
Abstract
While it is established that diffuse axonal injury (DAI) is a leading cause of death or disability among patients with traumatic brain injury (TBI), less is known about the frequency of DAI in patients with severe TBI (sTBI). Additionally, little is known about the mortality rate and proportion of males/females among patients with both sTBI and DAI. We conducted a systematic literature search in the databases EMBASE Ovid, PubMed, Scopus, and Web of Science Advance from inception until April 22, 2024. No filters or language restrictions were applied. Two reviewers (A.S. and P.S.) independently screened the obtained abstracts and full texts. We included full-text studies that reported the frequency of DAI after TBI or any measure of association between DAI and clinical outcome (e.g., death, Glasgow Outcome Scale). Animal studies, reviews, and non-original research articles were excluded. We qualitatively described the results of the included studies. Thirty-seven studies met our inclusion criteria: 18 retrospective, 18 prospective, and 1 was both retrospective and prospective, representing studies from 14 countries. Thirty-three were single-center studies, and four were multicenter. Five studies were exclusively conducted among pediatric patients, while the remaining 32 included adults. The pooled proportion of DAI among sTBI patients was 0.60 (95% confidence interval [CI]: 0.39, 0.78]), I 2 = 98%. The pooled mortality among patients with both sTBI and DAI is 0.16 [95% CI: 0.07, 0.30], I 2 = 12%. The pooled proportion of males among individuals with both sTBI and DAI was 0.81 [95% CI: 0.76, 0.85], I 2 = 46%. DAI is common in patients with sTBI. The comorbid state of having both sTBI and DAI can be life-threatening and is more often seen in males than females, possibly due to the increased tendency of males to partake in risky behaviors that increase the likelihood of head trauma. There might be a difference in outcome after DAI between the pediatric and adult patient populations, possibly due to increased plasticity of brain tissue in younger patients.
Introduction
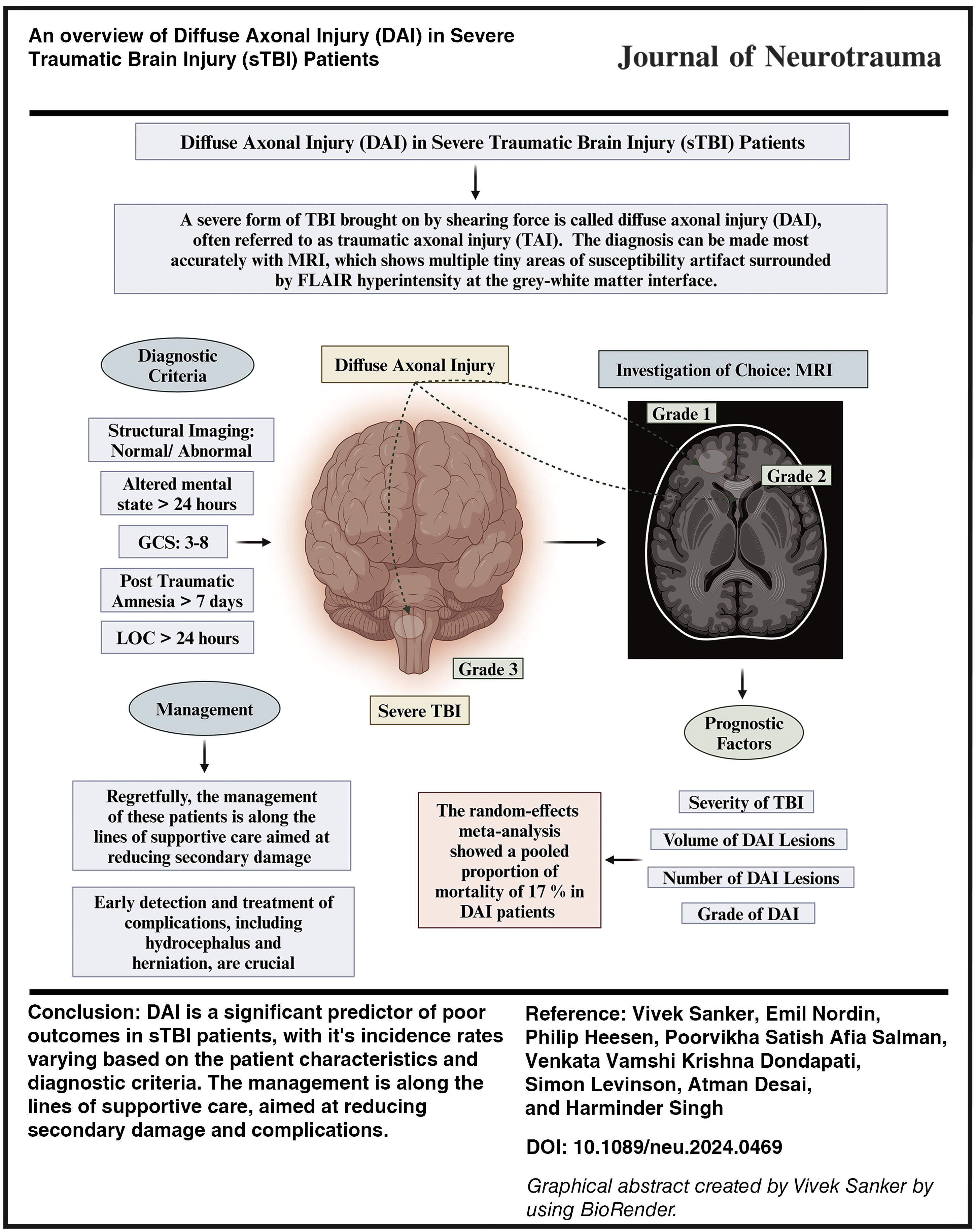
Globally, traumatic brain injury (TBI) stands as a leading cause of morbidity and disability. 1,2 TBI encompasses a broad spectrum of neurological deficits and associated complications. Within this spectrum, diffuse axonal injury (DAI) is particularly prevalent and associated with exceptionally high morbidity and mortality rates. 3 It is also an early predictor of neurological and functional outcomes. 4,5 DAI results from shearing injuries caused by traumatic acceleration–deceleration forces along multiple axes, directly injuring blood vessels and axons. 6 Despite its clinical significance, early diagnosis of DAI remains challenging. 1,7
Several grading schemes exist for DAI, with the most common based on the injury’s location. Stage I DAI lesions are limited to the cerebellum or lobar white. Stage II refers to lesions in the corpus callosum, with or without accompanying lobar white matter lesions. Stage III refers to the occurrence of traumatic lesions in the brainstem. 4 The Glasgow Coma Scale (GCS) is typically used to classify the degree of consciousness, which determines the severity of clinical damage during the acute phase. 8 In the treatment of TBI, the GCS score continues to be crucial in determining the time of diagnostic tests and treatment decisions. It has been demonstrated to be a significant predictor of functional prognosis. 9 The duration of post-traumatic amnesia is an additional measure of the severity. 10
