
Abstract
After moderate to severe traumatic brain injury (TBI), sleep disturbance commonly emerges during the confused post-traumatic amnesia (PTA) recovery stage. However, the evaluation of early sleep disturbance during PTA, its recovery trajectory, and influencing factors is limited. This study aimed to evaluate sleep outcomes in patients experiencing PTA using ambulatory gold-standard polysomnography (PSG) overnight and salivary endogenous melatonin (a hormone that influences the sleep-wake cycle) assessment at two time-points. The relationships between PSG-derived sleep-wake parameters and PTA symptoms (i.e., agitation and cognitive disturbance) were also evaluated. In a patient subset, PSG was repeated after PTA had resolved to assess the trajectory of sleep disturbance.
Participants with PTA were recruited from Epworth HealthCare's inpatient TBI Rehabilitation Unit. Trained nurses administered overnight PSG at the patient bedside using the Compumedics Somté portable PSG device (Compumedics, Ltd., Australia). Two weeks after PTA had resolved, PSG was repeated. On a separate evening, two saliva specimens were collected (at 24:00 and 06:00) for melatonin testing. Results of routine daily hospital measures (i.e., Agitated Behavior Scale and Westmead PTA Scale) were also collected. Twenty-nine patients were monitored with PSG (mean: 41.6 days post-TBI; standard deviation [SD]: 28.3). Patients' mean sleep duration was reduced (5.6 h, SD: 1.2), and was fragmented with frequent awakenings (mean: 27.7, SD: 15.0). Deep, slow-wave restorative sleep was reduced, or completely absent (37.9% of patients). The use of PSG did not appear to exacerbate patient agitation or cognitive disturbance. Mean melatonin levels at both time-points were commonly outside of normal reference ranges. After PTA resolved, patients (n = 11) displayed significantly longer mean sleep time (5.3 h [PTA]; 6.5 h [out of PTA], difference between means: 1.2, p = 0.005). However, disturbances to other sleep-wake parameters (e.g., increased awakenings, wake time, and sleep latency) persisted after PTA resolved.
This is the first study to evaluate sleep disturbance in a cohort of patients as they progressed through the early TBI recovery phases. There is a clear need for tailored assessment of sleep disturbance during PTA, which currently does not form part of routine hospital assessment, to suggest new treatment paradigms, enhance patient recovery, and reduce its long-term impacts.
Introduction
Post-traumatic amnesia (PTA) is a transient phase of early recovery following a moderate to severe traumatic brain injury (TBI). 1 The PTA phase occurs immediately after coma, 1 and it is characterized by the presence of sleep-wake cycle disturbance (up to 80% of patients), 2 confusion, disorientation, memory disturbance, agitation, and uncharacteristic behavior. 1 During PTA, individuals experience decreased sleep efficiency, 3 poor sleep quality and maintenance, 4 disruption to sleep staging 4 and abnormal endogenous melatonin levels (a sleep signaling hormone). 4 The early onset of sleep disturbance is likely a cumulative effect of pathophysiological, environmental, and individual factors (e.g., trauma to sleep-regulating brain systems, age, hormone system disruption, pain, and/or agitation). 5,6 However, there has been limited investigation into sleep disturbance during PTA, its recovery trajectory, and contributing factors.
The gold standard in sleep assessment is a polysomnography (PSG) sleep study, 7 which directly monitors physiological body signals to determine sleep-wake parameters and staging. Prior research has assumed that confused, restless, and behaviorally disturbed patients in PTA would be unable to comply with the requirements of PSG. 3,8 Therefore, PSG has often been precluded, in favor of simpler, albeit less accurate, 9 sleep assessment modalities (e.g., accelerometer-based wristwatches that indirectly estimate sleep from wrist activity). 2 Our group recently demonstrated in a pilot study that ambulatory PSG (adherence rate: 63.0%) and endogenous salivary melatonin assessment at two time-points are feasible for rehabilitation inpatients experiencing PTA. 4 During PTA, patients displayed significant sleep disruptions including increased sleep latency, frequent awakenings, increased wake time, reduced slow-wave sleep, poor sleep efficiency, and abnormal melatonin levels. 4
Melatonin is a stable and commonly used phase marker of the circadian rhythm, which can be evaluated through urine, blood, or saliva samples. 10,11 Melatonin has a temporal 24-h rhythm, being predominantly secreted in the evening to facilitate sleep onset 12 and reducing by morning to promote wakefulness. Studies have frequently reported decreased and disrupted melatonin secretion patterns post-TBI. 13 –16 Melatonin abnormalities can dysregulate the sleep-wake cycle 17 and may contribute to sleep disturbance. 18 Prior TBI studies have implemented frequent sampling to determine dim light melatonin onset (DLMO; the onset of melatonin secretion) and circadian timing (e.g., half-hourly or hourly sampling). 13,15,16,19 However, these studies included participants who had either emerged from PTA or whose PTA status was not specified. 13,15,16,19
During PTA, sampling at frequent intervals is likely impractical due to patients' agitation, restlessness, disorientation, and/or confusion, and would require increased patient burden. Given the symptoms of PTA, management guidelines recommend the provision of a low-stimulation environment and limiting assessments that can cause agitation or excessive fatigue. 1 Research has reported that frequent overnight nursing activities have been significantly associated with poorer sleep efficiency, sleep fragmentation, and daytime fatigue during inpatient rehabilitation. 20 A pilot study 4 successfully determined abnormalities to salivary melatonin levels during PTA at two time-points, which were selected based on the habitual rhythm of melatonin secretion. Limited research has also suggested a bi-directional association between sleep disturbance and other PTA symptoms, such as agitation and cognitive impairment. 7 Agitation is characterized by behavioral disturbances 1 (i.e., restlessness, aggression, disinhibition, and/or emotional lability). One study reported that agitated patients in PTA had significantly decreased sleep time and sleep efficiency (measured through actigraphy), when compared to non-agitated patients in PTA. 21 Cognitive function also appeared to improve in parallel with sleep efficiency during PTA. 3 Further research is needed to evaluate the impact of these factors on disturbed sleep parameters during PTA and patient tolerability of PSG.
The duration of PTA is considered an important indicator of TBI severity 1 (i.e., prolonged periods of PTA indicate a more severe TBI). However, improved sleep has also been significantly associated with the resolution of PTA. 3 Studies have reported that patients who are no longer in PTA displayed significantly increased sleep efficiency, 2,3 more consolidated rest-activity cycles, 8 increased sleep time, 2 and reduced sleep-wake cycle disturbance 2 compared to patients in PTA. However, these studies compared separate and unmatched patient groups in each recovery stage, which may be vulnerable to the factors that influence sleep (e.g., age, sex, pre-injury sleep-wake habits, pain, medication). 6 Studies could potentially control for the effect of these factors by comparing individual patient results across two distinct phases (during PTA and after PTA resolves).
