
Abstract
Cognitive impairment is a common complication following spinal cord injury (SCI) and imposes a significant negative impact on adjustment, functional independence, physical and mental health, and quality of life. It is unclear whether interventions for cognitive impairment following SCI are effective. A systematic review of controlled trials was performed to evaluate the effect of interventions on cognitive functions in adults with SCI using search engines: Embase, The Cochrane Library, MEDLINE, Scopus, CINAHL, and Web of Science up to December 2023. Two reviewers independently screened the articles, and study findings were synthesized and summarized. The risk of bias was evaluated using the Cochrane Risk of Bias 2.0 tool. Eight moderate-quality studies were found that investigated the effects of physical exercise/activity-based therapy plus cognitive training or intermittent hypoxia, diet modification and dietary supplements, tibial nerve or cortical stimulation, and drug therapy on cognitive function in SCI. Physical exercise/activity–based therapy plus cognitive training showed most promise for improving cognitive functions, while drug therapy, diet modification, and dietary supplements showed potential for improving cognitive function. However, about half of the participants experienced heightened instability in blood pressure following the administration of midodrine, and one participant reported gastrointestinal side effects after taking omega-3 fatty acids. There was no evidence of improvement in cognitive function for stimulation techniques. The current review highlights the scarcity of research investigating the effectiveness of interventions that target cognitive function after SCI. Further, the effects of these eight studies are uncertain due to concerns about the quality of designs and small sample sizes utilized in the trials, as well as the employment of insensitive neurocognitive tests when applied to adults with SCI. This review highlights a significant gap in knowledge related to SCI cognitive rehabilitation.
Introduction
Spinal cord injury (SCI) is a neurological disorder resulting in partial or complete sensory and/or motor function loss below the injured level. 1 According to the Global Burden of Disease Study, there are more than 20 million people living with SCI in the world and this number is increasing yearly. 2 Advancements in medical care, technology, and health services have led to an increased life expectancy for people with SCI, and so the emphasis is now on improving rehabilitation outcomes. 3 The level of functioning, participation, and satisfaction with life after SCI may be reduced by the occurrence of various secondary health conditions, such as autonomic dysreflexia, chronic pain, and fatigue. 4 There is a greater recognition of the importance of addressing psychosocial aspects during rehabilitation to improve adjustment for community reintegration such as returning to work. 5
Cognitive impairment is a common complication following SCI with research suggesting occurrence most likely lies around 30% of the adult SCI people, with some research suggesting that it could be as high as 60%. 6 –8 Cognitive impairment, if present, could arguably hinder functional improvements throughout rehabilitation and challenge the acquisition of daily living skills needed for successful community reintegration for people with SCI. 7 Cognitive impairment can develop in people with SCI of any age and can present in both the acute and chronic stages. 6 In addition, it has been reported that the risk of developing any form of cognitive impairment after SCI is 13 times greater than in the able-bodied population, 6 and compared with middle-aged or older adults without SCI, adults with SCI are more likely to develop Alzheimer’s disease. 9 Cognitive impairment imposes a significant negative impact on adjustment, functional independence, mental health, and quality of life in the SCI population. 10 In addition, cognitive impairments could indirectly affect physical health by influencing their health behaviors (e.g., physical activity or understanding self-management strategies). 10
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), there are six principal domains of cognitive function, including executive function, complex attention, learning and memory, language, perceptual-motor function, and social cognition. 11 In adults with SCI, the most commonly reported deficits are in the attention and executive function domains. 12 These two domains involve complex cognitive processes such as processing incoming information, planning, decision-making, and mental flexibility. 12 Further, recent research has indicated that, similar to patients with multiple sclerosis or traumatic brain injury (TBI), adults with SCI often encounter challenges in immediate learning but may retain intact delayed recall compared with age-matched healthy controls. 7,13,14
