDEs. They include identifiers: TOP-NT-ID, center (or study), covariates: sex, age, injury elapsed time, ROI (for MRI and histopathology), and modality-appropriate quality controls: tissue preservation, CV, assay controls, calibrations and other imaging and assay quality and acquisition controls. These canonical CDEs are shared between domains and centers, and are used in pre-clinical and clinical fields. Hence, canonical CDEs link data across domains and realms. CDEs, common data elements; MRI, magnetic resonance imaging; ROI, region of interests; TOP-NT, Translational Outcomes Project in NeuroTrauma.

Data management framework for cross-domain association. Robust cross-site data alignment for analytics requires data structure and formatting that facilitates digital linkage of heterogeneous, domain-specific datasets. Domains are from left to right: biomarkers, behavior, MRI, and histopathology. Each domain contains a different data structure due to unique repeated measures over time periods (blue arrows; “concur” and “predict”-type links, blue) and in different brain regions (right side, “align”-type link, brown). Defining and streamlining each domain’s metadata harnesses dissimilarity and helps to identify essential links for connecting domains. Mapping links deliver concurrent or predictive relations over time and brain co-registration in space between volumes from histology sections and MRI masks. MRI, magnetic resonance imaging.

Pre-clinical General Animal and Injury CDEs alignment. The 114 General TOP-NT CDEs are indexed under three first generation pre-clinical structures (left). 38 Aligned are 72 adopted (left) and 42 newly introduced (right) pre-clinical “General Animal” and “General Injury” CDEs. Among these are included five FITBIR canonical CDEs (left, yellow). CDEs, common data elements; TOP-NT, Translational Outcomes Project in NeuroTrauma. FITBIR, Federal Interagency Traumatic Brain Injury Research.
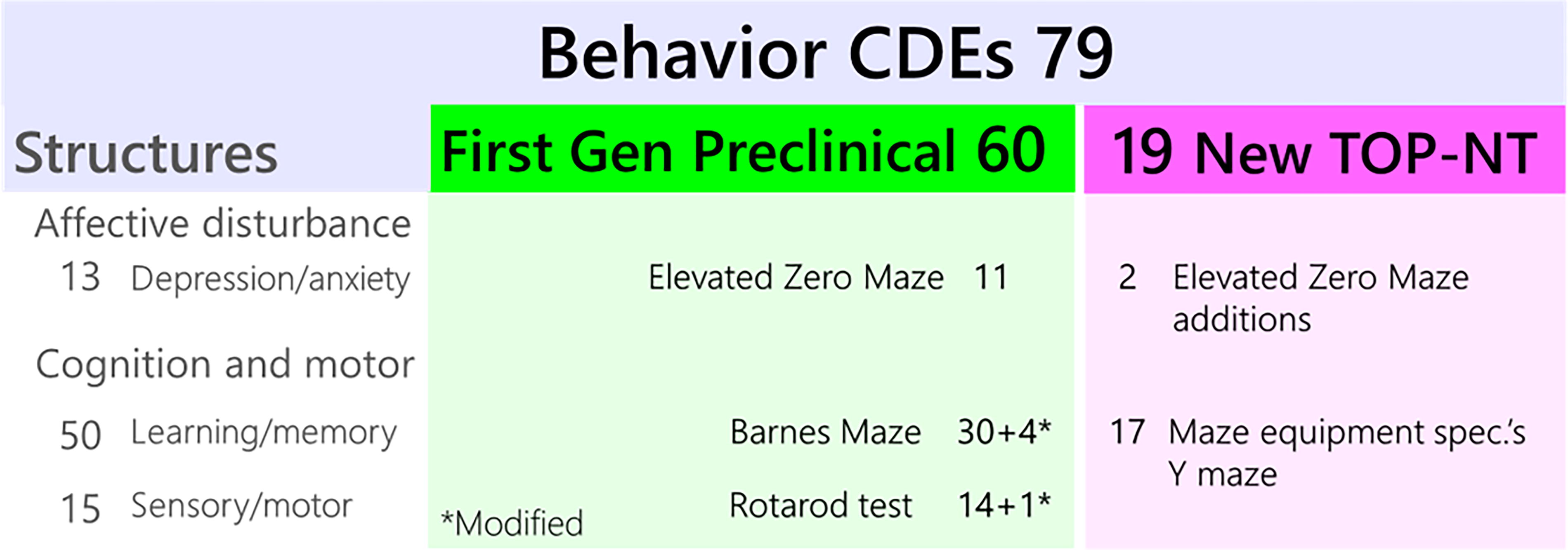
