
Abstract
This article explores the diagnostic performance of a panel of six biomarkers (glial fibrillary acidic protein [GFAP], neurofilament light [NFL], neuron-specific enolase [NSE], S100 calcium-binding protein B [S100B], total tau [t-tau], and ubiquitin C-terminal hydrolase L1 [UCH-L1]) in the context of the “2023 UK National Institute for Health and Care Excellence (NICE) Head Injury: Assessment and early management (NG232)” guideline. Emphasis is placed on subjects where clinical equipoise remains concerning the decision for head computed tomography (CT), medium-risk subjects. All adult subjects from the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) dataset with a complete biomarker profile and interpretable CT scan within 24 h of injury were classified as high, medium, and low-risk according to the NICE NG232 Clinical Decision Rule (CDR) for CT head imaging following head injury. In subjects classified as medium-risk, the area under the receiver operating characteristic curve (AUC) was used to assess the diagnostic performance of biomarkers to identify those with (1) CT abnormality or (2) potential neurosurgical lesion, with CT considered the gold standard diagnosis. A time-to-biomarker sub-analysis was performed in subjects with a time from injury to sampling within 6 h, in keeping with current clinical usage of biomarkers. Among 1979 CENTER-TBI participants with sufficient clinical information to facilitate classification, 385 subjects were classified as medium-risk. Biomarker concentrations were significantly higher in those with traumatic CT abnormalities as compared with those without for all biomarkers aside from NSE (all p < 0.05). When sampled within 24 h of injury, GFAP demonstrated the best diagnostic performance for CT abnormality (AUC 0.81 [0.77–0.86]), with NFL, t-tau, and UCH-L1 showing moderate performance. At a threshold to provide a 95% sensitivity, GFAP, NFL, t-tau, and UCH-L1 demonstrated specificities ranging from 18% to 33% corresponding to a potential reduction of total CT images performed in these subjects by 14–23%. S100B and UCH-L1 showed improved performance when biomarker sampling time was limited to 6 h following injury. In intoxicated subjects with a persistent Glasgow Coma Score of 13–14, biomarker levels were significantly higher in subjects with CT abnormality as compared with those without. In conclusion, serum biomarkers demonstrate potential for the reduction in CT scan requirements in those classified as medium-risk in reference to the NG232 CDR criteria. These results highlight a need for further prospective studies on the use of diagnostic TBI biomarkers in current emergency medicine practice, with future consideration given to the integration of biomarkers in the NICE NG232 head injury guidelines.
Introduction
Traumatic brain injury (TBI) is a leading cause of morbidity and mortality. 1 The acute management of head injury in the emergency department (ED), following initial stabilization, often focuses on identifying those with a clinically significant brain injury requiring admission or neurosurgical intervention. The diagnostic modality of choice following TBI remains a computed tomography (CT) scan of the head, with clinical decision rules (CDRs) used by clinicians to help guide when this acute imaging is indicated. CDRs aim to identify patients at higher risk of traumatic pathology on CT scan while also avoiding unnecessary radiation exposure in patients deemed low risk.
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) Head injury: Assessment and Early management (NICE Guideline NG232), first released in 2003 and last updated in 2023, contains the most commonly used CDR for this purpose. 2 The NG232 CDR is largely derived from the Canadian Head CT Rule 3,4 and while CDRs including the NICE NG232 have been shown to be sensitive for traumatic CT findings, the specificity is often low. 5 This means that over 90% of those with imaging performed in the ED will have no acute findings. 5,6 Although a higher specificity has been shown using the NICE guideline as compared with other CDRs, 5 there remains a need for additional diagnostic tools to help refine the pretest probability of clinically important CT findings, improving specificity and reducing unnecessary imaging.
The NICE NG232 CDR classifies patients into low, medium, and high-risk categories and includes all levels of Glasgow Coma Score (GCS) in the algorithm. 2 In high-risk patients (Table 1), there are correspondingly high rates of clinically important brain injuries observed on CT imaging making the need for a scan clear. 7 In comparison, patients with medium-risk criteria less frequently exhibit clinically significant radiographic features. 8 Therefore, the requirement for imaging is less evident in this patient population. CT imaging is not routinely recommended for low-risk patients, making medium-risk patients the most suitable group for targeted diagnostic interventions to minimize costs and reduce the risks associated with unnecessary CT scans.
National Institute for Health and Care Excellence Head Injury Guidelines Criteria for Investigating Clinically Important Traumatic Brain Injuries (2023), Reproduced Directly from the Guideline 2
CT, computed tomography; DOACs, direct-acting oral anticoagulants; ED, emergency department.
There is growing interest in the use of diagnostic proteomic biomarkers, sampled from the blood, to screen patients following TBI for the requirement of acute CT imaging. There are several candidate biomarkers in the literature, including the axonal marker neurofilament light (NFL); dendritic marker total tau (t-tau); neuronal markers neuron-specific enolase (NSE) and ubiquitin C-terminal hydrolase L1 (UCH-L1); and the astroglial markers S100 calcium-binding protein B (S100B) and glial fibrillary acidic protein (GFAP). 9
S100B has been used in the Scandinavian NeuroTrauma Committee (SNC) TBI guidelines since 2013 for a select group of patients with TBI (GCS 14–15 and suspected/confirmed loss of consciousness or ≥2 episodes of vomiting presenting within 6 h) to determine the requirement for CT imaging, with validation studies showing a reduction in the number of unnecessary CT images performed. 10,11 Following the results of the Prospective Clinical Evaluation of Biomarkers of Traumatic Brain Injury (ALERT-TBI) trial, which demonstrated the utility of a combined UCH-L1 and GFAP test for ruling out the need for head CT when sampled within 12 hours of injury, combined UCH-L1 and GFAP tests have now received both U.S. Food and Drug Administration (FDA) clearance and Conformité Européenne (CE) marking for the assessment of patients with mild TBI. 12,13 A subsequent targeted assessment of subjects where biomarker sampling would be recommended by the SNC TBI demonstrated superior performance with the sampling of GFAP and UCH-L1 as compared with S100B in predicting CT-positivity. 14 Other guidelines have suggested a combined biomarker approach, with recent French guidelines from the French Society of Emergency Medicine (SFMU) and the French Society of Anaesthesiology and Critical Care Medicine (SFAR) recommending either the use of GFAP/UCH-L1 within 12 h of injury, or S100B if sampled within 3 h, to screen patients at intermediate risk for the requirement of CT scan, with the stated goal being “to limit the number of brain scans.” 15
In the United Kingdom, no proteomic biomarker (or combination thereof) is currently recommended for clinical use owing to the lack of validation in the context of the higher specificity of the NICE NG232 CDR. The medium-risk population, as identified by the NG232 CDR, represents an intermediate risk population where clinical equipoise remains concerning the requirement of CT imaging and the targeted use of biomarkers may present the most pragmatic method for integration of biomarkers into current UK clinical practice. Although there has been a single previous examination of S100B in reference to the NICE guidelines, showing a potential 27% reduction in CT scans, no previous study has examined a wider panel of biomarkers or specifically focused on medium-risk patients. 6
Therefore, we performed an exploratory, targeted analysis of the Collaborative European NeuroTrauma Effectiveness Research (CENTER)-TBI cohort aiming to assess whether day-of-injury biomarkers (GFAP, NFL, NSE, S100B, t-tau, UCH-L1) can identify (1) CT abnormalities and (2) lesions requiring neurosurgery in patients classified as medium-risk in reference to the “2023 UK NICE Head injury: assessment and early management (NG232)” guideline CDR.
