
Abstract
To compare the incremental prognostic value of pupillary reactivity captured as part of the Glasgow Coma Scale–Pupils (GCS–P) score or added as separate variable to the GCS+P, in traumatic brain injury (TBI). We analyzed patients enrolled between 2014 and 2018 in the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI, n = 3521) and the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI, n = 1439) cohorts. Logistic regression was utilized to quantify the prognostic performances of GCS–P (GCS minus number of unreactive pupils) and GCS+P versus GCS alone according to Nagelkerke’s R 2. End-points were mortality and unfavorable outcome (Glasgow Outcome Scale–Extended score 1–4) at 6 month post-injury. We estimated 95% confidence intervals (CIs) with bootstrap resampling to summarize the improvement in prognostic capability. In a meta-analysis of CENTER-TBI and TRACK-TBI, GCS as a linear score had a R 2 of 25% (95% CI 19–31%) for mortality and 33% (4–41%) for unfavorable outcome. Pupillary reactivity as a separate variable improved the R 2 by an absolute value of 6% (4.0–7.7%) and 2% (1.2–3.0%) for mortality and unfavorable outcome, respectively, while comparatively half of this improvement was captured by the GCS–P score (3% [2.1–3.3%], 1% [1–1.7%], respectively). GCS–P showed a stronger association with 6-month outcome after TBI than GCS alone and provides a single integrated score. However, this comes at a loss of clinical and prognostic information compared with GCS+P. For prognostic models, inclusion of GCS and pupillary reactivity as separate factors may be preferable to using a GCS–P summary score.
Background
Traumatic brain injury (TBI) is a pressing, multifaceted health concern affecting millions of people worldwide annually. 1 –3 The initial clinical severity of TBI is commonly reported using the total Glasgow Coma Scale (GCS) score of 3–15, which is often grouped into three classes of severity: mild (GCS 13–15), moderate (GCS 9–12), and severe (GCS ≤8). This tripartite division is embedded in clinical practice and research; however, it does not fully capture the heterogeneity within the divisions such as the detailed neurological exam and clinical information. Consequently, therapeutic nihilism may result in patients with presumed “severe” injuries while disabling complaints and symptoms may be disregarded in patients with presumed “mild” injuries. 4 –6 Under the direction of the National Institute of Neurological Disorders and Stroke (NINDS), the TBI Classification and Nomenclature Workshop in Bethesda, USA, in January 2024 was convened as part of the international initiative to develop and implement more precise approaches to TBI classification. 7
In preparation of this workshop, the working group on clinical assessment considered the relative value of using the total GCS score (3–15) or the GCS–Pupils (GCS–P) score for classifying the clinical severity of TBI. The GCS–P was proposed in 2018, in which one point is deducted from the total GCS score for each unreactive pupil, resulting in a score from 1 to 15. 8,9 Both the total GCS and pupillary reactivity are important factors to guide clinical decision-making, as lower scores corroborate greater injury severity and consequently are associated with poorer outcome. Moreover, the GCS (or its motor component) and pupillary reactivity are key components of well-validated TBI prognostic models using large multi-institutional datasets, such as the International Mission for Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (IMPACT) and Corticosteroid Randomization after Significant Head Injury (CRASH) models. 10 –12
Studies in patients with moderate to severe TBI from the IMPACT and CRASH datasets showed that merging the GCS and pupillary reactivity into the GCS–P may yield comparable prognostic information compared with using these two factors separately. 8,9 It is, however, uncertain if this remains consistent across all severities. The current study aimed to analyze the performance of the GCS–P and the GCS and pupillary reactivity as separate features (GCS+P) for outcome prediction across the spectrum of TBI severity (GCS 3–15) from two large, recently completed multi-institutional datasets encompassing patients with acute TBI from Europe, Israel, and the United States.
Methods
Study population
We analyzed data from two prospectively enrolling observational cohorts: the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) and the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) studies. 13,14 CENTER-TBI enrolled patients presenting to one of 65 participating centers across Europe and Israel between 2014 and 2017. TRACK-TBI enrolled patients presenting to one of 18 U.S. Level 1 trauma centers between 2014 and 2019 through convenience sampling. CENTER-TBI and TRACK-TBI are registered on ClinicalTrials.gov (number NCT02210221 and NCT02119182, respectively). Inclusion and exclusion criteria for these two studies are publicly available. 13 –16
All adults (≥18 years) with a TBI recruited to these two studies were included in the current analysis. Exclusion criteria were missing the motor component of the initial GCS score or pupillary reactivity upon emergency department (ED) admission or missing the 6-month Glasgow Outcome Scale–Extended (GOS-E) scores.
GCS−P and pupillary reactivity
In CENTER-TBI, initial GCS and pupillary reactivity were defined using IMPACT methodology as the most recent non-missing value between ED discharge (post-stabilization) and pre-hospital assessment. Untestable eye (swelling) and verbal (intubation) components of the GCS were imputed with the number “1.” 17 In TRACK-TBI, initial GCS and pupillary reactivity were defined as the assessment at ED presentation. Missing GCS eye and verbal components were imputed as follows:
In case only verbal score is untestable: Total GCS = 0.55 + 1.45*[eye]+1.44*[mot].
In case both eye and verbal score are untestable: Total GCS = 0.6 + 2.4*[mot].
Extensive information and reasoning regarding imputation strategies are publicly available for both cohorts. 13,15,17
The total GCS was analyzed as an ordinal scale between 3 (lowest score) and 15 (highest score). Pupillary reactivity was expressed using the Pupil Reactivity Score (PRS), which was scored as both reactive, one reactive, and none reactive, resulting in a score of 0, −1, or −2, respectively. The GCS and PRS were combined into an integrated GCS–P score in accordance with the predefined methodology from the source study using the GCS–P, which subtracted the PRS from the GCS, yielding scores from 1 to 15. 8
Outcomes
Patient functional outcome was expressed using the GOS-E scale at 6 months post-injury. GOS-E consists of an 8-point scale ranging from 1 (death) to 8 (upper good recovery, i.e., back to baseline functional status). 18 GOS-E of 2 (vegetative state) and 3 (lower severe disability) were merged as these could not be differentiated on assessments performed by postal questionnaire. Primary outcomes were death and unfavorable outcome at 6 months. Unfavorable outcome was defined as GOS-E of 1–4 (death, vegetative state, or severe disability). In CENTER-TBI, missing outcomes at 6 months postinjury were imputed using a multinomial model if assessments at one or more other time points were available. 13 In TRACK-TBI, only patients with available GOS-E scores at 6 months were included.
