
Abstract
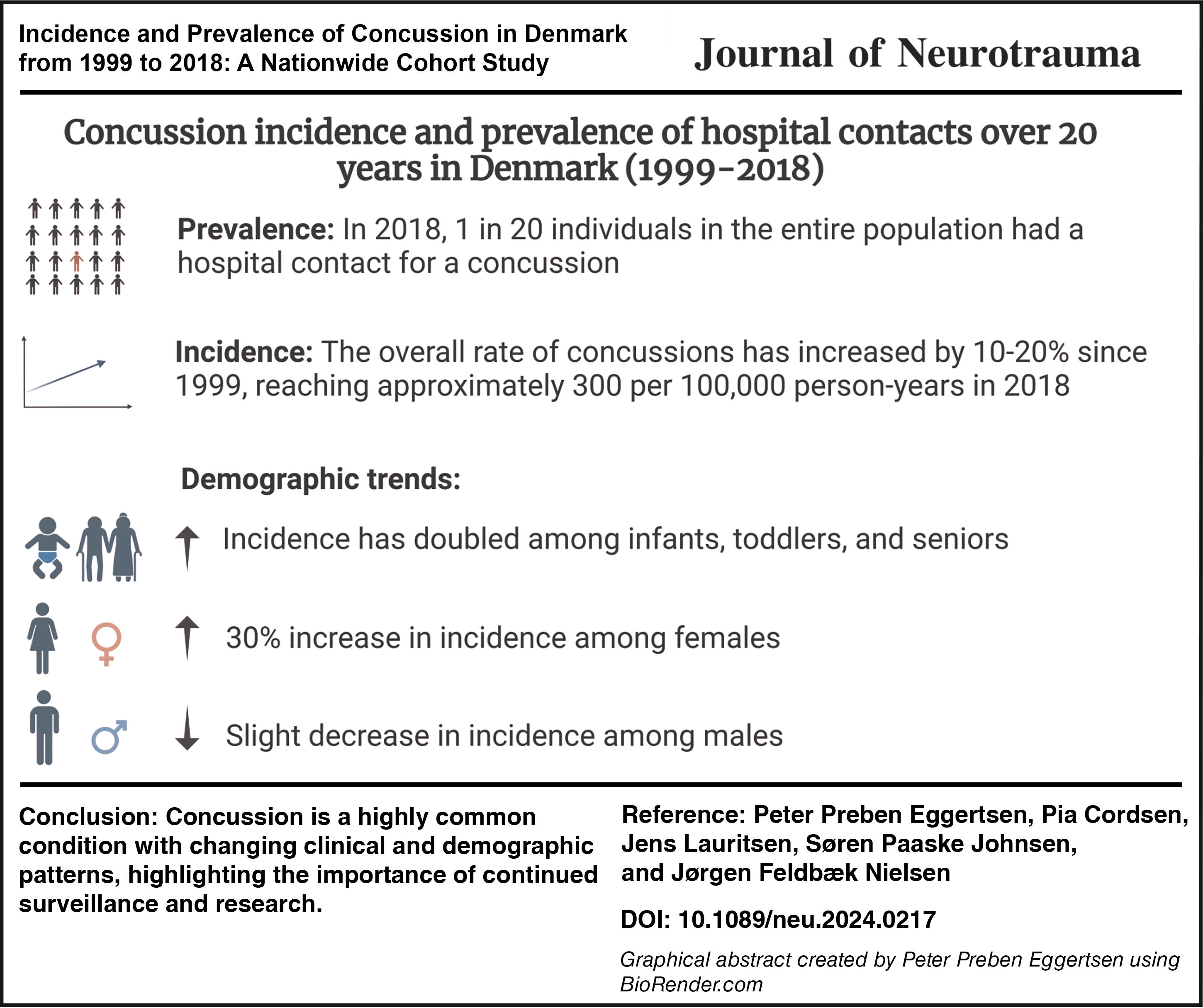
Concussion is a common diagnosis in emergency rooms, yet contemporary incidence and prevalence estimates are sparse and rely on self-reported data. A nationwide cohort study was conducted to provide up-to-date information, covering the entire Danish population from 1999 to 2018. Hospital contacts with a concussion diagnosis, including emergency room visits, hospital admissions, and outpatient contacts, were retrieved from the Danish National Patient Registry (DNPR), and incidence rates were age-standardized and stratified. The 20-year prevalence was defined as the percentage of Danes alive in 2018 who had experienced a concussion since 1999. The diagnostic codes used were the ICD-10 code S06.0 and a local Danish code for ‘observation for concussion’ (DZ033D). Additional data on activities related to concussion injuries were obtained from the Accident Analysis Group at Odense University Hospital through DNPR. Findings from the study showed that during the period 1999–2018, the total age-standardized concussion incidence rate increased by 10% to 308 per 100,000 person-years (95% confidence interval [CI]: 304–313). Notable time trends included (1) a reduced sex difference from 40% to 6% (95% CI: 3%−9%), (2) a doubled incidence rate in children aged 0–1 and in seniors aged over 80, (3) an increased utilization of head imaging across all age groups, except children, (4) a decline in the proportion of traffic-related concussions, and (5) a prevalence of concussion of 4.9% (95% CI: 4.89%–4.93%) in 2018. The increasing incidence of concussions among the elderly is concerning in light of an aging population and warrants further investigation, as evidence-based preventive interventions for falls exist. In addition, the increased utilization of head imaging across all age groups except children calls for attention toward avoidance of unnecessary radiation exposure. Despite a drop in traffic-related cases, concussions remain highly prevalent. In conclusion, these findings indicate that concussions are an important public health concern, necessitating ongoing surveillance, research, and targeted resource allocation to address concussion management and prevention effectively.
