
Abstract
Spinal cord injury (SCI) negatively impacts individuals’ functional independence, and motor and sensory function. Intense walking training has been shown to facilitate recovery for individuals with chronic SCI. Powered robotic exoskeletons provide therapists with a tool that allows them to conduct walking training with less therapist effort as compared to conventional walking training. Exoskeletal-assisted walking (EAW) has been studied in the chronic SCI population with preliminary reports showing benefits in mobility, health, and quality-of-life outcomes. However, few reports have studied EAW’s benefits in the acute (<90 days post) SCI population at a time when neural plasticity is most dynamic and modifiable. The purpose of the study was to conduct a pilot randomized controlled trial (RCT) to understand the effects of incorporated EAW in acute inpatient rehabilitation (AIR) for individuals with SCI on functional, motor, and sensory recovery. The study outcomes included the Spinal Cord Independence Measure (SCIM) III and International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) motor and sensory scores that were assessed by unblinded assessors. We also recorded EAW session data, including adverse events, walking and up time, step counts, Borg Rating of Perceived Exertion (RPE), and compliance with scheduled EAW training. From August 2019 to July 2022, 16 participants completed the AIR with incorporated EAW, and 12 completed the standard AIR, all with SCI and preserved leg function within 90 days post-injury. During each session, the AIR with incorporated EAW group averaged 34.3 (±9.4) min of up time, 25.4 (±7.7) min of walk time, and 536 (±157) steps. Analysis via two-by-two mixed-effects models showed significant increases in the SCIM total score and ISNCSCI total motor and sensory scores over time for the AIR with incorporated EAW group [SCIM total score: F(1, 26) = 5.59, p = 0.03; total motor score: F(1, 26) = 8.06, p < 0.01; total sensory score: F(1, 19.2) = 5.08, p = 0.04], outperforming the standard AIR group. The AIR with incorporated EAW group showed 13, 14, and 22 points higher changes in the SCIM total score, total motor score, and total sensory score (respectively) by discharge compared with the standard AIR group. Incorporating EAW into AIR may facilitate functional, motor, and sensory recovery for individuals with SCI during AIR better than standard AIR. However, the study had a limited sample size. Further studies are needed to clarify the effects of EAW in AIR.
Introduction
For people with spinal cord injury (SCI), the ability to walk and the restoration of bowel and bladder function consistently rank among the highest priorities for recovery. 1,2 Walking is one of the most important training strategies for SCI rehabilitation. Previous studies have shown that intense walking training improves walking function for individuals with incomplete SCI 3 –5 and is associated with improvement in bowel and bladder function for people with chronic SCI. 6,7 Walking and standing also help prevent pressure injuries and improve self-esteem, blood circulation, and daily living independence. 8,9
About 80% of American Spinal Injury Association (ASIA) Impairment Scale (AIS) conversions occur within 100 days post-SCI. 10 –13 Of those individuals with AIS grade B at one year post-SCI, only 16% convert to AIS grade C or D by five years post-injury. 14 Results from previous studies support that rehabilitation in the acute/subacute phase of SCI is critical because it can exploit a heightened level of neural plasticity before neuronal degeneration and muscle atrophy occur. 15,16
Combining locomotor training and acute inpatient rehabilitation (AIR) has the potential to improve functional and motor recovery through neuroplasticity. 17,18 However, applying intensive walking training during AIR for individuals with SCI is difficult because of the need for several clinicians working together to assist with leg advancement, weight shifting, trunk stability, and preventing knee buckling. 19,20 Patients in AIR have busy training and examination schedules, thereby reducing the amount of time available for walking training. Lower extremity-powered exoskeletons are a technology that can offer upright, weight-bearing overground locomotion for people with SCI who would ordinarily be unable to or would need assistance to walk. Exoskeletal-assisted walking (EAW) training can be performed using less effort than would typically be used during conventional gait training that requires manually facilitated gait movement and trunk control. 19 –21 After EAW training, previous studies have shown that individuals with chronic SCI have better cardiovascular and bowel functions 22,23 and improved body composition. 24,25 However, there are limited studies related to the effects of EAW training during AIR. 26,27
Our previous studies of individuals with acute/subacute SCI showed that incorporating EAW training into an AIR program (AIR with incorporated EAW) was safe and feasible 26 and had the potential to foster greater improvements in functional and motor recovery compared to a standard of care AIR (Standard AIR) 27 These results were limited because of the small sample size and potential selection bias due to the lack of a prospectively randomized comparison group. Our previous studies did not investigate the effects of EAW on sensory recovery, which is essential for movement recovery and the generation of precise movement. 28 Therefore, the purpose of this study was to conduct a pilot randomized controlled trial (RCT) to determine the effects of AIR with incorporated EAW compared with Standard AIR on accelerating functional, motor, and sensory recovery during AIR for inpatients with SCI who have preserved lower extremity motor function [i.e., a lower extremity motor score (LEMS) of at least 1.0]. We hypothesized that individuals with SCI who undergo AIR with incorporated EAW would have better functional, motor, and sensory recovery than those who would undergo Standard AIR.