Statistical analysis
Logistic regression modeling was used to analyze the relationships between GCS, PRS, GCS–P, and patient outcome (GOS-E and mortality). Nagelkerke’s pseudo R 2 was used as primary measure to quantify the prognostic capability of the included parameters. 19 Nagelkerke’s R 2 is calculated at the log-likelihood scale. It is a measure of how much better the model fits the data compared with a model with no predictors. Nagelkerke’s R 2 can be interpreted as a measure of the proportion of variation explained in the dependent variable (the 6-month outcome) that is explained by the independent variables (predictors) in a logistic regression model. 20,21 The uncertainty of the R 2 estimate was quantified by bootstrap resampling (5000 repetitions). We estimated the increase in R 2, the ΔR 2, for GCS–P versus GCS models and GCS plus PRS (GCS+P) versus GCS–P models within each bootstrap sample. The distribution of bootstrapped R 2 estimates was used to estimate 95% confidence intervals (CIs) for R 2 and differences between R 2 estimates. A pooled estimate across the CENTER-TBI and TRACK-TBI studies was estimated with inverse variance weighting. The regression analyses estimated odds ratios (OR) and 95% CI. The OR indicates the ratio of the odds of a less favorable outcome (over more favorable outcome) per 1-point increase in the GCS, PRS, GCS–P, and GCS+P scales.
A subgroup analysis was performed to assess the prognostic capabilities (mortality and unfavorable outcome) of GCS+P and GCS–P versus GCS alone in patients with moderate to severe TBI (GCS 3–12). Moreover, an additional age-stratified subgroup analysis was performed on three different age-groups based on the age distribution in the cohorts, namely age <45, age 45–64, and age ≥65 years.
Statistical analysis was performed using R version 4.1.2. 22 Rather than p-values for statistical tests, 95% CIs were provided throughout.
Results
Demographics and baseline characteristics
Overall, the CENTER-TBI and TRACK-TBI cohorts enrolled 4509 and 2552 patients, respectively; 3521 from CENTER-TBI and 1439 from TRACK-TBI subjects were eligible for the current study (Fig. 1).
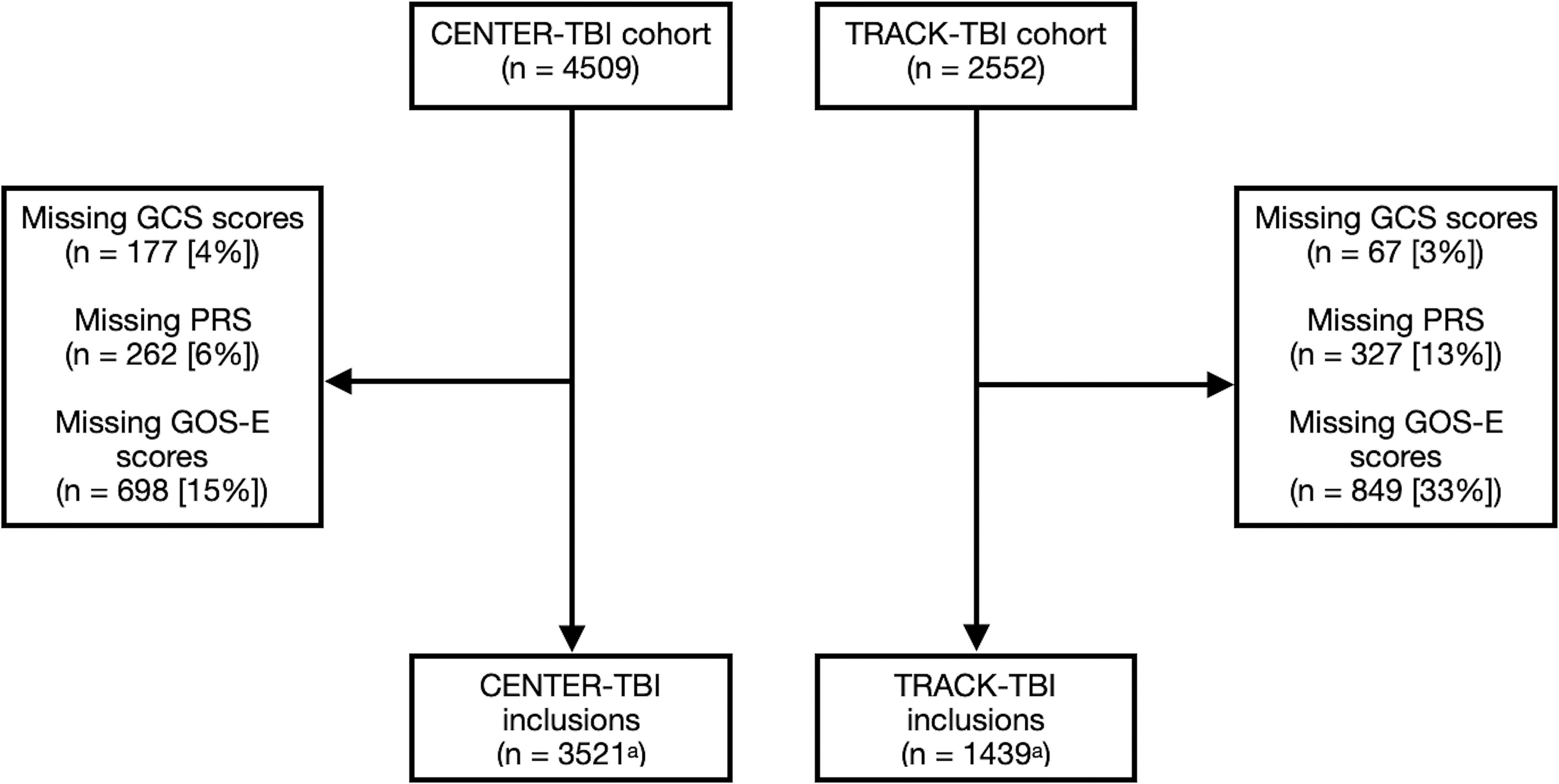
Flowchart of inclusions. CENTER-TBI, Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury; GCS, Glasgow Coma Scale; GOS-E, Glasgow Outcome Scale Extended; n, number; PRS, Pupil Reactivity Score; TRACK-TBI, Transforming Research and Clinical Knowledge in Traumatic Brain Injury. aTotal number of patients without any GCS, PRS, or GOS-E missing. Certain patients had both GCS and PRS or GOS-E scores missing and are therefore counted twice in the exclusion.
The included patients from both studies were similar in sex, median GCS, PRS, and computed tomography imaging variables such as the presence of epidural hematoma, acute subdural hematoma, traumatic subarachnoid hemorrhage, and diffuse axonal injury (DAI; Table 1). TRACK-TBI patients were generally younger than CENTER-TBI patients (median age: 39 years vs 51 years, respectively). Furthermore, mild TBI was more frequent in TRACK-TBI (78%) patients compared with CENTER-TBI (67%). Moreover, cerebral contusions (36% and 25%, respectively) and midline shift (16% and 11%, respectively) were more prevalent in CENTER-TBI compared with TRACK-TBI, respectively.
Baseline Patient Characteristics
Defined as midline shift more than 5 mm.
CENTER-TBI, Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury; DAI, diffuse axonal injury; GCS, Glasgow Coma Scale; GOS-E, Glasgow Outcome Scale Extended; IQR, interquartile range; No, number; TRACK-TBI, Transforming Research and Clinical Knowledge in Traumatic Brain Injury.
