
Abstract
Traumatic brain injury (TBI)-induced intracerebral hematoma is a major driver of secondary injury pathology such as neuroinflammation, cerebral edema, neurotoxicity, and blood–brain barrier dysfunction, which contribute to neuronal loss, motor deficits, and cognitive impairment. Cluster of differentiation 47 (CD47) is an antiphagocytic cell surface protein inhibiting hematoma clearance. This study was designed to evaluate the safety and efficacy of blockade of CD47 via intravenous (i.v.) administration of anti-CD47 antibodies following penetrating ballistic-like brain injury (PBBI) with significant traumatic intracerebral hemorrhage (tICH). The pharmacokinetic (PK) profile of the anti-CD47 antibody elicited that antibody concentration decayed over 7 days post-administration. Blood tests and necropsy analysis indicated no severe adverse events following treatment. Cerebral hemoglobin levels were significantly increased after injury, however, anti-CD47 antibody administration at 0.1 mg/kg resulted in a significant reduction in cerebral hemoglobin levels at 72 h post-administration, indicating augmentation of hematoma clearance. Immunohistochemistry assessment of glial fibrillary acidic protein (GFAP) and ionized calcium-binding adaptor molecule 1 (IBA1) demonstrated a significant reduction of GFAP levels in the lesion core and peri-lesional area. Based on these analyses, the optimal dose was identified as 0.1 mg/kg. Lesion volume showed a reduction following treatment. Rotarod testing revealed significant motor deficits in all injured groups but no significant therapeutic benefits. Spatial learning performance revealed significant deficits in all injured groups, which were significantly improved by the last testing day. Anti-CD47 antibody treated rats showed significantly improved attention deficits, but not retention scores. These results provide preliminary evidence that blockade of CD47 using i.v. administration of anti-CD47 antibodies may serve as a potential therapeutic for TBI with ICH.
Introduction
Complications resulting from traumatic brain injury (TBI) represent some of the most detrimental and costly health burdens in both the civilian and military populations. 1 –7 Traumatic intracerebral hemorrhage (tICH) occurs in approximately 25–45% following severe TBI. 8 –10 Studies suggest that the hemorrhagic lesion expands during the first 12 h, and up to three to four days after injury. 11 –14 Progression of hemorrhage and resultant hematoma are critical drivers of injury pathology and can prolong recovery in TBI patients with ICH. 13,15 –18 Markedly, hematoma expansion was found to be associated with a fivefold increase in risk of death. 16 The tICH-induced injury pathology is not only driven by damage sustained directly from the initial injury but also by the secondary damage that occurs in the following hours and days. 19 The resultant hematoma can increase intracranial pressure (ICP) due to mass effect and can destroy the cerebral architecture leading to hemolysis and release of neurotoxic degradation products, including hemoglobin, heme, and iron. 20 –23 These substances could cause significant secondary pathologies, involving increased cerebral edema, 24 hemoglobin-derived iron-induced neurotoxicity, 25 –27 blood–brain barrier (BBB) dysfunction, 28 –30 and neuroinflammation. 19,31 –33 The neurological sequelae can manifest as motor deficits, cognitive impairments, depression, and neurodegenerative diseases. 34 –37
Upon cessation of bleeding and clot formation, microglia/macrophages are rapidly recruited to the injured sites and trigger the erythrophagocytosis, which can detoxify hemolytic products, facilitate clearance and termination of the hematoma progression, and promote neurological recovery following TBI. 38,39 This process is mediated by a cascade of signal transduction, including “find-me” signals, “eat-me” signals, and “don’t eat me” signals. Inhibitory, “don’t eat me”, signals prevent phagocytosis, often mediated by interaction of cluster of differentiation 47 (CD47) on erythrocytes and other cell types with microglia/macrophage receptor signal-regulatory protein alpha (SIRPa). 38 Interestingly, CD47 levels in a piglet ICH model were observed to reduce hematoma over time and were associated with increased erythrocyte phagocytosis, rapid blood cell clearance, and reduced hemoglobin. 40 In addition, CD47-deficient erythrocytes have been shown to be more prone to phagocytosis than wild-type erythrocytes. 41 Several studies demonstrated inhibition of CD47-SIRPa signaling as a means to enhance phagocytic microglia/macrophages, to augment tICH clearance, resulting in improvements in brain trauma-induced secondary injury pathophysiology. 39,42 –45 CD47 is not only a signal mediator for erythrophagocytosis, but has also been implicated in the neuroinflammatory response. Studies of TBI and stroke have demonstrated that the CD47 inhibition can reduce the inflammatory burden and improve lesion volume and brain swelling. 46,47 This previous work highlights the potential multi-faceted benefits of anti-CD47 therapy making it a promising candidate for TBI treatment.
Therapeutic inhibition of CD47 using monoclonal antibodies has been successfully performed for various forms of cancer and currently undergoing clinical trials for FDA approval. 48 –50 Inhibition of CD47 using antibody treatment has also been shown to be efficacious in ICH when given directly to the hemorrhage site, which may not be clinically feasible in many scenarios. 39,42,43 Thus far, no studies have investigated the use of intravenous (i.v.) anti-CD47 antibody administration as an acute treatment for TBI-induced hematoma. In this study, we seek to evaluate the safety and efficacy of i.v. anti-CD47 antibody therapy in a rat model of penetrating TBI. Rats receive a frontal, unilateral penetrating ballistic-like brain injury (PBBI) by inserting a probe into the frontal cortex of the fully anesthetized rat and rapidly inflating/deflating the probes elastic tubing into an elliptical balloon causing a temporary injury cavity. The PBBI offers an optimal testing platform because of the presence of significant intracerebral hematoma. The overall hypothesis for this work is that anti-CD47 antibody therapy will be safe and the treatment will improve TBI recovery through enhanced hematoma clearance and reduced neuroinflammation. To test this hypothesis, we performed a dose–escalation study to identify the minimal dose required for acute neurological efficacy in the absence of adverse reactions and used that dose to further investigate the functional recovery from TBI.
Materials and Methods
Animals were housed under a normal 12-h light/dark cycle in a facility accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International and allowed at least 7 days for acclimation to the housing facility before any procedures are performed. All experimental procedures involving animal use were reviewed and approved by the Institutional Animal Care and Use Committee of Walter Reed Army Institute of Research (Silver Spring, MD). Animal studies was conducted under compliance with the Animal Welfare Act, Guide for the Care and Use of Laboratory Animals (NRC Publication, 2011 edition), and other federal statutes and regulations relating to animals and experiments involving animals.
Surgical procedures
Adult male Sprague-Dawley rats (300 g to 400 g; Charles River Laboratories, Raleigh, VA) were used for all experiments. All surgical procedures were performed under isoflurane anesthesia (3–5% for induction and 2% for maintenance) and aseptic conditions. Normothermic (37°C) body temperature was maintained using a heating blanket (Harvard Apparatus, South Natick, MA). For post-injury i.v. drug administration, all rats were surgically implanted with a sterile indwelling catheter with a soft silastic tip inserted into the right external jugular vein at least 24 h before PBBI. PBBI surgery was performed as previously described. 51,52 Briefly, anesthetized rats were fixed in a stereotaxic frame. A right frontal PBBI was produced using a simulated ballistic injury device (Mitre Corp, McLean, VA) with a custom stainless steel probe (Popper & Sons Inc., New Hyde Park, NY). The probe was manually inserted 12 mm into the right frontal cortex through a cranial window (AP: +4.5 mm, ML: +2 mm from Bregma). The elastic tubing on the probe was inflated by a rapid water pressure pulse creating an elliptical balloon to a volume equal to 10% of the total brain volume. After deflation, the probe was manually retracted from the brain, the cranial opening was covered with sterile bone wax, and the skin incision closed with wound clips. Sham animals were treated similarly with only a craniectomy performed.