TOP-NT Behavior CDE align with first generation pre-clinical TBI behavior CDEs. The 78 Behavioral CDEs are indexed under groups and structures created by La Placa and colleagues separating “Affective disturbance” and “Cognition and motor” related behaviors (left). 38 Additional 18 new TOP-NT CDEs (right) address Elevated Zero and Y mazes and are aligned accordingly. CDE, common data elements; TBI, traumatic brain injury; TOP-NT, Translational Outcomes Project in NeuroTrauma.
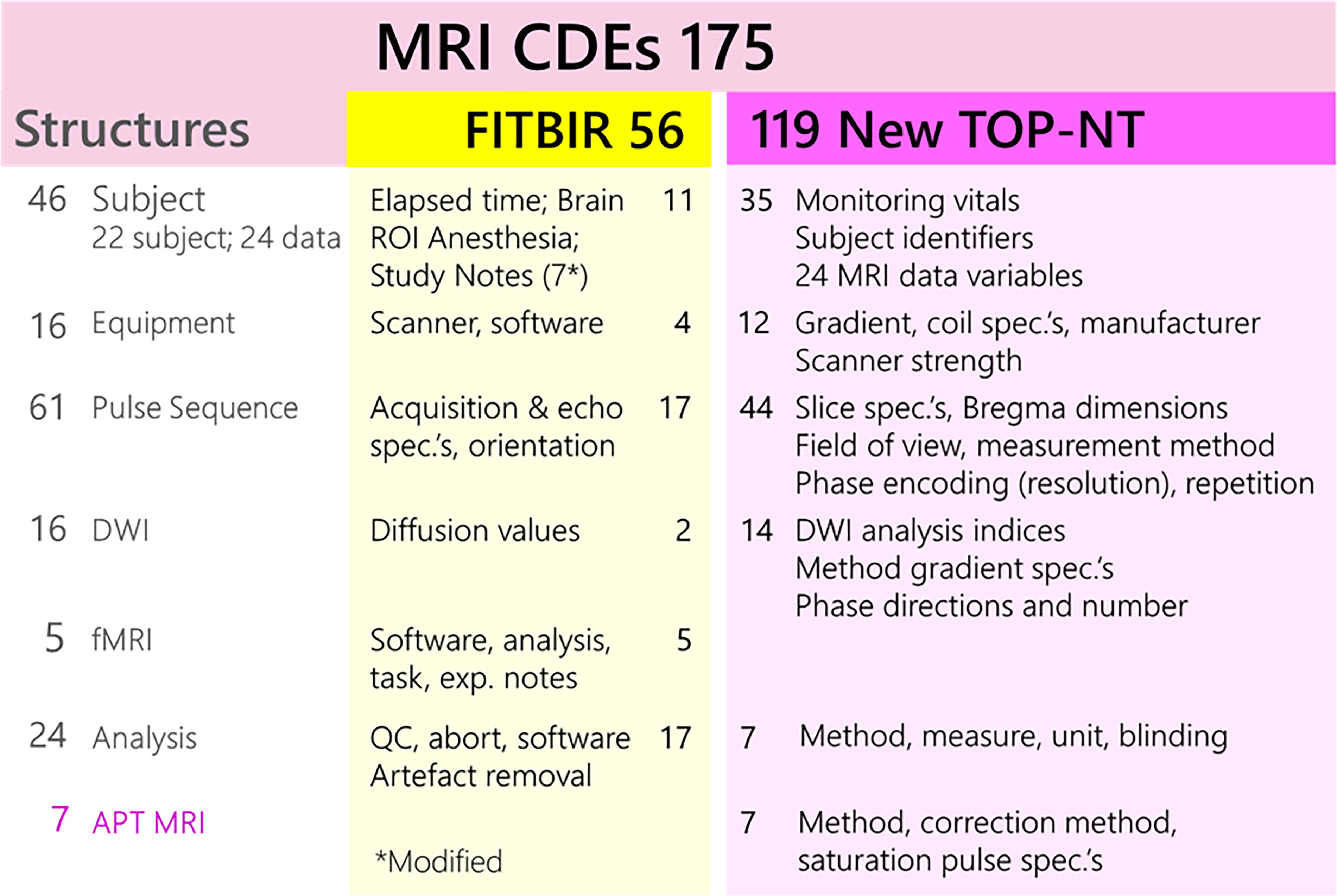
Pre-clinical MRI CDEs align with FITBIR clinical MRI CDEs. The 175 MRI CDEs are grouped under structures in alignment with FITBIR clinical CDEs (left) and include “subject, equipment, pulse sequence, diffusion weighted imaging (DWI), functional MRI (fMRI),” and “analysis” as well as a new group for amide proton transfer (APT) MRI. Some CDEs are modified for animal use (e.g., on anesthesia and brain ROIs). These groups are expanded by 119 new CDEs providing substantial new information on instrument specifics, data processing, quality controls and blinding as well as specific definitions on measurement variables. CDEs, common data elements; MRI, magnetic resonance imaging; ROIs, region of interests.
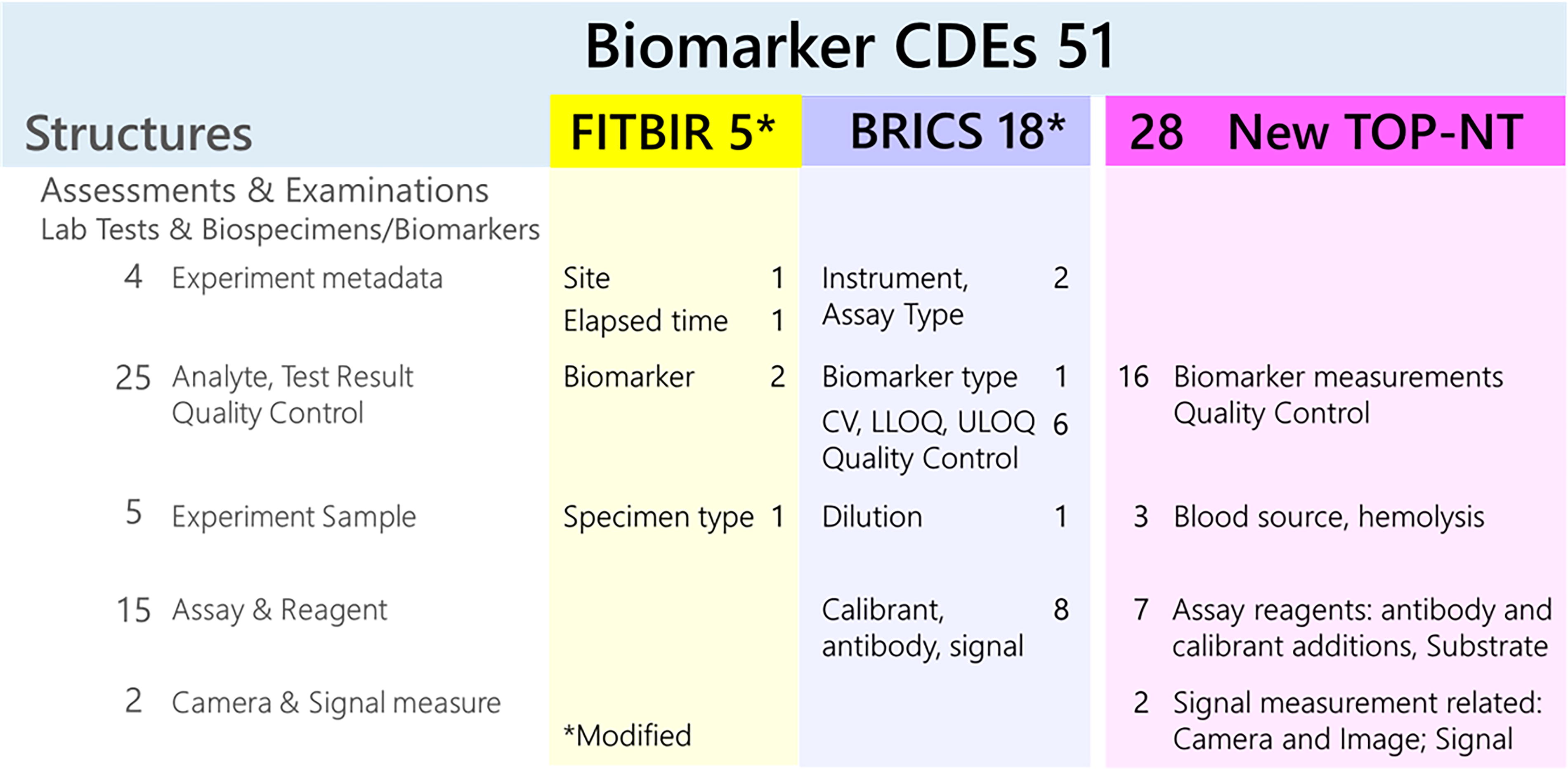
Pre-clinical Biomarker CDEs align with FITBIR/Biomedical Research Informatic Computing System (BRICS) clinical assay CDEs. The 48 Biomarker CDEs were organized and aligned with clinical FITBIR BRICS structure group “Assessments and Examinations” with subgroup on “Laboratory Tests and Biospecimens/Biomarkers” (left) with 18 modified CDEs. Newly added 25 biomarker CDEs are fitted to same groups (right). Biomarker CDEs include definitions on assay specifications, assay reagents, specimen and sample handling, quality controls including coefficient of variation (CV) as well as lower and upper limipt of quantification (LLOQ, ULOQ), metadata and specific measurement variables. Camera and image acquisition elements are shared between biomarker and histopathology domains. CDEs, common data elements.