Distribution of outcomes
Mortality and unfavorable outcome occurred more in CENTER-TBI (12% and 25%) versus TRACK-TBI (7% and 14%). However, there were no large differences in the distribution of unfavorable outcome and mortality per GCS and PRS and within GCS–P scores (Supplementary Table S1 and S2). In CENTER-TBI, a small decrease in mortality at both GCS and GCS–P = 7 and 8 was observed while mortality increased again at GCS and GCS–P = 9 (Fig. 2). Moreover, low GCS–P (1–2) displayed higher percentages of mortality and unfavorable outcome compared with low GCS (3–4). Mild and moderate TBI displayed similar distributions (Fig. 2). In TRACK-TBI, low GCS–P (1–2) displayed lower mortality percentages at 6 months compared with CENTER-TBI (Fig. 2 and Supplementary Table S3).

Distribution of mortality versus GCS and GCS-P in CENTER-TBI (left) and TRACK-TBI (right). GCS, Glasgow Coma Scale; GCS−P, Glasgow Coma Scale−Pupils.
Associations of GCS−P and PRS with outcome
The explained variance was higher for the regression model containing GCS+P (R 2 30% and 35%; Table 2) as separate predictors compared with the model containing GCS–P (R 2 27% and 33%) for mortality in both CENTER-TBI and TRACK-TBI, respectively (Fig. 3).

Overall prognostic model performance. GCS, Glasgow Coma Scale; GCS−P, Glasgow Coma Scale−Pupils.
Overall Prognostic Performance of Different Regression Models
Estimates and bracketed 95% CI are bootstrapped unless mentioned otherwise.
ΔR 2 values are based on the model containing only GCS.
CENTER-TBI, Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury; CI, confidence interval; GCS, Glasgow Coma Scale; GCS−P, Glasgow Coma Scale−Pupils; Mo, month; No, number; PRS, Pupil Reactivity Score; TRACK-TBI, Transforming Research and Clinical Knowledge in Traumatic Brain Injury.
A model containing only GCS had the lowest model performance in CENTER-TBI and TRACK-TBI (R 2 24% and 30%, respectively). GCS had a lower range of predicted risks compared with GCS–P and GCS+P (Supplementary Fig. S1). Regarding unfavorable outcome, explained variance was highest in the model containing GCS+P as separate predictors compared with GCS–P in both CENTER-TBI and TRACK-TBI (GCS+P: R 2 32% and 40% and GCS–P: R 2 31% and 39%, respectively; Table 2). Moreover, a model containing only GCS had the lowest model performance in both cohorts (R 2 29% and 38% for CENTER-TBI and TRACK-TBI, respectively). In a meta-analysis, pupils as a separate variable improved the R 2 by an absolute value of 6% and 2% for mortality and unfavorable outcome, with half the improvement captured in the GCS–P score (3% and 1%, respectively; Table 2, Figs. 3 and 4).

Forest plot of R 2 values between cohort studies. CENTER-TBI, Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury; GCS, Glasgow Coma Scale; GCS−P, Glasgow Coma Scale—Pupils; PRS, Pupil Reactivity Score; TRACK-TBI, Transforming Research and Clinical Knowledge in Traumatic Brain Injury.
For both cohorts, in a logistic regression model containing GCS, an incremental 1-point increase in GCS significantly decreased the odds for mortality within 6 months after injury (OR 0.79, 95% CI 0.77–0.81 and OR 0.75, 95% CI 0.72–0.79 for CENTER-TBI and TRACK-TBI, respectively; Table 3). Similarly, more favorable GCS–P showed comparable odds ratios in both CENTER-TBI and TRACK-TBI (OR 0.79, 95% CI 0.77–0.81 and OR 0.76, 95% CI 0.73–0.79, respectively). In a model with GCS+P, incremental 1-point decreases in PRS decreased the odds of mortality more strongly (OR 0.40, 95% CI 0.33–0.45 and OR 0.43, 95% CI 0.32–0.58 for CENTER-TBI and TRACK-TBI, respectively) than the odds for GCS (OR 0.84, 95% CI 0.82–0.86 and 0.80, 95% CI 0.76–0.85).
Odds Ratios and Logistic Regression Coefficients of Baseline Variables Predicting Outcome
Odds ratios are expressed using decreases in PRS score, for example, lower number of unreactive equally lower odds of mortality and unfavorable outcome.
CENTER-TBI, Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury; CI, confidence interval; GCS, Glasgow Coma Scale; GCS−P, Glasgow Coma Scale−Pupils; IQR, interquartile range; Mo, month; No, number; PRS, Pupil Reactivity Score.
When predicting unfavorable outcome (GOS-E 1–4) using comparable models, similar associations were found (Table 3). Again, in a model with GCS+P, a poorer PRS was more strongly associated with a lower odds of unfavorable outcome in both CENTER-TBI and TRACK-TBI patients (OR 0.50, 95% CI 0.42–0.59 and OR 0.56, 95% CI 0.42–0.76, respectively) than a lower GCS score (OR 0.81, 95% CI 0.79–0.83 and OR 0.77, 95% CI 0.74–0.8, respectively).
Subgroup analysis
In the subgroup of 1161 patients in CENTER-TBI and 317 patients in TRACK-TBI with moderate and severe TBI (GCS 3–12), strong correlations were confirmed for GCS–P, GCS, and GCS+P with similar differences in explained variability (Supplementary Table S4, Supplementary Fig. S2). In the age-stratified subgroups, similar differences in explained variability between GCS–P, GCS, and GCS+P were found, with greater explained variance in younger patients in CENTER-TBI and older patients in TRACK-TBI (Supplementary Table S4).
Discussion
This study confirmed that across all prognostic models explored, pupillary reactivity adds important prognostic information over the GCS. Including PRS above GCS separately had the greatest increment in prognostic performance for mortality and unfavorable outcome (ΔR 2 6% and 2%), with half of this increase captured by GCS–P (ΔR 2 3% and 1%).
These results are consistent with findings reported by the original GCS–P paper using the IMPACT and CRASH cohorts. 8 In these studies, the addition of PRS to GCS as separate predictors (i.e., the GCS+P) in a regression model had a ΔR 2 of 4.0% and 3.2% with a ΔR 2 of 3.4% and 2.2% between GCS and GCS–P for mortality and unfavorable outcome, respectively. 8,9 The authors of the Original Articles suggested that the GCS–P is a valuable summary score over the GCS alone. Our study confirms that the GCS+P provides an incremental advantage in prognostic information across the full spectrum of TBI severity (GCS 3–15). The replication of these results in our main analysis and subgroup analyses is remarkable in the presence of disparities between cohorts. A major difference is the fraction of patients with mild and moderate TBI (GCS >8): 78% in CENTER-TBI and 67% in TRACK-TBI compared with 21% in the combined IMPACT and CRASH cohorts. 11 Patients in the original IMPACT and CRASH cohorts were considerably younger compared with CENTER-TBI and TRACK-TBI, with the median age in CENTER-TBI over 20 years higher than the median age in IMPACT. 11 Pupillary abnormalities were also more common in the IMPACT cohort.
