
Abstract
Our recent improved understanding of traumatic brain injury (TBI) comes largely from cohort studies of TBI patients with indication for computed tomography (CT). Using CT head as an inclusion criterion may overestimate poor outcomes after TBI with Glasgow Coma Scale (GCS) 13–15. We aimed to compare outcomes after TBI in adults who had a head CT scan (with negative findings) versus those who had no CT when presenting to an emergency department. This was a secondary analysis of a trial that recruited adults with GCS = 13–15 after TBI in Vancouver, Canada. We included 493 participants (18–69 years, 54% female), after removing n = 19 with traumatic abnormalities on CT (intracranial and/or skull fracture). Outcomes were Glasgow Outcome Scale Extended (GOSE), Rivermead Post-Concussion Symptoms Questionnaire (RPQ), Patient Health Questionnaire (PHQ)−9, and generalized anxiety disorder (GAD)−7 at 6 months post-injury. Over half (55%) of participants received a CT. At 6 months, 55% of participants with CT and 49% without CT had functional limitations on GOSE; 32% with CT and 33% without CT reported severe post-concussion symptoms (RPQ ≥16); 26% (with CT) and 28% (without CT) screened positive for depression (PHQ-9 ≥ 10), and 25% (with CT) and 28% (without CT) screened positive for anxiety (GAD-7 ≥ 8). In regression adjusted for personal variables, participants with CT had somewhat higher odds of worse functioning (ordinal GOSE; 1.4, 95% CI 1.0–2.0) but similar odds of severe post-concussion symptoms (1.1, 95% CI: 0.7–1.7), and depression (1.1, 95% CI: 0.7–1.7) and anxiety (1.0, 95% CI: 0.6–1.5) symptoms. Adults with and without head CT have mostly comparable outcomes from TBI with GCS = 13–15. Requiring CT by clinical indication for study entry may not create problematic selection bias for outcome research.
Introduction
Our improved understanding of traumatic brain injury (TBI) over the past decade is strongly influenced by large cohort studies of TBI patients with a clinical indication for computed tomography (CT) of the head, such as United States-based Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) 1 and Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI). 2 These studies reported that approximately half of adults with “mild” TBI (Glasgow Coma Scale [GCS] score = 13–15 at hospital arrival) have functional limitations, 30–50% experience post-concussion symptoms, and 10–20% report mental health symptoms 6–12 months after injury. 3 –7 The rates of poor outcome do not appear to be (completely) driven by a subgroup of patients with trauma-related intracranial abnormalities on CT, because they are nearly as high in TRACK-TBI 8 and CENTER-TBI 9,10 participants with negative head CT. However, the rates of incomplete recovery and persistent symptoms in these cohorts are considerably higher than were reported in the decades prior, 11,12 where clinical indication for head CT was rarely used as an inclusion criterion.
Up to 70% of adults who present with GCS 13–15 following head trauma receive a CT scan. 13 –16 The primary role for head CT after TBI in the emergency department (ED) setting is to rule out lesions that would require urgent neurosurgical intervention (e.g., craniotomy). 17 Approximately one-third of head CT scans are ordered in patients for whom clinical prediction rules indicate nearly no risk of actionable CT findings. 18,19 However, the majority are ordered by clinical indication, consistent with clinical decision rules. 20,21 Clinical decision rules for head CT include variables that have also been found to be associated with poor outcome from TBI, such as post-traumatic amnesia (PTA) and acute headache. 22 –24 Therefore, there is reason to believe that adults who get head CTs have worse outcomes from TBI than those who do not get CTs. A corollary is that using CT head as an inclusion criterion may overestimate poor outcomes after TBI with GCS 13–15.
The present study compared outcomes after TBI in adults who had a head CT scan (with negative findings) versus those who had no CT when presenting to the ED. Given that head CT status (ordered vs. not) may be a proxy for injury severity or other patient factors associated with long-term outcome, we hypothesized that adults who had a head CT would report greater disability, post-concussion symptoms, and mental health symptoms 6 months after TBI with GCS 13–15. If supported, these findings would suggest the need for caution when extrapolating results from studies with head CT as an inclusion criterion to 30–50% of patients with TBI of GCS 13–15 who do not receive a head CT in the ED.