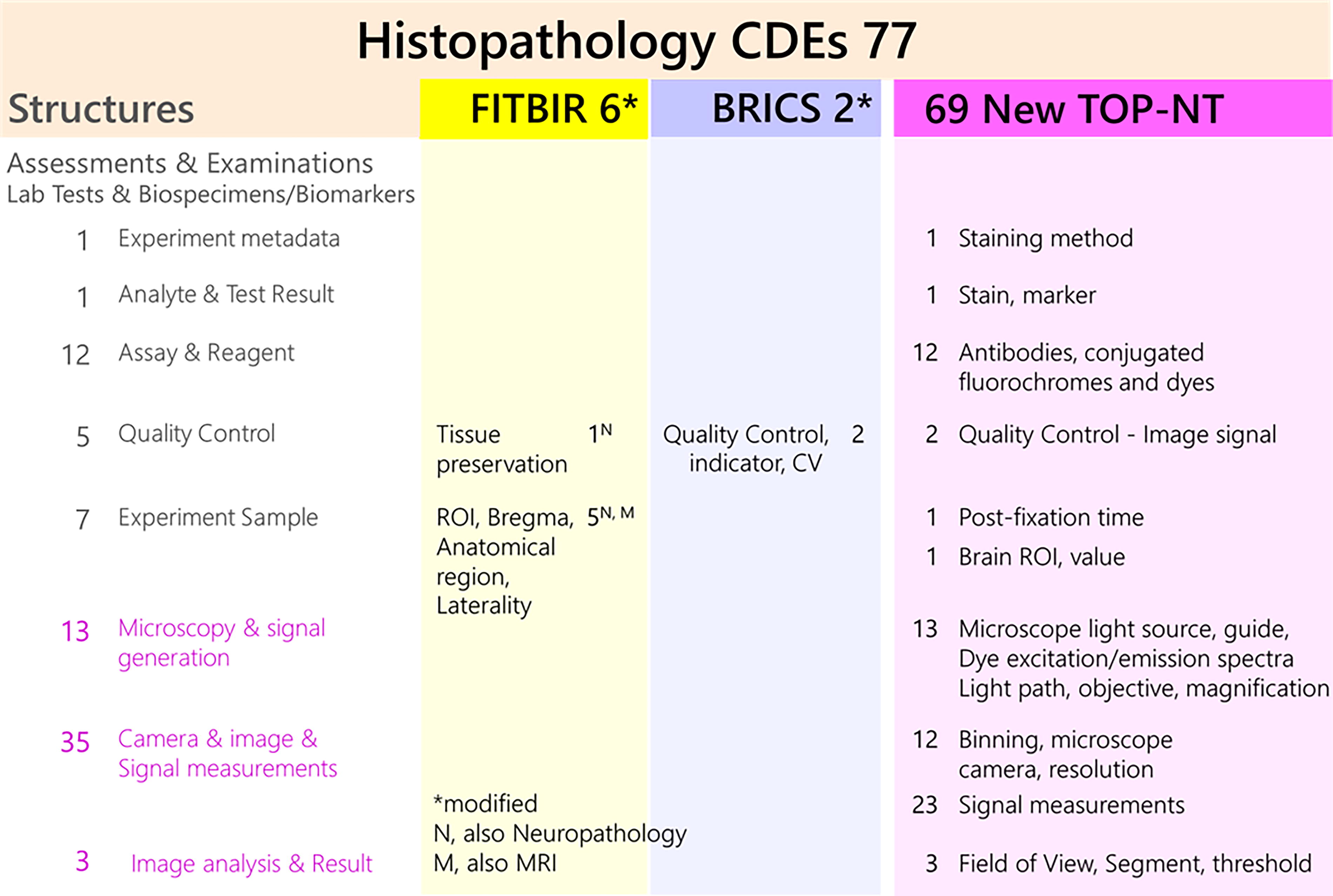
Quantitative Histopathology CDEs align with clinical BRICS and FITBIR Neuropathology structures. The 77 Histopathology experimental CDEs are aligned with FITBIR BRICS structures “Assessments and Examinations, Laboratory Tests and Biospecimens/Biomarkers” (left) covering antibodies and protein markers. Four TOP-NT-CDEs are similar to the drafted “Neuropathology of TBI” elements covering tissue preservation and brain ROIs, also used by MRI. New structures address “Microscopy and signal generation” to describe light and pixel pathway specifics. “Camera and image and signal measurements” describe microscopic imaging settings and all CDEs for quantitative analyses (see Supplementary Data S1, Study Design and Methods). BRICS, Biomedical Research Informatic Computing System; CDEs, common data elements; ROI, region of interest, CV, coefficient of variation, MRI, magnetic resonance imaging; TBI, traumatic brain injury; TOP-NT, Translational Outcomes Project in NeuroTrauma.
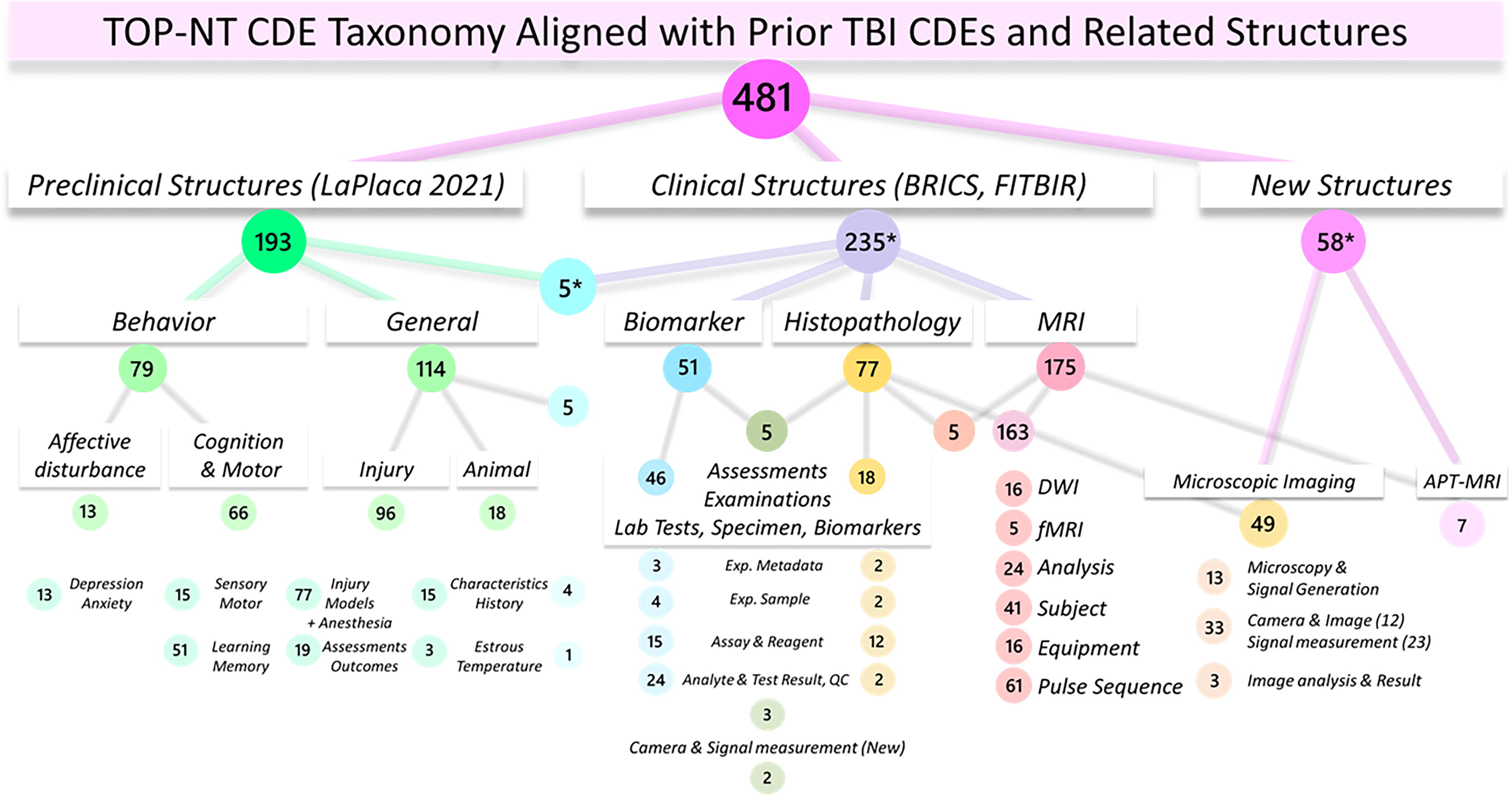
TOP-NT CDE taxonomy aligned with prior CDE structures. This dendrogram documents TOP-NT CDE alignment with selected pre-clinical and clinical TBI CDEs and TBI-related groups, subgroups and structures. 38,39,46 –48 Many new and modified TOP-NT CDEs are subsumed under previously existing groups, subgroups, and structures (previously called form structures). The content of these groups, subgroups and structures is summarized by domain in Figures 5–9. Harmonization with existing CDE organization facilitates communication for easier use by other pre-clinical teams as well as for establishing translational inference (see also Table 1 Provenance). New structures are created for APT-weighted MRI and microscopy-specifics addressing the quantitative histopathology workflow. APT, amide proton transfer; CDE, common data elements; MRI, magnetic resonance imaging; TBI, traumatic brain injury; TOP-NT, Translational Outcomes Project in NeuroTrauma.
