
Abstract
This narrative review addresses the critical issue of arterial transducer positioning for cerebral perfusion pressure (CPP) measurement in neurocritical care. Despite CPP’s importance in guiding management, optimal transducer placement remains ambiguous and unaddressed by current guidelines. We synthesized evidence from 20 relevant articles to inform standardization efforts. Key findings include a 10–12 mmHg CPP discrepancy between phlebostatic axis and Monro foramen transducer locations at 30° head elevation. There is no consensus on anatomical landmarks for “head-level” measurement, and only one guideline explicitly advises against the phlebostatic axis approach. Limited clinical evidence suggests increased institutionalization rates for patients with measurement discrepancies. Emerging dual-transducer strategies aim to address these challenges. The review highlights significant variability in CPP measurement practices, potentially impacting patient care and research interpretation. We emphasize the urgent need for standardized protocols and improved reporting in research. Addressing this variability is crucial for optimizing neurocritical care management and enhancing research comparability. Our findings underscore the importance of consistent arterial transducer positioning in neurocritical care and call for further research to establish evidence-based standardization, ultimately improving patient outcomes and research quality in this critical field.
Introduction
Cerebral perfusion pressure (CPP) is a key estimator of cerebral blood flow (CBF) in neurocritical care, determined by the difference between mean arterial pressure (MAP) and intracranial pressure (ICP). 1 In neurocritical illness, autoregulatory dysfunction is common, potentially altering or abolishing the correlation between CPP values and adequate CBF. 2 Maintaining appropriate CPP levels may aid in preventing secondary cerebral ischemia and cellular dysfunction. 3
Cerebral autoregulation, both static and dynamic, plays a crucial role in maintaining CBF across a range of perfusion pressure. 4 Static autoregulation refers to the steady-state relationship between CBF and CPP, while dynamic autoregulation describes the rapid response of cerebral blood vessels to transient changes in blood pressure. 5 In neurocritical care patients, impaired autoregulation makes the brain more vulnerable to changes in systemic blood pressure, emphasizing the importance of accurate CPP measurement 6 due to its availability as a neuromonitoring tool (Fig. 1).

Cerebral autoregulation curves in normal and pathological states. Panel A illustrates static autoregulation, showing the classical curve and various alterations seen in neurocritical care scenarios. These include complete loss of autoregulation, displacement of the curve (as in chronic hypertension), reduced autoregulation range, and altered autoregulation points due to acute brain injury. The x-axis represents mean arterial pressure (MAP) in millimeters of mercury, while the y-axis shows cerebral blood flow (CBF) in milliliters per 100 grams per minute. Panel B demonstrates dynamic aspects of autoregulation. The top graph shows fluctuations in optimal cerebral perfusion pressure (CPP) over time. The bottom graph, labeled “Cerebral Autoregulation Evolution,” displays overlapping curves representing how static autoregulation can vary between patients or change over time in critical conditions. Image created using BioRender. Giglio, A. (2025) https://BioRender.com/humw494.
Invasive arterial blood pressure monitoring in critically ill patients is routinely performed along the phlebostatic axis, a standardized and widely adopted approach. 7 However, when patient positioning deviates from the supine position (e.g., 30° head-of-bed elevation), 8 the downward pressure exerted by the fluid column is altered. An average heart-to-head distance of 30 cm results in a differential pressure of ∼6 mmHg at a 15° incline and ∼11 mmHg at 30°. 9,10 Furthermore, a 45° head elevation can generate a 16 mmHg MAP difference between the atrium and Monro foramen. 9 Exposing to the already described over- and undertreatment. 11,12 However, an absolute MAP does not consider vascular autoregulation, which is frequently impaired in brain injury, 6,13,14 while it can be preserved in the rest of the body, protecting it from potential overtreatment harm.
The optimal arterial line transducer position for CPP measurement in patients with elevated head-of-bed remains ambiguous and is not addressed by current guidelines. 8 This results in potential CPP differences of up to 12 mmHg depending on the reference level used. 9 Such variability raises concerns and presents a barrier to consistency in CPP-targeted management for individual patient care and in the published literature. A recent survey done in the Latin American Brain Injury Consortium found that experts were equally divided (50/50) on the preferred measurement level for arterial line transducers in neurocritical care.