Materials and Methods
Study details, demographics, and clinical characteristics
Demographics, injury characteristics, imaging findings, and biomarker levels were extracted from the CENTER-TBI core study (RRID/SCR_017004, Core Data Version 3.0, EC Grant 602150). 16,17 CENTER-TBI is a prospective observational study conducted at 65 sites across 18 countries between December 19, 2014, and December 17, 2017 (https://clinicaltrials.gov/ct2/show/NCT02210221). CENTER-TBI was conducted in accordance with all relevant European Union laws, where directly applicable or of direct effect, as well as all relevant laws of the countries where the recruiting sites were located. Details on sites, ethics, approval numbers, and dates are available online (https://www.center-tbi.eu/project/ethical-approval).
All subjects in the CENTER-TBI core study aged 16 years or over with a non-penetrating brain injury were assessed for classification according to the NICE NG232 CDR criteria. 2 Subjects without an acute CT report or complete biomarker panel within 24 h were excluded. The extra-cranial Injury Severity Score (ISS) was calculated by considering injuries to the face, abdomen, chest, extremities, and external areas, but excluding the head. Subjects with an extra-cranial ISS ≥15 were excluded as these were considered polytrauma cases requiring CT regardless of NG232 CDR criteria as part of current major trauma management practice.
NG232 CDR criteria for head CT were mapped to prospectively recorded variables collected in the CENTER-TBI study, allowing retrospective identification of the NICE NG232 CDR risk categories (Supplementary Table A1). The CENTER-TBI clinical variables were extracted by trained researchers in a standardized format from the available clinical records data using an electronic case report form (eCRF) based on common data elements (CDE) (https://www.commondataelements.ninds.nih.gov/). 17 A source data verification process was conducted in the CENTER-TBI study to ensure there was no discrepancy between clinician and study recordings. However, data were not extracted in duplicate, with no formal assessment of inter-rater reliability between data abstractors. Where multiple variables from the CENTER-TBI CRF were mapped to one NG232 CDR criterion, a positive recording in one or more variables was required for a subject to meet that criterion. Medium-risk subjects were those who did not meet the NG232 CDR criteria for imaging within 1 h of identifying risk factors (with these subjects considered high-risk), but (1) met the NG232 CDR criteria for CT scan within 8 h (some loss of consciousness or amnesia since injury AND either: aged >65, bleeding or clotting disorder, dangerous injury mechanism or over 30 min of retrograde amnesia), and (2) did not meet other NG232 CDR criteria but had a record of anticoagulant or antiplatelet use (excluding those on aspirin monotherapy), in which case CT imaging is currently advised to be “considered” by NICE. Low-risk subjects were those with no confirmed risk factors in either the high or medium-risk NG232 CDR criteria and not taking antithrombotic medication. A variable was recorded as either present, absent, unknown, or missing.
To avoid misclassification due to missing data, all subjects classified as medium or low-risk were excluded if they had missing or unknown recordings of variables used to classify subjects as high-risk. 2 Low-risk subjects were then further excluded if they were missing variables that were used to classify subjects as medium-risk, with a complete case analysis presented. Where multiple variables in the CENTER-TBI CRF were used to assess if subjects met a single criterion of the NG232 CDR, the presence of at least one of the CENTER-TBI variables was considered sufficient. A CONSORT diagram of the analysis cohort is presented in Figure 1, with the variables used to derive the subjects’ risk category from the CENTER-TBI clinical record forms available in Supplementary Table A1.
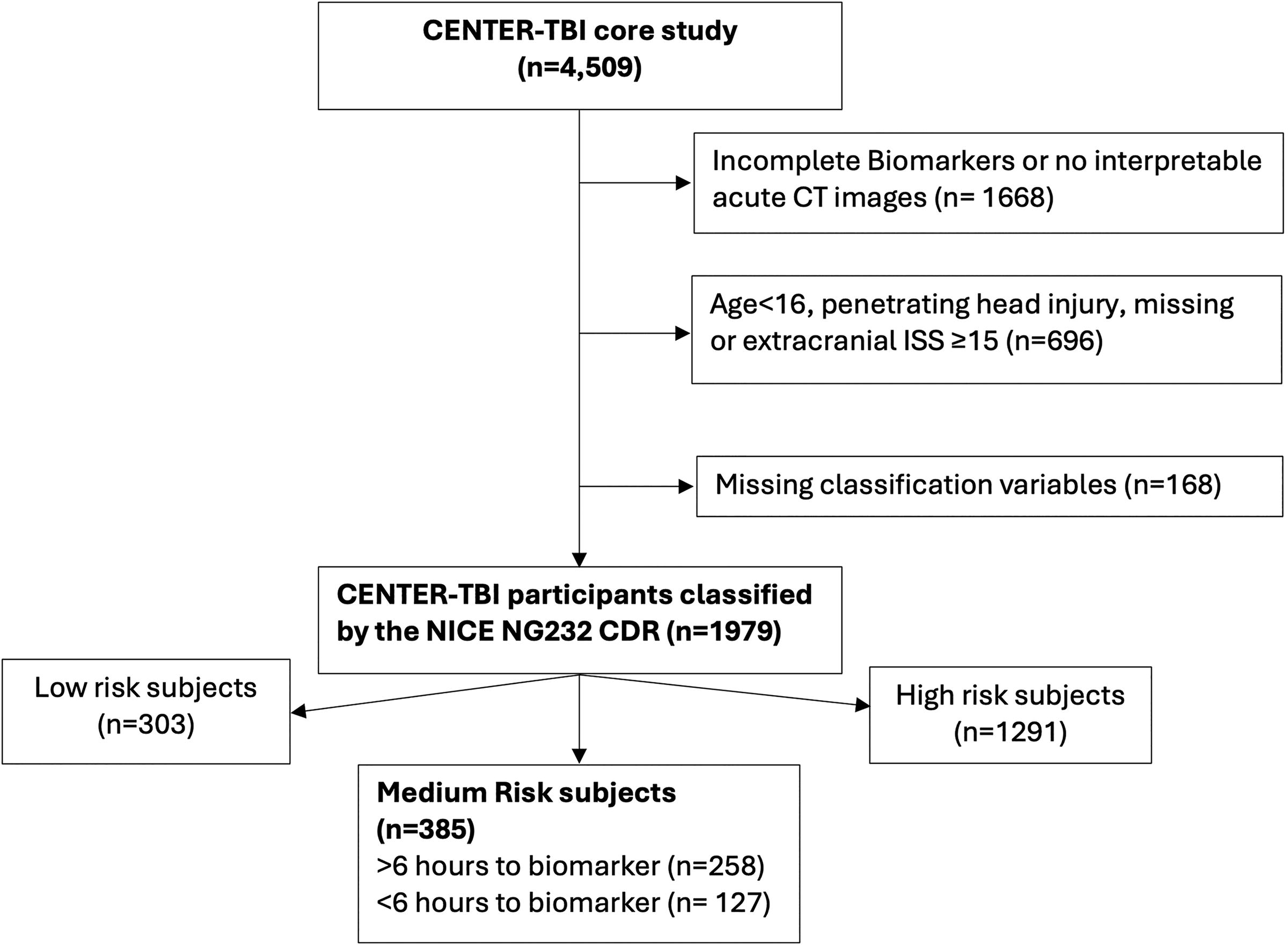
CONSORT diagram of the analysis cohort.
