
Abstract
The purpose of this study was to assess the performance of predictive blood biomarkers for responsiveness to targeted treatments for chronic psychological issues years after traumatic brain injury (TBI). Targeted Evaluation Action and Monitoring of TBI was a prospective 6-month interventional trial of participants with chronic TBI sequelae (n = 95). Plasma biomarkers were analyzed pre-intervention: glial fibrillary acidic protein (GFAP), tau, hyperphosphorylated tau Thr231 (p-Tau), von Willebrand factor (vWF), brain lipid-binding protein (BLBP), ubiquitin C-terminal hydrolase-L1 (UCH-L1), vascular endothelial growth factor-a (VEGFa), and claudin-5 (CLDN5). Clinical outcomes included the Post-Traumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5) and Brief Symptom Inventory-18 (BSI-18). Regression models were built for change in PCL5/BSI-18. Biomarkers and covariates were included. Two models were built to identify responders (improved beyond the minimum clinically important difference). The model to predict change in PCL5 (R 2=0.64; p < 0.001) included vWF (p = 0.032), BLBP (p = 0.001), tau (p = 0.002), VEGFa (p = 0.015), female sex (p = 0.06), and military status (p = 0.014). The model to predict change in BSI-18 (R 2=0.42; p = 0.003) included vWF (p = 0.042), VEGFa (p = 0.09), BLBP (p = 0.01), CLDN5 (p < 0.001), female sex (p = 0.012), and military status (p = 0.004) as predictors. The model to differentiate participants who improved for PCL5 (R 2=0.68; p < 0.001; AUC = 0.93) included vWF (p = 0.02), VEGFa (p = 0.008), and BLBP (p = 0.006). The model to differentiate participants who improved for BSI-18 (R 2=0.25; p = 0.04; AUC = 0.75) included UCH-L1 (p = 0.03), GFAP (p = 0.06), and vWF (p = 0.03). Combinations of pre-intervention blood biomarkers were able to differentiate responders from nonresponders in both post-traumatic stress and overall psychological health domains.
Introduction
Traumatic brain injury (TBI) is a major public health concern predominantly due to its association with many debilitating sequelae, such as headache/migraine, cognitive complaints, vestibular dysfunction, sleep issues, and/or psychological concerns. A growing body of evidence suggests that early and active treatments directed by the individual’s specific clinical phenotype can reduce symptom burden and improve outcomes following TBI. 1,2 As more validated treatments for TBI continue to emerge, there will be an increasing need to appropriately triage patients into the most efficacious treatment pathway. Objective assessments that can aid the clinician in determining if a targeted treatment will be effective could reduce time to recovery for patients with TBI while optimizing resource allocation for health care systems. Predictive blood biomarkers are established in other medical specialties, such as oncology. 3 Few studies have examined the efficacy of predictive blood biomarkers for targeting treatments to chronic TBI management, 4,5 and none have assessed their efficacy in psychological sequelae of TBI. The purpose of this study was to assess the performance of predictive blood biomarkers for responsiveness to targeted treatments for chronic psychological issues years after TBI.
Methods and Materials
TEAM-TBI study design and participants
This is a secondary analysis of the Targeted Evaluation Action and Monitoring of TBI trial, which was a prospective multiple interventional trial of patients with chronic issues from TBI lasting at least 3 months (NCT02657135). Participants were 18–60 years of age, English-speaking, and had a documented history of TBI (n = 95). Participants were baseline tested with a comprehensive assessment battery of demographics/medical history questionnaires, symptoms, neurocognitive performance, and sleep health. 6 A multidisciplinary clinical adjudication committee determined clinical trajectories unique to the individual participant, to which six-month interventions were developed targeted to the individual’s needs. 7 Members of the adjudication committee included clinicians in neurosurgery, neuropsychology, otolaryngology, vestibular therapy, nursing, and concussion specialists. Trajectories were ranked in order of importance to the individual patient’s health as primary, secondary, and tertiary. 7 Possible trajectories included psychological, vestibular, ocular, sleep, cognitive, and headache/migraine. Trajectories were subcategorized based on specific clinical needs (e.g., post-traumatic stress, depression, and anxiety disorder). Primary results of the trial and specific treatment pathways have been reported elsewhere. 7 This study was reviewed and approved by the University of Pittsburgh Institutional Review Board for human subjects research.
