
Abstract
Balance and mobility problems are common consequences after mild traumatic brain injury (mTBI). However, turning and nonstraight gait, which are required for daily living, are rarely assessed in clinical tests of function after mTBI. Therefore, the primary goals of this study were to assess (1) the added value of clinic-based turning task variables, obtained using wearable sensors, over standard general assessments of mobility, and (2) assess the associations between general assessments of mobility, objective variables from clinic-based turning tasks, and ecologically relevant functional tasks. Fifty-three civilians with mTBI, 57 healthy civilian controls, and 36 healthy active-duty military controls participated across three sites. Participants were tested in a single session that encompassed self-reported questionnaires including demographic information and balance and mobility testing including the use of wearable sensors. Lasso regression models and the area under the receiver–operator characteristic curve (AUC) assessed diagnostic accuracy. Partial correlation coefficients assessed the relationship between each variable with ecologically relevant functional tasks. Multivariate models revealed high diagnostic accuracy, with an AUC of 0.92, using multiple variables from instrumented clinic-based turning tasks. The complex turning course (CTC) yielded the highest multivariate AUC (95% confidence interval [CI]) of 0.90 (0.84, 0.95) for a single task, and the average lap time from the CTC had the highest univariate AUC (95% CI) of 0.70 (0.58, 0.78). Turning variables provided added value, indicated by higher AUCs, over standard general assessments of mobility. Turning variables had strong associations with ecologically relevant functional tasks and outperformed general assessments of mobility, though there were slight differences in the relationship based on civilian versus military population. Clinic-based turning tasks, especially the CTC and modified Illinois Agility Test (mIAT), have high diagnostic accuracy, strong associations with ecologically relevant functional tasks, and require relatively short time(s) to complete. Compared to general assessments of mobility, clinic-based turning tasks may be more ecologically relevant to daily function. Future work should continue to examine the CTC and mIAT alongside other promising tools for return-to-activity assessments.
Introduction
Balance and mobility problems are common consequences after mild traumatic brain injury (mTBI), with variable presentations depending on the specific cognitive, motor, and sensory demands of the task as well as personal and injury factors of the individual with mTBI. 1,2 Consequently, results from objective assessments of balance and mobility are important clinical tools that can inform rehabilitation prescription and track recovery over time. While extensive literature on dual-task (DT) gait, where mobility tasks are combined with a simultaneous cognitive task, demonstrates diagnostic utility in people with mTBI, 3 –8 these tasks are often limited to straight-line walking and artificial cognitive tasks such as serial three subtraction. Other multifaceted batteries such as the Functional Gait Assessment (FGA), 9 High-level Mobility Assessment Tool (HiMAT), 10,11 4-Item Hybrid Assessment of Mobility for mTBI (HAM-4-mTBI), 12 and mini Balance Evaluation Systems Test 13 include a variety of tasks, but the majority of individual items within these assessments similarly focus on straight-line walking. Recent work on developing complex and ecologically relevant tasks such as the Assessment of Military Multitasking Performance, 14,15 and the Portable Warrior Test of Tactical Agility (POWAR-TOTAL) 16 indicate complex tasks that are relevant to battle drills may contribute to return to duty decisions in the military. Similar tasks that identify issues with key components of everyday mobility, such as those involving nonstraight walking and turning, may also provide important information about function in a targeted fashion.
Ambulatory turning is an important characteristic of daily mobility as individuals inevitably must navigate through complex environments that do not permit straight-line travel. Video-based analyses of activities of daily living suggest that 40% of all steps are nonstraight steps involving some degree of turning. 17 Stable turning requires anticipatory postural control, 18 asymmetrical loading across limbs, 19 dynamic reweighting of sensory information to account for time-varying gravitoinertial accelerations, 20,21 and sequential rotations of the head, trunk, pelvis, and feet to reorient to the new direction of travel. 22 –24 These characteristics of turning are unique from straight gait, and models of mobility should include turning as an independent factor. 25,26
Preliminary work in a sample of individuals with persisting balance-related symptoms after mTBI (i.e., chronic mTBI) demonstrated slower turning speeds and more variable head-on-body coordination when walking along a complex turning course (CTC) simulating turns performed in daily life. 27 Other studies have reported abnormal balance control during turning in otherwise asymptomatic athletes recovering from mTBI. 28 When selecting an optimized set of clinical items from the FGA and HiMAT, the gait with pivot turn test item from the FGA was one of only four test items retained for use in populations with chronic mTBI. 12 These studies suggest assessments of turning may have clinical value in populations with mTBI. 29,30 However, the clinical value of turning may depend on the specific demands, instructions, and outcomes of the turning task. For example, tasks requiring faster turning speeds can elicit more severe symptoms due to greater rates of change in visual and vestibular sensory stimulation, 31 –33 and this provocation of symptoms may affect performance. Other methodological considerations, like the sharpness of the turn angle, 27 the height of objects such as cones versus lines on the ground outlining the course, 34 or the cognitive complexity and modality of the task, 35 can similarly affect turning behavior.
The need for objective measurements of turning becomes evident due to the limitations of self-report questionnaires and the often subtle and diverse ways mTBI can manifest. 4,36 –40 For instance, instrumented sway from the modified Clinical Test for Sensory Interaction in Balance reveals balance abnormalities where clinical ratings show normal function after mTBI. 41 Clinical scales that include turning, such as the Berg Balance Scale, 42 often have ceiling effects and may not detect subtle deficits after mTBI, especially in highly fit and athletic populations. 36 In contrast, instrumented measures of turning, such as peak velocity and segmental coordination across various turn angles, provide reliable measures capable of detecting subtle deficits without relying on subjective visual ratings. 43 Both the Veterans Affairs/Department of Defense (VA/DoD) Clinical Practice Guideline for the Management and Rehabilitation of Post-acute mTBI 44 and Sixth Consensus Statement on Concussion in Sport, 45 recommend multimodal screenings that include gait, with the VA/DoD guidelines specifically calling for the evaluation of “walking, tandem walking, walking with head turns, and whole-body turning.” The clinical recommendations for including gait, especially turning and DT measures, in mTBI screenings underscore the importance of such measurements, and emphasize the need for objective tools that can detect residual and subtle deficits.