The exact pathogenesis of cognitive impairment in adults with SCI remains uncertain. 15 Yet several possible mechanisms have been proposed, occurring at different phases of SCI. 16 In the primary injury phase, mechanical injury directly damages blood vessels, axons, and neuronal cell membranes, leading to ischemia, hypoxia, hemodynamic abnormalities, and neuronal inflammation. 17,18 The secondary injury phase occurs for several weeks or months following the primary injury. During this phase, pro-inflammatory cytokines are released, accompanied by glutamate excitotoxicity and mitochondrial dysfunction triggering “endoplasmic reticulum stress,” which contributes to further damage and an increased release of extracellular vesicles (EVs) containing pro-inflammatory cytokines. 15,19 These EVs can reach critical areas of the brain through the bloodstream, leading to a reduction in synaptic strength and density, as well as structural damage in regions such as the hippocampus. 15 This process may contribute to long-term neurodegeneration and associated cognitive impairments following SCI. 20 Secondary complications following SCI may also contribute to cognitive impairment, such as TBI. 6 Other contributors include older age at the time of injury, psychological disorders, substance abuse, polypharmacy, chronic pain and fatigue, respiratory disorders, sleep disorders, body temperature dysregulations, post-intensive care unit syndrome, abnormal changes in the prefrontal cortex, hippocampus, and medial prefrontal cortex caused by cortical reorganization following SCI, and abnormal variations in blood pressure caused by autonomic nervous system dysfunction. 15,21
Current SCI rehabilitation programs mainly focus on the promotion and recovery of physical and psychosocial function, with limited attention given to the assessment and treatment of cognitive function. 12,22 Despite the prevalence of cognitive impairment in adults with SCI and growing recognition from researchers and clinicians regarding its significance, targeted clinical interventions are still in the early stages of development. 23 In recent years, researchers and clinicians have initiated some preliminary interventional strategies, such as drug therapy, transcutaneous tibial nerve stimulation, and dietary modification and supplements during inpatient or community-based rehabilitation. However, the evidence for these interventions remains inconclusive, especially regarding their effect on different cognitive domains, safety, feasibility, and acceptability. A previous systematic review, which searched relevant databases up to 2019, synthesized findings on the effect of intervention studies on cognitive function only in adults with traumatic SCI. 24 Findings indicated that the evidence for improving cognitive function after traumatic SCI was sparse and inconclusive, with inpatient rehabilitation showing a small but beneficial effect. However, additional relevant studies have been published since this published review. Further, this previous review included observational studies that may introduce bias when estimating the causal effects of the target interventions.
Therefore, the aim of this systematic review was to comprehensively evaluate the evidence supporting the effect of interventions on cognitive function in adults with SCI and to provide recommendations for subsequent research and practice in this field.
Materials and Methods
This systematic review is reported in accordance with the most recent 2020 Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Statement 25 and was prospectively registered in the Open Science Frame (OSF) (doi: 10.17605/OSF.IO/7S9BY).
Eligibility criteria
We defined the eligibility criteria according to the PICOS (population, intervention, comparison, outcomes, and study design) framework. Population: adults with SCI (≥18 years old). No restrictions were placed on demographic variables, time since injury, level of injury, cause of injury, or completeness of injury. Intervention: no restrictions on the content and form of interventions received by the intervention group. Comparison: the control group was time wait control or usual care. Outcomes: global cognitive function and/or specific cognitive domains based on the DSM-5.
11
Study design: controlled trials; we excluded letters, protocols, reviews, case reports, conference abstracts, dissertations, studies not published in a peer-reviewed journal, and studies with no full text available. We restricted reports to those written in English. If a study consisted of a population with mixed conditions, the study was only included if at least 50% of the participants had a SCI.
Literature search
Studies were retrieved from six databases (Embase, The Cochrane Library, MEDLINE, Scopus, CINAHL, Web of Science) using search terms such as cognition, cognitive impairment, cognitive function, and spinal cord injuries (see Supplementary Appendix S1 for the complete search strategy). All databases were searched from inception (their earliest available date) until December 2023. Reference lists of full-text reviewed articles were manually scanned to identify any additional studies. An updated Google Scholar search was conducted right before the submission of the article to identify any potential new studies. The retrieved studies from different databases and other sources were imported into literature management software (EndNote 21).
Study selection and data extraction
EndNote 21 was used to automatically remove duplicate entries. Two reviewers (Y.L., Y.L.H.) independently reviewed the titles and abstracts of the remaining studies. For studies that potentially met the inclusion criteria, further assessment of the full text was performed by reviewers (Y.L., Y.L.H.) to identify if they met all criteria. Differences between the two review authors were resolved by discussion and, when necessary, were arbitrated by a third author (A.C.).
