
Abstract
Chronic post-traumatic headache (CPTH) after a mild traumatic brain injury (mTBI) has been reported in up to 60% of patients and can be extremely debilitating. While pharmacological treatments are typically used for CPTH, they frequently cause side effects and have limited effectiveness, leading individuals with CPTH to be unsatisfied with current treatment options and to seek nonpharmacological options. Acupuncture has been identified as a potential treatment option; however, the evidence in this population remains limited. The overall goal of this study was to examine the effect of a once weekly (e.g., low dose) versus twice weekly (e.g., high dose) of acupuncture treatment on CPTH in individuals with mTBI. Thirty-eight individuals were randomized to receive either 5 or 10 acupuncture treatments using a standard protocol over 5 weeks. The protocol consisted of 14 points using traditional acupuncture and 4 points using electroacupuncture. Headache outcomes, safety, treatment adherence, sleep quality, and quality of life (QOL) were assessed. The results showed that while there were no differences between dose groups for any of the outcomes assessed, acupuncture significantly reduced the number of headache days and headache pain intensity in individuals with CPTH. There were no significant changes in acute medication use or sleep quality. While there were some QOL improvements identified, these results should be interpreted with caution. Overall, acupuncture was shown to be safe and well-tolerated in people with CPTH after mTBI, and five acupuncture treatments using a standardized protocol shows promise in providing headache relief for this population.
Introduction
Chronic post-traumatic headache (CPTH) after a mild traumatic brain injury (mTBI) is the most frequent type of chronic pain reported after injury. 1 It has been estimated that approximately 17.1 million Americans experience a traumatic brain injury (TBI) each year, 2 with up to 90% of individuals experiencing headache in the acute period (<3 months) 3 and up to ∼60% in the chronic period (≥3 months). 4 CPTH typically presents as a tension-like (mild-moderate dull pain), migraine headache (moderate-severe throbbing pain), or combined tension-like and migraine headache. 1 On average, the number of reported headache days each month for individuals with CPTH is 25–26, 5,6 or almost daily. Individuals with CPTH have been reported to be more likely to have post-traumatic stress disorder, cognitive symptoms, and somatic symptoms. 6 They are also more likely to perceive difficulties in their physical and social function. 6 Thus, CPTH can be extremely debilitating and dramatically impact function and quality of life (QOL).
There are currently no Food and Drug Administration-approved pharmacological treatments specifically for CPTH, and the long-term effects of pharmacologic treatments on recovery after TBI are unclear. 7 CPTH often results in symptoms similar to primary headache disorders; therefore, they are typically treated off-label with pharmacologic treatments based on the primary headache phenotype, which is due to the lack of research evidence. 3,8 However, in a recent study examining 100 people with CPTH after mTBI, 87% reported that they are not satisfied with their current treatment status. 5 The long-term effects of pharmacologic treatments on recovery after TBI are unclear 7 but are often prescribed for headache and migraine treatment. These prescription medications are often coupled with the recommendation of including nonpharmacological treatments, such as physical therapy, biofeedback, and relaxation training. 9
Acupuncture, a traditional Chinese method where fine needles are inserted into specific areas of the body to achieve a therapeutic benefit, 10 is a potential nonpharmacologic, complementary treatment for CPTH. Acupuncture has been used and reported by physicians in the United States as early as the 1600s and has been researched since the 1800s. Most of the early reports were of individual patient cases, whereas the first randomized controlled trial (RCT) of acupuncture treatment was published in 1975. 11
Research has provided evidence for the benefits of acupuncture for several medical indications. Acupuncture has been shown to be a safe and effective treatment for individuals with chronic pain, 12 tension headache, 13,14 and migraine. 15 In addition, acupuncture has been shown to be more effective than, or as effective as, pharmacotherapy with fewer side effects for several conditions. 15 –17 It has also been shown to decrease migraine 15,16 and tension headache 15 frequency, reduce pain intensity, 15,16,18 decrease the use of acute medication, 18 and improve QOL. 16 Importantly, the safety of acupuncture has also been well documented. Although both minor and serious adverse events (SAEs) have been reported, serious complications related to acupuncture are very rare. 19
While acupuncture is currently a well-accepted nonpharmacological treatment for several medical conditions, it has not been extensively examined in individuals with CPTH. Although there have been acupuncture studies as early as the 1980s that have shown improvements in headache symptoms for individuals who have experienced an mTBI, 20,21 there have been a limited number of English-language reported studies since. In two case reports, acupuncture improved acute post-traumatic headache symptoms in individuals with an mTBI. 22,23 In another three-arm RCT, acupuncture improved headache-related QOL and reduced overall pain in adult service members with mild-to-moderate TBI and CPTH. 24 There have also been two recent protocols published for systematic reviews on the topic of acupuncture for CPTH, which will both examine Chinese and English databases; however, to our knowledge, these systematic reviews have not yet been published. 25,26 Although there is a paucity of research examining acupuncture for CPTH, acupuncture has shown safety and efficacy in patients with chronic headache and migraine and has therefore been recommended as an adjunctive treatment for CPTH. 24,27 While they did not examine CPTH specifically, four RCTs investigated acupuncture treatment in individuals with TBI and reported no AEs. 28 Thus, acupuncture could potentially be a safe and viable treatment option for individuals with mTBI and CPTH.
Because acupuncture for CPTH has not been extensively examined, there is also no consensus on the number of acupuncture sessions that are necessary for improvement. 22,23 In the study of service members with mild-to-moderate TBI and CPTH, 10 sessions of acupuncture were administered over 6 weeks led to an improvement in headache-related QOL and reduced overall pain. 24 In a recent article regarding clinical indications for acupuncture for CPTH, 6–10 weekly or twice-weekly acupuncture sessions were reported to be most effective. 27 Consequently, the amount of acupuncture necessary for headache improvement in individuals with CPTH is still unclear. Thus, the primary goal of this study was to determine the effect of a low versus high dose of acupuncture treatment on number of headache days, headache outcomes, and acute medication use for individuals with CPTH. Due to the paucity of literature, this study also aimed to determine the safety and tolerability of acupuncture in individuals with CPTH and to explore the effects of acupuncture on sleep quality and QOL in individuals with CPTH.
