
Abstract
The existing research on the microstructural alterations associated with sport-related concussions (SRCs) has primarily focused on deep white matter (DWM) fibers, while the impact of SRCs on the superficial white matter (SWM) and gray matter (GM) remains unknown. This study aimed to characterize the altered metrics obtained from neurite orientation dispersion and density imaging (NODDI) in boxers with SRCs, and thereby determine whether distinct regional patterns of microstructural alterations can offer valuable insights for accurate diagnosis and prognosis. Concussed boxers (n = 56) and healthy controls (HCs) with typically developing (n = 72) underwent comprehensive neuropsychological assessment and magnetic resonance imaging (MRI) examinations. The tract-based spatial statistics approach was used to investigate alterations in the DWM and SWM, while the gray matter-based spatial statistics approach was used to examine changes in the GM. The median time from the last SRC to MRI in the SRC group was 33.5 days (interquartile range, 45.25). In comparison with HCs, the SRC group exhibited lower fractional anisotropy (FA), neurite density index (NDI), and isotropic volume fraction (ISOVF), as well as higher mean diffusivity, axial diffusivity (AD), and radial diffusivity in both the DWM and SWM. Moreover, the SRC group exhibited lower FA, NDI, orientation dispersion index, and ISOVF in the GM, as well as higher AD. The altered microstructure of both gray and white matter was found to be associated with deficits in working memory and vocabulary memory among boxers. In addition to characterizing the DWM impairment, NODDI further elucidated the effects of SRCs on the microstructure of GM and SWM, offering a reliable imaging biomarker for SRC diagnosis and shedding light on the pathophysiological changes underlying SRCs.
Introduction
Sport-related concussion (SRC) is a frequent injury that affects millions of individuals annually and has garnered significant public attention. 1 Boxing is a common cause of SRCs, with boxers frequently experiencing numerous concussions and sub-concussions that result in substantial neurological damage throughout their careers. 2 The repetitive heavy impact of punches to the boxer’s head can induce linear or rotational acceleration, leading to distortion, stretching, and potential rupture of the white matter, 3 followed by progressive pathological changes. 4 Unlike injuries in adults, injuries sustained by young athletes participating in contact sports can affect the brain development trajectory, resulting in long-term adverse effects. 5 Thus, research focusing on the effects of these injuries on young athletes is necessary to minimize the adverse consequences of SRCs.
Because of limitations in scanning protocols and post-processing techniques, most previous studies primarily focused on the deep white matter (DWM), often neglecting damage to the superficial white matter (SWM) and gray matter (GM). The SWM, which is located at the subcortical gray–white matter junction region, constitutes approximately 57% of all white matter fibers and plays a crucial role in processing speed, attention, and working memory. 6 Injured SWM fibers at the gray–white matter interface have been recorded in autopsy findings after traumatic brain injury. 7 Furthermore, the potential for injury or “bruising” in the GM areas of the brain after mild traumatic brain injury (mTBI) is another important factor worth consideration. 8 Studies on brain morphometry have shed light on the chronic effects of mTBI, which typically manifest as cortical thinning in regions susceptible to Alzheimer’s disease and accelerated age-related cortical thinning. 9,10 However, the underlying SRC-induced GM microstructural alterations may occur long before measurable morphological alterations are detected. Given the irreversible nature of neuronal loss, reliable early detection of gray and white matter damage in individuals sustaining SRC is crucial for evidence-based treatment strategies in concussed athletes.
The absence of evidence for brain injury in conventional magnetic resonance imaging (MRI) has led to the development of more refined approaches. One such approach is diffusion MRI, which offers distinctive insights into brain microstructural alterations by quantifying the diffusion patterns of water molecules within the tissue. 11 The diffusion tensor imaging (DTI) model has been extensively used for investigating the microstructural properties of the DWM in SRC. 12 However, DTI is constrained by the Gaussian model and shows limitations in analyzing the intricacy of white matter as well as cortical GM microstructure. 13 Neurite orientation dispersion and density imaging (NODDI) models segregate signals generated by three distinct tissue compartments: intracellular water, extracellular water, and cerebrospinal fluid, offering protocols for complex pathological changes in dendrites and axons. 14 Both DTI and NODDI metrics can be derived from NODDI scans, and alterations in these diffusion metrics may indicate disruption of the microstructural barrier. A DTI study conducted by Transforming Research and Clinical Knowledge in Traumatic Brain Injury revealed that at 2 weeks and 6 months post-injury, individuals with traumatic brain injury exhibited higher values of axial diffusivity (AD), mean diffusivity (MD), and radial diffusivity (RD), as well as lower values of fractional anisotropy (FA) in most major white matter fiber tracts within the cerebral hemispheres in comparison with controls. 15 In addition, a longitudinal study conducted using NODDI demonstrated a progressive reduction in the neurite density index (NDI) and isotropic volume fraction (ISOVF) within white matter fiber tracts. 16 However, to date, limited studies have used NODDI to investigate the microstructures of GM and SWM in the brain, despite their susceptibility to damage caused by SRC. One study conducted on adolescents revealed that individuals with mTBI exhibited a higher number of voxels displaying reduced FA in the SWM than control participants without mTBI. Furthermore, these SWM microstructural abnormalities were found to be associated with reductions in processing speed. 17
Given the limitations of previous studies, this investigation aimed to compare young boxers with SRC to a control group of typically developing healthy individuals and explored the patterns of SRC-associated microstructural alterations in the DWM, SWM, and GM by using a multi-shell NODDI model. The study hypotheses were as follows: 1) SRC may affect the SWM and GM; 2) the DWM and SWM show different susceptibilities to SRC; and 3) the extent of microstructural alterations in the DWM, SWM, and GM is correlated with the cognitive performance in young boxers.