Provenance and New TOP-NT Pre-Clinical CDEs by Domain
288*: Within 293 assessment 5 FITBIR CDEs overlap with pre-clinical CDEs in “general” (see Figs. 3 and 5).
211*: Among new assessments 5 CDEs overlap between 28* new biomarker CDEs and 69* new histopathology CDEs.
77*: 10 CDEs overlap: 5 are in histopathology and MRI; 5 are in histopathology and biomarker.
8*: 2 BRICS, 1 neuropathology, 3 neuropathology + FITBIR, 2 FITBIR.
Alignment and derivation: TOP-NT sources with preexisting CDEs for harmonization and for establishing translational inference.
CDEs, common data elements; BRICS, Biomedical Research Informatic Computing System; MRI, magnetic resonance imaging; TOP-NT, Translational Outcomes Project in NeuroTrauma.
Groundwork for Establishing a Multicenter Study Architecture
During an initial UG3 phase, each center’s candidate imaging and blood-based biomarkers were assessed and selected (or rejected) to move forward to the UH3 phase based on their discriminative ability for TBI versus sham. Candidates needed to have an effect size of ≥1 and a unanimous vote from all centers. It was also agreed to develop and implement an observer-independent, unbiased quantitative “field of view” (FOV) histopathology approach for validating MRI and blood biomarker changes (Supplementary Data S1). Teams then determined postinjury time points for blood draws, behavioral testing, and MRI acquisition measures considering clinical relevance and rodent-specific injury time courses. 9,37 Sample size, rigor, and bias are addressed during the UH3-phase by using the same animal models and the same assessment tools across centers. This prospective harmonization and external validation require independent teams to standardize experimental and acquisition conditions and provide transparency on the outcomes. For reproducibility, the research teams needed to communicate clearly and cooperate at all levels throughout the course of the UH3 phase. To arrive at a shared data dictionary, unique protocols at each site are adapted, which is accomplished during regular group discussions. At first, each center defined its unique data elements (UDEs) for key experimental conditions, instrumentation, data acquisition, and postprocessing settings of their respective UG3 phase projects (see companion paper Radabaugh et al.). Where possible, the teams incorporated pre-clinical first-generation TBI CDEs and harmonized site-specific UDEs arriving at a unified set of elements: the TOP-NT CDEs (Supplementary Table S2, CDE data dictionary, Fig. 1). Subsequent protocol sharing and experimental optimizations produced TOP-NT SOPs that were then used to conduct the UH3 studies (Fig. 1, Supplementary Data S1, Study Design and Methods). The TOP-NT study design and SOPs have been facilitating replication across sites (Fig. 1). The TOP-NT CDEs are here assembled into a CDE data dictionary (Supplementary Table S2 CDE Data Dictionary). These CDEs are all actively in use by the consortium centers for data reporting into the ODC-TBI centralized data repository. 38,39
SOPs and CDEs Facilitate Multisite Experiment Alignment for Prospective Harmonization
This report provides an expanded pre-clinical TBI CDE dictionary and taxonomy for rat TBI models, instrument settings, experimental methods, outcome measurements, and metadata including covariates and quality controls (Supplementary Table S2, CDE data dictionary). Prospective harmonization involves (1) standardized experimental conduct, (2) defined terminology, and (3) a common data structure. (1) Standardized experimental conduct is achieved by thoroughly written instructions in understandable language and details allowing for accurate reproduction of experiments and injury models. (2) Defined terminology uses jointly agreed-upon language that clearly defines all aspects of data acquisition and content, arriving at critical terms to capture experimental objectives, analyses, and data types. This effort led to the assembly of CDEs for procedures, data, and metadata. 40 Pre-clinical neurotrauma CDEs are established for animal studies in spinal cord injury and TBI. 38,39,41 These first-generation CDEs cover pre-clinical injury models, animal characteristics and study design, and selected animal assessment and behavioral outcome measures. At present, however, the neurotrauma community does not have standardized language for quantitative histopathology and immunohistochemistry, blood-based biomarkers, and MRI in animal TBI studies. These areas are now covered in the TOP-NT CDEs (Supplementary Data S2 Table CDE Data Dictionary). (3) A common data structure enables data pooling across sites (Fig. 3). The common use of canonical, shared metadata facilitates linking multimodal datasets with their innate domain-specific data structure that then allows digitally joining measurements in an organized fashion, for centralized informatics across domains and sites (Fig. 4). 15,40
The SOPs provide the foundation for establishing CDEs agreed upon by all centers within domain-specific working groups. TOP-NT CDE categories are procedural TOP-NT CDEs to assure consistent application of assays, surgery, anesthesia conditions, TBI models, and behavioral testing to obtain compatible datasets across centers (Fig. 2). Acquisition specifications on how data were measured include instrument settings, digital parameters, and software specifics (Fig. 2). Definitions for outcome measurements and quality controls were assembled providing succinct parameters on the data type, formulas, range, and units of acquired data. Data types included marker concentration, amount, intensity, image area, volume, z-score, number, density, and medians of MRI-derived values. Standardized definitions for metadata, for example, injury-elapsed time and animal features, were included in the data dictionary as key experimental covariates (Fig. 2). As TOP-NT CDEs from all domains were combined, several elements were identified as essential canonical CDEs defined as being used across domains (Supplementary Data S1 Glossary, Fig. 3). Metadata includes animal ID, injury-elapsed time, age, sex, estrous cycle phase, and quality controls of coefficient of variations, (CVs), CV, and detection limits 9,42 –45,73 as well as brain regions used in MRI and histopathology. As such, canonical CDEs enable linking heterogeneously collected data from various domains to facilitate multimodal and multicenter data correlation (Fig. 4). Where possible, existing structures were adopted, modified, or amended from first-generation CDEs, as illustrated in the General and Behavior groups (Figs. 5 and 6), and new structures were made for APT-MRI, and microscopy and imaging (Figs. 7, 9 and Supplementary Figure S3). 38 Overall, harmonizing logistic, analytics, and semantics for all experiments and measurements resulted in jointly reaching a common CDE dictionary of 481 TOP-NT CDEs. These TOP-NT CDEs are used by the consortium sites during the UH3 phase experiments.