Introduction
Concussion is one of the most common diagnoses in emergency rooms, 1 with millions of cases worldwide annually. 2 It is often referred to as a mild traumatic brain injury (mTBI), although experts continue to debate whether the two terms describe the same condition. 3 The debate primarily focuses on whether a concussion should be viewed solely as a minor injury without visible lesions on imaging or if it can also encompass more severe injuries, akin to an mTBI, which might involve structural damage. 4 This article does not distinguish between ‘concussion’ and ‘mTBI’, aligning with a recent comprehensive Danish knowledge report in the field 5 and will use ‘concussion’ throughout. Despite being defined as a mild head trauma, approximately 30% of concussion cases develop severe persistent post-concussion symptoms that may last for months to years. 6 Persistent symptoms attributed to concussion may entail frequent visits to general practitioners, 7 unemployment, 8 and may also be linked to an increased risk of neurological and psychiatric diseases such as dementia and anxiety/depression. 9
Despite the far-reaching consequences of concussion, incidence rate estimates are notably conflicting. For example, reports on the annual number of cases in Denmark between 1994 and 1996 have varied widely, with figures as low as 10,000 10 and as high as 25,000. 11 The conflicting nature of existing evidence is mirrored across Europe with incidence rates ranging from 80–600 per 100,000 person-years. 12 Potential reasons for the conflicting evidence include methodological issues, such as the lack of age standardization, 13 insufficient transparency in reporting age-specific estimates, and failure to distinguish between first-time and recurrent concussions. 14 Furthermore, the interpretation of existing incidence and prevalence estimates is clouded by multiple factors, including the reliance on data from studies conducted more than two decades ago and demographic shifts toward an increasing proportion of elderly individuals in most populations. 15 Elderly people may live a more active lifestyle today and, thus, be more prone to fall accidents, which may result in an increasing incidence. 16 In contrast, safer vehicles 17 and the more frequent use of protective equipment such as bicycle helmets 18 may result in a decline in the incidence. Finally, only a few studies have encompassed all age groups, resulting in an incomplete overview of the field. The need is growing for an accurate up-to-date estimate of the incidence of concussion. This knowledge is crucial to facilitate prevention and inform health care planning. Therefore, we aimed to study the incidence and prevalence of concussion leading to hospital contacts in Denmark.
Methods
Population, setting, and data sources
This was a registry-based historical cohort study of persons with permanent residence in Denmark between January 1st, 1999, and December 31st, 2018. Concussion cases were extracted from the Danish National Patient Registry (DNPR), which contains detailed information on all contacts with Danish hospitals, including emergency room contacts, outpatient visits, and hospital admissions. Cases were identified as having received a diagnosis code for concussion at a hospital. These included the International Classification of Diseases (ICD-10) code for concussion (S06.0), as well as a Danish code for ‘observation for concussion’ (DZ033D). The DZ033D code is an expansion of the ICD-10’s Z03-codes, which are used when a diagnosis is suspected, but not confirmed. 19 Diagnoses given as a primary diagnosis (type A), secondary diagnosis (type B), and complementary diagnosis were all included. A first-time concussion case was defined as a person’s first concussion (outpatient, emergency room, or hospital admission) between 1999 and 2018, with no recorded concussion diagnosis codes since 1994. In addition, in a supplementary analysis, recurrent concussion incidents were included. For a concussion incident to be considered recurrent, it had to occur more than 90 days after a previous concussion discharge in alignment with previous registry-based studies. 20,21 Although this threshold might risk underestimating the incidence, prior research indicates that general practitioner visits increase within the first three months following a concussion, 7 supporting the use of 90 days as an appropriate threshold. In addition, recurrent outpatient contacts were excluded to further increase the likelihood that the incident represented a truly new concussion event.
Data on activities that led to the concussion (e.g., sports, traffic accidents) were extracted from the DNPR from Odense University Hospital during the entire 20-year study period. Data on protective equipment and violence were available from 2014–2018. Data from other Danish hospitals were not utilized due to extensive changes in coding practice over time. In contrast, Odense University Hospital, supported by its Accident Analysis Group, has maintained rigorous monitoring of accident developments, ensuring accurate data registration since 1980. 22 Odense, the third largest city in Denmark, is located in the Region of Southern Denmark. The catchment area of Odense University Hospital includes approximately 5% of the total Danish population and is considered a representative sample of the overall Danish population. 22 In addition to registering data on accident activities, the registry also contains data on whether the concussion was due to a fall injury. However, due to changes over time in the categorization of fall injuries, data on the proportion of fall-related concussions were not feasible for use and were therefore excluded. All data were obtained through Statistics Denmark.
Data on deaths were extracted from the Danish Register of Causes of Death, which classifies deaths according to ICD-10 criteria. 23
Statistics
The crude incidence rate was calculated as follows:
Given that the population is in a steady state, the incidence rate can be converted into a rate per 100,000 person-years. 24 Yearly population figures were obtained from Statistics Denmark. 25 In most studies, age standardization is lacking, making comparisons of studies difficult. 13 Therefore, the total incidence rates were standardized using direct standardization with the Danish population in 2018 serving as the standard population (Supplementary Table S1).
The 20-year prevalence in 2018 was calculated as follows:
The all-cause 30-day mortality risk was calculated by:
95% confidence intervals (CI) were calculated using standard methodology as described by Kirkwood and Sterne. 26 Stata version 17 for Windows was used for the calculations (StataCorp, College Station, USA), and GraphPad Prism was used for graphs (GraphPad Software, San Diego, USA).