Drug administration
The treatment drugs were formulated fresh immediately before the experiment and were blinded to the experimenters using a lettered coding system. The drug was administered via a single i.v. injection immediately following PBBI. Animals (n = 8–10/group) were randomly assigned to sham, control, vehicle (VEH) (Cat# 16–4321-85, Rat IgG2a kappa Isotype Control, Life Technologies Corp, Carlsbad, CA), or 0.5 mg/kg, 0.2 mg/kg, 0.1 mg/kg anti-CD47 (Cat# 16–0471-85, Anti-Mouse CD47, Clone: miap301, Life Technologies Corp, Carlsbad, CA). For analysis of the pharmacokinetic profile of the drug, an fluorescein isothiocyanate (FITC)-tagged equivalent was used (Cat# 11–0471-82, FITC-tagged Anti-Mouse CD47, Clone: miap301, Life Technologies Corp, Carlsbad, CA).
Safety analysis
Blood and urine samples were collected at the indicated time-points (see Fig. 1) via the jugular vein catheters placed 1 day before PBBI, and blood was processed for serum and plasma isolation. Serum was analyzed for measurement of serum chemistry panel. Plasma was measured for complete blood count. Urine samples were assessed via dipstick urinalysis. All tests were used for assessment of adverse effects of anti-CD47 administration and were performed by the Clinical Pathology Division at the Walter Reed Army Institute of Research (WRAIR).
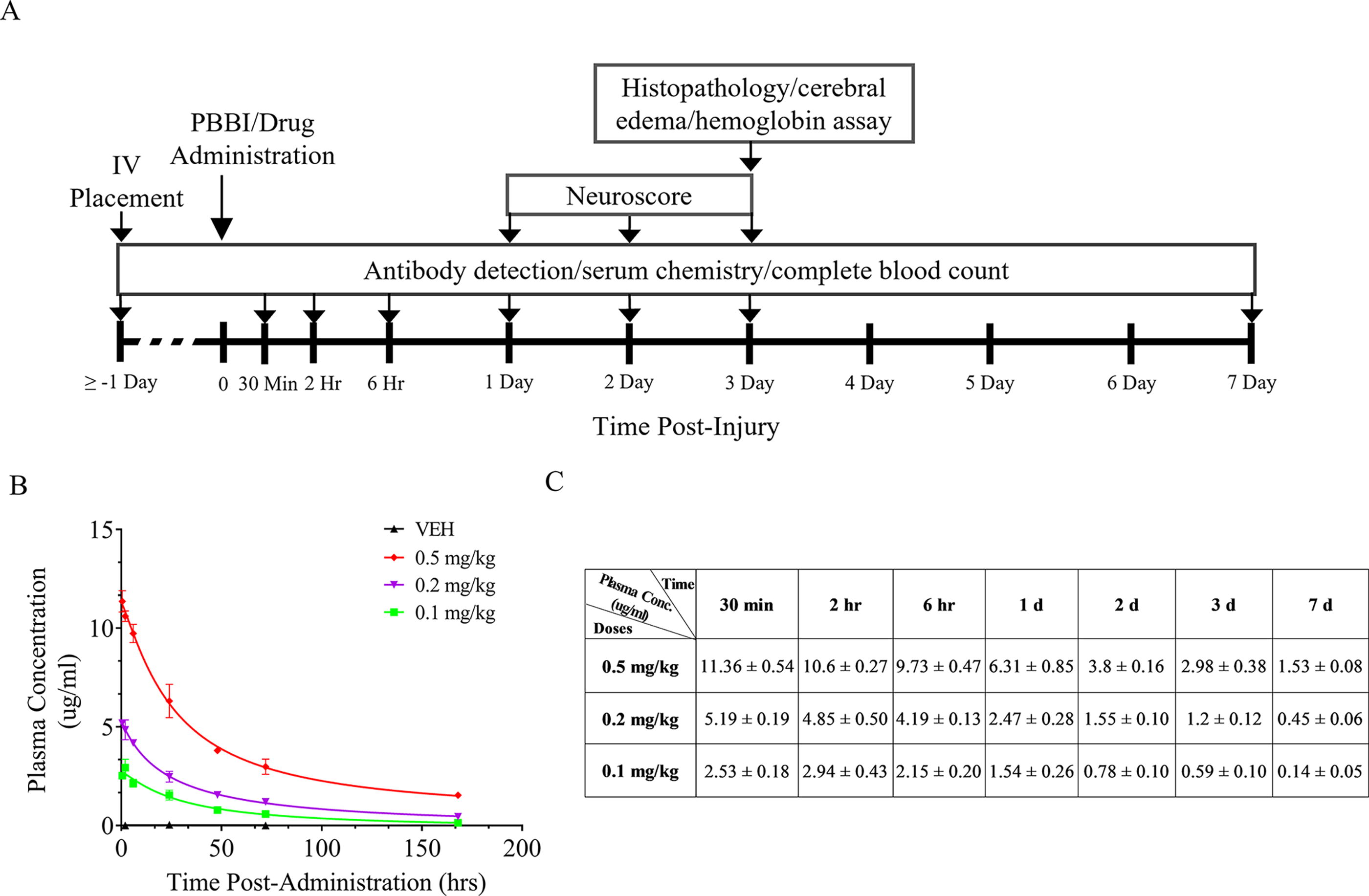
Experimental time line for i.v. administration of anti-CD47 antibodies
At the 72-h end-point, animals were transcardially perfused with phosphate-buffered saline followed by ice-cold 4% paraformaldehyde. The heart, lung, liver, spleen, femur, and kidney were collected for a diagnostic necropsy performed by a veterinary pathologist blinded to the treatment, for pharmacodynamic (PD) analysis.
Pharmacokinetic analysis
Animals underwent regular sampling of blood up to 7 days post-administration. Brains were collected and homogenized for subsequent drug content analysis. FITC-tagged, anti-CD47 antibody concentration in blood was detected using an optimized fluorescence-based spectrophotometric assay. The presence of anti-CD47 antibodies was measured in plasma at 30 min, 2 h, 6 h, 24 h, 48 h, 72 h, and 7 days post-administration.
Neurological evaluation
Neurological deficits were evaluated using the modified Bederson’s criteria. 53 Neurological scores were based on a 12-point scale that comprised four separate neurological tests evaluating contralateral forelimb flexion during tail suspension, shoulder adduction during tail suspension, impaired resistance to lateral push, and abnormal circling behavior. Deficits on each test were scored from 0 (normal) to 3 (severely impaired). Scoring was performed independently and agreed upon by two investigators blinded to the treatment. The final score was taken as the summation of all individual examinations.
Cerebral edema measurement
Cerebral edema was measured using the wet–dry weight method. 54 At the 72-h end-point, ipsilateral and contralateral hemispheres of the cerebrum were collected, and further divided into three, 4-mm sections along the anterior–posterior axis. Each section was weighed to obtain the wet weight, then dried at 60°C for seven days, and reweighed to obtain the dry weight. The percentage of brain water content was calculated by the difference between wet and dry weights divided by the wet weight.
Cerebral hemoglobin content analysis
At 72 h post-injury, the brain was rapidly isolated and the cerebellum and olfactory bulbs were removed. The remaining tissue was divided into ipsilateral and contralateral hemispheres. Cerebral hemoglobin content was used to quantify intracerebral hematoma, as previously described. 55 Briefly, brain hemispheres were manually homogenized in ice-cold saline. After manual homogenization, lysates were sonicated with a pulse ultrasonicator and centrifuged at 13,000 rpm for 30 min and the supernatant was isolated and the protease and phosphatase inhibitor was added. Hemoglobin concentration in each lysate was determined by enzyme-linked immunosorbent assay (ELISA), following the manufacturer’s recommendations.
Histopathological analysis
Cryopreserved brain samples were prepared in 40 micron coronal sections from +4 mm to −7 mm relative to the Bregma for hematoxylin and eosin (H&E), glial fibrillary acidic protein (GFAP), ionized calcium-binding adaptor molecule 1 (IBA1), and fibrin immunostaining. All histopathological preparation was performed by FD Neurotechnologies Inc. Images of the sections were digitized using a VS120 Virtual Slide Microscope (Olyumpus, PA) at uniform criteria for sensitivity and exposure time. H&E sequential sections were used for lesion tracing and volume estimate using Cavalieri’s estimator. 56 Analysis of neuroinflammation (GFAP and IBA1) and fibrin deposition was performed on various regions of interest, including the lesion, peri-lesion, cerebral cortex, hippocampus, striatum, and thalamus. Regions of interest (ROIs) were defined in three sections by an investigator blinded to the treatment, and the percent of positive signal was determined by thresholding performed in ImageJ. For quantification of all markers, the average above threshold signal density of three sections was quantified using ImageJ software. The images were subjected to threshold analysis at 4× magnification. Both the ipsilateral and contralateral regions were examined separately for each specific brain ROI.