Further research that develops the understanding of sleep disturbance trajectories and influencing factors is needed for several reasons. In TBI research, sleep abnormalities have been associated with various negative repercussions including fatigue, 22 decreased patient adherence to rehabilitation (often the result of sleepiness), 23 increased pain, 24 depression/anxiety, 24 psychotic symptoms, 7 and decreased cognition. 25,26 Sleep disturbance can also protract patient recovery by prolonging confusion and memory disturbance, 7 thereby delaying the recovery from PTA. This could be detrimental given sleep disturbance is not routinely assessed in hospital and rehabilitation settings. 27 Therefore the objective of this study is to expand the results of the earlier pilot study, 4 with further consideration of the limitations of current research.
Study aims and hypotheses
To examine the feasibility and outcomes of overnight gold-standard PSG and salivary endogenous melatonin assessment at two time-points (24:00 and 06:00) in a larger sample of patients experiencing PTA following a moderate to severe TBI;
To assess the relationship between sleep-wake parameters, PSG tolerance, and other symptoms of PTA, including agitation and cognitive disturbance; and
To evaluate the trajectory of sleep disturbance in a subset of patients, by comparing the outcomes of PSG and salivary endogenous melatonin assessment during PTA to the period after PTA resolves.
Consistent with prior literature, it was hypothesized that patients experiencing PTA would display a greater degree of sleep disturbance, indicated by abnormalities to sleep quality and staging, compared to the period after PTA resolved. It was hypothesized that during PTA, melatonin levels at the specified time-points will be abnormal when compared to reference ranges. It was also hypothesized that there will be a significant association between PSG-derived sleep parameters and assessments of agitation and cognition during PTA.
Method
This prospective, observational study was initially approved as a pilot study by the Epworth HealthCare Human Research Ethics Committee (HREC). 4 Following the success of the pilot study, 4 this study was expanded to include a larger sample that replicated the pilot study's methodology. The full-scale study was approved by Monash Health's HREC (study number RES-19-0000-156E).
Participants
Prospective participants were recruited from consecutive admissions to Epworth HealthCare's specialist, inpatient Acquired Brain Injury (ABI) Rehabilitation Unit. The unit includes a dedicated and secured area for patients in PTA who are cared for in single, low-stimulation rooms (e.g., low noise, consistent staff and environment, limited visitors, assessment and therapy according to patient agitation and fatigue, and flexible sleep opportunities). 1 The eligibility criteria for participation included: (1) being in PTA as determined by the Westmead PTA Scale (WPTAS), 28 (2) having sustained a moderate to very severe TBI (measured by PTA duration), 29 and (3) being an adult age ≥18 years. The duration of PTA is a frequently employed indicator of TBI severity, and it is regarded as the best single clinical predictor of patient outcomes, and as compared to other indices. 30 –32 Current guidelines 1 recommend the WPTAS as the preferred measure for determining the duration of PTA, and it is also the most predominately used measure throughout Australasia. 1,33 This study excluded patients with a documented pre-existing sleep disorder and/or sleep problem, behaviorally disturbed patients on an extreme level who would be unable to tolerate the study protocol (as was advised by the treating rehabilitation physician), and patients prescribed medications for the treatment of sleep disturbance (e.g., melatonin).
Measures
Ambulatory PSG
The Compumedics Somté (V1 system; Compumedics, Ltd., Abbotsford, Australia) is a portable multi-channel PSG recording device that enabled unattended and ambulatory monitoring at the patient's rehabilitation bedside. This lightweight device was attached to the patient's torso overnight with a Velcro strap. Multiple physiological parameters were recorded via surface electrodes that were secured to the patient's face and scalp. The channels selected were based on the Australasian Sleep Association's guidelines for type 2 studies (unattended, ambulatory PSG). 34 The sites for electrode placement have been described previously. 4 For a standard PSG, the minimum required recording time is 6 h. 35 The PSG recordings were scored by Epworth HealthCare's senior sleep scientists according to the American Academy of Sleep Medicine Scoring Manual (AASM; version 2.3). 36 Sleep-wake parameters were determined such as sleep latency (time to sleep onset), total sleep time, sleep efficiency (the ratio of time spent asleep compared to time spent in bed) and sleep staging.
This study monitored additional parameters as the prior pilot study, 4 and these were reported as per the AASM manual. 36 The additional parameters determined by the Compumedics Somté software included: total wake time ([Sleep Period] – [Total Sleep Time]), sleep period ([Total Recording Time] – [Sleep Onset]) and awakenings (number of transitions from any sleep epoch to an epoch of wake after sleep onset, excluding the final awakening). In this study, arousals that led to awakenings were reported, and are recognized as a “critical” or “important” parameter for clinical decision-making and outcomes within the AASM Clinical Practice Guidelines. 37
Salivary endogenous melatonin
Melatonin Hormone Profile Kits were provided by Australian Clinical Labs Pathology Service (Australia), and they contained test tubes to collect saliva at two time-points overnight: 24:00 and 06:00. The midnight saliva specimen was taken in dim room lighting. These two time-points were specified by the Pathology Service given melatonin levels are on the rise at 24:00 in healthy individuals, 38 and naturally decline by the morning sample including post-TBI. 16 The study protocol did not include additional time-points, which are only required if small phase changes are of interest, 11 and was beyond the aims of the study. Saliva specimens were supplied to a collection center to be assayed. The analysis process is detailed elsewhere. 4 The pathology report provided melatonin levels in picomoles per liter (pmol/L), which were converted to picograms per milliliter (pmol/L/4.30 = pg/mL) 39 as per prior research. 4,16 The normal reference ranges provided by Australian Clinical Labs were based on healthy population studies and included 10–40 pg/mL (midnight sample) and <3.0 pg/mL (morning sample).
Westmead PTA Scale (WPTAS)
The 12-item WPTAS 28 is a standardized, bedside assessment to prospectively monitor daily PTA status and duration. Seven items assess orientation (age, date of birth, month, time of day, day of week, year, name of place) and five items assess anterograde memory (person recall and picture recall). Once a patient achieved perfect scores (12/12) on the WPTAS for 3 consecutive days, they were cleared of PTA. The duration of PTA was calculated as the days elapsed between the injury to the first day of the 3 consecutive days of perfect scores.