Beyond diagnostic accuracy, the degree to which objective measures of turning reflect a patient’s ability to return to activity (RTA), such as work, military duty, or sport remains unclear. This association with real-world function is particularly relevant for rehabilitation decisions that must determine whether subtle residual deficits after mTBI impact one’s readiness for duty, work, or sport. In military populations, where an individual must be able to perform warrior tasks and battle drills such as moving under fire, reacting to contact, and maintaining situational awareness, performance on such duty-relevant tasks is essential to maintain combat effectiveness and ensure survival for themselves and their fellow service members. Common general measures of mobility such as the FGA and HiMAT may not represent the demands imposed by daily work, life, sports, or specific warrior tasks (urban assault, movement to contact, etc.) that require complex multi-segmental coordination while under cognitive load. 46,47 The clinical utility of turning metrics is jointly determined by the diagnostic accuracy and association with real-world mobility and for military personnel, combat readiness.
Therefore, the first goal of this study, 39 was to assess diagnostic accuracy—the added value of objective turning measures over standard, general assessments of mobility in identifying individuals with symptomatic mTBI. We expected that variables from clinic-based turning tasks would have better diagnostic accuracy for identifying individuals with mTBI, as indicated by a greater area under the receiver–operator characteristic (ROC) curve (AUC) compared to general measures of mobility such as self-selected gait speed, FGA, and HiMAT. The second goal of this study was to support the validity of the turning variables and assess the associations between general measures of mobility (e.g., gait speed, FGA, and HiMAT) and clinic-based turning tasks with performance in a community ambulation task (CAT) and a military-relevant simulated urban patrol (SUP) task, which are steps toward ecologically valid assessments and designated as ecologically relevant functional tasks with face validity in this study. We hypothesized that objective turning variables obtained during the clinic-based turning tasks would be more strongly associated with performance in ecologically relevant functional tasks compared to performance in general measures of mobility. Finally, we sought to provide recommendations on the best turning tasks and variables for future clinical implementation based on the diagnostic accuracy, added value, and association with the ecologically relevant functional tasks.
Materials and Methods
Participants
As part of the ReTURN study protocol (ClinicalTrials.gov: NCT03892291) 39 a total of 53 civilians with mTBI, 57 healthy civilian controls, and 36 healthy active-duty service member controls (Table 1) were recruited from May 15, 2019, to March 26, 2022, across four sites (Oregon Health and Science University, Portland, OR; University of Utah, Salt Lake City, UT; Courage Kenny Research Center—Allina Health, Minneapolis, MN; Joint Base San Antonio—Fort Sam Houston, TX). Inclusion criteria for those with mTBI were: (1) have a diagnosis of mTBI made by a physician according to the VA/DoD diagnostic criteria, 44 (2) be between 18 and 50 years of age, and (3) be outside of the acute stage (>3 weeks postconcussion) but within 3 years of their most recent mTBI and still reporting symptoms. As turning can involve vestibular, ocular, and cognitive functioning, participants were not restricted based on the type or subtype of symptoms. Control participants either had no history of mTBI or were more than 3 years removed from their most recent mTBI and had no reported residual symptoms. Potential participants were excluded if they: (1) had a history of any other injury, medical condition, or neurological illness that could potentially impair their balance (i.e., lower extremity injury, recent surgery, and stroke), (2) had a current substance abuse disorder, (3) were pregnant, or (4) were unable to communicate in English. The study was conducted in accordance with the Declaration of Helsinki (1964) and approved by the institutional review board at each of the sites. Informed written consent was obtained prior to participation. Data from civilians were used to assess the diagnostic accuracy of turning outcomes. Data from both civilians and military service members were used to assess the associations between general measures of mobility and clinic-based turning tasks with ecologically relevant functional tasks.
Demographic Characteristics for 53 Civilians with Mild Traumatic Brain Injury, 57 Healthy Civilian Controls, and 36 Healthy Military Service Member Controls Reported as Mean (SD) Unless Otherwise Noted
This sample is part of a larger study (37)—the civilian subjects included here are identical to the subjects included in other studies. 48 –50
Reported as median (min-max).
Seven of 57 healthy civilian controls and 6 of 36 healthy military service member controls had a remote history of concussion.
Reported as n (percentage).
DHI, dizziness handicap inventory; NSI, neurobehavioral symptom inventory.
Procedures
Participants completed one testing session that encompassed self-reported questionnaires including demographic information and symptom checklists, neurocognitive testing, and balance and mobility testing including the use of wearable sensors. 39 For the purposes of this study, only the mobility procedures are further described in detail.