Methods
Study design and setting
A prospective, two-group, pilot RCT in individuals with acute SCI and preserved lower extremity motor function was conducted. Prospective participants were recruited following admission to our hospital’s AIR unit. After completing the consent process and screening, eligible participants were randomly assigned to either the AIR with incorporated EAW or Standard AIR group via a computer-generated allocation table using a simple 1:1 randomization method. Physicians and therapists who performed pre-screening and screening of potential participants did not have access to the computer-generated allocation table used in the randomization procedure and therefore remained blinded to the randomly assigned group membership. However, once a participant began their EAW with incorporated AIR training, it was difficult for the clinicians to remain blinded due to the visibility of the training. After an interim analysis for the second annual report, we modified the randomization to a 2:1 ratio to accommodate participants’ and therapists’ satisfaction and cooperation (see Discussion). All study procedures were conducted in an SCI AIR facility within the same hospital and were approved by the hospital’s Institutional Review Board (STUDY-19–00614). The study was registered on the clinicaltrial.gov website (NCT04221373).
Inclusion/exclusion criteria
Table 1 indicates the inclusion/exclusion criteria for the study. Eligible participants were adults admitted to SCI AIR within 3 months post-injury 13,29,30 who were eligible for locomotor training with enough hand function to partially manage a walking aid. Participants need to use a walking aid to walk in the EksoGT to maintain dynamic balance while walking. The criterion for within 3 months post-injury was to reduce the variability of natural recovery speed among our participants. Eligibility for locomotor training included having an LEMS greater than or equal to 1.0 or a neurological level of injury (NLI) at or below T10. 31
Eligibility Criteria
SCI, spinal cord injury.
Intervention
Both groups received 15 hours of AIR therapy per week, which included physical therapy (PT) and occupational therapy (OT) for bed mobility, seated and standing balance, strength, gait, transfers, and wheelchair mobility training to improve participants’ independence in activities of daily living (ADLs). The AIR with incorporated EAW group received EAW training for overground walking utilizing a powered exoskeleton (EksoGT, Ekso Bionics, Inc.)a as part of a minimum of their 15 hours per week of AIR therapies. 26 The EksoGT-powered exoskeleton is an FDA-cleared device for performing ambulatory functions in rehabilitation institutions [510(k) number K143690] and allows persons with higher-level injuries to use an exoskeleton due to the trunk support provided by the device. In addition, the EksoGT is designed to be adjusted between patients, making it a more feasible device to use in a clinical rehabilitation setting. The Standard AIR group received the same amount of AIR therapies incorporating walking with the use of parallel bars, a treadmill with an overhead lift, and ceiling track (Guldmann Inc., Tampa, Florida)b, or a body-weight support device on wheels (LiteGait, Mobility Research, Tempe, Arizona)c. Both groups also had the same discharge criteria. Participants would be discharged from AIR when they had achieved the functional mobility and performance of ADLs goals set by the clinicians or when their progress in reaching those goals had reached a plateau.
The EAW training for the AIR with incorporated EAW group started from the earliest time that participants were identified by the clinicians with the ability to safely stand, without severe symptomatic orthostatic hypotension (OH) or severe pain, and continued through the AIR period. EAW sessions included device fitting and walking training protocols developed by Asselin et al. 32 using EksoGT’s total or variable device assistance modes. In the first few EAW sessions, participants walked with 100% device assistance. Once participants were familiar with EAW, for example, by reaching 300 steps within one session, therapists reduced the device assistance based on participants’ ability to walk. The target of decreasing the device assistance level was to make participants feel somewhat hard to very hard exertion during EAW training [Borg Rating of Perceived Exertion (RPE) rating = 12 to 17, Borg RPE ranges from 6 to 20, with 6 indicating very light exertion and 20 indicating maximum exertion]. 33 –35 We aimed to provide two to three 1-hour sessions of EAW training per week until discharge. Our therapists sometimes would transition from EAW training to overground walking in parallel bars or with a body weight support system during the last 10 min of an EAW training session. The total duration of each walking session remained constant at 1 hour. In this way, we could see if the effects of EAW training carried over to affect overground walking without using an exoskeleton.