Subgroup analyses
Comparable with the primary analysis, we observed similar trends in the prognostic information from GCS+P and GCS–P in the subgroup analysis on patients with moderate and severe TBI (GCS 3–12). Differences in explained variance between groups were more pronounced in moderate and severe TBI and among younger patients (Supplementary Table S4).
Pros and cons of a summary score
Simplifications of the GCS inevitably convey less information and therefore loss of clinical value. Such considerations hold, for example, for the trichotomy of the GCS into mild, moderate, and severe categories versus use of the full ordinal GCS sum score, but also to the GCS sum score compared with use of the underpinning eye, motor, and verbal components, as their cumulative prognostic value is higher than that of the sum score alone. 23
The integration of multiple clinical characteristics into a single score attempts to provide a single integrated articulation of TBI severity and status, without substantial loss of information. A balance should be sought between loss of information and practical utility. A strength of the GCS–P is that it combines two of the most relevant clinical predictors for TBI into a summary score and yet maintains the simplicity and ease of use of the GCS. Relative disadvantages include some loss of information compared with the use of PRS as a separate predictor. Its utility as an overall parameter of injury severity is influenced by its additional value in patients with moderate to severe TBI. However, the subtraction of PRS from the GCS across the entire GCS range potentially reduces efficacy when nonreactive pupils occur at higher GCS scores. We also recognize implementation barriers, which may be substantial when introducing a modification of the GCS, which is deeply embedded in clinical practice.
Importantly, different contributions from unreactive pupils and motor responses may add up to identical GCS–P scores but may have widely different clinical import and outcome. For example, a patient with a GCS of 3 and two reactive pupils (GCS–P = 3) may indeed have a very severe brain injury but could also have relatively less severe injury with examination confounded by alcohol, residual sedative drugs or a post-ictal state. However, a patient who has extensor motor responses and one unreactive pupil (E1 V1 M2 P-1) would be more uniformly likely to have a severe brain injury. Indeed, despite a small sample size and missing combinations, a comparison of outcomes of categories equaling a GCS–P score of 3 confirmed the variability in outcome in the first category, and a more dominant poor outcome in the second (Supplementary Table S2). Similarly, differences in type of severe brain injuries and lesions might also result in different prognosis with identical GCS−P scores, such as DAIs without brain herniation versus with brain herniation and brainstem compression.
On balance, we consider the superiority of the GCS–P over the GCS modest, and from a prognostic perspective, scoring of GCS and pupillary reactivity should be preferred. We further emphasize on a more general note that we would not recommend use of summary scores as replacements for the separate assessment of neurological status using GCS and PRS in individual patients. 8
Study strengths and weaknesses
The major strength of this study is the thorough analysis of prospectively collected contemporary data from two large multicenter observational studies across all severities in different continents with standardized data collection. The broad inclusion criteria improve generalizability but potentially result in significant disparities between the CENTER-TBI and TRACK-TBI cohorts. 24 –26 CENTER-TBI patients were generally older and suffered more severe TBI compared with TRACK-TBI patients. These factors potentially delineate the apparent differences in mortality and unfavorable outcome between both cohorts. Care should be taken comparing the model performance between the CENTER-TBI and TRACK-TBI models. Discrepancies in case-mix, however, do not preclude comparative analysis of GCS versus GCS–P or GCS+P separately and may even increase generalizability.
Limitations of our study include the restriction of data collection to North America and Europe, while the majority of TBI worldwide occurs in low- and middle-income countries. Further limitations stem from its observational design with pragmatic data collection. We cannot exclude the possibility that some bias may have occurred by missing values. In CENTER-TBI, a derived baseline GCS score was used with imputation of missing GCS scores according to IMPACT methodology. In TRACK-TBI the GCS scores were always calculated using the GCS ED admission scores and only imputed if the motor score was available. 14
In conclusion, the GCS–P has a stronger association with outcome after TBI than the GCS alone, and provides a single integrated score. However, this comes at a loss of clinical and prognostic information compared with the GCS+P. For prognostic models, inclusion of GCS and pupillary reactivity as separate factors may be preferable to the use of a GCS–P summary score.
Transparency, Rigor, and Reproducibility Summary
CENTER-TBI and TRACK-TBI are pre-registered at clinicaltrials.gov (number NCT02210221 and NCT02119182, respectively). 1 The analysis plan for the current study was presented in a protocol available on: https://www.center-tbi.eu/data/approved-proposals.2 The sample size was the available one from both cohort studies, namely, 4509 subjects in CENTER-TBI and 2552 subjects in TRACK-TBI. After excluding patients with missing data in crucial predictor and outcome variables, 3521 and 1439 subjects were included from CENTER-TBI and TRACK-TBI, respectively. 3,4 Data were labeled using Global Unique Patient Identifier codes. 5 CENTER-TBI included patients between 2014 and 2017, and TRACK-TBI enrolled patients between 2014 and 2019. 6 Data were analyzed using R version 4.1.2. All equipment and software used to perform analysis are publicly available from: https://www.R-project.org. 7 The key prognostic factors used in the current study are established standards in the neurosurgical field. 8 Statistical analysis was supervised by well-known statistical expert in the field of TBI research and prognostic modeling. 9 Missing data have been handled in CENTER-TBI using imputation according to IMPACT methodology and using motor score-based imputation in TRACK-TBI, as reported in the methods. Extensive methodology statements of both CENTER-TBI and TRACK-TBI are publicly available, as stated and referenced to in the methods. 9 This report serves as an external validation of an earlier study on the GCS–P score in the IMPACT and CRASH cohorts. 11 Data and analytic code from this study are available upon reasonable request to the study authors, after approval by the management teams of CENTER-TBI and TRACK-TBI. Packages used for coding are publicly available on GITHUB. Common Data Elements used are based on the NIH Common Data Elements for TBI (https://www.commondataelements.ninds.nih.gov/Traumatic%20Brain%20Injury). 12,13 The authors agree to provide the full content of the article on request by contacting the corresponding author.
Footnotes
Acknowledgments
The authors would like to gratefully thank The Clinical Assessment Work Group of the NIH-NINDS on classification and nomenclature of TBI and the CENTER-TBI and TRACK-TBI participants and investigators listed below.
The Clinical Assessment Work Group of the NIH-NINDS
Workgroup Leads: Adam R Ferguson, University of California San Francisco; David K Menon, University of Cambridge; Noah D Silverberg, University of British Columbia.
Workgroup Members: Thomas J Bayuk, HCOS/NICoE/WRNMMC; Matt Breiding, Centers for Disease Control and Prevention; David L Brody, Uniformed Services University of the Health Sciences; Todd A Cesar, TBICoE DHA; Scott A Cota, TBICoE DHA; Ari Ercole, University of Cambridge; Anthony Figaji, University of Cape Town; Guoyi Gao, Capital Medical University, Beijing; Christopher Giza, University of California Los Angeles; Fiona Lecky, University of Sheffield; Rebekah Mannix, Boston Children’s Hospital; Kasey Moritz, Combat Casualty Care Research Program; Claudia S Robertson, Baylor College of Medicine; John Yue, University of California San Francisco.