Agitated Behavior Scale (ABS)
The 14-item ABS 40 is a serial assessment of agitation and behavioral aspects of agitation. Each behavior (item) was rated on a 4-point Likert scale based on its severity and impact ranging from 1 (absent) to 4 (present to an extreme degree). Scores were summed to produce a total score, and an ABS of greater than 21 indicated clinically significant agitation. A recent factor analysis of the ABS produced two constructs (aggression/lability and restlessness), which can provide additional information as to the type of behavioral agitation. 41 The scoring of these constructs (subscales) is detailed therein. 41
Procedure
A study team member reviewed the consecutive admissions to the ABI Unit according to the pre-determined criteria. Patients in PTA have an insufficient capacity to make reliable decisions due to daily memory disturbance. Written informed consent was instead sought from the designated person responsible (i.e., family member or close other). Study measures were conducted at the rehabilitation bedside by trained associate nurse unit managers. The Somté device was connected to the patient overnight at bedtime (21:00 to 06:00 “lights-out” period on the ward). The skin sites for electrode placement were prepped and electrodes were secured, as described previously. 4 On a separate evening, the nursing staff collected two saliva specimens at the specified times. Saliva sampling occurred on a separate evening, to ensure that PSG monitoring was not interrupted. Study measures were repeated in a subset of patients after 2 weeks and once PTA had resolved (determined by the WPTAS) if they remained as inpatients. Patients therefore acted as their own controls.
After patients recovered from PTA, they participated in an inpatient rehabilitation program that could vary in duration and intensity. The timing of rehabilitation discharge was therefore unrelated to the timing of the repeated PSG. A ward neuropsychologist or nurse administered the WPTAS (daily) and the ABS (on weekdays only) while patients were in PTA. These measures were collected on patient rehabilitation admission and over 3 consecutive days: (1) the day before PSG, (2) the day of PSG, and (3) the day after PSG. Patient and clinical characteristics recorded in electronic health records were also collected. Injury Severity Scores (ISS) 42 were calculated retrospectively by a senior physiotherapist using patients' admission medical documentation. Higher total ISS indicated increased trauma severity.
Statistical analysis
All outcome variables were initially examined for normality and other assumptions using standard techniques such as box plots, histograms, and normal probability plots. 43 Where distributions appeared to be skewed, results were confirmed using both conventional parametric tests applied to (natural) log transformed outcome variables and negative binomial regression 44 applied to the original, untransformed outcomes. Descriptive statistics including the means and standard deviations (SDs) of collected data were performed. The significance and strength of the association between ABS scores, WPTAS scores, and PSG-derived sleep-wake parameters were evaluated using Pearson correlation analysis. In this study, the following correlation coefficients (r) were used to define the strength of the association: 0.10 (small effect), 0.20 (medium effect), 0.30 (large effect), and 0.40 or greater (very large effect). 45 Independent sample t-test comparisons were conducted to evaluate mean differences between groups. Within group comparisons of ABS scores and WPTAS scores over the 3 consecutive days were evaluated using paired samples t-tests. Statistical significance was set at p < 0.05. IBM SPSS Statistical software (IBM SPSS, version 29; IBM Corp., New York) was employed to conduct the statistical analyses.
Results
Sample characteristics
This study recruited 57 participants. Following informed consent, 11 patients' recovery progression took them out of the criteria for the study (e.g., they emerged from PTA) and PSG had not yet been completed. Of the remaining 46 patients, 29 had ≥6 h of PSG recording time (PSG adherence rate: 63.0%). In patients with <6 h of PSG recording time, this was either due to lost signals from unattended monitoring (n = 12 patients) or the patient removed the device (n = 5). Of the total sample (n = 57), saliva sampling for melatonin assessment occurred in 47 patients who were in PTA at the time of measurement. However, the WPTAS retrospectively determined the end date of PTA (i.e., the first day of 3 consecutive perfect score days). On this basis, 6 patients were considered to have emerged from PTA on the day of melatonin assessment and were excluded from the analyses. In 4 patients, only one saliva sample was obtained and successfully assayed for melatonin; however, these data were included. The analytic sample therefore comprised 29 patients with PSG monitoring, and 41 patients from whom saliva samples were collected and assayed for melatonin. Patient demographics and clinical characteristics are displayed in Table 1. A subset of 11 patients had PSG conducted during PTA and again after PTA resolved. Within the PSG sample, the mean age was 47.2 years, 62.1% were male, and 75.9% experienced a very severe TBI.
Patient Demographics and Clinical Characteristics
GCS, Glasgow Coma Scale; ISS, Injury Severity Score; LOS, length of stay; MVA, motor vehicle accident; N, number; PED, pedestrian; PSG, polysomnography; PTA, post-traumatic amnesia; SD, standard deviation; TBI, traumatic brain injury.
PSG-assessed sleep-wake parameters during PTA
Ambulatory PSG was conducted at a mean of 41.6 days (SD: 28.3) post-TBI. The PSG-assessed that mean sleep and wake parameters in patients experiencing PTA were divergent from normal values 46,47 and were indicative of poor sleep quality 48 (refer to Table 2). Patients displayed delays in falling asleep (mean sleep latency: 42.9 min, SD: 36.9). Sleep duration was reduced (mean: 5.6 h, SD: 1.2), and appeared to be unconsolidated and fragmented with repeated awakenings (mean: 27.7, SD: 15.0). This led to increased wake time during sleep periods (mean: 92.3 min, SD: 68.1) and reduced mean sleep efficiency (the latter was below normal values 48 in 82.8% of patients).
PSG-Assessed Sleep and Wake Parameters
h, hour; min, minutes; N, number; NREM, non-rapid eye moment; N1, NREM stage 1; N2, NREM stage 2; N3, NREM stage 3; PSG, polysomnography; pts, patients; PTA, post-traumatic amnesia; REM, rapid-eye movement sleep; SD, standard deviation.
Patients also displayed disruptions to sleep macro-architecture (staging). The mean proportion of non-rapid eye movement (NREM) sleep and its specific stages (NREM Stage 1 [N1] and 2 [N2]) were higher than normal values, 46 indicating that the majority of sleep time was spent in lighter sleep. Deep, slow-wave sleep (NREM Stage 3 [N3]) was reduced or completely absent (37.9% of patients). Patients with N3 sleep displayed significantly longer periods of total sleep time (mean: 362.1 min, SD: 79.4) compared to patients who were unable to enter N3 sleep (mean: 292.5 min, SD: 35.5) (difference between means: −69.6, 95% confidence interval [CI]: −114.0 to −25.2, p = 0.003). Sleep efficiency was also poorer for patients who were unable to enter N3 sleep (mean: 63.2%, SD: 13.2) compared to patients with N3 sleep (mean: 71.3%), SD: 16.2, albeit statistically non-significant.