Outcome assessments
The total score of the Spinal Cord Independence Measure III (SCIM III), ranging from 0 to 100, was the primary outcome measure assessing functional independence. 36 –38 The SCIM III can be divided into three subscales: self-care, respiration and sphincter (R&S) management, and mobility. A higher final score indicates more independence. The SCIM version III has high reliability and sensitivity to functional changes for people with SCI. 38
Motor and sensory functions were assessed using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) to determine the total motor score (TMS, ranging from 0 to 100), upper extremity motor score (UEMS, ranging from 0 to 50), LEMS (ranging from 0 to 50), total light touch score (TLTS, ranging from 0 to 112), total pin prick score (TPPS, ranging from 0 to 112), and total sensory score (TSS, ranging from 0 to 224). 39 –41 In this study, the SCIM scores, TMS, UEMS, LEMS, TLTS, TPPS, and TSS at admission were compared with those scores at discharge from AIR. These scores were also compared between the AIR with incorporated EAW group and the Standard AIR group.
This study was conducted in a hospital AIR setting (not a laboratory setting), where the SCIM III and ISNCSCI assessments were performed as the standard of care assessments. The assessors were the participants' therapists, nurses, and physicians, who provided daily care. Therefore, none of the assessors were blinded to the group assignments of the participants in this study.
Age, sex, days of inpatient stay (DIS), SCI etiology, AIS, and NLI for participants from both groups were recorded. For the AIR with incorporated EAW group only, the number of EAW sessions performed, adverse events, Borg RPE at the beginning, middle, and end of EAW, total steps, and total up and walk times in each EAW session were recorded. We only reported study-related adverse events in this article, which are defined as any unfavorable or unintended symptom, or disease temporally associated with the study interventions (EAW training). Compliance with completing scheduled EAW training was defined as the number of EAW training sessions completed as a percentage of scheduled training sessions, and the reasons that lead to the training being rescheduled or suspended were recorded.
Statistical analysis
All statistical analyses were performed using SPSS version 17.d Descriptive statistics were reported for demographic information, SCI characteristics, and primary and secondary outcomes. Because of the small sample size and uneven number of participants between the AIR with incorporated EAW and the Standard AIR groups, Mann-Whitney U tests were used to compare the baseline data between the two groups for age, DIS, ISNCSCI, and SCIM scores at admission. Variables with significant differences in baseline data between the two groups were added as covariates in subsequent analyses if the factor had a significant association with the outcome. Chi-square was used to compare the differences in sex, SCI etiology, baseline NLI, and baseline AIS between the two groups. All statistical tests were two-sided with the alpha set at 0.05. The Shapiro-Wilk test was used to test if the outcomes were normally distributed. Two-way group (AIR with incorporated EAW vs. Standard AIR) by time (baseline, discharge) mixed-effects models were used to examine outcomes, including the SCIM total score (primary outcome and analysis), SCIM subscale scores, and ISNCSCI TMS, UEMS, LEMS, TLTS, TPPS, and TSS. Fixed effects included the main effects of group assignments and time and an interaction effect of group by time. A random effect included individual participants. A covariate, baseline SCIM total score, was included in these mixed-effect models because there was a significant baseline difference in SCIM total score between the two groups (see Results and Table 2). The assumptions of a mixed-effects model, including the normal distribution of the residuals and random effect coefficients, were examined by assessing the histograms of residuals. A previous study showed that mixed-effects models are robust to the violation of the distributional assumptions. 42 Mean between-group difference for each outcome and their 95% confidence interval (CI) were calculated as well. Post hoc power analyses for the group comparisons on each outcome were calculated using each group’s outcome changes between admission and discharge, with the alpha set at 0.05.