Clinic-based turning tasks
Participants completed three clinic-based turning tasks in a randomized order (Fig. 1): (1) a one-minute walk test (1 MW) that involved walking at a comfortable pace between two lines on the ground marked 6 m apart and included 180° turns, (2) a modified Illinois Agility Test (mIAT) that involved running at a maximal safe speed around cones with multiple turns (end, slalom, and mid), and (3) a 140-sec walk around a CTC designed to mimic turns performed in daily life, which involved walking at a comfortable pace around 45°, 90°, and 135° turns. Each of the three turning tasks was completed twice (once under single-task [ST] and another time under DT conditions). The cognitive component for the 1 MW and mIAT DT conditions was an 8-digit alpha-numeric grid coordinate memorization task that was introduced within the context of a civilian geocaching activity. 15 The cognitive overlay for the CTC DT condition involved monitoring and responding to keywords in a custom-developed simulated radio chatter task designed to mimic the demands of military service. 14,15
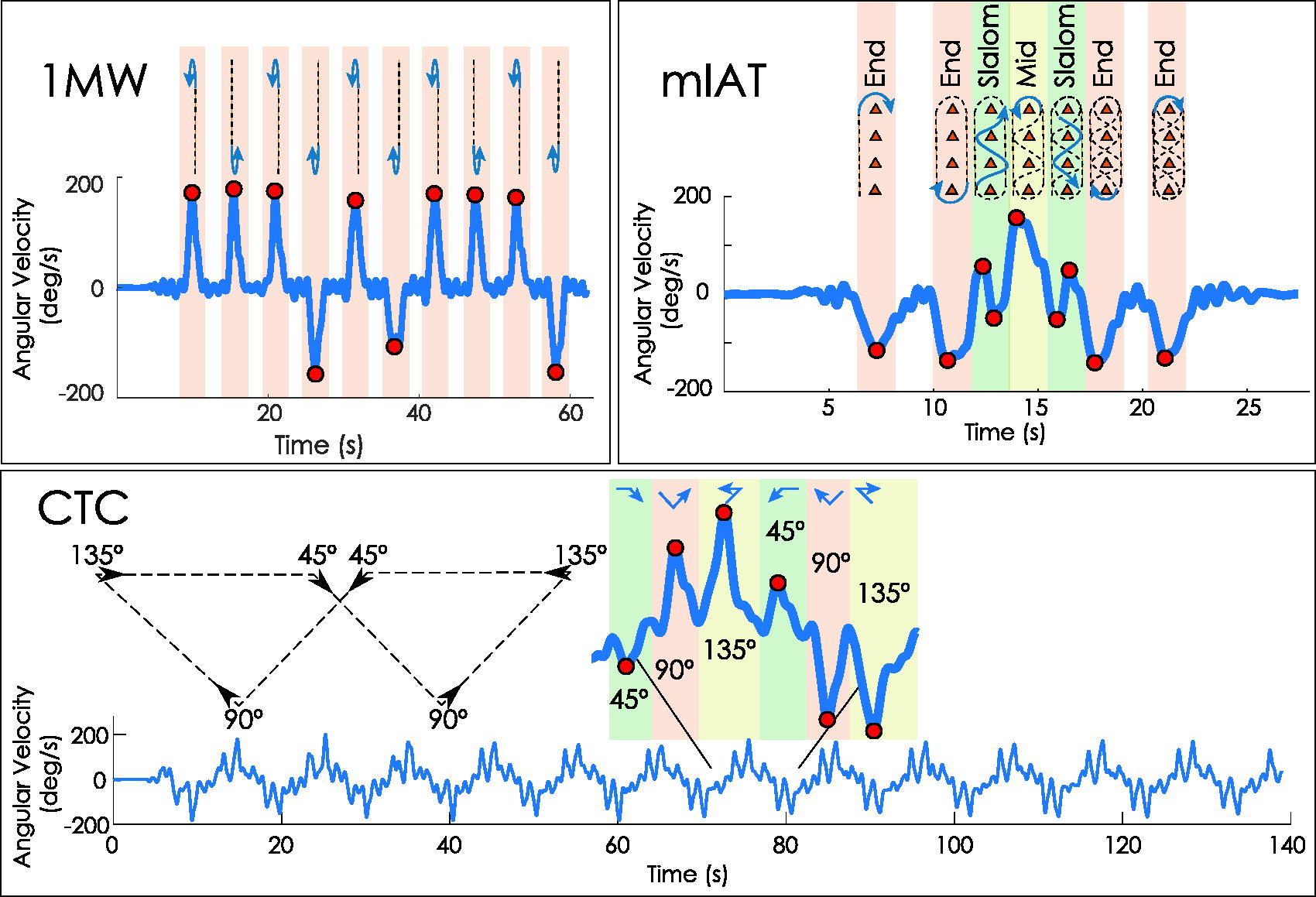
Schematic of the three clinic-based turning tasks with individual turns marked. Turn angles for the complex turning course (CTC) are with respect to straight walking.
General measures of mobility
In addition to the clinic-based turning tasks, participants completed two standard clinical assessments to obtain general measures of mobility including the FGA 9 and the HiMAT. 10 These two clinical assessments were completed and scored based on standard instructions.
Ecologically relevant functional tasks
The CAT involved participants walking at their self-selected pace while navigating through a building following landmark-based directions (e.g., “walk down the hallway toward the black doors”). Instructions were provided verbally by a researcher who walked 3–5 feet behind the participant to avoid affecting the pace of the participant. The CAT was unique to each site, but all took approximately 6–7 min to complete and contained a standardized set of components common to everyday ambulation (i.e., turns, stairs, use of signage).
The SUP involved navigating a small, subdivided room containing light emitting diode (LED) targets representing hostile (red) and friendly (blue) targets. The room was constructed using polyvinyl chloride (PVC) pipe and 2.44 m tall black fabric walls. The LED targets were constructed using an Adafruit Circuit Playground Express circuit board (Adafruit Industries, LLC; New York, NY) programmed to display red or blue LEDs and to respond to an infrared LED signal from a laser-tag weapon (Model T1504, Dynasty Toys, Inc., Yorba Linda, CA, USA). Upon “tagging” the targets with the laser-tag weapon, the targets were programmed to turn off. If a friendly target was tagged, the target was programmed to turn white. Three hostile targets were programmed to require multiple shots to fully clear—the target would illuminate 2/3 of the red LEDs (1/3 cleared) after one shot, 1/3 of the red LEDs (2/3 cleared) after two shots, and no LEDs (fully cleared) after three shots. Ten total targets were displayed in the subdivided room.
Using a laser-tag weapon, participants were instructed to clear all hostile targets as quickly as possible without tagging friendly targets. Participants were given one practice trial where all targets were set to hostile (red). Following the practice trial, three SUP trials were completed and recorded. The location of the targets was fixed throughout the test, but the configuration of each target (hostile vs. friendly) was changed between trials and each participant experienced the same order of trials and target configurations.