Early diagnosis of DAI presents several challenges. Imaging limitations, subtle clinical symptoms that can easily be overlooked in acute trauma patients, distracting injuries, and the confounding effects of multiple intracranial injuries complicate the diagnostic process. The microscopic nature of axonal damage in DAI often goes undetected in traditional imaging techniques such as computed tomography scans. This necessitates the use of advanced imaging modalities such as magnetic resonance imaging (MRI), requiring specialized equipment and expertise that may not be universally available.
While it is challenging, an early diagnosis of DAI is crucial for multiple reasons. It helps predict clinical outcomes, guides treatment decisions, and optimizes rehabilitation strategies. Timely identification of DAI allows for tailored treatments that can prevent secondary brain injuries. Therefore, an early diagnosis can shorten hospital stays, reduce health care costs, improve patient care, and ultimately enhance the efficiency of health care resource allocation.
Previous research has predominantly focused on the relationship between DAI characteristics and clinical outcomes. However, few studies explicitly compare patient outcomes across different stages of DAI and the prevalence of DAI among sTBI patients. The existing studies often have imprecise results. 11 –13 While stage III DAI is generally associated with poor clinical outcomes, impacts of stages I and II are less well-defined due to a lack of consensus on the classification criteria for DAI. 14,15
The clinical factors associated with DAI outcomes remain uncertain. Some studies, 16 –18 though not all, 19,20 have demonstrated a correlation between the volume and number of DAI lesions and clinical prognosis, as well as the severity of TBI. To develop precision medicine approaches to TBI treatment, a comprehensive understanding of the natural history, mechanism, and pathophysiology of DAI is required. 21,22 The goal of this article is to systematically review and synthesize the existing literature on the frequency of DAI in patients with sTBI and to examine the association between DAI and gender, and clinical outcomes, such as mortality and functional recovery. This article aims to provide a comprehensive overview of the incidence of DAI among sTBI patients and to identify potential differences in outcomes between pediatric and adult populations.
Methodology
Search strategy
We searched PubMed, Scopus, Web of Science Advance, and Embase (Ovid) databases to identify relevant studies, using a search query with specific keywords such as “Diffuse axonal injury,” “severe traumatic brain injury,” and “prognosis” (Table 1). Individuals of all ages were considered. The objective was to identify studies reporting the frequency of DAI in patients with sTBI, along with associated outcomes. Studies that were either unrelated to sTBI or did not include patients with diagnosed DAI were excluded. Animal studies, reviews, and non-original research articles were also excluded from our analysis to ensure the inclusion of primary research data relevant to our objective. The electronic search ranged from the period’s earliest available date up to April 22, 2024.
The Adjusted Search Terms as per Searched Electronic Databases (as of April 22, 2024)
Screening of studies
The initial screening phase was led by two coauthors (A.S. and P.S.) responsible for assessing the articles’ suitability for subsequent review and data extraction. Each study’s title and abstract underwent independent assessment by at least two (A.S. and P.S.) reviewers. Any discrepancies were addressed through consultation with a third coauthor (V.S.) and further discussion with the entire team. The screening of studies adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Fig. 1).
