
Abstract
The effect of sex in outcomes after severe traumatic brain injury (TBI) remains uncertain. We explored whether outcomes differed between women and men after standardized care management during the first 5 days in the intensive care unit (ICU). This study was an observational analysis of the OXY-TC multicenter randomized clinical trial between June 15, 2016 and April 17, 2021. Recruited patients had a pre-hospital Glasgow Coma Scale (GCS) score of 3–8, mechanical ventilation, and intracranial pressure (ICP) with or without brain tissue oxygen pressure (PbtO2) monitoring. Objectives were to maintain ICP at 20 mmHg or below and PbtO2 above 20 mmHg at all times. The primary end-point was the proportion of women and men with poor outcomes at 6 months, corresponding to an extended Glasgow Outcome Scale (GOSE) score of 1–4 (death to upper severe disability). Of 318 randomized patients, 200 men and 71 women were analyzed. They were comparable in age, comorbidities, and initial injury severity scores. However, women had larger doses of ICP as the proportion of monitoring time of ICP above 20 mmHg 8% (3–18; median, interquartile range) versus 3% (1–10), respectively (p = 0.002). They required more often at least one tier-3 treatment, i.e., barbiturate coma and therapeutic hypothermia, for refractory intracranial hypertension during the first 5 days in the ICU: 33/68 (48%) versus 60/193 (31%), respectively (p = 0.012). At 6 months, the proportion of women with GOSE 1–4 was significantly higher than men: 48/71 (68%) versus 94/200 (47%), respectively (odds ratio 2.35 [1.33–4.16]; p = 0.003]. Similar differences were found using Disability Rating Scale and Functional Independence Measure at 6 and 12 months, and GOSE at 12 months. Sex differences in neurological outcomes persisted after adjustment for other determinants of outcome such as age, initial GCS score, and dose of ICP during the 5-day monitoring. In conclusion, women sustained more severe ICP and required more active treatment, both of which would explain a worse outcome after severe TBI. Prospective research is required to confirm these findings and identify possible mechanisms.
Trial registration: ClinicalTrials.gov Identifier NCT02754063 (April 28, 2016).
Introduction
Considerable progress has been achieved over the past decades in the understanding of the pathophysiology, risk factors, prevention, and management of patients with traumatic brain injury (TBI). 1 TBI is, however, heterogeneous, and the outcome is influenced by a combination of factors including age, injury location, severity, genetics, and environment. Sex as a biological variable and gender as a social construct have recently emerged as possible contributors in the rehabilitation of patients after TBI. 2,3 Despite promising results in experimental models, two clinical trials of progesterone treatment, as a protective agent, failed to demonstrate improved neurological outcomes in patients with TBI. 4,5 Although the incidence of TBI is higher in men than in women, sex differences in outcomes showed inconsistent results, partly due to the interference of multiple factors including injury severity, age, comorbidities, and quality of care management in hospital. In a scoping review, Gupte and colleagues identified 73 studies with a higher mortality in women than in men after any type of TBI while 41 studies showed a better outcome, 28 studies found no sex differences, and 14 studies showed inconclusive results. 6 Most of these reported studies were, however, based on patients with mild or moderate TBI.
Although severe TBI, as defined by an initial Glasgow Coma Scale (GCS) score of less than 9, is a devastating condition since 50–55% of patients have permanent severe disabilities, 7 the impact of sex on neurological outcome has been scarcely studied in this population. No sex differences in outcomes were found in severe isolated patients with TBI at hospital discharge or at 6 months. 8,9 By contrast, a lower rate of survival was found in women with severe TBI at hospital discharge. 10,11 Because many factors can interfere with outcomes such as the initial presentation, management in the intensive care unit (ICU), care pathways at ICU discharge, and family environment, it is difficult to conclude on the reality of sex differences after severe TBI.