The data extraction was completed independently by two reviewers (Y.L. and Y.L.H.) and reviewed by a third reviewer (A.C.). This was performed using a modified version of the data extraction form in the Cochrane Handbook for systematic reviews of interventions. The following data were extracted: the first author, publication year, country, study design, study setting, sample size, characteristics of the study population (age, gender, duration and level of injury, American Spinal Injury Association (ASIA) impairment scale (AIS) grade, cause of injury, comorbid conditions), description of intervention (dosage, frequency, type of intervention), cognitive assessment tool used, measurement points and results of cognitive outcomes and other outcomes, and the feasibility and acceptability of the intervention. 26 The assessment of feasibility was conducted by evaluating its recruitment rate (i.e., the percentage of participants who gave consent after being determined to be eligible), dropout rate (i.e., the percentage of participants who left the study before the intervention was finished), and intervention completion rate (i.e., the percentage of participants who completed the interventions as the researchers defined them). 27 The acceptability of interventions was shown by: (1) any adverse events recorded associated with the intervention and (2) participants’ or clinical staffs’ satisfaction with the intervention. 27
Risk-of-Bias Assessment
The Revised Cochrane Risk of Bias tool for randomized trials (RoB 2) tool was used to assess the quality of controlled trials included in this review. The RoB 2 tool includes the following domains: (1) randomization/allocation process; (2) deviations from intended interventions; (3) missing outcome data; (4) measurement of the outcome; (5) selection of the reported result; and (S) period and carryover effects. Domain S was completed for crossover trials only. This tool classifies the risk of bias for each domain and provides an overall risk of bias outcome (three categories: low, some concerns, and high). 28,29
Data synthesis
Due to the diversity of interventions, variations in outcomes (involving different dimensions of cognitive function), and differences in measurement tools, no meta-analysis was conducted. The results are described narratively, and the substantive significance (effect size) and statistical significance (p value) were extracted and reported. 30 Cohen’s d was used as the index of effect size. For studies that did not provide Cohen’s d, this value was calculated by dividing the mean difference between the intervention group and control group after the intervention by the pooled standard deviation. 31
Results
Search results
A total of 2,640 records were initially captured through the database searches, and an additional eight articles were identified through a manual search of the references. After removing duplicate records and articles that were deemed not relevant through screening of titles and abstracts, there were 36 articles eligible for full-text screening. After screening based on the inclusion and exclusion criteria, eight studies remained for the final synthesis. A PRISMA flow diagram provides a visual summary of the screening process, shown in Figure 1.
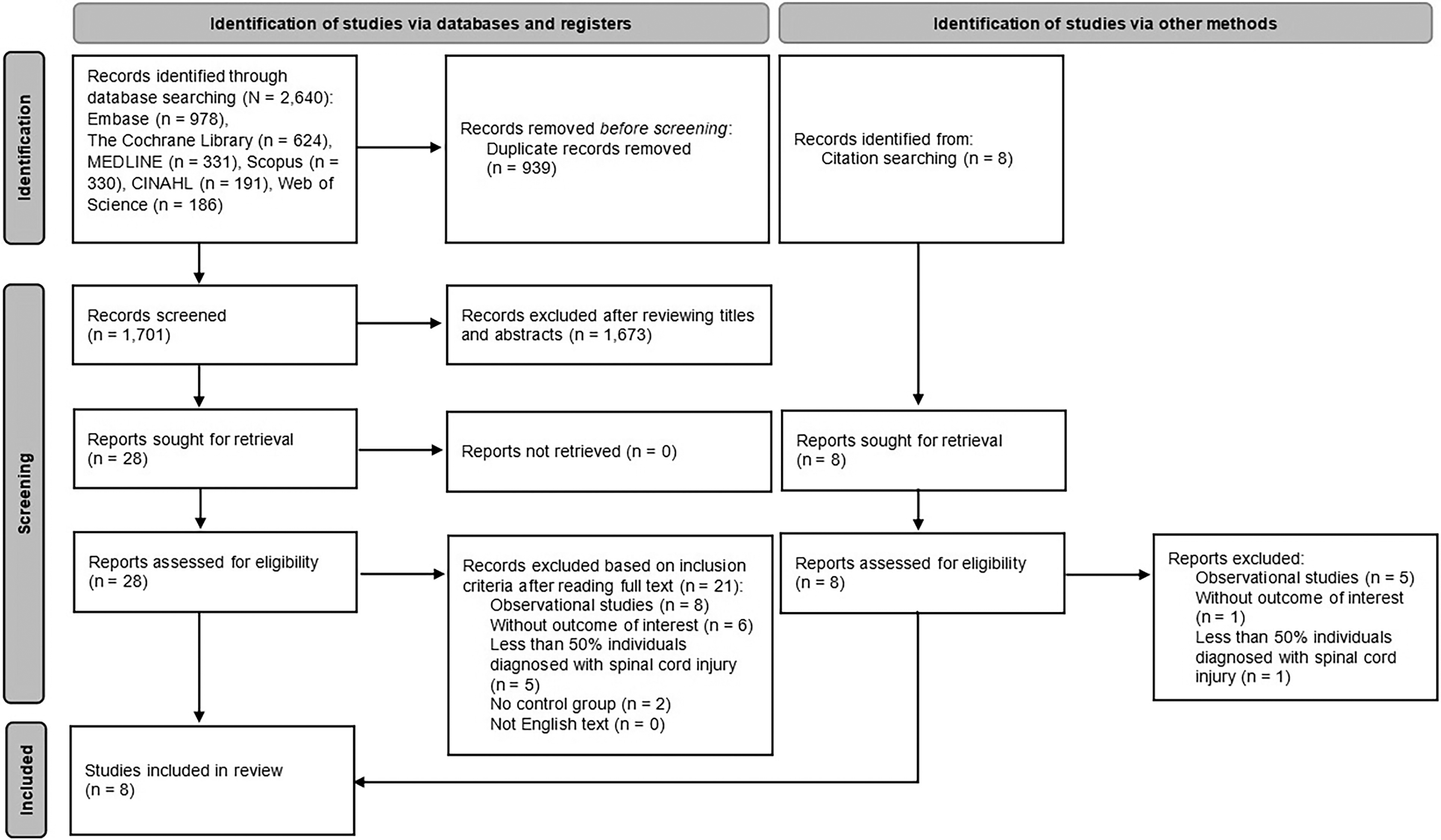
PRISMA flow diagram.