Participants’ Demographic and Sci Characteristics and The Results of Baseline Comparisons
Results were reported as mean (±SD). p values were calculated using the Mann-Whitney Test for continuous variables and chi-square statistic for categorical variables.
p < 0.05, statistical difference.
AIR, acute inpatient rehabilitation; AIS, ASIA Impairment Scale; EAW, exoskeletal-assisted walking; LEMS, lower extremity motor score; NLI, neurological level of injury; SCIM, spinal cord independence measure; SD, standard deviation; TLTS, total light touch score; TPPS, total pin prick score; UEMS, upper extremity motor score.
Results
Participants
This report followed the guidelines of the Consolidated Standards of Reporting Trials (CONSORT guideline, Fig. 1). During the funding period from August 1st, 2019, to July 31st, 2022, we had 48 potential participants admitted to our inpatient unit. Fifteen of them were pre-screening failures (31%) due to progressive SCI (n = 3), the ability to independently walk (n = 4), weight greater than the EksoGT upper limit (n = 4), severe pain (n = 1), insufficient hand function (n = 1), and pressure injuries at contact points with the EksoGT (n = 2). One person declined enrollment due to a lack of interest. A total of 32 participants were enrolled in the study (Fig. 1). Twenty participants were assigned to the AIR with incorporated EAW group and 12 in the Standard AIR group. Four participants in the AIR with incorporated EAW group were withdrawn from the study and not included in data analysis due to the temporary suspension of the study during the beginning of the COVID-19 pandemic (n = 1), severe upper extremity pain while using a walker during EAW (n = 1), severe OH during EAW (n = 1), or severe psychosocial issues (n = 1), respectively (attrition rate = 12.5%) (Fig. 1). Therefore, 16 participants in the AIR with incorporated EAW group and 12 in the Standard AIR group completed the study. Baseline age, etiology, NLI, AIS, age, inpatient stay days, UEMS, LEMS, TMS, TLTS, TPPS, TSS, and SCIM mobility scores were not significantly different between the two groups, but the AIR with incorporated EAW group had a significantly lower baseline SCIM total score (18.6 ± 6.4) than the Standard AIR group (27.0 ± 12.3) (Table 2).
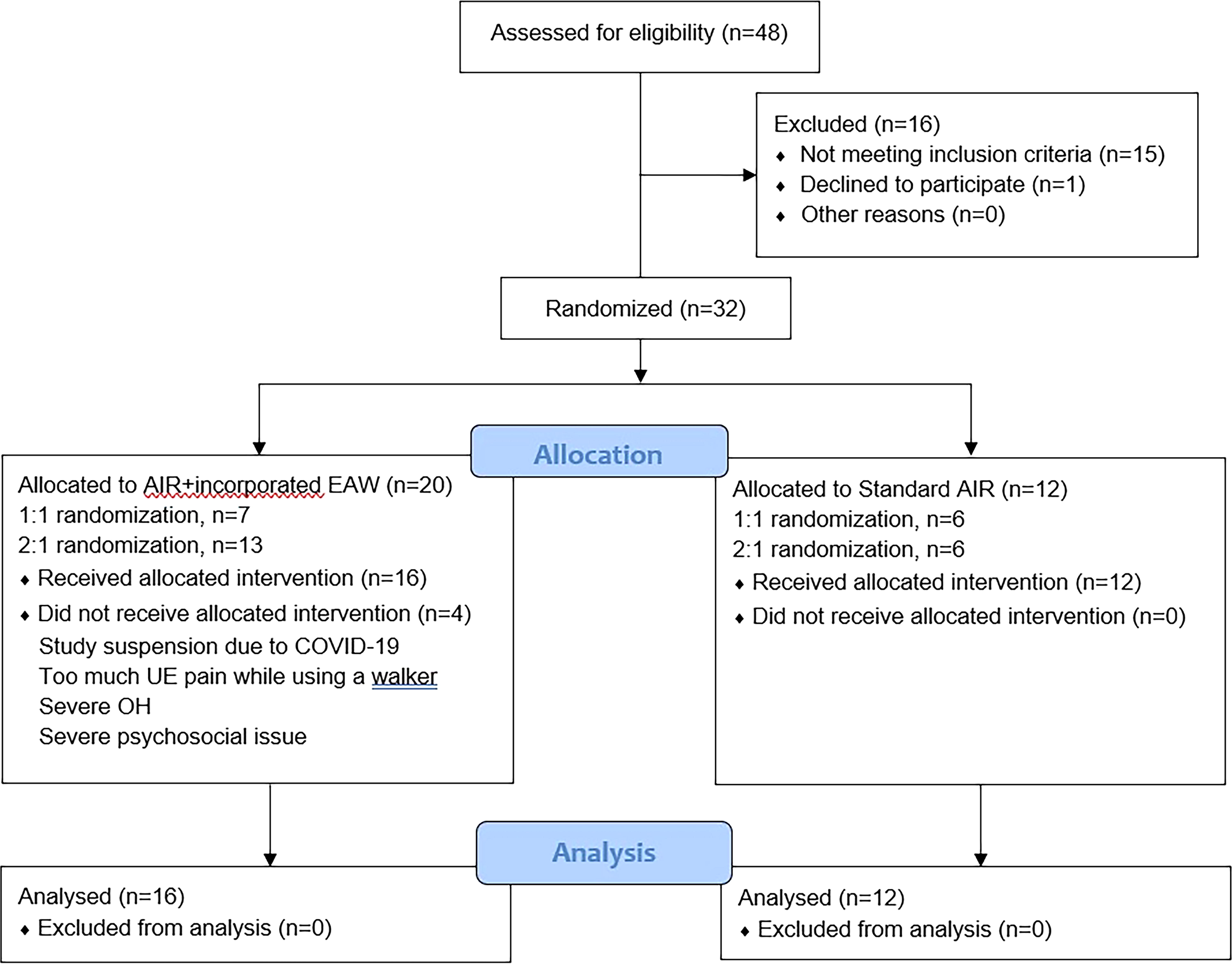
Study consort diagram. AIR, acute inpatient rehabilitation; EAW, exoskeletal-assisted walking; OH, orthostatic hypotension; UE, upper extremity.
EAW training sessions