Methods
Study procedure and population
The present study was a secondary analysis of a clinical trial examining the effectiveness of a practice guideline implementation tool to support mental health screening and treatment initiation in primary care, the Mobilizing Early Management of Mental Health Complications After Mild Traumatic Brain Injury (M4) study. 25 Participants were randomized (1:1) to usual care or to an experimental intervention that involved providing the participant and their general practitioner with tailored information about their mental health screening test results and associated recommendations from a clinical practice guideline. Study procedures were approved by the University of British Columbia’s Research Ethics Board (H20-00562).
The M4 study recruited participants who presented to an ED or urgent care center within 72 h of mild TBI (with GCS 13–15) in Greater Vancouver, British Columbia (six EDs and two urgent care centers). Research assistants identified patients meeting criteria for probable or possible mild TBI on chart review, mailed them a consent form, and telephoned consented participants for further eligibility screening within a week of injury. Inclusion criteria for the parent study were: age 18–69 years; diagnosis of mild TBI confirmed with a structured interview (based on World Health Organization Neurotrauma Task Force diagnostic criteria) 26 ; ability to designate a family medicine clinic where they would seek follow-up care. Exclusion criteria were: a prior TBI within 6 months before the index injury; a pre-existing severe and unstable condition (e.g., cancer, psychotic disorder requiring hospital admission in the previous year). For this secondary analysis, we also excluded participants who presented to an urgent care center (n = 25) or had a positive finding on CT (n = 19 with intracranial abnormalities or skull fracture; Supplementary Fig. S1).
Information about injury characteristics and whether a CT was ordered/performed within first 72 h was extracted from medical charts. CT scan orders were naturalistic—emergency medicine physicians did not participate in study recruitment and were generally unaware of the study. Participant screening and recruitment began after ED discharge. Head CT scans were coded as having trauma-related abnormalities or not based on radiologists’ clinical reports. Subsequently, abnormal findings were coded according to the National Institute of Neurological Disorders and Stroke TBI Neuroimaging Common Data Elements 27 by a board-certified neurologist (W.P.). Demographic and medical history variables were assessed by research assistants in an eligibility screening call. Race/ethnicity was self-reported.
Outcomes
Outcomes were assessed at 2 weeks, 3 months, and 6 months post-injury. The Glasgow Outcome Scale Extended (GOSE) 28 was assessed via videoconference by trained research assistants, and self-reported questionnaires were administered online as a REDCap survey. If one item was missing on self-reported questionnaires, the value was imputed (prorated) by the mean rating of other nonmissing items, otherwise the score was considered missing.
The GOSE is a structured interview 29 measuring the change in functioning after TBI compared to the pre-injury level. It provides eight categories of outcome ranging from dead (1) to complete return to a pre-injury level of functioning without symptoms that disrupt function (8). We analyzed the GOSE-All ratings (level of functional limitation associated with the overall injury), 30 and reported if the most important factor in outcome was the head injury, injury to other body parts, or a mixture of the two. We analyzed GOSE as ordinal, and dichotomized as complete (GOSE = 8) versus incomplete recovery (GOSE <8). 3
The Rivermead Post-Concussion Symptoms Questionnaire (RPQ) 31 measures the severity of 16 symptoms that commonly occur after TBI. The severity of symptoms experienced within the last 24 h was rated on a scale from 0 (“never experienced”) to 4 (“severe problem”). The total RPQ score was calculated as the sum of all RPQ items, with responses 1 (“no more of a problem” than pre-injury) counted as 0. The total score can range from 0 to 64, with higher values indicating more severe symptoms. We analyzed the total score and severe symptoms, defined as total score ≥16. 3,32
The Patient Health Questionnaire (PHQ)−9 33 measures the severity of depression symptoms experienced in the past two weeks. It contains nine items that can be scored from 0 (not at all) to 3 (nearly every day). The total score, with possible range 0–27, was calculated as the sum of all items, with higher score indicating more severe symptoms. We analyzed the total score and positive screen for depression/probable Major Depressive Disorder defined as total score ≥10. 3,33,34
The Generalized Anxiety Disorder (GAD)−7 35 questionnaire measures the severity of anxiety symptoms experienced in the past two weeks. It consists of seven items that can be scored from 0 (not at all) to 3 (nearly every day). The total score, with possible range 0–21, was calculated as the sum of all items, with higher score indicating more severe symptoms. We analyzed the total score and positive screen for anxiety/probable GAD, defined as total score ≥8. 3,36
Statistical analyses
We described continuous variables with means and standard deviations, and categorical variables with percentages. Differences in baseline variables were tested with t-test and chi-square, respectively. The change in total scores over time (2 weeks, 3 months, and 6 months) was illustrated graphically with means and standard errors/percentages, separately for adults with CT performed and no CT performed.