Results
Figure 1 depicts the inclusion process of concussion cases over a 20-year period. Out of 527,345 incidents, 149,867 duplicates within 90 days of the first concussion were removed. Of these duplicates, 95% (≈142,000) occurred within the first week. Of the remaining 377,478 concussion incidents recorded, 327,826 were identified as first-time cases, with no prior concussion history since 1994. The diagnosis codes used for concussion showed similar characteristics (Table 1). The cases had a median admission length of one day, and half of the cases were diagnosed with at least one other condition on the day of the concussion, the most common being superficial head lesions, contusions, and fractures. Only 1.8% had a diagnosis code for intracranial lesions (Table 1).
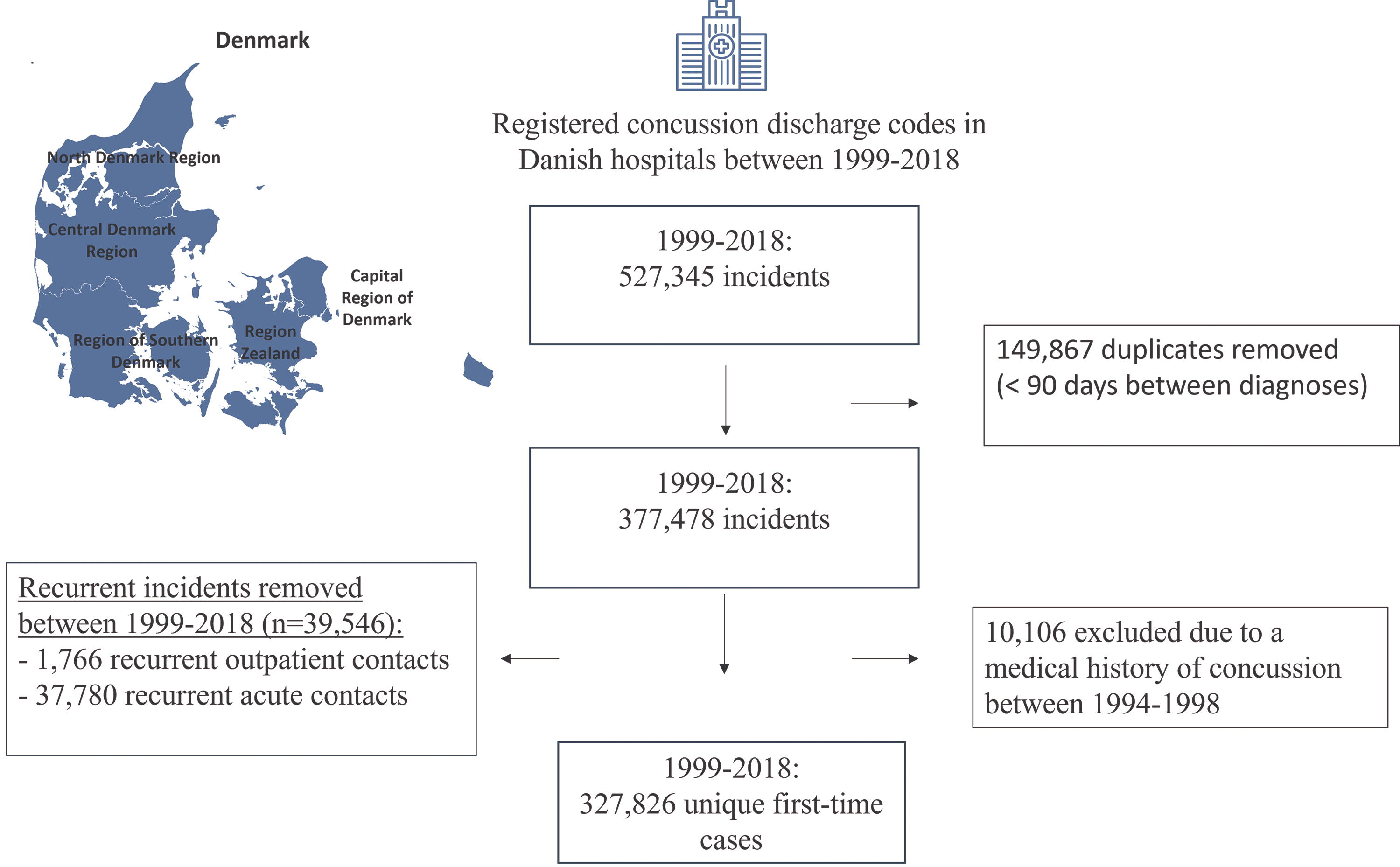
Flowchart outlining the selection of concussion cases recorded in Danish hospitals from 1999 to 2018. First-time cases were defined as the first ICD-10 code (S06.0) or a Danish code for concussion (DZ033D) within 1999–2018, with no prior history with the codes since 1994.
Concussion Diagnoses in Danish Hospitals (1999–2018)
Overview of all concussion cases between 1999 and 2018 diagnosed in Danish hospitals.
ICD-10, International Classification of Diseases, 10th revision.
Incidence rates
Figure 2 illustrates the total age-standardized incidence rates over the 20-year period for first-time cases. From 1999 to 2018, the total concussion incidence rate increased from 280 to 308 per 100,000 person-years, corresponding to a 10% rise (95% CI: 7.6%−12.4%). When including recurrent incidents (allowing each person to have more than one concussion episode), the incidence rate increased from 306 to 363 per 100,000 person-years, representing a 19% increase (Supplementary Table S2 and Supplementary Fig. S1). Sex stratification revealed that the increase was attributed to a 28% rise (95% CI: 24%−32%) in concussion incidence in females from 234 to 299 person-years, whereas the incidence rate in males tended to decrease by −2.5% (95% CI: −5.5% to 0%) from 326 to 318 per 100,000 person-years (Fig. 2). Consequently, the incidence rate ratio shifted from males having a 1.39 (95% CI: 1.35–1.44) higher rate than females in 1999, to only a 1.06 (95% CI: 1.03–1.09) ratio in 2018.