Methods
Subjects and study design
Thirty-nine patients were recruited from 2019 to 2023 to participate in this two-arm RCT (NCT04369911). The study was approved by the organization’s Institutional Review Board, was conducted according to the Declaration of Helsinki, and followed Good Clinical Practice Guidelines. All participants provided informed consent. Inclusion criteria included: (1) age 18–70, (2) diagnosis of mTBI (as defined by ICHD-3L a. either no loss of consciousness or loss of consciousness of <30 min duration, b. Glascow Coma Scale (GCS) ≥13, and c. symptoms and/or signs diagnostic of concussion 29 ), ≥3 months and ≤2 years at the time of study enrollment, (3) CPTH of any etiology (e.g., tension or migraine) with chronic defined as developed within 7 days after injury and lasting ≥3 months from the time of injury, 29 and (4) ability to provide and provision of signed and dated informed consent form. Exclusion criteria included: (1) individuals who were non-English speaking, (2) participation in acupuncture treatment outside of the study, while enrolled, (3) history of pre-existing primary headache, defined as more than 12 days of tension-type headache annually and/or more than one migraine attacks per month in the last year, 6 (4) history of any other serious neurological, psychiatric, chronic pain disorders, or seizures, (5) history of bleeding diathesis, other bleeding disorders, or syncope with needle puncture, (6) history of cardiac arrhythmia or current pacemaker, neurostimulator, or other implanted stimulation device, (7) recent or active substance use disorder, (8) women who are currently pregnant, lactating, or planning to become pregnant during the study, (9) any other medical conditions that could affect their ability to participate in acupuncture treatments for the study duration (as determined by study investigators), (10) active participation or past participation ≤3 months in any other interventional study, and (11) unwilling to participate in all study-related activities.
Participants were primarily recruited from the institution’s outpatient clinics and rehabilitation departments. Study recruitment materials were also provided to researchers and clinicians in other local health care systems, as well as community outreach and advocacy partners. Following consent, participants were randomized into two arms: (1) low acupuncture (5 total treatments) and (2) high acupuncture (10 total treatments). Balanced treatment assignments were achieved using permuted block randomization with random block sizes stratified by sex, based on evidence that females have reported higher rates of headache. 30 The study biostatistician generated a randomization schedule using the SURVERYSELECT procedure in SAS. Assignments were not seen by the other study personnel and were not changed after randomization.
Following randomization, participants were instructed to track information about their headaches via a headache diary (Supplementary Table S1) for the next 4 weeks. Each day, participants were instructed to record whether they had a headache, and if applicable, the headache duration, pain intensity (rated on a scale of 0–10 with 0 being no pain and 10 being the most severe pain), headache type (e.g., tension, migraine), and the name and dose of any medication taken. Prior to their first acupuncture treatment, participants completed sleep quality and QOL assessments (see Outcome Measures) during a pretreatment visit (Fig. 1). Next, participants underwent approximately 5 weeks of acupuncture treatment (once a week or twice a week depending on randomization). On the last day of acupuncture treatment, participants were provided post-treatment headache diaries and instructed to track their headaches for the next 4 weeks (weeks 1–4 following acupuncture), then take a 4-week break, and then begin tracking their headaches again for the last 4 weeks of the study (weeks 9–12 following acupuncture). Participants completed the sleep quality and QOL assessments again at the 4-week post-treatment visit and the 12-week post-treatment visit (Fig. 1). All data for the study were collected electronically via Research Electronic Data Capture (REDCap). REDCap is a secure, web-based software platform designed to support data capture for research studies. 31,32

Study timeline of participant activities.
Intervention
Acupuncture treatments were administered by licensed acupuncturists with a master’s degree level of training in acupuncture (or higher) from accredited institutions, and >5 years of clinical experience. Acupuncturists had prior experience treating patients with neurological injuries or diagnoses. Before administering the study intervention, the acupuncturists completed training sessions of the treatment protocol with practice of the methods of administration to ensure intervention consistency between providers.
Standard, sterile stainless-steel, disposable needles (DongBang™ Corporation, Spring Ten 0.25 × 30 mm; Boryeoung, Republic of Korea) were inserted in the acupuncture point locations (described below), with a total of 18 needles used for each treatment session. The depth of the needle insertion was approximately 10–20 mm. Needle reaction (soreness, numbness or distended feeling around the point, also known as a Deqi sensation) occurred during the initial insertion. Following 10 min of retention, all needles (except points St36 and LI4 under electrostimulation) were rotated to maintain Deqi sensation. Maintaining Deqi sensation has been shown to increase the effectiveness of acupuncture. 33,34 All needles were left in place for a total of 30 min, which is a typical duration in clinical practice. It also is a common duration of previously reported clinical trials of acupuncture for headache and migraine. 15,16,35
Acupuncture points were selected for their classical indications, anatomical locations, effect on pain networks 36,37 and influence on cerebral blood flow. 38 The anatomical location for each point was based on the World Health Organization’s acupuncture point guideline. 39 Electroacupuncture was administered with a Pantheon Research electrostimulation 8c pro machine (Pantheon Research Inc; Huntington Beach, CA), with a continuous milliampere wavelength of 2 Hz at bilateral points, stomach 36 (ST36) and large intestine 4 (LI4). The intensity was gradually increased to a comfortable level that participants could tolerate, without the sensation of pain. Traditional Chinese manual acupuncture was used at eight acupuncture points: yin tang (YT) and Du20, and bilateral points, liver 3 (LV3), urinary bladder 2 (UB2), small intestine 19 (SI19), extra point Anmian (EX-22), and two auricular points Shen Men (SM) and point zero (PtZ) (Fig. 2). During treatment sessions, up to two acupuncture needles were allowed to be removed if needed, due to extreme pain or discomfort.