To examine differences in 6-month outcomes between adults with CT and without CT, we first performed mixed-effects regression models with random intercept for site. Because random effects had a very low variance, the models were simplified (random effects excluded). We fitted univariable binary logistic models for dichotomized outcomes (GOSE <8, RPQ ≥16, PHQ ≥10, GAD ≥8). We fitted univariable proportional odds (ordinal) models for ordinal GOSE and ordinary least squares (linear) models with robust covariance matrix for continuous total scores. Further, we performed multivariable regression analyses adjusted for baseline variables that showed associations with CT indication and outcomes in this study and previous studies, 3 but are not part of commonly used clinical prediction rules for head CT 14,20 (sex [male/female], race [White/People of color] and mental health history [yes/no]). As sensitivity analyses, we also adjusted for site (ED) and group (intervention vs. usual care). We did not adjust for characteristics that differed between adults with CT and without CT, but were components of commonly used clinical decision rules for CT, such as age, GCS, presence of PTA, and injury mechanism. We reported odds ratios/regression coefficients with 95% confidence intervals. Analyses were performed in R Studio 4.2.1 using rms 37 package.
Results
In total, n = 493 participants were included in this study. (Supplementary Fig. S1). Over half (54%) had a head CT ordered/performed and 46% did not have a head CT. As expected, participants who had a CT scan were older, more frequently had a loss of consciousness (31% vs. 16%, p < 0.001; Table 1), PTA (71% vs. 46%, p < 0.001), GCS 13–14 (10% vs. 1%, p < 0.01), and dangerous mechanism of injury (pedestrians/cyclists struck by a motor vehicle or falls from height, 10% vs. 3%, p = 0.004). A higher proportion of participants who had a CT sustained their injury due to ground falls (41% vs. 30%) and smaller due to blows to the head (12% vs. 21%; Table 1). Additionally, participants who had a CT were more frequently White (69% vs. 58%, p < 0.01). As this was an unexpected finding, we analyzed the difference in receiving a CT for White versus minoritized participants adjusted for site, injury severity, dangerous mechanism, and age (1.3, 95% CI: 0.9, 2.0, p = 0.22). Almost all included participants completed 2-week questionnaires and around 92% completed 3-month and 6-month outcome assessments (Fig. 1).