Total first-time concussion incidence rates in Denmark are illustrated along with 95% confidence intervals. The incidence rates are standardized according to the Danish population in 2018 (Supplementary Table S1) to account for demographic change. Raw total numbers and estimates, including recurrent incidents, are provided in Supplementary Table S2 and Supplementary Figure S1.
To further explore the incidence rates, we stratified them by age as shown in Figure 3 and detailed in 5-year bands in Supplementary Table S3. Throughout the entire 20-year period, the concussion incidence was highest in children and young adults (0–29 years) and in the elderly (above 80). The incidence rates in these groups ranged from 300–1400 per 100,000 person-years. In contrast, the rates were consistently lower, ranging 150–300 per 100,000 person-years in the intermediate age groups (30–79 years) (Supplementary Table S3 and Fig. 3). Furthermore, it became evident that the decrease in the incidence rate ratio between males and females observed in Figure 1 was primarily caused by a decreased incidence rate in male adults between 18 and 29 years of age (from approximately 480 to 350 per 100,000 person-years).

Age-stratified incidence rates of first-time concussions between 1999 and 2018. Raw incidence rates in 5-year bands are provided in Supplementary Table S3.
In children aged 2–17, males had consistently a 20–30% higher incidence rate throughout the entire study period. In contrast, female seniors above 80+ tended to have a 5–20% higher incidence than males across the entire study period (Fig. 3).
The incidence rate increased 2.5-fold in infants and toddlers (under 2 years) to approximately 1,400 per 100,000 person-years in 2018, whereas in elderly (80 and above), it nearly doubled to around 800 per 100,000 person-years. A stratified analysis of each of the five Danish regions showed that the observed rise in infants and toddlers was observed in all regions, except the Central Denmark Region (Fig. 4).
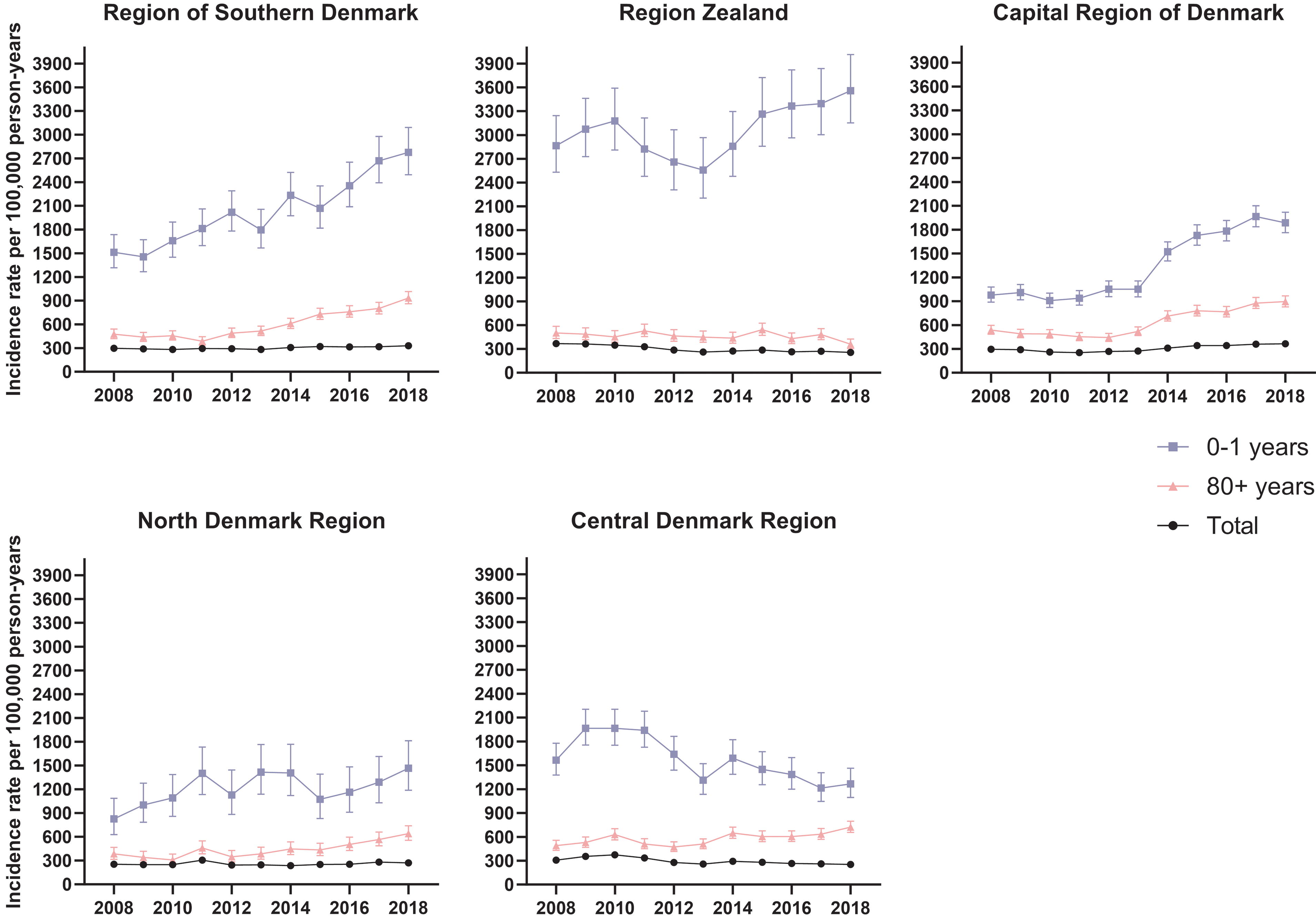
First-time concussion incidence rates of children aged 0–1 year, seniors aged 80 years and above, and the total incidence across the five Danish Regions. Location of each region can be seen in Figure 1. Average inhabitants in each region during the 20 years: Region of Southern Denmark (n = 1.20 million), Region Zealand (n = 0.82 million), Capital Region of Denmark (n = 1.7 million), North Denmark Region (0.58 million), Central Denmark Region (n = 1.27 million).