Rotarod test
The fixed-speed version of the rotarod task (Rotamex-5 apparatus; Columbus Instruments, Columbus, OH) was used to assess motor performance. Eight days before PBBI or sham procedures, rats were subject to 3 days of handling and 1 day of shaping using sequential fixed-speed increments of 5, 10, and 15 rpm for a maximum of 60 sec per trial, and two trials for each speed. To ensure no difference in performance between groups, rats were pre-trained at 10 rpm for 3 days. A minimum of 40 sec at 10 rpm were used as a cutoff. Animals were then tested at sequential fixed-speed increments of 10, 15, and 20 rpm for a maximum of 60 sec per trial at 4 days before PBBI (baseline levels) and at 7 and 10 days following injury. Data from two trials for each speed were obtained. The mean latency (two trials) to fall off the rotating rod and the overall mean latency (i.e., Motor Score) across all speeds from 2 post-injury testing days were used to evaluate the treatment effects of anti-CD47 antibodies.
Cognitive task
Cognitive function was evaluated on days 13–17 following injury and treatment in a spatial learning paradigm using the Morris Water Maze (MWM) task (Noldus EthoVision XT; Noldus Information Technology, Inc., Leesburg, VA). The water maze apparatus contains a circular pool (75 cm deep; 175 cm diameter) filled with water (22°C; 60 cm deep) and monitored with an automated video-tracking system. A transparent Plexiglas platform (5 cm radius) was submerged 2 cm below the water surface and centered in the southwest quadrant (35 cm from the pool wall). The MWM task was performed during the light phase in a dimmed room with visual cues as described in a study. 57 In each trial, rats were placed into the pool facing the wall at one of four start locations (north, south, east, west). The trial was complete once the rat found the platform or 90 sec had elapsed. If the rat failed to find the platform in 90 sec, it was manually guided onto the platform. Rats were given four trials per day (30 min inter-trial interval; ITI) for 5 consecutive days. This was followed by a probe trial (missing platform task) on the last day to assess memory retention for the platform location. Primary outcome measures included latency/distance traveled to find the hidden platform (spatial learning), percent time spent in the thigmotaxis zone (attention), and percent time searching in the target zone (missing platform) during the probe trial (memory retention).
Statistical analyses
All statistical analyses were performed using GraphPad Prism. The non-parametric (categorical) neuroscore data were converted to ranks using the aligned rank transformation. Two-way analysis of variance (ANOVA) was used to analyze the transformed neuroscore. A mixed-effects model was used for the MWM and rotarod analysis across testing days. The remaining data were analyzed using a one-way ANOVA. Outliers were determined and removed using the robust regression and outlier removal method (Q = 1%). 58 Bartlett’s and Shapiro–Wilk tests were used to test assumptions of homoscedasticity and normality. If the assumption of normality could not be met, a transformation of the data was performed using logarithmic or square root functions before the analysis. In the case of failing Bartlett’s test, a Welch’s ANOVA was used instead. When needed, post hoc analyses using the Tukey’s multiple comparison test were performed. In all cases, a p value of 0.05 was considered statistically significant.
Results
PK/PD profile
FITC-tagged, anti-CD47 antibody concentration was determined using a fluorescence detection assay in plasma to determine bioavailability. Following a single i.v. administration of FITC-tagged, anti-CD47 antibody at 0.1, 0.2, and 0.5 mg/kg, the concentration peaked within 30 min post-administration, and decayed overtime up to 7 days post-administration (latest time-point test). PK followed a non-linear pattern at all doses (Fig. 1A and B). At 72 h post-injury, the anti-CD47 antibody was detected in plasma at 2.98 ± 0.38 ug/ml, 1.20 ± 0.12 ug/ml, and 0.59 ± 0.10 ug/ml, respectively (Fig. 1C).
Since this is the first study to evaluate anti-CD47 antibody therapy for treatment of tICH, a diagnostic necropsy was performed by a veterinarian team blinded to treatment. Analysis included a complete blood count, serum chemistry panel, urinalysis, and tissues samples (heart, lung, spleen, liver, kidney, and bone). No significant differences were observed from the complete blood count (Supplementary Table S1). Serum analysis showed that the 0.5 mg/kg elicited an increase in potassium concentrations compared with 0.1 mg/kg (a p < 0.05), and an increase in total protein compared with both sham and VEH groups (Supplementary Table S2, b p < 0.05, c p < 0.05). The remaining serum analysis remained unchanged between groups. Urinalysis demonstrated some evidence of hemoglobin and leukocyte presence in the treated groups. These observations were minor and predominantly observed at higher doses. There was no significant effect of treatment on organ pathology observed.
Neurological impairment
The neuroscore was examined daily starting at 24 h post-injury. The neuroscore was converted to ranks, and two-way ANOVA was used to compare neuroscore ranks between the sham, PBBI-VEH, and PBBI-anti-CD47 cohorts. All injured groups displayed neurological impairment as evidenced by significantly elevated neuroscores (ranging from 4 to 7) within 24 h post-injury, compared with sham (p < 0.05; Fig. 2A). All injured groups, regardless of treatment, showed a progressive increase in neuroscores between day 1 and 2. However, the neurological deficit remained relatively stable between days 2 and 3 of the experiment and no significant differences were detected between treatment groups at any time-point. During the behavioral testing, the neuroscore was monitored at days 1, 3, 7, 10, and 23 (Fig. 6A). Neurological deficits remained unaffected by treatment from post-administration day 1 to day 23 (Fig. 6B).
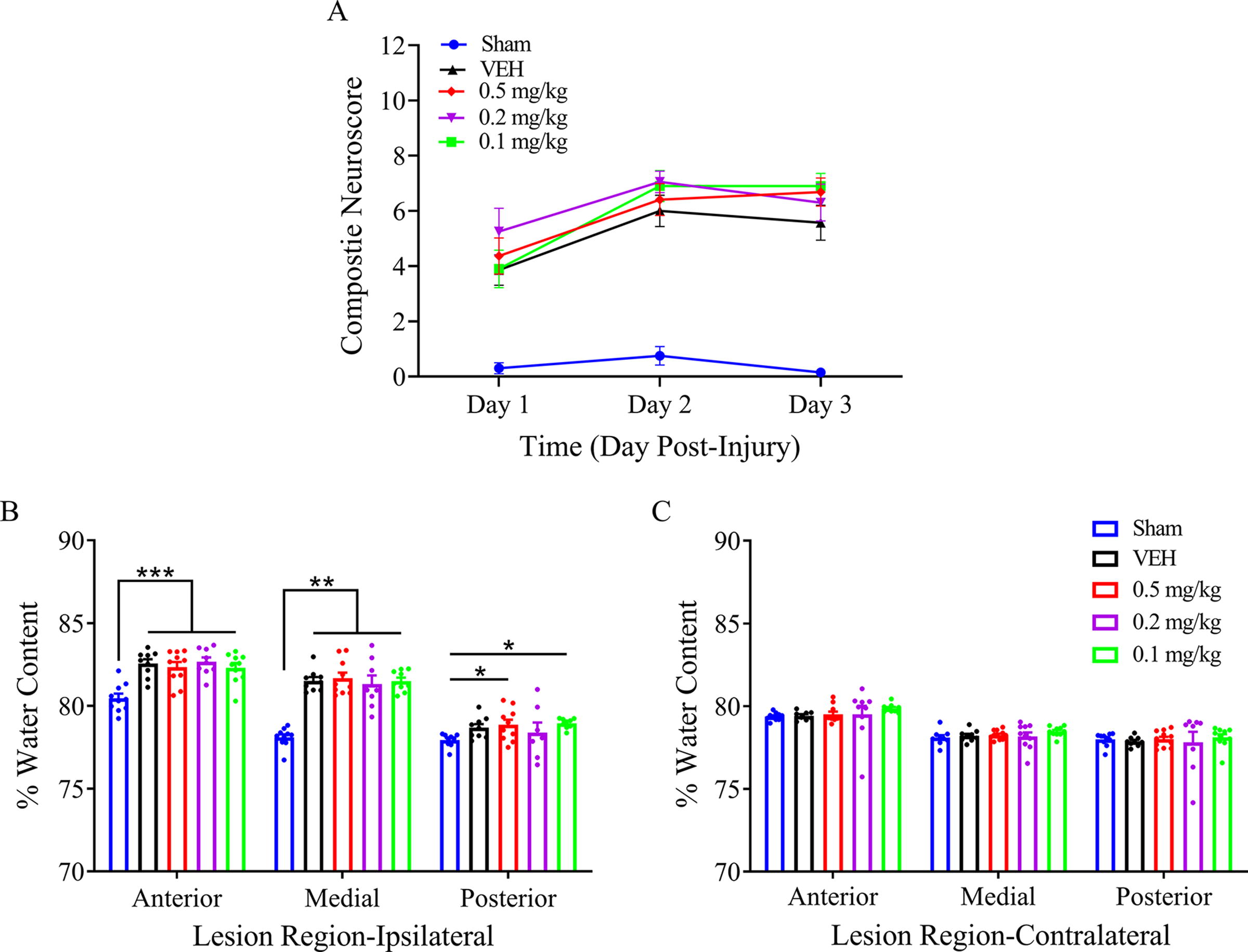
Effects of anti-CD47 antibody on neuroscore and cerebral edema following penetrating ballistic-like brain injury (PBBI). All VEH and anti-CD47 antibody treatment groups exhibited a similar degree of neurological dysfunction. Neurological deficits remained unaffected from post-injury day 1 to day 3
Cerebral edema
Cerebral edema was measured using a wet–dry method at 3 days post-injury and treatment. All injured groups, regardless of treatment, showed a significant increase in the percentage of water content, suggesting the presence of cerebral edema following injury. The edema occurred predominantly at the anterior and medial part of the ipsilateral cerebrum. No edema was detected at the contralateral cerebrum. Anti-CD47 antibody did not affect cerebral edema at 3 days post-administration at all doses tested (Fig. 2B and 2C). No significant differences were observed among treatment groups, which suggested that an increase in cerebral edema by penetrating TBI (pTBI) was not improved or exacerbated by anti-CD47 administration.