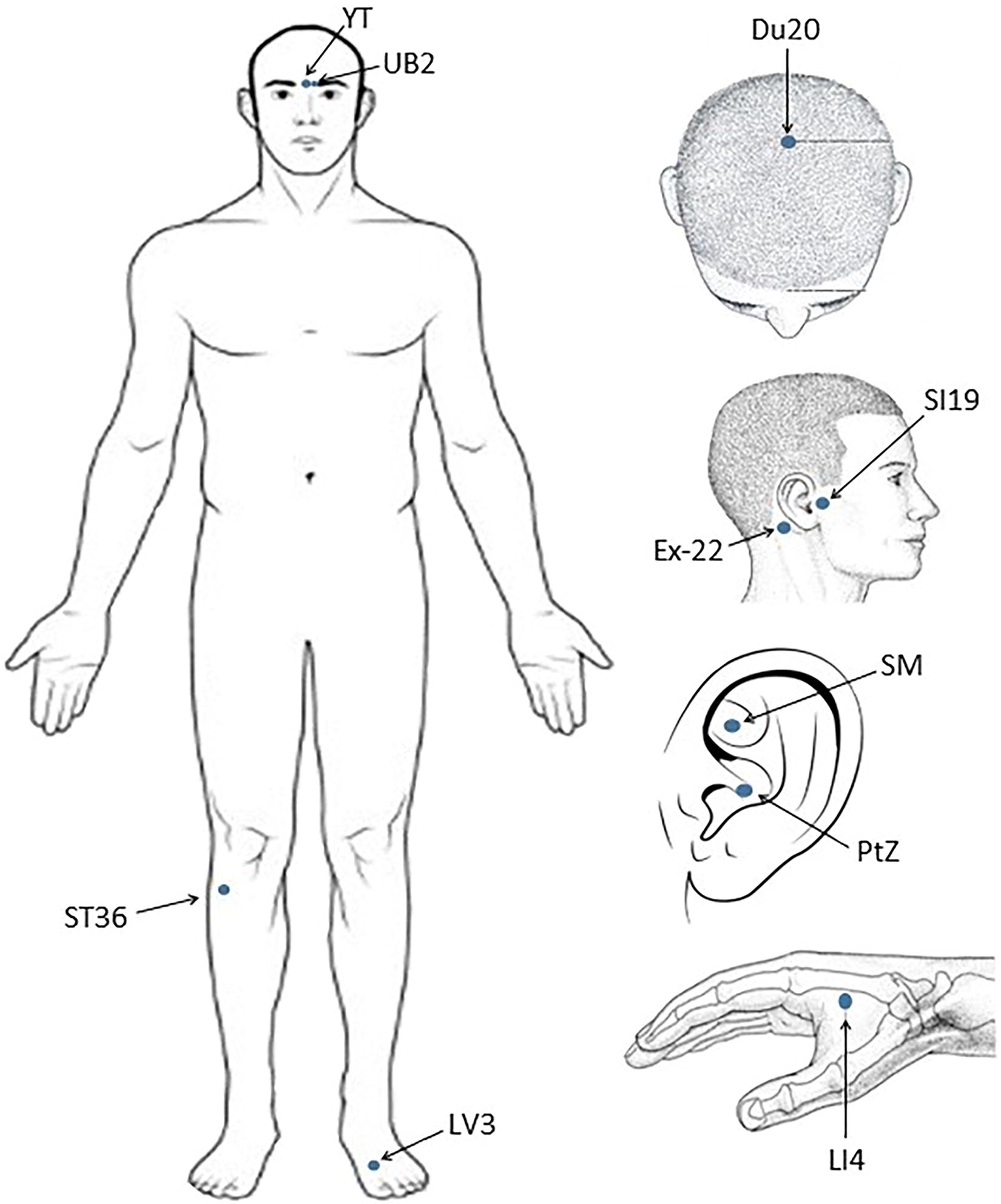
Acupuncture treatment points used for the study intervention. *Note: Bilateral acupuncture points were utilized, as appropriate.
Outcome measures
The primary outcome measure for Aim 1, number of headache days over a 4-week period, was captured via self-report headache diaries in the 4 weeks before treatment (pretreatment), 4 weeks immediately after treatment (4 weeks post-treatment) and weeks 9–12 after treatment (12 weeks post-treatment). Headache intensity (scored 0–10 with 0 being no pain and 10 being the most severe pain) and acute medication use (percent of headache days with medication use reported) were also collected via the self-report headache diaries.
Aim 2 outcomes included safety and treatment adherence. Safety was assessed by recording any AEs or SAEs. AE/SAEs were classified by type, severity, and relatedness to treatment. Treatment adherence was assessed by calculating the percentage of treatment sessions completed for each participant.
Exploratory outcomes included sleep quality and QOL and were assessed via survey at pretreatment, 4-week post-treatment, and 12-week post-treatment visits. Sleep quality was assessed via self-report using the Pittsburgh Sleep Quality Index (PSQI), which contains 19 items regarding one’s usual sleep habits during the past month. 40 Each item is weighted on a 0–3 interval scale. The global score is calculated and ranges from 0 to 21, with a lower score indicating a healthier sleep quality. 40 QOL was assessed via self-report using the traumatic brain injury-quality of life (TBI-QOL) v1.0 short forms, which includes the following item banks: ability to participate in social roles and activities, anger, anxiety, cognition-general concerns, communication, depression, emotional and behavioral dyscontrol, executive function, fatigue, grief-loss, headache pain, independence, mobility, pain interference, positive effect and well-being, resilience, satisfaction with social roles and activities, self-esteem, stigma, and upper extremity. 41 Scores for each short-form were summed to create a raw score, which was converted to a T-score (mean of 50 [SD = 10]) using the lookup tables provided. For each item bank, a higher score indicated either better or worse functioning compared to the average for individuals with TBI. 41
Statistical analysis
Baseline variables were compared between arms to ensure randomization achieved balanced treatment assignments. Variables were summarized using descriptive statistics (e.g., mean and SD, or frequency and proportion) and compared inferentially. Continuous variables were compared using two-sample t-tests or Wilcoxon rank tests and discrete variables were compared using chi-square tests for independence or Fisher’s exact tests. Sex-stratified randomization resulted in two comparable arms; therefore, all planned analysis was performed without adjustment for covariates.
The average number of headache days, headache intensity, and acute medication use at all three time points (pretreatment, 4 weeks post-treatment, 12 weeks post-treatment) were calculated from self-reported headache diaries. A set of linear mixed models (LMMs), with a random intercept to account for individual effects, were used to evaluate the change in outcome over the study period, accounting for differences between arms and any interaction between treatment arm and time period.
Safety was assessed by summarizing the occurrence of AEs/SAEs, severity, and relatedness to treatment. AEs were stratified by study arm, severity, and relatedness to treatment. Treatment adherence was assessed by calculating the percentage of treatment sessions completed for each participant. Aim 3 exploratory outcomes were summarized and analyzed similarly to the Aim 1 analysis.
Target enrollment was determined based on achieving adequate power to detect a 4.5-day difference in mean number of headache days over 4 weeks from a parallel-group design using a two-sided, two-sample t-test with a p value of <0.05. Assuming a standard deviation of 4.530 and equal variances between arms, the target total sample size of 36 (18 per arm) provided 80% power to detect the predetermined effect size. No formal power calculations were performed for safety or exploratory outcomes. Any discussion of these comparisons is considered unpowered and exploratory.