The 16 participants in the AIR with incorporated EAW group completed 147 out of the 183 scheduled sessions of EAW training, resulting in a compliance rate of 80%. The 36 sessions that our participants missed were due to scheduled surgical interventions or exams (13 sessions), participant sickness (14 sessions), participant rejection (2 sessions), lack of an EksoGT trainer (2 sessions), and device malfunction issues (5 sessions). Five adverse events were reported. One participant had right trochanteric bursitis after his 8th EAW session. One participant had severe OH on his 10th session of EAW training due to the participant forgetting to take the prescribed blood pressure (BP) medications that morning. One participant had left-hand numbness for two nights after his 12th EAW training session. These issues were resolved after these participants took prescribed medications. Two device malfunction-related events happened during this three-year project. One event occurred when the EksoGT fell backward and hit the ground while we were transferring a participant out of the device. The participant did not have any injuries, but it took two weeks to fix the device, which caused us to miss four EAW sessions. The other event occurred due to a controller malfunction, which took four days to fix and caused us to miss one EAW session.
The participants in the AIR with incorporated EAW group had an average of 9 (±4) sessions of EAW training during their AIR stay. Their average stand time and walk time were 34.3 (±9.4) and 25.4 (±7.7) minutes, respectively, with an average of 536 (±157) steps per session during their inpatient stay. At the end of each EAW training session, participants’ average Borg RPE was 14 (±2), which indicated that they felt it was more than somewhat difficult to complete the EAW training session.
Outcome assessment results
Primary outcome
There was a significant main effect of time in the SCIM total score [F(1, 26) = 117.78, p < 0.01]. Participants had significantly higher SCIM total scores at discharge compared with the scores at admission (Table 3 and Fig. 2A).

The group comparisons for each assessment outcome:
The Study Groups’ Assessment Outcomes at Admission and Discharge from Acute Inpatient Rehabilitation and The Results of Statistical Comparisons and the Post Hoc Power Analyses
Results were reported as mean (±SD, [95% CI]). p values were calculated using a mixed-effects model. Post hoc power was calculated using the group count, means, and SD for each outcome variable from a web-based calculator.
p < 0.05, significant statistical difference in interaction effect.
AIR, acute inpatient rehabilitation; AD, admission; bw, between; CI, confidence interval; DC, discharge; EAW, exoskeletal-assisted walking; LEMS, lower extremity motor score; MBGD, mean between-group differences; R&S, respiration and sphincter; SCIM, spinal cord independence measure; TMS, total motor score; TLTS, total light touch score; TPPS, total pin prick score; TSS, total sensory score; UEMS, upper extremity motor score.
