
Abstract
Traumatic brain injury (TBI) affects over 48 million people worldwide each year. Suicide is common in TBI, and there are several known contributing factors, including severe TBI, depression, alcohol use, and male sex. Impulsivity, or the tendency to act quickly with little thought, may be an early predictor of suicidality following TBI. The purpose of this study was to evaluate the risk of suicidality in patients with a prior history of impulsivity following a TBI. Using de-identified electronic health records from the TriNetX U.S. Collaborative Network with Natural Language Processing, three cohorts were generated: the impulsivity TBI cohort (I+TBI+) included subjects with a diagnosis of impulsivity before a diagnosis of TBI; the no impulsivity TBI cohort (I−TBI+) included patients with TBI but no impulsivity; the impulsivity no TBI cohort (I+TBI−) included patients with impulsivity but TBI. Two analyses were conducted, including analysis 1 (impulsivity TBI vs. no impulsivity TBI) and analysis 2 (impulsivity TBI vs. impulsivity no TBI). Patients were 1:1 matched by age, sex, race, ethnicity, psychiatric diagnoses, and antidepressant use. Outcomes included a diagnosis of self-harm, suicidal ideation, or a suicide attempt within 1 year after the index event. The all-time incidence of each outcome was assessed across different age categories. The chi-square test (categorical variables) and t-test (numerical variables) were used to assess for differences between groups. A total of 1,292,776 patients with TBI were identified in the study. After 1:1 matching, there were 20,694 patients (mean [standard deviation, SD] age, 48.1 [21.8]; 8,424 females [40.7%]) with impulsivity and TBI (I+TBI+), 1,272,082 patients (mean [SD] age, 46.0 [23.1]; 562,705 females [44.2%]) with TBI alone (I−TBI+), and 90,669 patients (mean [SD] age, 43.7 [22.6]; 45,188 females [49.8%]) with impulsivity alone (I+TBI−). Within the first year after a TBI, patients with impulsivity were more likely to exhibit self-harm (p < 0.001), suicidal ideation (p < 0.001), or a suicide attempt (p < 0.001). Compared with patients with TBI without impulsivity, those with impulsivity had a 4-fold increase in the incidence of self-harm (2.81% vs. 0.63%), an 8-fold increase in suicidal ideation (52.42% vs. 6.41%), and a 21-fold increase in suicide attempts (32.02% vs. 1.50%). This study suggests that impulsivity diagnosed before a TBI may increase the risk of post-traumatic suicidality, with a 4-fold increased risk of self-harm, an 8-fold increased risk of suicidal ideation and a 21-fold increased risk of suicide attempts. This characterizes a group of at-risk individuals who may benefit from early psychiatric support and targeted interventions following a TBI.

Introduction
Traumatic brain injury (TBI) affects over 48 million people worldwide each year. 1 Patients with TBI are predominantly male, and age-at-onset is bimodal, with adolescent and elderly patients at the greatest risk. 1,2 A heterogeneous condition, TBI encompasses a broad scope of injury types with a shared etiology: trauma to the brain. Injuries can be classified by location (e.g., lobe, laterality), bleed type (e.g., subdural, epidural, subarachnoid), or clinical status at presentation (e.g., Glasgow Coma Scale [GCS]). 3 –6 Assessed via the GCS, TBI severities include mild, moderate, and severe, with more severe injuries associated with worse functional and neurological outcomes, yet this severity classification system may be a gross simplification. 7,8 TBI is characterized by two distinct injuries: the primary, mechanical trauma to the brain parenchyma and the secondary, neurochemical response to the initial insult, resulting in inflammation and cell death. 9 –13 Patients with more dysregulated secondary injuries are at greater risk of adverse neuropsychiatric outcomes, including depression, cognitive impairment, bipolar disorder, mixed affective disorders, and suicide. 14 –23
Suicide is common in TBI, with an absolute rate of ∼41 per 100,000 person-years.21,24,25 The risk of suicide following TBI has been associated with severe TBI, skull fractures, male sex, depression, and alcohol use. 14,21,24 Recently, impulsivity was proven a key driver of suicidal ideation and suicide attempts in 95 veterans with TBI; similarly, a 1995 study demonstrated that 6 of 14 patients with TBI (42.9%) with suicidal ideation disclosed that their head injury was caused by impulsive behavior.25,26 Despite the known correlation between impulsivity and suicidality in TBI, much of this assumption rests on datasets from small, poorly generalizable populations.