Provenance and Domain Organization of Pre-Clinical TBI CDEs
TOP-NT CDEs were indexed under existing overall domains and subgroups and structures, and their relationships to existing CDEs gives their provenance (Table 1). Domains are General (114 CDEs) with subgroups for Animal (18) and Injury (96), including anesthesia treatments; Behavior (79), MRI (175), Biomarker (51), and Histopathology (77). In all, 272 new CDEs were defined and assimilated with 209 preexisting CDEs (Table 1). 38 This included 132 pre-clinical and 77 clinical CDEs, a total of which 172 CDEs were adopted without change (123 pre-clinical, 49 clinical CDEs), and 37 CDEs were modified to suit TOP-NT animal studies (Table 1). Of 132 first-generation pre-clinical elements, 123 were adopted and applied without modification. Among all 193 pre-clinical CDEs, the “General” domain has been expanded by 42 new TOP-NT CDEs on estrous cycle, temperature and anesthesia control, apnea, righting reflex, and rat CHIMERA injury model with instrument settings (Fig. 5). First-generation “Behavior” CDEs were amended by 18 new TOP-NT CDEs addressing elevated zero and Y mazes (Fig. 6).
The TOP-NT MRI team assembled 175 pre-clinical “MRI” CDEs. Among these, 56 clinical Federal Interagency Traumatic Brain Injury Research (FITBIR) MRI CDEs were used, and among these 49 were adopted “as is,” while 6 were modified for anesthetized rat brain MRI (Fig. 7, Table 1). An additional 119 TOP-NT MRI CDEs were added for DWI, fMRI, and APT modalities to standardize analyses of quantitative, volumetric whole-brain MRI, slice MRI, and ROI-based measurements (ROI, Supplementary Fig. S2). Definitions include instrument specifications (e.g., gradient strength and slew rate, radiofrequency coil configuration, and scanner field strength), pulse sequences and image acquisition specifics, phase encoding direction, FOV, data matrix size and resolution, echo time, repetition time, image correction protocol, and quality control methods. These definitions are critical since instrument specifications (magnet strength, etc.), application of specific pulse sequences, and post-processing of MRI scans not only bring into line data acquired from various centers but also ensure comparable quality control and interpretation. Finally, CDEs on monitoring the animal’s recovery status and for analysts’ blinding were added to MRI CDEs (Fig. 7).
For measuring biomarkers in rats, TOP-NT investigators established 51 new “Biomarker” CDEs by adopting 23, of which 18 were modified, and formulated 28 new CDEs (Fig. 8, Table 1). 46 “Experiment metadata” include site, time, assay type, instrument/platform, and sample dilution following prior form structures. “Analyte, Test Results, and Quality Controls” includes biomarker measurement definitions as well as analytical accuracy elements that include CV and detection limits. 73 “Experiment Sample” includes specimen types such as serum, plasma, cerebrospinal fluid (CSF), and regional brain cell lysates. “Assay and reagent” is comprised of antibodies, conjugates, substrates, and calibrants.
TOP-NT defined 77 new “Histopathology” pre-clinical CDEs, including tissue preservation and ROI-related information, with only four being matched directly with similar clinical “Neuropathology of chronic TBI” drafted UDEs (Fig. 9). Two histopathology quality control elements were added that are analogous to similar FITBIR Biomedical Research Informatic Computing System (BRICS) elements and reflect SOP content. New quantitative histopathology TOP-NT CDEs structures capture three subgroups. “Microscopy and signal generation” (13) includes fluorochromes and microscope attributes for essential filters and beam splitters, objectives/magnification, light source, and cable. “Camera and image” and “Signal measurement” (35) include camera, image pixel dimensions/resolution. Analysis variables for quantitative histopathology along with “Image Analysis and Result” (3) are jointly used to relate quantitative histopathology with biomarkers and MRI. Histopathology measurements are described further under Study Conduct and in the histopathology SOPs and Supplementary Data S1.
Taxonomy to Harmonize TBI CDEs with First Generation and Clinical CDE Structures
Harmonization and translation can be enhanced by aligning TOP-NT CDEs with preexisting CDEs in neurotrauma and noninvasive assessment domains. This is formally achieved as TOP-NT CDEs are organized using antecedent domains, subgroups/bundles, and structures of first-generation pre-clinical and clinical neurotrauma CDE initiatives (originally called form structures, Fig. 10). 38,39,46 –48 New TOP-NT CDEs were added to the following existing pre-clinical TBI general groups “Animal and Study Metadata,” “Animal Injury Models,” “Animal Assessments and Outcomes” and behavior groups “Affective Disturbance: Depression/Anxiety,” “Cognition and Motor: Learning/Memory.” 38 This effort harmonized the TOP-NT CDE data dictionary with prior Animal CDEs to make it easier for pre-clinical researchers to find, apprehend, and use elements. Regarding clinical CDEs, where possible, assay-related definitions were grouped with existing clinical structures. This was to match clinical MRI groups (“Subject,” “Equipment,” “Pulse sequence,” “DWI,” “fMRI,” “Analysis”; fitbir.nih.gov/dictionary; Figs. 7 and 10). 46 –48 Biomarker CDEs were indexed under BRICS structures “Experiment Metadata,” “Experiment Sample,” “Assay and Reagent,” and “Analyte and Test Result and Quality Control” (Figs. 8 and 10). These are governed by a FITBIR umbrella category called “Assessments and examinations; Laboratory Tests and Biospecimen/Biomarkers.” TOP-NT used the same biomarkers biofluids, tissue lysates, and histopathology measurements. Thus, the BRIC-formulated structures for biomarker name, signal (stain), and quality control served well for organizing TOP-NT histopathology elements (Figs. 9 and 10).
Neuropathology and clinical histology working groups for clinical TBI-associated neurodegeneration recently drafted UDEs for neuropathology of chronic TBI, including traumatic encephalopathy assessment, based on prior consensus NINDS/National Institutes of Health (NIH) meetings. 49 –51 From their form structures, the following correspond to parallel TOP-NT histopathology elements: “Brain tissue and post-mortem CSF” and “Paraffin block Inventory” on tissue preservation, quality control, and “brain region/ROI.” This merely illustrates that TOP-NT regional elements map to similar clinical neuropathology CDEs, despite differences in processing and anatomy. However, clinical neuropathology CDEs frequently employ a qualitative scoring system, whereas TOP-NT has been conducting quantitative particle counts and densitometry, limiting further comparison. In fact, this notion applies to all clinical domains, as nearly all TOP-NT variables are continuous quantitative metrics that were categorically aligned with clinical equivalents, yet the latter often are qualitative or ordinal score data. Therefore, while matching in the general topic, aligning specific data types diverge, as pathologists, physicians, and radiologists mostly collect experience-based qualitative scores and evaluations. Nevertheless, loosely aligning pre-clinical with clinical classification structures establishes an architecture of similar categories offering a shared translational language for exploring parallels between the realms.