Relationship between ABS, WPTAS, and PSG-derived sleep-wake parameters
Table 3 displays the mean ABS and WPTAS scores. There were some missing data due to the practicalities of routine data collection within a working ward (e.g., the ABS was administered on weekdays only; refer to Table 3). Across the four time-points, patients displayed relatively low mean ABS scores, ranging from 16.4 to 18.9 (normal behavior). There was no statistically significant difference in mean ABS scores between admission and the day of PSG. There was also no statistically significant increase in agitation between the day of PSG and the day after PSG. Patient tolerability during PSG was further inspected by comparing mean ABS scores on the day of PSG between patients with ≥6 h (minimum recommended recording time) 39 and <6 h of PSG recording time. Total ABS scores did not significantly differ by PSG recording time, suggesting that agitation levels were not a significant contributing factor to PSG adherence. The ABS scale measured several behavioral aspects of agitation; however, there were low patient frequencies across most items (<30.0%; Fig. 1).
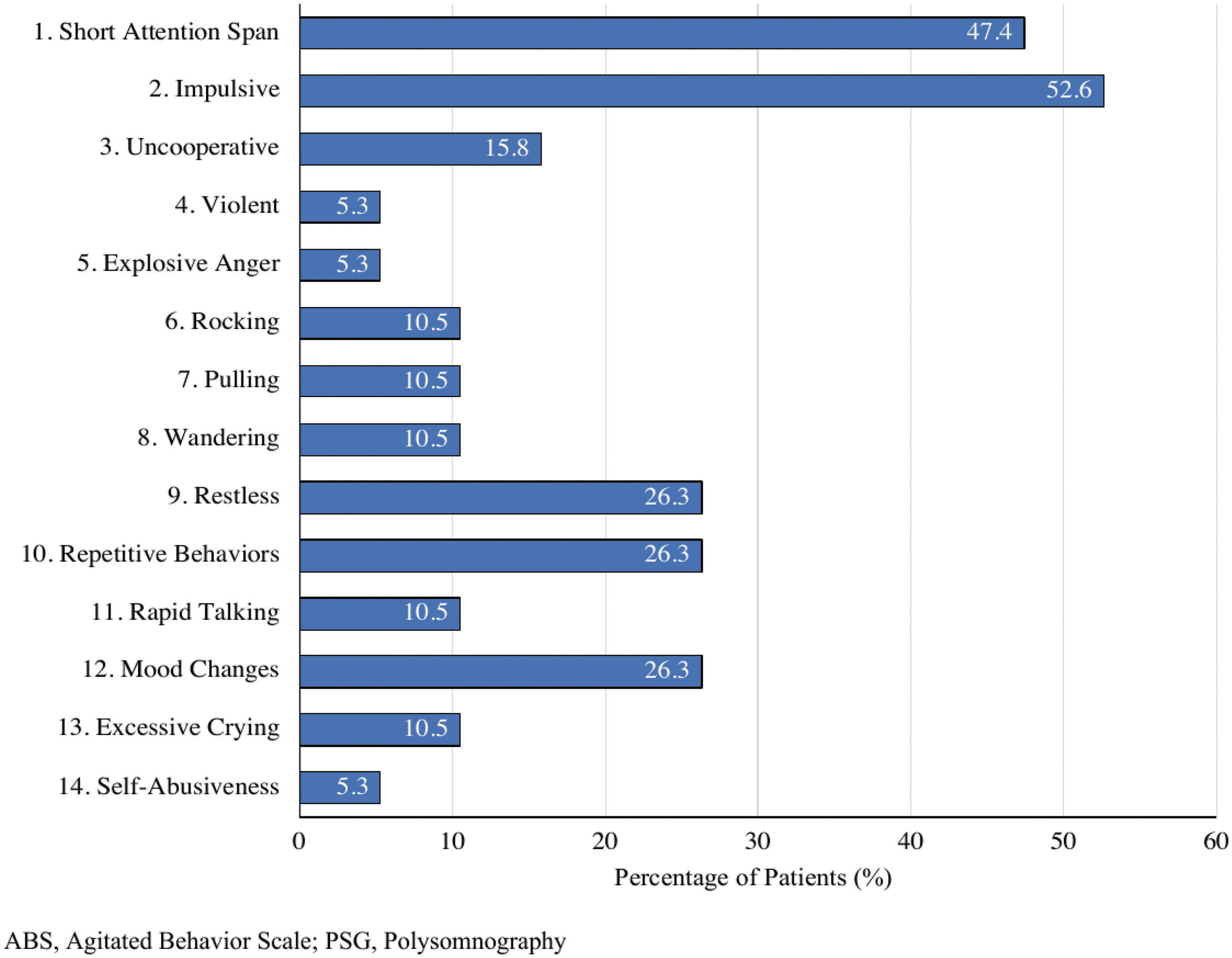
Frequency of patients (%) displaying individual ABS items on the day of PSG.
ABS and WPTAS Descriptive Statistics for 29 Participants with PSG Data
ABS, Agitated Behavior Scale; N, number; PSG, polysomnography; SD, standard deviation; WPTAS, Westmead Post-Traumatic Amnesia Scale.
There were no statistically significant correlations between PSG-derived sleep-wake parameters and total ABS scores on the day of PSG testing, apart from N2 sleep (%). There was a marginally significant, positive and very large association between total ABS scores on the day of PSG and the proportion of N2 sleep (%; Pearson correlation coefficient [r] = 0.5; p = 0.04; refer to Supplementary Fig. S1). This suggested that patients who had increased N2 sleep during sleep periods may have relatively higher levels of agitation. The WPTAS scores on the day of PSG testing were not significantly associated with the sleep-wake parameters.
Assayed endogenous melatonin levels
Mean endogenous melatonin level at midnight was 11.8 pg/mL (SD: 15.5), and at morning it was 14.0 pg/mL (SD: 14.7; see Fig. 2). Over two-thirds (70.7%) of the sample's midnight melatonin levels were outside the normal reference range (10–40 pg/mL). Similarly, 63.4% of the sample's morning melatonin levels were outside the normal reference range (< 3.0 pg/mL). The mean melatonin change between both time-points was −1.8 (SD: 12.6). The majority of patients displayed either a higher melatonin level for the morning sample (n = 18, 48.6% of sample) or no change (n = 7, 18.9%). This suggested abnormalities to melatonin secretion compared to its habitual rhythm and normal reference ranges. There were also no statistically significant associations between melatonin levels and the PSG-derived parameters.

Endogenous melatonin levels across both times-points for each patient.