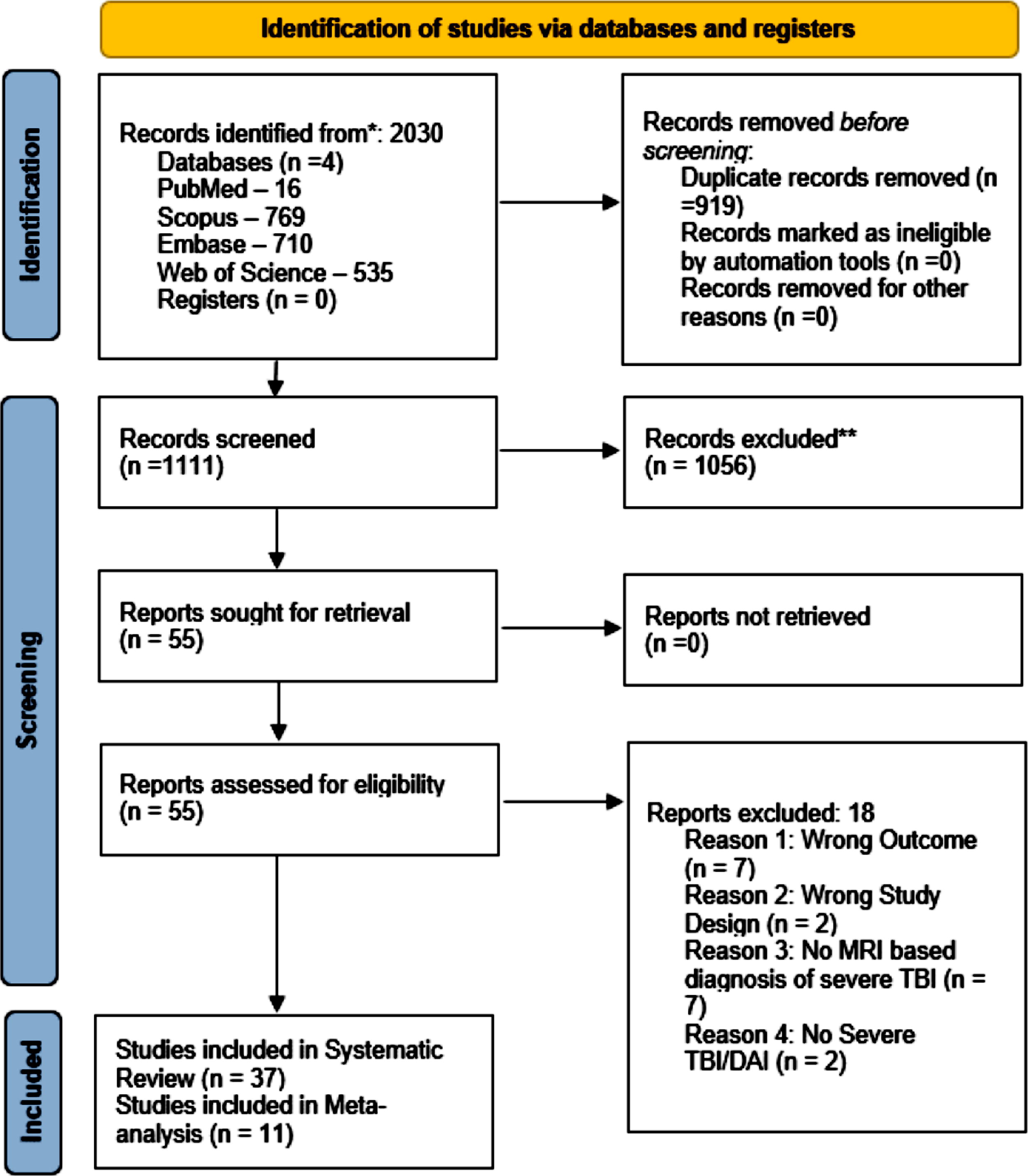
PRISMA flow diagram summarizing the article screening process for the review. DAI, diffuse axonal injury; MRI, magnetic resonance imaging; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; TBI, traumatic brain injury.
Data extraction
Four independent authors (E.N., A.S., P.S., and V.V.) extracted relevant data from selected studies. The data collected included study design, participant demographics, and the number of participants with respective outcomes and complications. Discrepancies in data extraction were resolved through consensus, and any unresolved disagreements were addressed by involving a third reviewer.
Data analysis
The statistical analysis was done using R statistical software (package “meta”). To determine the pooled proportion of DAI among sTBI patients, we only utilized data from studies in which DAI did not occur in all patients with sTBI (Fig. 2), ensuring that the data from studies where all the patients with sTBI also had DAI were excluded from this particular analysis. To determine the pooled proportion of mortality among patients with both sTBI and DAI, we only utilized data from studies where mortality data were available exclusively for patients who had both sTBI and DAI (Fig. 3). To determine the pooled proportion of males among individuals with both sTBI and DAI, we only utilized data from studies where we were able to determine the sex of the individuals with sTBI and DAI (Fig. 4). Study heterogeneity was assessed using I 2- and tau2-values. Heterogeneity ranges from 0% to 100% and is a measure of the variation in results between the studies being analyzed. High heterogeneity indicates considerable variability among studies included for analysis and that differences between study outcomes are not entirely due to chance but are influenced by actual variations in study characteristics such as populations, methodologies, inclusion criteria, exclusion criteria, diagnostic criteria, definitions, and clinical outcomes. 23 –26 A high level of heterogeneity necessitates a cautious interpretation of pooled results, as the average effect size may not accurately represent a single, definitive effect. Additionally, high heterogeneity limits the generalizability of findings, indicating that the results may not uniformly apply across all patient populations or clinical settings related to DAI in sTBI. There were no missing outcome data.