Data analysis and outcome measures
Clinic-based turning tasks
During all clinic-based turning tasks, inertial measurement units (128 Hz; APDM, a Clario Company, Portland, OR, USA) on the forehead, sternum, lumbar spine, and bilateral feet collected tri-axial acceleration and angular velocity data. During each of the turning tasks, peak angular rates for each segment, segmental coordination, and overall speed (e.g., lap times) were obtained from the inertial sensors using previously defined algorithms. 43,51 Briefly, body-fixed yaw angular velocities were extracted from each 1 MW, mIAT, and CTC test and filtered using a 1.5 Hz low-pass phaseless Butterworth filter. Specific turns for the mIAT and CTC were identified using a template-based approach based on the prescribed path, 51 and each turn variable was matched to each turn type (slalom, mid, and end turns for mIAT; 45°, 90°, and 135° turns for CTC). Speed variables (PeakHeadV, PeakTrunkV, and PeakLumbarV) were defined as the peak angular rate of each segment (head, trunk, and pelvis, respectively). Intersegmental coordination variables (Lumbar2Head, Lumbar2Trunk, and Trunk2Head) were defined as the difference in time between peak angular rates of two segments where positive values indicate the superior segment led the inferior segment (e.g., a Lumbar2Head value of +100 indicates the head reached its peak velocity 100 ms before the pelvis reached its peak velocity for a given turn type). 27 Since each task included multiple turns across each turn angle, variables were averaged within each turn angle. In addition to these measures, the task completion time for the mIAT, the average lap time for the CTC, and the variability (standard deviation) of lap time for the CTC were retained as variables. Therefore, all processing yielded a total of 6 variables (3 speed + 3 coordination) for the 1 MW, 19 variables (9 speed + 9 coordination + 1 completion time) for the mIAT, and 20 variables (9 speed + 9 coordination + 2 lap times) for the CTC. The greater number of variables for the mIAT and CTC was due to three different turn angles compared to only one turn angle (180°) for the 1 MW. Prior work has demonstrated these variables are reliable (test–retest intraclass correlation coefficients ranging from 0.52 to 0.91) 43 and can be equivalently measured across sites. 51
Additional exploratory variables were also examined for each task. These exploratory variables included measures of head turn symmetry, range of motion, and variabilities of peak turning speed and intersegmental coordination. Head turn symmetry was defined as the ratio of the peak turning speed of the head during turns to the left divided by the peak turning speed of the head during turns to the right. Head range of motion was defined as the difference between the 95th percentile and 5th percentile of the head-on-trunk angle, obtained through cumulative trapezoidal integration (cumtrapz function in MATLAB) of the head-on-trunk angular velocity, over the duration of the entire trial. The variabilities of peak turning speed and intersegmental coordination variables were defined as the standard deviation of each outcome within a given trial. This yielded a total of 152 different turning variables. A list and description of all variables are provided in the Supplementary Data (Supplement A).
General measures of mobility
Clinical outcomes of FGA total score and HiMAT total score were calculated for each respective battery. The four-item HAM-4-mTBI was calculated from the FGA and HiMAT using the individual item scores of walk with pivot turn, walk with horizontal head turns, fast forward walk, and fast backward walk. 12 In addition, to capture a traditional measure of self-selected walking speed, straight-path gait speed was extracted from the ST and DT 1 MW tests using validated and automated Mobility Lab software (APDM, a Clario Company, Portland, OR, USA).
Ecologically relevant functional tasks
Performance on the CAT was quantified as the total time to complete the course. Performance on the SUP was quantified using a throughput score (total accuracy score/total time), where points were awarded based on the Comstock method that allows for unlimited rounds, but heavily penalizes shooting the wrong target (i.e., shooting a friendly target is twice as bad as missing a hostile target). Each trial, therefore, had a total of possible points (possible points = 2 * [number of friendly targets] +1 * [number of hostile targets]) and an accuracy score (accuracy score = Possible points −2 * [number of tagged friendly targets] −1 * [number of untagged hostile targets]).
52
The final measure for performance on the SUP was the total throughput, defined as the sum of the total points divided by the sum of trial times (
Statistical analysis
To determine the diagnostic accuracy of turning outcomes to discriminate between civilian healthy controls and civilians with mTBI, we first conducted a variable reduction procedure on all 152 primary and exploratory variables using lasso regression with 10-fold cross-validation to minimize the model deviance. Next, we constructed separate logistic regression models for each variable retained by the lasso regression to investigate the AUC for each turning variable individually. Then, we constructed ROC curves for (a) the lasso model including all retained variables and (b) the univariate logistic regression model considering each retained variable separately. For each ROC curve, we calculated the AUC and the 95% confidence interval (CI) of the AUC using bootstrapping with 10,000 iterations.
Since it is possible that retained variables all originate from separate tests (i.e., 1 MW vs. mIAT vs. CTC), we further investigated the diagnostic accuracy of individual tests by running three separate lasso regressions, each with the same 10-fold cross-validation to minimize model deviance. Each lasso regression model included only variables from a single test (e.g., 1 MW vs. mIAT vs. CTC), but included both ST and DT conditions. AUCs and 95% CIs were generated for each test using the same process described above.
To determine if turning outcomes have added value over standard clinical assessment batteries, forward stepwise logistic regression models were implemented using each clinical assessment as the base predictor. Variables were added to the base model in order of their univariate AUC (highest AUC added first). Separate models were fit for each clinical assessment (FGA, HiMAT, gait speed). Stopping criteria were determined using the Akaike information criteria (AIC). AUC values and 95% CIs were determined from the final model using bootstrapping with 10,000 iterations. To help interpret the clinical value of changes in AUC between the initial (Base) model and the final added value (Base+n) model, the maximum sensitivities and specificities were calculated for each model at the optimal cut-point defined by the minimum of the index of union function. 53
To assess the capacity of objective turning measures to predict performance in the ecologically relevant functional tasks (CAT or SUP) in both civilians and service members, partial correlation coefficients assessed the linear relationship between each variable and the performance outcome for the CAT (completion time) and SUP (throughput score) while adjusting for age, body mass index, sex, mTBI status, and site. Partial correlation coefficients were assessed in the combined sample (civilians and service members) and separately by civilians and service members. A 0.05 significance level with Benjamini–Hochberg false discovery rate correction, 54 was used throughout.
Results
Descriptive statistics for each variable and tests for between-group differences are presented in the Supplementary Data (Supplement B).
Diagnostic accuracy
A total of 22 of the possible 152 turning variables were retained following the lasso regression (Fig. 2). The multivariate lasso model yielded an AUC (95% CI) of 0.92 (0.85, 0.96). Of the 22 retained turning variables, the average lap time during the ST CTC had the single largest AUC (95% CI) of 0.70 (0.58, 0.78). When lasso models were run as individual tests, the model initially including all 1 MW outcomes yielded an AUC (95% CI) of 0.71 (0.61, 0.81) with six variables retained in the final model, the mIAT yielded an AUC (95% CI) of 0.78 (0.69, 0.86) with eight retained variables, and the CTC yielded an AUC (95% CI) of 0.90 (0.84, 0.95) with 16 retained variables (Fig. 3). Variable inflation factors for each model are reported in the Supplementary Data (see Supplement C).

Areas under the receiver–operator characteristic curve (AUC) for the final lasso model (black) and univariate AUCs for each term included in the lasso model. Univariate AUCs are presented in different symbols for the type of variable (circle = speed, triangle = segmental coordination), different colors for the different tests (blue = complex turning course, yellow = modified Illinois Agility Test, red = one-minute walk test), and different fills for single- or dual-task (filled shape = single-task, empty shape = dual-task). Whiskers indicate the 95% confidence interval for each AUC.