Comparison of sleep-wake parameters between recovery stages
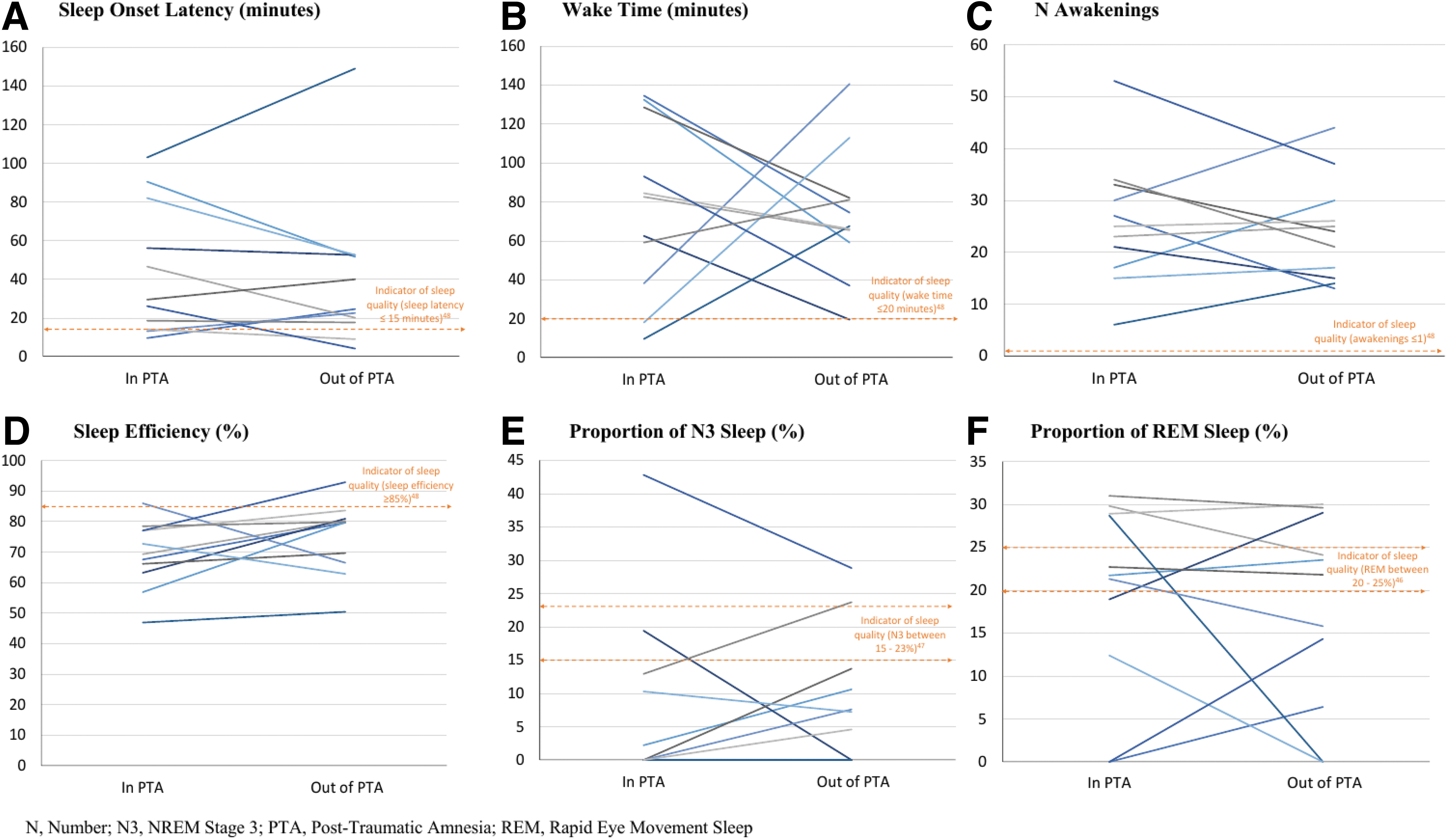
Table 4 and Figure 3 display patients' mean sleep and wake parameters measured with PSG during both recovery phases. After the emergence from PTA, patients displayed significantly longer mean sleep duration (5.3 h [PTA]; 6.5 h [out PTA], difference between means: 1.2, 95% CI: 0.5-2.0, p = 0.005). However, patients displayed sleep disturbance and fragmentation during PTA, which continued after PTA resolved. During both recovery phases, patients displayed increased mean sleep latency, number of awakenings, and wake time. Mean sleep efficiency slightly improved between the PTA phase (69.2%, SD: 11.0) to after PTA resolved (75.1%, SD: 11.7), albeit this was statistically non-significant. During both phases, mean sleep efficiency was still below normal ranges (≥ 85%). 48 The proportion of deep, slow-wave restorative sleep remained low. During both phases, patient means for all sleep and wake parameters were outside normal ranges and values indicative of “good sleep quality” 48 (see Table 4 and Fig. 3). Figure 4 displays a graphical representation of PSG recordings (hypnogram) in a patient example as the patient recovered from PTA.
Comparison of select sleep-wake parameters in same patients between recovery stages (n = 11).