Considering this lack of evidence, the investigators explored the effect of sex after severe TBI as an observational analysis of the OXY-TC trial. This trial compared the management of patients with TBI with intracranial pressure (ICP) only monitoring versus a combination of ICP and brain tissue oxygen pressure (PbtO2) monitoring during the first 5 days from admission in the ICU on the extended Glasgow Outcome Scale (GOSE) at 6 months. 12 In the present study, the investigators studied the hypothesis that long-term neurological outcomes differed between men and women after adjusting for confounding factors associated with poor outcomes. The primary outcome was the neurological status at 6 months after TBI.
Methods
This study was an observational analysis of the OXY-TC trial. 12 The OXY-TC was a multicenter, randomized, open-label, controlled trial, which explored the impact of a strategy combining ICP and brain tissue oxygen pressure (PbtO2) monitoring on neurological outcomes after severe TBI. Patients (18–75 years) with a pre-hospital GCS score of 3–8 following a non-penetrating TBI were admitted to 1 of the 25 tertiary French centers. Patients were included if they were sedated, mechanically ventilated in stable conditions, and monitored with ICP with or without PbtO2 within 16 h after the injury. Bilateral fixed and dilated pupils were among the exclusion criteria. Patients were then randomized through a dedicated website (Medsharing, Fontenay-sous-Bois, France) by blocks of variable size and stratified by center and age (<50 years and ≥50 years) in a 1:1 ratio. Randomized patients were managed either by ICP monitoring or by both ICP and PbtO2 monitoring during the first 5 days of admission in the ICU. The therapeutic objectives were to maintain ICP at 20 mmHg or lower, and PbtO2 above 20 mmHg at all times.
For all patients, clinical management followed international guidelines with tier-1 therapies if ICP and PbtO2 were kept within normal ranges. 13,14 If ICP exceeded 20 mmHg, tier-2 was introduced with no rank order: deep level of sedation/analgesia, cerebral perfusion pressure (CPP) higher than 70 mmHg through the use of vasopressors, moderate hyperventilation (PaCO2 30–35 mmHg), bolus osmotherapy, external ventricular drainage, neuromuscular blockade, and body temperature 35°C–37°C. Refractory intracranial hypertension initiated tier-3 treatments: therapeutic hypothermia (33°C–35°C), secondary decompressive craniectomy, and barbiturate coma. If the PbtO2 dropped below 20 mmHg, even with an ICP lower than 20 mmHg, the following interventions were initiated in a pre-defined order: PaO2 between 100 and 150 mmHg, PaCO2 between 35 and 45 mmHg, temperature between 35°C and 37°C, CPP between 60 and 100 mmHg, cardiac index higher than 2.5 L/(min·m2), hemoglobin content between 9 and 12 g/dL, and finally PaO2 higher than 150 mmHg. The current observational analysis explored the impact of sex on neurological outcomes in the enrolled patients at 6 and 12 months after TBI.
Ethics
The Institutional Review Board (IRB) of Sud-Est V (Dr. Grunwald, Grenoble) approved on December 3, 2014 (Ref#14-CHUG-48) and the National Agency for Medicines and Health Products Safety (ANSM, Agence Nationale de Sécurité du Médicament et des produits de santé) on February 3, 2015 (Ref#141435B-31) published OXY-TC trial protocol. 15 The trial began on June 15, 2016, and ended on April 17, 2021. Patient follow-up ended on April 17, 2022. Investigators obtained written informed consent from a next of kin or a legal surrogate. If next of kin or a legal surrogate were unable to provide written consent, the onsite investigator approved the enrollment of the patient according the French law (Procedural Authorization). 16
Data collection
Collected data into a web-based electronic case report form (eCRF; Medsharing, Fontenay-sous-Bois, France) contained demographic baseline information, intra-cerebral monitoring parameters (ICP, CPP, PbtO2) every hour (days 1–5), duration of mechanical ventilation and ICU stay, adverse events during the entire ICU stay, and survival status on day 28. The International Mission on Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (IMPACT-TBI) scoring (core + computed tomography [CT]) 17 was calculated on factors at randomization to predict the probability of unfavorable outcomes at 6 months. Trajectories of patients at discharge from the ICU were recorded, i.e., post-ICU neuro-rehabilitation unit, post-acute community-based rehabilitation center, neurosurgical ward, other clinical ward, and home. Marital status, i.e., single or living with a partner, was collected on admission to the ICU and at 6 months post-trauma.