A further patient group of particular interest to emergency physicians in relation to the use of acute blood-based biomarkers are those who present intoxicated with drugs or alcohol with a persistently low GCS, but no other high-risk features for acute CT imaging. According to current NICE guidelines, these patients are considered high-risk, requiring CT imaging within 1 h. However, intoxicated patients are often challenging to assess and manage. Therefore, a preplanned subanalysis was performed on subjects with a clinical suspicion (either confirmed or suspected) of intoxication with alcohol or drugs and a GCS score of less than 15 at 2 h after the injury on assessment in the ED as the only high-risk NICE guideline criteria for CT imaging. Subjects with a presenting or post stabilization GCS ≤12 were not included in this subset, and those with missing data in relation to other high-risk criteria were excluded.
Outcome measures
The primary outcome was the presence of a clinically significant traumatic CT abnormality (mass lesion, extra-axial hemorrhage, epidural hemorrhage [EDH], acute or chronic subdural hemorrhage [SDH], contusion, traumatic axonal injury, traumatic subarachnoid hemorrhage, intraventricular hemorrhage, midline shift, or cisternal compression). A skull fracture was included as a CT abnormality only if it was a depressed fracture or if the subject was taking antithrombotic medications, in accordance with NICE guidance (NG232, 1.9.1) 2 The secondary outcome measure was any potential neurosurgical lesion, as defined in the prior literature (EDH, acute SDH with mass effect, contusion with mass effect, depressed skull fracture, or any lesion with midline shift or signs of herniation). 5
Biomarker sampling
Samples were collected within 24 h of injury, centrifuged within 60 min, and processed locally. The serum was stored at −80°C and shipped to the CENTER-TBI biobank located in Pécs, Hungary. NSE and S100B were analyzed on a clinical platform assay using an electrochemiluminescence immunoassay kit (Elecsys S100 and NSE assays, run on the e602 module of the Cobas 8000 modular analyzer, Roche Diagnostics, Mannheim, Germany). GFAP, NFL, t-tau, and UCH-L1 were analyzed using a research-use only (RUO) assay, Single Molecule Arrays-based Human Neurology 4-Plex B assay, run on the SR-X benchtop assay platform (Quanterix Corp., Lexington, MA). 18 Biomarker analysis was performed in Pécs, Hungary, and Gainesville, USA, with the team members analyzing biomarker results blinded to relevant participant characteristics. The assay range was: GFAP 1.32–40,000 pg/mL; NFL 0.0971–2000 pg/mL, NSE 50–370,000 pg/mL, S100B 0.005–39 µg/L, t-tau 0.0231–400 pg/mL, and UCH-L1 1.34–40,000 pg/mL. If the levels were found above the assay range, the samples were diluted and analyzed again. All values of GFAP, NFL, NSE, S100B, and t-tau were greater than the lower limit of detection, with 0.7% (n = 13) of UCH-L1 below. The coefficient of variance between replicates of biomarkers assays, as calculated and reported previously across the overall CENTER-TBI cohort, was 7% for the clinical-platform assays (S100B and NSE) and ranging between 22% and 30% for the RUO assays GFAP, NFL, t-tau, and UCH-L1. 18
Neuroimaging
Initial CT scans were reported by a panel of three protocol-trained central reviewers in accordance with the CDE scheme for TBI. 19,20 All readers were blinded to clinical information except for gender, age, and care path stratum. Findings were recorded as present, absent or indeterminate. <0.6% of CT images had an indeterminate finding per lesion type, with the greatest number of indeterminate results concerning the presence of a skull fracture (n = 12). If a finding was reported as indeterminate, it was considered present.
Statistical analysis
Demographic and injury characteristics are presented using medians and interquartile ranges for continuous variables, and counts/percentages for categorical data. The sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio of the NICE NG232 CDR was calculated for the identification of patients with clinically important CT findings using a 2 × 2 table. To assess if the biomarker levels scaled to the NICE NG232 risk categories, the biomarkers levels were compared between the categories using the Kruskall–Wallis test with post-hoc Dunn testing.
In medium-risk subjects only, biomarker concentrations were compared between subjects with/without CT abnormalities and neurosurgical lesions using the Wilcoxon test with presentation of the biomarker values, p values, and p values adjusted for multiple comparisons using the Benjamini–Hochberg method. 21 The area under the receiver operating characteristic (ROC) curve (AUC) was calculated to determine the discriminative ability of serum biomarkers for both primary and secondary outcomes (with 0.6–0.7 considered poor, 0.7–0.8 moderate, 0.8–0.9 good, and >0.9 excellent) in medium-risk subjects, with 95% confidence intervals (CI) calculated using bootstrapping with 2000 replicates. Thresholds were calculated from the ROC curve analysis to achieve 95% sensitivity for CT abnormality and 100% sensitivity for any potential neurosurgical lesion. A confusion matrix was created at each threshold with reporting of true positives, false positives (FP), false negatives (FN), true negatives (TN), sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), and confidence intervals derived from bootstrapping with 2000 stratified bootstrap replicates. In addition, the performance of S100B at a clinically validated threshold of 0.1 μg/L was assessed. 11 The same processes were followed to return further sensitivity thresholds (100%, 95%, and 90%), with results presented in the Section 4, Supplementary Appendix.
Each biomarker has a different temporal profile of concentration and recommended sampling windows following injury. 22,23 For example, S100B is recommended to be sampled within 6 h of injury in the Scandinavian head injury guidelines and within 3 h in the SFMU/SFAR guidelines, due to its rapid peak and short half-life. 11,15 To assess the performance of the biomarkers at shorter sampling times from injury, a subgroup analysis was performed on subjects with biomarker samples collected between 0 and 6 h after injury, and reported separately from the overall cohort.
In a preplanned subanalysis of intoxicated participants with a persistent GCS of 13–14, biomarker concentrations were compared between subjects with and without CT abnormalities using the same statistical approach as described above.
P values are two-tailed, with adjusted p < 0.05 considered significant. Statistical analysis was conducted using R statistical software (R version 4.2.1, https://www.R-project.org/) with ROC analysis performed using the pROC package. 24 The work was conducted in accordance with the Standards for Reporting Diagnostic Accuracy (STARD) guidelines.
Data availability
Data access is conditional on an approved study proposal; there are no end dates to the availability. The CENTER-TBI data used in this study are available to researchers who provide a methodologically sound study proposal that is approved by the CENTER-TBI management committee to achieve the aims in the approved proposal. Further details are available online (https://www.center-tbi.eu/data).
