
Abstract
Mental health conditions and concussion history reported by a collegiate athlete may contribute to prolonged recovery and symptom severity after concussion. This work examined the potential associations among concussion history, preexisting conditions, and sex relative to initial symptom severity and recovery duration following sport-related concussion (SRC) in a cohort of Division 1 National Collegiate Athletic Association athletes. This prospective cohort study analyzed symptom severity, recovery, and return-to-play (RTP) times reported post-SRC using data collected as part of the Pac-12 Concussion Assessment, Research and Education Affiliated Program and Health Analytics Program. Health history questionnaires that included self-reported history of preexisting conditions were completed at baseline. When consented athletes were diagnosed with a concussion, daily postconcussion symptom scores were evaluated until an athlete was clinically determined to be asymptomatic. Generalized linear and Cox proportional hazards models were used to determine associations between preexisting conditions and recovery and RTP times. Ninety-two concussions met inclusion criteria. Notable differences in initial symptom severity existed between females and males who had mood disorders (effect size [d] = 0.51) and attention-deficit hyperactivity disorder (ADHD; d = 0.93). The number of previous concussions was a strong predictor of athletes reporting preexisting mood disorders, depression, anxiety, and ADHD (p = 0.008–0.04). Females with ≥2 previous concussions required more days to RTP than males (d = 0.31–0.72). Weekly recovery and RTP probabilities substantially differed between athletes who did or did not have learning disorders (LDs; hazard ratio [HR]Recovery = 0.32, HRRTP = 0.22, d = 1.96–2.30) and ADHD (HRRecovery = 3.38, HRRTP = 2.74, d = 1.71–4.14). Although no association existed between concussion history and acute symptom severity, collegiate athletes with a history of concussion had higher probabilities of reporting depression, mood disorders, anxiety, and ADHD. Having ADHD or LDs likely strongly affects time to recovery and RTP for collegiate athletes.
Introduction
Sport-related concussion (SRC) is a traumatic brain injury induced by biomechanical forces caused by a direct blow to the head, neck, face, or body during sport. 1,2 SRC causes neuropathological changes that can result in both acute and chronic morbidities, often resulting in absence from match play or training sessions, and can negatively affect the quality of life. 3 Epidemiological research from the National Collegiate Athletic Association (NCAA) reported 4.13 SRCs per 10,000 athlete exposures, occurring in both males and females and across all sports, with recurrent SRCs also noted. 4 Return-to-play (RTP) is a high priority for both athletes and stakeholders, including coaches, teams, and fanbases. Although SRC is typically associated with short recovery and RTP times, new evidence suggests that recovery time is longer in some athletes for various reasons, 5,6 some of which may be unknown. Recent research has focused on identifying factors, such as athlete demographic characteristics, that may influence symptom severity 7,8 and prolong recovery from SRC. 9 –11 Studies investigating the relationship between preinjury characteristics and recovery have yielded conflicting results. 10 –16 Furthermore, many of these studies were completed among pediatric and adolescent populations, 10 –12,15 with results not generalizable to collegiate athlete populations. Therefore, a knowledge gap persists in identifying collegiate athletes who may be at risk for a longer recovery following an SRC.
Although concussion history (number of previous concussions) has not been previously associated with symptom severity after concussion, 17,18 it may contribute to prolonged recovery. 12,19 Athletes with a history of concussion also may have elevated risks of developing attention-deficit hyperactivity disorder (ADHD), 20 –22 learning disorder (LD), 21,23 and psychiatric disorders, 24,25 though research on this remains limited. Furthermore, acute symptom severity 26,27 and preexisting conditions, 7 –9,17 such as ADHD, 12 LD, 11 psychiatric disorders, 28 or headache/migraine disorders, 11 may contribute to prolonged recovery after concussion. Although a high prevalence of reported preseason anxiety and depressive symptoms among collegiate athletes exists, 29,30 it is still unclear what potential relationship there may be between athlete demographics, reported preexisting conditions, and the number of prior concussions within this population.
Following concussion, females often report greater total symptom severity scores than males, 31 –34 though findings have been mixed. 35 Conflicting results may be due to differing sample sizes across studies, as well as target population discrepancies; for instance, many SRC studies have focused on pediatric athletes, but concussion outcomes observed in pediatric populations may not be generalizable to adult athletes. 36,37 Indeed, median postconcussion symptom severity scores reported among participants aged 8–12 and 13–17 were 19.0 and 27.0, respectively, 37 whereas collegiate athletes reported an average postconcussion symptom severity score of 27.7. 38 Similarly, studies that examined differences in postconcussion recovery times between males and females have yielded conflicting results. Although some studies found longer recovery times in female collegiate athletes, 39,40 other studies did not. 41,42 Recently, Caccese and colleagues found no sex differences in Sport Concussion Assessment Tool (SCAT) total or severity scores at baseline, immediately after concussion, or at RTP initiation between male and female collegiate athletes, with minimal sex differences in recovery trajectories overall. 34 This lack of consensus is likely at least partially due to male-biased SRC research; for example, most SRC research has focused on athletes in male-dominated sports, such as American football, 43 –45 rugby, 46,47 and boxing, 48,49 whereas fewer studies included female athletes. Given the prevalence of concussion in female athletes, 50,51 research is warranted to better understand how athletes’ sex may influence symptom severity and recovery times following SRC.