Cerebral hemoglobin levels
Intracerebral hematoma was quantified using an established ELISA at 72 h after injury by measuring cerebral hemoglobin content. 55 The VEH, 0.5 mg/kg, and 0.2 mg/kg groups all demonstrated a significant increase in cerebral hemoglobin levels compared with sham (p < 0.05). Interestingly, anti-CD47 antibody administration at the lowest dose tested (0.1 mg/kg) resulted in a significant reduction in cerebral hemoglobin levels at 3 days post-administration compared with the VEH group (p < 0.05). The cerebral hemoglobin level following 0.1 mg/kg dose was not statistically different from sham. Together, this suggests that intracerebral hematoma clearance was augmented in this group (*p < 0.05, Fig. 3).
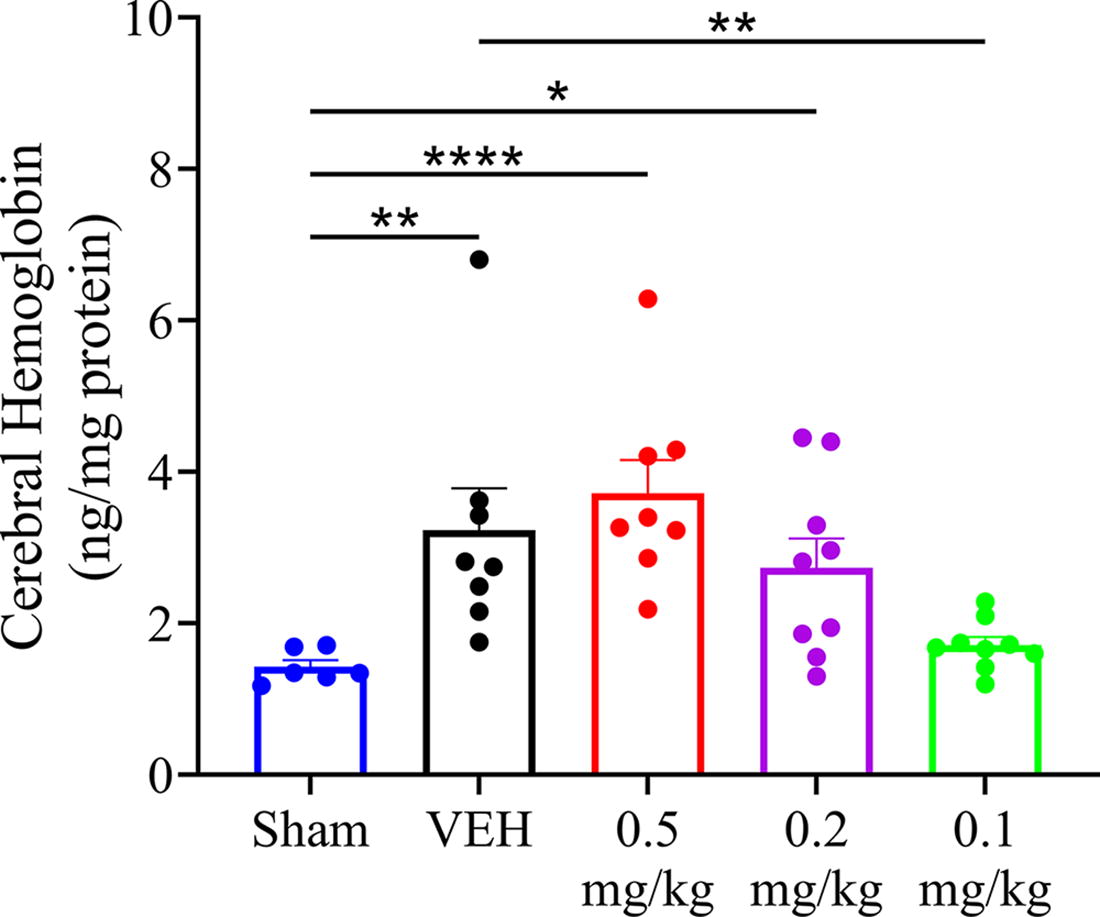
Effect of anti-CD47 on hematoma clearance. Cerebral hemoglobin levels were significantly increased at 3 days post-injury in VEH (**p < 0.01), 0.5 mg/kg (****p < 0.0001), and 0.2 mg/kg (*p < 0.05), all compared with sham. Anti-CD47 antibody administration at 0.1 mg/kg significantly reduced cerebral hemoglobin levels at 3 days post-administration (**p < 0.01) compared with VEH. There was no statistically significant difference between 0.1 mg/kg and sham groups. Data expressed as mean ± SEM. n = 6–9/group. VEH, vehicle.
Histopathology
Histological examination showed a significant reduction of GFAP levels in the lesion core at 0.1 mg/kg (p < 0.01 between control and 0.1 mg/kg groups) and peri-lesional area at both 0.1 mg/kg and 0.2 mg/kg doses (p < 0.05 between control and 0.2 mg/kg groups, p < 0.01 between control and 0.1 mg/kg groups) (Fig. 4A, 4B). There was also a significant reduction of GFAP levels detected in the striatum (ANOVA, p < 0.05 between control and 0.1 mg/kg groups) (Fig. 4A, 4C). There were no changes observed at 23 days post-administration (Supplementary Fig. S3). IBA1 levels in the lesion, peri-lesion, and striatum were not affected by treatment (Fig. 5A to 5F, Supplementary Fig. S1). Anti-CD47 antibody administration at lower dose (0.1 mg/kg) showed neuroprotective effects by reduced astrogliosis at 72 h. Immunostaining of fibrin was used to investigate the levels of clot formation. Anti-CD47 antibody showed a trending reduction of fibrin levels in the striatum at 0.1 mg/kg but this did not reach significance (Fig. 6C). There were no changes observed in the lesion, peri-lesion, cortex, thalamus, or hippocampus ROIs (Fig. 6A, 6B, 6D-6F).