Concussion activities and imaging
The use of cerebral imaging increased during the study period, starting from 6–18% in 2002 to up to 80% among elderly in 2018 (Fig. 5), with 99% of these scans being computed tomography (CT) scans and 1% magnetic resonance imaging scans. In children, the increase was more modest, rising from 6% to 9%. In contrast, the use of skeletal x-rays, spinal imaging, and other forms of imaging nearly halved across all age groups, except for individuals aged 60 and over, where it remained more stable.
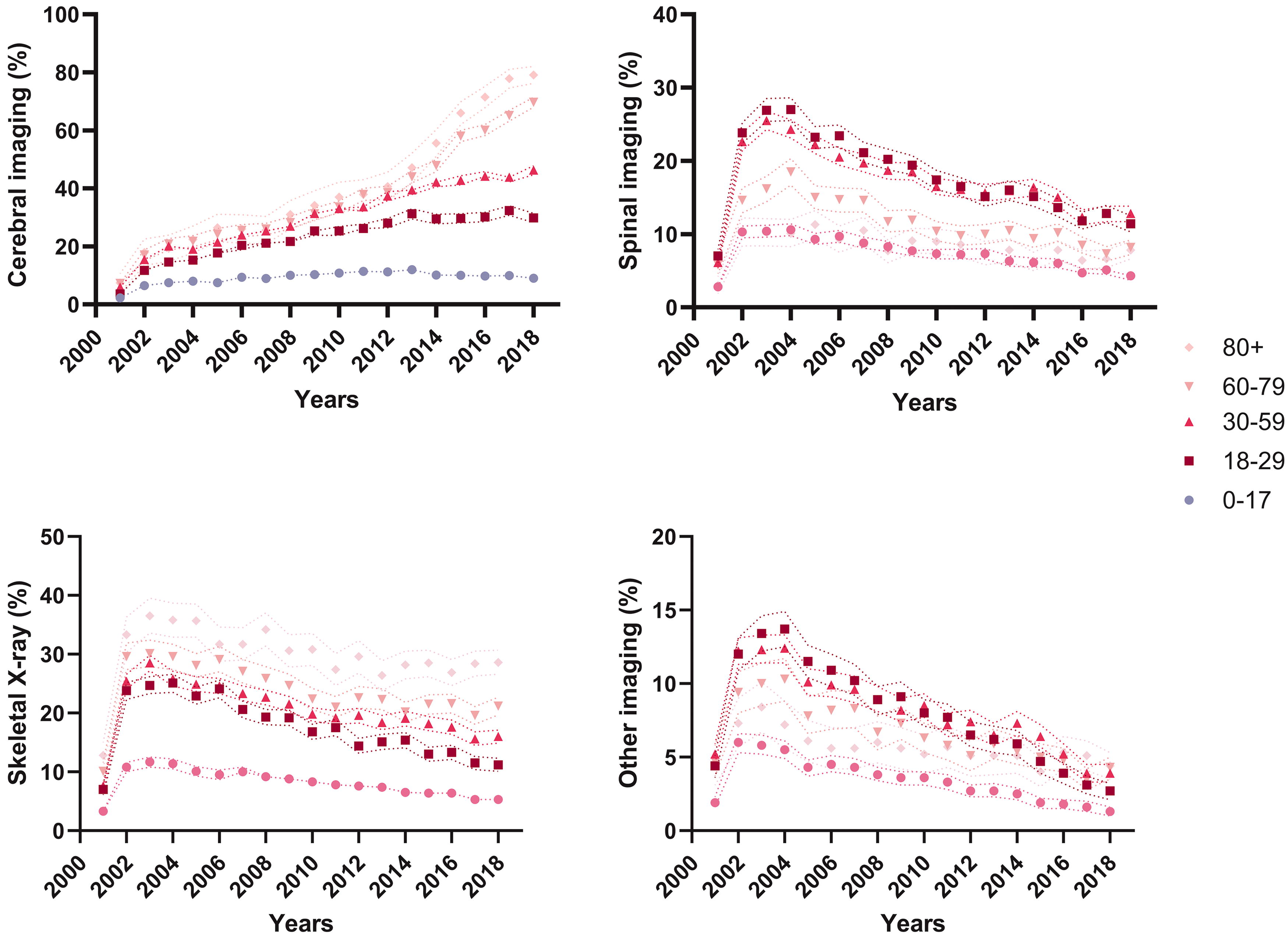
The figure shows the proportion (%) of radiological examinations conducted on first-time concussion cases in Denmark between 1999 and 2018, with 95% confidence intervals represented by dashed lines. Data on imaging were logged in the Danish National Patient Registry from 2001, likely explaining why this year is an outlier.
Information on the activities that led to concussions was retrieved from Odense University Hospital during the entire study period (n = 18,029) and is presented in Figure 6. The proportion of injuries due to sports and playing activities was higher in 0–17-year olds than the other age groups, whereas concussions due to paid work and house activities were more common in adults and seniors, respectively. The proportion of concussions due to transportation activities (traffic accidents) was higher among individuals aged 18–59 years than the other age groups throughout the study period. However, the proportion was reduced by half or more in all age groups over time (Fig. 6), as did the raw number of traffic accidents (Supplementary Fig. S2). Data on modes of transport involved in these traffic accidents are presented in Figure 7. Over the 20-year period (1999–2018), the proportion of concussion-related bike accidents increased from 40% to 60% in males, whereas the proportion of car and motorcycle accidents decreased by 10–20%. In contrast, the proportions in females remained stable across the 20-year period (Fig. 7).