Blood biomarkers
Plasma samples were analyzed using the Reverse Phase Protein Microarray system. Denatured samples were serially diluted in a five-step, 1:2 manner and printed onto nitrocellulose film slides via the Quanterix 2470 Arrayer. Azure protein-free blocking buffer was used to dry and block slides which were then incubated with primary antibodies overnight (8–12 h) at 4°C. After washing, slides were incubated with biotinylated secondary antibodies (1:100,000 dilution). Slides were scanned in an Innopsys InnoScan 710-IR scanner for extended dynamic range signal acquisition at 785 nm, and net intensity versus dilution was plotted on a log2–log2 scale. The total amount of antigen is determined by the Y-axis intercept, which was log2-transformed corresponding to the total net intensity of the undiluted plasma sample. Biomarkers analyzed included glial fibrillary acidic protein (GFAP), tau, hyperphosphorylated tau Thr231 (p-Tau), von Willebrand factor (vWF), brain lipid-binding protein (BLBP), ubiquitin C-terminal hydrolase-L1 (UCH-L1), vascular endothelial growth factor-a (VEGFa), and claudin-5 (CLDN5). These biomarkers were selected a priori due to their association with TBI and chronic issues secondary to TBI.
Outcome measures
The PTSD Checklist for DSM-5 (PCL-5) is a 20-item measure assessing 20 symptoms of post-traumatic stress from the DSM-5. Total PCL-5 score was used for analysis where higher scores indicate more post-traumatic stress symptoms (range: 0–80). The Brief Symptom Inventory-18 (BSI-18) was used to assess somatization, depression, and anxiety symptoms. Each domain has six individual items that are summed for a total subscale score within that domain and then converted into T scores. The total BSI-18T score was used for analysis, where higher scores indicate more psychological health symptoms (range: 0–100). Change scores for Brief Symptom Inventory-18 (BSI-18) were calculated after converting to T scores.
Statistical analysis
Change scores were calculated for each outcome as the participant’s post-intervention score subtracted from the pre-intervention score. As such, negative change scores indicate improvement in symptoms within that domain. Pearson correlations were conducted to evaluate the association between post-traumatic stress (i.e., PCL5) and overall psychological health (i.e., BSI-18) change scores and pre-intervention blood biomarkers. Five backward linear regression models were built for each outcome (i.e., change in PCL5, BSI-18 over the 6-month intervention period). The first two models used only participants adjudicated to have a psychological trajectory. The second two models used all participants, regardless of the assigned trajectory. A model to evaluate PCL5 change in a subgroup of participants who were adjudicated to have post-traumatic stress symptoms was also built. Blood biomarker concentrations (log-transformed) at pre-intervention and covariates (e.g., age, sex, military status [active or retired compared with civilian], time in years since last TBI, and blast vs. blunt mechanism of injury) were included in the original model with a cutoff of p < 0.1 required for inclusion in the final model. Akaike information criterion (AIC) and Bayesian information criteria (BIC) were used to compare models, where lower values indicate better model fit and optimized complexity. For included variables, standardized beta coefficients (β) are reported. Two backward logistic regression models were built for those with a psychological trajectory to predict those who would improve beyond the minimum clinically important difference (MCID) during the treatment period. MCID was defined as beyond 1 standard deviation in PCL5 and BSI-18 scores. Predicted probabilities were exported from these models and entered in an area under the receiver operating curve. Regression modeling assumptions were assessed and determined to be acceptable before analysis. Statistical significance was set at p < 0.05.
Results
Descriptive statistics of the overall sample can be viewed in Table 1. Approximately 82% of participants were adjudicated to have a psychological trajectory and were included in the present analysis (n = 75). Of those, 29.3% (n = 22) were determined to have probable post-traumatic stress. Approximately one in four participants improved beyond the MCID for PCL5 (n = 18; 24.0%) and BSI-18 (n = 19; 25.3%). Differences in demographics between responders and nonresponders can be viewed in Supplementary Table S1. Scatterplots for correlation results can be viewed in Figure. 1. PCL5 change scores correlated with vWF (r = −0.49; p = 0.001) and tau (r = −0.64; p < 0.001). BSI-18 change scores also correlated with vWF (r = −0.35; p = 0.02) and tau (r = −0.31; p = 0.046). No other significant relationships between blood biomarkers and PCL5 and BSI change scores were noted.
Regression Model Coefficients
Statistically significant at p < 0.05.
BSI-18, Brief Symptom Inventory-18; BLBP, brain lipid-binding protein; CLDN5, claudin-5; GFAP, glial fibrillary acidic protein; PCL-5, PTSD Checklist for DSM-5; TBI, traumatic brain injury; UCH-L1, ubiquitin C-terminal hydrolase-L1; VEGFa, vascular endothelial growth factor-a; vWF, von Willebrand factor.