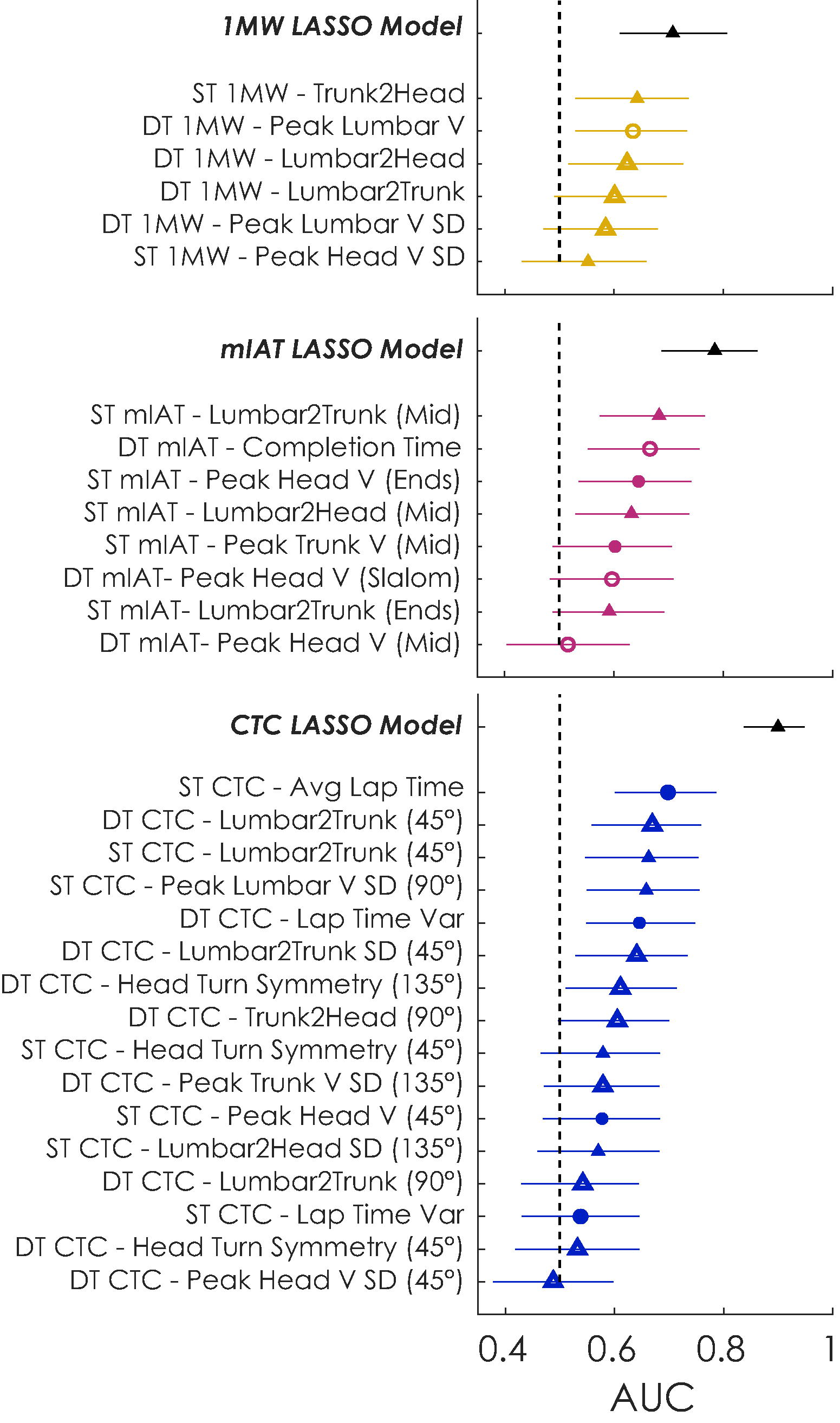
Areas under the receiver–operator characteristic curve (AUC) for the lasso models for individual tests. Each panel includes the final lasso model (black) and univariate AUCs for each term included in the lasso models. Univariate AUCs are presented in different symbols for the type of variable (circle = speed, triangle = segmental coordination), different colors for the different tests (blue = complex turning course, yellow = modified Illinois Agility Test, red = one-minute walk test), and different fills for single- or dual-task (filled shape = single-task, empty shape = dual-task). Whiskers indicate the 95% confidence interval for each AUC.
The added value of clinic-based turning tasks
The forward stepwise logistic models achieved stopping criteria (local minimum in AIC) after three turning variables for the FGA, HiMAT, and HAM-4-mTBI models (Table 2). The model based on the FGA achieved a final AUC (95% CI) of 0.80 (0.70, 0.87). The model based on the HiMAT achieved a final AUC (95% CI) of 0.79 (0.70, 0.86). The model based on the HAM-4-mTBI achieved a final AUC (95% CI) of 0.81 (0.73, 0.88). Stopping criteria were achieved after the addition of four turning variables for ST and DT gait speed, with final AUCs (95% CI) of 0.82 (0.72, 0.88) and 0.82 (0.73, 0.89), respectively. Comparatively, the AUC (95% CI) was 0.68 (0.57, 0.77) for the FGA, 0.65 (0.53, 0.74) for the HiMAT, 0.71 (0.61, 0.80) for the HAM-4-mTBI, 0.63 (0.52, 0.74) for ST gait speed, and 0.64 (0.53, 0.75) for DT gait speed. When adding the turning variables, sensitivity and specificity at the optimal cut-point increased for all tasks: 3.8% and 21.1%, respectively, for the FGA; 5.7% and 12.3%, respectively, for the HiMAT; 7.6% and 15.7%, respectively, for the HAM-4-mTBI; 5.6% and 21%, respectively, for ST gait speed, and 18.9% and 8.9%, respectively, for DT gait speed. At the optimal cut-points, the final FGA model had 64.2% sensitivity and 79.0% specificity, the final HiMAT model had 64.2% sensitivity and 79.0% specificity, the final HAM-4-mTBI model had 75.5% sensitivity and 75.4% specificity, the final ST gait speed model had 69.8% sensitivity and 80.7% specificity, and the final DT gait speed model had 77.4% sensitivity and 73.2% specificity.