This narrative review aims to summarize the current evidence on arterial transducer positioning in neurocritical care patients to inform appropriate standardization considerations. We will address six key questions: (1) Reported differences in CPP values according to measurement location, (2) Definition of “head-level” measurement, (3) Summary of transducer placement in existing clinical guidelines, (4) Evaluation of potential clinical impact of transducer location on patient outcomes, (5) Two-transducer strategies, and (6) Assessment of protocol needs for standardizing transducer placement.
Methodology
A literature review was conducted using PubMed and Google Scholar databases to identify relevant publications from the past 30 years (1994–2024) addressing arterial transducer positioning and CPP measurements in neurocritical care patients. The search strategy employed combinations of key terms including “Arterial Pressure,” “Cerebrovascular Circulation,” “Brain Injuries,” “Intracranial Pressure,” and “Neurophysiological Monitoring.”
The review included original research articles, systematic reviews, clinical guidelines, and position statements that discussed arterial line positioning protocols, measurement techniques, or their impact on neurocritical care management. Three independent reviewers assessed the abstracts and full texts of potentially relevant articles. Articles were included if they contained information about: Arterial line positioning protocols in neurocritical care Impact of measurement location on CPP values Clinical outcomes related to arterial line positioning Recommendations for standardization of measurements Technical considerations for accurate pressure monitoring
Given the historical variability in reporting standards and the lack of standardized protocols across institutions, we chose a narrative review approach rather than a systematic review methodology. This approach allowed for a more comprehensive exploration of the evolving understanding and practices in the field. Twenty articles were ultimately selected as representative of the current evidence base and clinical practices.
Our focus was to synthesize the available evidence through a qualitative analysis addressing our six predefined review goals rather than conducting a systematic assessment of intervention effects. This approach was deemed most appropriate given the heterogeneous nature of the available literature and the need to include expert opinion and technical considerations alongside empirical evidence.
Results
Narrative review goals synthesis
See Table 1.
Results Synthesis
CPP, cerebral perfusion pressure; NACCS, Neuro Anaesthesia and Critical Care Society; SBNS, Society of British Neurological Surgeons.
Reported differences in CPP values according to the measurement location
Invasive arterial blood pressure monitoring in critically ill patients is routinely performed along the phlebostatic axis, a standardized and widely adopted approach. 7 However, when patient positioning deviates from the supine position (e.g., 30° head-of-bed elevation), 8 the downward pressure exerted by the fluid column is altered (Fig. 2). An average heart-to-head distance of 30 cm results in a differential pressure of ∼6 mmHg at a 15° incline and ∼11 mmHg at 30°. 9,10 Furthermore, a 45° head elevation can generate a 16 mmHg MAP difference between the atrium and the Monro foramen, 9 exposing to the already described over- and undertreatment. 11,12 However, an absolute MAP does not consider vascular autoregulation, which is frequently impaired in brain injury, 6,13,14 while it can be preserved in the rest of the body, protecting it from potential overtreatment harm.
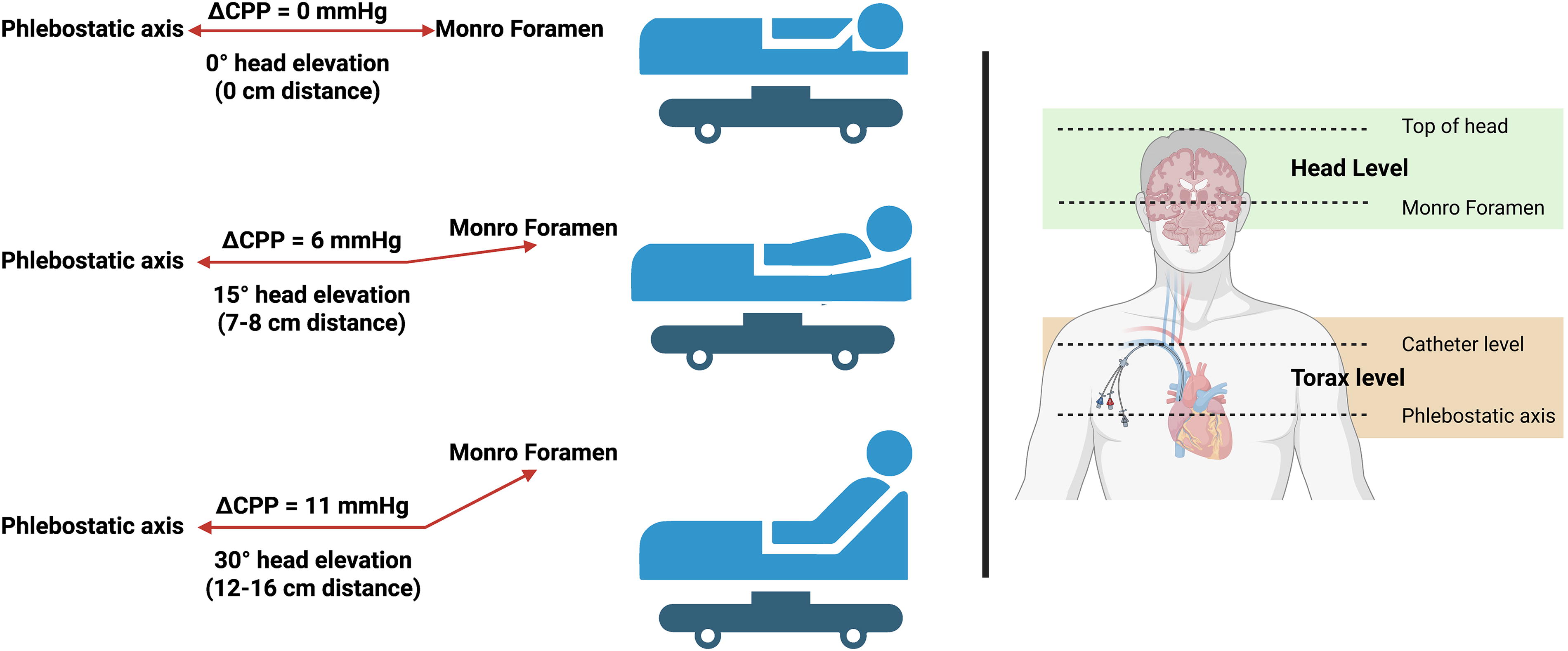