Descriptive Statistics of the Overall Sample [Mean ± Standard Deviation or Number (Percentage)]
BSI-18, Brief Symptom Inventory-18; BLBP, brain lipid-binding protein; CLDN5, claudin-5; GFAP, glial fibrillary acidic protein; PCL-5, PTSD Checklist for DSM-5; TBI, traumatic brain injury; UCH-L1, ubiquitin C-terminal hydrolase-L1; VEGFa, vascular endothelial growth factor-a; vWF, von Willebrand factor.
Predicting change in PCL-5 and BSI-18 scores in participants with a psychological trajectory
Regression model coefficients can be viewed in Table 2. The linear regression model to predict change in PCL5 scores was statistically significant (R 2=0.64; p < 0.001; n = 41) and included vWF (β = −0.31; p = 0.032), BLBP (β = 1.00; p = 0.001), tau (β = −0.47; p = 0.002), VEGFa (β = −0.77; p = 0.015), female sex (β = 0.32; p = 0.06) and military status (β = −0.42; p = 0.014) as predictors. The final model had an AIC = 284.3 and BIC = 296.1.
The linear regression model to predict change in BSI-18 scores was statistically significant (R 2 = 0.42; p = 0.003; n = 39) and included vWF (β = −0.35; p = 0.042), VEGFa (β = 0.67; p = 0.09), BLBP (β = 1.02; p = 0.01), CLDN5 (β = −1.65; p < 0.001), female sex (β = 0.65; p = 0.012), and military status (β = −0.76; p = 0.004) as predictors. The final model had an AIC = 271.4 and BIC = 283.6.
Predicting change in PCL-5 and BSI-18 scores in all participants
The linear regression model to predict change in PCL5 scores for the entire cohort was statistically significant (R 2 = 0.31; p < 0.001; n = 94) and included vWF (β = −0.35; p = 0.002), BLBP (β = 0.73; p = 0.006), tau (β = −0.29; p = 0.007), CLDN5 (β = −0.56; p = 0.034), and military status (β = −0.26; p = 0.003) as predictors. The final model had an AIC = 214.6 and BIC = 325.2.
The linear regression model to predict change in BSI-18 scores for the entire cohort was not statistically significant (R 2 = 0.08; p = 0.05; n = 94) and included vWF (β = −0.25; p = 0.070), CLDN5 (β = −0.35; p = 0.05), and GFAP (β = 0.35; p = 0.08) as predictors. The final model had an AIC = 350.1 and BIC = 354.0.
Predicting change in PCL-5 in participants with probable post-traumatic stress
The linear regression model to predict change in PCL-5 scores in participants with post-traumatic stress was statistically significant (R 2 = 0.58; p = 0.002; n = 22) and included UCH-L1 (β = 0.55; p = 0.004), tau (β = −0.66; p < 0.001), and years since TBI (β = −0.37; p = 0.03) as predictors. The final model had an AIC = 75.6 and BIC = 80.0.
Predicting improvement in PCL-5 and BSI-18 beyond the MCID in participants with a psychological trajectory
The logistic regression model to differentiate participants who improved beyond the MCID for PCL5 over the treatment period was statistically significant (R 2 = 0.68; p < 0.001) and included pre-intervention vWF (β = 2.29; p = 0.02), VEGFa (β = 9.36; p = 0.008), and BLBP (β = −12.70; p = 0.006) as predictors. This model differentiated responders from nonresponders with an AUC = 0.93 (Fig. 2a).