Primary and secondary outcomes
The primary end-point was the proportion of women versus men with poor outcomes at 6 months, i.e., with a GOSE score of 1–4 (death to upper severe disability). 18 Trained outcome assessors blinded to the group allocation conducted a centrally, structured telephone interview to assess the GOSE. Secondary outcomes were the GOSE at 12 months and the Disability Rating Scale (DRS) at 6- and 12-month post-injury in both sexes. DRS scores range from 0 (no disability) to 29 (extreme vegetative state). The quality of life was assessed at 6- and 12-months post-trauma using the Functional Independence Measure (FIM) instrument to assess cognitive and motor independency, ranging from 18 (complete dependence) to 126 points (complete independence). Recording therapies to control ICP allowed the calculation a posteriori of the daily highest therapy intensity level (TIL) score during a 5-day monitoring period (TILmax) 19 and of the number of patients who received at least one tier-3 treatment for refractory intracranial hypertension. The dose of ICP, which accounts for both intensity and duration of intracranial hypertension, was calculated as the proportion of monitoring time of hourly ICP values above 20 mmHg over the first 5 days. 20 Critical events in both groups during the first 5 days of the ICU stay were defined by an ICP higher than 30 mmHg lasting for more than 30 min, and a PbtO2 below 10 mmHg for more than 30 min. The mortality rate was determined at day 28 and over 12 months follow-up post-trauma.
Statistical analysis
Results were expressed as median and interquartile ranges and numbers (percentages). Odds ratios (ORs) were expressed as mean with an associated 95% confidence interval (CI). The primary outcome measure was analyzed using logistic regression with GOSE 1–4 at 6 months as dependent variable and sex group as independent variable and was expressed using OR and 95% CI. Factors with a possible impact on the neurological outcome at 6 were listed from the analysis of the literature (see review 21 ). These factors were included into a univariate logistic regression with the Sidak correction for multiple comparisons. Variables with a p value of less than 0.20 were retained for a forward stepwise multivariate logistic regression model to determine factors independently associated with GOSE 1–4 at 6 months. Sex-related GOSE analysis at 6 months was completed with an ordinal analysis based on proportional odds logistic regression (sensitivity analysis). 22 Interaction between sex and age was tested using a logistic model. The changes in ICP, CPP, and PbtO2 values between the two groups over each 6 h period were analyzed using a mixed linear regression model with patient as a random effect.
For secondary outcomes, GOSE at 12 months, DRS and FIM at 6 and 12 months, and mortality at 28 days between women and men were compared using non-parametric Fisher or Mann–Whitney tests. Kaplan–Meier curves compared survival rates between women and men over 12 months post-trauma using a log-rank test from a Cox model. Analyses were performed using Stata version 15·0 (Stata Corp., College Station, TX). All p values were two-sided, and statistical significance was declared when p was less than 0.05. The OXY-TC trial was registered with Clinical Trials NCT02754063 on April 28, 2016.