Graphical representation of cerebral perfusion pressure (CPP) differences based on transducer positioning and head elevation. The left panel illustrates how CPP measurements vary between phlebostatic axis and Monro foramen reference points at different head elevation angles (0°, 15°, and 30°). As head elevation increases, the pressure difference (ΔCPP) grows from 0 mmHg at 0° to 11 mmHg at 30° elevation. The right panel shows the anatomical reference points for arterial transducer placement, including top of head, Monro foramen, catheter level, and phlebostatic axis. Image created using BioRender. Giglio, A. (2025) https://BioRender.com/y9qy6bl.
As such, the 10–12 mmHg CPP discrepancy between the phlebostatic axis and head-level transducer locations is an expected consequence of standard neurocritical head positioning. 9 An isolated hydrostatic effect may contribute to conflicting perfusion adequacy interpretations if universal reference points are not defined. 9,15
What does “at head level” mean?
Although no definitive physiological rationale has been proven, some neurocritical recommendations advocate transducer measurement at the level of the head rather than the heart to better approximate cerebral conditions. 16
Most articles advocating a head-level reference point for zero calibration for arterial pressure line transducer when calculating CPP describe reference to the foramen of Monro based on an external anatomical landmark, such as tragus, or the external ear conduct level. This approach references a formative CBF analysis by Lassen published in 1959, which proposed the Monro foramen level as the ideal perfusion pressure site without substantive supporting evidence. 17
It is crucial to note that there is no consensus on which anatomical landmark best corresponds to the Monro foramen. 18 Nonetheless, many institutions opt for head-level monitoring using these surface landmarks. 9,11,15,17 This lack of agreement is further complicated by several factors. First, there are two foramina of Monro (left and right), and their position can be altered by midline shift, changes in ventricular size, 19 or mass effect lesions. Second, most external landmarks only approximate the Monro foramen’s location when the patient is supine with zero head elevation. 20 Magnetic resonance imaging (MRI) studies reveal ICP misestimations at the tragus when using it as a reference to the foramen of Monro, which increases according to head elevation and changes in head position. 20 The precision of these landmarks is further compromised by the specific location of intracranial lesions, whether frontal, temporal, basal ganglia, or elsewhere. A more reliable reference can be the top of the head, which consistently underestimates Monro foramen level CPP, a difference that can be corrected by providing a more accurate CPP measurement. 20
Summary of transducer placement in the existing clinical guidelines
Major neurocritical care guidelines provide limited direction regarding the standardization of arterial transducer positioning (Table 2). The 2016 Brain Trauma Foundation (BTF) guidelines include a chapter on CPP measurement in traumatic brain injury, but do not specify details on reference points for calculation. 8 Similarly, the Seattle International Traumatic Brain Injury Consensus Conference (2019–2020) discusses CPP targets and autoregulation-based management without recommendations on the zeroing methodology. 21,22 The seminal Lund Concept paper (2006) also lacks guidance regarding measurement locations. 23
Summary of Recommendations for Arterial Line Transducer Placement in Neurocritical Care Guidelines
NACCS, Neuro Anaesthesia and Critical Care Society; SIBICC, Seattle International Severe Traumatic Brain Injury Consensus Conference; SBNS, Society of British Neurological Surgeons.