Results
Demographics
Out of 4509 subjects in the CENTER-TBI core study, 1979 adult subjects had available biomarker results, CT reports, and sufficient clinical variables available for classification (Fig. 1, Supplementary Table A2). Of these, 385 were classified as medium-risk for clinically important CT findings, with 303 low-risk, and 1291 high-risk (Supplementary Table A3). The sensitivity of the NICE NG232 CDR for identifying subjects for CT imaging with clinically important CT abnormalities was 95% (95% CI: 94–96%), with a specificity of 29% (95% CI: 26–32%), NPV of 83% (95% CI: 78–87%), and PPV of 63% (95% CI: 61–66%). The percentage of positive and negative CTs in relation in the presence of each high and medium risk criterion are presented in the supplement (Supplementary Table A4–A5).
The demographics, imaging findings, and biomarker levels of the medium-risk population are presented in Table 2 with 140 (36%) having a clinically important CT abnormality, and 20 (5%) having a potential neurosurgical lesion. CT imaging was performed at a median of 2 h (interquartile range [IQR] 1.5, 4.1) from injury, while biomarker sampling was spread more widely across the first day of injury with a median time to sampling from injury of 10 h (IQR 4.9, 18.5) (Supplementary Fig. A1 and A2). Among all medium-risk subjects, 127 had biomarker samples taken between 0 and 6 h following injury.
Demographics of Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury Subjects Classified as Medium Risk in Reference to the National Institute for Health and Care Excellence NG232 Clinical Decision Rule
Median [Q1, Q3] of continuous variables; count (percentage) of categorical variables.
ASA, American Society of Anesthesiologists; CT, computed tomography; GCS, Glasgow Coma Score; GFAP, glial fibrillary acidic protein; ICU, intensive care unit; ISS, Injury Severity Score; NFL, neurofilament light, NSE, neuron-specific enolase, S100B, S100 calcium-binding protein B; UCH-L1, ubiquitin C-terminal hydrolase L1.
Biomarker comparisons
Although there was variability in the biomarker levels in each risk group, all biomarker concentrations, except for NSE, were significantly higher in medium-risk subjects than in the low-risk group. Additionally, all biomarkers were significantly higher in high-risk subjects compared with the medium-risk group (Supplementary Fig. A3).
In the medium-risk subjects, the concentrations of all biomarkers, except NSE, were significantly elevated in those with a CT abnormality when sampled at any time up to 24 h post-injury (Fig. 2, Supplementary Table A6). GFAP, NFL, t-tau, and UCH-L1 levels were significantly elevated in medium-risk subjects with a potential neurosurgical lesion compared with those without (Supplementary Table A6). When sampling was restricted to 0–6 h following injury, GFAP, S100B, t-tau, and UCH-L1 levels were significantly higher in medium-risk subjects with a CT abnormality (Supplementary Table A7). The small number of potential neurosurgical lesions prevented the examination of this outcome in the subset with restricted biomarker sampling times.
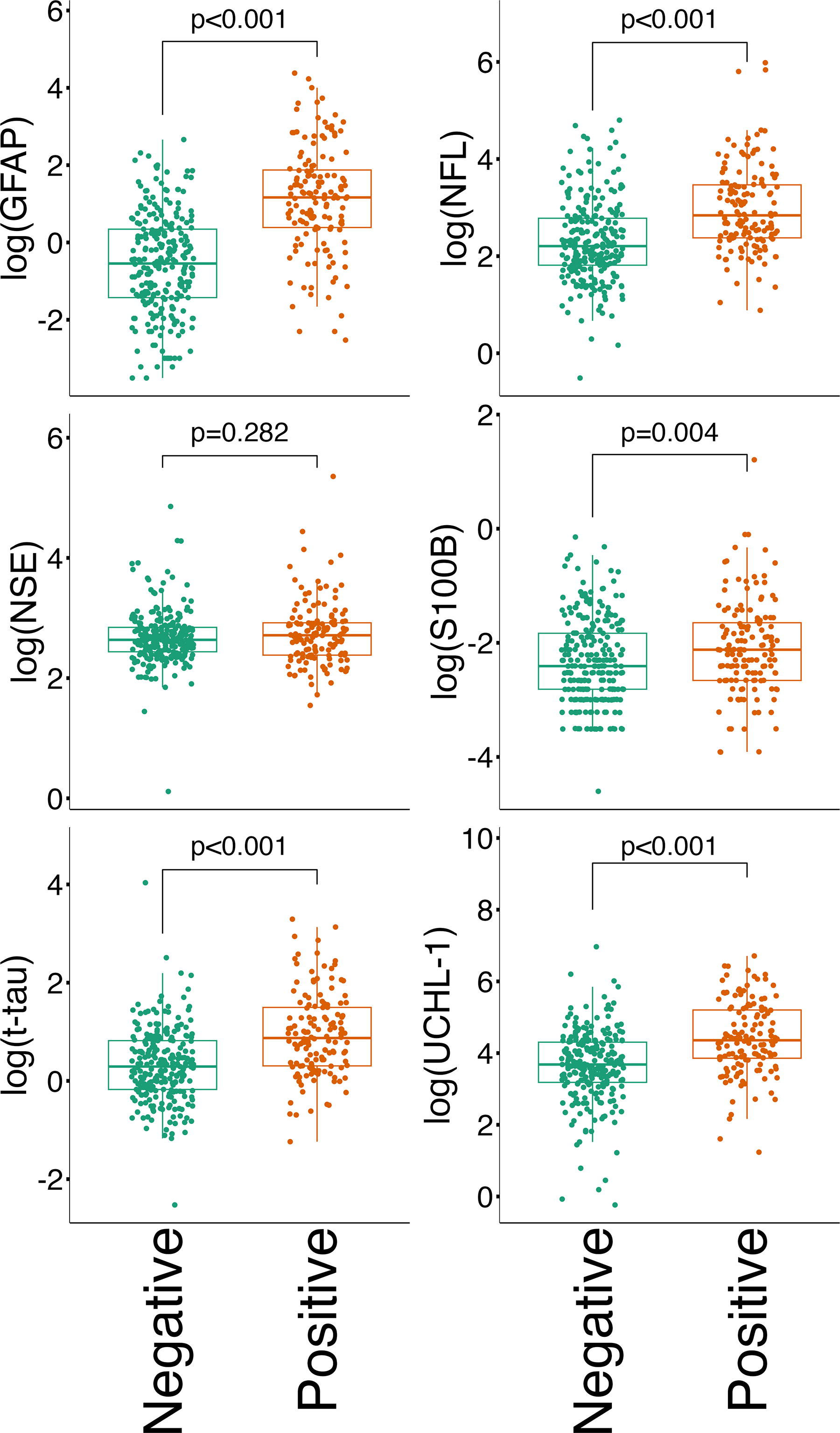
Boxplots demonstrating the median and interquartile range of the natural log of the biomarker sample between CT negative (n = 245) and positive (n = 140) medium-risk subjects. p-Values determined by the Wilcoxon test with correction for multiple comparisons using the Benjamini–Hochberg method. CT, computed tomography.
ROC curve analysis
The ROC curves and AUCs for biomarker performance for the detection of any clinically important CT abnormality and for a potential neurosurgical lesion are presented in Figure 3A and B. GFAP showed the best discrimination for clinically important CT abnormalities, demonstrating good performance when sampled between 0 and 24 h with NFL, t-tau, and UCH-L1 all demonstrating moderate performance. GFAP, NFL, and UCH-L1 all demonstrated moderate or good discrimination for detecting potential neurosurgical lesions (Fig. 3).