The purpose of this study was to rigorously investigate potential associations among concussion history, preexisting conditions, and sex with initial symptom severity and recovery time following SRC in a cohort of NCAA Division 1 athletes in the Pac-12 Conference (Pac-12). Understanding if and how these characteristics may influence SRC outcomes has important implications for preseason assessment of athletes and can inform the management and treatment of concussions to promote efficient recovery following SRC.
Methods
Study participants
In 2014, the Pac-12 Conference established the Student-Athlete Health and Well-Being Initiative uniting all Pac-12 universities in an organized, structured scientific collaboration. The Pac-12 Conference is comprised of the University of Arizona, Arizona State University, University of California, Berkeley, University of Colorado Boulder, University of Oregon, Oregon State University, Stanford University, University of California, Los Angeles, University of Southern California, University of Utah, University of Washington, and Washington State University. Also, in 2014, the NCAA in collaboration with Department of Defense (DoD) established the NCAA-DoD Concussion Assessment, Research and Education Consortium (NCAA-DoD CARE Consortium). 52 In August 2017, the Pac-12 collectively became a CARE-Affiliated Program (CAP) serving as a “regional hub” for the CARE Consortium. During this time, the Pac-12 also established the Health Analytics Program (HAP; formerly SIRMAP) that serves as the primary sports injury registry and database for the conference. The structure and standardized procedures of CAP and HAP were previously published. 42,53
For the purpose of the current analyses, deidentified data were obtained from CAP and HAP. Data collected as part of the Pac-12 HAP were derived from clinical documentation in a Health Insurance Portability and Accountability Act (HIPAA)-compliant electronic medical record by sports medicine clinicians in the Pac-12 Conference. Data were deidentified using HIPAA Safe Harbor method for deidentification (45 CFR 164.514). Resulting project data included deidentified records only from student-athletes who provided authorization for secondary research as part of the HAP.
Student-athletes were enrolled in CAP and HAP after providing consent during the period between July 2018 and September 2022. Prior to July 2019, institutions across the Pac-12 did not maintain records on diagnosed preexisting conditions. Therefore, for the purpose of this analysis, data collected from student-athletes enrolled between July 2019 and September 2022 were included. These consented athletes remained in the study, and incident concussions were tracked while the student-athlete was enrolled at their respective university.
Prior to the start of each sport’s season, the SCAT5 symptom checklist 54 was administered and defined as baseline. Participants also completed a medical history questionnaire from which information on sex, concussion history prior to enrolling at university, sport played at the time of injury, and self-reported medical history, including previously being diagnosed with ADHD, LD, depression, anxiety, and other mood disorders, was obtained. Subsequent concussion diagnoses were made by team physicians at each institution using the Concussion in Sport Group definition. 3 The SCAT5 symptom checklist was administered within 48 h of injury and then daily until asymptomatic or return to baseline and also within 24 h of the athlete beginning RTP protocol. Recovery was defined as the time to completion of daily symptom forms, during which a clinician determined the student-athlete to be asymptomatic or had returned to baseline. Time to RTP was defined as the days from injury when a student-athlete was determined to return to full competitive play. RTP progression was dependent on subjective symptom reporting by student-athletes, and to complete RTP, athletes must have reported being asymptomatic for 24 h after daily progressive exercise overload and cleared by clinical evaluation. Participants were categorized according to the self-reported responses of having been diagnosed with ADHD, LD, depression, anxiety, mood disorders, or headache/migraine disorders. Mood disorder was a category included in the medical history form for student-athletes to describe disorders that were not depression. This may have included, but was not limited to, bipolar disorder, schizophrenia, hypomania, and disruptive mood dysregulation. All athlete demographics and self-reported diagnoses of these preexisting conditions were taken from the evaluation Year 1 health history questionnaire only. All concussions that occurred in season that were used in these analyses did not require hospitalization, and therefore, no imaging of acute concussion was collected.
Statistical analyses
Preexisting conditions, concussion history, and their association with initial symptom severity scores
Using generalized linear models, we investigated if athletes with a given preexisting condition or a greater number of previously diagnosed concussions predicted the initial SCAT5 symptom severity scores. We first conducted exploratory analyses to determine whether Poisson or negative-binomial distributions, or zero-inflated versions of those distributions, best described the initial symptom severity scores. 55 –57 To do this, we fit models with said distributions and then conducted information-theoretical model selection using Akaike’s information criterion (AIC) to identify the model with the best distribution for describing the data (i.e., the model with the lowest AIC value 58 ). Using the most supported error distribution, we then fit preexisting condition-specific models that included a two-way interaction between athlete sex (male vs. female) and a binary variable that denoted whether the athlete did (1) or did not (0) have the preexisting condition, as well as a model that included a two-way interaction between athlete sex and the number of previously diagnosed concussions. We included sex as a predictor in all those models because we suspected that males may have different preexisting conditions and a higher number of previous concussions than females. 59,60
Sex differences in concussion history and the association between concussion history and reporting preexisting conditions
Using generalized linear models, we investigated if the number of previously diagnosed concussions differed between sexes, if the probability of athletes having a given preexisting condition was influenced by the number of previously diagnosed concussions, and if recovery and RTP times were influenced by the number of previously diagnosed concussions. Similar to the analysis of initial symptom severity scores described above, we conducted exploratory analyses to determine whether Poisson or negative-binomial distributions, or zero-inflated versions of those distributions, best described the number of previously diagnosed concussions, recovery times, and RTP times, by fitting models with said distributions and then conducting information-theoretical model selection using AIC to identify the most supported model. Using the most supported error distribution for each response, we then fit the following models: (1) a number of previous concussions response model with only a fixed effect predictor for athlete sex; (2) six preexisting condition-specific response models with a binomial error distribution (because individuals could either have [1] or not have [0] a given preexisting condition) and a two-way fixed effects interaction between athlete sex and number of previous concussions; (3) a recovery time response model with a two-way fixed effects interaction between athlete sex and number of previous concussions; and (4) a RTP response model with a two-way fixed effects interaction between athlete sex and number of previous concussions.