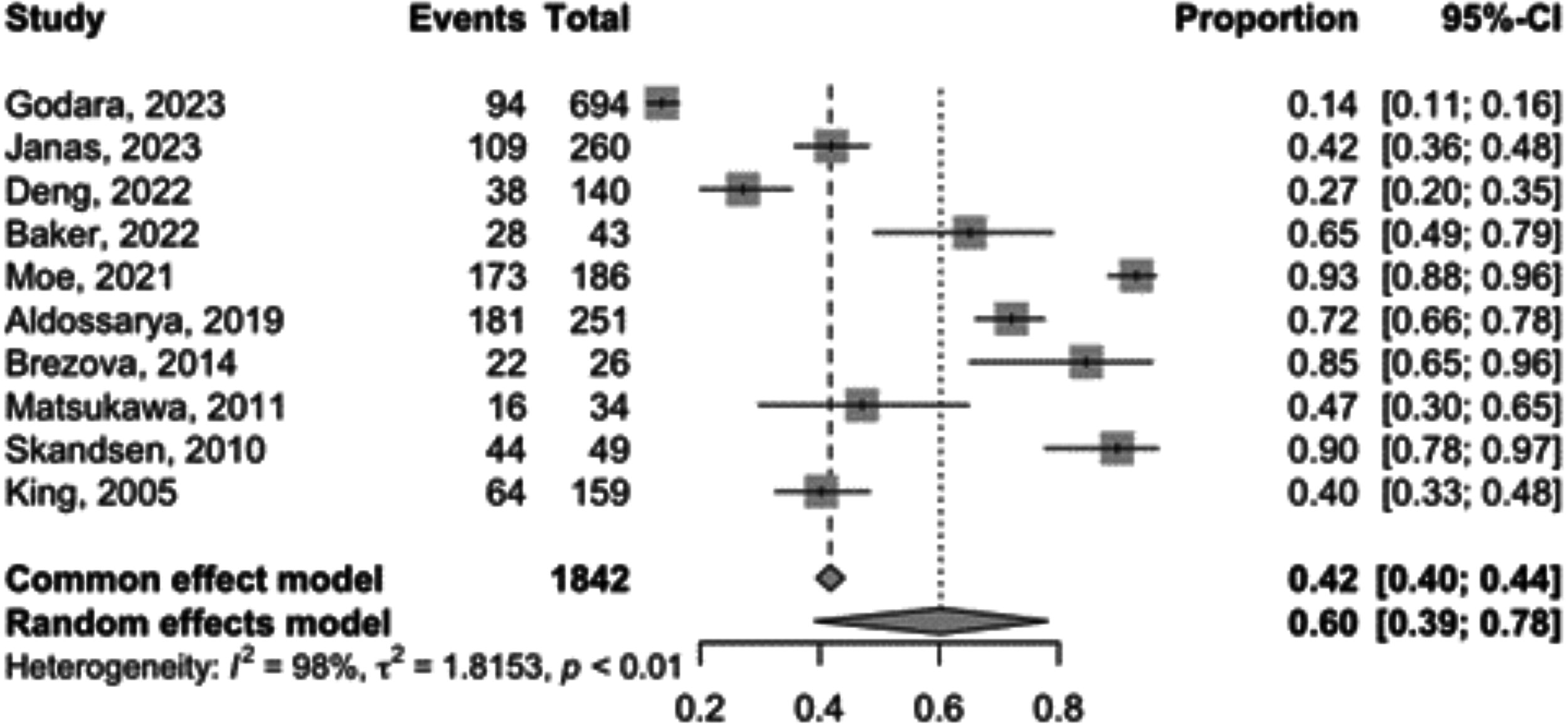
Forest plot depicting the pooled proportion of DAI in patients with sTBI. CI, confidence interval; DAI, diffuse axonal injury; sTBI, severe traumatic brain injury.

Forest plot depicting the pooled proportion of mortality in patients with both sTBI and DAI. CI, confidence interval; DAI, diffuse axonal injury; sTBI, severe traumatic brain injury.
