
Abstract
Early activity-based therapy (E-ABT) has the potential to decrease complications and radically improve neurofunctional recovery following traumatic spinal cord injury (TSCI). Unfortunately, E-ABT after TSCI has never been attempted in humans due to practical obstacles and potential safety concerns. This study aims to report on the safety and feasibility outcomes of the Protocol for Rapid Onset of Mobilization in Patients with Traumatic SCI (PROMPT-SCI) trial: the first-ever trial of E-ABT in critically ill patients who suffered a severe TSCI. To do so, 45 patients with severe TSCI were recruited to participate in the PROMPT-SCI trial between April 2021 and August 2023. The intervention consisted of daily 30-min sessions of motor-assisted in-bed leg cycling for 14 days, starting within 48 h of early surgery (≈72 h from the initial trauma). Adverse events were closely monitored, and completion rates were evaluated. Out of the 45 participants, 36 (80%) completed a full and safe session within 48 h of surgery and all participants managed to achieve this outcome within 72 h of surgery. Over the full 14-day protocol, the average completion rate of sessions was 87.2 ± 22.7% (range: 7.1–100.0%). A total of three patients were mechanically ventilated during the protocol and all three had 100% completion of sessions. Frequent reasons for unattempted/incomplete sessions were scheduling conflicts with activities related to care (e.g., bronchoscopy) and fatigue/uncontrolled pain before initiating cycling. We also report no neurological deterioration caused by cycling and no major adverse event recorded during or between sessions. In conclusion, this study suggests that E-ABT can be safely initiated within 48–72 h after a severe TSCI with no major adverse event. In the form of daily passive in-bed leg cycling, E-ABT is also acceptable for target users, and feasible over the course of the first weeks after the initial trauma, as shown by our excellent rate of completed sessions (87%). The present results also suggest that improved collaboration with intensive care unit staff, including intensivists and nurses, could improve these rates even further.
Introduction
There is growing evidence that early activity-based therapy (E-ABT) in critically ill patients can improve the course of care, decrease complications, and accelerate recovery in a wide variety of patient subgroups. 1,2 Unfortunately, E-ABT has never been attempted in patients with severe traumatic spinal cord injury (TSCI) due to practical obstacles (paralysis, associated injuries) and potential safety concerns related to their medical acuteness. 3,4 However, out of all intensive care unit (ICU) patients, individuals with acute TSCI represent a subgroup that could potentially benefit the most from such interventions, notably due to their inherent paralysis, which places them at an exceptionally high risk of immobility-associated complications. In addition, there is also growing evidence from the pre-clinical literature that supports the use of E-ABT after TSCI to improve neuroplasticity and neurofunctional recovery. 5,6
In this context, our team designed the Protocol for Rapid Onset of Mobilization in Patients with Traumatic SCI (PROMPT-SCI), the first-ever trial (NCT04699474; registration date: 2021–01-07) of E-ABT in humans, with a strong potential to drastically improve the short and long-term outcomes of patients with TSCI. Specifically, the objectives of this pilot trial were to evaluate the safety, feasibility, and clinical benefits of E-ABT during acute hospitalization.
7
The E-ABT intervention consisted of 14 continuous days of early in-bed leg cycling (EBC) starting within 48 h of the early decompressive surgery. In preliminary work based on the first 15 trial participants, we have shown that initiating the first session of EBC within this timeframe was safe and feasible. This report aims to discuss the final results of all safety and feasibility end-points. With respect to both these end-points, our main hypotheses were: There will be no serious adverse events associated with EBC (safety). At least 90% of participants will achieve a full and safe session of EBC within 48 h of the early decompressive surgery (feasibility). At least 80% of participants will complete ≥ 11 of the 14 planned EBC sessions (feasibility).