The association between preexisting conditions and weekly recovery and RTP probabilities
Using time-to-event survival analysis implemented with semiparametric Cox proportional hazards models, 59,61,62 we evaluated the effects of athlete sex and preexisting conditions on weekly recovery and RTP probabilities. We first expanded both the recovery and RTP times into weekly (7-day) binary events, such that each athlete had multiple week-long data points within which they either did (1) or did not (0) recover or RTP. We then fit Cox models that included either a single fixed effect for athlete sex or a single fixed effect for whether athletes did or did not have a given preexisting condition; we specified clusters for athletes’ injury identification numbers in all models to account for the multiweek entries for each athlete.
We conducted all statistical analyses in the R statistical computing environment. 63 We fit all generalized linear models using the package glmmTMB, 64 and we fit all Cox proportional hazards models using the package survival. 65,66 We obtained scaled quantile residuals from fitted generalized linear models via simulation and evaluated model fit with Q-Q plots and diagnostic tests (e.g., dispersion and Kolmogorov–Smirnov tests) using the package DHARMa. 67 We used a combination of diagnostic plots and proportional hazards tests of the fitted Cox models to evaluate the proportional hazards assumption. 68 We produced conditional predicted effects from generalized linear models and Cox models using the packages ggeffects and survminer, respectively. 69,70 For the Cox models, we produced adjusted survival curves and obtained conditional inverse survival probabilities to present weekly recovery and weekly RTP probabilities. 71 For both the generalized linear and Cox models, we calculated effect sizes for categorical comparisons (e.g., difference between sexes) as Cohen’s d and for continuous relationships (e.g., effect of number of previous concussions on preexisting conditions) as Pearson’s correlation coefficient. 72 We based inferences on a combination of coefficient (β) or hazard ratio (HR) estimates, 95% confidence intervals, p values, and effect sizes. The statistical significance threshold was p < 0.05, whereas biological importance was determined based on effect size values with the following scale 72,73 : (1) nominal magnitude: d < 0.2 or r < 0.7; (2) small magnitude: 0.2 ≤ d < 0.5 or 0.7 ≤ r < 0.8; (3) medium magnitude: 0.5 ≤ d < 0.8 or 0.8 ≤ r < 0.9; and (4) large magnitude: d ≥ 0.8 or r ≥ 0.9. Because effect sizes are invariant to sample size, we placed more inferential weight on effect sizes. 72,74
Results
Females had slightly more (56.5%) concussions than males (43.5%), but the sex ratio was not statistically different from 1:1 (χ 2 = 0.08; p = 0.78). All student-athletes reported either having or not having a history of concussion; 56.5% responded as never having been diagnosed with a concussion before, and only 1 male participant reported a history of >3 previous concussions. For questions regarding prior diagnosis of preexisting conditions, participants responded either “yes” or “no” for preexisting conditions: ADHD (n = 6; 7.1%), anxiety (n = 10; 12.7%), depression (n = 11; 12.2%), mood disorders (n = 5; 6.5%), LDs (n = 4; 4.6%), and headache/migraine disorders (n = 5; 7.4%). A participant could report “yes” to more than one condition; see Table 1 for summary.
Descriptive Characteristics of Sex, Age, Sport, Concussion History, and Preexisting Conditions Reported Among College Athletes in the Pac-12 Conference
A majority of participants were female, with overall mean age of 20.5 years. There was a total of 92 concussion incidents, which met inclusion criteria. A majority, but not all participants, had information regarding preexisting ADHD (n = 85), anxiety (n = 79), depression (n = 90), mood disorders (n = 90), learning disorders (n = 77), and headache/migraine disorders (n = 87). All participants reported previous concussion history.
Percent “yes” of total number of participants who responded to each condition.
Percent “yes” of total females who responded to each condition.
Percent “yes” of total males who responded to each condition.
ADHD, attention-deficit hyperactivity disorder.