Although there is evidence of an association between impulsivity and suicidality following TBI, little is known about the risk of suicidality in patients with a history of impulsivity before a TBI. Moreover, several therapeutic strategies to mitigate the risk of violence toward self or others in impulsive patients do exist, but no drug has proven efficacious for post-TBI impulsivity. 27 To address this knowledge gap that may highlight the need for risk-reduction strategies early after a TBI, we conducted a retrospective cohort study on adult patients with impulsivity before a TBI.
Methods
Data source
This is a retrospective cohort study using the TriNetX U.S. Collaborative Network with Natural Language Processing (NLP). This network facilitates access to de-identified electronic health records from ∼112 million patients across 64 health care institutions in the United States who subscribe to the TriNetX software. Data were sourced from inpatient and outpatient settings, including hospitals, primary care facilities, and specialized clinics, most of which were affiliated with large academic medical centers. The chosen network, the U.S. Collaborative Network with NLP, utilizes natural language processing to extract data from clinical documentation for specified diagnoses. The Carilion Clinic Institutional Review Board (IRB) determined that this study does not meet the definition of human subject research and did not require IRB approval (IRB 24-2208).
Study protocol and statistics
Data were obtained from June 1, 2016, to May 13, 2024, for all cohorts, including demographics and comorbidities. Three cohorts were generated: the impulsivity TBI cohort (I+TBI+) was defined as subjects over the age of 18 with a diagnosis of impulsivity (International Classification of Diseases, ICD-10-CM: R45.87) before a diagnosis of TBI (ICD-10-CM: S02.0, S02.1, S02.8, S02.91, S04.02, S04.03, S04.04, S06, S07.1); the no impulsivity TBI cohort (I−TBI+) was defined as patients over the age of 18 with a diagnosis of TBI but no prior diagnosis of impulsivity; the impulsivity no TBI cohort (I+TBI−) was defined as patients over the age of 18 with a known diagnosis of impulsivity but no diagnosis of TBI. Prior impulsivity was defined as a diagnosis within the study period. Impulsivity within the NLP network incorporates references to the specified diagnosis code R45.87, as well as unstructured data with references to the diagnosis “impulsivity.” The combination of structured electronic medical record data and NLP-extracted data provides a richer, more thorough dataset.
Two analyses were conducted, including analysis 1 (impulsivity TBI vs. no impulsivity TBI) and analysis 2 (impulsivity TBI vs. impulsivity no TBI). For each analysis, patients were 1:1 matched based on the presence or absence of covariates known to be associated with the measured outcomes, including age, sex, race (White, Black, other), ethnicity, psychiatric diagnoses (mood disorders [ICD-10-CM: F30–F39], anxiety disorders [ICD-10-CM: F40–F48], and substance use disorder [ICD-10-CM: F10–F19]), and antidepressant use. 28 –42 In the matching, covariates and outcomes of interest were represented in the following forms: yes/no for binary, categories for categorical, and mean for continuous (e.g., age). For each patient, a value was computed for each covariate and outcome of interest, comprising a patient-specific matrix. Logistic regression was then performed to generate a propensity score (range 0–1) for each patient. Matching was completed using the greedy nearest neighbor algorithm with a caliper of 0.1 with pooled standard deviations. For each patient in the smaller of the two cohorts, an unmatched patient in the larger cohort with the closest score was identified. The remaining patients in the larger cohort remained unmatched. The index event was defined as the time the subjects were diagnosed with TBI (impulsivity for the impulsivity no TBI cohort). Outcomes included first-time instances of self-harm (ICD-10-CM:X71-X83), suicidal ideation (ICD-10-CM: R45.851), and suicide attempts (ICD-10-CM: T14.91) within 1 year after the index event. All outcomes with less than 10 patients per group were rounded to 10 to protect confidentiality per TriNetX protocol. Descriptive statistics were conducted to assess differences between groups before and after matching, including a chi-square test for categorical variables and a t-test for numerical variables. Risk ratios were generated for each outcome of interest. Concurrently, we evaluated the incidence of self-harm, suicide attempts, and suicidal ideation at all times in each group across age strata. The TriNetX Analytics platform was utilized for statistical analyses, and GraphPad Prism (Version 9.5.1) was used for graphical representation. Significance was set at p < 0.05.