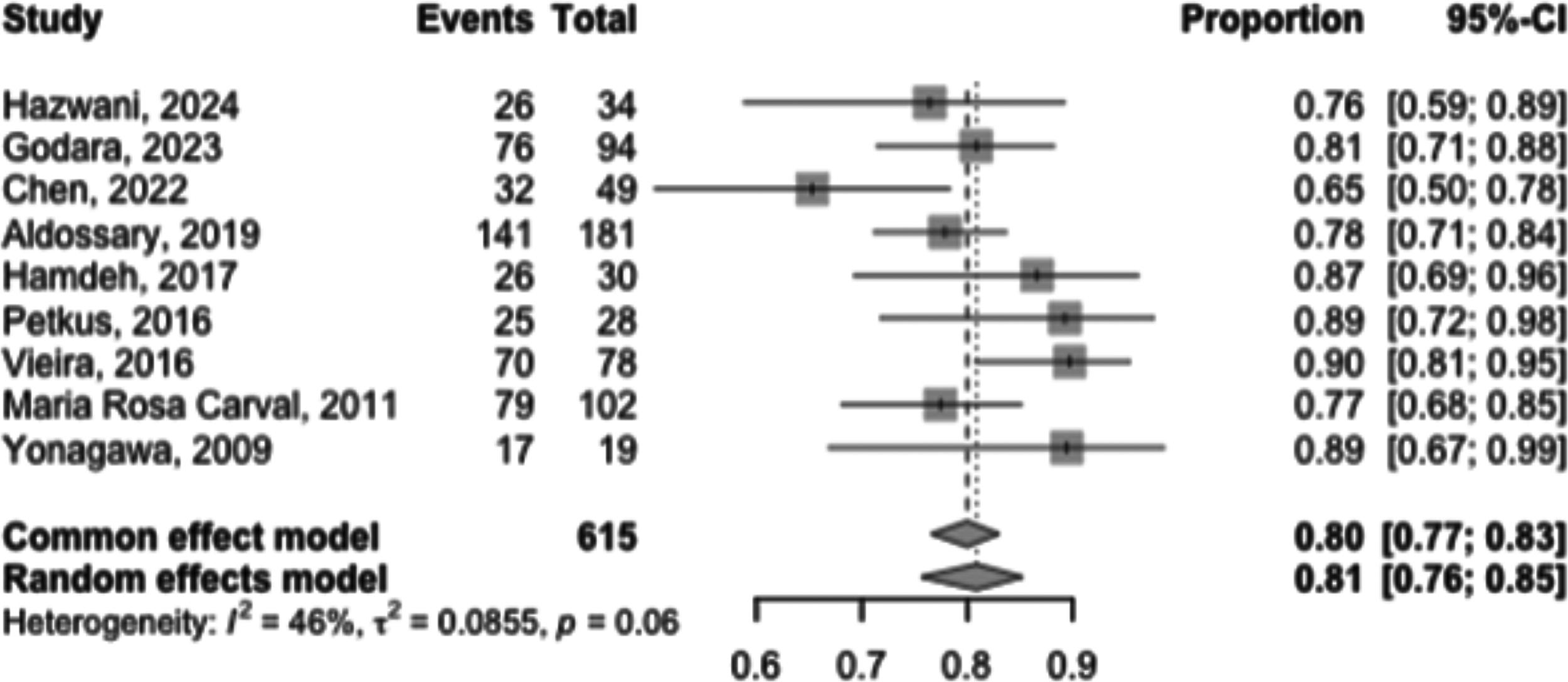
Forest plot depicting the pooled proportion of males among patients with sTBI and DAI. CI, confidence interval; DAI, diffuse axonal injury; sTBI, severe traumatic brain injury.
Quality assessment
The quality assessment was performed using the Risk of Bias In Non-randomized Studies - of Interventions (ROBINS-I) assessment tool for non-randomized studies. Each article was screened twice, and no article was excluded following the assessment (Table 2). The following bias domains were assessed: bias due to confounding (D1), bias due to selection of participants (D2), bias in classification of interventions (D3), bias due to deviation from intended interventions (D4), bias due to missing data (D5), bias in measurement of the outcome (D6), and bias in selection of the reported result (D7).
Summary of Quality Appraisal for the Included Studies Using the ROBINS-I Tool
Risk of bias domains: D1, bias due to confounding; D2, bias due to selection of participants; D3, bias in classification of interventions; D4, bias due to deviation from intended interventions; D5, bias due to missing data; D6, bias in measurement of the outcome; D7, bias in selection of the reported result;  , low risk of bias;
, low risk of bias;  , serious risk of bias;
, serious risk of bias;  , some concerns.
, some concerns.
The risk of bias assessment revealed that the majority of included studies had no or low risk of bias (22), while seven studies had some concerns.
Results
Thirty-seven studies met our inclusion criteria: 18 were retrospective, 18 were prospective, and 1 was both retrospective and prospective. Thirty-three were single-center studies, and four were multicenter. Five studies were exclusively conducted among pediatric patients, while the remaining 32 included adults. A total of 14 countries (United States, China, Brazil, India, Saudi Arabia, Pakistan, Sweden, Japan, Norway, Italy, Tunisia, South Korea, Lithuania, Netherlands) were represented across the 37 studies.