Characteristics of selected studies
The characteristics of the included studies are shown in Table 1. The studies were conducted in seven countries, which were distributed across North America (n = 3), 33,36,37 South America (n = 2), 38,39 Asia (n = 2), 34,35 and Europe (n = 1). 32 This review included five randomized controlled trials, 35 –39 two randomized crossover trials, 33,34 and one controlled trial. 32 The types of study settings included research center (n = 4), 32,33,35,36 hospital (n = 2), 37,39 and rehabilitation institute (n = 1). 38
Study Characteristics and Data Extraction
AIS, American spinal injury association (ASIA) impairment scale; BF, bayes factors; C, cervical spine; CG, control group; d, Cohen’s d; FAM-cog, Functional Assessment Measure-Cognition; FIM, Functional Independence Measure; FIM-cog, Functional Independence Measure-Cognition; IG, intervention group; L, lumbar spine; MoCA, Montreal Cognitive Assessment; NR, not reported; RCT, randomized control trial; SCI, spinal cord injury; T, thoracic spine; TTNS, transcutaneous tibial nerve stimulation.
Participant characteristics
The sample sizes in the included studies ranged from 19 to 104 participants, resulting in a total sample of 379 individuals with a SCI, and 68.6% were males. The mean age of the participants in the included studies ranged from 41.0 ± 17.0 years to 58.6 ± 12.6 years.
The majority of studies included patients with chronic SCI who had a duration of injury of one year or longer, 33 –36,38 with two studies comprising patients at least three months post-injury 32,39 and one study that recruited subacute SCI patients within six weeks of injury. 37 Regarding the cause of SCI, two studies focused on patients with traumatic SCI, 35,37 two studies involved patients with traumatic and non-traumatic SCI, 34,38 and four studies did not provide the relevant information. 32,33,36,39 Two studies included patients with SCI classified by the AIS as grade A or B, 32,35 two studies only focused on patients with motor-incomplete lesions (AIS grade C or D), 34,38 and the remaining studies did not impose restrictions in relation to the extent of injury for the participants. 33,36,37,39 There were three studies that explicitly used the history of brain injury as one of their exclusion criteria, 33,38,39 while the other five studies did not mention whether the study participants included those with an identified brain injury. 32,34 –37
Intervention effects
Broadly, four types of interventions were used in the included studies, consisting of: (1) physical exercise/activity-based interventions (n = 3); 32,34,38 (2) diet modification and dietary supplements (n = 2); 35,36 (3) stimulation techniques (n = 2); 37,39 and (4) drug therapy (n = 1) 33 (see Table 1). All eight studies evaluated cognitive function pre- and post-intervention without conducting follow-up measurements. Four of the included studies did not set cognitive function as the primary outcome. 33,34,37,39 Regarding the intervention effect, only the studies conducting physical exercise/activity-based interventions (n = 3) demonstrated a statistically significant improvement in cognitive function. 32,34,38
Physical exercise/activity–based interventions and cognitive training
Of these three studies, two used either standard physiotherapy exercises or partial body weight–supported treadmill training (i.e., repeated bouts of physical training) 32,38 and one used short-term training with obstacle crossing on a walkway (i.e., a single bout of training). 34 The duration of these interventions ranged from 30 min 34 to 8 weeks. 32 All were conducted at research centers for patients with chronic SCI. 32,34,38 Two studies combined exercise with cognitive training. 32,34 The third study combined body weight-supported treadmill training with intermittent hypoxia. 38
Maggio et al. conducted an eight-week intervention with 42 participants, including the same amount of physical exercise and cognitive training (three sessions per week), using different platforms [semi-immersive virtual reality (VR) versus the control using in-person pencil and article tasks with a therapist present]. 32 In the VR group, patients interacted with the projected environment using photoelectric infrared sensors to perform specific physical and cognitive exercises, such as reaching, touching, or grabbing a series of objects, or playing with projected images (e.g., a ball) on the floor. Compared with the in-person traditional training group, patients in the VR group obtained real-time audio/visual feedback and personalized training in terms of difficulty levels. There was a significant improvement in global cognitive function among the VR patients (p = 0.001) compared with the control group.