Methods
Study participants
Forty-five adult patients were recruited from a single Level 1 trauma center in Montreal, Canada (Hôpital du Sacré-Coeur de Montréal) between April 2021 and August 2023. To be included in the trial, patients were required to meet the following criteria: (1) severe TSCI (i.e., American Spinal Injury Association Impairment Scale (AIS) grade A, B, or C); (2) neurological level of injury (NLI) between C0 and L1; (3) blunt (nonpenetrating) trauma; and (4) spinal decompression surgery performed ≤ 48 h of the injury (Table 1A). AIS grade and NLI were both determined from the pre-operative neurological examination performed according to the principles of the International Standards for the Neurological Classification of Spinal Cord Injuries (ISNCSCI). 8 Patients were excluded if they presented one of the following criteria: (1) a condition limiting patient’s ability to engage in cycling (e.g., pelvis or lower extremity injury or deformity); (2) medical contraindication to cycling, as determined by the caring team (attending intensive care physician and/or spine surgeon); (3) presence of moderate or severe traumatic brain injury; (4) unwillingness or inability to comply with follow-up schedule; (5) pre-existing medical condition impairing walking ability (including, but not limited to prior neurological diseases such as cerebrovascular disease, myasthenia gravis, and spinal cord injury; Table 1B). All patients provided informed written consent before enrollment. This study was approved by the Comité d’Éthique de la recherche du CIUSSS du Nord-de-L’Île de Montréal (“Mobilisation précoce suite à une lésion médullaire,” study #2020–1901, approved on March 12, 2020) and was conducted in accordance with the principles of the Declaration of Helsinki.
Inclusion, Exclusion, Daily Exemption, and Stopping Criteria
MRI, magnetic resonance imaging; SCI, spinal cord injury; SpO2, blood oxygen saturation.
The sample size calculation was based on the detection of the impact of the intervention on certain long-term neurofunctional outcomes, which will be discussed in a subsequent article that is currently in preparation. Specifics on sample size calculation are extensively described in the study protocol. 7
Standard of care
All recruited participants received the usual standard of care for TSCI patients. In our institution, all TSCI patients are managed by a specialized neurotrauma team composed of spine surgeons, acute care physiatrists, intensive care physicians, and paramedical staff (physical therapists, occupational therapists). Shortly after admission and initial medical stabilization, a priority is set on performing early decompressive spinal surgery in order to minimize the secondary injury. 9,10 After surgery, patients with severe TSCI are transferred to the ICU for monitoring and maintenance of mean arterial pressure (MAP) ≥ 85 mmHg for 1 week, using vasopressors if needed. During their stay in the hospital, physiotherapy is administered six times/week with a focus on passive range of motion exercises, resistance training, and balance training. Occupational therapy sessions are also delivered 2–3 times/week, along with other paramedical interventions on an as-needed basis. 11 Average length of stay in our institution is around 25 days before transfer to a specialized inpatient rehabilitation facility.
Intervention
The intervention consisted of daily 30-min sessions of continuous in-bed leg cycling for 14 consecutive days, starting within 48 h of spinal surgery, as soon as patients were deemed medically/hemodynamically stable. Prior to every session, participants were screened to assess their fitness to engage in cycling and ensure that there was no medical contraindication to cycling (Table 1C). During sessions, patients engaged in cycling at a target cadence of 40 revolutions per minute, which replicates a low-normal step frequency. 12 The ergometer used to perform cycling sessions was the APT-5 ergometer from Tzora Active Systems (Tzora Active Systems, Ohio, USA). Depending on their motor strength and tolerance, patients achieved this cadence without motor assistance from the ergometer (active cycling), limited assistance (active-assisted cycling), or total assistance (passive cycling). Patients with residual motor strength in the lower limbs were always encouraged to contribute as much as possible to the cycling motion and the motor output from the ergometer was titrated accordingly to reach the target cadence. During cycling, MAP, heart rate (HR), respiratory rate (RR), and blood oxygen saturation (SpO2) were closely monitored by a research assistant with medical training who remained at the bedside during sessions. Adverse events were systematically noted and reported to the principal investigator. Sessions were stopped if patients or their caring team requested termination if vital signs fluctuated outside of the following ranges in a sustained fashion: MAP: 60–110 mmHg; HR: 40–140 bpm; SpO2: ≥90%, or if there were signs of medical instability (Table 1D). After each session, the neurological status of patients was assessed to ensure neurological safety. All neurological exams were conducted in accordance with the ISNCSCI. 8
Primary outcomes
As noted above, the safety of the intervention was evaluated based on the vital signs observed during sessions, daily neurological status, and occurrence of adverse events. The two main feasibility end-points were: (a) success/failure to complete safe and full cycling session within 48 h of early decompression surgery and (b) number of safe and full sessions completed during the planned 14-day protocol. Reasons for missed or interrupted sessions were also analyzed.