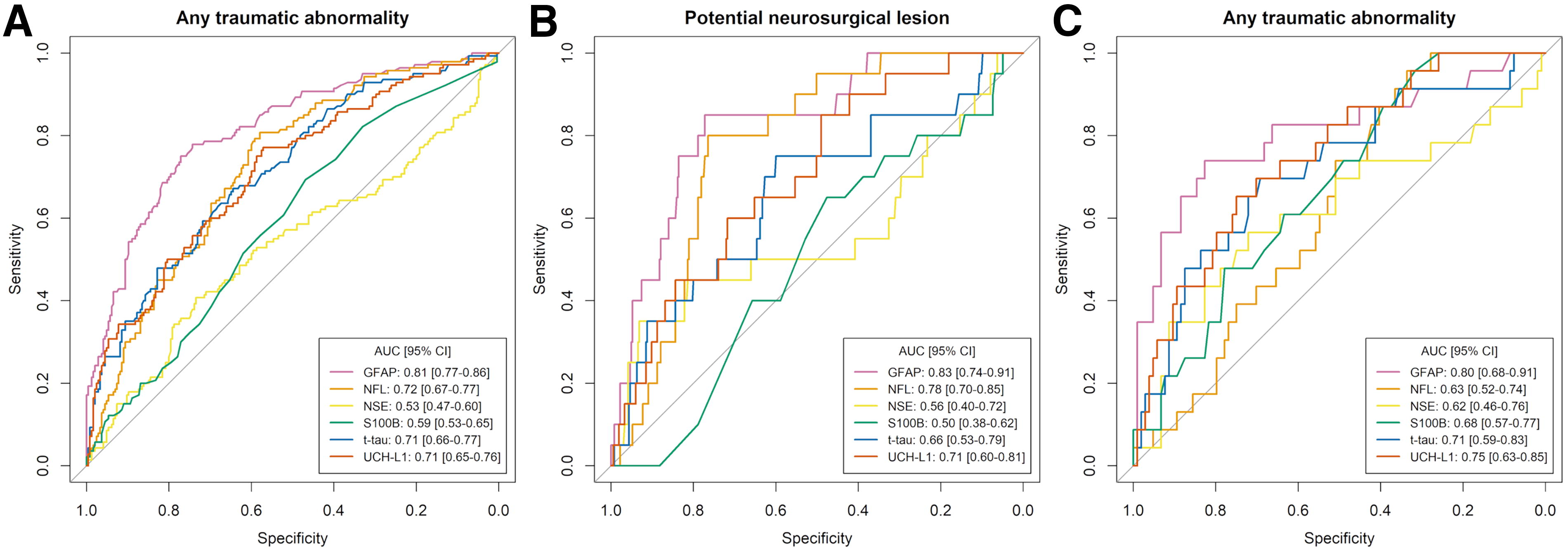
ROC analysis for prediction of CT abnormality in all medium-risk subjects (n = 385) and time to biomarker-limited subgroup (n = 127).
The threshold values for achieving 95% sensitivity in detecting CT abnormalities and 100% sensitivity in detecting potential neurosurgical lesions for each individual biomarker are provided in Table 3. The best-performing biomarkers in the medium-risk sample were GFAP and NFL, followed by UCH-L1 and t-tau. Thresholds of: GFAP 300 pg/mL, NFL 6.57 pg/mL, t-tau 0.78 pg/mL, and UCH-L1 17.87 pg/mL were required to return a 95% sensitivity in detection of CT abnormality, with respective specificities of: GFAP 33% (95% CI: 27–39%), NFL 29% (95% CI: 24–36%), t-tau 21% (95% CI: 16–26%), and UCH-L1 18% (95% CI: 13–24%); and NPVs of: GFAP 92% (95% CI: 86–97%), NFL 91% (95% CI: 85–97%), t-tau 88% (95% CI: 79–95%), and UCH-L1 87% (95% CI: 77–95%). These results corresponded to a potential reduction in the total number of CT scans of: GFAP 23% (95% CI: 18–28%), NFL 21% (95% CI: 16–26%), t-tau 15% (95% CI: 11–20%), and UCH-L1 14% (95% CI: 9–18%), with approximately 7 FN per biomarker (<2% of the total sample). GFAP and NFL were the best-performing biomarkers for identifying potential neurosurgical lesions, with respective specificities at the threshold to return 100% sensitivity of 38% (95% CI: 33–43%) for GFAP and 35% (95% CI: 30–39%) for NFL (threshold values: GFAP 575 pg/mL, NFL 8.1 pg/mL). Additional threshold analyses for each biomarker to return a 100%, 95%, and 90% sensitivity for both any traumatic abnormality and potential neurosurgical lesion are provided in Supplementary Table A8.
Performance at the Threshold Value to Return 95% Sensitivity for Any Traumatic Abnormality, and 100% Sensitivity for Potential Neurosurgical Lesion in the Medium-Risk Subjects
Values and 95% CI calculated from the ROC analysis using bootstrapping with 2000 replicates.
TP, true positive; TN, true negatives; FP, false positive; FN, false negatives; sens, sensitivity; spec, specificity; PPV, positive predictive value; NPV, negative predictive value.
When the sampling window was restricted to 0–6 h, GFAP continued to be the best-performing biomarker, with the ROC curves and AUCs shown in Figure 3C. The performance of both S100B and UCH-L1 improved substantially when the sampling time was restricted to a shorter window from injury, whilst performance of NFL dropped in the shorter sampling time window (Fig. 3, panel C). Thresholds of: GFAP 145 pg/mL, NFL 6.25 pg/mL, S100B 0.095 μg/L, and UCH-L1 31.56 pg/mL all returned a 95% sensitivity, with a corresponding potential reduction of CT scans of: GFAP 16% (95% CI: 9–24%), NFL 28% (95% CI: 20–38%), S100B 27% (95% CI: 19–35%), and UCH-L1 28% (95% CI: 20–37%) (Table 3, Supplementary Table A9).
The sensitivity of S100B at the threshold of 0.1 μg/L when sampled at any time up to 24 h post-injury was 61% (95% CI: 52–69%) with a specificity of 52% (95% CI: 46–59%). However, when sampling was limited to 0–6 h, consistent with current clinical practice, the sensitivity improved to 96% (95% CI 87–100%, with a specificity of 32% (23–40%) and a potential reduction in CT scans performed of 27% (95% CI: 19–35%). Figure 4 illustrates the number of FN when applying the S100B threshold of 0.1 μg/L to the cohort across various times of biomarker sampling (Fig. 4).