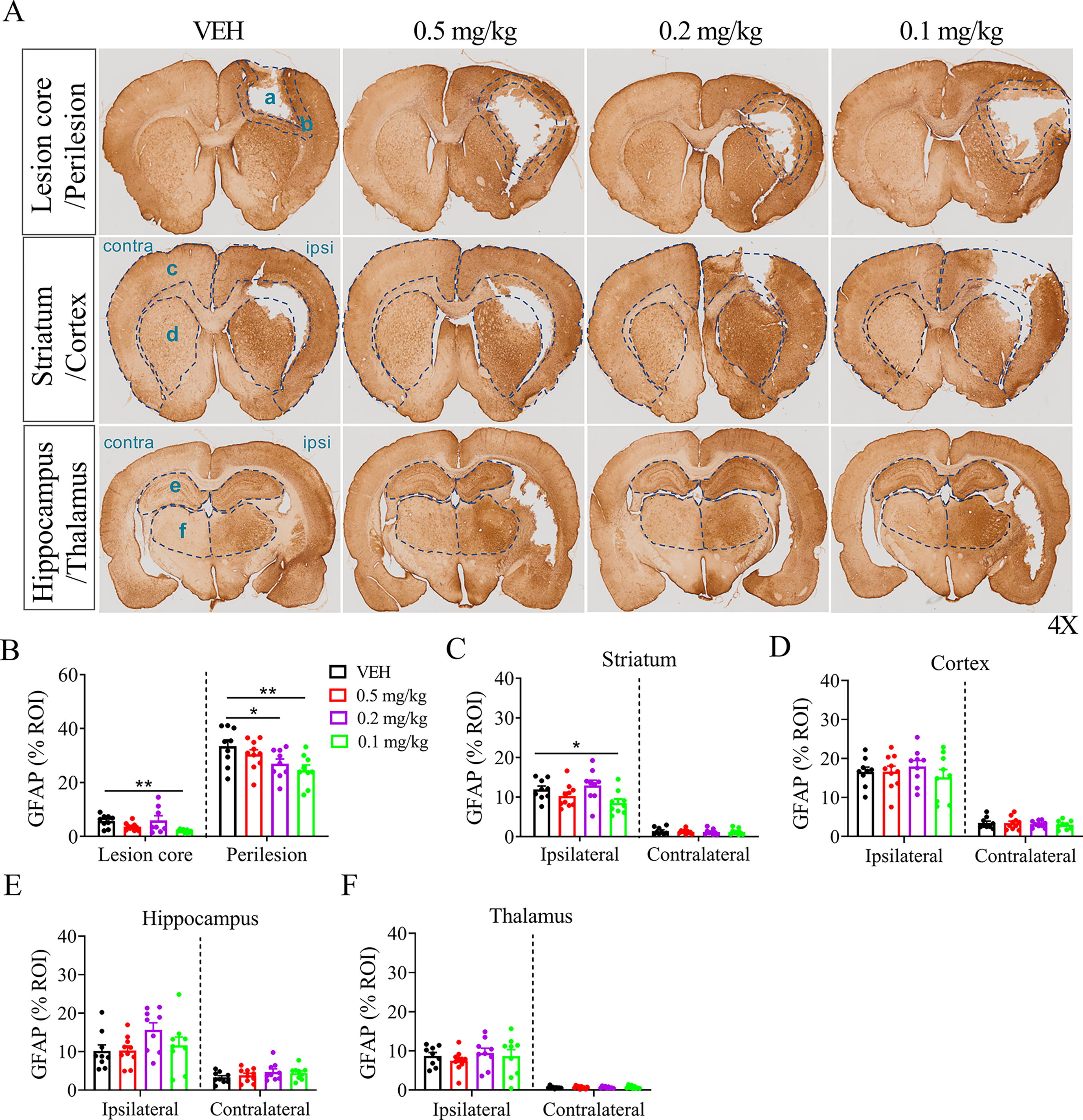
Histological assessment of GFAP demonstrated a significant reduction of GFAP levels in the lesion core (A, zone a) at a dose of 0.1 mg/kg (**p < 0.01) and peri-lesion (A, zone b) at both 0.1 mg/kg (**p < 0.01) and 0.2 mg/kg doses (*p < 0.05) compared with VEH
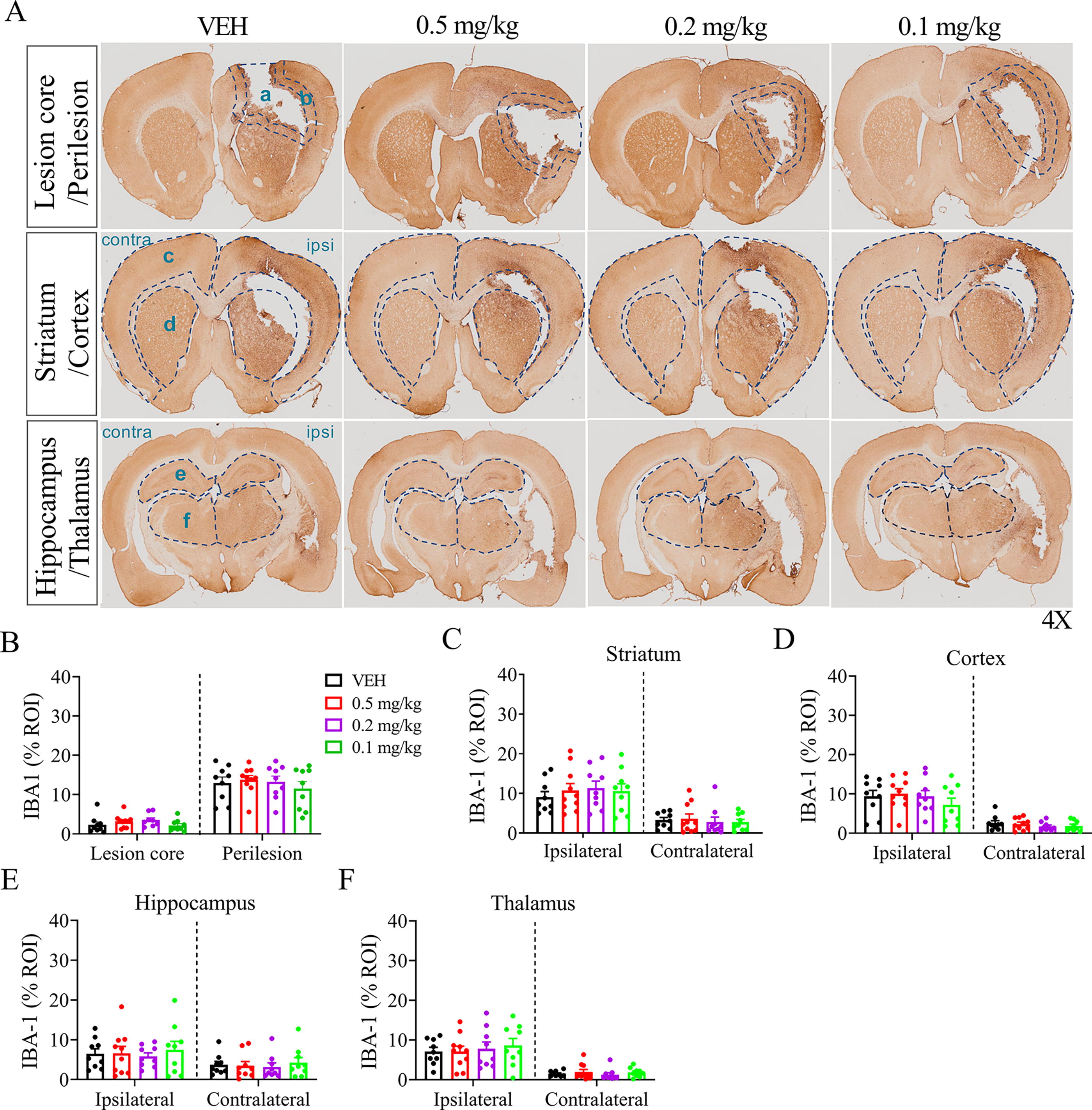
Histological assessment of IBA1 showed no significant differences in all the regions examined
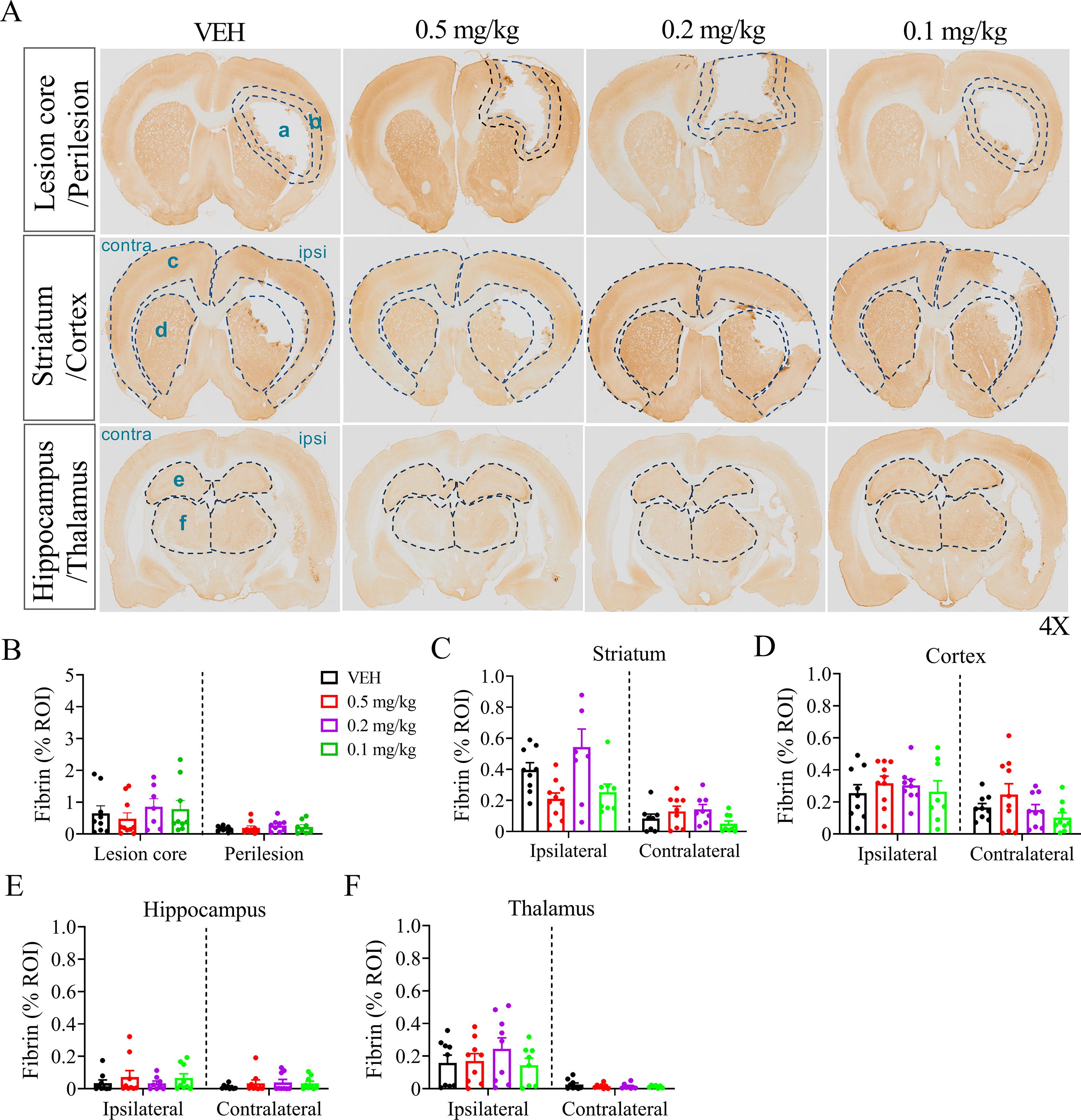
Histological assessment of fibrin showed no significant differences in all the regions examined
H&E staining was performed to assess total lesion volume between anti-CD47 antibody at 0.1 mg/kg and VEH groups at 3 days and 23 days post-administration. As expected, frontal PBBI resulted in asymmetrical brain damage to the right frontal cortex and striatum that extended to the anterior regions of the corpus callosum and caudate nucleus. Lesion volumes in anti-CD47-treated rats showed a reduction by ∼2.5% compared with the VEH-treated group that reached statistical significance (p < 0.05) (Fig. 7A and 7B). This decrease was particularly observed at the core lesion area (Fig. 7A). In addition, progression of lesion volume was also examined at 23 days post-administration (Supplementary Fig. S2A and B). Lesion volume, expressed as the percentage of whole-brain volume, changed from 12.72 ± 1.06 (at 3 days) to 8.05 ± 0.85 (at 23 days) in the VEH group. A similar trend was also observed for the antibody-treated group (0.1 mg/kg), changing from 10.18 ± 0.53 (at 3 days) to 6.88 ± 0.57 (at 23 days).

Effect of anti-CD47 antibody on lesion size. Representative images of VEH and anti-CD47-treated PBBI animals showing lesion location and progression following 3 days post-injury, and lesion volume analysis demonstrated that anti-CD47 antibody at dose of 0.1 mg/kg reduced lesion volume by 2.5%, which is calculated as the percentage of the whole-brain volume (p < 0.05 by unpaired t test)
Motor performance
Motor function was evaluated using the fixed-speed rotarod task at 7 and 10 days post-injury (Fig. 8A). A single i.v. dose of 0.1 mg/kg anti-CD47 antibody immediately following PBBI had a mild effect on motor outcomes after injury. All injured groups, regardless of treatment showed significantly reduced latency to fall compared with sham at all speeds tested (10, 15, and 20 rpm) on both testing days. Similarly, injured groups demonstrated a significant reduction in average motor score on both testing days, indicative of motor impairment following injury (**p < 0.01, *p < 0.05; Fig. 8C). Anti-CD47 antibody-treated rats tended to improve motor performance with mean motor scores increased by and on both test days, but the increases did not reach sham levels and were not statistically significant, suggesting that PBBI-induced motor deficits were not significantly improved by anti-CD47 administration.