Results of the Area Under the Receiver–Operator Characteristic Curve from the Stepwise Logistic Regression Models to Evaluate the Added Value of Turning Variables Over Standard Mobility Assessments
Base models included the Functional Gait Assessment (FGA), high-level mobility assessment tool (HiMAT), 4-item hybrid assessment of mobility for mild traumatic brain injury (HAM-4-mTBI), single-task (ST) gait speed, and dual-task (DT) gait speed. Each model included the following terms added, in order, to the base model: average lap time for the ST complex turning course (CTC); lumbar-to-trunk coordination during the middle turn on the ST modified Illinois Agility Test (mIAT); lumbar-to-trunk coordination during 45° turns of the DT CTC; and completion time for the DT mIAT.
Association with ecologically relevant functional tasks (CAT and SUP)
Descriptive statistics for the CAT and SUP are presented in the Supplementary Data (Supplement D). Better performance on the CAT was significantly associated with faster overall lap times of the ST and DT CTC across all participants (|r| = 0.39, p < 0.0001 and |r| = 0.35, p < 0.0001, respectively) and faster peak turning speed of the sternum and lumbar spine during the 1 MW and CTC tasks (|r| = 0.24–0.35, p < 0.05; Fig. 4 and Table 3). Instrumented measures from ST and DT straight gait were similarly associated with CAT completion time (|r| = 0.40, p < 0.05), with DT gait speed having the strongest association. Performance on the CAT was not significantly associated with performance on the FGA, HiMAT, or HAM-4 (|r| = 0.13–0.21, p > 0.05). However, these associations appeared to vary based on the population; there were stronger associations between ST and DT CTC completion times and CAT performance in civilians (|r| = 0.47–0.53) compared to military service members (|r| = 0.00). Similarly, ST and DT gait speed had notably stronger associations with CAT performance in civilians (|r| = 0.46–0.51) compared to in-service members (|r| = 0.02–0.18).

Partial Pearson correlation coefficients for each turning variable obtained from the complex turning course (CTC), modified Illinois Agility Test (mIAT), and one-minute walk test (1 MW) with completion time on the community ambulation task (CAT; left) and simulated urban patrol (SUP; right). Correlation coefficients are shown in different symbols for the type of variable (circle = speed, triangle = segmental coordination), different colors for the different tests (blue = complex turning course, yellow = modified Illinois Agility Test, red = one-minute walk test), and different fills for single- or dual-task (filled shape = single-task, empty shape = dual-task).
Partial Correlation Coefficients Between Variables from the Clinic-Based Turning Tasks, General Measures of Mobility, and the Community Ambulation Task in Civilians and Healthy Military Service Members
All variables are ranked by the magnitude of the correlation coefficient. Partial correlation coefficients are also shown for civilian and healthy service member participants separately. Variables from clinic-based turning tasks are noted with an * and only variables with significant associations across all participants (adjusted p < 0.05) are shown.
1 MW, one-minute walk test; CTC, complex turning course; DT, dual-task; FGA, Functional Gait Assessment; HAM-4-mTBI, 4-item hybrid assessment of mobility for mild traumatic brain injury; HiMAT, high-level mobility assessment tool; mIAT, modified Illinois Agility Test; ROM, range of motion; SD, standard deviation; ST, single-task.
Better performance on the SUP was only significantly associated with faster DT mIAT times (|r| = 0.31, p = 0.010). The association between SUP performance and head-body coordination variability and peak trunk turning speed during the CTC approached but failed to reach significance (|r| = 0.29–0.30, p > 0.05; Fig. 4 and Table 4). No clinical measure (FGA, HiMAT, and HAM-4-mTBI) was significantly associated with SUP performance (|r| = 0.14–0.24, p > 0.05). Amongst clinical measures, the ST gait speed and HiMAT score were most strongly associated with SUP performance (|r| = 0.24 and 0.23, respectively). Like the CAT results, association with SUP performance varied based on the population, with military service members demonstrating a stronger association between DT mIAT completion time and SUP performance (|r| = 0.49) compared to civilians (|r| = 0.34).
Partial Correlation Coefficients Between Variables from the Clinic-Based Turning Tasks (*), General Measures of Mobility, and the Simulated Urban Patrol Task in Civilians and Healthy Military Service Members
All measures are ranked by the magnitude of the correlation coefficient. Partial correlation coefficients are also shown for civilian and healthy service member participants separately. Instrumented turning measures are noted with an * and only instrumented turning measures with significant associations across all participants (adjusted p < 0.05) are shown.
HAM-4-mTBI, 4-item hybrid assessment of mobility for mild traumatic brain injury; HiMAT, high-level mobility assessment tool; mIAT, modified Illinois Agility Test.
Discussion
This study sought to assess the clinical utility, including the diagnostic accuracy and associations with performance on ecologically relevant functional tasks, of objective turning measures from clinic-based turning tasks. Our results indicate that individual, objective turning measures from clinic-based turning tasks offer similar diagnostic capacities to standard clinical batteries such as the FGA, HiMAT, and HAM-4-mTBI. The value of instrumented clinic-based turning tasks, however, stems from the ability to capture multidimensional variables at once. Regression models using multiple variables from the same test yielded higher AUCs compared to standard clinical assessments alone (e.g., CTC AUC of 0.90 vs. FGA AUC of 0.68). Further, objective outcomes, including lap time from the ST CTC and segmental coordination from the ST mIAT and DT CTC, provided added value by improving the AUC of the FGA, HiMAT, HAM-4-mTBI, and standard assessments of ST or DT gait speed. This superior diagnostic capacity and added value of clinic-based turning tasks, with time commitments (<10 min) that are similar or shorter than standard clinical batteries, suggests adding instrumented, clinic-based turning tasks could improve clinical RTA decisions, including return to duty, work, or sport. In addition, several of the strongest individual variables need minimal instrumentation, requiring only a stopwatch. The military’s progressive RTA: primary care for acute concussion management outlines a physical and cognitive RTA screening “to objectively measure readiness for return to duty.” However, the physical RTA screening only requires 2 min of supervised aerobic activity at an exertion rate of 16 or greater on the borg rate of perceived exertion scale. Overt symptom provocation is the only metric for determining readiness to progress to the cognitive RTA screening, the final step before returning a service member to full duty. Clinic-based turning tasks, especially when instrumented, could complement a service member’s overt symptom provocation or self-report of worsening symptoms with exertion to better inform readiness for RTA.