Systematic review
Thirty-seven studies (Table 3) met our inclusion criteria. The frequency of DAI after TBI varied widely according to the inclusion criteria of the primary studies. In patients with a clinical suspicion of DAI (i.e., patients with prolonged unconsciousness above 6 h), DAI occurred in as much as 80% of cases. In studies that included all patients with TBI, the DAI occurrence ranged from 3.5% to above 58%. The association between DAI and outcome was variable and mainly depended on the form of outcome measure used. One study, including 51 pediatric patients, even found that the improvement in the Pediatric Glasgow Outcome Scale–Extended was more pronounced in patients with DAI of Adams grades II and III compared to patients with DAI of Adams grade I or without DAI.
Summary of the Included Studies for Systematic Review
Pooled proportion of DAI in sTBI
Among the 2746 patients with sTBI we identified, 1607 had DAI. However, multiple studies only included patients with both sTBI and DAI. Therefore, to ensure our analysis of the pooled proportion of DAI among patients with sTBI remained unbiased, we excluded studies in which all patients had both sTBI and DAI for this particular analysis Table 4. Including such studies would have inaccurately represented the proportion of DAI among patients with sTBI by focusing solely on those who presented with both conditions. That left us with 1842 patients with sTBI, of which 769 had DAI. Using the random effect model to adjust for the between-study variance (heterogeneity; I 2 = 98%) with respect to the data presented in Figure 2, we found the pooled proportion of DAI among these 1842 patients with sTBI to be 0.60 [95% CI: 0.39, 0.78]. This suggests that among patients with sTBI, 60% have DAI.
Summary of the Included Studies for Meta-Analysis
CT, computed tomography; DAI, diffuse axonal injury; GCS, Glasgow Coma Scale; GOS, Glasgow Outcome Scale; GOS-E, Glasgow Outcome Scale–Extended; MRI, magnetic resonance imaging; TAI, traumatic axonal injury; TBI, traumatic brain injury; sTBI, severe traumatic brain injury.
Pooled proportion of mortality in patients with both sTBI and DAI
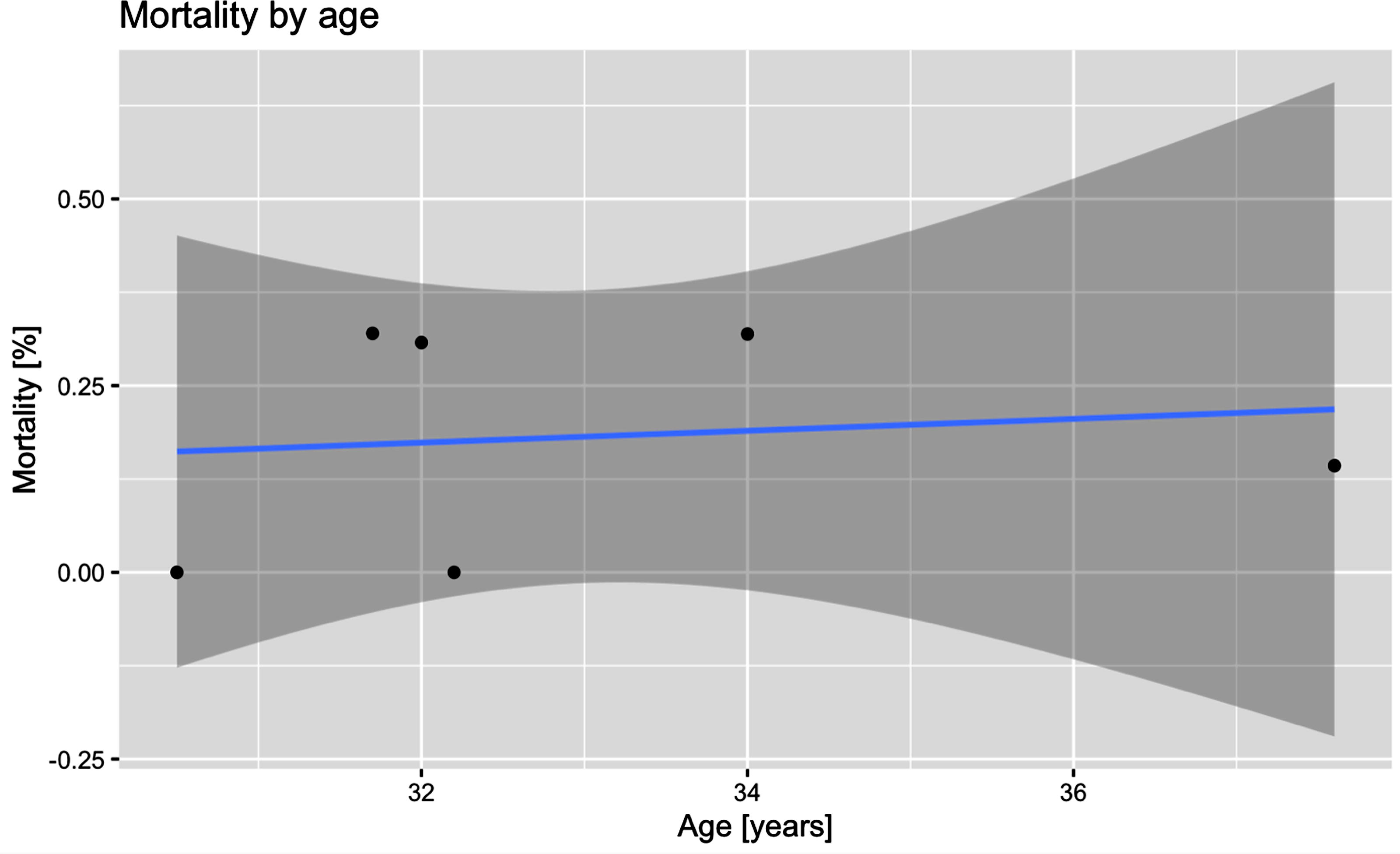
Among the 1607 patients we identified to have both sTBI and DAI, we found that the mortality data were given for 590 of them. Using the random effect model to adjust for the between-study variance (heterogeneity; I 2 = 12%) with respect to the mortality data presented in Figure 3, we found the pooled proportion of mortality among these 590 patients to be 0.16 [95% CI: 0.07, 0.30]. This suggests that among patients with sTBI and DAI, 16% die. A meta-regression showed no association between mean age and mortality, beta coefficient = 0.32 [95% CI: −0.42, 1.06], p = 0.40. Figure 5 presents the relationship between age and mortality in patients with sTBI and DAI.