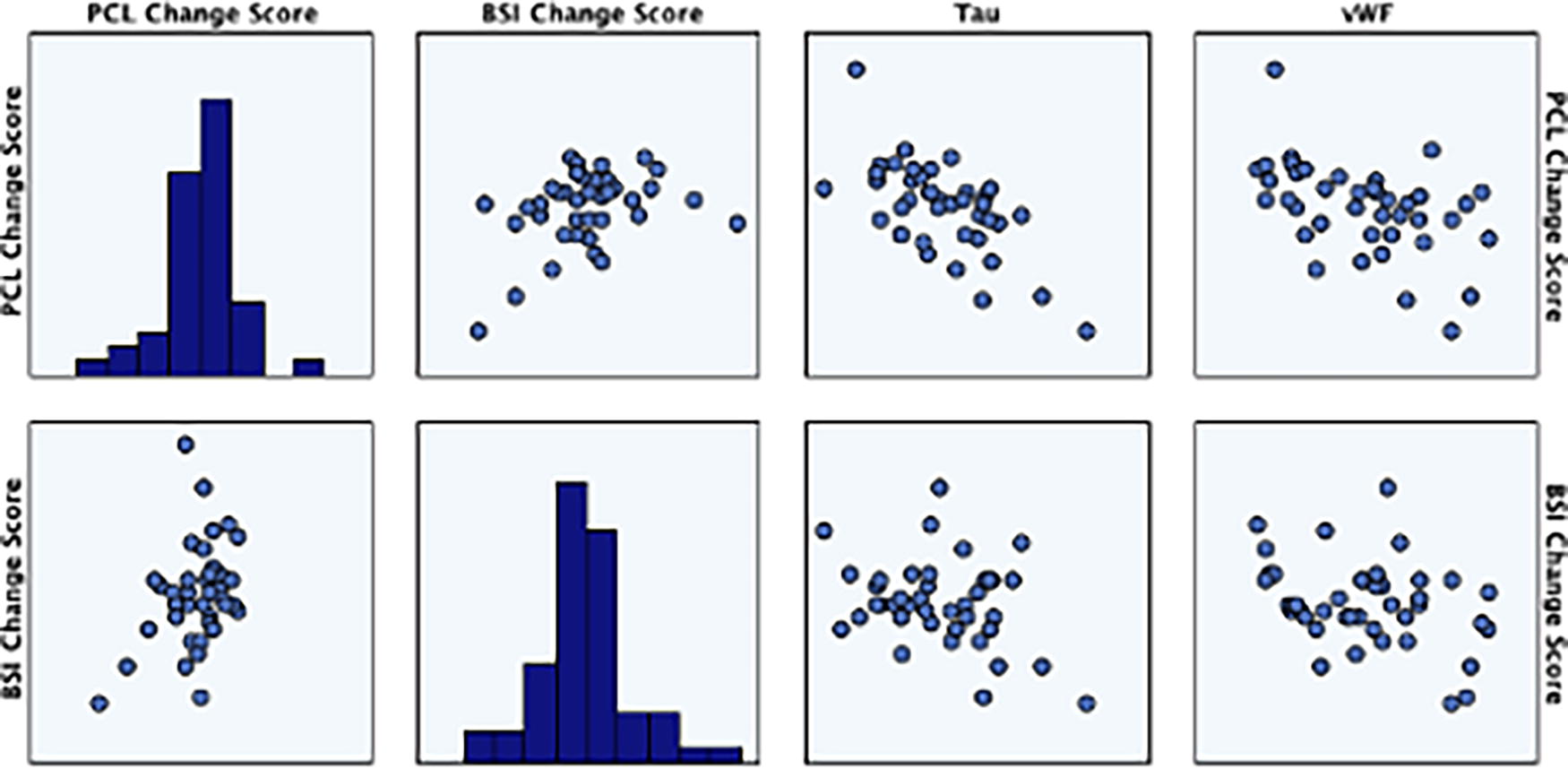
Scatterplot matrix of PCL5 change score, BSI-18 change score, pre-intervention tau, and pre-intervention vWF. PCL5 change scores correlated with vWF (r = −0.49; p = 0.001; top right image) and tau (r = −0.64; p < 0.001; top middle image). BSI-18 change scores also correlated with vWF (r = −0.35; p = 0.02; bottom right image) and tau (r = −0.31; p = 0.046; bottom middle image). BSI-18, Brief Symptom Inventory-18; PCL-5, PTSD Checklist for DSM-5; vWF, von Willebrand factor.