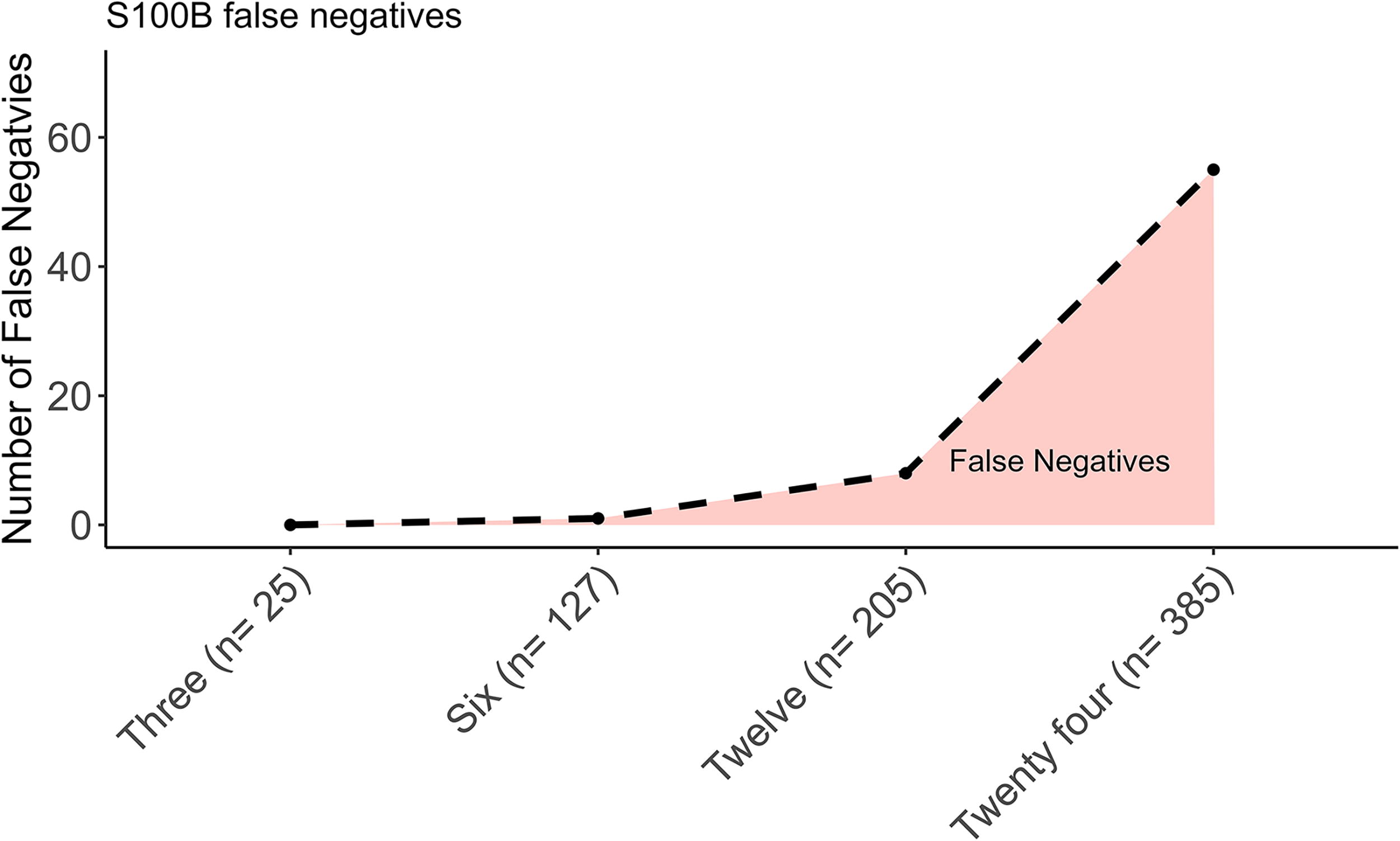
The number of false negatives (positive CT images) when the S100B threshold of 0.1 μg/L was applied to all samples within 3-, 6-, 12-, and 24-h following injury. CT, computed tomography; S100B, S100 calcium-binding protein B.
Intoxicated subjects
A total of 42 subjects had a clinical suspicion of intoxication with drugs (2.4%) or alcohol (97.6%) and a GCS remaining between 13 and 14 in the ED as the only indication for CT imaging. The demographics, imaging findings, and toxicology when available for this cohort are provided in the (Supplementary Tables A10–A11). All biomarker concentrations were significantly higher in intoxicated subjects with CT abnormalities as compared with those without (p < 0.05) (Supplementary Table A12).
Discussion
We investigated the diagnostic utility of day-of-injury serum biomarkers in CENTER-TBI participants classified as medium risk for CT abnormalities in accordance to the “NICE Guideline for Head Injury: Assessment and Early Management [NG232].” 2 Within the medium-risk subjects, GFAP, NFL, t-tau, and UCH-L1 sampled within 24 h post-injury demonstrated moderate to good discrimination for detecting CT abnormalities, with GFAP having the highest overall discrimination. When achieving a sensitivity of 95% for detection of a CT abnormality, the top-performing biomarkers (GFAP, NFL, t-tau, UCH-L1) demonstrated a corresponding specificity ranging between 18% and 33%, potentially reducing unnecessary CT scans by up to 23%. When sampling was restricted to within 6 h of injury, the potential reduction increased, with over a quarter of CT scans potentially avoided in the medium-risk subjects. Overall, our exploratory analysis suggests that targeted biomarker use in patients classified as medium-risk according the NICE NG232 CDR may reduce CT scan requirements following TBI and expedite discharge from the ED. 2
Biomarkers have been shown to be sensitive for the presence of CT pathology on acute imaging, and to improve the performance of prediction models for CT abnormality based upon clinical characteristics alone. 12,18 Blood-based proteomic biomarkers, namely S100B and a combined GFAP/UCH-L1 assay, are in current diagnostic use across multiple clinical guidelines to act as a screen in intermediate risk patients for acute neuroimaging, with the stated aim to reduce unnecessary CT imaging. 11,15 In the United Kingdom, decisions about CT imaging are made in accordance with the NICE NG232 CDR, which classifies head injured patients into three risk categories, and recommends CT imaging in both high and medium-risk patients. However, considering the high rates of CT findings in the high-risk group make imaging essential, and that imaging is already not routinely recommended in low-risk patients, the medium-risk group represent a population where clinical equipoise remains concerning CT requirement. Implementing biomarkers selectively within this medium-risk cohort to as a secondary screening tool for CT imaging would aim to enhance the specificity of existing NICE guidelines, thereby reducing unnecessary CT scans.
In our analysis of the CENTER-TBI core study population, biomarker concentrations scaled to the assigned NICE NG232 risk categories and were higher in medium-risk subjects with clinically significant CT abnormalities as compared with those without. This is consistent with published literature showing biomarker levels reflecting the presence and severity of CT-detected brain injury following trauma. 6,18,25 On ROC curve analysis with sampling any time up to 24 h after injury, GFAP was the best performing biomarker in the medium-risk subjects on ROC curve analysis with sampling any time up to 24 h after injury, with good discriminative performance shown for identification of CT pathology. Thresholding of the ROC curve at a 95% sensitivity demonstrated potential reductions in CT images of up to 23% in the medium-risk subjects when sampled within 24 h, or 28% when sampled within 6 h of injury for the best performing biomarkers. Although this is lower than the 32% reduction in CT images previously shown with the addition of S100B to the SNC TBI guidelines it aligns with the potential 27% reduction observed previously when S100B was assessed in relation to the NICE CT criteria. 6,10
Poor performance was shown by S100B when sampling time was unrestricted up to 24 h following injury. However, S100B has a short half-life with an acute peak following injury. 26 When sampling time was limited to 6 h following injury, in keeping with the SNC TBI guidelines, 11 S100B performance improved substantially with a sensitivity of 96% and a potential CT reduction of 27%. The joint SFMU and SFAR French guidelines currently recommend a shorter sampling window of 3 h for S100B, 15 which may further improve performance. This sampling window was not directly assessed in this analysis due to low subject numbers with biomarkers sampled within 3 h. In a previous analysis of S100B performance in relation to the NICE CT head guidelines, Rogan et al. reported an AUC of 0.73 for S100B sampled within 6 h of injury, slightly higher than the AUC of 0.68 found in our analysis. 6 This difference may be attributed to a mix of high- and medium-risk patients in their study, as well as a shorter time from injury to biomarker sampling (median of 4 h), a factor that would be expected to enhance S100B performance.