Objective turning variables were strongly associated with performance on ecologically relevant functional tasks such as the CAT or SUP, indicating a highly desirable feature for informing RTA decisions. A summary of key stakeholders, including rehabilitation specialists and military command leaders, reported that RTA decisions are primarily based on whether an individual can complete the required duties of their position. 55 Yet, few clinical assessments accurately reflect the demands of daily living, especially specialized military tasks. 55 Out of the standard clinical assessments, only ST and DT gait speed was associated with the CAT, while 19 turning measures were associated with CAT performance. Given the nature of the CAT (walking and navigating through a building), it is unsurprising that gait speed was associated with CAT performance. However, lap time from the ST CTC exhibited a slightly stronger association with CAT performance. This result indicates that assessments of ambulatory turning may be more relevant to a person’s daily life than straight-line walking. Similarly, completion time on the DT mIAT was the only clinic-based turning variable associated with performance on the SUP; no standard clinical assessments were associated with this military-relevant activity. These results suggest the maximum running and turning speed during the DT mIAT better reflects high-demand simulated battle drills and may be more important than standard clinical assessments for extrapolating an individual’s performance in combat-related scenarios. Movements during the DT mIAT may be similar to cognitive demands and individual movement techniques service members must perform, such as the 3–5 sec rush (moving under fire). Notably, these associations seemed to vary depending on the population. Civilians demonstrated a stronger relationship between the lap time of the ST CTC and CAT performance compared to service members, while service members demonstrated a stronger relationship between the completion time of the DT mIAT and SUP performance compared to civilians. Combined, these results emphasize the need for RTA assessments that are targeted to the real-world task and population of interest.
Using inertial sensors to capture multiple objective measures of turning enabled individual tasks to achieve high diagnostic capacity, but isolated variables of CTC lap time and mIAT completion time had the strongest clinical utility. Average lap time from the ST CTC had the largest AUC of any clinic-based turning variable and the strongest association with CAT performance. Similarly, DT mIAT completion time had the fourth highest AUC and was the only variable associated with SUP performance. These simple measures of average lap time and completion time reflect an overall performance on the CTC and mIAT tasks, respectively, without regard to specific segmental kinematics or coordination during the task. While other variables such as peak turning speed and segmental coordination are isolated to specific turns within a task, these measures of lap/completion time include all aspects of the task. Specific features, such as the anticipatory adjustments when initiating or terminating a turn, and the walking or running in between turns, were not quantified by our selected variable set and may be important to understanding an individual’s deficits, particularly during daily life. Notably, these lap time and completion time variables are reliable and do not require sophisticated instrumentation. 43 Both CTC lap time and mIAT completion time could be obtained from a stopwatch for rapid implementation in military and civilian clinics without access to inertial sensors.
The final goal of this study was to provide recommendations for future clinical adoption. Based on the available evidence from this study and prior studies on test–retest reliability, the CTC likely offers the best clinical utility for civilians, while the DT mIAT likely offers the best clinical utility for military populations. The CTC yielded the largest AUC values as a combined test, the individual variables with the largest univariate AUCs (ST CTC average lap time), and the individual variables with the strongest association with daily living. Combined, this suggests that the CTC may be a valuable addition to clinical mTBI evaluations, particularly if objective measures from inertial sensors are available to generate the full variable set. However, military populations may benefit most from the DT mIAT, which exhibited stronger associations with the SUP task. Before CTC or mIAT variables can inform clinical decisions, future research should explore how these measures change during rehabilitation and whether better performance on these tasks is associated with outcomes such as faster RTA in the military population, return to sport in athletic populations, risk for musculoskeletal injuries that are common after mTBI, 56 –61 and overall performance in work activities and military occupational roles.
While the CTC and DT mIAT may offer the best clinical utility out of the tasks examined here, it is unlikely to be a panacea for RTA assessments. Complex and ecologically valid assessment techniques incorporating DT and multitask methods may prove useful in validating return-to-activity requirements in civilian and military populations as they more closely mimic real-world activity and are a step beyond single-domain measures of impairment that do not capture the full picture of function. 14 There are trade-offs to using more complex functional performance testing for RTA decisions based on environment (e.g., deployed or garrison environment for military) and timeframe or operational needs for decisions to be made. Recently developed assessments like the POWAR-TOTAL may be useful for testing military populations with combat roles, given its ability to discriminate service members with mTBI from controls and its responsiveness to rehabilitation. 16,62 However, such tasks may not be relevant for individuals with non-combat roles, including civilian populations. While the POWAR-TOTAL established construct validity using the HiMAT, 62 the present CAT results suggest that the HiMAT lacks construct validity for functional tasks for civilians and service members. Rather than relying on a single assessment, the continued development of multiple complementary, short, and clinically useful assessments that serve as a “menu” based on the patient’s needs may be ideal.
Limitations and future directions
A primary limitation of this study is the inclusion of only civilians with symptoms persisting beyond 3 weeks postinjury; military service members with mTBI were not included. Consequently, comparisons to diagnostic accuracy were limited to civilians who were matched at each civilian site. This study’s patient population was selected because they represent individuals who typically seek rehabilitation and where RTA can be most complicated and were accessible to the study team at each site. However, these patients with mTBI may not represent all individuals, including active-duty military personnel, law enforcement officers, or other tactical athletes for whom the SUP task is most ecologically relevant.
Second, the number of variables included in this analysis, and collinearity between similar variables (see Supplementary Data, Supplement C), may have affected the variables selected in the final multivariate lasso regression models. Collinearity was strongest between variables from the same test (e.g., variables from the CTC were associated with other variables with the CTC, but weakly associated with variables from the mIAT). Therefore, the exact variables that were selected by the lasso regression may vary—nearly collinear variables may be selected instead and yield similar results. However, the lasso models depicted here are not meant to be a replicable model that is ‘optimal.’ Instead, the multivariate models depict the potential of using information from the clinic-based turning tasks to discriminate groups. Determining a robust, cross-validated model for clinical implementation would require a much larger sample size and independent validation samples. Therefore, the results here should not be interpreted as a multivariate regression model that can be applied in the clinic. Instead, the results support the selection of tests, specifically the ST CTC and DT mIAT, for future research and use of specific variables (e.g., ST CTC average lap time and DT mIAT completion time) for potential clinical translation as further work on instrumented variables continues. The multivariate models demonstrate the utility of extracting many variables from a single test, but further development is needed to make the data collection, analysis, and variable extraction clinically feasible. Wearable systems that can combine sensing, computing, and data visualization/reporting capabilities, such as smartphone devices, 63,64 may automate these analyses in the future and offer simple, automated platforms for clinical use.