The figure shows the proportion of different activities that led to a first-time concussion, along with 95% confidence intervals, across children, adults, and seniors. The data were from a representative sample of the Danish population from Odense University Hospital encompassing 18,029 cases over a 20-year period. Data stratified by sex and additional details are available in Supplementary Figure S2. Vital activity refers to activities such as eating or bathing.
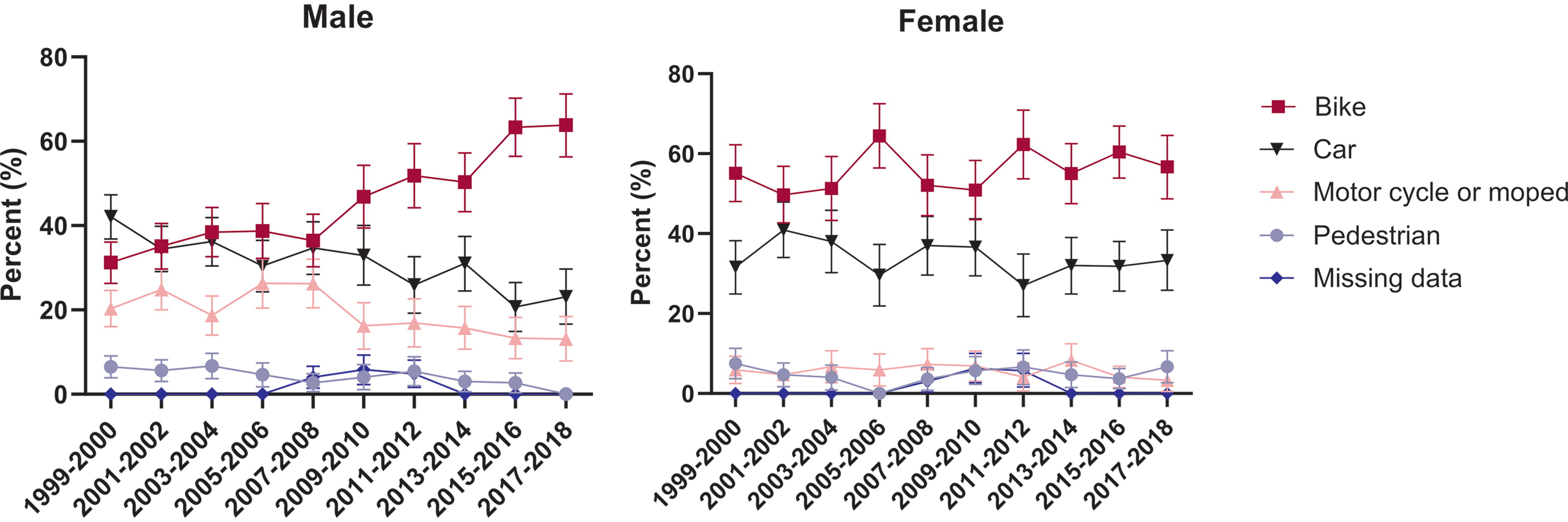
The figure details the distribution of modes of transportations in transportation-related concussions recorded between 1999 and 2018, as identified in the “transportation” category in Figure 6. Out of the 3,970 first-time cases of transportation-related concussions registered in the 20 years at Odense University Hospital, detailed information on the mode of transport was available for 3901 cases, indicating minimal missing data.
Prevalence, mortality, and most recent numbers
Table 2 shows the latest concussion characteristics. In 2018, 15% of the concussion incidents were recurrent incidents, and the prevalence of having experienced at least one concussion was 4.9% in the total Danish population. The 30-day mortality risk in 2018 was ≤0.1% for younger age groups (0–59 years), whereas it was 5.9% in elderly aged 80+, and the total mortality risk remained stable since 1999 (Supplementary Fig. S3). The underlying cause of death in 2018 was most commonly registered as heart diseases (n = 15), cerebrovascular diseases (n = 15), and bronchitis, emphysema, and asthma (n = 11). Most concussion cases were due to accidents (80%) or violence (4.8%) according to the representative sample from Odense University Hospital (Table 2). Violence was more common in males than females (6.9% vs. 2.4%), but concussions due to partner violence were more common in females (34% vs
Detailed Characteristics of Most Recent Concussions Recorded in Denmark
Includes all concussion cases alive and with a residence in Denmark in December 2018, including those whose medical records indicate a concussion between 1994 and 1999.
Exact estimates are not provided to protect anonymity.
Data on accidents were obtained from a representative sample of the Danish Population at Odense University Hospital between 2014 and 2018.
Discussion
This nationwide study set out to explore the incidence and prevalence of hospital visits due to concussions in Denmark over the 20-year period 1999–2018. The overall concussion incidence rate slightly increased over time, but remained around 300 per 100,000 person-years, which closely aligns with the European average. 13,27 Interestingly, while the incidence rate was 40% higher in males than in females in 1999, this sex difference had dropped to 6% in 2018, which is a novel finding. Furthermore, to the best of our knowledge, this study is among the first to report the prevalence of a concussion history without relying on patient self-reports. The prevalence was 5% in the total Danish population in 2018, which is comparable to the prevalence of lifestyle diseases such as type-2 diabetes. 28 Since up to 30% of persons who experience a concussion develop persistent post-concussion symptoms (PPCS), 6 as many as 1.5% of the population (≈ 85,000 Danes) could have experienced or been living with PPCS in 2018. This potentially makes PPCS one of the most common neurological disorders, only surpassed by migraine and mononeuropathies, which affects 120,000 to 150,000 Danes. 29
Narrowing sex differences
Contrary to previous concussion research, which shows a male-to-female ratio ranging from 1.2 to 4.6, 27 the present study reveals a narrowing sex gap. This shift was driven by a decrease in incidence among males aged 18–29 years. Young males are more often involved in car crashes 30 and tend to engage in riskier driving behaviors, including speeding, committing traffic violations, and driving under the influence of drugs and alcohol. 31 A possible explanation of the decreased incidence among young males may be the introduction of safer vehicles over time. 32 This is backed up by the fact that the proportion of car accidents was declining in males (Fig. 7). Furthermore, the proportion of skeletal x-rays and spinal imaging declined over time as well, which further points toward milder traumas (Fig. 5). Another factor contributing to the narrowed difference between sexes was the observed 30% increase in incidence among females. This rise could be linked to a heightened participation in sports in the general population. 33 Numerous studies have shown that females may face a higher risk of sustaining sport-related concussions, although the evidence remains inconclusive. 34 However, the proportion of sport-related concussions only increased marginally in the present study, suggesting that it cannot fully account for the observed trend (Fig. 6 and Supplementary Fig. S2). Interestingly, a recent Finnish study showed a similar pattern of a declining incidence in males and an increasing cincidence in females of traumatic brain injuries, suggesting that our findings may reflect a broader trend. 35 This highlights the need for further research into sex-specific differences in concussions/traumatic brain injuries.