Statistical analysis
Descriptive statistics were used to characterize the study cohort and report the above-mentioned outcomes. All statistics were performed using SPSS v. 27 (IBM, Chicago, IL).
Results
Between April 2021 and August 2023, 106 adult patients presented at our center with an acute severe TSCI that comprised an NLI between C0 and L2. Of these, one had a penetrating lesion, three had a complete transection of the spinal cord (in the context of severe spinal fracture-dislocation), and 15 were operated on more than 48 h of the initial trauma and were thus not considered for this study. An additional four patients were not included because obtaining a proper physical examination was not possible due to intubation and sedation or altered consciousness. Out of the remaining 83 patients who were eligible for the project, 35 were excluded due to exclusion criteria. The most frequent reasons for exclusion were lower limb fracture (n = 11) and medical instability as defined by the care team (n = 6). Out of the 48 remaining patients, only three did not agree to be enrolled in the study (consent rate of 94%). A flowchart describing the patient selection and recruitment process is available in Figure 1.
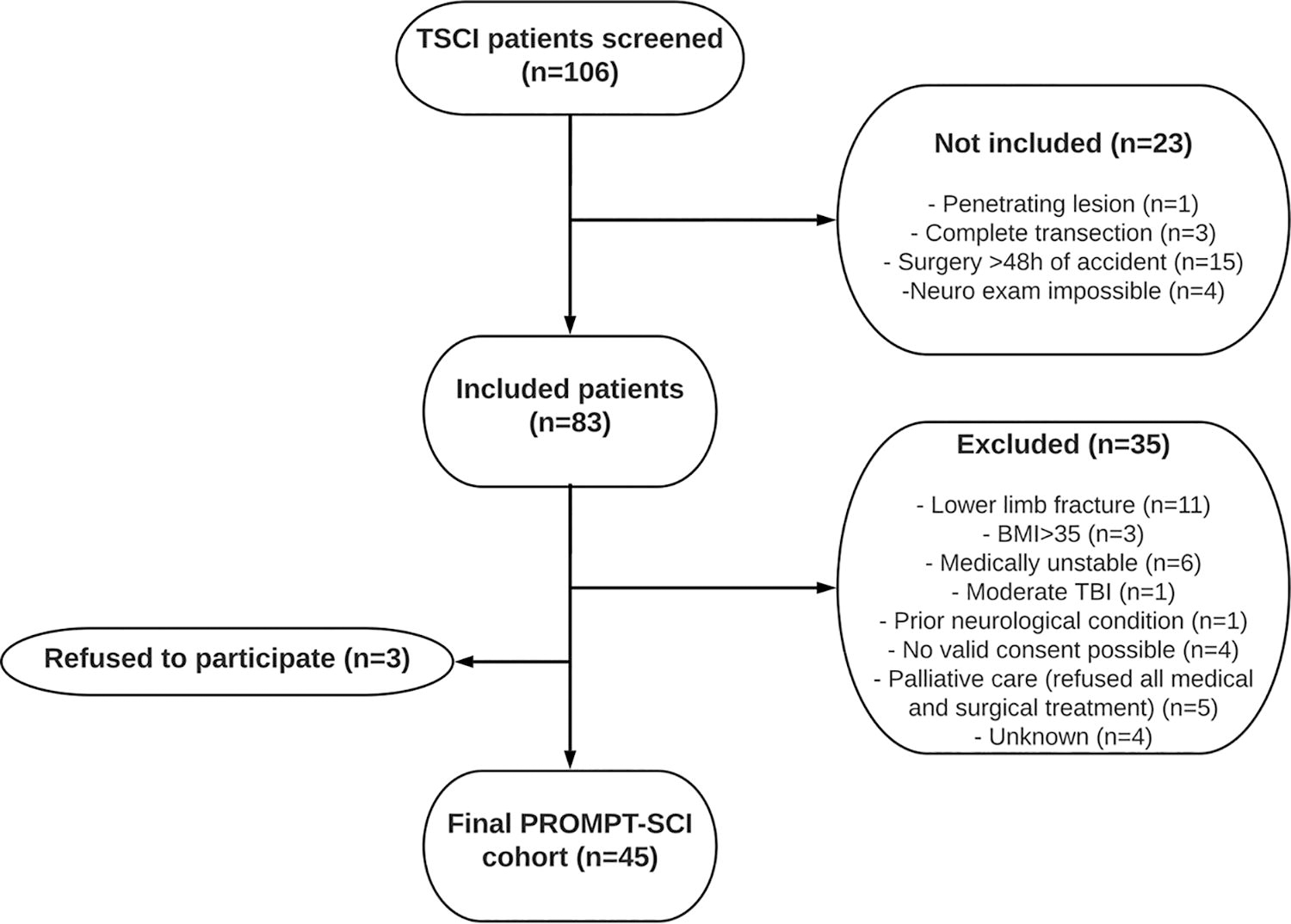
Flowchart.
The final PROMPT-SCI cohort comprised 40 (88.9%) males and 5 (11.1%) females. The mean age at injury was 53.1 ± 18.4 years. A total of 27 participants (60.0%) were AIS grade A, 9 (20.0%) were AIS grade B, and 9 (20.0%) were AIS grade C. The majority of participants (57.8%) also presented an NLI between C1 and C8. In addition, three patients were mechanically ventilated at the time of their recruitment for the project. A complete description of the final cohort is presented in Table 2.
Baseline Characteristics of the 45 Final Patients Constituting the PROMPT-SCI Cohort
Body mass index.
Charlson comorbidity index.
American Spinal Injury Association Impairment Scale.
Neurological level of injury.