Affiliate Members: Shubhayu Bhattacharyay, University of Cambridge; Carl Marincowitz, University of Sheffield; Ana Mikolic, University of British Columbia; Abel Torres-Espin, University of Waterloo; Spyridoula Tsetsou, Baylor College of Medicine.
CENTER-TBI Participants and Investigators (to be Indexed as “Collaborators” in PubMed)
Cecilia Åkerlund, Department of Physiology and Pharmacology, Section of Perioperative Medicine and Intensive Care, Karolinska Institutet, Stockholm, Sweden; Krisztina Amrein, János Szentágothai Research Centre, University of Pécs, Pécs, Hungary; Nada Andelic, Division of Clinical Neuroscience, Department of Physical Medicine and Rehabilitation, Oslo University Hospital and University of Oslo, Oslo, Norway; Lasse Andreassen, Department of Neurosurgery, University Hospital Northern Norway, Tromso, Norway; Audny Anke, Department of Physical Medicine and Rehabilitation, University Hospital Northern Norway, Tromso, Norway; Anna Antoni, Trauma Surgery, Medical University Vienna, Vienna, Austria; Gérard Audibert, Department of Anesthesiology & Intensive Care, University Hospital Nancy, Nancy, France; Philippe Azouvi, Raymond Poincare hospital, Assistance Publique—Hopitaux de Paris, Paris, France; Maria Luisa Azzolini, Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy; Ronald Bartels, Department of Neurosurgery, Radboud University Medical Center, Nijmegen, The Netherlands; Pál Barzó, Department of Neurosurgery, University of Szeged, Szeged, Hungary; Romuald Beauvais, International Projects Management, ARTTIC, Munchen, Germany; Ronny Beer, Department of Neurology, Neurological Intensive Care Unit, Medical University of Innsbruck, Innsbruck, Austria; Bo-Michael Bellander, Department of Neurosurgery & Anesthesia & Intensive Care Medicine, Karolinska University Hospital, Stockholm, Sweden; Antonio Belli, NIHR Surgical Reconstruction and Microbiology Research Centre, Birmingham, UK; Habib Benali, Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France; Maurizio Berardino, Department of Anesthesia & ICU, AOU Città della Salute e della Scienza di Torino-Orthopedic and Trauma Center, Torino, Italy; Luigi Beretta, Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy; Morten Blaabjerg, Department of Neurology, Odense University Hospital, Odense, Denmark; Peter Bragge, Behaviour Works Australia, Monash Sustainability Institute, Monash University, Victoria, Australia; Alexandra Brazinova, Department of Public Health, Faculty of Health Sciences and Social Work, Trnava University, Trnava, Slovakia; Vibeke Brinck, Quesgen Systems Inc., Burlingame, California, USA; Joanne Brooker, Australian & New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia; Camilla Brorsson, Department of Surgery and Perioperative Science, Umeå University, Umeå, Sweden; Andras Buki, Department of Neurosurgery, Medical School, University of Pécs, Hungary and Neurotrauma Research Group, János Szentágothai Research Centre, University of Pécs, Hungary; Monika Bullinger, Department of Medical Psychology, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany; Manuel Cabeleira, Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Alessio Caccioppola, Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Emiliana Calappi, Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Maria Rosa Calvi, Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy; Peter Cameron, ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia; Guillermo Carbayo Lozano, Department of Neurosurgery, Hospital of Cruces, Bilbao, Spain; Marco Carbonara, Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Simona Cavallo, Department of Anesthesia & ICU, AOU Città della Salute e della Scienza di Torino-Orthopedic and Trauma Center, Torino, Italy; Giorgio Chevallard, NeuroIntensive Care, Niguarda Hospital, Milan, Italy; Arturo Chieregato, NeuroIntensive Care, Niguarda Hospital, Milan, Italy; Giuseppe Citerio, School of Medicine and Surgery, Università Milano Bicocca, Milano, Italy, and NeuroIntensive Care Unit, Department Neuroscience, IRCCS Fondazione San Gerardo dei Tintori, Monza, Italy; Hans Clusmann, Department of Neurosurgery, Medical Faculty RWTH Aachen University, Aachen, Germany; Mark Coburn, Department of Anesthesiology and Intensive Care Medicine, University Hospital Bonn, Bonn, Germany; Jonathan Coles, Department of Anesthesia & Neurointensive Care, Cambridge University Hospital NHS Foundation Trust, Cambridge, UK; Jamie D. Cooper, School of Public Health & PM, Monash University and The Alfred Hospital, Melbourne, Victoria, Australia; Marta Correia, Radiology/MRI department, MRC Cognition and Brain Sciences Unit, Cambridge, UK; Amra Čović, Institute of Medical Psychology and Medical Sociology, Universitätsmedizin Göttingen, Göttingen, Germany; Nicola Curry, Oxford University Hospitals NHS Trust, Oxford, UK; Endre Czeiter, Department of Neurosurgery, Medical School, University of Pécs, Hungary and Neurotrauma Research Group, János Szentágothai Research Centre, University of Pécs, Hungary; Marek Czosnyka, Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Claire Dahyot-Fizelier, Intensive Care Unit, CHU Poitiers, Potiers, France; Paul Dark, University of Manchester NIHR Biomedical Research Centre, Critical Care Directorate, Salford Royal Hospital NHS Foundation Trust, Salford, UK; Helen Dawes, Movement Science Group, Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK; Véronique De Keyser, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Vincent Degos, Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France; Francesco Della Corte, Department of Anesthesia & Intensive Care, Maggiore Della Carità Hospital, Novara, Italy; Hugo den Boogert, Department of Neurosurgery, Radboud University Medical Center, Nijmegen, The Netherlands; Bart Depreitere, Department of Neurosurgery, University Hospitals Leuven, Leuven, Belgium; Đula Đilvesi, Department of Neurosurgery, Clinical Centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia; Abhishek Dixit, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Emma Donoghue, Australian & New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia; Jens Dreier, Center for Stroke Research Berlin, Charité—Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany; Guy-Loup Dulière, Intensive Care Unit, CHR Citadelle, Liège, Belgium; Ari Ercole, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Patrick Esser, Movement Science Group, Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK; Erzsébet Ezer, Department of Anaesthesiology and Intensive Therapy, University of Pécs, Pécs, Hungary; Martin Fabricius, Departments of Neurology, Clinical Neurophysiology and Neuroanesthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; Valery L. Feigin, National Institute for Stroke and Applied Neurosciences, Faculty of Health and Environmental Studies, Auckland University of Technology, Auckland, New Zealand; Kelly Foks, Department of Neurology, Erasmus MC, Rotterdam, the Netherlands; Shirin Frisvold, Department of Anesthesiology and Intensive care, University Hospital Northern Norway, Tromso, Norway; Alex Furmanov, Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel; Pablo Gagliardo, Fundación Instituto Valenciano de Neurorrehabilitación (FIVAN), Valencia, Spain; Damien Galanaud, Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France; Dashiell Gantner, ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia; Guoyi Gao, Department of Neurosurgery, Shanghai Renji hospital, Shanghai Jiaotong University/school of