Materials and Methods
Participants
The study was approved by the Ethics Institutional Review Board, and all participants provided written informed consent in person. The study recruited 50 amateur boxers from provincial sports authorities and eight professional boxers from boxing clubs. The amateur boxers were equipped with protective headgear during training sessions. Seventy-two typically developing individuals were recruited through advertisements as healthy controls (HCs). Typically developing individuals were defined as those without significant developmental delays or adverse physical conditions, who could complete the questionnaire independently. 18 The HCs group engaged in physical activities such as long-distance running, badminton, or basketball at least twice a week. Based on the American Congress of Rehabilitation Medicine’s definition of mTBI 19 and The Sport Concussion Assessment Tool 20 to determine prior exposure to brain injury, participants in the HCs group all denied having a history of mTBI. The selection of boxers was based on the definition of SRC from the Consensus Statement on Concussion in Sport, held in Berlin in October 2016, 21 which includes traumatic brain injury resulting from a direct blow to the head, face, or neck; the presence of transient neurological deficits; the presence of clinical signs and symptoms, which may or may not include loss of consciousness; and the absence of abnormalities on structural neuroimaging. Exclusion criteria included acute phase (within 7 days) concussion, severe multiple and combined injuries, presence of mental or neurological disorders, drug or alcohol abuse, and MRI contraindications. The exclusion criteria for the HCs group were identical to those for the SRC group.
All 130 participants completed neuropsychological and MRI assessments. Each image generated during processing underwent careful inspection and rigorous quality control. We excluded T1WI images reconstructed with low quality or segmentation errors by FreeSurfer as well as any images with NODDI preprocessing failures or incorrectly fitted metrics. The NODDI data of two boxers were excluded due to preprocessing failures, while T1WI segmentation errors prevented the analysis of GBSS data from 9 boxers and 10 HCs. Finally, DWM and SWM analyses were conducted on a cohort consisting of 56 boxers and 72 HCs (Table 1). In addition, GM analyses were performed on a subset of 47 boxers and 62 HCs.
Demographic and Neuropsychological Data of All Participants
Two-sample t-test.
Chi-square test.
Mann–Whitney U test.
HCs, healthy controls; IQR, interquartile range; MoCA, montreal cognitive assessment; NA, not applicable; RAVLT, rey auditory verbal learning test; SD, standard deviation; SRC, sports-related concussions.
Clinical assessments and neuropsychological tests
The participants underwent clinical assessment and neuropsychological testing before the MRI scans. They were interviewed to ascertain the duration of participation in boxing, the number of concussions and knockouts, common sites of injury, the time since the last SRC, and the duration of symptoms. They also underwent an assessment of the neuropsychological areas commonly affected after SRC, including cognitive function, emotional assessment, and post-concussion symptom assessment. Global cognitive function was assessed using the Montreal Cognitive Assessment (MoCA). Information processing speed was assessed using Trail Making Test (TMT) A and B. 22 TMT A involved measurement of the time participants were required to connect 25 randomly arranged numbers from the smallest to the largest (1-2-3, etc.). TMT B involved the measurement of the time the participants needed to connect randomly arranged letters and numbers in sequence (1-A-2-B, etc.). TMT B-A was the total time required to complete TMT B minus the total time required to complete TMT A. The color-word Stroop test consisted of three subtests: Stroop color naming required participants to name a series of colored dots; Stroop inhibition required participants to name a series of word colors; and Stroop inhibition-switching, which required participants to report the color in which the name of the color was printed (e.g., if the word “blue” is printed in red, the participant had to report red). All three tests required participants to name the corresponding color as quickly and accurately as possible. Executive function assessment included inhibition and set-shifting of color-word Stroop tests and TMT B-A. Vocabulary learning and recall (immediate and delayed) were evaluated using the Rey Auditory Verbal Learning Test (RAVLT), 23 which assesses language learning ability (asking participants to recall 15 words immediately after hearing them, repeat the process five times, and recording the sum of the scores on items 1–5), immediate recall (introducing a new list for interference and then asking participants to repeat the original list, and recording the score on item 6), delayed recall (requiring participants to recall the original list after a 20-minute interval, and recording the score on item 7), and recognition score. Working memory capacity was assessed using the Forward and Backward Digit-span Test. Anxiety and depression were assessed using the Self-rating Anxiety Scale and Self-rating Depression Scale (SDS). 24 The post-concussion scale was used to assess frequently reported physical and psychological symptoms following SRC. 25 All measures were the raw scores.
MRI data acquisition
MRI data acquisition was performed on a 3T GE Premier scanner equipped with a 48-channel head coil. Each subject underwent the same neuroimaging protocol. Three-dimensional T1-weighted images (3D-T1WI) were obtained using Magnetization Prepared-Rapid Gradient Echo imaging sequence with TR/TE = 2,632/3 ms, TI = 1,000 ms, 256-mm FOV, 256 × 256 matrices, voxel size = 1.0 mm × 1.0 mm × 1.0 mm, 392 contiguous partitions. The acquisition times for 3D-T1WI were 6 min and 8 sec. The NODDI data were acquired using a multi-slice single-shot spin-echo echo-planar image sequence along 20, 40, and 60 motion-probing gradient directions with b-values of 1,000, 1,800 and 2,500 s/mm2, respectively. The protocol also included a b = 0 s/mm2 image with a reversed phase-encoding direction (Fig. 1A). The other acquisition parameters were TR/TE = 5,705/68.8 ms, flip angle = 90°, 240-mm FOV, 120 × 120 matrices, voxel size = 2.0 mm × 2.0 mm × 2.0 mm, 78 slices, 2 mm slice thickness, and multiband acceleration factor = 2. The acquisition times for NODDI were 11 min and 42 sec.

An overview of the processing pipeline.