Although some patients may be seen acutely following head injury, given potential delays to both ED attendance following injury and time to assessment in ED, many head injured patients are seen by a clinician greater than 6 h after injury. In recent French guidelines the use of S100B is recommended if the patient presents withing 3 h of injury, however, a combination UCH-L1 and GFAP test is recommended to 12 h following injury providing a wider sampling window. 15 This combination approach is largely supported by our analysis. Biomarkers with a shorter half-life (UCH-L1 and S100B) performed well when sampling time was limited, but worse over a longer sampling window. Alternatively, biomarkers with longer half-lives such as GFAP and NFL showed sustained performance when sampled at any time up to 24 h from injury. In future head injury guidelines, alternative biomarkers, or indeed a panel of biomarkers with different temporal courses, may safely extend the time window of biomarker sampling following injury while retaining sensitivity in the acute period following injury.
False Positives, or participants with an elevated biomarker but negative CT images, require consideration. In a prior CENTER-TBI analysis, a greater percentage of CT negative mild TBI participants with an acute biomarker concentration in the highest quintile had impaired functional recovery as compared with those in the lower quintiles. 27 This demonstrates that even if a CT is performed and shows no traumatic abnormalities, a raised biomarker level is of potential clinical importance. Furthermore, in patients with mild TBI without acute findings on CT, an elevated GFAP concentration is associated with increased chance of a structural MRI abnormality, 28 with the level of acute biomarkers suggested to act as a potential screen to select patients who would most benefit from advanced neuroimaging. 29 In relation to our analysis, the so-called FP group would require thoughtful evaluation of the ongoing care plan, whether admission for observation, scheduled outpatient follow-up, or further investigation with alternative imaging modalities such as MRI.
Patients on antithrombotic medication, but without additional risk factors, were classified as medium risk in accordance with the NICE NG232 CDR recommendations for considering CT imaging. 2 It is important to note that there is limited prior literature concerning the use of biomarkers in this population. Patients on antithrombotic medications may have an increased risk of delayed intracranial bleeding, 30,31 or expansion of existing hemorrhage. 32 A small acute bleed, or a delayed bleed, may not lead to a detectable rise in the acute biomarkers, potentially giving a falsely reassuring result. While the risk of expansion or delayed bleed is low, 30,31 this risk should be considered when evaluating the clinical adoption of biomarkers.
We conducted a preplanned subanalysis of patients with suspected intoxication who had a persistent GCS of 13 or 14 as their only high-risk feature based on the NICE NG232 CDR criteria. These patients run the risk of being under triaged with the depressed GCS score attributed wrongly to intoxication, potentially leading to delays to neuroimaging or the initiation of appropriate neuroprotection and neurosurgical procedures. Although limited by the small sample size, our analysis found high rates of traumatic injury on CT in the intoxicated subset, with significantly elevated biomarker levels in subjects who had intracranial pathology on imaging. This aligns with a prior study on the TRACK-TBI cohort, which reported that approximately 50% of individuals with an elevated blood alcohol level (BAL) had a positive brain CT and that an elevated BAL did not affect the diagnostic accuracy of UCH-L1 and GFAP. 33 Overall, these results support the current imaging advice that all that all patients with a persistently depressed GCS, irrespective of intoxication, are a high-risk patient population requiring urgent neuroimaging. Additionally, the results suggest a potential role for biomarkers in guiding decision making concerning the urgency of imaging and the extent of acute clinical interventions. Managing intoxicated patients in the ED can be challenging, with sedation or other methods commonly required to facilitate neuroimaging. It may be possible, in those with normal biomarker levels, to delay imaging until the intoxication subsides and GCS improves, potentially avoiding unnecessary sedation and improving compliance with the procedure. However, the results in this analysis are from a small retrospectively identified cohort, and therefore should be interpreted cautiously, with larger and more representative prospective studies needed to further assess this hypothesis.
Limitations
An important consideration in the interpretation of this analysis is the requirement of a CT head for inclusion to CENTER-TBI. The cohort studied, therefore, may not be representative of the overall head injured population presenting to the ED, being more severely injured with more frequent CT abnormalities. For example, even in those classified as low risk, over 10% of subjects had traumatic CT findings (Supplementary Table A3). This selection bias reduces the comparability of this analysis to some previous studies 6 and is an important limitation when considering the translatability of our findings to the clinical head injured population where the NG232 CDR has a lower FN rate. 5,34 In a more representative sample used in a prior analysis, the addition of S100B was shown to potentially reduce the number of CT head scans performed by 27%, similar to that shown in our analysis. 6 In general, if the prevalence of CT findings decreases and a given level of sensitivity is achieved, the number of TN increases relative to the number of FP, leading to an increase in NPV and likely cost-effectiveness. Although the ROC AUC value is typically considered independent of prevalence, 35 this assumes the sample population is fully representative, which may not be the case in our sample and may enhance biomarker performance in this analysis as compared with real-world practice.
For clinical use, biomarker levels would need to be assessed prior to decisions about CT imaging. Although our analysis included a time-limited assessment for biomarkers sampled up to 6 h post injury, the absence of samples from a narrower time window, such as within the first 3 h, restricts our ability to fully evaluate biomarker performance in a timeframe more reflective of the clinical environment. The discrepancy between clinical practice and the study’s sampling timeline may impact the applicability of our findings. Specifically, biomarkers such as UCH-L1 and S100B have a relatively short half-life. Consequently, their diagnostic value may be better when sampled closer to the injury, while the performance of other biomarkers with a longer half-life, such as NFL, may worsen. Although the time-frame patients are seen by a clinician following injury can vary greatly, the timing of biomarker sampling in this analysis is unlikely to truly reflect clinical practice due to many samples being taken after the CT scan. Further prospective study with biomarker sampling prior to clinical decision making is required to assess biomarker performance in a clinical environment.
In this analysis, we retrospectively identified NICE NG232 CDR risk categories for CT imaging using prospectively recorded clinical variables from the CENTER-TBI study. The variables were not collected prospectively at the time of clinical assessment from the physicians assessing the patient. Therefore, the data will not fully reflect the clinical decision making of the physician in these patients, or the presence or absence of the clinical variables as determined by the physician at the time of clinical assessment. Although the NICE head injury guideline criteria were mapped as closely as possible to CENTER-TBI variables, the variables were not specific for those criteria and were instead the closest approximation available and therefore risks misclassification. For example, for the high-risk criterion concerning the GCS score at 2 h following assessment in ED, a positive recording was either the risk factor for CT imaging being provided as a GCS score of 14 or below, or the post-stabilization GCS, which was a centrally imputed GCS score using the IMPACT methodology. 36 A single criterion (clinical suspicion of depressed skull fracture) did not have a corresponding value in the CENTER-TBI dataset that could be reliably known to have been recorded without influence of the CT findings. A sensitivity analysis was performed excluding patients (n = 2) with a depressed skull fracture later reported on CT, with no effect on the results of the primary analysis. Although a source data verification process was conducted in the CENTER-TBI study, data were not extracted in duplicate with no formal assessment of inter-rater reliability to ensure consistency between different data extractors.
