
Abstract
U.S. Service members and Veterans (SM/V) experience elevated rates of traumatic brain injury (TBI), chronic pain, and other non-pain symptoms. However, the role of non-pain factors on pain interference levels remains unclear among SM/Vs, particularly those with a history of TBI. The primary objective of this study was to identify factors that differentiate high/low pain interference, given equivalent pain intensity among U.S. SM/V participating in the ongoing Long-term Impact of Military-relevant Brain Injury Consortium-Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC) national multi-center prospective longitudinal observational study. An explainable machine learning was used to identify key predictors of pain interference conditioned on equivalent pain intensity. The final sample consisted of n = 1,577 SM/Vs who were predominantly male (87%), and 83.6% had a history of mild TBI(s) (mTBI), while 16.4% were TBI negative controls. The sample was categorized according to pain interference level (Low: 19.9%, Moderate: 52.5%, and High: 27.6%). Both pain intensity scores and pain interference scores increased with the number of mTBIs (p < 0.001), and there was evidence of a dose response between the number of injuries and pain scores. Machine learning models identified fatigue and anxiety as the most important predictors of pain interference, whereas emotional control was protective. Partial dependence plots identified that marginal effects of fatigue and anxiety were associated with pain interference (p < 0.001), but the marginal effect of mTBI was not significant in models considering all variables (p > 0.05). Non-pain factors are associated with functional limitations and disability experience among SM/V with an mTBI history. The functional effects of pain may be mediated through multiple other factors. Pain is a multi-dimensional experience that may benefit most from holistic treatment approaches that target comorbidities and build supports that promote recovery.
Introduction
Chronic pain affects ∼50 million U.S. adults, ∼20 million of whom report high-impact chronic pain with disability. 1 Both the prevalence and intensity of chronic pain are further elevated among U.S. Service Members and Veterans (SM/V) with a history of traumatic brain injury (TBI). 2 –4 Pain is a multi-dimensional experience with distinct phenotypic presentations among SM/V, including the polytrauma clinical triad of persistent post-concussive symptoms, chronic pain, and post-traumatic stress disorder (PTSD), 3 –8 alongside other phenotypes such as suicidality. 9,10 In addition to pain, people with TBI also report high rates of somatic and non-somatic symptoms and pain and non-pain-related comorbidities. 9 –11 Non-pain and pain-agnostic factors commonly co-occur with pain, 6 but it is unclear how these factors may influence functional limitations among SM/Vs with TBI.
In the biopsychosocial model, chronic pain is framed as a product of multi-faceted symptoms and conditions, 12 yet pain management often treats these as unrelated factors. 6,13 –15 Similar to TBI, chronic pain conditions present with a phenotypical variance that is challenging to define. One common approach for capturing and assessing this phenotypic diversity is to classify chronic pain in terms of intensity (mild, moderate, or severe). 16,17 However, the U.S. National Pain Strategy has proposed that measures of pain intensity alone are insufficient to assess the severity of chronic pain in a clinical meaningful way, as the assessment of a patient’s functional state and disability are equally essential. 18 To address this gap, new pain interference measures were created to capture functional limitations attributed to chronic pain and classify it based on severity. 10,18 Together, the combination of pain severity and pain interference provides a better representation of the functional status of people with chronic pain, yet even emerging pain intensity and pain interference measures do not account for non-pain factors that may critically inform the functional status of people with chronic pain. 2,3
Recent studies reveal that individuals who seek care for chronic pain simultaneously report numerous non-pain symptoms. 1,2,4 –8,19 –21 Specifically, reported non-pain factors include negative affect (anger, anxiety, irritability, negative mood), cognitive symptoms (memory problems, attention and focus problems, etc.), non-pain somatic symptoms, fatigue, lethargy, low energy, and social isolation. Pain agnostic factors refer to dimensions that are not directly related to the sensory experience of pain, but can influence the overall experience and management of pain, such as other health conditions or burdens. There is evidence these may have a greater impact on the pain-related functional experience than the intensity of pain experienced. 5 –7,10,11,21 For example, in a recent study of U.S. pain patients, a graded scale of severity manifested across many non-pain symptoms. 4 Similarly, Pitcher et al. found pain with disability co-occurred with non-pain symptoms such as fatigue more than with pain intensity. 1 As SM/Vs with history of TBI are at elevated risk for a wide range of pain- and non-pain-related comorbidities, further investigation of the role of non-pain/pain-agnostic factors 6 is needed in this population. 9,15,22 –24
The goal of this study was to identify and characterize non-pain and pain agnostic factors associated with pain interference conditioned on equivalent pain intensity in a sample of SM/Vs with mild TBI (mTBI) history. Machine learning models were trained to predict pain interference, given pain and non-pain factors, and validated on test data not used in model training. We hypothesized that non-pain symptoms would have a greater association with the experience of pain-related functional limitations than pain intensity alone.