Amatachaya et al. and Navarrete-Opazo et al. focused on patients with chronic motor-incomplete (AIS grade C and D) lesions. 34,38 Amatachaya et al. recruited participants with SCI who could walk for at least 17 meters with or without assistive technology and tested the effects of a single task (walking unaided or with an aid through a 30-minute obstacle course) versus a dual task (walking the obstacle course while also performing cognitive tests such as the Stroop test). They found that those performing the dual task (n = 22) had improved executive function compared with those who received the single task (n = 22) (p = 0.014, d = −0.39, 95%CI [−0.99 to 0.20]). 34 Navarrete-Opazo et al. designed a four-week body weight-supported treadmill training program, incorporating either moderate intermittent hypoxia or continued normoxia. 38 Compared to the baseline, the intermittent hypoxia training group (n = 17) showed significant improvements in immediate, short-term, and long-term memory performance (p < 0.05). The continuous normoxia training group (n = 16) only exhibited significant improvement in immediate memory performance (p = 0.002). There was no significant difference in post-intervention memory performance between the two groups. 38
Diet modification and dietary supplements
Two studies investigated the potential of diet modification and dietary supplements to reduce inflammation and enhance cognitive function in patients with chronic SCI. 35,36 Allison et al. implemented a three-month anti-inflammatory diet intervention in 20 patients with SCI and an injury duration of over four years. 36 While the levels of inflammatory mediators decreased, there were no significant group-by-time interaction effects observed in verbal learning and memory, 36 as assessed by the California Verbal Learning Test. 40
A similar conclusion was obtained by Norouzi-Javidan et al. 35 They studied changes in disability and dependency scores in patients with SCI and an injury duration longer than one year following a 14-month period of ω-3 fatty-acid consumption. 35 The overall number of participants in this study was 104, with 54 patients in the intervention group. The results indicated no significant improvement in cognitive domain scores measured by the United Kingdom (UK) version of the Functional Independence Measure and Functional Assessment Measure (FIM + FAM) scale. 41
Stimulation techniques
Two studies utilized cognitive function as one of the indicators to evaluate the safety of different types of neurostimulation for treating complications in patients following SCI. 37,39 Stampas et al. investigated the effect of a two-week period of transcutaneous tibial nerve stimulation primarily for control of the neurogenic bladder in patients with acute SCI (n = 19). 37 They observed no significant difference in cognitive function assessed using the cognition subscale of the FIM at admission and discharge between the groups. Similarly, as the secondary outcome analyses of the effect of long-term deep transcranial magnetic stimulation (d-TMS) with multiple sessions on pain intensity reduction, Selingardi et al. reported no significant differences in comprehensive cognitive evaluation among the two active d-TMS groups (33 patients in each group) and the sham d-TMS group (n = 32) after 12-weeks of treatment (p > 0.180). 39 Both studies concluded that stimulation applied to either the tibial nerve or cortex, following established safety guidelines, appeared to have no significant additional impact on cognitive function in adults with SCI. 37,39
Drug therapy
Wecht et al. evaluated the efficacy of a single dose of midodrine (10 mg) as a pharmacological agent to increase and normalize systolic blood pressure in chronic SCI patients with hypotension (n = 41). 33 As secondary outcomes, the effects of midodrine on the improvement of cerebral blood flow velocity and global cognitive function were also investigated. Cognitive function was assessed in all participants at the beginning, 45 and ∼90 min after dosing. 42 The results showed that, compared to the placebo, a single dose of midodrine administration did not have a significant effect on global cognitive function. Moreover, concerns regarding the safety of midodrine were raised due to notable heterogeneity in individual responses and the potential for midodrine to exacerbate blood pressure instability. 33
Feasibility and acceptability of the interventions
Only one study reported the exact recruitment rate, which was 56.7%. 38 The dropout rate ranged from 0% 34,36,37 to 5.7%. 38 All studies reported a 100% intervention completion rate among the participants who were not lost to follow-up. 32 –39 One study reported the satisfaction of the intervention, in the form of qualitative feedback, from the perspective of clinical staff. It was reported that transcutaneous tibial nerve stimulation was a safe and feasible modality that could be applied in clinical care for patients with SCI. 37 Regarding the adverse event record associated with the intervention, Wecht et al. reported an increase in blood pressure instability in about half of the participants following the administration of antihypertensive medication (Midodrine). 33 Norouzi-Javidan et al. reported that one participant withdrew from the study due to gastrointestinal side effects of taking ω-3 fatty acids 35 (Table 1).