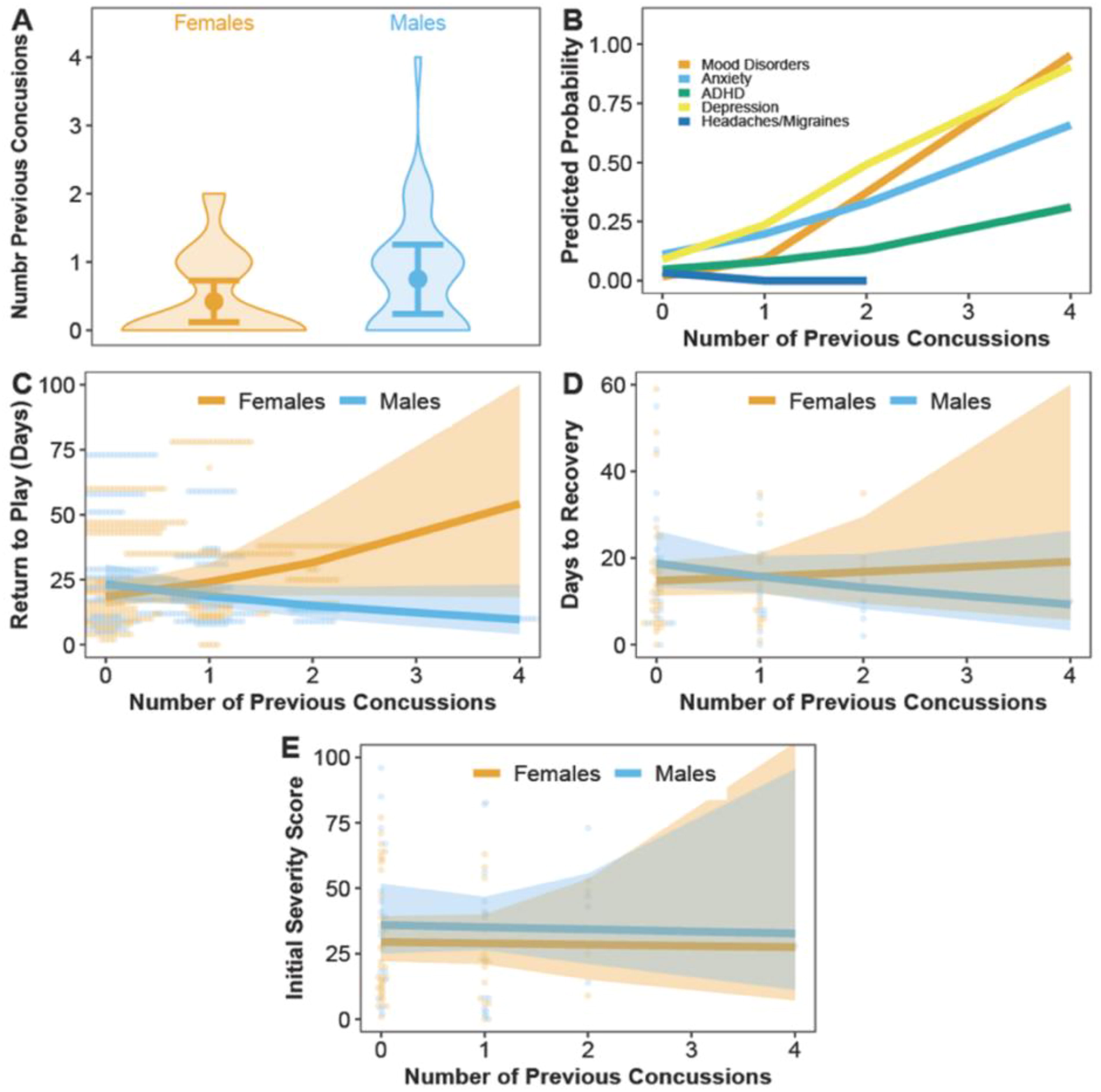
Among all considered distributions, generalized linear models with the negative-binomial error distribution best described the SCAT5 initial symptom severity scores (ΔAIC = 1.58–1452.47). Because of the small sample size for males, models that evaluated the influence of athletes having the learning disability preexisting condition on initial symptom severity scores did not converge and were therefore excluded from further consideration. Although no statistically significant differences existed between female and male athletes who did or did not have the other five preexisting conditions (βSex*Condition = −0.43–1.12; p = 0.07–0.91; Fig. 1A–E), effect sizes for differences between females and males who had mood disorders or had ADHD were medium (d = 0.51) and large (d = 0.93), respectively. Male athletes with mood disorders or ADHD were estimated to have 8 and 17 units higher initial symptom severity scores than females, respectively. The number of previous concussions that an athlete had was not predictive of initial symptom severity scores (βConcussions = −0.02; p = 0.93) nor did a difference between sexes exist (βConcussions = −0.006; p = 0.98; Fig. 2E).

Model-predicted mean marginal effects point estimates (solid dots) and their 95% confidence intervals (error bars) of sex-specific initial injury severity scores for student-athletes who sustained a concussion and reported “no” or “yes” to having
Model-predicted mean marginal effects point estimates (solid dots or solid lines) and their 95% confidence intervals (error bars or ribbons) of the
Among all considered distributions, generalized linear models with the Poisson error distribution best described the number of previous concussions that athletes had (ΔAIC = 2.00–185.44). Male athletes were estimated to have, on average, one more previous concussion than females, which was a statistically significant difference with medium effect size (βSex = 0.57; p = 0.04; d = 0.57), and males were also more likely than females to have >2 previous concussions (Fig. 2A). No evidence existed for sex differences in the probabilities of having any of the considered preexisting conditions (βSex = −0.11–1.63; p = 0.07–0.99); however, the number of previous concussions was a statistically significant predictor of athletes having mood disorders, depression, and anxiety (βConcussion = 1.14–1.77; p = 0.04). After disregarding the uninformative sex effect (i.e., combining sexes), the probabilities of athletes having mood disorders, anxiety, ADHD, and depression all increased with increasing numbers of previous concussions (p = 0.008–0.04), whereas the probability of athletes having headaches or migraines was low and approximately stable as the number of previous concussions increased (p = 0.33; Fig. 2B).