Results
Demographics
The raw demographics for the TriNetX U.S. Collaborative Network were reflective of the general population (Supplementary Table S1). For the first analysis, we identified a total of 1,292,776 patients with TBI including 20,694 patients (mean [standard deviation, SD] age, 48.1 [21.8]; 8,424 females [40.7%]) with impulsivity before the TBI in the I+TBI+ cohort and 1,272,082 patients (mean [SD] age, 46.0 [23.1]; 562,705 females [44.2%]) without impulsivity in the I−TBI+ cohort. Compared with those without impulsivity (I−TBI+), subjects with impulsivity (I+TBI+) were more likely to be older (46.0 [23.1] vs. 48.1 [21.8]; p < 0.001) or White (65.4% vs. 80.2%; p < 0.001) and less likely to be female (44.2% vs. 40.7%; p < 0.001). Regarding psychiatric diagnoses, subjects with impulsivity (I+TBI+) were more likely to have a mood disorder (19.3% vs. 69.0%; p < 0.001), an anxiety disorder (21.4% vs. 70.4%; p < 0.001), or substance use disorder (18.1% vs. 67.0%; p < 0.001). After 1:1 matching for age, sex, ethnicity, race, psychiatric diagnoses, and antidepressant treatment, there were 20,693 patients (mean [SD] age, 48.1 [21.8]; 8,424 females [40.7%]) in the I+TBI+ cohort and 20,693 patients (mean [SD] age, 48.1 [21.7]; 8,422 females [40.7%]) in the I−TBI+ cohort. After matching, there were no differences in age, sex, race, ethnicity, or psychiatric diagnoses (Table 1).
Demographics and Clinical Characteristics of Patients Before and After Propensity Score-Matching
SUD, substance use disorder; TBI, traumatic brain injury.
For the second analysis, we identified a total of 111,363 impulsivity patients including 20,694 patients (mean [SD] age, 48.1 [21.8]; 8,424 females [40.7%]) with a prior TBI as the I+TBI+ cohort and 90,669 patients (mean [SD] age, 43.7 [22.6]; 45,188 females [49.8%]) without a prior TBI as the I+TBI− cohort. Compared with those without TBI (I+TBI−), subjects with TBI (I+TBI+) were more likely to be older (43.7 [22.6] vs. 48.1 [21.8]; p < 0.001) or White (77.9% vs. 80.2%; p = 0.002) and less likely to be female (49.8% vs. 40.7%; p < 0.001). Regarding psychiatric diagnoses, patients with TBI (I+TBI+) were more likely to have a substance use disorder (51.5% vs. 67.0%; p <0.001), a mood disorder (60.7% vs. 69.0%; p = 0.042), or anxiety (62.1% vs. 70.4%; p < 0.001). After 1:1 matching for age, sex, ethnicity, race, psychiatric diagnoses, and antidepressant treatment, there were 20,694 patients (mean [SD] age, 48.1 [21.8]; 8,424 females [40.7%]) with TBI (I+TBI+) and 20,694 patients (mean [SD] age, 48.1 [21.8]; 8,504 females [41.1%]) without TBI (I+TBI−). After matching, there were no differences in age, sex, or psychiatric diagnoses (Table 1).
Risk of outcomes across matched groups
After matching, the risks of suicide attempts or ideation within the first year after the TBI were evaluated across cohorts (Table 2, Supplementary Fig. S1).
Risk of Outcomes Across Matched Groups
TBI, traumatic brain injury.