Materials and Methods
Parent Study: This study analyzed data collected at the enrollment visit for the Long-term Impact of Military-relevant Brain Injury Consortium-Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC) multi-center Prospective Longitudinal Study (PLS). The PLS is an ongoing multi-center cohort of current and former U.S. SM/Vs with combat exposure and measurement of lifetime mTBI. Participants were enrolled at 11 Veterans Affairs (VA) and military health care complexes.
Briefly, the overall PLS objective is to answer questions about the long-term effects of combat deployment and mTBI. At the baseline visit after enrollment, all participants undergo comprehensive assessment that includes structured interviews, neuropsychological testing, symptom inventories, and biometrics. Participants are primarily recruited through mass mailings, TBI care clinics, and non-paid advertisements. All individuals aged 18 years or older with a history of combat exposure are eligible.
Exclusions included history of moderate-to-severe TBI or major neurological or psychiatric disorders, such as spinal cord injury and schizophrenia, that reduce independence. The PLS was approved by the local Institutional Review Boards at each site. All participants provided written consent before procedures. More details of the LIMBIC-CENC PLS objectives and methods have been previously described. 25 –27
Sample Selection: Participants enrolled in the PLS as of 2022 were included (n = 2,069), except for those excluded by the following criteria: (1) non-credible symptom profiles (n = 167) as determined by the mild brain injury atypical symptoms scale 10 and/or (2) answered “I have no pain or discomfort” on the EuroQol-5D pain item 6 (n = 326). These criteria resulted in n = 1,577 eligible SM/Vs. The resulting sample included those with and without a history of mTBI.
All included measures were classified into one of the following five categories: (1) Demographics and military occupational measures; (2) pain measures; (3) support measures (i.e., factors broadly protective against pain interference); (4) measures of physical and mental health burdens (e.g., headache, sleep problems, depression, anxiety); and (5) neurobehavioral symptoms. 28 –30
TBI, demographics, and military occupational measures
Lifetime mTBI History was measured by the number of lifetime mTBIs determined through a structured interview and standardized process described more fully elsewhere. 31 Final diagnostic determinations adhered to the VA and DoD (Department of Defense) common definition of mTBI 32 and the American Congress of Rehabilitation Medicine. 33 The mTBI definition involved classification according to evidence of a physiological disruption of brain function as a result of a traumatic event manifested by at least one of the following: alteration of mental state, loss of consciousness, loss of memory, or focal neurological deficit, where the severity of the injury does not exceed standard mTBI criteria.
Demographics and Health Comorbidities: Standardized demographic data and self-report of select comorbidities were collected at baseline using the Behavioral Risk Factor Surveillance System (BRFSS). 34
Military Occupational: Self-reported military descriptive variables included military status, service branch/division, total number of months on combat deployments, and combat intensity measured using section D of the Deployment Risk and Resiliency Inventory 2 (DRRI-2). 35
Pain measures
Pain Interference, the primary outcome, was measured with the TBI quality of life (QOL) pain interference short form score. 36 Scores ranged from 10 to 50, with a higher score indicating greater interference of function by pain (i.e., more dysfunction). The pain interference scale is the sum score of ten items that ask the examinee to quantify on a 5-point scale how much pain interferes with one aspect of their life, such as memory, socialization, and family life. We used thresholds established in prior work classifying the following three levels of pain interference 37 : Low/insignificant (scores from 10 to 14), Moderate (scores from 15 to 29), and High pain interference (scores ≥30).
Pain Intensity, the primary conditioning variable, was derived from the NIH Toolbox Cognition Battery, 38 which asks “In the past 7 days; how would you rate your pain on average?” with responses ranging from 0 = No pain to 10 = Worst pain imaginable. We classified pain intensity responses into the following three groups: None/low (scores from 0 to 3), Moderate intensity (scores between 4 and 6), and High intensity (scores ≥7).