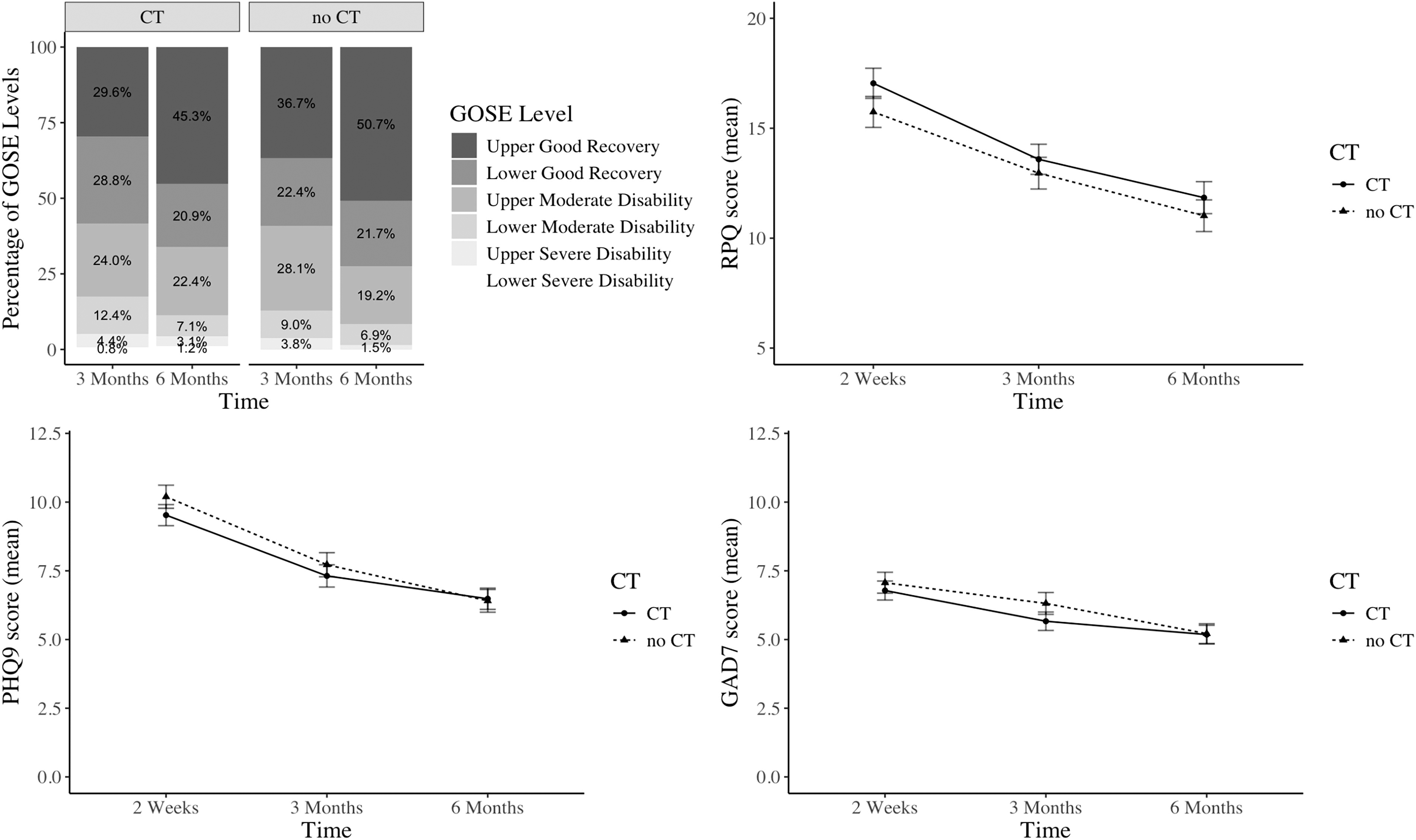
Outcomes at 2 weeks,1 3 months,2 and 6 months3 for adults who had a head CT scan performed and those who had no CT: functioning (GOSE), post-concussion symptoms (RPQ), depression (PHQ-9), and anxiety symptoms (GAD-7). 1RPQ: n = 491, PHQ-9: n = 489, GAD-7: n = 492; 2GOSE: 460; RPQ: n = 454; PHQ-9, GAD-7: n = 456; 3GOSE: 457; RPQ, PHQ-9, GAD-7: n = 451. CT, Computed Tomography; GAD, Generalized Anxiety Disorder; GOSE, Glasgow Coma Scale Extended; PHQ, Patient Health Questionnaire; RPQ, Rivermead Post-concussion Symptom Questionnaire.