Per-protocol analysis of the Aim 1 outcomes was pursued to account for any confounding resulting from incomplete treatment schedules. Missing outcome data was described at each measurement time point. Use of LMMs allowed for unbalanced data within arms, with all participants with at least one measurement contributing to the regression estimates. Sensitivity analysis included use of repeated measures ANOVA limited to the participants with outcomes recorded at each time point. All analysis was performed in R version 4.2 with significance determined using a two-sided alpha of 0.05.
Results
The flowchart of participants is included in Figure 3. From 2019 to 2023, 73 patients were assessed for eligibility. Thirty-four patients did not meet the inclusion/exclusion (I/E) criteria; therefore, 39 patients signed the consent form. Of those, one was withdrawn by the study principal investigator (PI) prior to randomization, as it was discovered that they did not meet one of the inclusion criteria, and one patient chose to withdraw prior to the start of the acupuncture treatment but after randomization due to medical issues. Thus, 37 participants started acupuncture treatment. Of those, one participant was uncomfortable during the first treatment session and chose to withdraw, one participant was unable to commit to the treatment schedule of the high-dose arm, and two participants missed an acupuncture appointment and were unable to be reached to reschedule, so they were withdrawn. Four participants completed acupuncture treatment but were eventually lost to follow-up. In total, 29 participants completed the full study.
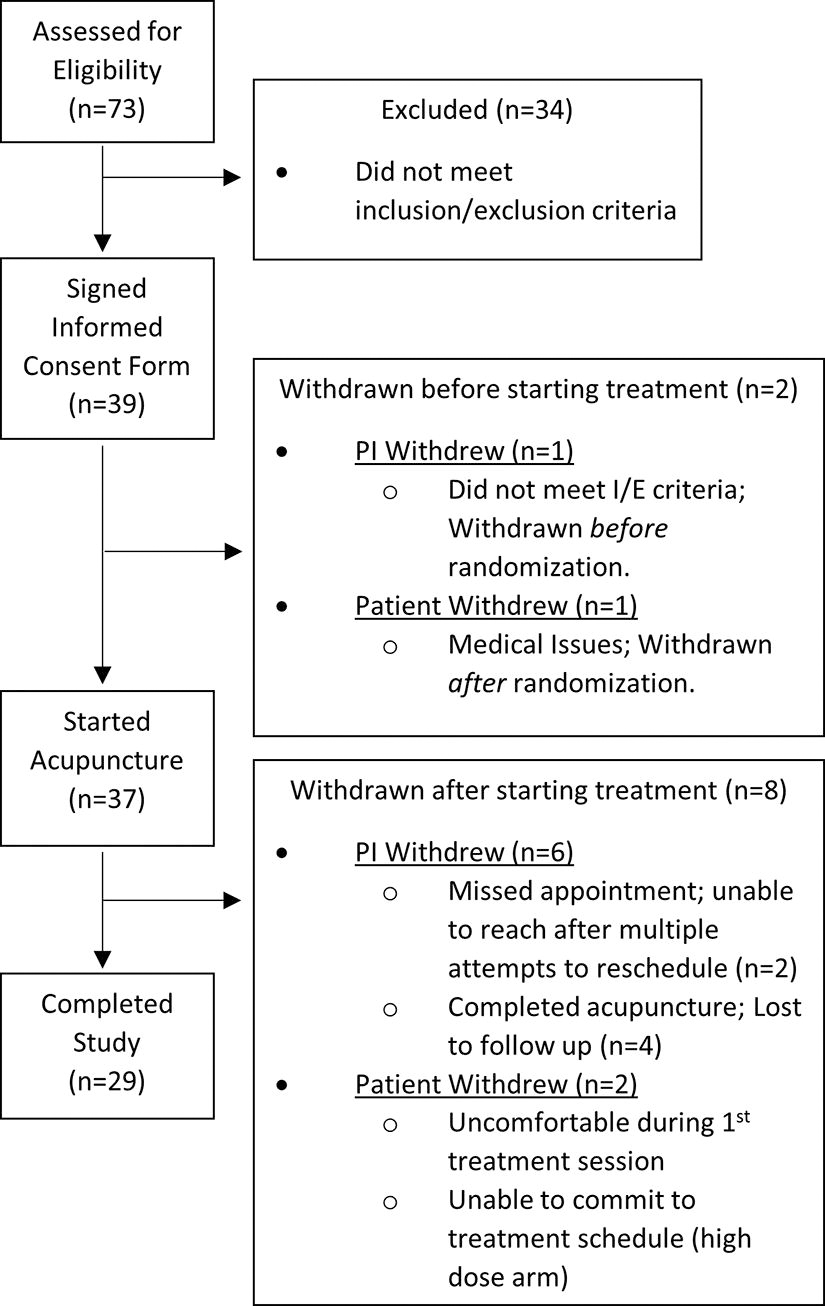
Consort diagram of study participants.
Participant characteristics were described and compared between the two arms (Table 1). Participants were primarily 45–64 years old (55%), female (76%), and white (76%), with a median time between mTBI diagnosis and enrollment of 7.7 months (IQR: 5 to 12).
Two arms compared using Wilcoxon rank test (time to mTBI diagnosis) or Fisher’s exact tests (all other variables).
mTBI, mild traumatic brain injury; IQR, interquartile range.
All summary stats n (%) or median (IQR).
Summaries of the headache diary outcomes at each of the three time points along with LMM regression results evaluating change in outcome over time are presented in Table 2. Before acupuncture treatment, both arms reported an average of 22 headache days out of 28 (Fig. 4). After acupuncture treatment, the low-dose and high-dose arms separately demonstrated a reduction at 4 weeks post-treatment (15, 18 headache days, respectively) and at 12 weeks post-treatment (17, 17 headache days, respectively) (Fig. 4). Although there was no significant difference in number of (p = 0.99) or change in headache days between arms (p = 0.37, 0.70), there was a significant decrease in headache days for all study participants at 4 weeks post-treatment (β: 7.4 decrease, 95% confidence interval [CI]: 3–11, p < 0.01) and at 12 weeks post-treatment (β: 5.1 decrease, 95% CI: 1–9, p = 0.02).