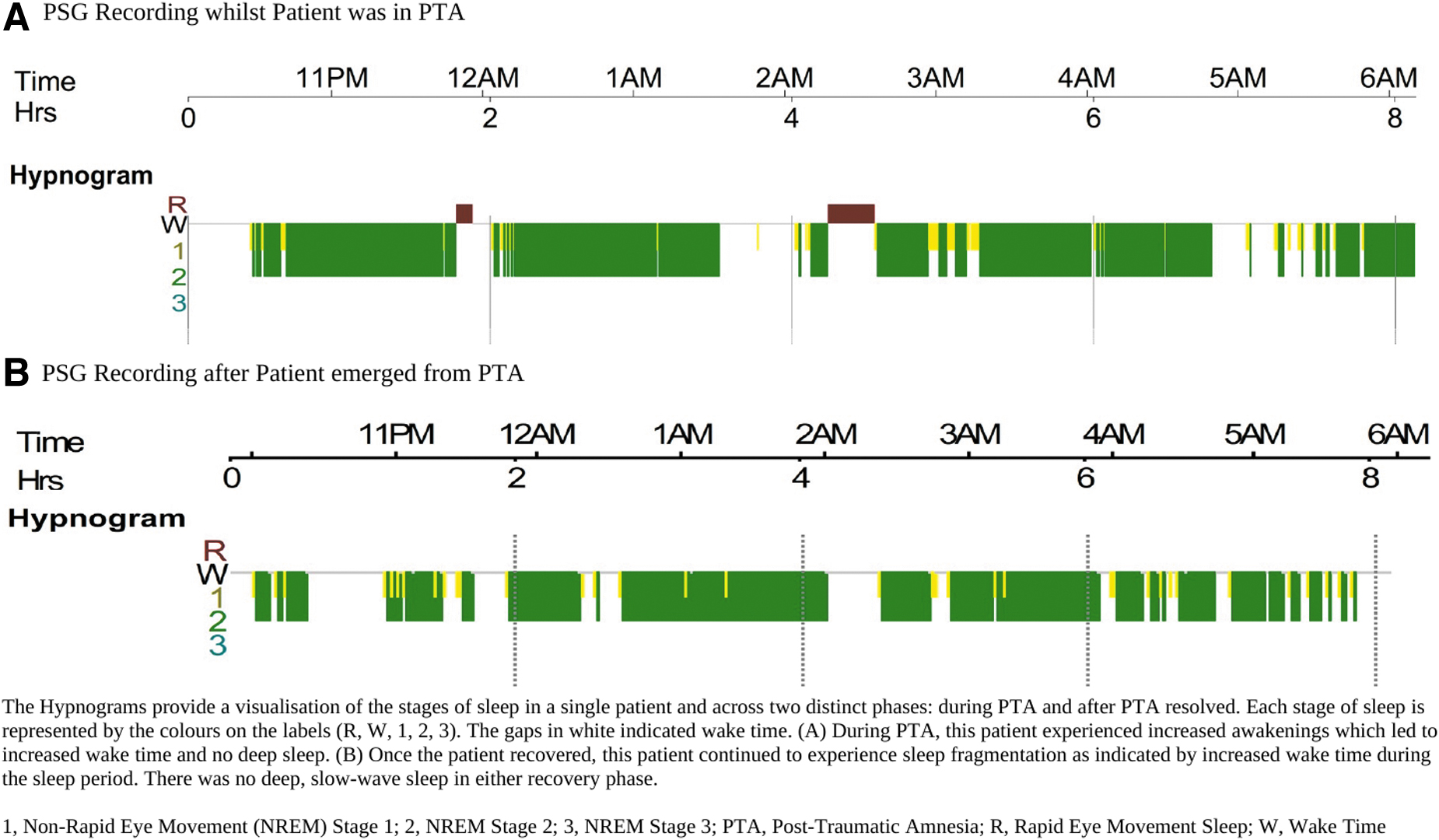
Hypnogram visualisation of sleep (PSG) in a single patient while in PTA and after PTA resolved.
Comparison of Sleep-Wake Parameters in Same Patients between Recovery Stages (n = 11)
Bolded rows indicate statistically significant differences (p < .05).
CI, confidence interval; h, hour; min, minutes; N, number; N1, NREM stage 1; N2, NREM stage 2; N3, NREM stage 3; NREM, non-rapid eye movement; ns, non-significant; PTA, post-traumatic amnesia; REM, rapid eye movement; SD, standard deviation.
Discussion
The present study demonstrated that ambulatory PSG (adherence rate: 63.0%) and endogenous melatonin assessment are feasible for patients experiencing PTA. This study confirmed the results of a preceding pilot study, 4 and reported the disruption to several sleep-wake parameters, sleep macro-architecture, and endogenous melatonin synthesis, which did not meet consensus guideline values for optimal sleep quality 48 or normal reference ranges. 46,47 Patients in PTA displayed sleep-onset difficulties, sleep fragmentation from frequent awakenings, and reduced deep, slow-wave sleep (N3). Melatonin levels at the two time-points were also commonly outside the normal reference ranges. There were relatively low mean agitation levels within the sample, which did not appear to be exacerbated following the incorporation of a non-routine sleep assessment method (PSG). Interestingly, during PTA, there were no statistically significant associations found between cognitive disturbance, agitation, and sleep-wake parameters, apart from N2 sleep (%), in patients with >6 h of PSG. Following the resolution of PTA, patients continued to experience similar sleep disturbances, indicating its long-term impact. The study hypotheses were therefore partially supported, given patients in PTA commonly displayed abnormal melatonin levels and had increased disturbances to certain sleep-wake parameters compared to after PTA resolved. Agitation levels also only appeared to be significantly associated with N2 sleep.
Sleep disturbance is a distinctive feature of PTA
To our knowledge, this is one of the largest studies reporting the feasibility of ambulatory PSG for patients in PTA. Ambulatory PSG permitted sleep monitoring in patients' naturalistic hospital environment (i.e., at rehabilitation bedside). This also overcame the limitations of traditional, laboratory-based, technician-attended PSG, which is comparatively expensive, 49 does not include nursing or resources 49 required for patients in PTA, and can cause a “first night effect” 50 (whereby sleep disturbance is induced by a new environment and/or the awareness of being watched by technicians). Patients displayed significant disruption to sleep continuity measures, which indicated impaired sleep quality 48 (i.e., increased sleep latency, reduced sleep duration, frequent and prolonged awakenings, and poor sleep efficiency). Sleep periods that are highly fragmented and unconsolidated appear to be a distinctive sleep pattern during PTA.
A systematic review similarly reported that most patients in PTA experienced moderate to severe sleep-wake cycle disturbance (described as day-night reversal of sleep-wake cycles, frequent awakenings, decreased night-time sleep, sleepiness, or fragmented sleep). 2 The review also reported that approximately 70.0% of patients in PTA displayed decreased daytime activity (suggesting unconsolidated sleep-wake cycles). In the present study, more than 80% of patients displayed abnormal sleep efficiency (≤ 85%). 48 Poor sleep efficiency during PTA has also been reported in other studies, 3,4 which may be caused by prolonged wakefulness and sleep latency, 51 also common in our sample. Fedele and colleagues reported an arousal index during PTA that was similar to normative values, and it did not appear to accurately reflect the sleep disturbances observed during PTA. 9 In this study, the number of arousals that then transitioned into awakenings was high compared to normative values, and frequent awakenings have also been reported in other studies. 4,9 An index of awakenings is regarded as important for clinical outcomes and is a key indicator of sleep continuity. 37,48 Research has indicated that awakenings cause the greatest sleep disturbance, 52 higher levels of sleep fragmentation, and neurobehavioral deficits. 51,52 Sleep fragmentation can affect the composition of sleep architecture (particularly N3 and REM, 53 also seen in this study), and thereby impact the restorative benefit of sleep.