Through extended collaboration across sites, a resulting TOP-NT Data Dictionary is now in place that each center has been using during the UH3 studies (Supplementary Table S2). Having this structure makes it easier to harmonize and align data. Implementing the elements between centers helps strengthen rigor and provides tools for multicenter pre-clinical TBI research with translational perspective. In this sense, this work creates now an opportunity to facilitate bidirectional translation because (1) clinical quality control elements are added to pre-clinical studies, (2) pre-clinical elements are connected where possible with clinical ones by a built-in parallel structure for translation, (3) pre-clinical-clinical assessment differences are revealed, and (4) continuity in the field is established by building and expanding TOP-NT CDEs on prior CDEs.
Data Structuring for Centralized Analysis Across Sites and Domains
Defined language and data processing pipelines are helpful but do not, by themselves, organize data from different centers and domains. Achieving interoperable datasets that map well between domains and centers often requires extensive restructuring (“data wrangling”). Hence, we report here steps that promote unified data structures for joint analyses of diverse, multidomain and multisite datasets (Figure 4, and Supplemental Figures S1, S2 and S3). These steps address format matching, achieving alignment, table organization, data management, and data sharing on a secure online portal.
A common analysis plan
As typical for multisite projects, a statistical analysis plan was designed and documented prior to conducting the UH3 phase experiments. Two analytic pathways will be used. At the univariate level, a repeated measures factorial design analysis of variance (ANOVA) is being applied to simultaneously assess main effect of injury, with severity, and effects of covariates (sex, time, and center), and their potential interaction with TBI outcome measures. The effect of “center” addresses reproducibility and models external validity. These statistics will inform on TBI-induced changes, data robustness, and weighted interactions of covariates. Second, exploratory multivariate analyses will be applied to reveal TBI signatures or phenotypes for future hypothesis testing 83,84 and Supplementary Table S1. The ANOVA reports will determine the design for subsequent covariate-controls when conducting multivariate analyses and are outlined below.
Data management guides for multimodal data analytics
The TOP-NT replication phase (UH3) is designed to retain domain-specific data depth. For multimodal TBI signatures, data need to be compatible across domains, to allow going beyond more traditional single-domain TBI assessments. Toward this goal, a first step is to recognize matching metadata between domains and centers. Data merging requires first a close look at the domain-specific data structure with repeated measures over time or in different brain regions, both affected by TBI progression. Thus, we developed detailed data structures in our datasets to facilitate centralized analyses. Consistent metadata link domains and provide clarity on the kind of correlations between variables: whether they concur, predict, or colocalize (Fig. 10). True technical replicates, measurements taken at the same experimental time point, brain region, and condition, become increasingly important for measurement reproducibility. Adopting replicates and quality controls provides clarity to differentiate technical variance from the natural distribution and spectrum of variability between subjects in specific injury models.
Practical points to organize data for multicenter studies
Data organizing steps have been jointly developed and implemented by the TOP-NT teams to ensure smooth cross-center multivariate and machine-accessible analytics. Each measurement is listed in a row aligned with columns linking it with the animal TOP-NT-ID, specimen type, marker, data type, and metadata. Key metadata specify each data point (row) with the unique group, sex, time point, and region, with all specifiers entered for each data point in the same row. Repeated measures that differ over time are hence assigned to separate data rows with a column designating injury-elapsed time (or time bin). Similarly, repeated measures in different brain regions are listed in separate rows indicating the anatomical region and coordinate positions (e.g., mm distance from bregma) in separate “region” column variables. Columns of injury specifics that do not apply to sham rats are indicated as not applicable (“NA”) minimizing perceived missingness. Alternatively, data, specifiers, and metadata are linked solely by a primary key, in this case each rat’s TOP-NT-ID. These are constructed to be less prone to entry errors. True technical replicates are listed as numbered replicates in separate columns residing in the same row for a given rat; one column for each replicate value. If replicate measures are listed in rows, then a separate naming column provides information on the relation to other replicates, and all metadata are copied to specify the replicate measure. Alternatively, technical replicates are averaged, and CV or deviations are reported instead. 73 Quality controls that apply to the entire data cohort, such as detection limits, standard deviations, and sham cohort CVs, are separately determined and are not part of the data list. The data set retains outliers and data points that fall out of the expected range (https://clsi.org). 52 This avoids list-wise software deletion of an entire dataset for a particular animal due to the omission of one individual data point and minimizes the loss of all associated variables in subsequent multivariable algorithms. 53,54 Extreme data points with an absolute differences larger than 4.5× of the median of the cohort can be inspected for possible technical or data entry mistakes. Furthermore, data retention allows for matching exceptional data points with potential extreme values across different variables that could provide clues about the source of the variability. 55,56
ODC-TBI data repository is a secure sharing portal
TOP-NT data are housed in the ODC-TBI online repository, together with the TOP-NT CDE data dictionary and SOPs, and data that will be made public upon DOI issue (https://odc-tbi.org). 3 ODC-TBI is a trusted, community-governed data repository with standards that are compliant with the NIH Data Management and Sharing Plan requirements. Its development is directed by the UCSF data analytics team of the Data Science, Brain, and Spinal Injury Center in collaboration with the FAIR Data Informatics Lab at the University of California-San Diego. This repository offers secure, controlled portal access for each individual laboratory as well as Consortium “MultiLab” pages for cross-site data sharing, management, and analyses.
Multivariate Analytics: Tools for Generating Multimodal TBI Signatures
Preprocessing steps that are needed for cross-domain analytics
Clear data structure and transparent temporal and spatial mapping as outlined above facilitates combining multiple datasets and their interrogation for higher-order analysis. The TOP-NT CDE data dictionary provides a semantic structure for standardized handling of data and metadata. Metadata, instrument specifications, and quality controls identify possible confounds and covariates. 57 This data organization has an advantage over separating measurements from conditions and metadata for two reasons: First, recording settings may reveal unexpected influences on measurements as opposed to just being named by subject matter experts. Second, animal and injury covariates allow connecting domains. 22,58,59 Hence, TOP-NT investigators have developed a data organization and language structure for multisite multimodal analyses to derive new information and relationships from several noninvasive assessment tools.
Additional data preprocessing steps allow applying linear principal component analysis (PCA). Heterogeneous data on nonlinear scales are common in neurotrauma and could impede PCA success. 60,61 Log-transformation, standardizing onto a common scale, or centering by each variable’s mean, among other tools, can render heterogeneous datasets more uniform to make them accessible for linear models. A prior group consensus was to run statistical analyses on both untransformed and transformed data with caution not to dilute any potential effects. 61,62
Principal component analysis
PCA is a variable reduction and feature extraction tool that identifies a series of principal components (PCs), which are new variables composed of combinations of the input variables arranged in such a way that they describe the greatest possible variance within the data. These PCs capture multimodal TBI features that subsequently can be associated across domains to arrive at diagnostic TBI patterns and profiles that quantitatively address the complex underlying pathophysiology. 63,64 PCA used in this manner can provide an unbiased grouping of data features and can capture which variables follow similar trends. PCA can provide a more complete understanding of measures that have the strongest or weakest influence on certain patterns of TBI pathophysiology.