Association between mean age as reported by the included studies and mortality in patients with sTBI and DAI. DAI, diffuse axonal injury; sTBI, severe traumatic brain injury.
Pooled proportion of males among patients with sTBI and DAI
Among the 1607 patients with sTBI and DAI, we identified 615 patients where we could determine their sex. This allowed us to determine the pooled proportion of males among patients with both sTBI and DAI. Using the random effect model to adjust for the between-study variance (heterogeneity; I 2 = 46%) with respect to the sex distribution data presented in Figure 4, we found the pooled proportion of males among these 615 patients to be 0.81 [95% CI: 0.76, 0.85]. This suggests that males make up 81% of patients with sTBI and DAI, an observation we suspect can be partially attributed to the increased tendency of males to engage in risky behavior that can result in head trauma, compared to that of females. However, none of the articles found any statistically significant differences with respect to outcomes between males and females with both sTBI and DAI.
Implications of heterogeneity and publication bias
The heterogeneity in our analyses ranges from 12% to 98%, and results should be interpreted accordingly. Furthermore, Supplementary Figures S1 to S3 show the funnel plots of the three meta-analyses that were conducted. The funnel plots show a high level of asymmetry, indicating a high heterogeneity in study results or a potential for publication bias. Since the heterogeneity (as measured by I 2) is very high, asymmetry in the funnel plots likely stems from a high heterogeneity in results.
Discussion
This study aimed to analyze the frequency and outcomes of DAI in patients with sTBI. Our findings contribute to the growing body of literature on the clinical implications of DAI, particularly regarding its frequency in sTBI, mortality among patients with both sTBI and DAI, and the proportion of males among individuals with both sTBI and DAI. Our systematic review and meta-analysis indicate a broad range of DAI incidence rates among patients with sTBI. The variation, ranging from 3.5% to over 80%, is largely attributable to differences in study populations and diagnostic criteria. Studies focusing on patients with clinical suspicion of DAI, often identified through prolonged unconsciousness, reported higher incidence rates. This finding aligns with previous research, suggesting that the diagnostic approach significantly influences reported incidence rates. 5,45
The pooled mortality rate of 16% among patients with sTBI and DAI underscores the impact of this injury type. Furthermore, the low heterogeneity (I 2 = 12%) suggests that differences in mortality data across the included studies are likely due to random variation, thereby affirming the reliability of our findings. However, it is important to contextualize this finding within the broader spectrum of TBIs. For example, acute subdural hematoma (ASDH), a prevalent neurosurgical emergency associated with sTBI, demonstrates markedly higher morbidity and mortality rates. Occurring in up to 70% of TBI cases, ASDH rapidly progresses in its acute phase with mortality rates reaching as high as 50%, underscoring its critical nature. This pronounced disparity in mortality rates between patients with sTBI experiencing DAI and those with traumatic ASDH underscores the variable clinical severity and outcomes inherent to different TBI types. Such differential mortality rates necessitate tailored therapeutic approaches and underscore the imperative for clinicians to prioritize specific treatment strategies based on the distinct injury characteristics and associated risks. 58 –63
Our analysis also highlights the prognostic significance of DAI stages. While stage III DAI is consistently associated with poor outcomes, the prognosis for stages I and II remains less clear. Some studies have reported worse outcomes for higher stages, yet others have found no significant differences. 33,36,42 This inconsistency may be due to small sample sizes and varying definitions of clinical outcomes used in these studies.
This variability in outcomes across stages has important implications for clinical management and patient counseling. Stage I DAI, confined to the cerebral hemispheres, generally has a more favorable prognosis. Patients with stage I injuries often experience shorter periods of unconsciousness and may have a higher likelihood of functional recovery. However, even mild DAI can lead to persistent cognitive deficits, particularly in areas such as attention and executive function. Stage II DAI, involving the corpus callosum, presents a more complex picture. These patients typically have longer periods of unconsciousness and may face more significant challenges in recovery. The involvement of the corpus callosum can disrupt interhemispheric communication, potentially leading to cognitive and motor coordination issues. Stage III DAI, extending to the brainstem, is associated with the poorest outcomes. Patients with stage III injuries often experience prolonged coma and have a higher risk of remaining in a persistent vegetative state or dying. The brainstem involvement can affect critical functions such as consciousness, respiration, and autonomic control, complicating treatment and rehabilitation efforts.