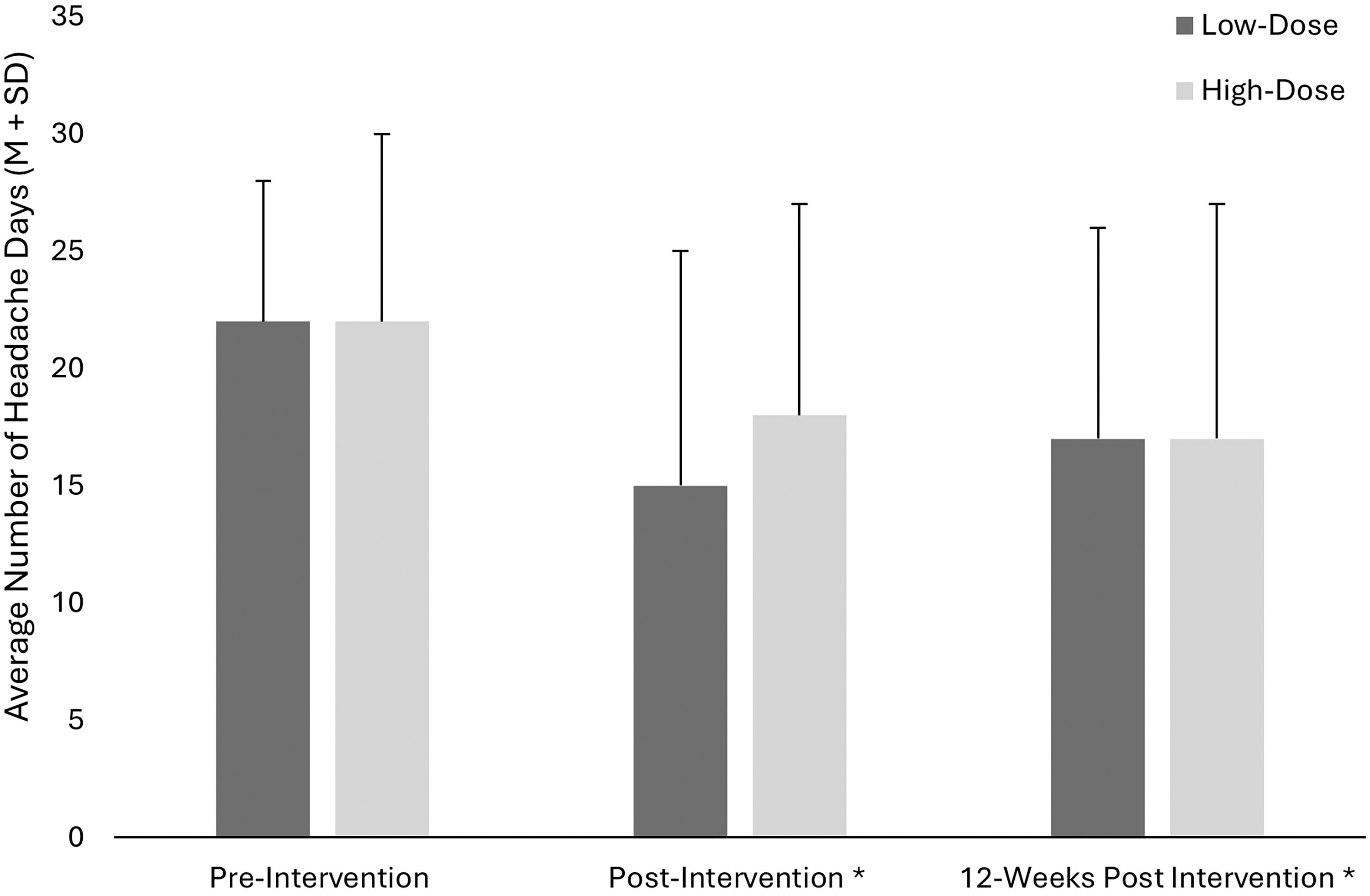
Summary of average number of headache days collected via self-report headache diaries and reported by arm.
Summary and Analysis of Primary Outcomes Collected via Headache Diaries—Number of Headache Days, Rating of Headache Pain Intensity, and Proportion of Headache Days Requiring Acute Medication Use
Regression coefficient estimates extracted from linear mixed models with outcome regressed against measurement time (reference, pretreatment), intervention arm (reference, low dose), the interaction between the two (estimates of differential change between arms), and a random intercept to account for repeated measures within the same participant.
Two arms compared using two-sample t-tests with equal variances.
SD, standard deviation.
Similarly, there were no differences in headache intensity between arms, although a significant decrease in intensity at 4 weeks post-treatment and 12 weeks post-treatment (β: 0.6 decrease, 95% CI: 0.1–1.1, p = 0.02, β: 0.8 decrease, 95% CI: 0.3–1.3, p < 0.01, respectively) was found for all study participants. Acute medication use was constant for both arms across the study time period; however, the magnitude of change between pre-treatment and 12 weeks post-treatment was found to be significantly different for the high-dose participants (p = 0.01). Per-protocol analysis limited to the participants who completed all planned sessions (n low = 16, n high = 17) and repeated measures ANOVA performed with the participants who completed headache dairies at all three time points (n low = 15, n high = 15) aligned with the ITT LMM findings (Supplementary Table S1).
Regarding safety, it is important to note that there were no SAEs reported in this study. Table 3 presents the prevalence of AEs, stratified by study arm, severity, and relatedness to treatment. Of the 95 AEs reported, 35 (37%) occurred in the low-dose arm and 60 (63%) in the high-dose arm. Thirty-one of the 38 participants reported AEs, with 14 participants in the low-dose arm and 17 in the high-dose arm. Further details regarding the types of AEs reported are shown in Figure 5. Only one SAE, definitely or probably related to treatment was recorded, which was a report of pain for a participant in the high-dose arm. Site reaction was the most common type of AE reported in the high-dose arm, representing 16 (64%) of the 25 AEs definitely or probably related to acupuncture treatment. For the low-dose participants, pain and site reaction were the two most common types of AEs reported definitely or probably related to treatment. There was no significant difference (p = 0.57) in treatment adherence between the low-dose and high-dose arms, with an average adherence of 95% (SD 19%) and 91% (SD 0.27%), respectively.