Preprocessing of T1WI and NODDI data
The 3D-T1WI was preprocessed using the “recon-all” process in FreeSurfer version 7.1 (http://surfer.nmr.mgh.harvard.edu/) to reconstruct the cerebral cortex and segment subcortical structures according to a standardized pipeline (Fig. 1C). Each image was resampled onto fsaverage and smoothed with a 15 mm full-width half maximum Gaussian kernel. The NODDI was preprocessed using the tools provided in the FMRIB Software Library (FSL, version 5.0.7, https://www.fmrib.ox.ac.uk/fsl). The preprocessing steps included eddy current distortions, motion artifacts correction, skull-stripped, and the DTI tensor fitting and calculated DTI metrics. 26 NODDI metrics fitting was performed using the CUDA Diffusion Modelling Toolbox (cuDIMOT, https://users.fmrib.ox.ac.uk/∼moisesf/cudimot/) running on graphics processing units. Subsequently, FA, MD, AD, RD, NDI, orientation dispersion index (ODI), and ISOVF metrics images were generated for each participant. The meanings of DTI and NODDI metrics are summarized in Supplementary Table S1.
Tract-based spatial statistics analyses
The whole brain white matter fiber bundles were analyzed using tract-based spatial statistics (TBSS). Create a white matter skeleton with an FA threshold of 0.3 and project the FA, MD, AD, RD, NDI, ODI, and ISOVF images to the corresponding values (Fig. 1B). In addition, DWM was registered into the diffusion space using the Johns Hopkins University (JHU) white matter tracts atlas (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Atlases).
SWM tractography and analyses
Using FMRIB’s linear image registration tool, the gray matter–white matter boundaries and subcortical white matter of both hemispheres and DWM were linearly registered into the FA space to generate the corresponding SWM seed masks and exclusion masks. Probabilistic tractography is performed at the voxel level using BedpostX on FSL and generates the necessary parameters. 27 After that, a probabilistic tractography of the gray matter–white matter boundary of each hemisphere was performed for each subject excluding the white matter mask. The TBSS in FSL Randomise software was used to nonlinearly transform the individual SWM tracts into a standard space and generate an average SWM mask, and individual FA images into a standard space and generate average FA images. Next, multiply the average FA image by the thresholded SWM mask to generate the SWM mean FA image. Finally, the SWM mean FA skeleton was created with a threshold of 0.15. 28 Subsequently, using the tbss_non_FA script to build other parameters of DTI and NODDI (Fig. 1D).
Gray matter-based spatial statistics analyses
The whole brain’s gray matter was analyzed using gray matter-based spatial statistics (GBSS). For each subject, the skull was stripped, and segmentation of gray and white matter was performed on T1WI. The DARTEL method is used to non-linear warping the segmented gray matter to Montreal Neurological Institute (MNI) 152 common space (http://www.mni.mcgill.ca/). For NODDI data, after B0 was co-registered with individualized T1WI and converted into MNI space by the nearest neighbor interpolation method, the diffusion maps of all subjects in the standard space were summarized into 4D volume data for group analysis. Next, the skeleton was generated from the mean GM image, and the threshold was set to 0.55 to generate the skeleton mask. 29 Finally, each diffusion image was projected onto the skeleton for group-level statistical analysis. Tbss_fill is used to thicken the result (Fig. 1E).
Statistical analyses
SPSS software (version 22.0; IBM Corp., Armonk, NY) was used for statistical analyses. Continuous variables conforming to normal distribution were analyzed by independent t-tests and expressed as mean ± standard deviation (SD). Mann-Whitney U test was used for variables with non-normal distribution. Sex distribution among the two groups was compared through the chi-square test. To analyze the association between neuropsychological assessment outcomes and days since the injury or the number of knockouts, Pearson correlation analysis was employed.
Cortical thickness and area were evaluated using a vertex-based general linear model with age, gender, and education as covariates. Vertices with thresholds higher than 3.0 are considered statistically significant. Group voxel-wise TBSS and GBSS analysis were performed using a general linear model (GLM) design matrix using Randomize (FSL). Significant voxels were identified by controlling for family-wise error (FWE) rates using Threshold-Free Cluster Enhancement (TFCE) and 5,000 permutation tests for multiple-test corrections with age, gender, and education as nuisance variables. The accuracy of distinguishing the SRC group from the HCs group was analyzed using receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) of diffusion metrics in the region of significant difference was analyzed. Associations between mean values of diffusion metrics in WM, SWM, and GM and neuropsychological domains were examined also using Pearson correlation analysis. The results of all comparisons were corrected using the FDR method. Statistical significance was set at p < 0.05.
Results
Demographic and clinical results
The mean age of the SRC group was 20.84 years (SD, 4.4 years), with a mean education duration of 11.73 years (SD, 1.76 years). The HCs group had a mean age of 21.78 years (SD, 3.16 years), and a mean education duration of 12.4 years (SD, 2.46 years). The age and years of education did not differ significantly between the SRC and HCs groups. In the SRC group, the average duration of participation in boxing was 5.25 years (SD, 2.75 years), and the median number of knockouts was 1 (interquartile range [IQR], 3). The median time from the last SRC to MRI in the SRC group was 33.5 days (IQR, 45.25). On neuropsychological tests, boxers showed reductions in processing speed, executive function, vocabulary memory, and working memory in comparison with the control participants. The two groups showed no significant differences in global cognitive ability, anxiety, and depression scores (Table 1). As expected, a correlation was observed between the frequency of the number of knockouts and the duration of participation in boxing (p = 0.004, R = 0.38). However, no correlations were observed among the results of the neuropsychological scales between the duration of participation in boxing, the number of days since the last injury, and the number of knockouts.
Whole-brain white matter analyses
Group comparisons revealed significantly lower FA, NDI, and ISOVF and higher MD, AD, and RD in the whole-brain white matter in youths with SRC than in the HCs (Fig. 2A). After registration to the JHU ICBM-DTI-81 White Matter Labels, the DWM fiber bundles involved were mainly located in the corpus callosum (CC), corona radiata (CR), internal capsule (IC), external capsule (EC), thalamic radiation (TR), superior longitudinal fasciculus (SLF), and middle cerebellar peduncle (Supplementary Table S2). Comparisons between groups showed no changes in the ODI of the whole brain white matter. Except for FA, the significance of the other metrics was p < 0.01 after the family-wise error (FWE) correction.