Sample size is a limitation, notably in the time-limited subanalysis and the intoxicated subanalysis. Missing data is common in TBI research, 37 with most subjects in this analysis excluded due to missing neuroimaging or biomarker data, which may introduce bias. Furthermore, 166 patients were excluded because of missing clinical variables that were used to assign to a NICE guideline risk, further introducing a potential selection bias.
We should not over interpret the suggested biomarker thresholds from this analysis. Thresholds were calculated to return a set sensitivity, and clinically thresholds will differ depending on sampling time window used. Future work should follow clinical considerations to define a plausible range of thresholds: How many CT scans are we willing to make per lesion detected? In other words, what ratio of saved CT scans to missed lesions is acceptable? In other diagnostic decision rules, a very high sensitivity was usually postulated. 3 Requiring a high sensitivity implies that we set infinite costs to missing a lesion. For this analysis we considered a sensitivity of 95% for detection of CT abnormality, and 100% for a potential neurosurgical lesion.
Threshold values for biomarkers in this analysis are higher when compared with those commonly reported in previous literature, likely due to differences in assay platforms used for biomarker analysis. 12 Biomarker concentrations vary by assay platform, 38 leading to discrepancies in reported cut-off values. While values may correlate across platforms, cut-offs should not be directly compared. In the CENTER-TBI study, GFAP, NFL, t-tau, and UCH-L1 were analyzed using RUO assays, whereas S100B and NSE were measured on clinically approved platforms. Among the biomarkers assessed, only S100B was measured on a clinically approved platform with an established cut-off value currently used to determine the need for CT imaging following TBI. Consequently, the evaluation of biomarker performance at clinically validated thresholds was limited to S100B with other the other biomarker thresholds not validated outside of this analysis. Further research is required to develop standardized thresholds for biomarkers across different analytical platforms.
Conclusion
The use of serum biomarkers to determine the requirement for acute CT imaging may potentially reduce the number of unnecessary CT images performed in patients classified as medium-risk according to the 2023 NICE head injury guidelines (NG232) CDR. GFAP demonstrated the greatest discrimination overall. Further prospective studies are needed to establish safe biomarker thresholds across different assay platforms, and to evaluate the efficacy and cost-effectiveness of the incorporation of biomarker sampling within the NICE head injury guidelines.
Transparency, Rigor, and Reproducibility
This study is a secondary analysis of the CENTER-TBI core study (registration number: NCT02210221; https://clinicaltrials.gov). The analysis plan was approved by the CENTER-TBI Management Committee following data collection at https://www.center-tbi.eu/data/approved-proposals. Sample size and power calculations were not conducted, with the sample size based upon the number of patients in the CENTER-TBI dataset meeting the inclusion criteria. Of the 4509 subjects in the CENTER-TBI core study, 2530 were excluded and 1979 were included in this analysis, with a detailed description in the methodology for the reasons for exclusion (Fig. 1). Participants were blinded to biomarker results throughout the study. Team members handling and analyzing the biomarkers were blinded to participant characteristics. Team members reporting the CT images were blinded to clinical information except for gender, age and care path stratum. All equipment and analytical reagent are available from Roche Diagnostics, Mannheim, Germany and Quanterix Corp., Lexington, MA. Patients missing biomarker, imaging or key clinical data to facilitate classification as per the NICE NG232 CDR were removed as reported in the text. Confidence intervals have been reported in the abstract for primary outcome where provided, and main text or Supplementary Appendix for all outcomes. Correction for multiple comparisons was performed using the Benjamini-Hochberg method. Deidentified CENTER-TBI data is available to researchers who provide a study proposal for review and approval by the Management Committee (submitted online at: https://www.center-tbi.eu/data). Access and use of CENTER-TBI data requires adherence to the CENTER-TBI Data Use Agreement and harmonized procedures for data access requests.
Footnotes
Authors’ Contributions
D.W.: Conceptualization, methodology, formal analysis, investigation, resources, writing—original draft, writing—review and editing, and visualization. A. Mikolić: Methodology, writing—original draft, and writing—review and editing. E.C.: Investigation and resources. S.R.: Conceptualization, methodology, writing—original draft, writing—review and editing, and visualization. A.B.: Investigation, resources, data curation, writing—review and editing, visualization, supervision, project administration, and funding acquisition. K.K.W.: Investigation, resources, data curation, writing—review and editing, project administration, and funding acquisition. E.S.: Methodology, writing—review and editing, visualization, supervision, project administration, and funding acquisition. A. Maas: Conceptualization, methodology, investigation, resources, data curation, writing—review and editing, supervision, project administration, and funding acquisition. D.M.: Conceptualization, methodology, investigation, resources, data curation, writing—review and editing, supervision, project administration, and funding acquisition. F.L.: Conceptualization, methodology, writing—original draft, writing—review and editing, supervision, project administration, and funding acquisition. V.N.: Conceptualization, methodology, investigation, resources, writing—original draft, writing—review and editing, supervision, and project administration.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the National Institute for Health Research (NIHR), Rosetrees Trust, or the Department of Health and Social Care.
Author Disclosure Statement
D.M. reports grants, personal fees, and nonfinancial support from GlaxoSmithKline; personal fees from Neurotrauma Sciences, Lantmannen, Pressura, and Pfizer, outside of the submitted work. E.S. receives royalties from Springer during the conduct of this study. A. Maas declares consulting fees from PresSura Neuro, Integra Life Sciences, and NeuroTrauma Sciences. F.L. was Topic Advisor for the NICE head injury: assessment and early management guideline. V.N. holds investigator led grants with ROCHE Pharmaceuticals and Abbott. V.N. was a member of the Update Committee for the NICE head injury: assessment and early management guideline and represented the Royal College of Emergency Medicine to review the UK Concussion Guidelines for Grassroots Sport.
Funding Information
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article. The CENTER-TBI study was supported by the European Union 7th Framework Program (EC grant 602150), with additional funding from Hannelore Kohl Stiftung (Germany), OneMind (USA) and Integra LifeSciences Corporation (USA), and NeuroTrauma Sciences (USA). No individual funding was sort for this analysis. This work was supported by researchers at the NIHR Cambridge Biomedical Research Centre. D.W. is funded by the Royal College of Emergency Medicine doctoral research fellowship. V.N., NIHR Rosetrees Trust Advanced Fellowship, NIHR302544, is funded in partnership by the NIHR and Rosetrees Trust.
Supplementary Material
Supplementary Data
Supplementary Appendix
Supplementary Figure A1
Supplementary Figure A2
Supplementary Figure A3
Supplementary Table A1
Supplementary Table A2
Supplementary Table A3
Supplementary Table A4
Supplementary Table A5
Supplementary Table A6
Supplementary Table A7
Supplementary Table A8
Supplementary Table A9
Supplementary Table A10
Supplementary Table A11
Supplementary Table A12
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.