Assessment tools of cognitive function in the SCI population
There were three studies that assessed global cognitive function, with one study using the Montreal Cognitive Assessment (MoCA) 32 and the other two studies utilizing multiple neuropsychological tests. 33,39 Three studies evaluated multiple cognitive domains. 35 –37 One used the UK version of the FIM plus FAM scale, 35,41 and one used the FIM-cognitive scale to assess language, communication, executive function, and social cognition. 37,43 One study utilized the California Verbal Learning Test 40 to evaluate verbal learning, verbal memory, recognition, and executive function. 36 Two studies assessed the single cognitive domain: one used the Stroop Color and Word Test task to assess cognitive inhibition, 34,44 a subdomain of executive function, whereas the other applied the Spanish Complutense Verbal Learning Test 45 and the Rey–Osterrieth Complex Figure Test 44 to assess episodic verbal memory and episodic visual memory, respectively. 38
Risk of bias
Table 2 reports the risk of bias within studies. Two studies were identified as having a high overall risk of bias, 32,35 five had some concerns about the overall risk of bias, 33,34,36,37,39 and one exhibited a low overall risk of bias. 38 One study did not conduct intention-to-treat analyses, although it reported dropouts and reasons for dropouts. 35 Regarding the randomization process, half of the studies were rated as having some concerns due to inadequate details about allocation concealment. 32,35,36,39 Two studies were identified as having some concerns about deviations from the intended interventions, as participants and people delivering interventions were aware of the assigned interventions. 32,34 One study had a high risk of bias due to missing outcome data. 35 In this study, different numbers of dropouts occurred between groups due to intervention-related gastrointestinal side effects or difficulty to maintain scheduled clinical visits. Concerns were raised about the outcome measurements in half of the studies, either due to a lack of mention about blinding of outcome assessment 33,35,37 or the use of inappropriate neurocognitive assessment tools (e.g., MoCA or FIM-cognitive scale with unsuitable items for patients with upper extremity motor limitations or low sensitivity). 32,35,37 Five studies had some concerns about the selection of reported results, primarily due to insufficient information on pre-specified analysis plans or blinding of data analyses. 33,35 –37,39 None of the eight included studies reported the calculation of the minimum required sample size based on statistical power and cognitive function.
Risk of Bias Assessment according to RoB 2 Tool
N/A, not applicable.
Discussion
This systematic review presents a comprehensive and updated synthesis of evidence from controlled trials evaluating the effect of interventions on cognitive function in adults with SCI. It is worth noting that the number of controlled trials that met quality criteria remains very limited, highlighting the need for further research and practice development in this important area.