Out of the 45 final participants, 36 (80.0%) completed a full and safe session within 48 h of surgery. Out of the nine who did not achieve this outcome, six did not initiate a session by this time-point (two due to scheduling conflicts with activities related to care—emergency bronchoscopy for secretion management and tracheotomy, two due to medical contraindications, two due to patient refusal in the context of pain and fatigue), and three initiated a session but it was stopped prematurely (two due to pre-existing back and abdominal pain that persisted with cycling and one due to prolonged SpO2 < 89% that resolved quickly after stopping cycling). In addition, 38 of the 45 participants completed at least 11 out of the 14 possible sessions—corresponding to ≈80% completion rate—and 24 (53.3%) had a 100% completion rate. At the group level, the average completion rate observed was 87.2 ± 22.7% (range: 7.1–100.0%).
The vast majority of incomplete sessions were sessions that were not attempted (83.5%) rather than interrupted prematurely due to stopping criteria (16.5%). Reasons for not attempting sessions were the following: medical contraindication to cycling (n = 30), pressure ulcer on the sacrum (n = 8), scheduling conflicts with activities related to care (n = 6, of which five were an emergency bronchoscopy for secretion management in patients with high cervical lesions/mechanical ventilation), patient refusal due to fatigue or uncontrolled pain (n = 18), and unknown (n = 8). Reasons for premature termination of cycling sessions were the following: pre-existing back or abdominal pain that persisted with cycling (n = 7), patient fatigue (n = 2), scheduling conflicts with activities related to care (patients had to leave their room for a scheduled appointment with another medical specialty in the hospital; n = 2), muscle spasms precluding smooth pedaling motion (n = 1), and SpO2 < 89% during cycling (n = 2). Both patients with SpO2 decreases during sessions had normal SpO2 before starting (98% and 93%). Both unattempted and prematurely stopped sessions were distributed homogeneously across the 14 days of the protocol. Missed or incomplete sessions were more frequent in the ICU than in the wards (the rate of missed or incomplete sessions was 16% vs. 5%, respectively).