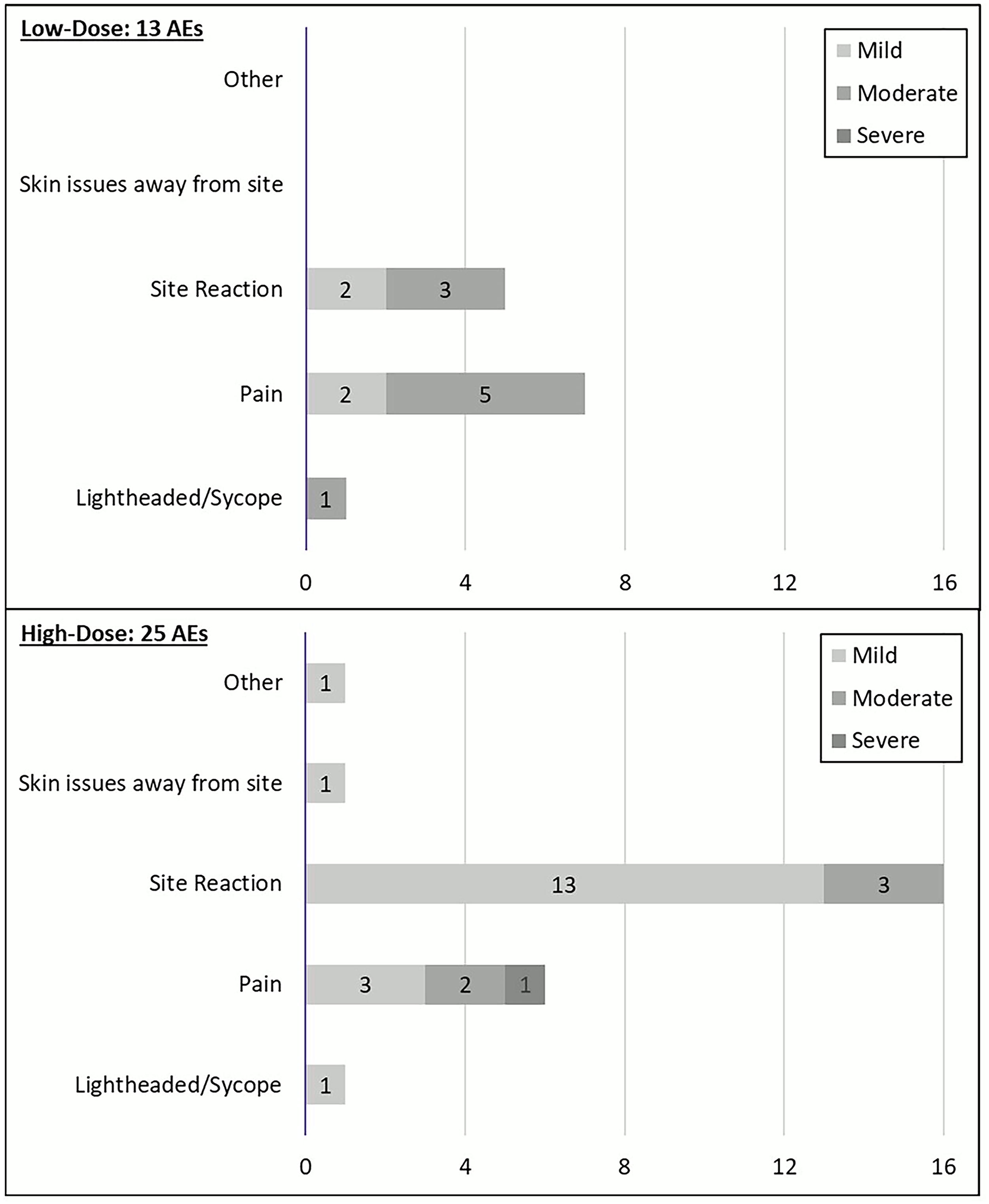
Type and severity of adverse events definitely or probably related to treatment reported by arm. Notes: AEs, adverse events.
Summary of Safety Outcomes for All Participants and Within Treatment Arms
AEs, adverse events.
There were no documented serious AEs, severity, and treatment association determined by study investigators and clinicians.
Sleep quality and measures of QOL were compared between arms in Table 4. Analogous to our findings in Aim 1, there was no consistent difference between treatment arms for these outcomes. Sleep quality did not show significant differences associated with acupuncture treatment. In general, participants reported a significant decrease from pre-treatment in pain interference at 4 weeks post-treatment (p = 0.001) and 12 weeks post-treatment (p = 0.004). Acute improvements in communication, executive function, and self-esteem were reported at 4 weeks post-treatment (Table 4).
Summary and Analysis of Exploratory Outcomes—Sleep Quality and QOL
All summary statistics mean ± standard deviation. Regression coefficient estimates extracted from linear mixed models with outcome regressed against measurement time (reference, pretreatment), intervention arm (reference, low dose), the interaction between the two (estimates of differential change between arms), and a random intercept to account for repeated measures within the same participant. No differences by treatment arm identified. See superscript for significant changes (p < 0.05) at each post-treatment measurement time point.
Significant change from pre- to 4 weeks post-treatment regardless of treatment.
Significant change from pre- to 12 weeks post-treatment regardless of treatment.
Tx, treatment; PSQI, Pittsburg sleep quality index; QOL, quality of life.
Discussion
To our knowledge, this is the first study to examine the effect of a low versus high dose of acupuncture treatment for CPTH in individuals with mTBI. Our results showed that while there were no differences between arms, participants in both arms had a significant reduction in the number of headache days and headache pain intensity from pre-treatment to post-treatment and to long-term follow-up. This indicates that participants had headache improvements after only five acupuncture treatments and that the improvements were sustained 3 months after treatment. Therefore, individuals with mTBI and CPTH may only need to undergo five treatments using a standardized protocol to receive some headache relief, which would be a lower cost and less time commitment for patients.