There was also a significant treatment group-by-time interaction effect in the SCIM total score [F(1, 26) = 5.59, p = 0.03]. The pattern of improvement in the SCIM total score between admission and discharge was significantly different between the AIR with incorporated EAW and Standard AIR groups, which was in favor of the AIR with incorporated EAW group (Table 3; Fig. 2A). Changes in the SCIM total scores between admission and discharge were approximately 13 points (95% CI [1.7, 24.1]) higher in the AIR with incorporated EAW group compared with the Standard AIR group (Table 3). The post-hoc power for the comparison between the two groups on the SCIM total score changes between admission and discharge was 64.7%.
Secondary outcomes
There were significant main effects of time in all the secondary outcomes [SCIM self-care score: F(1, 26) = 83.58, p < 0.01; SCIM R&S score: F(1, 26) = 72.49, p < 0.01; SCIM mobility score: F(1, 26) = 111.75, p < 0.01; LEMS: F(1, 26) = 33.29, p < 0.01; UEMS: F(1, 26) = 15.34, p < 0.01; TMS: F(1, 26) = 38.91, p < 0.01; TPPS: F(1, 20.7) = 10.53, p < 0.01; TSS: F(1, 19.2) = 8.30, p = 0.01) besides TLTS F(1, 26) = 4.14, p = 0.05]. Participants had significantly higher SCIM and ISNCSCI scores, besides TLTS, at discharge compared with the scores at admission (Table 3 and Figs. 2A, B, and C).
There were significant treatment group by time interaction effects in the SCIM R&S scores [F(1, 26) = 8.02, p = 0.01], LEMS [F(1, 26) = 5.82, p = 0.02], UEMS [F(1, 26) = 4.58, p = 0.04], TMS [F(1, 26) = 8.06, p < 0.01], TLTS [F(1, 21.7) = 6.23, p = 0.02], and TSS [F(1, 19.2) = 5.08, p = 0.04]. The patterns of improvement in SCIM R&S score, LEMS, UEMS, TMS, TLTS, and TSS from admission to discharge were significantly different between the AIR with incorporated EAW and Standard AIR groups, which were in favor of the AIR with incorporated EAW group (Table 3 and Figs. 2A, B, and C). Changes in SCIM R&S score, LEMS, UEMS, TMS, TLTS, and TSS between admission and discharge were approximately 7, 9, 5, 14, 12, and 22 points higher, respectively, in the AIR with incorporated EAW group compared to the Standard AIR group (Table 3). The post-hoc powers for the comparisons between the two groups on SCIM R&S score and TMS changes between admission and discharge were 83.1% and 93.5%, respectively.
Discussion
The study results indicated that incorporating EAW training into Standard AIR is feasible, safe, and more effective than Standard AIR alone in facilitating functional, motor, and sensory recovery for individuals with acute/subacute SCI and preserved lower extremity motor function. The study results were consistent with the results of our and others’ pilot studies. 27,43
An AIR setting has a complex and compact schedule requirement, which includes multiple exams, multiple therapies, sometimes additional surgical procedures, wheelchair fittings, and family meetings. Even with these barriers due to the nature of AIR, we still had a compliance rate of 80% with completing scheduled EAW training during AIR. The advanced preparation for EAW in AIR can improve the compliance rate, such as asking participants to complete their bowel routine before training, prescribing prophylactic anti-hypotension medication, and performing routine device maintenance with a service contract. However, the device price, service contract, and cost for training and certifying therapists to use EksoGT are very high for a rehabilitation institution, which can be another limitation for EAW training and may lead to missing EAW sessions.
Most previous studies suggested high-intensity walking training and three to five EAW training sessions per week for individuals with chronic SCI. 23,34,44 –46 This current study targeted individuals with acute/subacute SCI during AIR, which needs to include the other components of a comprehensive AIR program, such as training in ADLs, transfers, toileting, bed and mat mobility, etc. Another consideration is the need to prevent participants from becoming overly fatigued or developing musculoskeletal injuries from overtraining. Based on the study results, two to three EAW sessions per week is a feasible and effective dose of EAW training during AIR.