Among the included studies, only the physical exercise/activity-based interventions combined with cognitive training or intermittent hypoxia demonstrated significant improvement in cognitive function post-intervention. 32,34,38 The findings from these studies suggest that augmented exercise or activity-based therapies for brief or extended periods may benefit cognitive function across adults with SCI. 32,34,38 The effects of exercise on improving cognitive function have also been found in studies related to patients with stroke, Parkinson’s disease, and dementia. 46 Exercise has been shown to reduce oxidative damage and chronic inflammation, improve cerebral blood flow, increase autophagy, and promote mitochondrial function. 47,48 Further, it has the potential to modulate the myokine profile, activate the insulin-like growth factor-1 signaling pathway, and enhance insulin sensitivity, which can have a positive contribution to cognitive function. 47 Mental health issues such as depression have been shown to influence cognitive function in adults with SCI. 15 The improvement of cognitive function in adults with SCI through physical exercise or activity plus cognitive training may also be related to a positive impact on mental health. The study by Maggio et al., included in this review, reported significant improvements in both global cognitive function and depressive symptoms in participants who underwent a combined exercise–cognitive intervention. 32 This may be partially explained by the positive impact of physical exercise on promoting the function of the hippocampus and stimulating neuroplasticity. 49 It is known that mental health issues and cognitive impairment are associated with hippocampal dysfunction. 50
The results from Maggio et al. and Amatachaya et al. showed that adults with SCI who received both exercise and cognitive training exhibited significant improvements in global cognitive function or executive function. 32,34 Dual task cognitive training may improve physical and cognitive function by strengthening the relationship between sensory information and motor tasks (information-action coupling). 51 Moreover, Maggio et al. found that the utilization of a semi-immersive VR system may strengthen the effectiveness of this dual-task training. 32 The reinforcing effect of VR technology on cognitive training has been confirmed in patients with TBI and multiple sclerosis. 52,53 The use of VR could offer real-time audio/visual feedback to stimulate the patient, facilitating greater involvement in training sessions. 53 Further, VR technology enables patients to engage in realistic and highly immersive exercises in a virtual environment, thereby promoting enhanced control in various sensory, motor, and cognitive domains. 32 However, due to the non-random generation of allocation sequence and the use of an inappropriate neurocognitive screening tool (MoCA) in this study, the results should be interpreted with caution. 32
Hypoxic exercise is a novel training approach that creates unique biological effects on the human body by combining physical activity with high-altitude natural hypoxia or artificial hypoxia stimulation. 54 In the current review, the study by Navarrete-Opazo et al., with an overall low risk of bias, found that the exercise recovery strategy induced by a moderate intermittent hypoxia environment did not negatively impact cognitive function. On the contrary, it may be associated with some improvement in cognitive function compared to continuous normoxia supply. 38 Previous studies have shown that exposure to hypoxia increases the generation of new neurons in the adult hippocampal regions and upregulates the expression of proteins related to erythropoietin, brain-derived neurotrophic factor (BDNF), and serum hypoxia-inducible factor-1α (HIF-1α). 55 –57 The hippocampal regions are associated with the process of learning and the formation of new memory. 15 The activation of HIF-1α and BDNF promotes angiogenesis, neuronal survival, and development, while inhibiting inflammation, leading to enhanced cognitive function. 57 In addition, hypoxic exercise has shown potential benefits for attention, a cognitive domain most likely impaired in adults with SCI. 57 However, it is worth noting that Navarrete-Opazo et al. only assessed memory-related outcomes, and further research is needed to explore the intervention effects on other cognitive domains. 38
It is noted that chronic neuroinflammation associated with SCI may lead to neurotoxicity and induce neurodegeneration in crucial brain areas linked to cognitive impairment. 15 The possible mechanisms involve chronically elevated levels of inflammation leading to disruption of receptors in the hippocampus, which would be related to learning and memory, by influencing neuroactive compounds of the kynurenine pathway, thereby indirectly affecting cognitive processes. 36 Two studies aimed to improve cognitive function in patients with chronic SCI by reducing oxidative damage and inflammation through dietary modifications and supplements but did not find significant cognitive improvements. 35,36 Possible reasons might be that, although there was a successful reduction in pro-inflammatory mediators, it may have been insufficient to induce significant cognitive changes. 36 In addition, brain structures implicated in cognitive function, like the hippocampus, may have already experienced irreversible damage after several years of SCI, but this hypothesis requires further investigation and correlation with neuroimaging data. 36 Further, the lack of a sufficient sample size and acceptable statistical power, in combination with the insensitive tool (FIM plus FAM scale) used to assess cognitive function, may have also contributed to the insignificant results. 35,36 More research is required to examine the causal relationship between inflammatory treatment and the cognitive functions of adults with SCI.