Results
A total of 318 patients with severe TBI were randomized in the OXY-TC trial. 12 Of these, 47 patients were not included in the primary analysis due to consent withdrawals (n = 8), protocol violations (n = 19), and lost to follow-up (n = 20). There were 271 patients available for the primary analysis: 200 men and 71 women. The baseline characteristics of these patients are shown in Table 1. Although the initial injury severity scores and the IMPACT-TBI score at randomization were comparable between the two groups, women had more frequently at least one pupil unresponsive and traumatic subarachnoid hemorrhage (SAH) than men on admission. They also had lower alcohol blood levels on admission. The brain monitoring using ICP alone or ICP + PbtO2 was distributed evenly between men and women. The dose of ICP was significantly larger in women than men and more women were treated with at least one tier-3 treatment to control ICP, i.e., therapeutic hypothermia or barbiturate coma (Table 2). Tier-2 treatments were requested for all patients and equally distributed between the two groups, except temperature 35°C–37°C which was more frequently used in women than in men. Although ICP, CPP, and PbtO2 values remained within the pre-defined ranges for therapeutic outcomes during the 5-day monitoring period, women had both ICP and PbtO2 values significantly higher than men over time (p = 0.015 and p = 0.004, respectively) (Fig. 1). CPP did not differ between the two groups.

Intracranial pressure (ICP)
Characteristics of the Study Population at Baseline
Data are expressed as the median (25–75th percentiles) or numbers (percentages). Proportions are calculated from the whole studied groups, i.e., 200 men and 71 women, unless otherwise specified. Major extracranial injuries were defined by abbreviated injury severity score ≥3.
aSDH, acute subdural hematoma; CPP, cerebral perfusion pressure; CT, computed tomography; EDH, epidural hematoma; GCS, Glasgow Coma Scale; ICP, intracranial pressure; ICU, intensive care unit; ISS, injury severity score; IVH, intra-ventricular hemorrhage; MAP, mean arterial blood pressure; PbtO2, brain tissue oxygen pressure; SAPS, simplified acute physiology score; SBP, systolic blood pressure; tSAH, traumatic subarachnoid hemorrhage.
Dose of ICP and Management to Control ICP During the First 5 Days of Management in the ICU in the Study Population
Data are expressed as the median (25–75th percentiles) or numbers (percentages). The dose of ICP was the proportion of monitoring time of ICP above 20 mmHg.
CPP, cerebral perfusion pressure; HSS, hypertonic saline solution; ICP, intracranial pressure; ICU, intensive care unit; PbtO2, brain tissue oxygen pressure; TILmax, highest therapy intensity level score.
At 6 months post-TBI, the proportion of women with GOSE 1–4 was significantly higher than men: 48/71 [68%] in women versus 94/200 [47%] in men, respectively, with an OR of 2.35 (1.33–4.16; p = 0.003) (Fig. 2). Ordinal analysis with proportional odds regression showed a significant effect of sex with women more exposed to have poor outcome than men (OR 2.24 [1.39–3.62]; p = 0.001). Sex differences persisted for survivors with bad outcome, i.e., GOSE 2–4 at 6 months: OR = 2.13 (1.10–4.12; p = 0.025). The impact of sex on poor neurological outcome was more visible in younger patients than older (Fig. 3). Other factors were significantly associated with poor outcome as shown in Table 3: age of 50 years or more, simplified acute physiology score II score, and ICP dose during the first 5 ICU days. The allocation of the monitoring-guided strategy group, i.e., ICP alone or ICP + PbtO2, had no effect on outcome at 6 months. A positive blood alcohol level on admission did not affect the outcome (OR = 0.88 [0.67–1.15]; p = 0.35; n = 202 patients). In multivariate analysis, female sex, age of 50 years or more, and a larger dose of ICP during the 5-day monitoring were the most important factors independently associated with poor outcome at 6 months (Table 4).

Distribution of GOSE scores at 6 months. Each scale corresponds to a score on the scale and the length of each cell represents the proportion of patients with equivalent scores. GOSE, extended Glasgow Coma Scale.

Logistic model of linear correlation between age and probability (mean and 95% confidence interval) to have poor outcome at 6 months for women (light gray) and men (dark gray). Poor outcome is defined by an extended Glasgow Coma Scale score of 1–4.