While walking in an exoskeleton, people with SCI stand upright with full weight bearing through the feet 47 and walk while activating the trunk and upper and lower limb muscles. This could provide whole-body sensory stimulation. 48 EAW training also meets three important motor learning principles that could promote activity-dependent plasticity: practice, specificity, and effort. 48,49 Individuals with SCI can achieve more overground steps 19,21,43 during EAW training than during conventional walking training because the exoskeleton device can provide proper assistance to advance users’ legs automatically during overground walking. Our study results showed that our participants could complete more than 500 steps during 25 min of EAW. EAW is also a form of overground walking training, not walking training on a treadmill, which has been shown to be less effective at increasing walking distance and speed for individuals with SCI than overground walking. 50,51 This investigation and other previous studies show that participants’ Borg RPE can reach 14–15 during EAW training, 21,52 which indicates that participants exerted a high level of effort in the training. Previous studies also showed that intensive task-specific training has the potential to increase presynaptic inhibition in individuals with chronic SCI that leads to decreased co-contraction between knee and ankle antagonistic muscles. 53,54 By combining all the benefits mentioned above, EAW training may be able to facilitate improvements in neural connectivity in the motor centers. 55 Previous studies have shown that after EAW, individuals with chronic SCI have less spasticity and better walking ability, including improved walking speed, endurance, and step length. 23,56 According to a previous study, a change of 10 points in the SCIM total score represents a substantial and clinically significant improvement in functional ability. 57 In this current study, the AIR with the incorporated EAW group improved by more than 12 points on the SCIM total score during AIR compared to the Standard AIR group (Table 3), indicating that EAW led to a substantially better functional improvement than Standard AIR. The AIR with incorporated EAW group had 9 and 14 points greater changes in LEMS and TMS than the Standard AIR group, respectively. Besides, the study showed that the AIR with incorporated EAW group had greater sensory improvement compared to the Standard AIR group, which has been rarely reported in other studies. These results highlighted the benefits of EAW training during AIR.
EAW training provides psychological benefits for individuals with SCI. During EAW training, individuals with SCI stand upright, walk indoors and/or outdoors, and talk with friends and family at the same eye level. 20,58 This provides them with improved self-confidence, self-esteem, hope, and motivation. 20,58 Individuals in AIR after SCI from this current and previous studies have remarked that walking training facilitated with technology could result in both psychological and physical benefits. 20 Motivation is important for promoting recovery, especially during AIR, which can push individuals with SCI to accept intense training that leads to better recovery. 59 –61 A previous study indicated that about 75% of study participants with SCI want to use an exoskeleton. 62 Our study participants and therapists also reported a strong preference to incorporate EAW training into their AIR program. The participants in the Standard AIR group often expressed disappointment about missing the opportunity to use a powered exoskeleton while seeing others in EAW training and expecting to have similar training. 19 Our therapists preferred to conduct EAW training rather than facilitated overground training due to the need for fewer staff and usually allowed participants to take more steps than they would during conventional gait training. 19,20 Therefore, the randomization ratio was modified after an interim analysis to increase our therapists’ satisfaction and participants’ chances to undergo EAW training.
Study limitations
The results may not be generalizable because of the small sample size. However, the study results were consistent with previous studies. 55,56,63 This study did not have a control group of no rehabilitation training to represent and compare natural recovery results but did include an active treatment group (the Standard AIR group) to show that incorporating EAW into AIR could have superior effects compared to standard AIR alone. Theoretically, randomization would evenly distribute known and unknown confounding factors, including the differences in natural recovery among participants, across groups as well. Besides, other than the overall AIR time being the same, an accurate comparison of walking training dose between the two study groups was not able to be performed because we did not collect walking training data in the Standard AIR group. We acknowledge that it is possible that the better improvement in the AIR with the incorporated EAW group was due to the higher walking training dose, i.e., longer walking time, more walking steps, or more frequent walking sessions that can be provided by EAW. Conventional walking training may reach the same walking training dose as EAW training. However, it will require significant clinicians’ effort (2 to 3 therapists or assistants per session) and be less comfortable for the patients/participants with the harness system of the body weight support system or irideal gait pattern (i.e., hyper-extension knees). The learning curve for therapists to use the exoskeleton or for participants to walk was not a factor since our therapists had more than five years of experience with EAW; all participants received training of comparable quality. The change in the randomization ratio, the interim analysis in the 2nd year of this 3-year study, and the limited sample size that failed to reach the target sample size contributed to most outcomes being underpowered (Table 3). However, the results of the SCIM R&S management score and TMS did reach higher than 80% power.