An important observation was the overall mean reduction of deep, slow-wave sleep when compared to normal values. This is likely the result of increased sleep fragmentation 51 as displayed during PTA. Further, over one-third of the sample were unable to enter N3 sleep. However, future studies with larger samples could evaluate whether this observation is replicated. Low proportions of N3 sleep appear to be specific to early TBI recovery, given increased N3 sleep has been alternatively reported in a chronic TBI sample. 54 Slow-wave sleep is the most restorative sleep stage 55 and it has been associated with several essential cognitive and physiological functions (i.e., learning and memory processes, energy restoration, immune function, and hormone secretion). 56 Insufficient proportions of N3 sleep during PTA could disrupt these processes, which are integral to overall patient recovery. For instance, the emergence from PTA is commonly measured by serial assessments of memory and/or orientation (e.g., WPTAS, the Galveston Orientation and Amnesia Test, or the Orientation Log). 28,57,58 In patients with chronic severe TBI, slow-wave activity (low-frequency brain waves that characterise N3 sleep) 59 was significantly associated with increased next day episodic memory performance. 60
Prior literature has also demonstrated associations between increased sleep quality and both the resolution of PTA (recovery of continuous memory) 3 and improved cognition. 26 In the present study, the WPTAS 28 (a measure of anterograde memory) was not related to sleep-wake parameters. Future studies may incorporate a comprehensive measure of memory and cognitive function. Beyond anterograde amnesia, studies have also reported disturbances to associative memory, information, processing speed, spatial working memory, and personal semantic memory during PTA. 61,62
Abnormalities to endogenous melatonin secretion during PTA
Although melatonin habitually increases at nighttime (i.e., melatonin onset in healthy individuals ranges from 18:13 to 00:26) 38 and declines by morning, this pattern was not observed in most patients in PTA. Mean melatonin levels were instead relatively stable between the two time-points and most patients were outside the normal reference ranges. This suggests that circadian regulation and the timing of melatonin were disturbed. Within the literature, there has been conflicting findings regarding endogenous melatonin rhythms in TBI samples. Duclos and associates reported a relatively comparable melatonin rhythm in terms of its timing and amplitude between patients post-TBI and orthopedic and/or spinal cord injury controls. 19 However, the present findings were aligned with other TBI studies, which reported abnormal melatonin production when compared to controls or normal reference values. 4,13 –16 For instance, Grima and colleagues reported 42.0% less melatonin production post-TBI and delayed DLMO (by approximately 1.5 h) compared to healthy controls. 16
Disturbed melatonin levels could contribute to sleep disturbance, 18 insomnia, 16 and reduced REM sleep. 13 Reduced REM was observed in this study. This study also reported that mean melatonin levels were higher at the second time-point (06:00), which may reflect delayed melatonin secretion. It's probable that head trauma can disrupt brain structures involved in sleep-wake regulation 6,19 and/or circadian signaling (i.e., melatonin synthesis by the pineal gland). 13 There are also other environmental factors that may contribute to delayed and/or lowered melatonin secretion. For instance, melatonin secretion is also tightly attuned to light exposure. 63 Dedicated PTA wards are similar to intensive care settings, and do not always include clear day-night cues 64 (featuring constant dimmed lighting, which could impact melatonin secretion). A central behavioral strategy for PTA management is the provision of a consistent and low-stimulation environment, with flexible sleep opportunities, to minimize patient confusion and agitation. 1 An absence of clear sleep-wake cues and routines within the hospital environment could potentially modify sleep-wake patterns. 6
There is some evidence that sleep hygiene interventions within a TBI rehabilitation unit (i.e., consisting of morning blue-light therapy and limited caffeine intake and daytime naps) led to significant increases in sleep metrics. 65 However, sleep metrics were similar between the intervention and control group, necessitating further research. 65 One randomized controlled trial reported that melatonin supplementation significantly improved sleep quality post-TBI. 66 Melatonin is also recognized for its neuroprotective role for patients (i.e., it can moderate inflammation and cerebral edema post-TBI). 17
For patients in PTA, the use of saliva sampling at two key time-points was a practical, reliable, 11 and non-invasive 67 collection method. Although multiple samples overnight would be required to determine DLMO or peak endogenous melatonin levels, this may be impractical during the confused and agitated PTA phase. Duclos and associates implemented more regular sampling via urinary catheter (e.g., hourly) during early TBI recovery 19 ; however, catheterization during PTA is not routine practice. Frequent sampling of saliva could stimulate patients, 67 exacerbate sleep disturbance, and/or lead to complete sleep deprivation. 11 One study also reported that patient care activities performed by staff overnight were a negative predictor of sleep efficiency in patients with acute TBI. 68 In this study, saliva sampling at two key time-points successfully determined abnormalities to melatonin synthesis in comparison to normative reference ranges.
The relationship between sleep and agitation during PTA
There was a relatively low proportion of patients who were clinically agitated on rehabilitation admission and within the 3 consecutive days surrounding PSG. On the day of PSG, patients primarily displayed impulsivity (52.6% of patients) and decreased attention span/distractibility (47.4%); however, the majority (> 80.0%) were relatively cooperative to hospital care and the study measures. A similar pattern of behavior has also been reported in other acute TBI studies. 69,70 In this study, patients in PTA were able to tolerate the requirements of PSG (adherence rate: 63.0%), and this did not appear to exacerbate patient agitation. In the majority of patients with <6 h of PSG recording, this was mainly due to lost signaling, which is generally common with unattended PSG monitoring (e.g., 3.0–18.0%). 71 This suggests that patients in PTA can tolerate non-routine and tailored additions to their low-stimulation hospital environment (i.e., sleep assessment). Recent PTA management guidelines have also recognized increased patient tolerability, and they now recommend incorporating modified physical therapy. 1
There was a marginally significant association between increased agitation scores and increased N2 sleep (%). It could be conjectured that high agitation led to increased proportions of light sleep (N2), altering the time spent in deep, slow-wave sleep, although further study is required. There were no associations found between patient agitation levels and other PSG-derived sleep-wake parameters, which may be due to the low overall agitation scores. It's probable that a combination of factors beyond agitation is contributing to sleep disturbance during PTA. 6 For instance, Baumann and colleagues reported that brain trauma accounted for sleep-wake disturbance in 43.0% of patients. 72 Prior studies have reported variable clinical agitation frequencies during acute TBI recovery and PTA (8.0–57.0%), 69,70,73,74 which were mainly mild in severity. 70,74 This suggests that agitation is heterogenous, and it highlights the value of evaluating patient-specific behaviors underlying agitation. However, there is some evidence that sleep quality indicators (i.e., sleep time, sleep efficiency) are significantly decreased in agitated patients in PTA compared to non-agitated patients in PTA. 21 A focus on improving sleep during PTA could potentially moderate or resolve both patient agitation and other concerns that have been associated with sleep abnormalities (i.e., decreased rehabilitation participation). 7
The trajectory of sleep disturbance
To our knowledge, this is the first study to monitor the trajectory of sleep disturbances in the same patient group, thus controlling for factors that can influence sleep. Following the resolution of PTA, patients' mean total sleep time significantly improved, and it almost reached the recommendations for sleep in adults (7 to 9 h). 75 During PTA, there were significant disturbances to the composition of sleep, which persisted after the emergence from PTA. During both phases, patients displayed decreased slow-wave (N3) sleep, increased light sleep (N2 sleep), and sleep fragmentation, evidenced by frequent awakenings, increased wake time, and abnormal sleep efficiency.