For the first analysis, we found that patients with impulsivity were at greater risk of self-harm following a TBI, with 92 of 20,693 patients (0.5%) with impulsivity (I+TBI+) and 42 of 20,693 patients (0.2%) without impulsivity (I−TBI+) (risk ratio [RR], 2.224; 95% confidence interval [CI], 1.545–3.202; p < 0.001). Patients with impulsivity were at greater risk of suicidal ideation following a TBI, with 854 of 20,693 patients (8.9%), compared with 571 of 20,693 patients (3.5%) without impulsivity (RR, 2.543; 95% CI: 2.294–2.819; p < 0.001). We found that patients in the with impulsivity (I+TBI+) were more likely to exhibit a suicide attempt following the TBI, with 564 of 20,693 patients (3.9%) with impulsivity (I+TBI+), compared with 233 of 20,693 patients (12%) without impulsivity (I−TBI+) (RR, 3.331; 95% CI: 2.864–3.874; p < 0.001).
For the second analysis, we found there were no differences in the development of self-harm (p = 0.791), suicidal ideation (p = 0.580), or suicide attempts (p = 0.641) across impulsivity patients with versus without TBI (Table 1, Supplementary Fig. S2).
Incidence of outcomes
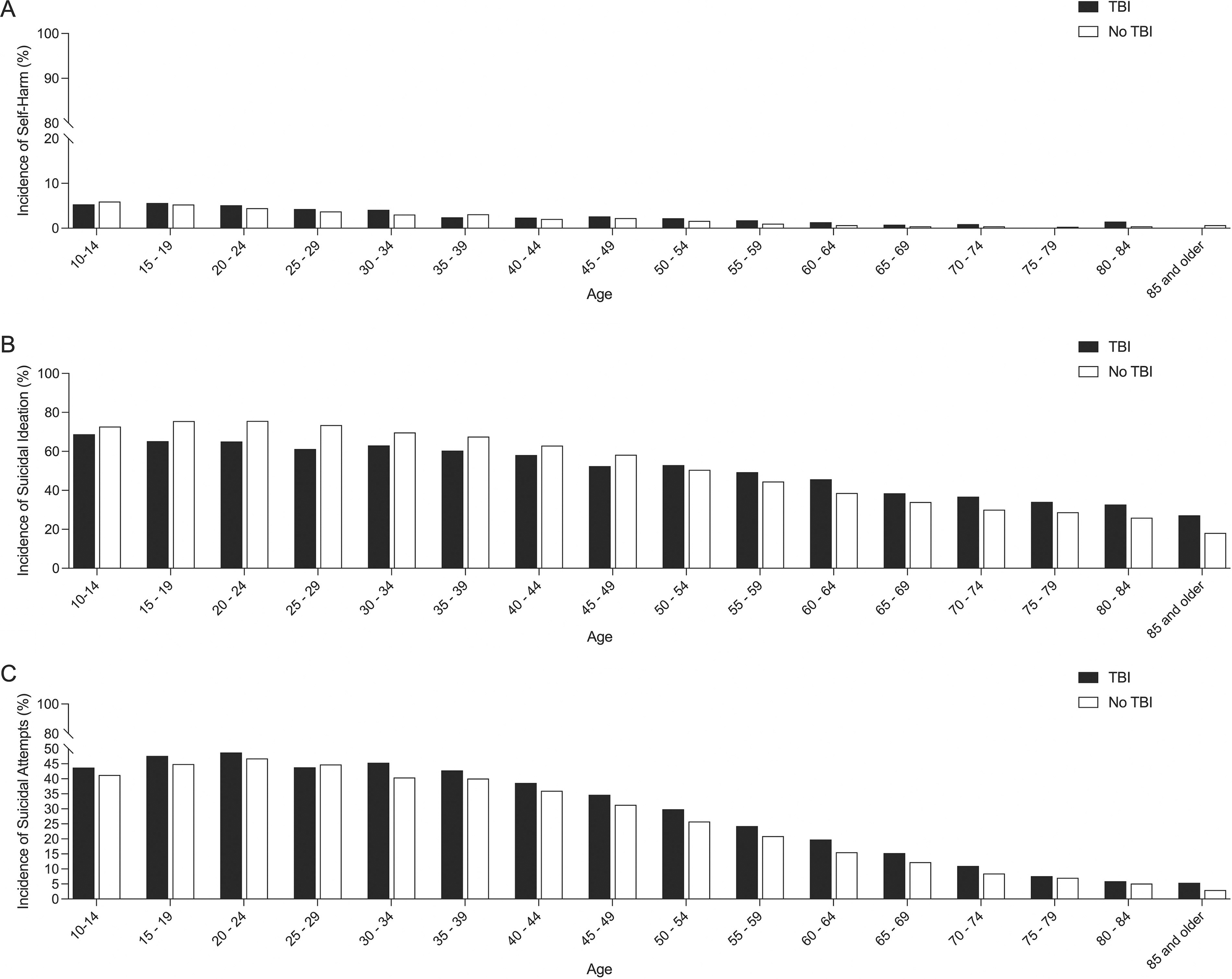
We then estimated the incidence of self-harm, suicide attempts, and suicidal ideation in each cohort during the specified times (Figs. 1 and 2). Self-harm was reported in 2.81% of patients with impulsivity and TBI (I+TBI+), 0.63% of patients with TBI but without impulsivity (I−TBI+), and 2.92% of patients with impulsivity but without TBI (I+TBI−). Regarding the influence of age, the highest incidence of self-harm was in patients with impulsivity only (I+TBI−) between 10 