Out of our 45 participants, 3 required mechanical ventilation during the study protocol. Of these, one managed their first full and safe sessions within 24 h of the surgery and the remaining two did so within 72 h of the surgery. All three completed all 14 sessions safely and fully thereafter. The first was intubated for the first six sessions and then had a tracheostomy for the remaining eight sessions, the second was intubated for the first four sessions and then had a tracheostomy for the remaining 10 sessions, and the third had a tracheostomy from the start for all 14 sessions.
Excluding the above-mentioned adverse events that led to the premature termination of cycling sessions (including two recorded episodes of hypoxia), there were no other notable adverse events due to cycling. However, out of the complete study cohort, two patients presented a post-operative neurological deterioration that was deemed unrelated to the intervention by the external members of the Data and Safety Monitoring Board (DSMB). The first patient was a 24-year-old female with a complete injury (AIS grade A) and NLI of T2. She performed four cycling sessions before increased motor deficits were observed by the care team. A control magnetic resonance imaging (MRI) study showed stigmata of subacute post-traumatic ascending myelopathy. The second patient was a 65-year-old male, also with a complete injury and NLI of T12. He performed his first cycling session successfully 24 h after his surgery. He complained of increased motor deficits around 24 h later. In his case, the control MRI showed a compressive epidural hematoma in addition to incomplete spinal decompression at the site of injury. A revision surgery was performed, and the patient improved thereafter.
In addition, one patient died during the cycling protocol. He was a 61-year-old male with AIS grade A and NLI of C4. He completed six full and safe sessions of cycling while in the ICU with the two first sessions while he was intubated. During the course of the following week, several attempts had been made to extubate the patient, but he systematically required re-intubation. During the last attempts, while briefly extubated, he clearly and repeatedly expressed his desire to stop all life support. His immediate family supported his decision. In this context, a meeting with the responsible attending physician from the ICU was organized and the situation was revaluated with the family present. A conjoined decision was made to respect the patient’s wishes and all life support was ceased on day 14 of the protocol (16 days post-surgery). His neurological status remained stable over the course of his participation in the study.
Discussion
The PROMPT-SCI trial is the first-ever attempt at performing E-ABT following TSCI in humans. Based on the results from the 45 included participants, this study suggests that initiating E-ABT within 3–4 days of the injury and performing daily sessions during the first weeks of acute hospitalization is both safe and feasible.
Before the PROMPT-SCI trial, the most important barrier that had precluded the implementation of E-ABT in human TSCI patients was theoretical concerns for neurological safety. As discussed above, these concerns were largely attributable to one landmark article by Smith et al. published in 2008. 3 In their study, contusive TSCI rat models were exposed to several bouts of swimming daily starting on post-injury day 3. At the group level, the experimental group had worse Basso–Beattie–Bresnahan scores 4–6 weeks following the injury when compared with the control group that was not exposed to swim training. 13 After histological analysis of the spinal cord specimens from their study, they observed that rats from the intervention group had significant extravasation of blood and pro-inflammatory macromolecules and increased tissue edema at the level of the lesion. Based on these findings, it was hypothesized that the physiological demands associated with swimming excessively increased the perfusion pressure of the spinal cord at a site where the blood–spinal cord barrier was impaired, leading to these poorer outcomes. 14,15 As a result, passive or passive-assisted in-bed leg cycling was the preferred E-ABT modality in the PROMPT-SCI trial, as several studies have shown that it represents a low-intensity form of mobilization that results in little to no change in hemodynamic parameters, even in critically ill and traumatized patients. 16 Since no neurological deterioration was observed in relation to the intervention, this study strongly supports the innocuity of E-ABT interventions when they are performed using low-intensity modalities.