All types of headache pain involve the trigeminal system. 42 Injuries to the brain and cerebrovasculature can cause maladaptive neuroplasticity within the trigeminal system leading to post-traumatic headaches. 43 Numerous acupuncture points on the face and scalp overlap with branches of the trigeminal nerve and exert their influence on the trigeminal system through the antidromic pathway, trigeminal parasympathetic pathway, and central pathway through the rostral ventral lateral medulla. 44 Acupuncture has been shown to modulate activity in the trigeminal cervical complex and the rostral ventral medulla in migraine patients, while simultaneously improving functionality of descending pain inhibitory pathways. 45 The insular cortex is also a key region involved in central processing of ascending pain signals from the trigeminal system. 43 Brain imaging research of stimulation at acupoint PC6 demonstrated strong functional connectivity between the cerebellar nodulus and insular cortex, 46 while animal research has also shown modulatory effects on the insula with the use of electroacupuncture on points including St 36 and St 37. 47 Acupuncture exhibits numerous effects on key subcortical and cortical structures involved in the processing of pain. 48
Unfortunately, there are limited acupuncture studies for comparison in mTBI and CPTH. Although our overall results were similar, there were several methodological differences between the main previous RCT 24 and our study. The study by Jonas et al. included three arms: usual care, traditional acupuncture, and auricular acupuncture. 24 For the traditional acupuncture group, they utilized a semi-standardized point protocol based on the participants’ headache presentation, with a limited number of additional points to be added for each session, 24 whereas this study utilized a standardized point protocol that included traditional acupuncture at 14 points and electroacupuncture at 4 points. In addition, participants in the traditional acupuncture group of the previous study underwent ten 60-min acupuncture treatments over 6 weeks, 24 whereas participants in this study underwent either five or ten 30-min treatments over 5 weeks. Similar to this study, they found that both acupuncture groups had improvements in their primary outcome, headache-related QOL, and in global pain severity (via the Numerical Rating Scale), 24 while we found improvements in number of headache days and headache pain intensity in both arms (low-dose and high-dose).
Utilization of self-report headache diaries with number of headache days as a primary outcome is typical in previous studies examining the effect of acupuncture on tension headache and migraine. 13 –15 It has also been suggested that headache diaries to monitor ongoing symptoms may be less prone to bias than questionnaires that retrospectively assess symptoms 15 and are the best instrument to determine the effectiveness of therapies for CPTH. 8 Thus, although Jonas et al. recorded daily headache frequency, severity, and prescription medicine use via a daily headache diary and medication log as this study did, they selected the Headache Impact Test as a primary outcome, which is a 6-item self-report questionnaire that assesses a person’s perception of headache burden during the previous month. While we found no differences in acute medication use between or within groups, they were unable to analyze their medication data, given that only 25% of participants provided consistent data. 24 Regarding safety and adherence, Jonas et al. reported fewer AE events (11 total) compared to the 35 AEs reported in the low-dose arm and 60 in the high-dose arm of the study. The higher reporting in this study is likely due to our participants reporting any AE even if it was considered unrelated to treatment (e.g., flu, COVID-19). Our participants also reported headache pain as an AE if it was on or close to the day of treatment. Jonas et al. also recorded sleep quality using the PSQI and QOL utilizing the Medical Outcome Study QOL Short Form 36 (MOS SF-36) and found no statistically significant differences, 24 similar to the PSQI and the majority of TBI-QOL results in this study.
Although the evidence for acupuncture for CPTH and mTBI is limited, there have been numerous studies examining acupuncture for headache and migraine in a non-mTBI population. A systematic review of 12 studies examining the effect of acupuncture on frequent episodic or chronic tension-type headaches found that the proportion of participants who experienced at least a 50% reduction in headache frequency was higher in the acupuncture groups when compared with control or sham groups. 13 In all studies, participants received a minimum of six acupuncture sessions at least once per week. 13 Regarding medication use, there was only 1 study that reported benefit compared to a control; however, compared to sham treatment, the results of a pooled analysis of three trials showed a small, significant effect. 13 In another recent systematic review and meta-analysis for tension-type headaches, acupuncture reduced headache frequency more than the sham group and was superior to no treatment. 49 Regarding the effect of acupuncture on migraine, a systematic review of 22 studies, Linde et al. found that acupuncture reduced headache frequency and improved response compared to routine care and that medication use strongly varied across studies. 15 Doses were variable across all studies, ranging from 6 to 20 treatment sessions total, generally provided once or twice per week. 15 However, their pooled analyses of acupuncture compared to sham treatment did not show statistical significance for any of the headache or medication outcomes. 15 Acupuncture was also shown to have improvements in response, migraine frequency and intensity, but no differences in medication use when compared to groups receiving prophylactic drug treatment. 15 In a recent overview of systematic reviews, the authors found that acupuncture for migraine treatment was more effective than a control group. 50 Thus, our overall findings of improvements in headache frequency and intensity for CPTH align with previous reports of acupuncture effectiveness for tension headache and migraine in a non-mTBI population, with slight variations related to acute medication use.
While the safety and efficacy of acupuncture for CPTH after mTBI has not been established 25 due to the scarcity of evidence, both Jonas et al. 24 and this study demonstrated that acupuncture was safe and well tolerated. There were no SAEs reported in this study and most of the AEs reported were mild site reactions (e.g., pain, bruising, or discomfort at a needle site) and mild to moderate pain (e.g., headache pain around a treatment session or mild pain at a needle site). It was often unclear whether the headache pain was related to treatment, but these were still recorded as AE reports from participants. Although acupuncture has also been used for rehabilitation treatment of TBI, a Cochrane review concluded that the due to low methodological quality, they were unable to make a definitive decision on the safety and efficacy of acupuncture for treatment of TBI. 28 Of the four studies included, only one reported the dose information, which was once daily for 10 days for the first treatment course, followed by once daily for 15 days for the second course. 28 Despite the sparse evidence for CPTH and mTBI, there have been numerous safety reports of acupuncture. In a recent overview of systematic reviews, acupuncture was shown to be a safe treatment for migraine. 51 This was based on evidence of previously reported AEs in systematic reviews and because acupuncture has been reported to have fewer AEs than medication in numerous studies. 51 Acupuncture was also reported to be safe in a recent systematic review and meta-analysis of AEs related to acupuncture. 52 Of the 21 studies included, SAEs were rarely reported, and the most commonly reported AEs were very mild. 52
Acupuncture has previously been shown to improve both primary sleep disturbances after >3 weeks of treatment, 53 as well as secondary sleep disturbances 54 ; however, the results for CPTH and TBI are limited. As previously mentioned, both Jonas et al. 24 and this study found that acupuncture did not improve sleep quality as assessed by the PSQI. Two studies examined acupuncture for sleep in a TBI population (chronic TBI and mTBI) with self-reported sleep disturbances and both found that acupuncture improved sleep quality (assessed via the Insomnia Severity Index and PSQI). 55 Regarding QOL, Jonas et al. did not find significant differences in QOL as measured by the MOS SF-36. However, this study found that of all the TBI-QOL measures assessed, there were no differences between arms, but there were improvements in both groups from pretreatment to 4 weeks post-treatment and to 12 weeks post-treatment for pain interference and self-esteem. There were also significant improvements in cognition, communication, executive function, anxiety, and headache pain; however, the QOL results should be interpreted with caution as these analyses were considered exploratory, and therefore no adjustments were made for multiple outcomes. In a systematic review of four studies examining acupuncture for TBI, none of the studies assessed QOL, which the authors identified as an important outcome. 28
Limitations
There are several limitations of this study. First, this study did not include a control or sham group, and therefore the study was not designed to conclude a significant treatment effect of acupuncture for CPTH. Consequently, our conclusions are limited to determining whether our participants experienced a significant change in headache outcomes after treatment, as compared with before treatment. Due to the level of existing evidence for safety and headache improvements with acupuncture in a non-mTBI population, the focus of this study was not to only show that acupuncture was safe and improved headache symptoms in individuals with CPTH but to also better understand the number of treatments needed for headache relief. In addition, inclusion of control group (e.g., no treatment or usual care group) would likely lead to an increased number of dropouts. In this study, of the 38 individuals who were randomized, 29 completed the full study, which overall was a good completion rate. Alternatively to a control group, the inclusion of a sham treatment group has been largely debated in the literature, as the use of placebo needles (or needles inserted into nontraditional points) could still activate unmyelinated afferent nerves that could influence pain perception. 56 A second limitation to this study was the lack of blinding. Because it would be clear to both participants and to the acupuncturists how many treatments each participant was randomized to receive, blinding in this study was not feasible. Nevertheless, it has been noted that the design of acupuncture trials remains a challenge, especially in regards to the selection of a control group and blinding. 15 Finally, participants were not randomized by headache presentation type. Because acupuncture is a precision medicine modality, in typical clinical practice, acupuncturists would learn more about the headache symptoms and presentation to determine the most effective treatment. While headache type information was reported via self-report headache diaries, our participants were not treated based on their headache presentation. Thus, the standardized treatment protocol used may not reflect the typical care they would receive in clinical practice.