Univariate Analysis for Variables Associated with Poor Outcome, i.e., GOSE 1–4 at 6 Months Post-Severe TBI
Data are expressed as the median (25–75th percentiles) or numbers (percentages) and unadjusted odds ratio (OR) and associated 95% confidence intervals (CIs). The threshold for significance was set at 0.003 according to the Sidak correction for multiple comparisons.
aSDH, acute subdural hematoma; CT, computed tomography; EDH, epidural hematoma; GCS, Glasgow Coma Scale; ICP, intracranial pressure; ICU, intensive care unit; ISS, injury severity score; IVH, intra-ventricular hemorrhage; MAP, mean arterial blood pressure; SAPS, simplified acute physiology score; tSAH, traumatic subarachnoid hemorrhage; TILmax, highest therapy intensity level score.
Adjusted Odds Ratio (OR) and Associated 95% Confidence Intervals (CIs) for Variables Associated with Poor Outcome, i.e., GOSE 1–4 at 6 Months Post-Severe TBI (n = 269 Patients)
ICP, intracranial pressure; ICU, intensive care unit; SAPS, simplified acute physiology score.
Similar differences between women and men were found in the GOSE scores at 12 months (OR = 2.10 [1.18–3.74]; p = 0.012) as well as in the DRS and FIM measurements at 6 and 12 months (Table 5). There was no statistically significant difference between sex in their survival rate on day 28 or over the 12 months follow-up (Fig. 4). Withdrawal of care in the ICU was not different between women and men: 11/71 (15%) versus 16/200 (8%) (p = 0.10).
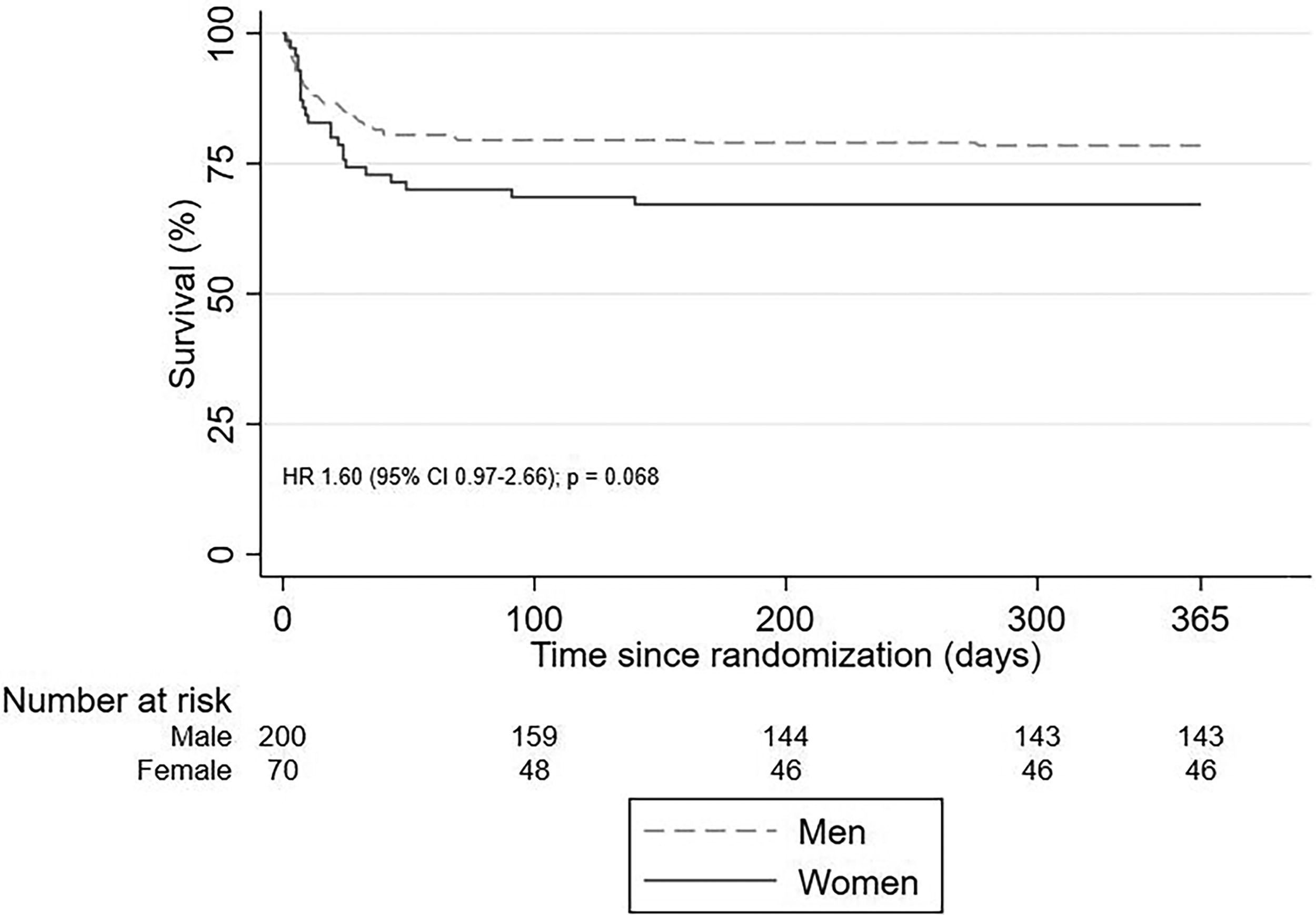
Survival at 12 months. Time from randomization was to 12-month follow-up or death. HR, hazard ratio.
Comparisons Between Men and Women in Secondary Neurological Outcomes
Data are expressed as the median (25–75th percentiles) or numbers (percentages).
DRS, Disability Rating Scale; FIM, Functional Independence Measure; GOSE, extended Glasgow Outcome Scale.
At discharge from the ICU, women and men had comparable trajectories from the ICU (p = 0.48) to either the post-acute rehabilitation unit (11/48 [23%] vs. 22/160 [14%]), community rehabilitation center (8/48 [17%] vs. 24/160 [15%]), neurosurgical ward (15/48 [31%] vs. 67/160 [42%]), other clinical ward (14/48 [29%] vs. 46/160 [29%]), or home (0 vs. 1/160 [1%]). Among patients with marital status on admission and at 6 months, the proportion of patients who lived with a partner on admission was similar between women and men (25/44 [57%] vs. 86/145 [59%], respectively; p = 0.86). This proportion significantly decreased for women at 6 months: 9/44 (20%) vs. 57/145 (39%), respectively (p = 0.029).