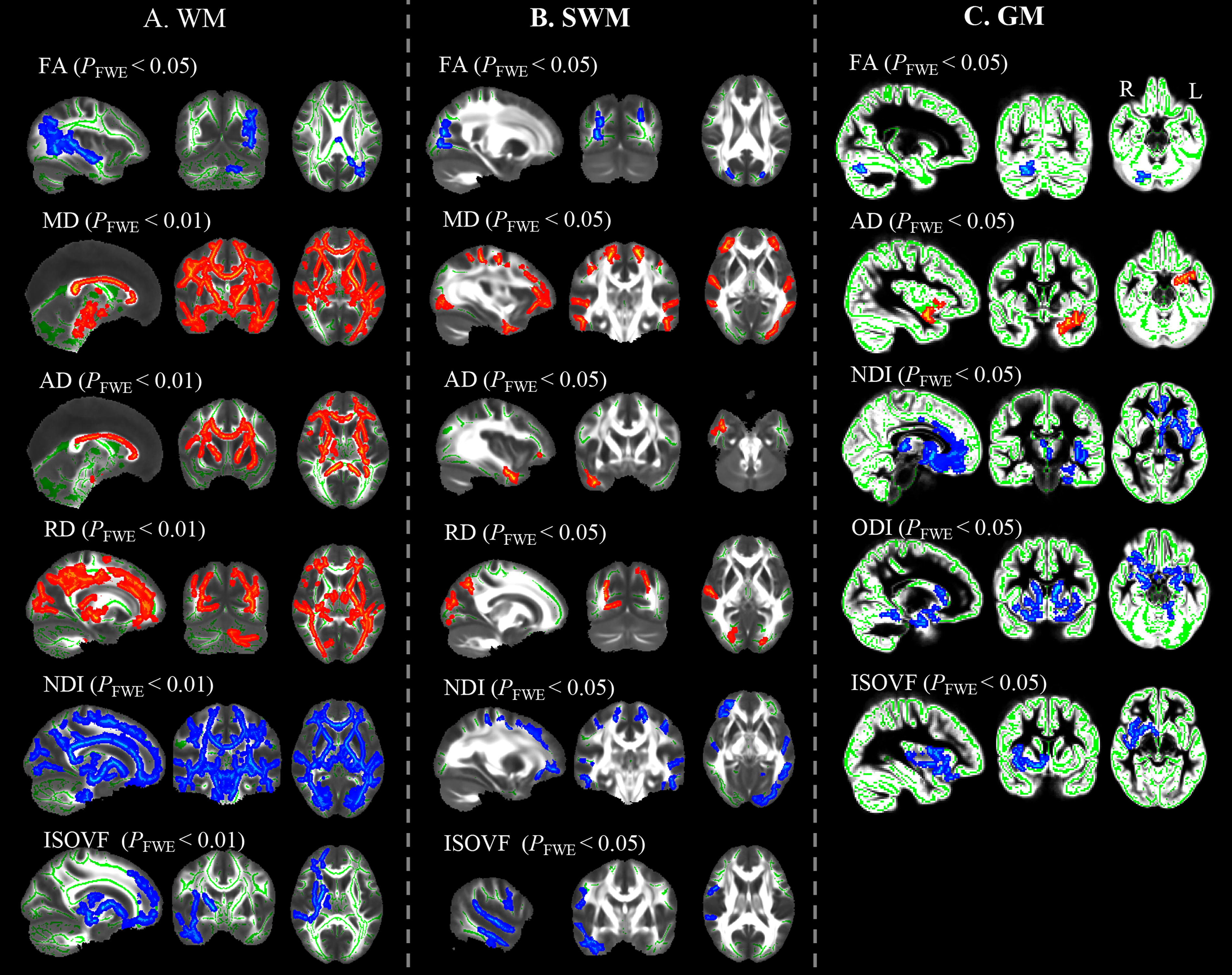
The results of the TBSS and GBSS analyses of the DTI and NODDI metrics between the SRC group and the HCs group. Red represents the SRC group voxels with significantly higher values than the HCs group. Blue represents the SRC group voxels with significantly lower values than the HCs group. Green denotes the mean FA skeleton. DTI, diffusion tensor imaging; FA, fractional anisotropy; GBSS, Gray matter-based spatial statistics analyses; HCs, healthy controls; NODDI, neurite orientation dispersion and density imaging; SRC, sport-related concussions; TBSS, tract-based spatial statistics analyses.
SWM analyses
The DTI and NODDI metrics in SWM were similar to those in the whole brain white matter, with the SRC group showing lower FA, NDI, and ISOVF and higher MD, AD, and RD than the control group (P FWE <0.05) (Fig. 2B). The MD and NDI metrics showed the widest range of brain regions with SWM abnormalities. Voxel clusters showed that the SWM abnormalities in the SRC group were mainly located in the temporal and occipital lobes in comparison with the HCs group (Supplementary Table S3).
Whole-brain gray matter analyses
The FreeSurfer calculation of cortical morphological characteristics revealed no statistically significant differences in cortical thickness and area between the SRC and HCs groups. GBSS was used to investigate the patterns of alterations in SRC cortical microstructure. Relative to the HCs group, the SRC group showed a lower FA in the right cerebellum and a higher AD in the left insular cortex (P FWE < 0.05). Cortical NDI, ODI, and ISOVF in the SRC group were significantly reduced in the frontotemporal cortex region (Fig. 2C) (Supplementary Table S4). In contrast to DWM and SWM, ODI abnormalities occurred only in the cortex.