and 14 years old (5.94%). Suicidal ideation was reported in 52.42% of patients with impulsivity and TBI (I+TBI+), 6.41% of patients with TBI but without impulsivity (I−TBI+), and 57.90% of patients with impulsivity but without TBI (I+TBI−). The highest incidence of suicidal ideation was in patients with impulsivity only (I+TBI−) between 20 and 24 years old (75.59%). A suicide attempt was reported in 32.01% of patients with impulsivity and TBI (I+TBI+), 1.50% of patients with TBI but without impulsivity (I−TBI+), and 31.38% of patients with impulsivity but without TBI (I+TBI−). The highest incidence of suicide attempts was reported in patients with impulsivity and TBI (I+TBI+) between 20 and 24 years old (48.76%).
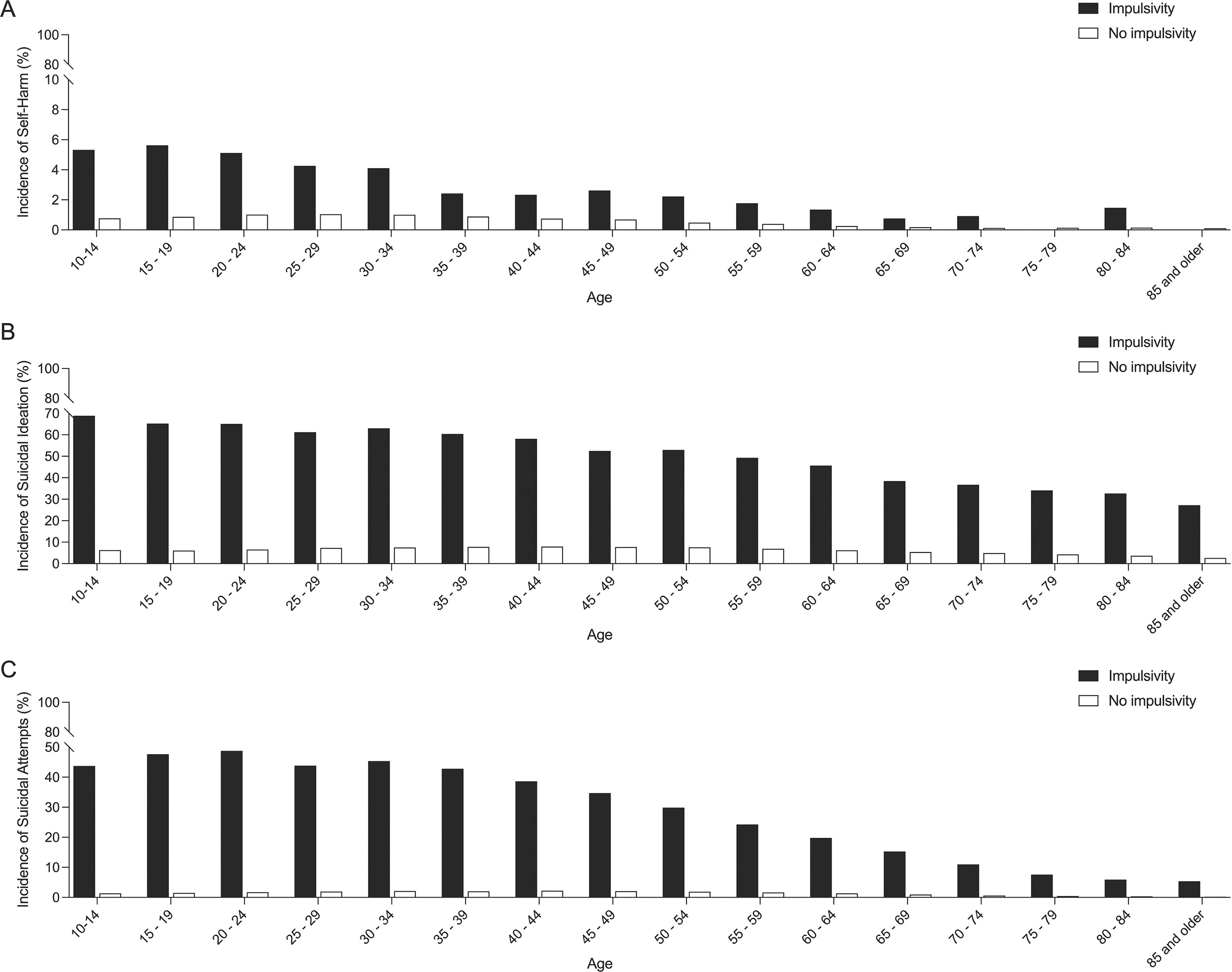
Incidence of outcomes stratified by age for the first analysis (TBI impulsivity vs. TBI no impulsivity), including self-harm
Incidence of outcomes stratified by age for the second analysis (TBI impulsivity vs. no TBI impulsivity), including self-harm
Discussion
This retrospective cohort study analyzed data from over one million patients with TBI and demonstrated an association between preexisting impulsivity and the risk of suicidality post-TBI. We found that individuals with impulsivity before TBI had a significantly heightened risk of suicidal ideation and suicide attempts within the first year post-injury compared with those without impulsivity. Moreover, this risk was age-specific and may be modulated by the known association between impulsivity and suicidality. These findings underscore the importance of comprehensive screening for impulsivity in patients with TBI and the development of targeted interventions to mitigate the risk of suicidality in those at greatest risk.
Prior studies have confirmed the association between impulsivity, TBI, and suicidality, but this is the largest and most generalizable study to date to confirm this finding. It is known that patients with TBI are at greater risk of suicide and that patients at greatest risk have comorbid depression and high injury severities. Still, other patient-specific risk factors remain to be elucidated. 43 –45 A recent study by Aaronson and colleagues of 164 veterans demonstrated a link between TBI, impulsivity, suicidal ideation, and suicide attempts.25 As this effect was no longer significant after controlling for confounders, there are likely other factors influencing a veteran’s predisposition toward suicidality, such as hyperarousal, affective instability, and comorbid psychiatric diagnoses. 46 –48 Our study, in contrast, controlled for known psychiatric mediators of suicidality, and the association was not lost, likely due to our large patient population. An early study by Klonoff and colleagues found that almost half (42.9%) of 14 patients with TBI with suicidal ideation acquired their head injury through impulsive behavior, highlighting a tendency toward impulsivity before a TBI in patients who progress to develop suicidality. 26 Our study investigates this assumption and utilizes advanced statistical methods to confirm its validity. This study should confirm impulsivity-associated suicidality in TBI, which was not validated in prior studies due to low sample sizes and limited statistical reporting.