Among all considered distributions, generalized linear models with the negative-binomial error distribution best described recovery and RTP times (ΔAIC = 1.00–656.71). The number of previous concussions was not a statistically significant predictor of recovery times for either sex (βSex*Concussion = −0.24; p = 0.30; d = 0.14; Fig. 2D). In contrast, a statistically significant interaction between sex and number of previous concussions existed in the RTP model (βSex*Concussion = −0.49; p = 0.02), such that females with 2, 3, and 4 previous concussions were estimated to have required 17, 30, and 44 more days to RTP than males; however, the lack of observations at 3 and 4 previous concussions and corresponding wide confidence interval around the point estimate for females resulted in considerable uncertainty about those sex differences (Fig. 2C). Effect sizes for those RTP time differences between sexes at 2, 3, and 4 previous concussions were d = 0.31, 0.51, and 0.72; effect sizes for the relationship between number of previous concussions and RTP times for females and males were very large (females: r = −0.99, p = 0.001; males: r = 0.99, p = 0.001). Male athletes with more previous concussions required fewer days to recovery and RTP than males that had fewer previous concussions (recovery: Δ0–4 concussions = 10 days; RTP: Δ0–4 concussions = 13 days).
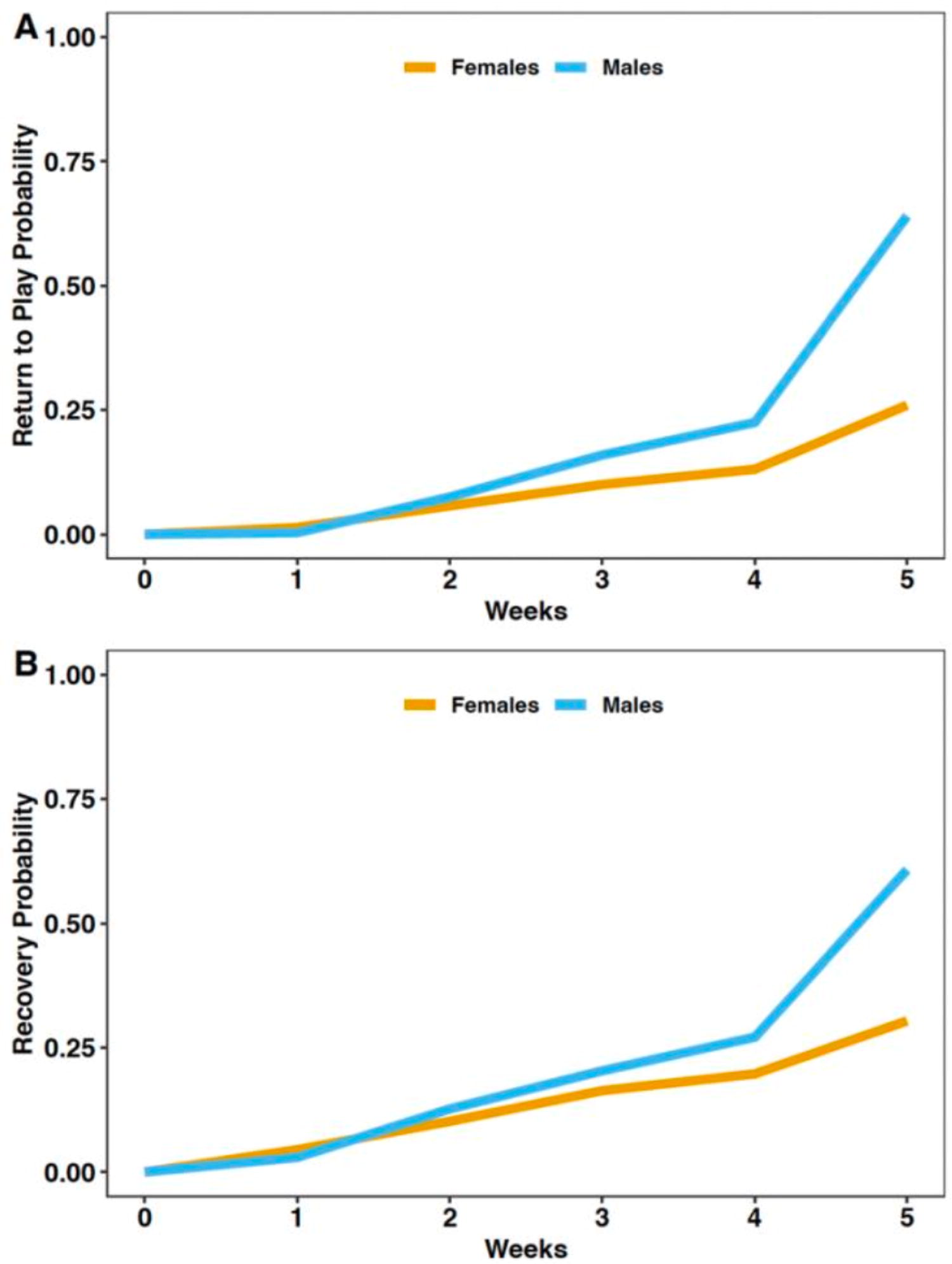
Although a statistically significant difference between sexes did not exist in the HRs for weekly recovery and RTP probabilities (recovery: HRSex = 1.62, p = 0.17; RTP: HRSex = 1.19, p = 0.57; Fig. 3A–B), the effect sizes were medium and very large, respectively (recovery: d
Sex = 0.56; RTP: d
Sex = 1.36). However, the fixed effect for sex violated the proportional hazards assumption of Cox models for both the recovery and RTP probabilities (recovery:
Predicted weekly probabilities of
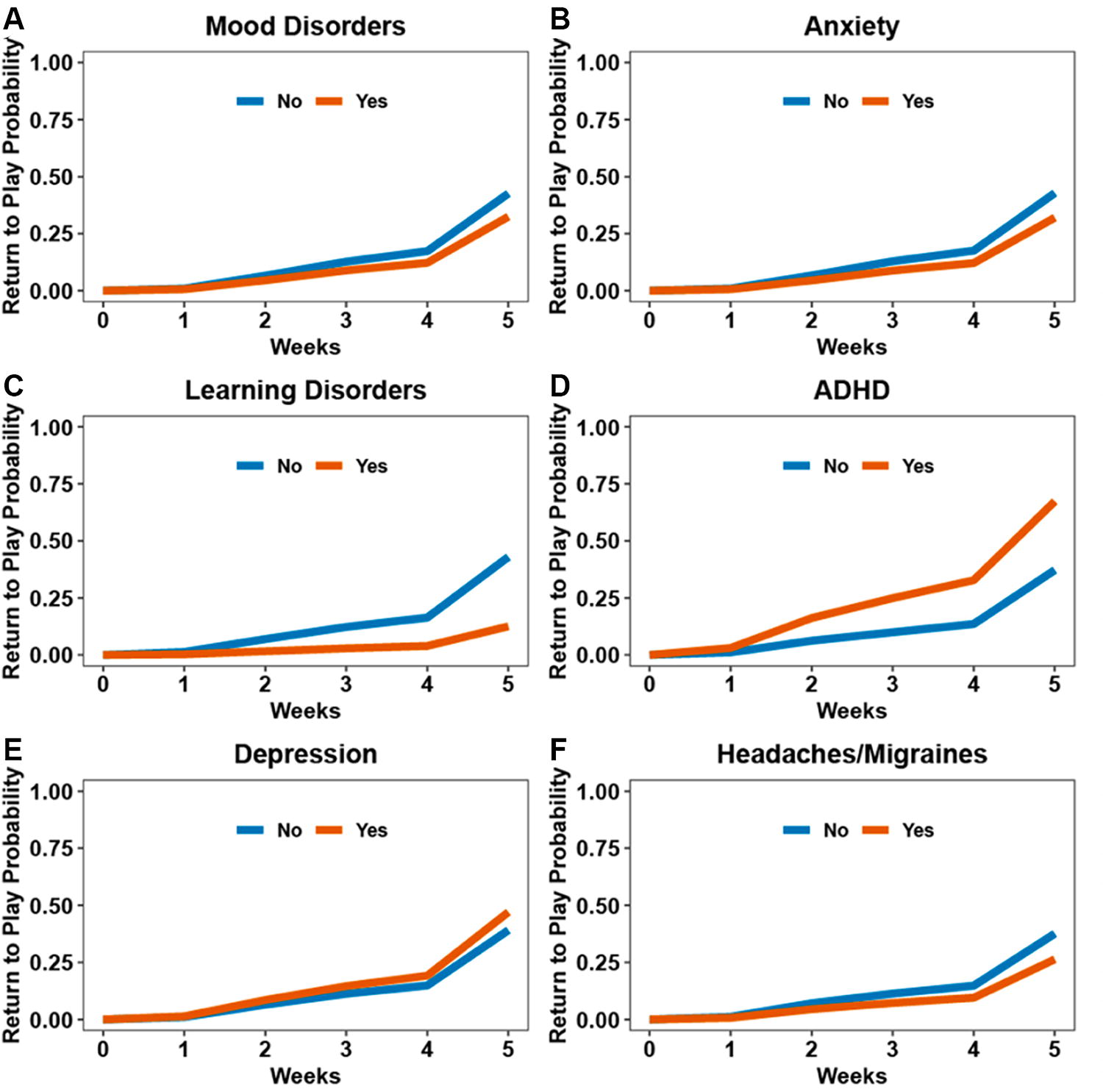
Statistically significant HRs for weekly recovery probabilities existed only for LDs and ADHD (HRLearning = 0.32, p = 0.04; HRADHD = 3.38, p = 0.02; Fig. 4A–F). Athletes without LDs or with ADHD had, on average, 0.14 and 0.26 higher weekly recovery probabilities than athletes with LDs or without ADHD, respectively. Athletes with ADHD also had the highest overall mean weekly recovery probability among all preexisting conditions (weekly mean Pr = 0.44). Effect sizes for the differences between athletes who did or did not have LDs or ADHD were very large (d = 1.96–2.30). In contrast, the HRs and weekly recovery probabilities were similar between athletes who did or did not have the other four preexisting conditions, and all those effects had small effect sizes (p = 0.37–0.90; d = 0.12–0.44).

Predicted weekly recovery probabilities for student-athletes who sustained a concussion and reported having
Similarly, statistically significant HRs for weekly RTP probabilities existed only for LDs and ADHD (HRLearning = 0.22, p = 0.0003; HRADHD = 2.74, p = 0.04; Fig. 5A–F). Athletes without LDs or with ADHD had, on average, 0.11 and 0.15 higher weekly RTP probabilities (faster weekly RTP times), respectively, than athletes with LDs or without ADHD. Athletes with ADHD also had the fastest weekly RTP time among all preexisting conditions (weekly mean Pr = 0.29). Effect sizes for the differences between athletes who did or did not have LDs or ADHD were very large (d = 1.71–4.14). Although the HRs and weekly RTP probabilities were statistically similar between athletes who did or did not have the other five preexisting conditions, all those differences had medium effect sizes (p = 0.49–0.60; d = 0.53–0.62).