Headache Impact Test (HIT-6): The six-item HIT-6 assesses how episodic and chronic migraine impacts the individual. HIT-6 assesses headache pain on a scale of 0 to 10, with 0 representing “No pain” and 10 representing “Pain as bad as it can be.” Prior work indicated the total HIT-6 score is positively correlated with headache pain severity (r = 0.46) and pain-related disability scores (r = 0.56). 39
Support measures
General Health was derived from the general health measure on the BRFSS. 34 The item assesses patient reported level of general health on a 5-point Likert scale, and scores were inverted so that higher scores indicated better health (1 = Poor; 5 = Excellent).
General Self-Efficacy (GSE) was derived from the sum score of the 10 self-reported items on the general self-efficacy questionnaire. 40 The GSE asks about the ability to solve problems and accomplish goals. Each response is measured on a 5-point Likert Scale (1 = Not at all true; 5 = Exactly true); scores range from 10–50.
Post-Deployment Social Support: A measure of level of social/family support in daily life after deployment was derived from the sum of the 10-item DRRI2 post-deployment social support scale (Section O). 35 Each item is measured on a 5-point scale (1 = Never; 5 = Always). Total scores range from 10 to 50.
Emotional Control: A measure of emotional regulation/control was derived by inverting the 10-item TBIQOL toolbox scale evaluating emotional dyscontrol. 41 The scale assesses disinhibition, emotional lability, irritability, impatience, and impulsiveness. Responses were inverted so that higher scores indicated better overall emotional control; total scores range from 10 to 50.
Cognitive Functioning: An objective measure of cognitive function 42 was taken from the NIHTB, which measures overall cognitive functioning. Scores were age-adjusted with a median normed to 100.
Measures of health burden
PTSD symptom severity was measured by the PTSD Checklist (PCL) for DSM-5 (PCL-5). PCL-5 scores are the sum of 20 items on 5-point Likert scales, and total scores range from 0 to 80. 43
Depressive Symptoms were measured with the Patient Health Questionnaire-9, a 9-item self-report measure of depression symptoms in the last 2 weeks with total scores from 0 (None) to 27 (Severe). 44
Anxiety, Fatigue: Measures of anxiety and fatigue were both derived from the 10-item TBIQOL Anxiety and Fatigue short-form item banks, which have both been previously linked to existing anxiety and fatigue measures. 30 The scales evaluate anxiety and fatigue-related interference in everyday life and range from 10 to 50.
Sleep Complaints: Subjective sleep quality was measured using the Pittsburgh Sleep Quality Index; 45 and sleep apnea risk using the STOP-BANG questionnaire with high risk classified as STOP-BANG ≥ 3. 46
Neurobehavioral Symptoms: Neurobehavioral symptoms were measured using the Cognitive, Affective, Somatosensory, and Vestibular subscales of the Neurobehavioral Symptom Inventory. 47
Statistical analysis
All analyses were scripted in Python 3. p values and 95% confidence intervals (95% CI) were calculated using the statsmodels python package. Logistic regression was used to estimate odds for moderate pain interference conditioned on pain intensity and other sociodemographic and military measures. High collinearity was observed between explanatory variables. Therefore, random forest models (RFMs) were used in the primary analysis due to their resistance to collinearity. 48 For radial plots, all variables were normed to the scale of 0–100 by using the following formula: scorenorm = 100 × (score−min)/(max−min) to facilitate visual comparison.
RFMs were constructed using the scikit-learn package, with n = 1000 trees, and a maximum of 10 variables observable per tree. Feature importance was used to determine the effect of variables on the model regressed on pain interference scores. Prediction in this context referred to the output of a model forecasting the likelihood of the outcome. RFMs were trained and evaluated using 50/50 test train splits. Random splits were repeated 40× for cross-validation to determine the 95% confidence interval on feature importance, and p-values were estimated by permuting sample indices and comparing the variance explained under random versus true indices.
Partial dependence plots (PDPs) were used to infer the marginal effects of variables on outcome predictions given all other data “as reported.” 49 PDPs can identify directionalities and nonlinearities between variables and outcomes. For example, if all individuals reported no anxiety at all (but all other variables were otherwise “as recorded”), how might pain interference levels change? To build a PDP, we intervene on one variable, keeping all others the same, and measure how model predictions change. First, a model is fit to the true data, which captures the true data relationships. This model then estimates the outcome scores using the altered data sets. We specifically model how pain interference scores change as each variable is “swept” across its full range, with all other variables unchanged.