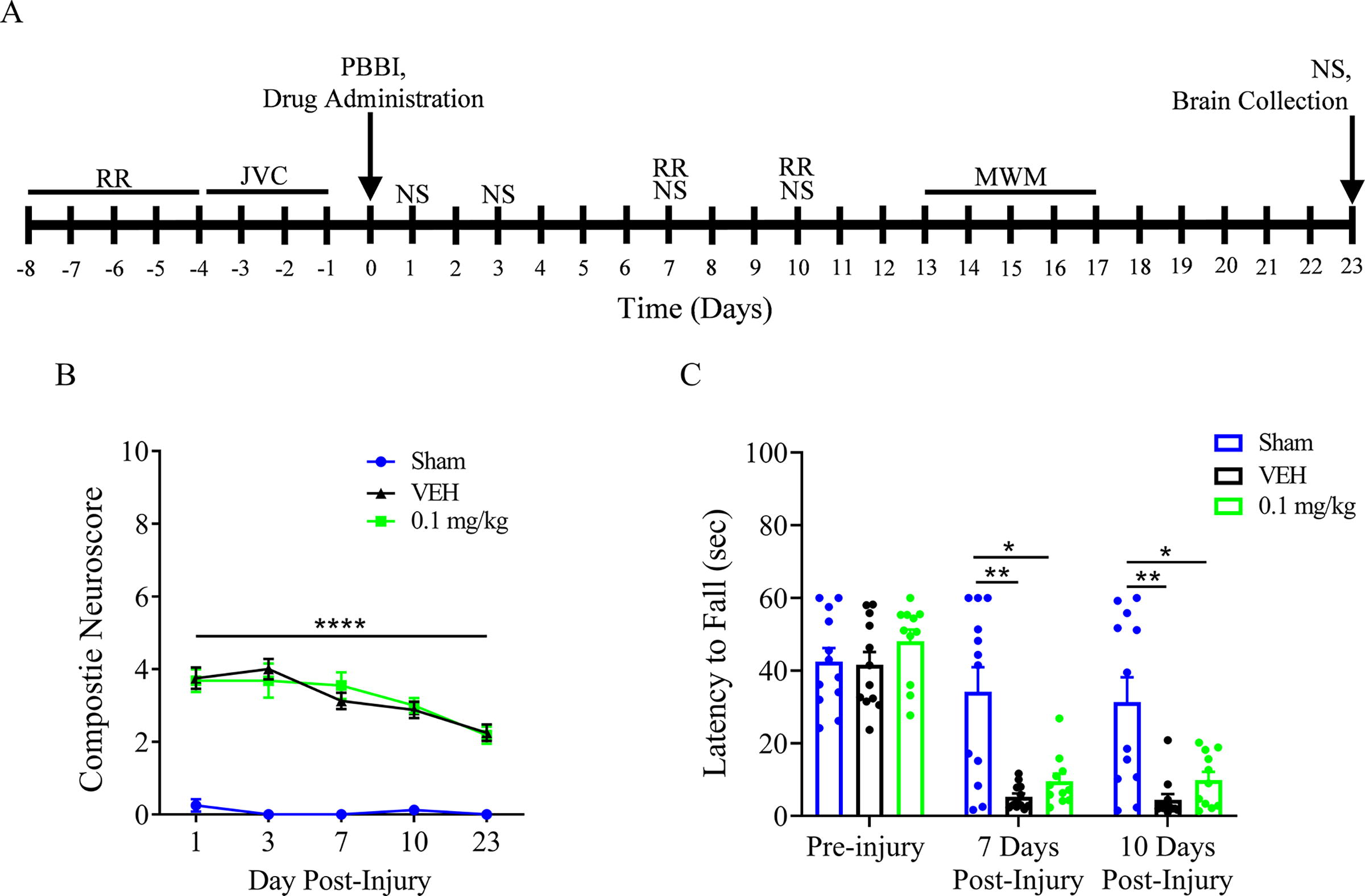
Experimental time line for motor function and cognitive performance following PBBI and anti-CD47 treatment
Cognitive function
Spatial learning, memory, and thigmotactic behavior to assess attention were evaluated in the MWM task from 13–17 days post-injury and treatment (Fig. 8A and Fig. 9A). Figure 9B shows the latency to platform for the 5-day MWM testing period. Each treatment group demonstrated a general decrease in latency across the testing days, which suggests acclimation and learning of the task. The VEH and 0.1 mg/kg groups demonstrated a significant reduction in cognitive performance compared with the sham group, which is demonstrated by the increased latency on days 13–16. On day 17, the treated (0.1 mg/kg) group demonstrated a significant improvement compared with the VEH group (p < 0.05) with no statistically significant difference between sham and 0.1 mg/kg groups, suggesting improved spatial learning.
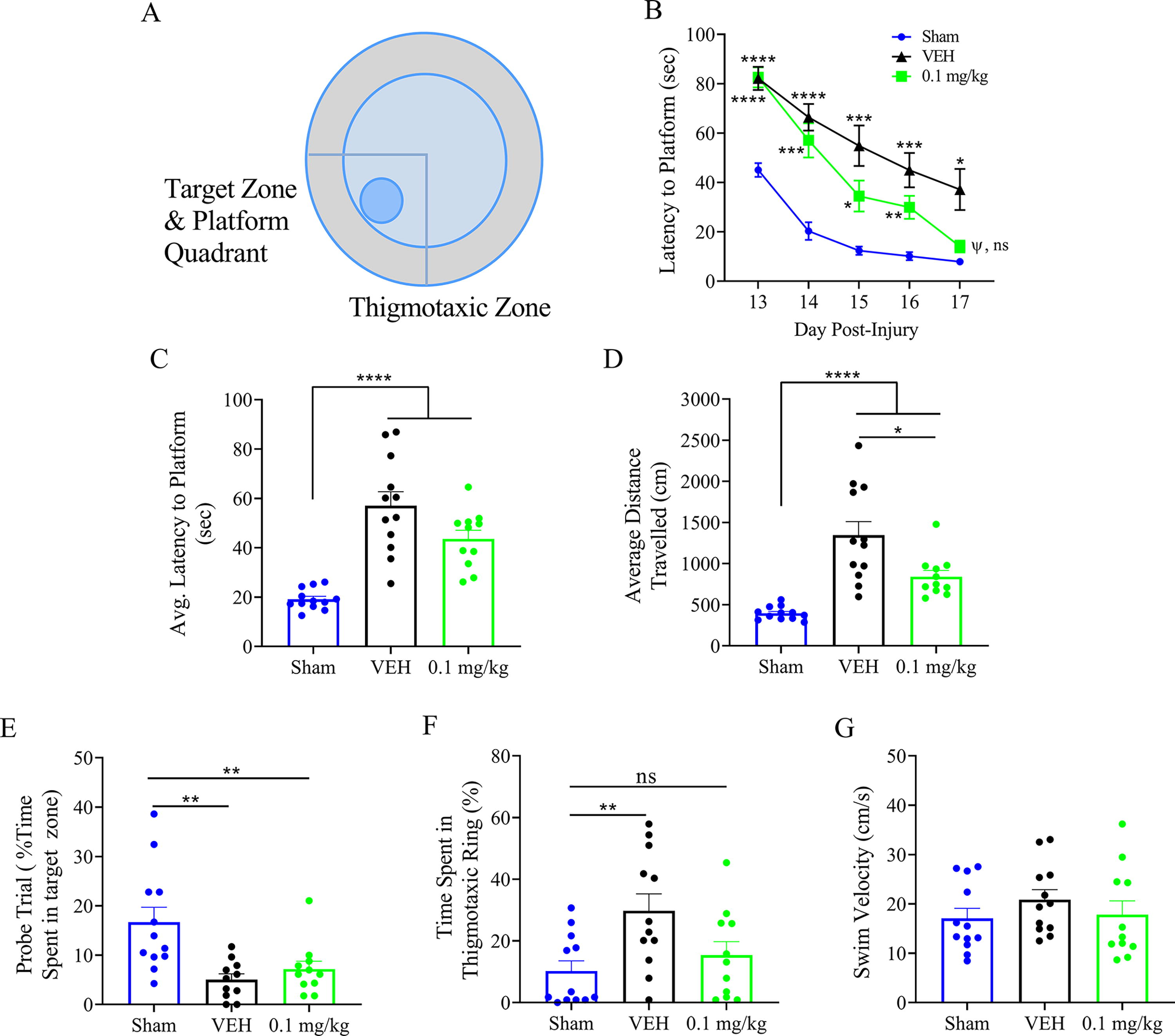
Schematic of MWM testing platform
When the cumulative performance was assessed by average latency across all testing days (Fig. 9C), a clear injury effect was observed, which was mitigated by treatment. The average latency was significantly higher in injured animals treated with VEH 38 (sec), and anti-CD47 antibody 24 (sec), compared with sham (sec; Fig. 9C; **** p < 0.0001). Rats treated with anti-CD47 antibody showed a trending reduction of average latency to find the hidden platform compared with VEH (Fig. 9C; p = 0.15). This trend was conserved in the total distance traveled during testing and was significant (Fig. 9D). The probe trial analysis showed significant injury impairments in retention scores with the time spent in the target zone decreased by approximately 12 and 10 sec, respectively (**p < 0.01, compared with sham; Fig. 9E). These impairments were unaffected by treatment. Thigmotactic swim pattern analysis showed a significant increase in the time spent in the thigmotaxis zone following PBBI (**p < 0.01, compared with Sham), and anti-CD47 antibody treatment reduced percentage of time circling the thigmotactic ring during the probe trial, which was indistinguishable to sham (Fig. 9F). There was no difference in swim speed between all groups, which may further support a lack of improved motor function (Fig. 9G).
Discussion
Surgical intervention is often indicated in the management of severe brain trauma and intracranial hematomas. This includes evacuation of space-occupying hematomas to reduce the ICP burden. While providing acute relief, previous studies have demonstrated a propensity for continued progression, which ultimately limits the effectiveness. 11,20,59,60 In addition, there are many cases where the size of the hematoma does not justify the surgical intervention and non-operative management is more appropriate via serial imaging and examinations. Therefore, identifying a therapeutic option to augment hematoma clearance may provide an adjunct therapy for surgical intervention and additional strategy for smaller hematomas that do not require surgical intervention.