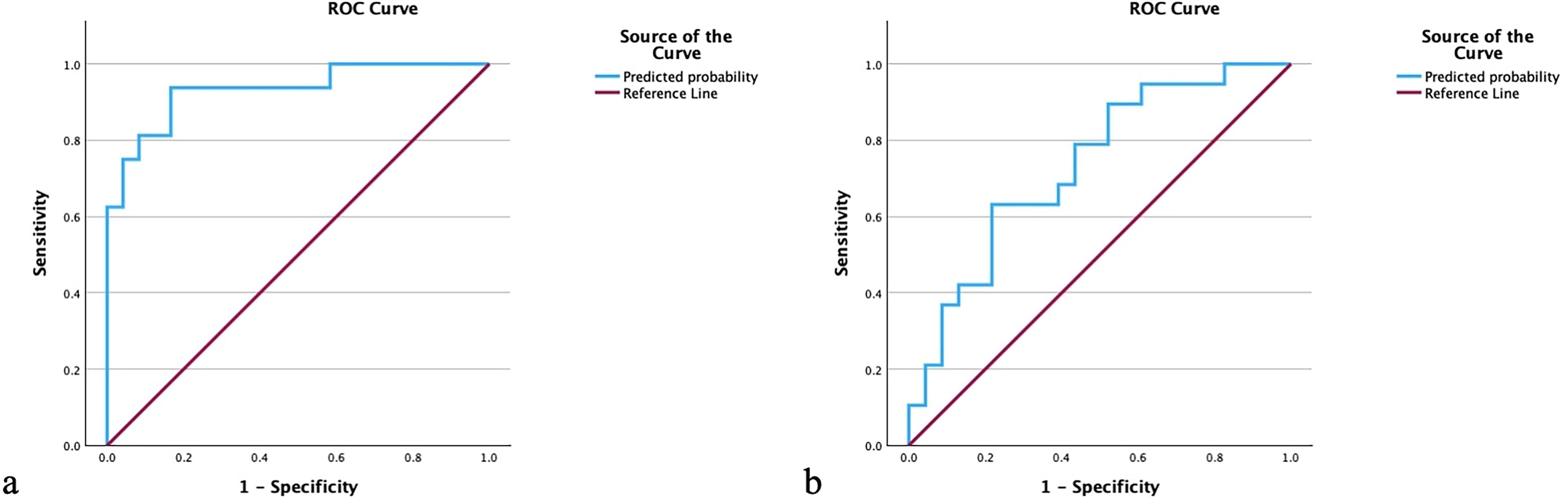
The logistic regression model to differentiate participants who improved beyond the MCID for BSI-18 over the treatment period was statistically significant (R 2 = 0.25; p = 0.04) and included UCH-L1 (β = 4.52; p = 0.03), GFAP (β = 0.20; p = 0.06), and vWF (β = 3.85; p = 0.03) as predictors. This model differentiated responders from nonresponders with an AUC = 0.73 (Fig. 2b).
Discussion
Predictive biomarkers provide a valuable framework for forecasting responsivity to treatment interventions and subsequent outcome. The models presented in this study accounted for 42–64% of the variance in responsiveness to a 6-month individualized treatment. When analyzing change in post-traumatic stress (i.e., PCL5) and psychological health scores (i.e., BSI-18) for the overall cohort, significantly less variance was accounted for (8–42%) by the same predictors, indicating that predictive biomarkers have more utility for identifying responsiveness to therapies tailored to the individual’s specific needs. Among participants with psychological trajectories, blood biomarkers were able to differentiate responders to targeted treatment for post-traumatic stress (AUC = 0.93) and overall psychological health (AUC = 0.73).
The data from this study show that proteins involved in neurovascular and endothelial health (i.e., vWF, BLBP) are significant predictors of long-term psychiatric symptoms after TBI. vWF was the strongest predictor of psychological intervention, as it was significant across all regression models. Interestingly, vWF has also been shown to be a predictive biomarker of therapeutic response to sleep therapy after chronic mTBI. Prior work has shown that psychological and sleep subtypes commonly overlap after TBI, 8,9 which suggests these subtypes may have similar biological mechanisms. BLBP (also known as fatty acid-binding protein 7) and claudin-5 were also significant predictors. These proteins are emerging blood biomarkers within the psychiatric field, due to their association with symptom development and severity, 10,11 mechanistic links to induction of (or protection against) depression-like behaviors, and responsivity to pharmacological treatments in pre-clinical models and human studies. 12 More research will be needed to understand the timeline and trajectory of these biomarkers and how that relates to clinical outcomes after TBI.
VEGFa was a significant predictive biomarker when isolating the overall cohort to those with a psychological trajectory. While also well studied as a marker and mechanism of psychiatric disorders, within specific diagnoses, there are conflicting reports on the direction of changes. For example, decreased biomarker levels are positively associated with the severity of illness in major depressive disorder, while decreases in anxiety disorders indicate improvements in symptom management. 13 Furthermore, increases in circulating VEGFa may confer neurovascular protection after TBI, while also indicating the degree of TBI severity. 14 The variability in directionality and the disease-specific nature might account for the reduced predictability of VEGFa in a homogenous TBI population versus those with a specific psychological trajectory.