Sensitivity of SWM and DWM to SRC-induced changes in the diffusion metrics
Extraction of the mean metric values of the DWM and SWM clusters in the SRC group showed more significant metric abnormalities in the DWM than in the SWM. The p-values after FWE correction for SWM and DWM were MD (0.004 vs 0.0003), AD (0.013 vs 0.005), RD (0.009 vs 0.001), NDI (0.004 vs 0.0003), and ISOVF (0.01 vs 0.02), respectively (Fig. 3). The mean FA and ODI values showed no significant differences between the SWM and DWM in young boxers.
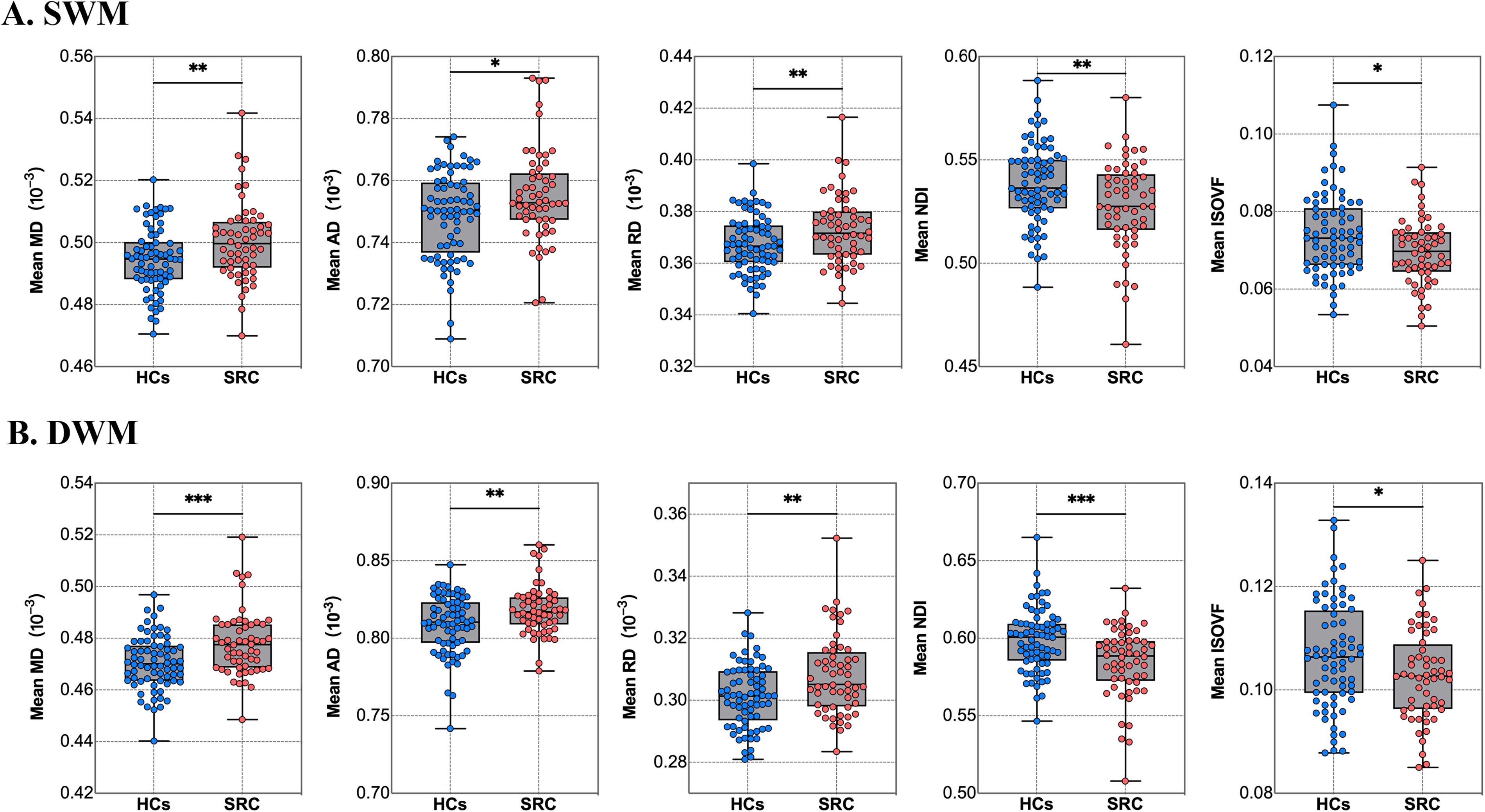
Average measures of DWM and SWM clusters in SRC and HCs group. Compared with SWM, the difference in DWM between the SRC group and the HCs group was more significant. . * indicate p < 0.05; ** indicate p < 0.01; *** indicate p < 0.001. DWM, deep white matter; HCs, healthy controls; SRC, sport-related concussions; SWM, superficial white matter;
Logistic regression analyses
Logistic regression analyses of diffusion metrics in regions showing significant differences between groups were performed to test the diagnostic accuracy of these microstructural metrics in distinguishing DWM, SWM, and GM damage between the SRC and the control groups. A multimodal model combining all the significantly different metrics showed the strongest ability to distinguish DWM damage in the SRC and HCs groups (area under the receiver operating characteristic curve [AUC] = 0.98), followed by GM damage (AUC = 0.96), and finally SWM damage (AUC = 0.94). Among the individual diffusion metrics, the best-performing diagnostic model for the DWM and SWM was ISOVF, with AUCs of 0.93 and 0.89, respectively, and the best-performing diagnostic model for the GM was ODI, with an AUC of 0.92 (Fig. 4).