Conclusions
The primary goal of this study was to determine the effect of a low versus high dose of acupuncture treatment on CPTH after mTBI. We found that although there were no differences between treatment doses, acupuncture significantly reduced the number of headache days and headache pain intensity in individuals with CPTH. There were no significant changes in acute medication use or sleep quality, and although there were some improvements identified for QOL, these results should be interpreted with caution. Overall, acupuncture was shown to be safe and well-tolerated in people with CPTH after mTBI. Five acupuncture treatments using a standardized protocol may be enough to see some headache relief in this population. Future studies could compare this standardized acupuncture protocol to less intensive methods (e.g., auricular acupuncture) or to standard of care.
Transparency, Rigor, and Reproducibility Summary
The study design and analysis plan were preregistered on http://clinicaltrials.gov (NCT04369911). A sample size of 18 subjects per arm was planned based on an expected effect size of 4.5 for the primary outcome measure, calculated to yield 80% power to detect a difference in mean number of headache days over 4 weeks from a parallel-group design using a two-sided, two-sample t-test with a p value of <0.05. All participants were assigned to arms using a random number generator, yielding arms that did not differ in baseline characteristics. Seventy-three participants were assessed for eligibility, with 34 participants who did not meet inclusion criteria. Thirty-nine participants signed the informed consent, 37 participants started acupuncture treatment, and 29 participants completed the study. Blinding of participants and investigators was not fully possible due to the nature of the therapeutic intervention. All materials required to perform the intervention are widely available from Pantheon Research (electrostimulator) and Lhasa OMS (acupuncture needles), among many other companies supplying the equipment/materials. The key inclusion/exclusion criteria were determined based on prior studies examining acupuncture for headache/migraine, with emphasis on TBI symptoms that may interfere with study participation. The primary outcome was number of headache days over a 4-week period via self-reported headache diaries. Number of headache days is an established standard outcome measure in the field. Statistical tests used were based on the assumptions of the parametric and nonparametric tests used for analysis. Missing data was described for each outcome/time point and excluded from repeated measures ANOVAs. No adjustment for multiple comparisons was necessary. Statistical analysis was performed by Ella A. Chrenka who has a Master of Science degree in Biostatistics and 5 years of experience analyzing neuroscience research data. No replication or external validation studies have been performed or are planned/ongoing to our knowledge. Data, analytic code, and materials (e.g., intervention protocol) used to conduct the analyses presented in this study are not available in a public repository. They may be available by emailing the corresponding author. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Footnotes
Acknowledgments
We would like to acknowledge Gwendolyn M. Kosevich, NP-F, and her team for referring interested patients to the study, Steven D. Jackson, MD, MBA, for assisting with the review of study adverse events, and Clarissa M. Howe, BA, for assisting with study calls/visits and other study-related tasks. We would also like to acknowledge HealthPartners’ Departments of Rehabilitation and Physical Medicine and Rehabilitation for their assistance and support with this study, as well as all the study acupuncturists. We would also like to thank the participants for their contributions to this study.
Authors’ Contributions
A.A.H.: Conceptualization (lead), funding acquisition (lead), investigation (equal), methodology (lead), project administration (lead), resources (lead), supervision (lead), validation (lead), visualization (supporting), writing—original draft (lead), and writing—reviewing and editing (equal). E.A.C.: Data curation (lead), formal analysis (lead), visualization (lead), writing—original draft (supporting), and writing—review and editing (equal). S.G.B.: Conceptualization (supporting), investigation (equal), methodology (supporting), and writing—review and editing (equal). E.K.T.: Conceptualization (supporting), investigation (equal), methodology (supporting), and writing—review & editing (equal). A.A.W.: Conceptualization (supporting), investigation (equal), methodology (supporting), writing—review and editing (equal). K.W.C.: Conceptualization (supporting), funding acquisition (supporting), investigation (equal), methodology (supporting), writing—review and editing (equal). M.T.F.: Conceptualization (supporting), funding acquisition (supporting), methodology (supporting), project administration (supporting), resources (supporting), supervision (supporting), writing—review & editing (equal). S.J.S.: Investigation (equal) and writing—review and editing (equal). A.L.S.: Software (lead) and writing—review and editing (equal). L.R.H.: Conceptualization (supporting), funding acquisition (supporting), methodology (supporting), project administration (supporting), resources (supporting), supervision (supporting), validation (supporting), and writing—review and editing (equal).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, AH, upon reasonable request.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded by the Minnesota Office of Higher Education’s Spinal Cord Injury and Traumatic Brain Injury Research Grant Program.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.