Nonetheless, the authors recognize the occurrence of two neurological deteriorations in the study cohort. However, as stated above, these neurological deteriorations were deemed unrelated to the cycling intervention by the DSMB. Indeed, in both these patients, the sessions performed prior to the neurological deterioration were all passive cycling, and there was no significant increase in MAP or HR during pedaling time that could attest to excessive physiological demands and/or major increases in spinal cord perfusion pressure. In addition, the rates of neurological deterioration observed in this cohort (4.4%) are well within the rates that are considered normal for this population of patients, further supporting the innocuity of the intervention in terms of neurological safety. 17
However, in order to improve safety even further in future studies, the authors stress that additional research will have to clarify the boundaries of MAP that are acceptable for the spinal cord in this vulnerable stage. Indeed, in this study, the range of acceptable MAP during sessions was pre-set at 60–110 mmHg. Based on the neurological safety profile of the proposed intervention that was observed in this study, our findings seem to support this empirical range as a “safe zone” of MAP fluctuations. This is also in line with the most recent research on this matter, 18 although it remains highly debated in current guidelines of MAP management after TSCI. 19,20
Finally, with respect to the safety end-points, we also observed one isolated instance of prolonged blood oxygen desaturation < 89% that required premature termination of a session for two of the 45 participants. In both, cases, the SpO2 quickly normalized when appropriate oxygen supplementation was provided. After careful chart review, no serious aetiologies (such as pulmonary embolism) were identified. In addition, both patients had received opiates almost immediately before initiating their cycling session, such that these events most likely resulted from central hypoventilation exacerbated by peripheral hypoventilation due to upper airway atelectasis (especially in the semirecumbent position adopted during sessions). However, irrespective of the relation of these adverse events to the EBC intervention, their occurrence highlights the importance of adequate monitoring of vital signs and close collaboration with care teams during any attempt at performing E-ABT in severe TSCI patients, as they still represent a vulnerable group of critically ill patients.
With respect to the feasibility end-points, we observed excellent overall completion rates. Confirming our preliminary results based on the first 15 PROMPT-SCI participants, we also report that initiating cycling within the first 72 h of surgery (translating to the first 4–5 days after the initial trauma) is feasible in 100% of cases despite severe injuries and intensive care (including ventilator support in some participants). 21 Our completion rates of the EBC protocol are also comparable to those reported in studies on activity-based therapy in critically ill patients, which directly challenges the perceptions of acute care therapists, who previously raised doubts regarding the feasibility of structured E-ABT programs in TSCI patients due to their “medical acuteness.” 4,22 In addition, although session completion rates were slightly lower for sessions that were attempted in the ICU as opposed to the wards (84% vs. 95%), we still achieved our target completion rate of >80% of sessions even in this more challenging setting. With the 100% session completion rates of our three participants who were mechanically ventilated during the cycling protocol, our results also support the inclusion of intubated and tracheostomized patients in E-ABT interventions, as long as their state of arousal allows proper neurological examinations before and after sessions.