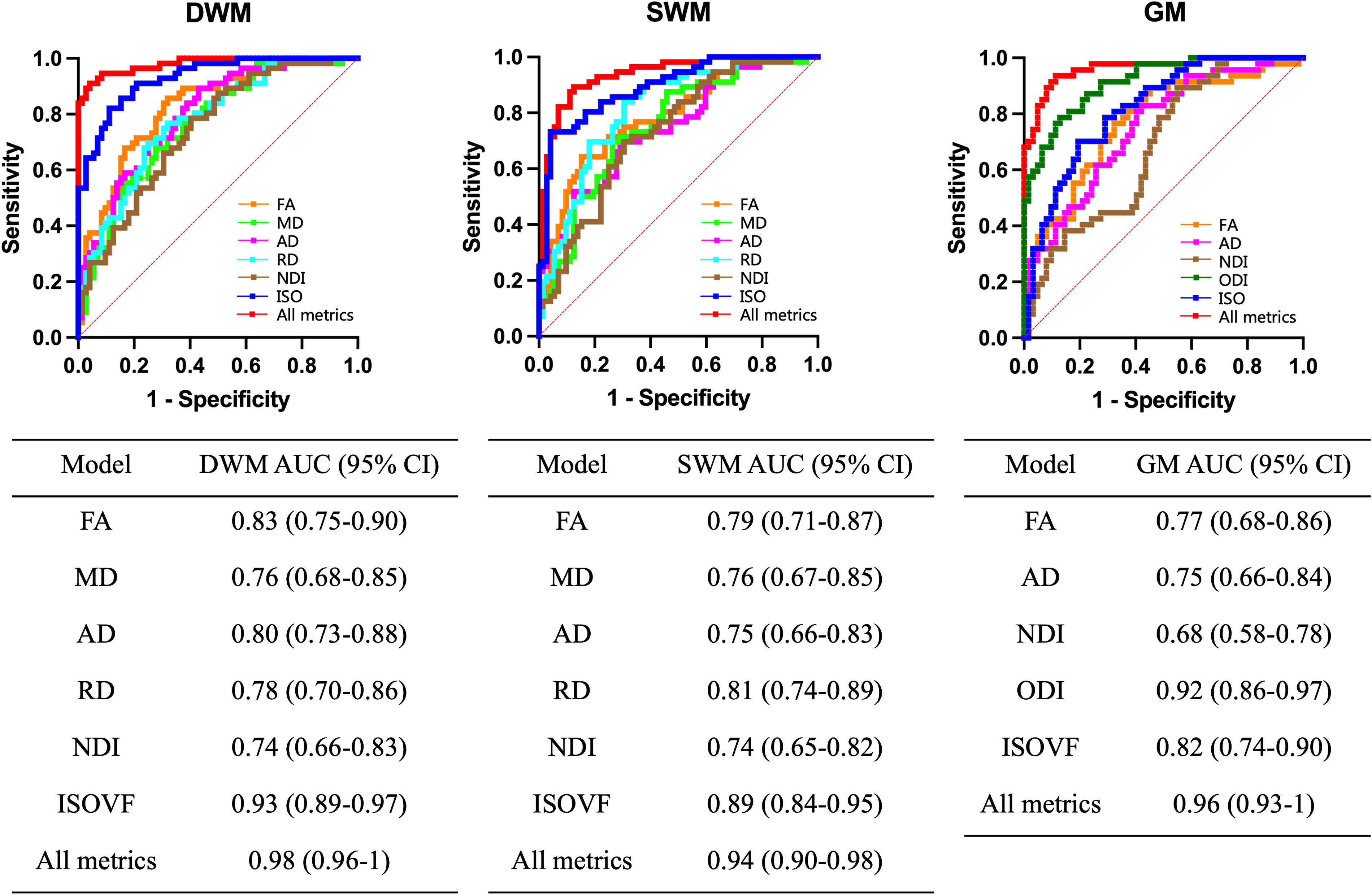
The ROC curve analyzed the area under the curve of the diffusion metrics in the region of significant difference and analyzed the accuracy of distinguishing between the SRC group and the HCs group in diagnosing DWM, SWM, and GM damage. DWM, deep white matter; GM, gray matter; HCs, healthy controls; ROC, receiver operating characteristic; SWM, superficial white matter.
Relationship between abnormal diffusion metrics and neuropsychological measures
The mean values of diffusion metrics in the DWM, SWM, and GM were extracted and correlated with the neuropsychological scale measurements. The findings indicated that abnormalities in the diffusion metrics of the DWM, SWM, and GM were associated with decreased working memory and vocabulary memory in young boxers, most of which showed a link with decreased immediate recall. The decline in the ODI in the GM was negatively correlated with the reaction time of the information processing speed of young boxers (Table 2).
R and P Values from Correlations Between Mri Metrics and Neuropsychological Measures
Note: Data are R(P). Significant results are reported in bold type (FDR corrected for the number of metrics).
AD, axial diffusivity; DWM, deep white matter; FA, fractional anisotropy; GM, gray matter; ISOVF, isotropic volume fraction; MD, mean diffusivity; NDI, neurite density index; ODI, orientation dispersion index; RAVLT, rey auditory verbal learning test; RD, radial diffusivity; SWM, superficial white matter.
Discussion
The current study involved a diffusion MRI analysis of demographically similar young boxers with SRC and HCs, along with a novel investigation of microstructure changes in the GM and SWM in young boxers. In the SRC group, the microstructure of the DWM, SWM, and GM showed significant spatial change patterns. In comparison with the HCs group, the SRC group showed lower FA, NDI, and ISOVF and higher MD, AD, and RD in the DWM and SWM, as well as lower FA, NDI, ODI, and ISOVF and higher AD in the GM. In comparison with the SWM, the DWM showed a wider range of involvement and more significant differences in diffusion metrics. In addition, the working memory and vocabulary memory of the SRC group were associated with abnormal diffusion parameters in the DWM, SWM, and GM, and information processing speed was associated with GM integrity.