Female sex was a significant predictor within the psychiatric trajectory group only. Sex differences in both psychiatric disorders and in TBI have been well documented. Particularly in veterans, depressive and anxiety disorders are more prevalent in women than in men. 15 In addition, following blast TBI, women are more likely diagnosed with depression, anxiety, and comorbid PTSD. 16 However, similar to this study, when generalizing to a mild TBI population, no significant interactions were found between TBI and sex for the outcome measures on the PCL-5 and BSI-18. 17 The active duty or veteran military populations demonstrates the utility of predictive biomarker panel in a psychiatric trajectory cohort. Especially given the onset of mental health conditions, including time to suicide, was significantly higher in soldiers with reported TBI compared with those without. 18 A predictive biomarker for particularly vulnerable TBI subgroups is key to optimizing evidence-based interventions for psychological issues after TBI.
Tau correlated with both PCL-5 and BSI-18 change scores. After controlling for other biomarkers in regression modeling, tau was only associated with PCL-5 change in both the psychological trajectory, post-traumatic stress subtrajectory, and overall population. Axonal injury is thought to be a contributing factor to the development of PTSD after TBI. 19 Tau, an axonal protein, is notably a diagnostic biomarker of neurodegenerative diseases such as chronic traumatic encephalopathy and Alzheimer’s disease. Given the increased risk of dementia that veterans with PTSD have over veterans without PTSD, 20 this potentially provides insights into distinguishing the pathophysiology of post-traumatic stress from other psychiatric diagnoses. It should be noted that participants in the present study who had higher pre-intervention tau levels had greater improvements in post-traumatic stress symptoms (and overall psychological symptoms in correlation analyses). This result suggests an optimistic outlook for patients with chronic psychological health symptoms after TBI is warranted and, even with higher detectable proteins associated with neurodegenerative disease, targeted treatments can provide relief.
Limitations
One limitation of this study is the unknown prevalence of neuropsychiatric diagnoses before TBI. Pre-injury psychiatric illness is a strong predictor of its development post-injury. 19 Another limitation is that questionnaires are self-reported, which may result in recall bias. Adherence to the prescribed treatments was not tracked. Approximately two-thirds of the sample was former military, which may limit generalizability to the general population. The standard deviation in years since last TBI was 3.6, indicating there was a wide range in time of experiencing chronic symptoms in these participants. Every participant was assigned more than one treatment trajectory and therefore received multiple treatment plans to address concerns other than psychological health (i.e., vestibular therapy and headache/migraine management). Determining which treatment effect was observed is not possible with this trial design, but all participants included in this analysis were adjudicated to have a psychological trajectory. Treatment prescriptions varied person-to-person specific to what the clinician deemed was appropriate to meet the participant’s needs.
In this secondary analysis of a prospective multiple interventional trial of targeted therapies for chronic psychological issues after TBI, predictive blood biomarkers, female sex, and military status accounted for approximately half the variance in responsiveness to a 6-month individualized treatment. Combinations of pre-intervention blood biomarkers were also able to differentiate responders from nonresponders in both post-traumatic stress and overall psychological health domains in the psychological trajectory subgroup. The results of this study indicate that predictive biomarkers have more utility for identifying responsiveness to targeted therapies to specific subgroups compared with analyzing as a homogenous cohort. This work can help inform future clinical practice and may elucidate underlying mechanisms of post-injury neuropsychiatric sequelae.
Footnotes
Authors’ Contributions
S.R.E.: Conceptualization (lead), writing original draft (lead), and reviewing and editing (equal). A.M.P.: Methodology (co-lead) and reviewing and editing (equal). D.V.A.: Conceptualization (supporting), methodology (co-lead), formal analysis (supporting), and reviewing and editing (equal). S.S.: Methodology (supporting) and reviewing and editing (equal). K.E.: Methodology (supporting) and reviewing and editing (equal). A.B.: Methodology (supporting) and reviewing and editing (equal). S.B.: Methodology (supporting) and reviewing and editing (equal). M.C.: Methodology (supporting) and reviewing and editing (equal). A.P.K.: Methodology (supporting) and reviewing and editing (equal). W.S.: Methodology (supporting) and reviewing and editing (equal). R.J.S.: Conceptualization (supporting), methodology (supporting), and reviewing and editing (equal). D.O.O.: Conceptualization (supporting), methodology (supporting), and reviewing and editing (equal).
Funding Information
This study was funded by the Department of Defense (USAMRMC Department of Defense Award Nos: W81XWH 14 2 0002 and W81XWH 12 2 0140).
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.