In contrast, a consensus statement from the Neuro Anaesthesia and Critical Care Society and the Society of British Neurological Surgeons actively advises against the phlebostatic axis approach, citing hydrostatic effects. 16 As an alternative, they recommend transducer placement at the ear tragus to account for postural impacts on pressure; however, evidence underlying this recommendation is lacking. 16 Local guidelines follow similar expert reasoning, such as Winnipeg Regional Health Authority CPP protocol 24 or the Chilean intracranial hypertension protocols, 25 favoring ear tragus measurement without citing a rationale.
Evaluation of potential clinical impact of transducer location on patient outcomes
The discrepancy in pressure measurement of ∼10 mmHg between phlebostatic and approximated Monro foramen transducer locations presents conflicting theoretical harm scenarios. 9,10 Anchoring at the phlebostatic axis promotes systemic pressure conservatism, but at the expense of an estimated 10 mmHg CPP overestimation and 10 mmHg MAP underestimation. These estimation differences could mask insights into true perfusion-related risk for secondary brain injury. 9 Conversely, Monro foramen placement provides accurate cerebral calculations but requires higher systemic pressure targets, raising concerns about avoidable cardiac, renal, and other end-organ damage. 10
Currently, only one study by McNett et al. directly investigated the impact of this discrepancy on patient outcomes. 11 After confirming 10–12 mmHg measurement differences between the simultaneous suprasternal notch and tragus of ear recordings in head-elevated neurocritical patients, discordance was noted in 18.8% of cohort CPP values, the 60 mmHg CPP threshold goal was met at phlebostatic axis but showed under goal values for the Monro measures. 11 Importantly, no mortality difference was observed between the concordant and discordant groups. However, mismatch patients showed a significant increase in institutionalization requirements for recovery, suggesting that potentially unrecognized cerebral hypoperfusion impacted outcomes when phlebostatic measures were falsely reassuring. 11
Arterial waveform quality
While analyzing pulse waveform quality and monitoring methodology, the arterial pressure waveform exhibits marked variations depending on the measurement site and conditions. Dynamic properties of the measurement system are determined by the natural frequency (usually ranging from 12 to 25 Hz) and damping coefficient (optimal at 0.64), which together characterize the ability to accurately transmit the pressure signal. 7,26 The arterial pressure waveform’s shape changes significantly when moving from central to peripheral arteries due to wave reflection and arterial compliance, with systolic pressure typically higher and dicrotic notch lower and later in peripheral arteries. This effect is especially pronounced during conditions of hemodynamic instability or with high-dose vasopressors, where radial arterial pressure may significantly underestimate central pressure by 10–15 mmHg or more. 27 Studies comparing femoral versus radial measurements under conditions of shock have demonstrated significant discrepancies, with femoral measurements generally providing more reliable estimates of central arterial pressure in unstable conditions. 28 The quality and reliability of the arterial waveform must therefore be carefully assessed, as underdamped or overdamped signals can lead to significant errors in both systolic and diastolic pressure measurements while having less effect on MAP. Fast-flush testing should be performed regularly to evaluate the dynamic response characteristics of the system. 7,27
Two-transducer strategy
Recently proposed systems by two different authors utilized a dual-transducer approach connected to a single arterial line, with simultaneous real-time measurement at both the anatomical phlebostatic axis and an approximation of the Monro foramen, such as the tragus. 29,30 This split-signal method provides distinct systemic and cerebral perfusion data to enable more accurate CPP calculation as well as unaltered MAP for end-organ perfusion guidance. However, the implications of splitting a signal from a single source have not been fully investigated. The aim is to avoid conflicting clinical interpretations and treatment targets between hypotension at the Monro level and falsely elevated phlebostatic measures in standard care. 30 Although not yet clinically validated, dual-transducer CPP assessment theoretically accounts for postural impacts on pressure to provide enhanced detection of true cerebral perfusion adequacy and limits risks for under-resuscitation or over-escalation of vasopressors to address measurement variability. 29
Assessment of protocol needs for standardizing transducer placement
Currently, no universal protocols exist to standardize arterial transducer placement for CPP measurements in neurocritical patients. Both mainstream guidelines and local policies overwhelmingly fail to provide specific directives for appropriate reference points and methodology. 8,16,21 –25 This allows for significant variability in clinical practice. When asked to experts, like it was made by Park et al. (2024), the measurement level was 50% for each strategy. 31
This lack of consistency likely contributes to the discordant interpretations of perfusion adequacy and treatment targets in managing unstable patients. 32 It also reduces the credibility of published data, meta-analyses, and guideline recommendations if methodological variability spans the 10–12 mmHg magnitude of documented measurement discrepancies. 6 –8 Establishing clear protocols is an essential first step in optimizing patient care, enhancing research quality, evaluating relevant approaches, and informing future consensus guidelines. Whether preference is given to the phlebostatic axis versus the Monro foramen approximation, improved standardization of this common but complex monitoring technique is imperative.