This study is the first to demonstrate the therapeutic effects of i.v. anti-CD47 antibody on augmenting hematoma clearance following severe penetrating TBI in rats. Previous studies in experimental ICH models have demonstrated the therapeutic efficacy of anti-CD47 antibody administration, but these used intracerebral or intraventricular delivery. 39,43,61 The peripheral administration of the treatment adds a layer of complexity due to BBB permeability and multi-organ system involvement that causes differential effects on drug metabolism. 62,63 The results from this study demonstrate detectable levels of anti-CD47 antibodies in the plasma to at least 7 days post-administration (longest time-point tested). Despite the ubiquitous expression of CD47 on a variety of cell types and tissues, rats with penetrating TBI tolerated this antibody well presumably because normal cells are not susceptible to CD47 blockade due to the lack of pro-phagocytic signals, except for red blood cell (RBC). While there was some evidence of adverse effects on kidney function at higher doses, diagnostic necropsy revealed no severe reactions to treatment at the time-points tested. Previous study showed that brain CD47 levels are increased significantly in the perihematomal area from 4 h to 2 weeks, with a peak at 3 days following ICH in a pig ICH model. 39,43,61 The current study found therapeutic benefits at the lower dose (0.1 mg/kg), indicating that this dose is sufficient to provide a therapeutic response to erythrocyte CD47 inhibitory levels. Side effects and adverse reactions are often dose related as we observed for the higher dose in this study. Our findings are in consistency with the biphasic dose–response pattern, thus identifying optimal dose balances between efficacy and adverse effects.
In line with human data, our penetrating TBI model used in this study produced a hemorrhagic core lesion immediately after injury (<5 min), which expanded to reach maximal volumetric size between 2 h and 24 h, remained significant at 72 h post-injury, and was still present up to 7 days. 51,57,64,65 CD47 blocking antibody administered immediately after injury significantly reduced hemoglobin contents at 3 days post-TBI (Fig. 3). Both microglia and macrophages are phagocytes that function to preserve tissue integrity by engulfing old and damaged cells, including erythrocytes in the hematoma. 66,67 Therefore, microglia/macrophages play an important role in hematoma resolution 45,68 and brain injury recovery after ICH. 69 The current study found no significant changes of IBA1-positive cells in the brain regions examined at 72 h post-injury. The lack of an increase in microglia combined with an increased hematoma clearance may imply the intended effect of the drug through increased phagocytosis in the microglia that are present at the hematoma site. To truly understand the effects of microglia, further analysis should characterize cellular phenotype and combined expression of IBA1 with others, including CD68 and HO-1, to further evaluate microglia/macrophage activation.
Astrocytes are critical early responders to TBI and are intimately involved in the neuroinflammatory response. Previous studies from our group to characterize the penetrating TBI rat model have shown that astrogliosis (as indicated by GFAP staining) was apparent in the injured hemisphere 72 h post-injury. 64 Activated astrocytes release a range of proinflammatory cytokines and chemokines, which have been shown to increase dramatically within hours following TBI. 70,71 Proinflammatory cytokines activate many intracellular signaling pathways, including c-Jun N-terminal kinase (JNK), p38 mitogen activated protein kinase (p38/MAPK), and extracellular signaling-related kinase (ERK) which are involved in synaptic plasticity, 71,72 and in promoting cell death through the activation of caspases. 71,73 Neuroinflammation has been shown to play an important role in cognitive dysfunction post-TBI. 74 –78 The current study found reduced gliosis after CD47 blockade antibody treatment, which may explain the improved cognitive performance.
The secondary injury sequelae can manifest clinically as both short and long-term cognitive deficits that occur in attention, learning, and memory and higher order executive functions. 71,79,80 In our study, we observed that penetrating TBI caused significant compromise to spatial learning, memory retention, motor function, and thigmotactic behavior (Figs. 8, 9). The anti-CD47 treatment showed no effect on neurological deficit scoring, motor function, or memory retention. However, the treatment demonstrated efficacy in improving spatial learning, distance traveled during testing, and thigmotactic behavior. These improvements are likely mediated through the beneficial effects on secondary injury mechanisms, including astrogliosis, hematoma clearance, and lesion volume reduction. These results imply that the CD47-SIRPa signaling pathway may play differential roles in regulating cognitive function compared with motor function. CD47 not only functions as a switch of phagocytosis, but has also been implicated in promoting neuronal cell death in cortical neurons exposed to CD47-activating peptide, and secondary injury pathologies involving neuroinflammation and BBB dysfunction via CD47-SIRPa signaling. 46,47,81 Studies have reported modulation of CD47-SIRPa signaling pathways implicated in synaptic plasticity and (spatial) memory formation. 82 –84 The results observed here are similar to those observed from previous ICH studies using direct, local administration methods. 39,43,44,46 Therefore, we have shown that we can effectively deliver the antibodies peripherally without significant compromise to the efficacy.
There are several limitations in this study. First, the rat PBBI model used in this study was established in our laboratory in 2005, and has been well characterized regarding physiological and neurological deficits. 51,57,64,65 The experimental injury consistently produces a robust intracerebral hematoma following TBI. By comparison, minimal hemorrhage is present in other injury models. 65 The use of rodents as models of human TBI is based on the assumption that these animals phenocopy human physiology and response to treatment. However, there are marked differences in coagulation parameters between humans and rodents. Therefore, alternative animal models (such as swine) that better replicate coagulopathy in humans should be considered in our future study. Second, tICH evolves over more than a week, and only a single time-point (72 h) was characterized following injury using ELISA. Magnetic resonance imaging can track the individualized temporal progression of tICH in vivo, which will be considered in our future experiments. Moreover, gliosis reduction is associated with reduced release of cytokines and chemokines, which have been implied in synaptic plasticity and long-term potentiation (LTP), resulting in cognitive dysfunction. These will be examined in our future study. At last, a single i.v. dose may be sufficient for acute treatment, whereas penetrating TBI often cause long-term functional deficits. Thus, a repeated dosing regimen could be considered for chronic treatment.
Conclusions
In conclusion, these results provide preliminary evidence that intravenously administrated anti-CD47 antibody following penetrating TBI was well tolerated and did not cause clinically relevant adverse events. Analysis of neuropathology showed enhanced hematoma clearance, reduced neuroinflammation, and decreased lesion volume. Anti-CD47 antibody administration provides significant protection against injury-induced cognitive dysfunction. Blockade of CD47 using i.v. administration of anti-CD47 antibodies may serve as a potential therapeutic for TBI with intracerebral hemorrhage.
Footnotes
Acknowledgment
This work was supported by the Combat Casualty Care Research Program, United States Army Medical Research and Materiel Command under award number CO20009.
Author Contribution Statement
Z.S.B. designed the overall project. Z.S.B. and P.W. plan out research experiments. P.W., X.F.Y., F.Z.Y., K.C., M.H., and N.C. performed the experiments. P.W. and Z.S.B. analyzed the data and wrote the article. A.H.S. and D.A.S. reviewed and provided critical comments for the article.
Disclaimer
The material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense. Research was conducted under an IACUC-approved animal use protocol in an AAALAC International-accredited facility with a Public Health Services Animal Welfare Assurance and in compliance with the Animal Welfare Act and all other federal statutes and regulations relating to animals and experiments involving animals, and adheres to principles stated in the Guide for Care and Use of Laboratory Animals, NRC Publication, 2011 edition.
Transparency,Rigor,and Reproducibility Summary
Sample size was 9–10 rats per group, based on a priori power analyses to detect significant differences with p < 0.05 and a power of >80%. A prior power analysis was performed using estimates of means and variance from previous studies of hemorrhage following PBBI.65 Sample size was 11–12 rats per group for the behavioral assay. Therapeutic administration occurred immediately after injury. Dose–response relationship was performed using 3 doses, ranging from low to high. Animals were randomly assigned to VEH or three treatment groups using a random number generator. Investigators who performed procedures, administered the therapeutic, and performed outcome assessments were blinded to the group using identical appearing solutions labeled with A, B, C, and D. Statistical analyses were performed using an appropriate test to confirm assumptions of normality and homoscedasticity. When appropriate, transformation was applied to the data before using a non-parametric alternative.
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
This work was supported by the Combat Casualty Care Research Program, United States Army Medical Research and Materiel Command under award number CO20009.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.