Discussion
In this observational analysis of the OXY-TC trial at level I trauma centers in France, women with severe TBI had poorer neurological outcomes than men at 6 and 12 months post-trauma. Sex differences in neurological outcomes persisted after adjustment for other determinants of outcome such as age, initial score, and dose of ICP during the 5-day monitoring. These findings were associated with a larger dose of ICP and more requirements for tier-3 treatments to control ICP in women than men during the first 5 days in the ICU.
Men sustain more frequently TBI at a younger age because of increased risk taken, and vehicle- and work-related accidents. Women more often sustain TBI due to falls and domestic violence. 23 The majority of studies reported that women had more psychological and functional health problems post-injury than men after mild TBI. 6,9,24 In moderate-to-severe TBI, however, data on outcomes from large cohorts or retrospective studies found no sex-related differences after adjustment for age, injury severity, and comorbidities. 8,9,24 A lower rate of survival at hospital discharge was found in women with pre-hospital hypotension and severe TBI. 10 Women aged 55 and older had a higher rate of mortality at hospital discharge after isolated severe TBI. 11 In the absence of robust information on cerebral monitoring and neurocritical care intensity directed at maintaining brain homeostasis, it is, however, difficult to conclude on whether women show worse neurological outcomes than men. In the present analysis of a randomized trial, therapeutic interventions were standardized to keep ICP and PbtO2 measurements within normal range according to pre-defined algorithms in line with international guidelines. 13,14,25 Despite this standardization of care and high protocol compliance, women sustained more severe ICP and required more active treatment, both of which were associated with worse outcomes as assessed using GOSE, DRS, and FIM instruments at 6 and 12 months.