Multivariate analyses will be adjusted to properly integrate relevant predetermined covariates such as sex, time, brain region, and center. New multimodal TBI signatures can emerge from such sequential analyses that will be described separately. Finally, data from the noninvasive tools will be aligned for validation with histopathology measures and behavioral outcomes. 65,66 Thus, the TOP-NT consortium design provides a structural framework for cross-domain validation to arrive at multianalyte biomarker and MRI patterns that may in the future inform clinical studies on TBI signatures derived from these diagnostic tools.
Adopting FAIR Data Sharing Principles
Data clarity advances an informatics framework for improved TBI classification through quality control, common language, shared structure, and an open dialog. 15,67 The TOP-NT consortium implements the Future of Research Communications and e-Scholarship working group’s FAIR guiding principles on good data management. 57
Findable
TOP-NT data are automatically given accession numbers upon upload to the ODC-TBI repository and serve as unique persistent identifiers for datasets and accompanying data dictionaries, metadata, and SOPs. Upon dataset publication, these accession numbers are converted to publicly available digital object identifiers (DOIs) released under a creative commons attribution license (CC-BY 4.0). This system complies with international data citation principles and data are indexed by the California Digital Library, Google, and other search engines on the public web. This makes the data findable using standard, freely available search tools. Findability within the datasets is further supported by the fact that data collected in TOP-NT share the same basic data organization: each data entry row is associated with a unique subject identifier, the TOP-NT-ID; canonical metadata were unified across domains and measurement types and units are explicit. New TOP-NT CDEs were also organized under existing pre-clinical and clinical FITBIR categories for a cohesive taxonomy to make searching and mapping easy. 38,46 Metadata and shared variables used general language, while some acquisition specifications needed more granular instrumentation and analysis expressions. Precise semantic definitions, such as CDEs, facilitate data findability.
Interoperable
To achieve interoperability, standardized experiment and analyses pipelines are streamlined across centers by TOP-NT SOPs and CDEs. Having an assembled consensus data dictionary facilitates harmonizing among TOP-NT sites and between TOP-NT and other CDE assembling efforts. Streamlining specific list-organizing steps improves data understanding, assembly, access, and computing across sites. Instances of interoperability in this study include (1) The TOP-NT data dictionary harmonizes the same and similar CDEs from different domains, for instance, by fusing canonical CDEs across domains. (2) An MRI code is used that expresses injury burden as a volumetric z-score-based cutoff. (3) Data formats are standardized across domains using z-scores to express changes observed from average sham measures at each center (Supplementary Data S1, Glossary). (4) An observer-independent large FOV digital cell counting and a densitometry-based histological approach is used. (5) Rat GFAP biomarker assay is replicated, and assay calibrants are exchanged and validated for comparison (see Supplementary Data S1).
Accessible and reusable
As stated, TOP-NT datasets, SOPs, and the CDE data dictionary will be accessible in the ODC-TBI repository (https://odc-tbi.org). Likewise, the curation of TOP-NT datasets to a DOI establishes provenance and a citation for author credit, making the data reusable and transparent. Ultimately, TBI pre-clinical CDEs will be accessible and reusable as TOP-NT and PRECISE teams are working on incorporating them for subsequent submission for approval by the NIH-endorsed CDE repository at the National Library of Medicine (NLM, see below).
TOP-NT is Embedded in Other Ongoing, and Future CDE Efforts in Neurotrauma
Considerable effort was made for new TOP-NT CDEs to align with existing CDEs, structures, and groups to promote the community effort in achieving a wider harmonization. The framework is useful because it provides continuity in pre-clinical CDE assembly and a taxonomy that, where possible, aligns pre-clinical CDEs with clinical CDEs. These efforts will improve rigor in experimental research. Several consortia presently work together on assembling a consensus pre-clinical TBI CDE dictionary and data organization format by defining language among pre-clinical neurotrauma and post-traumatic epilepsy (PTE) investigators. TOP-NT CDEs are being embraced by the PRECISE-TBI team (www.precise-TBI.org). TOP-NT investigators are also part of the NIH working group initiative for pre-clinical posttraumatic epilepsy, PTE CDEs. These efforts across consortia emphasize keeping core elements few and simple and definitions generalizable to suit each investigator’s need in an effort not to stifle research creativity. Consolidation efforts are underway that will result in curated, more generalized sets of CDEs by addressing challenges faced in different CDE structures and bundles as well as different data types used—for example, quantifying marker densities and cell numbers versus identifying cell types and their pathophysiological states. 68 Generalized CDEs will then be submitted to the NIH NLM and upon proofing, a set of endorsed TBI and PTE CDEs will be available as a NLM CDE repository. Thus, TOP-NT CDEs are already team-tested tools that now can help facilitate and validate translational TBI research.
Transparency, Rigor, and Reproducibility Summary
To increase rigor, reproducibility, and transparency in pre-clinical research, TOP-NT is rigorously documenting their SOPs for pre-clinical TBI models, instrumentation, and analyses using a range of multimodal measurements (see Supplementary Data S2, SOP Compendium). Prior to the work, the approaches for data analyses and reporting are outlined. All data, SOPs, and associated CDE dictionaries are being made available with assignment of a doi for permanent identification. Power calculations with UG3 phase data estimate effective power >0.80 for UH3 studies. Mortality is followed up with a replacement to ensure the planned sample sizes. Rigor is a planned component of the research, including close adherence at all research centers to the SOPs (see Supplementary Data S2, SOP compendium). Detailed reporting of all preidentified variables is achieved by documenting CDEs from the here compiled dictionary that are then associated with all datasets (see Supplementary Table S2, CDE Data Dictionary). 69 Rigor also includes random assignment of rodents to the experimental conditions, reporting of mortality replacement to ensure the planned sample sizes, excluson criteria, and blinding of investigators to animal treatments. Reproducibility is an inherent component of the project, where at least two centers conduct the same pre-clinical TBI models (FPI and CHIMERA), and four sites reproduce CCI. For transparency in documentation of potential site-specific differences, an a priori shared statistical analysis plan includes determining the degree of site-specific differences. True replicates are built-in for biomarker assays and histopathology data, allowing to compute CVs to evaluate technical variability.