Increasing incidence among infants and seniors
Surprisingly, the incidence rate of children aged 0–1 increased dramatically over time. One explanation could be increased accessibility to the emergency rooms. Notably, between 2011 and 2014, three out of the five Danish regions—the Capital Region of Denmark, Region Zealand, and the Region of Southern Denmark—implemented telephone-based triage systems for their emergency rooms. 36 These systems allowed for direct referrals to the emergency rooms, thereby bypassing primary care. Most notably, the largest region in Denmark, the Capital Region, introduced telephone-based triage in 2014, likely explaining the steep increase in incidence rates for that year. 36 However, the pronounced increase in incidence among children aged 0–1 contrasts with the relatively minor changes in overall regional incidence rates across all age groups (Fig. 4). This discrepancy could be due to the challenges of telephone-based triage for children aged 0–1. Given the inability of children aged 0–1 years to verbally communicate their symptoms, health care professionals might adopt a more cautious approach during phone consultations, preferring in-person evaluations to ensure that more serious conditions are not overlooked. In contrast, a slight decrease in incidence among children aged 0–1 was observed in the Central Denmark Region, possibly due to an initiative in 2012 aimed at increasing patient visits in primary care, thereby potentially reducing hospital admissions. 36 Our findings are in accordance with a recent study that investigated pediatric concussions, which reported highest incidence among infants, as well as an increase over time. 37 Apart from structural changes within the health care system, other explanations may be an increased awareness toward the condition. 38
Increasing concussion incidence in seniors aged 80 + was observed in all Danish Regions except Region Zealand. This pattern has been observed in previous studies as well. 39 –41 Apart from the aforementioned structural changes and increased awareness, it could also represent a genuine increase in incidence. One possible explanation is that the elderly may be more active today than they were in the past, a trend which has been observed in the United States and Australia. 42 In accordance with this, a rise in fall-related traumatic brain injuries has been observed among the elderly. 16 This increase in activity levels could be attributed to significant advancements in medicine. For instance, there have been significant advancements in treating diseases that affect mobility in seniors, such as osteoporosis 43 and rheumatoid arthritis, 44 as well as in surgical procedures for mobility issues, including knee and hip surgeries, in recent years. 45
Increased use of head imaging
Another noteworthy trend observed in the present study was the dramatic increase in the use of head imaging, especially among elderly (from 20% in 2002 to 80% in 2018). This increase is partly explained by the 2013 guidelines from the Scandinavian Neurotrauma Committee, which recommend CT scans for concussed individuals aged ≥65 using antiplatelet medication. 46 In addition, the use of antithrombotic drugs has increased considerably between 1999 and 2018, especially in individuals aged above 80. 47 Nonetheless, these explanations do not fully explain the increase in head imaging across all age groups. The 2013 guideline also introduced the S100B biomarker, which can be used to rule out intracranial bleeding and minimize CT scans. 46 Despite the implementation of S100B in several Danish emergency wards and a decreasing proportion of traffic accidents, CT scan usage has continued to rise. This could reflect a discrepancy between the recommended guidelines and actual clinical practices. This is in accordance with data from single-center studies in Norway and Sweden, reporting that the Scandinavian guidelines were only followed in 40–55% of head injury cases, 48,49 potentially resulting in unnecessary CT scans. Adherence to these guidelines could decrease the use of CT scans. Using S100B, a recent study showed that CT scans could be reduced by a third, 50 and its application in a prehospital setting has also been demonstrated. 51
The increased usage of CT scans has also been observed in other studies. For example, a concussion study showed that the use of CT scans increased despite less severe injuries over time. 52 This may be part of a general trend in the health sector. A report from the Danish Health Authority described that the use of CT scans of the brain almost increased by threefold between 2003 and 2014. 53 This trend has also been noticed globally. 54 –56 Apart from an aging population and the increased use of antithrombotic medicine, the increased availability of CT scans also plays a role. In addition, the physicians’ fear of overlooking a diagnosis may lead to unnecessary CT scans. 57,58
In contrast, head imaging of children kept stable. This may be due to the clinicians’ awareness of the cancer risk: It is known that 1:10,000 children may develop cancer after a CT scan. 59 Furthermore, specific Scandinavian guidelines for pediatric head injuries focus on reducing CT scans by favoring observation over imaging. 60
Mortality
In the present study, the total 30-day mortality risk was low (0.8%), reflecting the inclusion of concussion cases exclusively. The Scandinavian guidelines permit the prompt discharge of mild head injury cases, including concussions, without further observation, 46 and it is likely that more severe head injuries, for example, intracranial lesions, would not receive a diagnosis code of concussion. In contrast, the 30-day mortality risk for the elderly was higher at 5.9%. However, the underlying cause of death was often not directly connected to the concussion, such as heart and lung diseases, meaning that the mortality was likely attributed to comorbidities rather than the concussion itself.