As suicide is preventable and impulsivity is a known risk factor, this study highlights the need for an improved understanding of the neurobiological basis of impulsivity and targeted treatments to prevent suicidality in at-risk patients with TBI. Several studies have utilized magnetic resonance imaging to investigate the neural circuitry underlying impulsive behavior, demonstrating reduced volumes of cortical (medial prefrontal cortex, dorsolateral prefrontal cortex) and subcortical (ventral striatum) structures in suicidal patients. 49,50 Similarly, patients with suicidality demonstrate altered connectivity of the prefrontal cortex. 51,52 Medications that lessen this reduction in prefrontal cortex volume and function may prove helpful in mitigating suicidality in impulsive patients with TBI. A known suicide-preventing medication, lithium, has been proven to promote increased gray matter volume of the dorsolateral prefrontal cortex and other affected brain regions in suicidal patients with bipolar depression. 53 As the neurobiological effects of lithium have not been studied in a non-bipolar suicidal population, there is a need for future research on this topic. Beyond medications, neurosurgical interventional approaches to reduce suicide risk may be helpful. One such strategy, deep brain stimulation (DBS), demonstrated a potent antidepressant effect when targeting the medial prefrontal cortex in rats. 54 Although not widely accessible, with increasing technological advances and insurance support, DBS may be a treatment of the future for suicidality and other mood-related disorders in TBI. 55,56 One limitation to preventing suicidality in impulsive patients with TBI is that impulsivity is loosely defined; however, there are several validated scales such as the Barratt Impulsiveness Scale, the urgency, premeditation, perseverance, sensation seeking, and positive urgency scale (UPPS-P), and the Difficulties in Emotion Regulation Scale, which could be utilized at the time of TBI to assess the presence of impulsive behaviors and the need for preventative intervention. 57 –59 Due to the ambiguity in diagnostic criteria of impulsivity, at-risk patients are not easily identifiable. Still, it is possible that at-risk patients could be identified early at initial presentation to psychiatric units or prisons. It is known that prisoners have high rates of impulsivity, TBI, and suicide, so this is likely a highly vulnerable population. 60,61 Moreover, impulsivity correlates with the risk of suicidality in patients in an inpatient psychiatric setting and should serve as a sign for intensive intervention. 62 Further studies evaluating the neurobiological basis of impulsivity, as well as interventions to treat those at greatest risk, may aid in preventing suicidality in patients with TBI.
In addition, long-term brain injury rehabilitation may play an essential role in mitigating suicidal risk after a TBI. Several rehabilitation centers offer TBI support groups that can address patient-specific concerns as well as other suicide-related risk factors like substance use associated with the injury. 63 In addition to group support, involvement in meaningful activities in veterans with mild TBI has been linked to a reduced likelihood of suicidal ideation, demonstrating the crucial role of occupational therapy in a rehabilitation setting for suicide prevention. 64 While there is minimal evidence describing the neurobiological basis of suicidality following TBI, there may be a significant association between tumor necrosis factor (TNF)-α, an inflammatory biomarker, disinhibition, and suicidal ideation in the aftermath of TBI. 65 Moreover, growing evidence shows that aggressive and impulsive behavior is correlated with pro-inflammatory markers, such as TNF-α. 66 Although no U.S. Food and Drug Administration–approved pharmacological interventions target TNF-α post-TBI, rehabilitative exercise programs (most significantly, aerobic exercise) have been shown to alleviate depression and reduce TNF-α levels compared with stretching or a control group. 67 –70 Brain injury rehabilitation offers an opportunity to identify patients with TBI at risk and develop strategies to mitigate the risk of suicidality in this vulnerable population.
This study highlights the association between preexisting impulsivity and suicidality in patients with TBI. With future neuroimaging studies, longitudinal cohort studies, and interdisciplinary collaborations, we will better understand the pathways mediating this association between impulsivity, TBI-induced neurostructural changes, and suicidality. These insights will facilitate the development of targeted therapeutic interventions to prevent impulsivity-related suicidality in patients with TBI and guide risk-reduction strategies during rehabilitation, ultimately mitigating the risk of suicide in TBI.