Understanding these stage-specific prognoses is crucial for tailoring treatment approaches. For instance, patients with stage I or II DAI might benefit from more aggressive early rehabilitation to capitalize on neuroplasticity, while those with stage III injuries may require more intensive supportive care and have different goals in their treatment plan.
One notable finding is the pronounced improvement in the Pediatric Glasgow Outcome Scale–Extended among pediatric patients with stages II and III DAI compared to those with stage I or no DAI. This finding challenges the conventional understanding of DAI severity and outcomes, particularly in the pediatric population. Several factors may contribute to this unexpected trend: Neuroplasticity: The developing brain in children demonstrates remarkable plasticity, potentially allowing for more effective rewiring and compensation following severe injuries. Differing injury mechanisms: The biomechanics of injury in children may result in different patterns of axonal damage compared to adults, possibly leading to more favorable outcomes despite apparent severity on imaging. Age-specific recovery patterns: Younger patients may have different recovery trajectories, with initial severity not necessarily predictive of long-term outcomes. Intensive care advancements: Improvements in pediatric neurocritical care may be particularly beneficial for more severe injuries, potentially mitigating the impact of higher-grade DAI.
This observation aligns with discussions at international neurotrauma congresses and underscores the need for age-specific prognostic models and tailored treatment approaches in pediatric TBI cases. Although there are few studies examining the relationship between DAI grade and neurological outcomes in the pediatric population, some studies support the conclusion that most severely injured children with severe DAI had favorable outcomes after long-term follow-up, despite having neurological deficits at discharge. 64,65
This result suggests that the extent of axonal damage and its anatomical distribution may differentially affect recovery trajectories in children. Although grade III DAI was reported to be significantly related to worse outcomes than grades I and II in earlier research on adult TBI patients by Kim et al., 41 the study by Hazwani et al., 27 involving pediatric patients, revealed improvements with time across all DAI grades. This discrepancy in results could be explained by variations in the pediatric age group’s neurons, developing brain tissues, and adult brain structures. Pediatric brains also exhibit a remarkable degree of plasticity, which might explain these differences in outcomes. 35 Further research is needed to elucidate the mechanisms behind this phenomenon and to develop targeted interventions that can optimize outcomes across all DAI stages in pediatric patients. Long-term follow-up studies and advanced neuroimaging techniques may provide additional insights into the recovery patterns and functional outcomes of children with different grades of DAI.
The clinical factors associated with DAI outcomes remain a subject of debate. While some studies have confirmed the correlation between the volume and number of DAI lesions and clinical prognosis, others have not. 28,53 The heterogeneity in these findings points to the need for standardized assessment methods and larger, multicenter studies to validate these associations. The retrospective study design, small sample size, variable outcome measures, follow-up time points, and inclusion of children with all severities of brain injury have all hampered research on early MRI predictors of outcome following pediatric TBI. Further research is necessary to determine whether early MRI can be used to improve prognosis and guide therapies, but it may also play a part in future clinical trials of novel TBI therapies by enabling subject stratification by lesion type (DAI vs. non-DAI), location (brainstem vs. cortex), or severity (total lesion burden). The use of MRI in the pediatric population with sTBI is not well-defined, and this diversity in MRI procedures underscores the need for more research to ascertain the usefulness, optimal time, and best composition of clinical MRI studies following TBI. 66
Developing precision medicine approaches for TBI requires a thorough understanding of the condition’s initial severity and the various pathoanatomical entities involved. Our findings underscore the importance of early and accurate diagnosis of DAI, as well as the need for tailored therapeutic strategies based on the stage and extent of axonal injury. 39,67
Limitations
This study has several limitations. First, the heterogeneity among the included studies for our pooled estimates may have affected the reliability of our estimates, specifically with respect to the frequency of DAI in patients with sTBI. Second, the retrospective nature of most studies included in our analysis limits the ability to establish causal relationships. Last variations in MRI protocols and diagnostic criteria for DAI across studies could lead to inconsistent reporting and classification of DAI.
Conclusions
In conclusion, DAI is a significant predictor of poor outcomes in sTBI patients, with a wide range of incidence rates influenced by diagnostic criteria and patient characteristics. The stage of DAI plays a crucial role in determining clinical outcomes, highlighting the need for early and accurate diagnosis. Given the lack of standardized neuroimaging guidelines for pediatric TBI cases, future research should focus on standardizing diagnostic criteria and exploring tailored treatment approaches to improve outcomes for patients with DAI.
Footnotes
Authors’ Contributions
V.S., S.L., A.D., and H.S. contributed to project planning, study design, and prepared the first draft of the article. E.O.R.N., P.H., P.S., A.S., and V.V.K.D. contributed to screening and data extraction. All authors read, edited, and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.