Results
Table 1 summarizes the sociodemographic characteristics and key exposures of the SM/V cohort broken out by pain interference groups (see the Methods section). The average number of prior mTBIs was higher among those with higher pain interference (p < 0.001). The high pain interference group had almost double the rate (p < 0.001) of deployment-related mTBI (72.1%) compared with the low pain interference group (38.5%). The high pain interference group also reported more than double the average scores on symptom measures frequently associated with TBI (PTSD, depression, headache, and pain intensity) relative to the low pain interference group.
Sociodemographic Characteristics and TBI Exposure for Low, Moderate, and High Pain Interference Groups
Characteristics of Pain Interference Groups: Both pain intensity and pain interference scores increased with the number of mTBIs (p < 0.001, Fig. 1a), suggesting a dose response in the association between pain and brain injury history. Pain intensity scores and pain interference scores were correlated (r = 0.59), although individual pain interference levels varied widely within each pain intensity level (Fig. 1b).
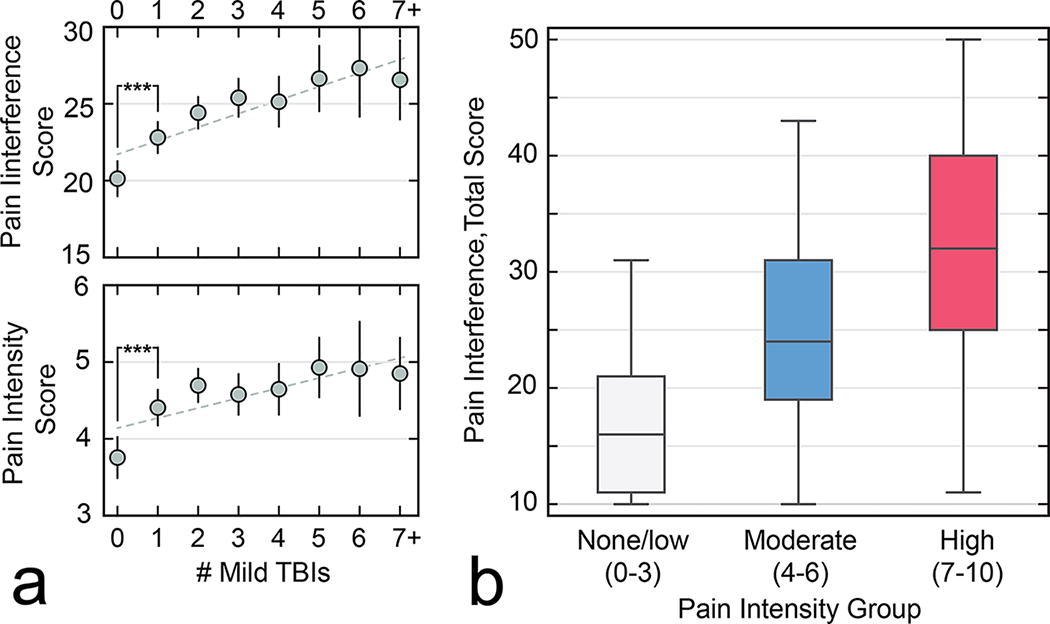
Figure 2 presents a radial plot visualizing physical and mental health burdens and comorbidities (black), support measures (green), and neurobehavioral symptom complaints (blue) broken out by TBI status group (Fig. 2a) and pain interference group (Fig. 2b). When compared with the TBI-negative group, those with a positive TBI history reported significantly more burdens and complaints (p < 0.001). Similarly, compared with the low pain interference group, the high interference group (Fig. 2b, red) reported significantly more burdens and complaints (p < 0.001). Higher pain was also associated with lower scores in family, social, health, and objective cognitive measures (p < 0.001), indicating that pain interference was associated with several non-pain factors.