medicine, Shanghai, China; Pradeep George, Karolinska Institutet, INCF International Neuroinformatics Coordinating Facility, Stockholm, Sweden; Alexandre Ghuysen, Emergency Department, CHU, Liège, Belgium; Lelde Giga, Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia; Ben Glocker, Department of Computing, Imperial College London, London, UK; Jagoš Golubovic, Department of Neurosurgery, University Hospitals Leuven, Leuven, Belgium; Pedro A. Gomez, Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain; Johannes Gratz, Department of Anesthesia, Critical Care and Pain Medicine, Medical University of Vienna, Austria; Benjamin Gravesteijn, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Francesca Grossi, Department of Anesthesia & Intensive Care, Maggiore Della Carità Hospital, Novara, Italy; Russell L. Gruen, College of Health and Medicine, Australian National University, Canberra, Australia; Deepak Gupta, Department of Neurosurgery, Neurosciences Centre & JPN Apex trauma centre, All India Institute of Medical Sciences, New Delhi-110029, India; Juanita A. Haagsma, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Iain Haitsma, Department of Neurosurgery, Erasmus MC, Rotterdam, the Netherlands; Raimund Helbok, Department of Neurology, Neurological Intensive Care Unit, Medical University of Innsbruck, Innsbruck, Austria; Eirik Helseth, Department of Neurosurgery, Oslo University Hospital, Oslo, Norway; Lindsay Horton, Division of Psychology, University of Stirling, Stirling, UK; Jilske Huijben, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Peter J. Hutchinson, Division of Neurosurgery, Department of Clinical Neurosciences, Addenbrooke’s Hospital & University of Cambridge, Cambridge, UK; Bram Jacobs, Department of Neurology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands; Stefan Jankowski, Neurointensive Care, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK; Mike Jarrett, Quesgen Systems Inc., Burlingame, California, USA; Ji-yao Jiang, Karolinska Institutet, INCF International Neuroinformatics Coordinating Facility, Stockholm, Sweden; Faye Johnson, Salford Royal Hospital NHS Foundation Trust Acute Research Delivery Team, Salford, UK; Kelly Jones, National Institute for Stroke and Applied Neurosciences, Faculty of Health and Environmental Studies, Auckland University of Technology, Auckland, New Zealand; Mladen Karan, Department of Neurosurgery, Clinical Centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia; Angelos G. Kolias, Division of Neurosurgery, Department of Clinical Neurosciences, Addenbrooke’s Hospital & University of Cambridge, Cambridge, UK; Erwin Kompanje, Department of Intensive Care and Department of Ethics and Philosophy of Medicine, Erasmus Medical Center, Rotterdam, The Netherlands; Daniel Kondziella, Departments of Neurology, Clinical Neurophysiology and Neuroanesthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark; Evgenios Kornaropoulos, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Lars-Owe Koskinen, Department of Clinical Neuroscience, Neurosurgery, Umeå University, Umeå, Sweden; Noémi Kovács, Hungarian Brain Research Program-Grant No. KTIA_13_NAP-A-II/8, University of Pécs, Pécs, Hungary; Ana Kowark, Department of Anaesthesiology, University Hospital of Aachen, Aachen, Germany; Alfonso Lagares, Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain; Linda Lanyon, Karolinska Institutet, INCF International Neuroinformatics Coordinating Facility, Stockholm, Sweden; Steven Laureys, Cyclotron Research Center, University of Liège, Liège, Belgium; Fiona Lecky, Centre for Urgent and Emergency Care Research (CURE), Health Services Research Section, School of Health and Related Research (ScHARR), University of Sheffield, Sheffield, UK, and Emergency Department, Salford Royal Hospital, Salford UK; Didier Ledoux, Cyclotron Research Center, University of Liège, Liège, Belgium; Rolf Lefering, Institute of Research in Operative Medicine (IFOM), Witten/Herdecke University, Cologne, Germany; Valerie Legrand, VP Global Project Management CNS, ICON, Paris, France; Aurelie Lejeune, Department of Anesthesiology-Intensive Care, Lille University Hospital, Lille, France; Leon Levi, Department of Neurosurgery, Rambam Medical Center, Haifa, Israel; Roger Lightfoot, Department of Anesthesiology & Intensive Care, University Hospitals Southampton NHS Trust, Southampton, UK; Hester Lingsma, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Andrew I.R. Maas, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Ana M. Castaño-León, Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain; Marc Maegele, Cologne-Merheim Medical Center (CMMC), Department of Traumatology, Orthopedic Surgery and Sport Medicine, Witten/Herdecke University, Cologne, Germany; Marek Majdan, Department of Public Health, Faculty of Health Sciences and Social Work, Trnava University, Trnava, Slovakia; Alex Manara, Intensive Care Unit, Southmead Hospital, Bristol, Bristol, UK; Geoffrey Manley, Department of Neurological Surgery, University of California, San Francisco, California, USA; Costanza Martino, Department of Anesthesia & Intensive Care, M. Bufalini Hospital, Cesena, Italy; Hugues Maréchal, Intensive Care Unit, CHR Citadelle, Liège, Belgium; Julia Mattern, Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Catherine McMahon, Department of Neurosurgery, The Walton centre NHS Foundation Trust, Liverpool, UK; Béla Melegh, Department of Medical Genetics, University of Pécs, Pécs, Hungary; David Menon, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Tomas Menovsky, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Ana Mikolic, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Benoit Misset, Cyclotron Research Center, University of Liège, Liège, Belgium; Visakh Muraleedharan, Karolinska Institutet, INCF International Neuroinformatics Coordinating Facility, Stockholm, Sweden; Lynnette Murray, ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia; Ancuta Negru, Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania; David Nelson, Department of Physiology and Pharmacology, Section of Perioperative Medicine and Intensive Care, Karolinska Institutet, Stockholm, Sweden; Virginia Newcombe, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Daan Nieboer, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; József Nyirádi, János Szentágothai Research Centre, University of Pécs, Pécs, Hungary; Otesile Olubukola, Centre for Urgent and Emergency Care Research (CURE), Health Services Research Section, School of Health and Related Research (ScHARR), University of Sheffield, Sheffield, UK; Matej Oresic, School of Medical Sciences, Örebro University, Örebro, Sweden; Fabrizio Ortolano, Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy; Aarno Palotie, Institute for Molecular Medicine Finland, University of Helsinki, Helsinki, Finland, Analytic and Translational Genetics Unit, Department of Medicine; Psychiatric & Neurodevelopmental Genetics Unit, Department of Psychiatry; Department of Neurology, Massachusetts General Hospital, Boston, MA, USA, and Program in Medical and Population Genetics; The Stanley Center for Psychiatric Research, The Broad Institute of MIT and Harvard, Cambridge, MA, USA; Paul M. Parizel, Department of Radiology, University of Antwerp, Edegem, Belgium; Jean-François Payen, Department of Anesthesiology & Intensive Care, University Hospital of Grenoble, Grenoble, France; Natascha Perera, International Projects Management, ARTTIC, Munchen, Germany; Vincent