Discussion
This review explored the current evidence regarding optimal arterial transducer positioning for CPP measurement in head-of-bed elevated neurocritical patients. We identified an expected 10–12 mmHg pressure discrepancy based on a standardized 30° elevation, with theoretical perfusion interpretation and treatment risks if the methods vary. 7,9 –12 Although anatomical approximations of the Monro foramen have been utilized, landmark offsets have also been reported. 9,11,15,17,20 Guidelines largely avoid specifics on techniques, while some expert reasoning favors the Monro approach. 8,21,22 Empirical clinical impact data remain limited, although one study found higher disability rates using phlebostatic methods. 11 Finally, early proposals exist for dual-transducer systems for integrated cerebral and systemic monitoring. 29,30
The phlebostatic axis approach centers the arterial transducer at the level of the right atrium. This allows for standardized arterial blood pressure interpretation and systemic monitoring of intensive care unit patients. However, with routine neurocritical head-of-bed elevation, a hydrostatic column is created between the heart and the brain. At 30°, this accounts for 10–12 mmHg of pressure loss, increasing to 16 mmHg at 45°. 9 As such, phlebostatic CPP calculations risk overlooking cerebral hypoperfusion by this margin. Still, systemic blood pressure management promotes cardiovascular stability in an already unstable patient. Determining the appropriate balance is challenging.
Alternatively, the anatomical approximation of the Monro foramen aims to achieve cerebral equivalence, which also has not been clearly defined as the cerebral zero, being planted, for example, as the cranial entry point of the carotid arteries as an alternative. Common external landmarks utilized are the tragus of the ear and the auditory canal. However, MRI studies revealed average offsets of 12 mmHg ICP overestimation at the tragus relative to invasive monitors. 20 Such offsets reduce the localized accuracy of noninvasive estimates. Nonetheless, this approach enhances the detection of cerebral perfusion adequacy and avoids occult ischemia. The trade-off is the requirement of higher systemic pressures to maintain ICP/CPP targets, which increases the risk of systemic injury. 12 These may have a cumulative impact on the recovery trajectories.
Proposals exist for integrated dual-pressure assessment, with simultaneous transducers placed at the anatomical phlebostatic axis and estimated Monro foramen. 29,30 This split-signal approach enables distinct interpretations of systemic and cerebral perfusion. Theoretically, it accounts for both tissue beds. However, clinical feasibility, signal accuracy, cost, and patient benefits require further evaluation before considering standardized adoption in guidelines or clinical practice. Its ultimate role, compared with consistent single-transducer placement, remains undetermined.
The results highlight a marked variability in clinical practice for a fundamental aspect of measuring and monitoring cerebral perfusion in unstable neurocritical patients. This likely contributed to the inconsistent interpretations and management plans. Formalizing protocols with staff education on specified methods, whether preference lies with the phlebostatic or estimated Monro foramen, will limit unnecessary practice variability. Complementing this, enhanced publication transparency enables an appropriate context for interpreting discordant values across institutions. If dual-transducer assessment demonstrates strong utility, selective augmentation in high-risk patients represents a transitional step toward standardization.