Radial plots visualizing physical and mental health burdens (black), protective supports (green), symptom complaints (blue), and pain measures (gray), broken out by
Modeling Pain Interference: Logistic regression was used to estimate odds for moderate pain interference or above conditioned pain intensity and other sociodemographic and military measures (see Supplementary Fig. S1). The number of mTBIs was significantly associated with higher pain. However, high collinearity precluded multivariate logistic modeling of burdens, supports, symptoms, and pain. Figure 3 illustrates the importance of factors for modeling pain interference using RFMs. Measures of fatigue, anxiety, pain intensity, and PTSD symptom severity (all symptoms and conditions commonly associated with TBI) were the most important features associated with pain interference (p < 0.001). Lower pain interference scores were associated with support measures overall (p < 0.001), with emotional control, cognitive ability, and social support being the most protective. Among demographic covariates, age and deployment history showed appreciable and independent importance when predicting pain interference.
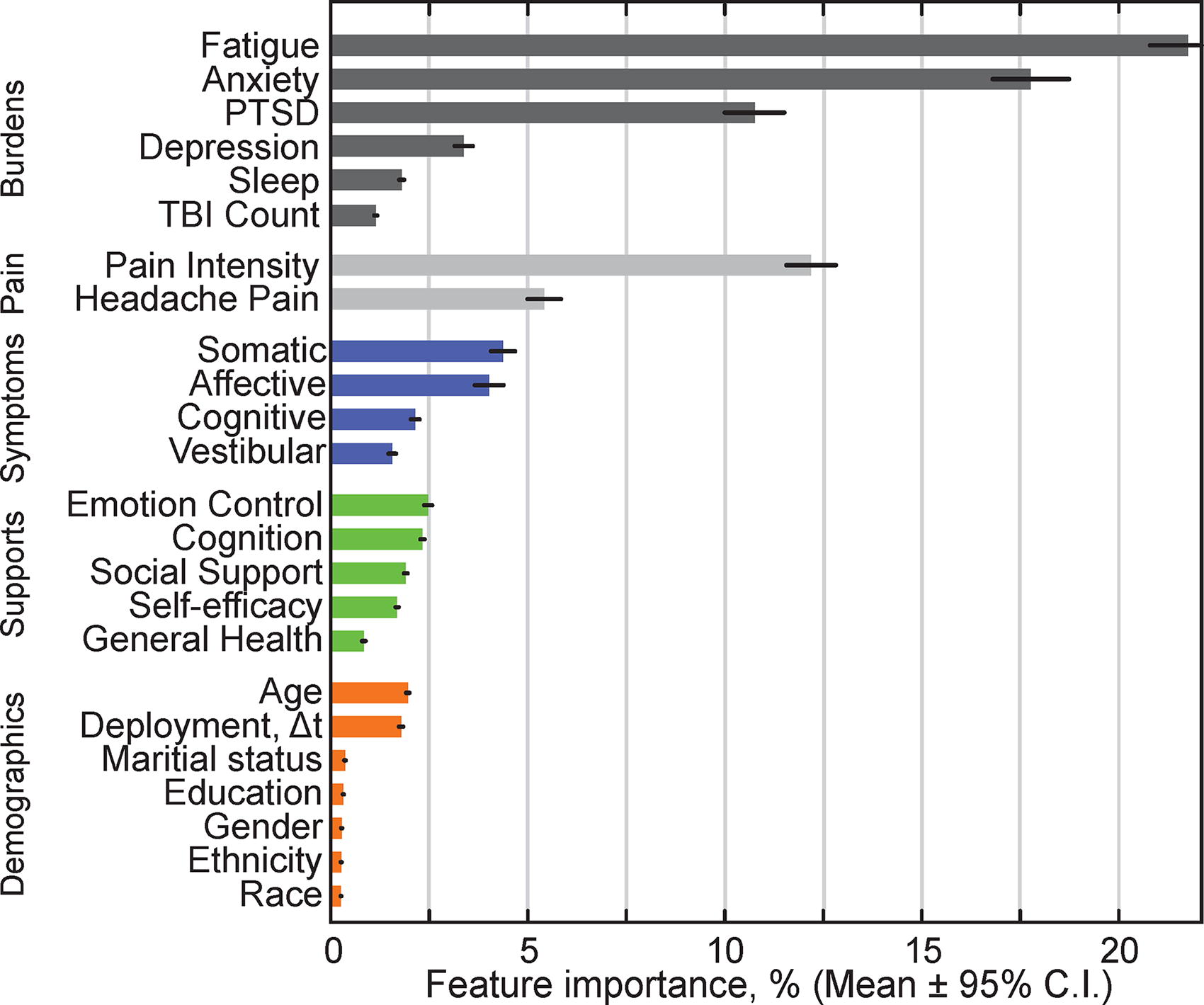
Predicting pain interference. Bar graph showing random forest feature importance for variables predicting pain interference scores for n = 1,577 post-deployment SM/Vs. When all other variables were included in models, number of mild TBIs showed only a small feature importance (1.2%, p < 0.01). At the other extreme, both fatigue and anxiety were individually more important when predicting pain interference than pain intensity (black bars: 95% confidence intervals, Δt: Time since, Race: White, Black, Asian, other). SM/V, U.S. Service members and Veterans.