Based on our results and experience, several recommendations for implementing E-ABT in acute TSCI patients can be made from this study. For example, although we already observed strong completion rates, these could potentially be improved further by ensuring close collaboration with care teams in charge of patient schedules and implicating patients more in the organization of their activities. This is directly supported by our results, since for the first 15 patients of the trial, the completion rate of sessions in the ICU was only 67%, which we managed to raise up to 88% for the last 30 patients, after introducing daily early morning meetings with nursing staff from the ICU to determine the optimal timing of cycling sessions. In addition, the authors highlight the importance of optimizing pain control prior to and after E-ABT sessions, which could also decrease the number of unattempted sessions by 25%. Specifically, we recommend that analgesia should be timed to maximize pain control during the session while minimizing the risk of excessive drowsiness and sedation during sessions (which has resulted in SpO2 decreases in two instances in our cohort). In practice, depending on the specific types of medications used and on clinical judgment, this could mean modulating the pharmacological schedule to plan for the administration of an interdose 30 min to 1 h before initiating cycling, as it is suggested for the prevention of pain induced by exercise and mobilization (PIEM). 23 Also, since patient fatigue was a frequent barrier to attempting and completing sessions, the use of a scale to measure fatigue before sessions and modulate the session parameters accordingly (session duration, level of motor assistance) could be envisaged. 24
Finally, in accordance with the existing—albeit limited—literature on E-ABT, we observed excellent acceptability of the intervention among target users with a consent rate of 94% and favorable participant response to sessions. Previous surveys among patients with SCI had already identified a desire of this population to receive E-ABT as early as possible in the continuum of care, with patients reporting perceived benefits for neurological recovery, general physical health, and mental health, although they had not been exposed to structured E-ABT protocols. 25
This study has several methodological strengths. However, the authors recognize that there are also some limitations. First, although the safety and feasibility of E-ABT were well evaluated through completion rates and adherence levels to the protocol, the impact of the intervention on various acute and long-term patient outcomes was not discussed. However, this was not the scope of this study, and future work, which is currently in preparation, will evaluate the potential benefits of E-ABT on complication rates and neurofunctional recovery. In addition, the authors recognize that the acceptability of the intervention among target users (patients but also medical and paramedical staff, including nurses, physical therapists, and occupational therapists), will have to be evaluated formally in future studies. Since previously cited studies showed that acute care therapists were unconvinced of the feasibility of structured E-ABT in TSCI patients, evaluating their response to the presented results will be crucial for the eventual integration of E-ABT in care.
Conclusion
In conclusion, the PROMPT-SCI trial is the first-ever trial of E-ABT in critically ill patients who suffered a severe TSCI. Based on the results from the final 45 study participants, we conclude that E-ABT in the form of daily passive or passive-assisted in-bed leg cycling is both safe and feasible in this patient population. Future work is required to formally evaluate acceptability among target users including acute care therapists and investigate the potential benefits of such interventions.
Transparency, Rigor, and Reproducibility Statement
The study design and analytic plan were pre-registered in ClinicalTrials.gov (NCT04699474; registration date: 01-07-2021). The sample size of 45 was calculated for outcomes other than those that are discussed in the present article. Sampling was made to ensure the minimum of 36 patients with complete follow-up to detect a significant increase in the ability to walk independently at 6 months, as compared with a retrospective matched control cohort, based on a one-tail McNemar test with a level of significance of 0.05. All patients provided informed written consent before enrollment. This study was approved by the Comité d’Éthique de la recherche du CIUSSS du Nord-de-L’Île de Montréal (“Mobilisation précoce suite à une lésion médullaire”, study #2020–1901, approved on March 12, 2020) and was conducted in accordance with the principles of the Declaration of Helsinki. The datasets that were generated during the course of this research are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors thank the research personnel at the Laboratoire d’Orthopédie-Colonne de l’Hôpital du Sacré-Coeur de Montréal for their contribution to this project. The authors also thank the study participants, without whom this research would not have been possible.
Authors’ Contributions
A.D.: Design of the work, data acquisition, analysis interpretation of data, drafting the work, critical revision, final approval, and agree to be accountable for all aspects of the work. D.M. and A.R.D.: Design of the work, analysis interpretation of data, critical revision, final approval, and agree to be accountable for all aspects of the work. Y.P., D.B., and F.B.: Design of the work, critical revision, final approval, and agree to be accountable for all aspects of the work. J.M.M.T.: Design of the work, analysis interpretation of data, critical revision, supervision, final approval, and agree to be accountable for all aspects of the work.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research was funded by the Craig H. Neilsen Foundation (grant number: 649997).