The investigators can only formulate assumptions to explain these observed differences. On admission, women and men had comparable age, comorbidities, GCS and injury severity scores, and Marshall classification on initial CT. However, the proportion of patients with at least one unresponsive pupil to light stimulation or with traumatic SAH was higher in women than men. Abnormal reaction to light stimulation should be differentiated from bilateral fixed and dilated pupils that was an exclusion criterion in the OXY-TC trial. Although pupil reactivity is a covariate in the IMPACT-TBI model, there are uncertainties on how this clinical item is collected and on the effect of an episode of one or two unreactive pupils on the outcome. 26 Assessing pupil light reactivity by standard visual examination could yield inaccurate results as found elsewhere. 27 Traumatic SAH is one CT predictor of outcome, 28 but its location or extent was not reported in the present study. We did not use double reading of brain CT scans with board-certified neuroradiologists. The IMPACT-TBI score, which includes both pupil reactivity and traumatic SAH, did not, however, differ between the two groups on admission, and these two variables were not subsequently retained as independent factors of outcome in the multivariate analysis. We found no association between outcome and positive blood alcohol level that might have artificially lowered GCS scoring on admission and did not confirm the previous study. 29 However, despite adjustment for several factors known to have a possible impact on neurological outcome, there were a few noticeable differences in baseline characteristics between men and women that could have affected the outcome.
In the ICU, a larger dose of ICP was found in enrolled women along with significantly higher ICP values than men, although average ICP during the first 5-day monitoring was maintained below 20 mmHg. Since its first description, 30 the determination of the dose of ICP has been confirmed as a robust predictor of outcome. 20,31,32 The pressure time dose can be calculated as the area under the curve above a specific threshold of ICP or the proportion of monitoring time above an ICP threshold. In this study, 5% of monitored time above 20 mmHg may represent until 6 h spent in intracranial hypertension over a full 5-day monitoring period. In parallel, women received more frequent barbiturates and therapeutic hypothermia as part of therapies to control ICP. These two tier-3 treatments were used only when tier-2 treatments were ineffective as required in the protocol and might reflect the aggressiveness of treatment. In a CENTER-TBI analysis, an association was found between the use of tier-3 treatments used after day 1 and worse functional outcome at 6 months. 33 Overall, these findings indicate that control of ICP was more difficult to achieve in women than in men during the first 5 days of brain monitoring. This might be due to sex differences in treatment thresholds for ICP. A recent observational study found an ICP threshold of 18 mmHg regarding survival and functional outcome, with lower thresholds in patients who were aged, women, or had a low admission GCS score. 34 Whether this sex difference is related to lower brain compliance and/or reduced responsiveness to therapies in TBI women should be explored. Our findings indicate also that sex might be included as a co-variable of outcome in ad hoc studies with patients with severe TBI.
After discharge from the ICU, care pathways and family environment may impact on outcome. Post-ICU care pathways were comparable between men and women in the present study, in line with studies in patients with moderate-to-severe TBI. 9 The family environment, specifically the presence of a primary informal caregiver, may contribute markedly to a favorable outcome. After stroke and TBI, the typical informal caregiver is often female and either a spouse or an adult child of the patient. 35,36 In analogy to stroke, the present study observed changes in the partnership status of women with TBI at 6 months. This finding could be caused by a less frequent return of women to the shared household due to poor presentation, or by the negative effect of an absent informal caregiver on the neurological outcome. Although the causal link between marital status and outcome at 6 months cannot be inferred from these data, these findings indicate that the impact of severe TBI at 6 months differed between women and men, and generated more frequently a change in the partnership status of TBI women.