The available clinical evidence directly linking arterial transducer placement technique to patient outcomes remains very limited. Existing data primarily consist of theoretical perfusion risks rather than empirical outcome associations. The single observational study by McNett et al., while raising concerns, cannot justify definitive practice changes. 11 Reproduction of their findings is needed. However, there are inherent challenges in achieving consistent methodological approaches across institutions to enable adequate comparisons. Even the feasibility of dual-transducer assessment may be limited by added costs in resource-constrained settings.
Significant knowledge gaps persist around the clinical prioritization and standardization of techniques. Progress requires enhanced reporting transparency on measured value discrepancies between anatomical locations, the potential magnitude of occult hypoperfusion if cerebral measures are not utilized, and any differences in patient recovery trajectories or complications. Such granular observational data may reveal patterns that can guide adoption decisions. In addition, pragmatic clinical trials randomizing patients to phlebostatic versus Monro foramen arterial lines with CPP-guided therapy could directly evaluate outcomes, although for ethical reasons, would likely require an integrated monitoring approach. While CPP has been a cornerstone of neurocritical care management for decades, providing a surrogate for CBF, the relevance of pressure-guided perfusion is now evolving with advances in multimodality monitoring. Since the early 2000s, complementary techniques such as brain tissue oxygen tension, microdialysis, jugular bulb venous saturation assessment, and near-infrared spectroscopy have provided enhanced insights into cerebral oxygenation, metabolism, cellular dysfunction, and perfusion adequacy. 33 –35 Such tools provide direct visualization of the end physiological processes that CPP aims to optimize, giving the unique opportunity to compare the perfusion impact of both measurement strategies.
As such, CPP is transitioning from an end-point itself to one more component of a multimodal analysis approach, providing a deeper understanding of patient physiology. This multimodal approach challenges the traditional >60 mmHg CPP threshold, suggesting a need for more individualized targets based on patient-specific physiological responses. However, not all centers worldwide have full neuro-monitoring capabilities. Pressure metrics have invaluable roles in broader guidance. Therefore, it is essential to determine reliable and standardized CPP measurement techniques tailored to the level of monitoring resources. This underscores the need to enhance the consistency around arterial pressure transducer placement as a ubiquitous and fundamental monitoring practice. In parallel, the ongoing adoption of multimodal monitoring should integrate the CPP context to optimize the translation of physiology to patient care. Opportunities exist to develop cerebral autoregulation assessment that pairs CPP with newer modalities as a further advancement in precision care.
A 10 mmHg CPP difference has potential clinical relevance. The maximum difference of 10 mmHg proposed by BTF guidelines, 8 the evidence found as damaging for Robertson et al., 12 and also are the differences seen by McNett as the potential cause for the differences in outcome of neurocritical care patients. 11
Conclusions
This review synthesizes the existing literature on the complex issue of arterial transducer placement for CPP calculation, revealing theoretical risks but highlighting insufficient evidence definitively linking measurement practices to outcomes. Significant variability persists, likely contributing to discordant interpretations in published literature. Optimizing cerebral perfusion monitoring in neurocritical care requires a multi-faceted approach. Although CPP has been fundamental for decades, the emergence of complementary multimodality techniques now allows more direct visualization of oxygenation, metabolism, and perfusion adequacy to guide management decisions. Thus, standardized and reliable CPP assessments are essential. We advocate that institutions establish standardized protocols with unified education on either phlebostatic or estimated Monro foramen approaches to limit inconsistencies. Furthermore, we urge scientific societies and journals to mandate reporting of transducer placement in all relevant studies to facilitate meaningful comparisons. Addressing this clinical equipoise requires not only increased transparency in measurement reporting from clinical trials but also direct investigation of this topic through well-designed comparative studies. Determining a consistent arterial transducer methodology tailored to institutional monitoring resources remains a critical step in optimizing the care of vulnerable neurocritical patients.
Footnotes
Authors’ Contributions
All authors have approved the final article, agreed to be accountable for all aspects of the work, and acknowledge that all those entitled to authorship are listed as authors.
Ethical Approval
This kind of study does not need an ethical approval.
Data Availability
All data are available in published literature.
Declaration of Generative Artificial Intelligence and Artificial Intelligence-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used Claude artificial intelligence to improve the redaction of this article and graphic images. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Funding Information
This study did not have any financial source or support.
Author Disclosure Statement
None of the authors declares a conflict of interest with the content of this article.