Patient Characteristics
p < .05.
p < .001.
Possible to select multiple responses.
Test Statistics: t-test for continuous outcome (age), chi-squared test for categorical outcomes.
GED, general educational development; VGH, Vancouver General Hospital; UBC, University of British Columbia.
Outcomes in adults who had a head CT scan versus those who had no CT
Generally, functional outcome (GOSE) and symptoms improved over time in both groups (Supplementary Table S1). Small (and statistically insignificant) differences in post-concussion symptoms at 2 weeks between adults who had a CT and had no CT were further reduced by 6 months (Fig. 1). Over half of participants (CT: 55%, no CT: 49%) did not completely return to their pre-injury functioning by 6 months, a third (CT: 32%, no CT: 33%) had severe post-concussion symptoms and more than a quarter screened positive for depression (CT: 26%, no CT: 28%) or anxiety disorder (CT: 25%, no CT: 28%; Table 2).
Six-Month Outcomes in Adults Who Had a Head CT Scan Performed and Those Who Had No CT (n = 457 for GOSE, n = 451 for Questionnaires)
adjusted for race, sex, mental health history.
CT, computed tomography; GOSE, Glasgow Outcome Scale-Extended; GAD-7, Generalized Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9; RPQ, Rivermead post-Concussion Symptoms Questionnaire.
At 6-months, adults with a head CT performed had similar odds of severe post-concussion symptoms and positive screen for depression/anxiety in univariable or multivariable analyses (Table 2). The difference was most pronounced for global functioning, with adults with a head CT showing slightly higher odds for worse (ordinal) GOSE (1.4, 95% CI: 1.0–2.0) and incomplete recovery (nonsignificant; 1.4, 95% CI: 0.9–2.1) in analyses adjusted for race, sex, and mental health history. Analyses adjusted for site and trial groups (Supplementary Table S2) and linear regression analyses (Supplementary Table S3) were consistent with those reported in Table 2.
Discussion
We examined outcomes in adults who presented to EDs after head injury with GCS 13–15 (mild TBI). Adults who had a head CT (with negative findings) and those who had no CT had mostly comparable outcomes at 6 months. The two groups had similar levels of post-concussion and mental health symptom reporting, but participants who had a head CT had a modestly higher odds of worse recovery based on the GOSE rating. This suggests that the rates of poor outcomes after TBI with GCS 13–15 are not markedly inflated in research studies that exclude patients without CT indication. However, slightly worse functional outcomes may be expected by restricting enrollment to those who received a head CT. Worse functional outcomes can probably be explained by patient (e.g., older age) and injury characteristics (e.g., lower GCS), which differed between participants with versus without CT in our study and have been identified as predictors of worse recovery in previous studies. 23,38,39 In other words, baseline factors underlying propensity to get a head CT likely account for any differences in outcome by CT status.
Interestingly, rates of functional impairments (49% and 55%) and severe symptoms (32% and 33%) observed in this study are very similar to those found in a recent meta-analysis 6 and cohort studies with CT indication as an inclusion criterion (such as TRACK-TBI and CENTER-TBI), while the rates of probable mental health disorders were even higher (over 25%). 3,7 This may be due to the self-selection of participants for a trial targeting mental health following mild TBI (i.e., patients with a history of mental health problems may be more motivated to participate). This finding is in line with previous studies identifying pre-injury mental health as a strong predictor of symptoms and functioning after TBI with GCS 13–15. 5,7,23,40,41 Moreover, higher levels of functioning (higher GOSE) seem to be strongly determined by mental health. 42
One unexpected finding worth noting is that participants who self-identified as White were more likely to receive a head CT scan than minoritized participants (69% vs. 58%); although the difference did reduce and was not statistically significant after adjusting for site, injury severity, dangerous mechanism, and age. As prior studies have reported racial differences in ED wait-times, likelihood of leaving the ED without seeing a physician, and having follow-up care arranged, 43,44 future studies should verify whether the underlying mechanisms of these differences are primarily related to the components of decision rules for CT, or other factors, such as cultural differences in patient expectations or overt advocacy, implicit bias in healthcare delivery, and tendency to present to ED.