Boxing involves two main types of strikes, a direct hit to the face, which produces linear acceleration, and a hit to the side of the face or chin, which produces rotational acceleration. 30 After the occurrence of SRC, the brain is subjected to acceleration and deceleration shocks, causing axons to shear and stretch, which may lead to traumatic axonal injury and progressive pathological changes in the gray and white matter. Diffusion MRI can quantify the diffusion of water molecules within tissues, and SRC-induced alterations in the brain also alter the diffusion of water molecules. FA usually reflects axonal cytoarchitecture, and low FA values after SRC indicate pathological microtubule disorganization, transport disturbance, and myelin loss in axons. 31,32 Increased MD represents tissue microstructural disruption. Increased AD and RD usually occur in repetitive SRC. 33 Previous studies have identified reduced FA and increased AD and RD in white matter regions of recently retired professional rugby league players in comparison with controls. 34 Similarly, one study conducted during a varsity university hockey season found an increase in AD and RD within the white matter of ice hockey players. 33 Diffuse axonal injury causes axonal degeneration and demyelination as well as reversible axonal remyelination and irreversible axonal breaks, 3 which may be associated with reduced NDI values. ISOVF is used to assess free water content, and a previous study found that the elevation of free water levels in early mTBI may be associated with inflammatory vasogenic edema. 16 The findings in the DWM in this study are consistent with the results of a previous longitudinal study of mTBI that showed a decrease in the NDI and ISOVF six months after injury. 16 The ODI is specific and sensitive to the neurite orientation dispersion and can provide valuable information about the myelinated microstructure of neurites. 35,36 Decreased ODI values represent a decrease in the complexity of the cortical GM structure. This study shows that the microstructure of DWM, SWM, and GM changes significantly even when boxers are young.
This study yielded results consistent with previous SRC studies in a larger study sample. 16,37 The present study found that the CC, which connects the cerebral hemispheres, was the most stressed area after SRCs, followed by the CR, IC, EC, and SLF. The long axons of the brain play an important role in higher cognitive functions, with the CC involved in the processes of attention and memory. 38 The SLF connects the front and back of the brain, and the CR connects the cerebral cortex and subcortical structures, both of which are key structures involved in working memory. 39 A study investigating traumatic brain injury found that patients with subsequent memory impairment showed a decline in DWM integrity. 40 The findings of these studies confirm our results, showing that DWM impairment is associated with decreased cognitive performance.
Located below the cortex, the SWM mediates local connections between adjacent cortices in the form of U-fibers or longer intralobular fibers, 41 which play an important role in developmental processes and cognitive functions. 28,42 Due to the relatively late formation of myelin in the SWM, 43 it is susceptible to damage from SRCs. Among the diffusion metrics, MD and NDI revealed a wide range of SWM impairments involving mainly both sides of the postcentral and middle temporal gyrus, left lateral occipital cortex, right frontal orbital cortex, and planum polare. One study showed that increased MD due to loss of short fiber integrity was associated with reduced cognitive efficiency in aging and dementia. 44 Previous studies have shown that increased MD, AD, and RD values in the SWM in the parahippocampal, temporal, and frontal regions are associated with Alzheimer’s disease. 45,46 One study investigating the effects of mTBI on the microstructure of the GM/WM boundary showed that both whole-brain and lobe-specific GM/WM boundary FA and deep WM FA were significantly reduced, and that microstructural changes at the GM/WM boundary were associated with poor mTBI prognosis. 47 This study found that the abnormal SWM in the SRC group was mainly located in the temporal and occipital lobes on both sides and related to decreased immediate recall ability. Successful encoding of memory usually involves extensive involvement of the attention network and the medial temporal lobe, 48 with the lateral occipital cortex, the medial temporal cortex, and the inferior temporal cortex forming part of the dorsal attention network. Higher cognitive functions require the integration of multiple intracortical connections, and the loss of SWM integrity may lead to structural connectivity dysfunction, which may affect memory function.
The surface-based morphological analysis in this study showed no significant difference in cortical thickness and surface area between the two groups, which is consistent with the results of previous studies, and the findings indicated that SRC may not cause macrostructural damage in the short term. 49 However, significant quantifiable GM microstructure changes were observed in assessments using the GBSS method. To the best of our knowledge, the present study is the first to investigate the GM structure of SRC using the NODDI technique. A previous study also identified a significant loss of neuronal density in the GM of patients with type 2 diabetes mellitus using the NODDI technique, while no abnormalities were detected by Freesurfer. 50 A study examining the effects of SRC on GM structure and diffusion metrics in college athletes found decreased MD in the left pallidum and increased FA in the right amygdala in acute SRC (1.64 days) relative to controls, with no acute differences in GM volume or cortical thickness. 49 Another study using diffusion kurtosis imaging to investigate the effects of sub-concussive head impact exposure on GM microstructure in high school football players over a season found that in the deep GM, the mean kurtosis (MK) decreased and the MD increased significantly in the thalamus and putamen, and in the cortical GM, decreased MK was observed in the inferior parietal cortex, and increased MD was observed in the rostral middle frontal cortices. 51 Our study demonstrates that NODDI may detect GM structural damage in boxers’ brains before the appearance of measurable macrostructural changes.
In this study, GM abnormalities in the SRC group were mainly located in the frontotemporal junction area, insula, caudate nucleus, and parahippocampal gyrus, and the NDI, ODI, and ISOVF in the corresponding brain areas of the SRC group were lower than those in the control group. In comparison with the DTI metrics, NODDI metrics can more clearly characterize the damage range in GM. Concussive shock to the brain has been reported to impair the length of dendritic microtubules and dendritic branches, resulting in dendritic skeleton destruction and a reduction in the number of dendrites, 52 which may reduce neuronal orientation variability and reflect the decrease in NDI and ODI values observed in this study. Neuroinflammation from concussion is often accompanied by morphological changes in the cells, including increased cell body size, fewer fine branches, and severe compression of the free water around the cell body, resulting in a dense appearance, which may be related to a decrease in ISOVF values. 53 In addition, abnormalities in the NDI and ODI of GM in the SRC group have been associated with memory function and information processing speed. One study found that a year of boxing training may impair a boxer’s working memory, short-term memory, and long-term memory. 54 The junction area between the anterior and middle fossae is highly vulnerable to damage as a result of traumatic brain injury. 55 Postmortem autopsy studies of boxers have shown diffuse, non-specific changes throughout the frontal and temporal lobes. 56 Diffuse frontotemporal lobe damage often results in disruption of attention. 57 The insula, as a limbic integration cortex, is responsible for integrating internal and external information and cognitive control. 58 From a microstructural perspective, our findings support the hypothesis that damage to gray and white matter is associated with cognitive memory dysfunction in SRC.