Marginal Effects: PDPs were used to estimate marginal effect of each variable on pain interference given real, equivalent pain intensities and all other variables “as reported” (Fig. 4). The marginal effects of the highest feature importance burden and support variables are shown in Figure 4 on the left (i—Fatigue, ii—Emotional control). For the pain variables (iii, iv), a significant discontinuity was evident at pain intensity of 4 and above, which is an established clinical cutoff. Only HIT-6 headache scores above 55 were associated with pain interference. The second- and third-most prominent burdens (Fig. 4, v—anxiety and vi—PTSD) were associated with higher pain. The marginal effect of TBI count was not significant when all other variable values were included “as reported” (Fig. 4 iii, <0.01 score per additional mTBI).

Partial dependence plots showing the marginal effect of six variables on pain interference scores (gray areas: 95% confidence intervals). With all the other variables and symptoms “as reported,” number of TBIs had a minimal effect of pain interference (middle, top). Conversely, the marginal effects of fatigue, pain intensity, anxiety, headache pain, and PTSD were all significantly associated with higher pain interference scores. Marginal increases in emotional control were significantly associated with lower pain interference. PTSD, post-traumatic stress disorder.
Discussion
Chronic pain among SM/Vs with TBI often arises as part of a multi-dimensional symptom and multi-morbidity experience. This study examined how variations in non-pain symptoms, comorbidities, and support factors were associated with pain interference in a sample of previously combat-deployed SM/V with and without TBI. The results of this analysis showed that SM/Vs reporting higher pain interference levels also report a significantly greater burden of non-pain symptoms and medical conditions when accounting and adjusting for pain intensity. Both pain interference and intensity increased with the number of mTBIs, but importantly, pain scores tended to be more strongly associated with the chronic symptoms associated with TBI than with the injury history themselves. This suggests TBI-type symptomology may be more influential for functional status than injury history and characteristics. Most strikingly, fatigue and anxiety were even more important predictors of pain interference than pain intensity, suggesting that non-pain factors play a critical role in the functional limitations of chronic pain after TBI.
A recent study that focused on comorbid depression, sleep problems, and anxiety also reported that fatigue had a stronger correlation with the outcome of health care costs and wage loss than pain intensity. 4 Similar to persistent pain, persistent fatigue can significantly interrupt daily life. Future work could investigate whether and how fatigue combined with pain intensity exacerbates functional limitations among people with chronic pain. 50,51 Figure 1 identified a strong, direct association between the number of mTBIs and pain intensity and interference scores. In marginal effects models, the TBI association with pain was reduced, which instead operated primarily through other TBI-related symptoms. Conversely, TBI-related symptoms such as fatigue, headache, and anxiety showed strong marginal relationships.
Our results are congruent with the biopsychosocial conceptualization that pain interference is defined by a collective effect that involves non-pain comorbidities, psychosocial distress, and the availability of protective supports. 6,13,15 This contribution is the first to examine how the collective experience of non-pain factors is an important part of the phenotypes that distinguish pain interference subtypes. Although social factors may be intractable, social support was associated with lower levels of pain interference, suggesting potential targets for treatment and management with social support that helps individuals lead a better life with social stressors.