Limited actigraphy-based studies have also evaluated sleep during both phases, albeit using separate and unmatched patient groups. 2,3,8 Studies have reported improved sleep efficiency 3 and rest-activity cycle consolidation 8 post-recovery from PTA. There is also evidence that PTA symptoms recover in a sequential pattern (i.e., nighttime sleep disturbance and decreased daytime arousal followed by disorientation and agitation). 76 It's possible that these study differences could relate to the limitations of actigraphy during PTA 9 or the study design (i.e., a cohort study can better control for the patient-specific characteristics that influence sleep). 6,77 Nonetheless, this study suggested that sleep disturbances persisted and did not appear to have completely recovered. 2 In the TBI population, there is evidence of long-term sleep disturbance, 78 sleep disorders, 79 and increased sleep needs. 80 Persistent and untreated sleep disturbances can further complicate the management and care for this complex patient population and may affect neuroplasticity (the brain's ability to adapt after trauma). This study therefore supports the routine assessment of sleep disturbance during both phases, which is not routine in clinical practice.
Study limitations and future research directions
A study limitation was that PSG monitoring occurred over one night only. However, the sleep disturbances displayed during PTA were aligned with prior research. 4 Given the symptoms of PTA (i.e., confusion, restlessness, disorientation, memory disturbance), the use of PSG over several nights may be impractical. Actigraphy has been commonly used in PTA, given its low-cost, non-invasiveness, and ability to monitor sleep-wake cycles over prolonged periods. 8 However, there is evidence that actigraphy is not analogous to PSG, and displayed low precision and poor specificity for patients in PTA. 9 In this population, this is likely attributable to actigraphy's mechanism, which relies on movement to estimate sleep. 9 Future studies could focus on improving the degree of concordance between actigraphy and PSG (i.e., through tailored algorithm development).
The PSG channels selected adhered to current guidelines for ambulatory PSG 34 and for determining sleep macro-architecture. There is evidence of sleep disorders post-TBI, 79 and decreased N3 sleep is also a common feature in sleep apnea. 56 The current PSG channels would not permit the diagnosis of sleep disorders; however, future studies could trial additional channels such as finger-probe oximetry. In some patients, the PSG signals were lost or the device was removed. This may have been influenced by patient confusion, restlessness, or short-term memory disturbance. However, data loss is generally common with unattended PSG monitoring (e.g., 3.0–18.0%). 71 The PSG device was removed in the morning after the “lights out” period; however, this likely had a negligible effect on the recorded sleep-wake parameters (e.g., N3 [%] or total sleep time). PSG was recorded for ≥6 h (minimum recommended recording time) 39 to capture a full-night's sleep prior to removing the device, and deep sleep (N3) also mainly occurs within the first third of the evening. 81 In this study, frequent awakenings, and subsequently increased wake time during PTA, likely prevented the proportion of N3 sleep. In addition, early awakenings are a common sleep complaint post-TBI. 79
Two time-points were selected to determine salivary melatonin levels and were compared to normal reference ranges. More frequent sampling (e.g., half-hour or hourly) is required to determine DLMO, which was beyond the aims of this study. However, it's likely that patient confusion and agitation during PTA would preclude compliance for frequent sampling. Although PTA management recommend a low-stimulation environment, 1 patient stress from repeated awakenings, and thus sampling, could also impact melatonin secretion. 82 There was some missing ABS data that related to the practicalities of routine data assessment. However, this did not appear to significantly affect study results given other studies have similarly reported low mean agitation levels during PTA. 74 Sleep disturbance during PTA is likely onset by multiple injury-related, personal (e.g., age) and environmental factors (e.g., noise, light), 6 which were not specifically measured in this study. This could be an area of investigation for further research and to guide treatment protocols. Another limitation was the timing of PSG once patients emerged from PTA (i.e., after 2 weeks). The 2-week period ensured that patients were still inpatients for the repeat PSG. However, it's possible that the nature of sleep disturbance may change with longer follow-up periods. Home PSG studies could be another focus in future research.
Conclusions
This study demonstrated that there are significant disturbances to sleep quality, sleep macro-architecture, and melatonin synthesis in patients experiencing PTA. Ambulatory PSG is a feasible method to evaluate sleep disturbance during PTA, which does not appear to worsen the symptom burden of PTA. Following the recovery from PTA, sleep disturbance persisted, which can potentially protract patient recovery. This study recommends routine sleep assessment early post-TBI and during PTA using gold-standard PSG, to ensure that patients receive appropriate treatment and to mitigate long-term impacts on recovery. Future studies could investigate the effect of environmental or pharmacological treatment (i.e., melatonin supplementation) to normalize sleep during PTA.
Transparency, Rigor, and Reproducibility Summary
This was an observational, cohort study and therefore was not formally registered. The study methodology and data analysis plan were pre-specified and approved by an HREC. Statistical analyses were conducted by the corresponding author and reviewed by a senior biostatistician and co-author. The Results section includes the full details of participant enrollment, including those excluded and missing data. Participant blinding was not included, given there was no control group, and this study incorporated objective sleep assessment methods. Self-report measures were not applicable due to the symptoms of PTA (i.e., confusion, memory disturbance). The Methods section includes details of data acquisition and handling and the equipment sources. Key inclusion criteria that determined the eligibility to participate were evaluated by each patient's treating rehabilitation physician. The statistical analyses were appropriate for the data collected, and they included confidence intervals. A central component of the analyses was the evaluation of correlations. This study did not include multiple comparisons when conducting between-group analyses. This study replicated the methodology of a previous successful pilot study. 4 De-identified data from this study and the associated analytic code are not available in a public archive. The authors agree to provide the full content of the manuscript by contacting the corresponding author.
Footnotes
Acknowledgments
The authors gratefully acknowledge the patients who participated in this study. We thank the Epworth HealthCare TBI Rehabilitation Nursing Team and Dr. Bridget Hill for their assistance with data collection. We also thank Natalie Swaby for analyzing the PSG recordings.
Authors' Contributions
The authors contributed as follows. Bianca Fedele: conceptualization, methodology, formal analysis, investigation, writing–original draft, writing–review and editing, project administration; Gavin Williams: conceptualization, methodology, writing–review and editing, supervision; Dean McKenzie: conceptualization, methodology, formal analysis, writing–review and editing, supervision; Robert Giles: conceptualization, methodology, resources, writing–review and editing; Adam McKay: conceptualization, investigation, resources, writing–review and editing; John Olver: conceptualization, methodology, writing–review and editing, supervision.
Funding Information
This research was supported by the Professor Jack Cade AM Intensivist Major Development Grant from the Epworth Research Institute (ERI) and the Epworth Medical Foundation Grant Family Bequest.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.