Limitations
The formation of the consortium was dictated by the funding announcements, and several a priori limitations are notable. There are limiting temporal constraints (grant term). No therapeutic arm has been incorporated into the research plan, which are summarized elsewhere. 7,8 A single species was chosen, and TBI models have been limited to three approaches bound by different levels of injuries. Assessing injury severity by design in animal TBI models remains controversial. It is well-known that severity assessment is problematic in the clinical setting, each TBI patient differs. This is, in part, also true among laboratory animals; severity is a complicated product of injury, covariates, and confounds. Thus, assessing TBI by developing specific TBI phenotypes beyond the conventional concept of severity is an alternative path. The sponsor requested the use of common TBI models in widely used laboratory rats. Funding limitations precluded the use of larger species with a gyrencephalic brain, greater astrocyte/neuron ratio, and greater white matter volume and complex subcortical geometry, all factors that may better mimic human TBI, the magnitude of axonal and astrocyte biomarkers, and scale and resolution of MRI responses. Aside from recording the righting reflex post-surgery and respiration rates during MRI recordings, a broad battery of extracerebral pathophysiological disturbances has not been included in this study. Funding was based on competition of individual investigator teams, not requiring any preforged multisite collaborative arrangement, as is otherwise typical for consortia. While completing first-stage studies, replication experiments started simultaneously with sharing and harmonizing protocols and training teams at partner sites. Clear communication across disciplines and levels is crucial to overcome jargon, break down silos, and achieve cross-domain alignment—by funding agencies recognized as vital for success, this remains underappreciated. These activities require added time investment. This work aims to provide outcomes with translational inference, yet marker choice was pragmatic based on prior tested effect size cutoff. Thus, other clinically relevant measures used in the intensive care unit, such as arterial and intracranial pressure, could not have been included in this study. Importantly, there is no mandate for pre-clinical TBI colleagues to adopt this framework nor will the provided suggestions for future studies affect the sponsor’s decision-making processes. However, this effort delivers an architecture of cross-site and multimodal pre-clinical harmonization that contributes to uncover TBI signatures and their pathophysiology. 14,16,59,69 –72
In conclusion, the TOP-NT efforts established a compendium of pre-clinical, translationally relevant TBI assessment tools and their validation for use in rodent TBI models. Here we provide prospectively harmonized language and unified data curation steps. This architecture facilitates team science by supporting rigorous, transparent, reproducible, and bidirectional exchange in neurotrauma research. A multidomain consortium of different subject matter experts can contribute toward a research-clinical continuum in using noninvasive TBI assessments and informing on their underpinnings. The presented work documents practical sharing steps to overcome barriers between domains and laboratories to achieve a joint goal. Prospective harmonization promotes multisite collaboration and facilitates multivariate analyses to arrive at a higher level, syndromic understanding of TBI signatures.
Footnotes
Acknowledgments
The authors are tremendously grateful for the determined work and continuous encouragement of current and previous NINDS/NIH Program directors, administrators, and program specialists for making the TOP-NT consortium come to fruition: Lyn Jakeman (NIH/NINDS), Director Division of Neuroscience in Extramural Programs; Patrick F. Bellgowan, NIH/NINDS, Deputy Associate Director of NINDS; Rebecca Berman; Carol Taylor-Burds; Diana Cummings. The authors are grateful for contributions from Hye-Young Heo, Qianqi Huang, Meiyappan Solaiyappan, Elizabeth Banyas, and Shruti Vadlakonda at Johns Hopkins University. The authors appreciate the generosity of Dr. Gerry Shaw, EnCor Biotechnology Inc. Gainesville, FL, for providing several antibodies for immunohistochemistry, immunoblotting, and for the ALDOC MSD assay. For their extended technical assistance, the authors want to express special gratitude to Victoria Parrilli, Isabella Bonacorsi, and Kaitlyn Tingus at the Semel Institute for Neuroscience and Human Behavior, IDDRC, Geffen School of Medicine, UCLA, Los Angeles, CA 90095-7332. The authors are indebted to the various contributions from the UCLA Undergraduate Research Students: Christian G. Hernandez, Sarah E. Stay, Isabella V. Manzano-Stettler, Diana Ikilikyan, Cynthia T. Bui, Taylor A. Pio, Santhosi S. Samudrala, Christiana Prekopa, Daniel Talebzadeh Shoushtari, Jiayi Wu, Justin Bui, Ishaan Deep Upadhyay, Radhika Singh, Rohita Thammineni, Suhas Yarra, Michael Leung, Saman Andalib, Victor Guitierrez-Garcia, Zubair Ahmed, and Bushra Shaia; Department of Neurosurgery, BIRC; Salma Arredondo, Hana Abdirahman, Sophia Newton, and Erijeana H. Colet; Semel Institute for Neuroscience and Human Behavior, IDDRC, Geffen School of Medicine, UCLA, Los Angeles, CA 90095-7332.
Nathan Vanderveer-Harris, ![]()
Yunfan Zou,
Babak Moghadas, ![]()
Adnan Bibic, PhD, ![]()
Jiamei Hou, MD, PhD,
Laura B. Tucker, MS, ![]()
Amanda Fu, MD, ![]()
Jiong Liu, MD,
Anya Fan,
Jacqueline C. Bresnahan, PhD, ![]()
Michael S. Beattie, PhD, ![]()
Susanna Rosi, PhD,
Majory Pompilus, MD,
Abel Torres-Espín, PhD, ![]()
Jeffrey S. Grethe, Ph.D, ![]()
Jonathan Lopez;
Madison P. Klee;
Annika Myers;
Aditi Vichare;
Melissa Walker, PhD,
Dara L. Dickstein, PhD,
Alex C. Harvey, MS,
Xiong Jiang, PhD,
Ruchelle G. Buenaventura, MS, ![]()
Bevan S. Main, PhD, ![]()
Bernard Dardzinski, PhD, ![]()
Esmeralda Mendoza, MPH;
Patricia J. Axtman,
Authors’ Contributions
All primary listed authors contributed substantially to the conception of the work, revising it critically for important intellectual content, approved the final version to be published, and agreed to all aspects of the work being accurate and integrative. I.-B.W., J.T.M., N.G.H., A.R.F., T.E.V.M., K.K.W., J.R.H., A.K., M.F., M.K., M.P.B., R.C.K., and Jin.Z. designed the study and methodology, curated data, SOPs, and defined CDEs. J.W., Jie.Z., J.R.H., M.P.K., A.P., A.T., J.L., A.B., A.M., A.V., and J.A.L. curated data, SOPs, and defined CDEs. I.-B.W. and J.T.M. drafted the article with input from N.G.H., J.R.H., R.C.K., A.R.F., M.F., T.E.V.M., A.K., J.A.L., F.K., M.P.B., R.R., J.W., K.K.W., H.L.R., S.A., H.O.A. I.-B.W., M.F., and C.M.M.-C. designed the figures with input from A.R.F., N.G.H., J.T.M., H.L.R., Jin.Z., I.-B.W., and L.M.D. assembled the glossary with edits from T.E.V.M., J.T.M., and H.O.A.
Author Disclosure Statement
No competing financial interests exist. J.T.M. is a federal employee, but the opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the U.S. Army, Department of Defense, the U.S. Government, or the Uniformed Services University of the Health Sciences. The use of trade names does not constitute an official endorsement or approval of the use of reagents or commercial hardware or software. The content is solely the responsibility of the authors and does not necessarily represent the official views of the
Funding Information
NINDS/NIH UG3/UH3 Cooperative agreement: UCLA: UG3/UH3NS106945; UF/MSM: UG3/UH3NS106938; JHU: UG3/UH3NS106937; Georgetown: UG3/UH3NS106941; UCSF: UG3/UH3NS106899 and UH3NS106899-04S1. The studies were supported by the NINDS/NIH efforts through the Translational Outcomes Project in NeuroTrauma (TOP-NT) program (RFA-NS-17-023), and through the generosity of the Vivian L. Smith Foundation.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.