Perlbarg, Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France; Paolo Persona, Department of Anesthesia & Intensive Care, Azienda Ospedaliera Università di Padova, Padova, Italy; Wilco Peul, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Anna Piippo-Karjalainen, Department of Neurosurgery, Helsinki University Central Hospital; Matti Pirinen, Institute for Molecular Medicine Finland, University of Helsinki, Helsinki, Finland; Dana Pisica, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Horia Ples, Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania; Suzanne Polinder, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Inigo Pomposo, Department of Neurosurgery, Hospital of Cruces, Bilbao, Spain; Jussi P. Posti, Division of Clinical Neurosciences, Department of Neurosurgery and Turku Brain Injury Centre, Turku University Hospital and University of Turku, Turku, Finland; Louis Puybasset, Department of Anesthesiology and Critical Care, Pitié -Salpêtrière Teaching Hospital, Assistance Publique, Hôpitaux de Paris and University Pierre et Marie Curie, Paris, France; Andreea Radoi, Neurotraumatology and Neurosurgery Research Unit (UNINN), Vall d’Hebron Research Institute, Barcelona, Spain; Arminas Ragauskas, Department of Neurosurgery, Kaunas University of technology and Vilnius University, Vilnius, Lithuania; Rahul Raj, Department of Neurosurgery, Helsinki University Central Hospital; Malinka Rambadagalla, Department of Neurosurgery, Rezekne Hospital, Latvia; Isabel Retel Helmrich, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Jonathan Rhodes, Department of Anaesthesia, Critical Care & Pain Medicine NHS Lothian & University of Edinburg, Edinburgh, UK; Sylvia Richardson, Director, MRC Biostatistics Unit, Cambridge Institute of Public Health, Cambridge, UK; Sophie Richter, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Samuli Ripatti, Institute for Molecular Medicine Finland, University of Helsinki, Helsinki, Finland; Saulius Rocka, Department of Neurosurgery, Kaunas University of technology and Vilnius University, Vilnius, Lithuania; Cecilie Roe, Department of Physical Medicine and Rehabilitation, Oslo University Hospital/University of Oslo, Oslo, Norway; Olav Roise, Division of Orthopedics, Oslo University Hospital, Oslo, Norway, and Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway; Jonathan Rosand, Broad Institute, Cambridge MA Harvard Medical School, Boston MA, Massachusetts General Hospital, Boston MA, USA; Jeffrey V. Rosenfeld, National Trauma Research Institute, The Alfred Hospital, Monash University, Melbourne, Victoria, Australia; Christina Rosenlund, Department of Neurosurgery, Odense University Hospital, Odense, Denmark; Guy Rosenthal, Department of Neurosurgery, Hadassah-Hebrew University Medical Center, Jerusalem, Israel; Rolf Rossaint, Department of Anaesthesiology, University Hospital of Aachen, Aachen, Germany; Sandra Rossi, Department of Anesthesia & Intensive Care, Azienda Ospedaliera Università di Padova, Padova, Italy; Daniel Rueckert, Department of Computing, Imperial College London, London, UK; Martin Rusnák, International Neurotrauma Research Organisation, Vienna, Austria; Juan Sahuquillo, Neurotraumatology and Neurosurgery Research Unit (UNINN), Vall d’Hebron Research Institute, Barcelona, Spain; Oliver Sakowitz, Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany, and Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany; Renan Sanchez-Porras, Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany; Janos Sandor, Division of Biostatistics and Epidemiology, Department of Preventive Medicine, University of Debrecen, Debrecen, Hungary; Nadine Schäfer, Institute of Research in Operative Medicine (IFOM), Witten/Herdecke University, Cologne, Germany; Silke Schmidt, Department Health and Prevention, University Greifswald, Greifswald, Germany; Herbert Schoechl, Department of Anaesthesiology and Intensive Care, AUVA Trauma Hospital, Salzburg, Austria; Guus Schoonman, Department of Neurology, Elisabeth-TweeSteden Ziekenhuis, Tilburg, the Netherlands; Rico Frederik Schou, Department of Neuroanesthesia and Neurointensive Care, Odense University Hospital, Odense, Denmark; Elisabeth Schwendenwein, Trauma Surgery, Medical University Vienna, Vienna, Austria; Charlie Sewalt, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Ranjit D. Singh, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Toril Skandsen, Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology, NTNU, Trondheim, Norway, and Department of Physical Medicine and Rehabilitation, St.Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Peter Smielewski, Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Abayomi Sorinola, Department of Neurosurgery, University of Pécs, Pécs, Hungary; Emmanuel Stamatakis, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Simon Stanworth, Oxford University Hospitals NHS Trust, Oxford, UK; Robert Stevens, Division of Neuroscience Critical Care, John Hopkins University School of Medicine, Baltimore, USA; William Stewart, Department of Neuropathology, Queen Elizabeth University Hospital and University of Glasgow, Glasgow, UK; Ewout W. Steyerberg, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands, and Dept. of Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, The Netherlands; Nino Stocchetti, Department of Pathophysiology and Transplantation, Milan University, and Neuroscience ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy; Nina Sundström, Department of Radiation Sciences, Biomedical Engineering, Umeå University, Umeå, Sweden; Riikka Takala, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital and University of Turku, Turku, Finland; Viktória Tamás, Department of Neurosurgery, University of Pécs, Pécs, Hungary; Tomas Tamosuitis, Department of Neurosurgery, Kaunas University of Health Sciences, Kaunas, Lithuania; Mark Steven Taylor, Department of Public Health, Faculty of Health Sciences and Social Work, Trnava University, Trnava, Slovakia; Aurore Thibaut, Cyclotron Research Center, University of Liège, Liège, Belgium; Braden Te Ao, National Institute for Stroke and Applied Neurosciences, Faculty of Health and Environmental Studies, Auckland University of Technology, Auckland, New Zealand; Olli Tenovuo, Division of Clinical Neurosciences, Department of Neurosurgery and Turku Brain Injury Centre, Turku University Hospital and University of Turku, Turku, Finland; Alice Theadom, National Institute for Stroke and Applied Neurosciences, Faculty of Health and Environmental Studies, Auckland University of Technology, Auckland, New Zealand; Matt Thomas, Intensive Care Unit, Southmead Hospital, Bristol, Bristol, UK; Dick Tibboel, Intensive Care and Department of Pediatric Surgery, Erasmus Medical Center, Sophia Children’s Hospital, Rotterdam, The Netherlands; Marjolein Timmers, Department of Intensive Care and Department of Ethics and Philosophy of Medicine, Erasmus Medical Center, Rotterdam, The Netherlands; Christos Tolias, Department of Neurosurgery, Kings college London, London, UK; Tony Trapani, ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia; Cristina Maria Tudora, Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania; Andreas Unterberg, Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Peter Vajkoczy, Neurologie, Neurochirurgie und Psychiatrie, Charité—Universitätsmedizin Berlin, Berlin, Germany; Shirley Vallance, ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia; Egils Valeinis, Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia; Zoltán