This study has some limitations. First, this is an unplanned analysis that was not of the published trial protocol. 15 Second, due to the lack of high-resolution ICP monitoring data, the investigators could not calculate with more accuracy the cumulative dose of ICP using the area under the curve of the magnitude and duration of ICP, as done elsewhere. 32 Third, the use of propensity-matched controls for men and women would require a larger sample size to construct two comparable groups, with no strong benefit in this study over multivariate regression. Adjustments for potential confounders were done in the multivariate analysis with the few differences between men and women found at baseline. Fourth, although all patients had at least two CT scans within the 5-day monitoring, we did not analyze the progression of hemorrhagic brain lesions and their potential impact on outcome. That would need accurate quantification of the volume of hematomas. Fifth, the state of cerebral autoregulation was not estimated in the present study. The self-regulation curve of study women might be shifted to the right or the plateau narrower.
In conclusion, women with severe TBI had a significantly poorer neurological outcome than men at 6 and 12 months. Sex was independently associated with outcome. In parallel, women sustained more severe ICP and required more active treatment to control ICP. These findings should stimulate studies to explain and mitigate the causes of these disparities between men and women after severe TBI.
Transparency, Rigor, and Reproducibility Statement
The study is an observational analysis of the pre-registered OXY-TC trial at clinicaltrials.gov (NCT02754063). The analysis plan was not formally pre-registered, but the team members with primary responsibility for the analysis, i.e., led author and biostatistician, certify that the analysis plan was pre-specified. Of the 318 patients randomized in the OXY-TC trial, a sample size of 271 patients was available with primary measurements collected, analyzed, and primary clinical outcomes assessed. The basis for the 47 exclusions were consent withdrawals (n = 8), protocol violations (n = 19), and lost to follow-up (n = 20). There were 53 patients who died from any cause at 28 days post-trauma. Data were acquired between June 15, 2016 and April 17, 2021, and collected using web-based eCRF (Medsharing, Fontenay-sous-Bois, France). Data analyses used Stata version 15·0 (Stata Corp., College Station, TX) and were performed by A.V., PhD in statistics and methodology. The time required for data acquisition was 5 years, and 2 years for preprocessing and analysis. The key inclusion criteria and the primary clinical outcome measure are established standards (Weir J et al., J Neurotrauma 2012; Horton L et al., J Neurotrauma 2018), and were assessed by clinical research associates with specific training. Effect sizes and CIs have been reported in the abstract for primary outcome and main text for all outcomes. Methods that do not require correction for multiple comparisons were used including univariate and multivariate logistic regressions for primary outcome and non-parametric tests for secondary outcomes. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. De-identified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Footnotes
Acknowledgments
The authors thank the French National Program for Clinical Research, La Fondation des Gueules Cassées, and Integra Lifesciences as sources of funding for the OXY-TC trial. The Neurocritical Care and Neuro Anaesthesiology French Speaking Association (ANARLF) endorsed the study.
Authors’ Contributions
J.-F.P., A.V., A.A., and J.-L.B. performed conception and study design, data collection and data analysis. J.-F.P. wrote the first draft of the article and all authors contributed to the interpretation of data and commented on previous versions of the article. All authors attest to having full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors verified the underlying data and approved the final article.
Author Disclosure Statement
J.-F.P. reports honoraria from Integra Lifesciences, Sedana Medical, IdMed, and CDM-Lavoisier/IDD. P.B. and T.G. report honoraria from Laboratoire du Biomédicament Français. The other authors declare no competing interests.
Funding Information
The OXY-TC trial received grants from the French National Program for Clinical Research (13-0119), and La Fondation des Gueules Cassées (49-2105). Integra Lifesciences graciously provided the PbtO2 catheters to participating centers. These funding sources had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.