Hypotension, a common secondary condition of autonomic nervous system dysfunction after SCI, may impact cognitive function negatively by reducing cerebral blood flow. 15 While single-dose midodrine therapy conducted by Wecht et al. did not result in improved cognitive function, further exploration in this promising area is warranted that investigates the causal relationship between treatment for hypotension and the cognitive function of patients with SCI. 33 Prolonging the duration of medication and/or adjusting the dosage may serve as potential avenues to enhance the efficacy of drug therapy on cognitive function. In addition, studies by Selingardi et al. and Stampas et al. indicate that peripheral nerve or cortical stimulation techniques following suitable guidelines do not result in additional improvement of cognitive function in adults with SCI. 37,39 However, due to the fact that participants in both studies generally had good cognitive function at baseline and Stampas et al. used a neurocognitive screening tool (FIM-cognitive scale) that is less sensitive to small changes in cognitive function, further research is still needed to validate this conclusion. 37
A variety of tools were utilized for assessing the cognitive function of adults with SCI, which might hinder effective comparisons of the findings across studies. Compared to multiple neuropsychological tests, cognitive screening tools used in the included studies, such as MoCA and the FIM-cognitive scale, have lower sensitivity with a ceiling effect. 58,59 In addition, certain tasks in the MoCA, such as drawing a clock and copying a cube, require hand-motor skills that will not be suitable for people with tetraplegia. 8 Thus, findings from studies that use neurocognitive screens like MoCA should be interpreted cautiously in adults with SCI, especially those with upper extremity motor limitations. 8 In studies focusing on the assessment of a single cognitive domain, it is suggested to use multiple neurocognitive tests to comprehensively evaluate the outcomes, especially in the executive and attention domains. 34,38
In the included studies, only the study by Navarrete-Opazo et al. reported the recruitment rate, raising concerns about the findings of all the included studies. 38 The dropout rates of the included studies were generally low. This may be related to the small sample size, 36,37 a single brief session of intervention with a randomized crossover experimental design, 33,34 or the intervention being conducted during the patient’s hospitalization period. 37 As for the acceptability of interventions, only one study reported feedback from clinical staff. 37 More surveys, especially qualitative surveys of patient satisfaction, are needed. The important issue of cost-effectiveness, lacking in all included studies, should also be assessed and reported to assess and compare the value and feasibility of interventions. 60,61 In addition, in the drug study, approximately half of the participants reported an increase in blood pressure instability after the administration of midodrine, so it is necessary to establish a safe and effective hypotensive treatment approach for adults with SCI. 33 In addition, further research is needed to investigate whether supplementation of polyunsaturated fatty acids may induce adverse gastrointestinal symptoms. 35
Compared with the review published by Pacheco et al., 24 this systematic review provides updated information with summarized evidence from controlled trials focusing on cognitive function in adults with SCI. However, there is limited relevant evidence in this field, and larger-sample size studies with cognitive function as the primary outcome are urgently needed. In addition, most studies did not differentiate between traumatic and non-traumatic causes of SCI when recruiting participants. This hampers further exploration of the mechanisms underlying cognitive impairments associated with different causes of SCI and the development of targeted interventions. Moreover, since all the included studies did not conduct long-term follow-up after the intervention, the duration of the intervention effects remains unclear. It is necessary to implement short- to long-term follow-ups of such interventions. Finally, potential influencing factors on cognitive impairments in adults with SCI, such as psychological disorders, substance abuse, polypharmacy, chronic pain and fatigue, respiratory disorders, sleep disorders, thermoregulation disturbances, and post-intensive care unit syndrome, do not yet have targeted interventions. It is recommended to develop corresponding intervention strategies encompassing these factors.
Limitations
This systematic review has several limitations. First, only peer-reviewed studies published in English were included, potentially overlooking studies published in other languages or within non-peer-reviewed articles (e.g., conference articles, dissertations). Second, a meta-analysis was not conducted due to the heterogeneity of the included interventions. Third, due to the inadequate sample sizes and the use of different cognitive function assessment tools, the findings need to be interpreted with caution. Moreover, there is a lack of qualitative findings on the acceptability outcomes. Cost-effectiveness analysis is also missing in all studies which need further investigation.
Conclusions
This review comprehensively examined the current available evidence in addressing problems with cognitive function after SCI and suggests directions for future research. Interventions targeting cognitive function of adults with SCI remain limited, and therefore, more studies are required. Combining physical exercise/activity with cognitive training is a promising direction for improving cognitive function after SCI. Interventions targeting treatment of inflammation, hypotension management, and intermittent hypoxia may also be potentially effective interventions, but current evidence cannot support any conclusions due to insignificant findings, small numbers of studies, and inadequate sample sizes. Tailored interventions are also needed to address specific cognitive domains (e.g., attention and executive functions) that might be the most severely impaired among adults with SCI. Finally, when assessing intervention effects, it is necessary to use sensitive neurocognitive tools suitable for individuals with SCI. 8
Transparency, Rigor, and Reproducibility
This review is reported in accordance with 2020 PRIMSA guidelines, and the protocol was prospectively registered on a public registry. A comprehensive search strategy was developed with the help of an academic librarian for each electronic database. For more details related to transparency, rigor, and reproducibility, please refer to the material and methods section.
Footnotes
Acknowledgments
The authors acknowledge the support in the literature search from the librarian Ms Kanchana Ekanayake from the library of the University of Sydney.
Authors’ Contributions
Y.L., Y.H., and A.C. were responsible for the conceptualization, methodology, formal analysis and investigation, writing—original draft, and writing—review and editing. I.P., M.A., J.S., C.M., and J.M. were responsible for the conceptualization, writing—original draft, and writing—review and editing.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing conflict of interest is declared.
Supplementary Material
Supplementary Appendix S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.