Vámos, Department of Anaesthesiology and Intensive Therapy, University of Pécs, Pécs, Hungary; Mathieu van der Jagt, Department of Intensive Care Adults, Erasmus MC– University Medical Center Rotterdam, Rotterdam, the Netherlands; Gregory Van der Steen, Department of Neurosurgery, Antwerp University Hospital and University of Antwerp, Edegem, Belgium; Joukje van der Naalt, Department of Neurology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands; Jeroen T.J.M. van Dijck, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Inge A. M. van Erp, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Thomas A. van Essen, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Wim Van Hecke, icoMetrix NV, Leuven, Belgium; Caroline van Heugten, Movement Science Group, Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK; Dominique Van Praag, Psychology Department, Antwerp University Hospital, Edegem, Belgium; Ernest van Veen, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Thijs Van de Vyvere, icoMetrix NV, Leuven, Belgium; Roel P. J. van Wijk, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Alessia Vargiolu, NeuroIntensive Care Unit, Department Neuroscience, IRCCS Fondazione San Gerardo dei Tintori, Monza, Italy; Emmanuel Vega, Department of Anesthesiology-Intensive Care, Lille University Hospital, Lille, France; Kimberley Velt, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Jan Verheyden, icoMetrix NV, Leuven, Belgium; Paul M. Vespa, Director of Neurocritical Care, University of California, Los Angeles, USA; Anne Vik, Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology, NTNU, Trondheim, Norway, and Department of Neurosurgery, St.Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Rimantas Vilcinis, Department of Neurosurgery, Kaunas University of Health Sciences, Kaunas, Lithuania; Victor Volovici, Department of Neurosurgery, Erasmus MC, Rotterdam, the Netherlands; Nicole von Steinbüchel, Institute of Medical Psychology and Medical Sociology, Universitätsmedizin Göttingen, Göttingen, Germany; Daphne Voormolen, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Rick J.G. Vreeburg, Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands; Petar Vulekovic, Department of Neurosurgery, Clinical Centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia; Kevin K.W. Wang, Department of Emergency Medicine, University of Florida, Gainesville, Florida, USA; Daniel Whitehouse, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Eveline Wiegers, Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Guy Williams, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Lindsay Wilson, Division of Psychology, University of Stirling, Stirling, UK; Stefan Winzeck, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Stefan Wolf, Department of Neurosurgery, Charité—Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany; Zhihui Yang, Broad Institute, Cambridge MA Harvard Medical School, Boston MA, Massachusetts General Hospital, Boston MA, USA; Peter Ylén, VTT Technical Research Centre, Tampere, Finland; Alexander Younsi, Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Frederick A. Zeiler, Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK, and Section of Neurosurgery, Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, Canada; Veronika Zelinkova, Department of Public Health, Faculty of Health Sciences and Social Work, Trnava University, Trnava, Slovakia; Agate Ziverte, Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia; Tommaso Zoerle, Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy.
TRACK-TBI Investigators (to be Indexed as “Collaborators” in PubMed)
Neeraj Badjatia, Department of Neurology, University of Maryland, Baltimore, Maryland, USA; Jason Barber, Department of Neurological Surgery, University of Washington, Seattle, Washington, USA; Yelena G. Bodien, Department of Neurology, Harvard Medical School, Boston, Massachusetts, USA; Brian Fabian, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Adam R. Ferguson, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Brandon Foreman, Department of Neurology, University of Cincinnati, Cincinnati, Ohio, USA; Raquel C. Gardner, Department of Neurology, University of California, San Francisco, San Francisco, California, USA; Shankar Gopinath, Department of Neurological Surgery, Baylor College of Medicine, Houston, Texas, USA; Ramesh Grandhi, Department of Neurological Surgery, University of Utah Medical Center; Salt Lake City, Utah, USA; J. Russell Huie, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; C. Dirk Keene, Department of Laboratory Medicine and Pathology, University of Washington, Seattle, Washington, USA; Hester F. Lingsma, Department of Public Health, Erasmus Medical Center, Rotterdam, The Netherlands; Christine L. Mac Donald, Department of Neurological Surgery, University of Washington, Seattle, Washington, USA; Amy J. Markowitz, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Randall Merchant, Department of Anatomy, Virginia Commonwealth University, Richmond, Virginia, USA; Laura B. Ngwenya, Department of Neurological Surgery, University of Cincinnati, Cincinnati, Ohio, USA; Richard B. Rodgers, Department of Neurosurgery, Goodman Campbell Brain and Spine, Indianapolis, Indiana, USA; Andrea L. C. Schneider, Department of Neurology, University of Pennsylvania, Philadelphia, PA, USA; David M. Schnyer, Department of Psychology, University of Texas at Austin, Austin, Texas, USA; Sabrina R. Taylor, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Nancy R. Temkin, Department of Neurological Surgery, University of Washington, Seattle, Washington, USA; Abel Torres-Espin, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Mary J. Vassar, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Kevin K. W. Wang, Department of Neurobiology, Morehouse School of Medicine, Atlanta, Georgia, USA; Justin C. Wong, Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, USA; Ross D. Zafonte, Department of Rehabilitation Medicine, Harvard Medical School, Boston, Massachusetts, USA.
Authors’ Contributions
R.J.G.V.: Writing—original draft (lead), formal analysis (equal), methodology (supporting), visualization (lead), writing—review and editing (equal), and data curation (equal). F.D.v.L.: Formal analysis (equal), writing—review and editing (equal), methodology (supporting), writing—original draft (supporting), and data curation (equal). G.T.M.: Conceptualization (equal), writing—review and editing (equal), and supervision (equal). J.K.Y.: Writing—review and editing (equal). P.M.B.: Writing—review and editing (equal). X.S.: Formal analysis (equal) and writing—review and editing (equal). S.J.: Formal analysis (equal) and writing—review and editing (equal). T.A.v.E.: Writing—review and editing (equal), methodology (supporting), writing—original draft (supporting), and supervision (equal). W.C.P.: Conceptualization (equal), writing—review and editing (equal), and supervision (equal). A.I.R.M.: Conceptualization (equal), writing—review and editing (equal), and supervision (equal). D.K.M.: Conceptualization (equal), writing—review and editing (equal), and supervision (equal). E.W.S.: Conceptualization (equal), methodology (lead), writing—review and editing (equal), and supervision (equal).
Funding Information
CENTER-TBI was supported by the European Union 7th Framework Programme for Research (grant no.
Author Disclosure Statement
The authors declare no competing interests.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.