An additional limitation of this work is the lack of reliable data on the CAT and SUP tasks. While prior work established the reliability of the clinic-based turning tasks, 43,51 it is unclear if CAT or SUP performance would change over time or repeated practice. Similarly, the CAT and SUP are a step toward real-world tasks, but these tasks are still simulated tasks. Future work is needed to validate the degree of ecological validity within these tasks. 14 An additional limitation of this work was not considering mechanisms of injury or time since injury in our analyses. It is possible that differences in the mechanisms of injury (e.g., motor-vehicle accident vs. sport-related vs. fall) or the time since the injury may influence performance differently.
Finally, this study did not assess other aspects that may influence an individual’s ability to return to pre-injury activity, such as their psychological readiness. Prior work in athletes has identified transient changes in psychological readiness, including a lack of confidence in their ability to handle the demands of competition. 65,66 While objective measures of turning offer a valuable clinical tool for measuring behavioral outcomes, RTA decisions should also evaluate the individual’s confidence to handle the task demands, which may also affect their readiness to return. 66
Conclusion
Clinical and RTA decisions should be based on assessments that can both discriminate impairments and reflect performance during daily tasks. Simple turning outcomes can discriminate individuals with persistent mTBI symptoms from healthy controls similar to the ability of standard clinical batteries to discriminate groups. Instrumented outcomes that quantify intersegmental coordination during these turning tasks provide even more benefit and can increase the diagnostic accuracy of these tests. For the civilian participants in this study, turning outcomes were strongly associated with ambulation during a simulated community ambulation task and simulated military-relevant battle drills; standard clinical assessments exhibited weaker, or nonsignificant, associations with these CAT and SUP tasks. Predicting real-world performance requires assessments that match the cognitive and physical demands of the operational environment, which can be challenging as firearms simulators or other high-cost equipment are not available in most rehabilitation settings. Future work should quantify the ambulatory demands of real-world tasks (such as ecological assessments during training tasks performed in the field) and compare them to normative performance on clinically feasible turning tasks to further establish their validity.
Footnotes
Acknowledgments
The authors wish to acknowledge Ben Cassidy and Ryan Pelo, PT, DPT from the University of Utah, Lindsey Lee and Josh Koch from Oregon Health and Science University, Patrick Michielutti, PT, DPT, and Max Klaiman from Courage Kenny Research Center-Allina Health, as well as Holly Richard, PT, DPT and CPT Stefanie Faull, PT, DPT who collected data at Fort Sam Houston. A previous version of the article was uploaded to a preprint server (![]() ).
).
Authors’ Contributions
P.C.F.: Conceptualization, methodology, software, validation, formal analysis, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, and funding acquisition. P.A.: Formal analysis, validation, investigation, and writing—review and editing. L.P.: Software, validation, formal analysis, investigation, data curation, writing—review and editing, and visualization. M.M.W.: Conceptualization, methodology, resources, writing—review and editing, supervision, and funding acquisition. L.E.D.: Conceptualization, methodology, formal analysis, resources, writing—review and editing, supervision, and funding acquisition. M.E.L., C.W.H.: Conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—review and editing, supervision, and funding acquisition. L.A.K.: Conceptualization, methodology, formal analysis, resources, writing—review and editing, supervision, project administration, and funding acquisition.
Transparency,Rigor,and Reproducibility Statement
The study design and analytical plan were published as a protocol article,
39
and preregistered on clinicaltrials.gov (![]() ). A sample size of 100 (50 per group) was planned based on an expected effect size of 0.78 (Cohen’s d) calculated to yield 90% power to detect significant differences at an adjusted 0.01 significance level. Over a 4-year period, data were obtained and successfully analyzed in 110 civilians and 41 military service members. Data from five military service member participants were excluded due to missing test data. Participant data were batch processed and analyzed together using custom MATLAB scripts, described in,
51
that were blinded to the participant group. Descriptions of equipment, procedures, and all processing scripts are available upon request. There are no current or planned replication studies ongoing to our knowledge. Deidentified data are available through the Federal Interagency Traumatic Brain Injury Research Informatics System (https://doi.org/10.23718/study/390). All data used to conduct the study were obtained by the investigators and all participants have provided permission for their data to be used for future research without requirement for specific additional informed consent.
). A sample size of 100 (50 per group) was planned based on an expected effect size of 0.78 (Cohen’s d) calculated to yield 90% power to detect significant differences at an adjusted 0.01 significance level. Over a 4-year period, data were obtained and successfully analyzed in 110 civilians and 41 military service members. Data from five military service member participants were excluded due to missing test data. Participant data were batch processed and analyzed together using custom MATLAB scripts, described in,
51
that were blinded to the participant group. Descriptions of equipment, procedures, and all processing scripts are available upon request. There are no current or planned replication studies ongoing to our knowledge. Deidentified data are available through the Federal Interagency Traumatic Brain Injury Research Informatics System (https://doi.org/10.23718/study/390). All data used to conduct the study were obtained by the investigators and all participants have provided permission for their data to be used for future research without requirement for specific additional informed consent.
Author Disclosure Statement
The views expressed in this article are those of the authors and do not necessarily represent the official policy or position of the U.S. Army Medical Center of Excellence, the U.S. Army Training and Doctrine Command, 59th Medical Wing, Defense Health Agency, Department of the Army, Department of the Air Force, Department of Defense, or any other U.S. Government agency. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by the Assistant Secretary of Defense for Health Affairs endorsed by the Department of Defense, through the Congressionally Directed Medical Research Programs under Award No. W81XWH1820049 (L.K.). An integrated SQL database at Oregon Health and Science University has housed all the data and is supported by the Oregon Clinical and Translational Research Institute funded by a grant from the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Award Number UL1TR002369.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.