Predicted weekly return-to-play probabilities for student-athletes who sustained a concussion and reported having
Discussion
This study examined potential associations among concussion history, preexisting conditions, and sex with initial symptom severity and recovery time from SRC within a cohort of collegiate athletes. Consistent with findings of previous research, concussion history was not associated with initial symptom severity after concussion, 17,18 nor did a difference between males and females exist. However, among athletes with mood disorders or ADHD, males were estimated to have higher initial symptom severity scores than females, with medium and large effect sizes, respectively. In a study of high school and college athletes, depression was elevated from baseline levels 2–14 days post-SRC, but no sex differences were reported. 76 Evidence also exists of higher concussion-like symptom reporting both pre- and post-SRC in high school and college athletes with ADHD, 77,78 and considerable symptom overlap exists between concussion and ADHD (e.g., difficulty concentrating and remembering, irritability, emotionality, and sleep difficulties). Consequently, athletes with ADHD may report greater symptom severity post-SRC as a result of ADHD symptom exacerbation. Sex-based differences in the effects of ADHD have been reported in adults, 79,80 with males often being more functionally affected in educational matters 79 and global functioning 80 than females. Collectively, said results from prior studies and our findings suggest that male athletes with ADHD may report greater initial symptom severity scores than females; although male athletes may be less likely to report symptoms of mood disorders because of stigma surrounding mental health, 81 male athletes are likely experiencing mood and depression-like symptoms that may ultimately exacerbate SRC symptoms and severity.
Despite our models estimating that male athletes had, on average, one more previous concussion than females, both sexes had similar probabilities of having all the considered preexisting conditions. Similarly, a separate study found that among collegiate athletes with ADHD, LD, and ADHD+LD, a statistically significant difference did not exist between sexes for history of one or multiple concussions. 21 Nevertheless, we found that, regardless of sex, the number of previous concussions was a statistically and biologically significant predictor of athletes reporting preseason mood disorders, depression, anxiety, and ADHD. Similar to our results, previous concussion history was associated with a 3.3-fold greater risk for depression diagnosis in participants aged 12–17 years. 82 Collegiate athletes with ADHD and a history of concussion had 16.4× and 7.9× greater odds of exhibiting clinically significant symptoms of state anxiety and depression, respectively, compared with control athletes. 83 Ultimately, our results support that having a history of prior concussion may increase the risk of developing symptoms of mood disorders, depression, anxiety, and ADHD. Therefore, it is imperative that athletes with a history of concussions are screened for mental illnesses and are provided mental health resources to mitigate the potential for long-term consequences.
Although the number of previous concussions reported was not a significant predictor of recovery time for either sex, which was similar to findings of other studies, 10,84 we found that female athletes with ≥2 previous concussions required more days to RTP than males. Additionally, weekly recovery and RTP probabilities between sexes, despite not being statistically significant, had biologically significant effect sizes (recovery: d Sex = 0.56; RTP: d Sex = 1.36) that strongly supported sex differences. Some previous studies found no sex difference in time to RTP, but those studies did not investigate differences between participants with concussion history and relied on a smaller sample size of female athletes. 41,42 In contrast, other studies found that female athletes often require more time to symptom resolution than males, 39,40 which may ultimately prolong RTP times in females. 85 Similarly, it has been reported that female athletes required significantly longer to start RTP progression after SRC than age-matched male athletes 86 ; however, athletes with a history of >1 SRC, or history of non-SRC, were excluded in that study. Thus, the inclusion of athletes with previous concussions is a strength of our study that contributes to a gap in SRC research.
RTP progression in our sample of collegiate athletes relied on subjective symptom reporting at stages of increased sport-specific training; therefore, it is possible that females with ≥2 prior SRCs exhibited more caution and therefore more accurate symptom reporting than males, which contributed to longer RTP times for females. Athletes with ≥2 prior SRCs may suffer from more numerous and more intense symptoms, 87 and females may more accurately report those symptoms. In general, females report more bodily distress and more intense and frequent somatic symptoms compared with males, 88 regardless of the response format and whether symptom recording is prospective or retrospective. It is also possible that male athletes may incur more pressure from coaches and fans to play while injured, 89 thereby inducing riskier decision-making and symptom underreporting that could reduce RTP times. However, more research is necessary to understand how previous concussion history may impact SRC symptom reporting and outcomes in both male and female athletes.
We also found substantial evidence that, regardless of sex, athletes without LD and with ADHD had much higher weekly recovery and RTP probabilities than athletes with LD and without ADHD, respectively. Athletes with ADHD also had the highest overall mean weekly recovery and RTP probabilities among all preexisting conditions. Some studies found that LD 11 and ADHD 12 were associated with prolonged concussion recovery, whereas others did not. 84,90 These mixed findings may be the result of considerable symptom overlap for LD and concussion, such as difficulty concentrating and attention and memory deficiencies. 91 Individuals with LD who experience those symptoms prior to concussion may exhibit symptom worsening postconcussion and require more time to symptom resolution. 91,92 In contrast, the faster time to RTP for athletes with ADHD may be influenced by characteristics typically associated with ADHD or the use of ADHD-related psychostimulants. 93 In a study of adults aged 20–40 years, ADHD was associated with a higher propensity to engage in risky behavior 94 ; therefore, athletes with ADHD may take greater risks and disregard symptoms of concussion or have less care to reach complete asymptomatic status before RTP than athletes without ADHD.