This current study investigated the short-term effects of EAW training on functional, motor, and sensory recovery in individuals with acute SCI and spared lower extremity motor function. The residual effects at a long-term follow-up visit, such as a one year follow-up, or the effects of continued outpatient EAW training would be outcomes in the next investigation. The changes in AIS score and NLI could be other potential outcomes for future studies. Neurophysiological outcomes, such as corticospinal connectivity, were not assessed. As such, the neural mechanism and benefits of EAW training remain unknown. The assessors in the study were the participants’/patients’ actual healthcare providers in the AIR unit of the hospital, making it difficult to blind them from the participants’ group assignments. Due to limited funding for this study, it was not possible to hire an outside blinded assessor. We recognize this as a limitation and plan to budget for this position in a future RCT.
Conclusion
The study results suggested that incorporating EAW into AIR facilitated functional, motor, and sensory recovery for individuals with SCI and preserved lower extremity motor function better than standard of care AIR. Proper communication and preparation between patients and clinicians, flexible schedule adjustments, and motivation to use EAW during therapy by both patients and clinicians are keys to successfully incorporating EAW into AIR. EAW is a therapeutic treatment that could be utilized to help maximize patients’ recovery during AIR while reducing therapists’ workloads. We will need more studies to further understand the effects and neurophysiological mechanisms of EAW training during AIR.
Transparency, Rigor, and Reproducibility
This study was registered and posted on the Clinicaltrial.gov website (NCT04221373) three months after the study began due to the preparation of posting materials and the internal review process of our institution. Our original sample size target was 30 individuals (1:1 randomization ratio) based on a power analysis utilizing our previous pilot data (which were published 27 ) to provide the study with a statistical power of 80% for the detection of an effect size (Cohen’s d) of 1.07 for the primary outcome measure. The randomization ratio was modified following an interim analysis for the second annual report to the funding agency, resulting in an increase in the target sample size to at least 36 individuals for 80% power (2:1 randomization ratio). The study was terminated at the scheduled end of the three-year funding period. The COVID-19 pandemic impacted study enrollment. The target sample size was not achieved. The available data were used in the analyses. We had pre-screened 48 potential participants admitted to our inpatient unit. Fifteen of them were pre-screening failures (31%). One person declined enrollment due to a lack of interest. A total of 32 participants were enrolled in the study (Fig. 1). All participants were assigned to the AIR with incorporated EAW group or the Standard AIR group via a computer-generated allocation table. Twenty participants were assigned to the AIR with the incorporated EAW group, and 12 were assigned to the Standard AIR group. Four participants in the AIR with incorporated EAW group were withdrawn from the study and not included in the data analysis (Fig. 1). Therefore, 16 participants in the AIR with incorporated EAW group and 12 in the Standard AIR group completed the study. Participant and outcome assessor blinding were not fully possible because of the nature of the therapeutic intervention. The primary outcome measure, SCIM version III total score, is standard in the field, with high reliability and sensitivity to functional changes for people with SCI. 38 The statistical tests used were based on the assumption of a normal distribution of the primary outcome. The findings have not yet been replicated or externally validated. De-identified data from this study are not available in a public archive yet. De-identified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Suppliers
EksoGT, Ekso Bionics, Inc., 101 Glacier Point, Suite A, San Rafael, CA 94901
Guldmann Inc., 14401 McCormick Dr., Suite A, Tampa, Florida 33626
LiteGait, Mobility Research, P.O. Box 3141, Tempe, Arizona 85280
SPSS Inc., 233S. Wacker Drive, 11th Floor, Chicago, Illinois 60606
Footnotes
Authors’ Contribution
C.-Y.T., T.N.B., and A.M.S. collaborated on the conception and design of the study. C.-Y.T., W.J.W., N.M., and V.H. significantly contributed to the data collection. C.-Y.T. was responsible for data analysis for this article. All authors assisted with interpretation of the results. C.-Y.T., T.N.B., and A.M.S. contributed to the writing and revising process.
Funding Information
The study was made possible in part by grants from New York State Department of Health (
Author Disclosure Statement
None of the authors have a financial or other relationship that might lead to a conflict of interest concerning the publication of this article or the research described. All participant consent forms have been collected.