Our results also highlight the challenges involved in the treatment of chronic pain in the context of SM/Vs with mTBI histories. It is challenging to identify which among many factors is the primary driver of reduced functional status. For example, fatigue can be a shared symptom of several comorbidities, or a secondary effect of pharmacotherapy. Providers assessing patients with pain should carefully determine how the patient’s pain experience is mediated by additional non-pain factors. At the same time, addressing every symptom using a traditional prescription medication approach can easily lead to polypharmacy and overtreatment, 52 and several of these symptom experiences, such as fatigue, lack effective treatments. Polytrauma, such as the combination of TBI, chronic pain, and PTSD, poses additional challenges, 53 –56 and this work supports a complex clinical picture where fatigue, anxiety, PTSD, emotion control, and cognition all play a role in the relationship between pain intensity and pain interference. 55
It may be that the combination of pain and several non-pain symptoms represents an injury recovery response of the body to mobilize the whole person in response to threats as a means to promote long-term healing. 57 For example, fatigue is not only a signature of distress but is also present during healing and recovery. 57 If pain and non-pain symptoms are a physiological recovery response, how is it that they can persist maladaptively without improvement, as is often the case for Veterans with post-concussive symptoms and related syndromes. Resolving how the body responds to perceived threats may yield benefits.
The primary diagnostic entities identified in this work, anxiety and depression, can have bidirectional relationships with pain. However, the relationship between pain and the symptoms of anxiety and depression remains less understood. Although the relationship between pain and fatigue is more ambiguous, pain can precede fatigue or exist concurrently. Beyond these singular framings, this work suggests that non-pain symptoms are not separate experiences with causal or temporally specific pathways, but are concurrent or synchronous syndromal experiences. 57 By illuminating the specific role of non-pain factors in the threat response process, future work could glean valuable new insights into the nature of pain phenotypes and disability. More generally, future work could benefit from exploring the interplay between pain and TBI in ways that consider factors such as the environmental context and sex differences in response to TBI. 58
Strengths and limitations
The strengths of this study included a large longitudinal sample of deployed Veterans with well-characterized lifetime TBI exposure who were assessed by a comprehensive evaluation, including multiple related health measures. Machine learning models were used to minimize the influence of collinearity among pain and non-pain factors, and a partial dependence framework was used to strongly condition the research question on a wide range of covarying factors, including pain intensity. There are several limitations that should be considered when interpreting these results. Pain intensity is a highly subjective variable and pain interference was self-reported. The current study analyzes data from combat-exposed SM/Vs with high rates of mTBI and may not generalize to non-combat-exposed individuals or the civilian population.
Conclusion
This study of combat SM/Vs with high rates of mTBI exposures and TBI-related symptoms assessed how pain and non-pain factors contribute to pain interference. TBI history was associated with both pain interference and pain intensity. However, in fully adjusted models considering multiple chronic effects of injury, the marginal effect of TBI on pain interference was no longer significant. Instead, the original TBI association with pain operated through other factors. Among these, the most influential factors for predicting pain interference were fatigue, anxiety, pain intensity, and PTSD, respectively, whereas emotional control was protective against pain interference. The effect of these variables persisted in marginal effects models. We confirmed our hypothesis and identified potentially impactful targets for reducing pain interference beyond pain intensity. This work suggests that self-reported pain that interferes with life among combat SM/Vs with TBI is a multi-dimensional experience not adequately captured by measures of pain alone. Addressing pain may benefit from care that more broadly incorporates the renewal of health through the treatment of comorbidities, and the enhancement of emotional and social supports in pain management.
Transparency, Rigor, and Reproducibility
This study was approved by the local Institutional Review Boards at all eight PLS enrollment sites. Consent to participate: All study participants signed the informed consent document before undergoing study procedures. Consent for publication: the consent form signed by all participants included consent for publication of their deidentified data. All LIMBIC-CENC PLS study data used for this investigation are available upon request to eligible investigators. For more information about using LIMBIC-CENC PLS data, visit https://www.limbic-cenc.org. All codes and scripts used for this investigation are available from the corresponding author upon reasonable request.
Footnotes
Authors’ Contributions
E.K. wrote the original article and acted as the primary investigator, and all authors contributed to the review and editing of the article. W.C.W. was responsible for the LIMBIC PLS design, data acquisition, and procedures. M.J.P. provided oversight and supervision for the study. E.K., A.M., and M.J.P. conceptualized the primary research question. Formal analysis was conducted by E.K. Data curation was conducted and overseen by H.M.
Author Disclosure Statement
The author(s) have no competing interest to disclose. The views, opinions, interpretations, conclusions, and recommendations expressed in this article are those of the authors and do not reflect the official policy of the Department of the Navy, Department of the Army, Department of Defense, Department of Veterans Affairs, or the U.S. Government.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.