Despite not being statistically significant, we also found evidence based on effect sizes that weekly recovery and RTP probabilities for athletes with anxiety, depression, mood disorders, and headache/migraine disorders may be lower than for athletes without those preexisting conditions. These findings corroborate those of prior studies that investigated collegiate athletes subjected to a SRC 95 and older adults subjected to a mild traumatic brain injury, in which participants with preinjury anxiety and depression were more likely to require prolonged recovery time. 96,97 Individuals with preexisting conditions may experience exacerbated symptoms of those conditions postconcussion, 30 ultimately prolonging recovery and RTP times as they attain asymptomatic status.
Limitations
Results from this study should be interpreted in the context of some methodological limitations. Due to the cross-sectional nature of retrospective self-reported preexisting condition diagnoses and prior concussion history, we cannot establish a causal influence of prior concussion and risk of developing those reported conditions. Nor were we provided any information regarding the mechanism or severity of prior concussions, which may contribute to the conditions being reported. However, to control for the mechanism of injury, only SRCs that took place in season were used to determine severity and recovery outcomes. Additionally, because of perceived stigma, it is possible that some athletes did not accurately report their diagnoses of preexisting conditions. 98 Furthermore, not all institutions required participants to complete reporting on these preexisting conditions, possibly causing underreporting of conditions at baseline, as well as small sample sizes across conditions. To the best of our knowledge, there are no prior studies that report the prevalence of depression, mood disorders, LDs, anxiety, or headache/migraine disorders within collegiate athlete populations. However, consonant with other studies, 7.1% of athletes reported a previous diagnosis of ADHD, 20,93,99 indicating that the prevalence of preexisting conditions reported within this population is likely generalizable to other collegiate athlete populations. Prior diagnosis of concussion was also self-reported and, therefore, may be underreported because of a lack of education for signs of concussion and prevalent underreporting of concussion in adolescent athletes. 100,101 However, heightened public concern over the long-term effects of concussion may be leading people of all ages to seek care, as the total number of concussion diagnoses has steadily increased over the last 5 years. 102 In clinical sports medicine, brain imaging prior to the start of a sport season is not a prescribed practice; therefore, no correlations between previous concussion diagnoses and pathological findings can be investigated. Lastly, the use of medication to treat some preexisting conditions, such as ADHD or depression, was not reported by athletes in our study and therefore could not be controlled for in the analyses.
Conclusions
The biologically significant findings from our study of Pac-12 collegiate athletes have important clinical implications. We found that collegiate athletes with a history of concussion had higher probabilities of reporting preexisting depression, mood disorders, anxiety, and ADHD. Yet, although those conditions are highly prevalent among collegiate athletes 29,30 and often comorbid, 103 ∼20% of queried sports medicine physicians reported not discussing psychological issues related to injury, such as depression and mood disorders, when treating athletes. 104 Although we cannot infer whether conditions developed before or after a participant sustained a prior concussion, noting previous diagnoses of concussion in medical history during preparticipation exams may help clinicians identify athletes who may also be experiencing symptoms of these conditions but have gone undiagnosed or untreated prior to starting collegiate athletics, as well as identify those who may be at risk for increased symptom severity and prolonged recovery after SRC. 7 –9,12,17,28,30,105
The present findings also suggest that having ADHD or LDs may influence time-to-recovery and time to RTP for collegiate athletes. Although ADHD was associated with shorter recovery and time to RTP compared with all other preexisting conditions, LD was associated with longer recovery and time to RTP. Athletes with ADHD and LD often exhibit concussion-like symptoms at baseline. 91 Athletes with ADHD may also engage in riskier behavior 94 and ignore symptoms of concussion in order to RTP quicker. Therefore, acknowledging the diagnosis of ADHD and/or LD may prove beneficial during neurocognitive testing and in recovery and management after SRC.
The results of this study highlight the importance of screening athletes for concussion history and preexisting conditions to determine the potential risks of negative outcomes postconcussion. Collegiate medical and coaching staff should expect that athletes with some preexisting conditions, particularly mental illnesses and mood disorders, may necessitate longer recovery and RTP times than athletes without those conditions. A yearly mental health screening should be provided to athletes throughout their collegiate career in order to account for the development of mental health conditions. Athletes diagnosed with preexisting conditions may also require tailored preventative care and extra support to manage symptoms experienced postconcussion.
Transparency, Rigor, and Reproducibility
This study was approved by the University of Colorado, Institutional Review Board (22-0289). This was a retrospective study that was not human subject research. A total of 92 concussions met inclusion criteria for this study. History of preexisting conditions was self-reported by the athlete during Year 1 baseline testing, which was completed prior to the start of their first athletic season. Concussion diagnoses were made by clinicians at each participating institute. Recovery from injury was assessed based on clinical visits and returned symptom surveys. Data were collected by clinicians and athletic trainers at each institute, with oversight completed by research coordinators to ensure completion and correctness. All information collected was confidential, and patients had a unique study ID, so that participants’ names were not associated with any information collected. Data may be provided upon reasonable request. The methods section explains the nature of the statistical tests used. All the analyses were performed by two of the coauthors using R.4.2 (R Foundation for Statistical Computing). All authors have agreed to publish the article, and consent for publication was given by the Pac-12 Health Analytics Program.
Footnotes
Authors’ Contributions
N.A.K. assisted with conceptualization, data collection, and formal analysis and led writing of the article. S.M.M. led statistical analyses and assisted with reviewing and editing the article. R.K.R. assisted with formulating the research questions, analysis, and reviewing and editing of the article. B.M.W., K.G.H., S.K.P., and T.D.H. assisted with reviewing and editing of the article and providing final approval of the version published.
Author Disclosure Statement
The authors have no competing interests to disclose.
Funding Information
This project was supported, in part, by the