Limitations
The study’s strengths lie in its large patient sample size, generalizability, and robust statistical methods, but several limitations should be addressed. The study relies on electronic health records, and the accuracy and completeness of the data are contingent on the quality of documentation in these records. Inaccuracies or missing information in patient records could impact the validity of this study. The study adopts a retrospective cohort design, relying on historical data. Moreover, this study evaluates outcomes at a pre-selected time point (1 year) and not at all time. This design may be subject to recall bias and limits the ability to establish causation due to the study’s observational nature. While the study controls for various demographic and psychiatric factors through 1:1 matching, there may be unmeasured or unknown confounding variables that should have been considered, potentially affecting the study outcomes. Moreover, the included characteristics were chosen based on prior literature and not validated within this study population due to limitations within the TriNetX platform, which may limit the interpretation of these results. The study defines impulsivity based on ICD-10-CM: R45.87, which may not capture the whole spectrum, but NLP has been utilized to capture miscoded or poorly coded cases.
Moreover, the results might be influenced by the specificity and sensitivity of this diagnostic code. In addition, this study relies on specific ICD-10-CM codes for identifying suicidal ideation and suicide attempts. The sensitivity of these codes in capturing all relevant cases might be limited, potentially affecting the precision of the reported outcomes. Despite efforts to match patients in the impulsivity cohort with the control cohort, there may still be residual bias due to confounding variables needing to be accounted for in the matching process. While efforts were made to mitigate these limitations, residual biases may exist, warranting informed interpretation of our findings within the context of these constraints.
Conclusion
In summary, this study demonstrates a link between pre-existing impulsivity and an increased risk of suicidality following TBI. Compared with previous studies, ours benefits from its large sample size and robust statistical methods, providing more substantial evidence for this association. Future research should investigate the neurobiological basis of impulsivity and develop targeted interventions to address suicidality in at-risk patients with TBI.
Transparency, Rigor, and Reproducibility Summary
This study was not formally registered because it utilizes de-identified patient information, and no intervention was performed. 1 The analysis plan was not formally pre-registered, but the team member with primary responsibility (lead author) certified that the analysis plan was pre-specified. 2 After matching, the sample size was 3,634 subjects per group. 3 A total of 1,068,963 patients with TBI were initially identified, including 3,634 with impulsivity before the TBI and 1,065,329 without. A total of 23,335 patients with impulsivity but without a prior TBI were identified. Matching was then conducted, resulting in 3,634 subjects per group. 4 Blinding was not deemed necessary due to the de-identified nature of patient data. 5 Data were acquired between June 1, 2016, and March 27, 2024. 6 Data were collected using the U.S. Collaborative Network with NLP that are available to participating institutions. 7 The inclusion criteria are diagnostic code-based and established in clinical practice, and investigators with research and clinical expertise assessed key inclusion criteria and clinical outcomes. 8 The lead and final authors, with support from the Carilion Clinic Department of Statistics, performed statistical analysis and/or review. 9 Comparisons and evaluated outcomes were kept to the minimum necessary to reduce the risk of multiple comparisons. 10 External validation studies in a retrospective, institution-specific manner, are being planned. 11 De-identified data and analytic codes from this study are not available in a public archive but can be made available upon request. 12,13 The authors agree to provide the full article content on request by contacting the corresponding author. 14
Footnotes
Acknowledgment
The authors acknowledge the Carilion Clinic Department of Statistics.
Authors’ Contributions
L.L.: Conceptualization, methodology, formal analysis, investigation, writing—original draft, and visualization. T.S.: Investigation, writing—original draft, and visualization. S.A.: Writing—reviewing and editing and visualization. E.M.: Writing—reviewing and editing and visualization. J.W.: W—reviewing and editing and visualization. A.K.: Conceptualization, methodology, writing—reviewing and editing, visualization, supervision, and project administration.
Funding Information
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.