Our findings align with prior Danish studies, showing a mortality risk of around 1%, 61 ranking concussions among the least lethal common emergency room diagnoses, with only ankle sprains and arm fractures presenting with a lower 30-day mortality risk. 1 However, comparing the mortality following concussion/traumatic brain injuries is challenging across international studies. For instance, a study reported a pooled mortality rate of 11.7 per 100,000 people for traumatic brain injuries across 24 European countries, but without specifying the follow-up duration. 12 The omission of specifying follow-up time is critical, as mortality rates will vary substantially according to duration of follow-up, that is, 30 days versus a year. Therefore, we encourage future studies to either report specific mortality risks or at least clearly define the follow-up period for mortality rate calculations.
Strengths and limitations
This study had several strengths. We included all concussion hospital contacts identified by both the ICD-10 code (S06.0) and the local Danish code, DZ033D, which limits concerns about selection bias. In contrast, previous Danish studies have not included the DZ033D diagnosis 20 or emergency room visits, 10,61 thus likely underestimating the incidence of concussion. In addition, the 20-year study period allowed us to evaluate temporal trends, which have often not been feasible in previous studies. Furthermore, we provided age-standardized total incidence estimates and segmented incidence estimates into 5-year bands in all age groups (Supplementary Table S3), thereby facilitating comparisons with future research. In contrast, most previous studies focus either on pediatric concussions or adult concussions alone and often do not provide age-standardized estimates. 13
This study also had limitations. Although we had data from all Danish hospitals, data from the primary sector were lacking, impacting the external validity of our results. In a population-based study in New Zealand, 8% were recruited from family doctors and 28% from other nonhospital sources, 62 indicating that a significant proportion of concussions are not seen at hospitals. As a result, the true concussion incidence rate and prevalence proportion were likely underestimated in this study.
Another limitation of the study is that the data on concussion activities were derived from a 5% representative sample, with 10–20% of the data missing. While all concussions, including those resulting from falls, are included in the present study, we were unable to determine the proportion of fall-related injuries due to inconsistencies in coding practice over time. Therefore, future epidemiological studies should prioritize the collection of comprehensive information on trauma mechanisms recorded by medical personnel to allow for the assessment of temporal trends. Moreover, the absence of diagnosis codes (ICD-8) before 1994 resulted in an underestimation of the prevalence, prohibited us from calculating the lifetime prevalence, and possibly led to the inaccurate classification of some “first-time” cases.
Conversely, the absence of detailed injury data, such as the Glasgow Coma Scale score and loss of consciousness, may lead to an overestimation of concussion cases due to potential misclassification. The absence of explicit diagnostic criteria for concussions in the Scandinavian Neurotrauma Committee’s guidelines 46,60 means that the concussion diagnosis largely depends on each physician’s own understanding of a concussion. In addition, the ongoing lack of a universally accepted concussion definition over the past two decades further complicates the validation of both the ICD-10 code (S06.0) and the local Danish code (DZ033D).
Despite these limitations, our total incidence estimates were closely aligned with the European average 13,27 and were comparable with a recent Norwegian study that applied the World Health Organization diagnosis criteria for concussion. 63
Conclusion
This study provided updated data on the incidence rate and prevalence of concussion leading to hospital contacts in Denmark. A prevalence of at least 5% shows that concussion is a common condition that requires clinical and public health attention. The overall concussion incidence in Denmark closely aligned with the European average, yet it revealed noteworthy time trends. The observed narrowing of the sex difference in concussion incidence, potentially linked to a decrease in traffic accidents, warrants further investigation in future studies. In addition, future studies should critically assess the increased usage of head imaging due to the importance of minimizing the radiation exposure. Finally, the observed increase in the concussion incidence in seniors should be monitored, especially since interventions to reduce fall injuries are available, 64 which could potentially mitigate this trend. With the demographic shifts toward an aging population, 65 proactive measures to prevent concussions are more crucial than ever.
Transparency, rigor, and reproducibility summary
This epidemiological study was not formally registered due to its observational nature, focusing on the incidence and prevalence of concussion without the need for hypothesis testing. This approach is consistent with the typical practices for studies reporting incidence and prevalence. To ensure rigor and transparency, this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. A detailed flowchart, illustrating the study design and inclusion process, is provided in Figure 2, with detailed inclusion criteria in the Methods section.
Nationwide concussion data were acquired after an application to Statistics Denmark, and analyses were conducted on their protected server to ensure the integrity and confidentiality of the data. The primary analysis focused on first-time concussion cases to maintain data independence, a crucial statistical assumption when calculating confidence intervals. Recurrent concussions were included in a supplementary analysis. Raw data can be accessed through the Danish National Patient Registry by applying to either Statistics Denmark or The Danish Health Data Authority. Stata codes for reproducing our findings will be made available upon request for research. By Danish law, deidentified registry-based studies do not require ethical approval.
Footnotes
Acknowledgments
The authors thank Sanne Svendsen, legal advisor, for facilitating the study by arranging a data agreement between the Central Denmark Region and the North Denmark Region. The authors also thank the statisticians Jakob Nebeling Hedegaard and Simon Grøntved for fruitful discussions on the statistical analyses in the present study.
Authors’ Contributions
P.P.E.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization, project administration, and funding acquisition. P.C.: Conceptualization, methodology, writing—review and editing, and supervision. J.L.: Conceptualization, resources, and writing—review and editing. S.P.J.: Conceptualization, methodology, resources, writing—review and editing, and supervision. J.F.N.: Conceptualization, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was funded by
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.