This study has some limitations. It was a secondary analysis of a trial that excluded participants aged 70 years or older. Differences in outcomes based on the CT indication, particularly GOSE, may be more pronounced without this criterion, due to higher levels of disability in older age groups. 45,46 As mentioned, a self-selection bias might be present, with more adults with mental health problems participating in this study. While this may have impacted the rates of poor outcomes, we do not expect it to have influenced our primary analyses and we statistically adjusted for mental health history. As we only examined self-reported outcomes, potential differences in other outcomes, such as functional neuroimaging and neuropsychological tests, cannot be ruled out. Further, we recruited patients from both academic medical centers and regional hospitals. The minority (25%) presented to a Level 1 trauma center (Vancouver General Hospital). We believe this recruitment strategy strengthens generalizability but complicates direct comparison to the TRACK-TBI and CENTER-TBI cohorts, who were only recruited from Level 1 trauma centers. Only 19 of 287 participants who received a head CT in the parent study had trauma-related abnormalities. This scan positivity rate (7%) is lower than in most prior studies, 5,23,47,48 perhaps suggesting CT overuse at our recruitment sites, at least for the subgroup considered eligible for the study and agreed to participate. We did not investigate whether the clinical decision to order a head CT for individual patients were made in adherence with evidence-based decision rules. To the extent that local physicians ordered CT scans for low-risk patients (decision rule-discordant), the present findings may underestimate the magnitude of differences in outcome between the CT and no-CT groups in the other clinical settings with more restrictive criteria for CT ordering. If practice patterns change towards more conservative CT use, larger differences between CT and no-CT groups could emerge, though decades of efforts to curb head CT overuse seem to have yielded little change. 49,50 This study was designed as a clinical trial; nevertheless, controlling for group (experimental vs. control) yielded consistent results.
In conclusion, adults with and without head CT have similar self-reported outcomes from TBI with GCS = 13–15. However, those who received a CT had modestly increased odds of worse recovery (GOSE). Requiring CT by clinical indication for study entry may create some, but likely not strong and problematic, selection bias for outcome research.
Transparency, Rigor, and Reproducibility Summary
The parent study was pre-registered at clinicaltrials.gov (Identifier: NCT04704037). The secondary analysis was not pre-registered. The number of participants approached (n = 4062), assessed for eligibility (n = 1520), enrolled (n = 537), and included in the current study (n = 493) are reported in the article (in the text and in a CONSORT diagram, Supplementary Fig. S1). Data were collected between February 2021 and April 20, 2023. Clinicians ordering CT did not participate in the study recruitment and were generally unaware of the study. Participant screening and recruitment began after ED discharge. Validated instruments and Common Data Elements for TBI were used for outcome assessment. Outcome assessment was performed by trained research assistants blinded to aim of this study. Confidence intervals for unadjusted and adjusted odds ratios/regression coefficients are reported for all outcomes. The analytic approach and statistical packages are described in the article, and more detailed information is available by contacting the corresponding author.
Footnotes
Authors’ Contributions
N.D.S. and A.M.: Conceptualization. S.S. and A.M.: Formal analysis. J.R.B. and F.X.S.: Data collection (recruitment). N.D.S.: Supervision. A.M.: Writing—original draft. S.S., W.P., J.R.B., F.X.S., L.D.N., and N.D.S.: Writing—review and editing.
Author Disclosure Statement
A.M. was supported by the University of British Columbia (UBC) Institute of Mental Health (IMH) Marshall Fellows Program. N.D.S. has received research operating funds from multiple granting agencies (Canada Foundation for Innovation,
Funding Information
The parent study (Clinicaltrials.org ID #NCT04704037) was funded by the Canadian Institutes for Health Research (CIHR).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.