This study also found that the anxiety and depression scores of young boxers were slightly higher than those of the HCs, but the differences did not reach a significant level. Previous studies have shown that boxers can experience psychological distress and loneliness, which can adversely affect their careers. 59,60 However, a recent study of former athletes found that athletes who sustained low-impact repetitive head hits had a lower risk of depression and suicide than the general population. 61 This seems to suggest that the apparent preventive effect of long-term patterns of physical activity on depression and suicidal thoughts may compensate for the harmful effects of mild head trauma. 61 This may explain why the boxers in this study only had cognitive impairment and did not show psychological impairment. Nevertheless, long-term prospective studies are still needed to determine the psychological state of boxers.
By extracting the average values of DWM and SWM diffusion parameters in both cerebral hemispheres, the difference in DWM diffusion parameters was more significant than that in SWM. White matter fiber orientation plays an important role in the strain experienced during trauma. 62 We hypothesized that since SWM has differently oriented fiber bundles and DWM has more homogeneous fiber bundles, the stress caused by SRC may lead to more injury in DWM than in SWM. In addition, because DWM usually consists of long axons and is located in the core of the brain, it is usually more vulnerable in response to SRC. 63 In What’s moreaddition, ROC curve analysis suggested that a multimodal model combining all measures of significance of difference can best distinguish between the SRC and HCs group, suggesting that the use of NODDI to assess DWM, SWM, and GM may be helpful in the clinical diagnosis of SRC.
The current investigation had several limitations. First, the absence of specific clinical diagnostic criteria for concussions and sub-concussions, coupled with boxers’ uncertain recollection of past concussion details, posed challenges in accurately quantifying these injuries. Consequently, we relied solely on self-reported knockouts as a measure. The inclusion of data on the frequency of boxers’ participation in games and daily fights may have allowed a more comprehensive evaluation of injury severity in future research studies. Second, the cross-sectional design of this study limited any exploration of longitudinal gray and white matter changes and their effects on cognitive decline. Third, although previous studies have shown that NODDI can capture the microstructure changes of gray matter and white matter, 16,64 there are still some methodological concerns. For example, the three-compartment model assumed by NODDI and its derived metrics do not necessarily accurately reflect the organizational characteristics of brain structures; 65 the use of a tensor model rather than a constrained spherical deconvolution model has limitations in accurately identifying cross-fiber structures; 66 the FA skeleton of SWM generated by the TBSS is, on average, smaller, as a result of cortical folding and mutation, leading to missing grey-white matter junction regions; 67,68 similarly, the GM skeleton generated by the GBSS is susceptible to partial volume effects and artifacts, and accurate registration between subjects is poor, with a few subjects excluded from this study due to registration errors. Lastly, large-scale gray and white matter network connectomes should be constructed in the future to analyze the effects of injury on the whole-brain network, which may help to explain the attention and memory deficits in SRC.
Conclusions
In summary, this study showed that repeated SRC leads to significant alterations in the brain’s DWM, SWM, and GM structures, and these alterations appear to underlie the neurodegeneration that occurs in boxers later in life. NODDI provides information on changes in gray and white matter microstructure that may facilitate the clinical diagnosis of SRC. The association of changes in gray and white matter microstructure with decreased working memory, vocabulary memory, and information processing speed could be a potential target for monitoring injury prognosis in future studies.
Transparency, rigor, and reproducibility statement
The study design and analytic plan were approved by the Ethics Institutional Review Board (2021A-219) but were not systematically registered on the website. This is because the data collection program was started before registration resulting in registration failure. The overall significant impact of the independent sample t-test was detected by the efficacy >80%, with the difference between the experimental group and the control group being p < 0.05 and an estimated sample size of 64 subjects per group. Seventy-two healthy controls and 58 boxers were included in the study, with two boxers excluded due to preprocessing failures. Complete data were obtained for 128 subjects for DWM and SWM analysis. When the GM analysis was performed, 10 healthy controls and 9 boxers were excluded from data processing failures. All participants were told the results of the imaging assessments after the final clinical observations had been made. Imaging data were acquired between May 8, 2022, and June 3, 2023. Imaging data were collected with subjects in the awake state. Imaging data were collected using the GE Premier scanner. All imaging was collected using the same scanner and protocol. Inadequate acquisition requiring repeat imaging occurred in 5% of participants because of participant motion. Imaging data were preprocessed using FreeSurfer and FSL. All imaging datasets were analyzed at the same time. Analysis failures occurred in 8% of individual imaging datasets. The complete imaging parameters are presented in the methods. The time required for preprocessing and analysis was 3 months. Quality control was assessed using visual inspection and calculated head movement parameters. Statistical tests were performed using the method described in the paper, and multiple comparisons were corrected using the FWE/FDR method. Data from the study will be available from the corresponding author upon reasonable request. Analytic codes used to conduct the analyses presented in this study are available on the official websites of Freesurfer and FSL. The authors agree or have agreed to publish the paper using the Mary Ann Liebert Inc. “Open Access” option under the appropriate license.
Footnotes
Acknowledgments
Many thanks to all athletes and healthy controls for their participation.
Authors’ Contributions
Conception and study design (J.Z. and W.J.H.), M.R. and clinical data acquisition (W.J.H. and J.H.Y.), data analysis and preparation of the original paper (W.J.H., J.W., and W.J.H.), interpretation of results (J.W. and Y.Z.). All authors were involved in paper revising and agreed to be accountable for the integrity and accuracy of all aspects of the work.
Author Disclosure Statement
All authors claim that there are no conflicts of interest.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.